Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 18
Early and Long-Term Retention in Facility-Based HIV Pre-Exposure Prophylaxis Service Delivery Model Among Women at High Risk of HIV Acquisition in Tanga, Tanzania
Authors Mikomangwa WP ![]() , Moen K, Mmbaga EJ, Metta E
, Moen K, Mmbaga EJ, Metta E ![]() , Leshabari MT, Kibusi SM, Sudfeld CR, Bakari M, Kamuhabwa AAR, Kwesigabo GP
, Leshabari MT, Kibusi SM, Sudfeld CR, Bakari M, Kamuhabwa AAR, Kwesigabo GP
Received 19 February 2026
Accepted for publication 6 May 2026
Published 15 June 2026 Volume 2026:18 604257
DOI https://doi.org/10.2147/HIV.S604257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Wigilya P Mikomangwa,1– 3 Kåre Moen,2 Elia J Mmbaga,1,2 Emmy Metta,4 Melkizedeck T Leshabari,4 Stephen M Kibusi,5 Christopher R Sudfeld,3 Muhammad Bakari,6 Appolinary AR Kamuhabwa,7 Gideon Paul Kwesigabo1
1Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 2Department of Community Medicine and Global Health, University of Oslo, Oslo, Norway; 3Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston, MA, USA; 4Department of Behavioural Sciences, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 5Department of Public Health, University of Dodoma, Dodoma, Tanzania; 6Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 7Department of Clinical Pharmacy and Pharmacology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Correspondence: Wigilya P Mikomangwa, Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, Ilala, Dar es Salaam, Tanzania, Email [email protected]
Introduction: Retention in HIV pre-exposure prophylaxis (PrEP) care among key populations is crucial to realize its benefits. Evidence is scarce on retention in PrEP care outcomes and associated factors among at-risk women in sub-Saharan Africa. We, therefore, evaluated the retention outcomes in the facility-based PrEP services delivery model and their associated factors among female sex workers in the city of Tanga, Tanzania.
Methods: We analyzed data of 313 female sex workers of a control arm of a pragmatic trial. Participants were followed for 16 months from 2022 to 2023. We categorized retention in care outcomes PrEP services as being early and long-term. A multivariable log-binomial regression model was used to determine factors affecting retention in PrEP services at p< 0.05.
Results: Early and long-term retention in PrEP care was 38.0% (95% CI: 33.25– 43.04) and 11.0% (95% CI: 7.67– 15.61), respectively. Having sex work as the only source of income negatively affected early retention compared to those with alternative sources of income (aRR 0.58, 95% CI: 0.36– 0.94, p=0.028). Having 10– 29 sexual clients/month was 34% times lower risk of being retained compared to those with less than 10 sexual clients per month (aRR 0.66, 95% CI: 0.47– 0.92, p=0.014). Self-perceived “high” PrEP stigma negatively affected long-term retention compared to perceiving “low” PrEP stigma (aRR 0.16, 95% CI: 0.03– 0.99, p=0.049) and self-perceived “moderate” HIV risk was associated with increased retention compared to self-perceived “high” HIV risk (aRR 5.03, 95% CI: 1.37– 18.47, p=0.015).
Conclusion: The retention in facility-based HIV PrEP care among female sex workers was low. Having sex work as the only source of income, having sex with 10– 29 clients, and self-perceived “high” PrEP stigma negatively affected retention in PrEP care. Self-perceived “moderate” HIV risk positively affected retention in PrEP care. Establishing client-centred approaches targeting PrEP stigma and HIV risk awareness is crucial to optimize retention in facility-based PrEP services.
Trial Registration: Pan African Clinical Trials Registry PACTR202003823226570.
Keywords: HIV facility-based PrEP service delivery model, PrEP, HIV, women at risk of HIV, female sex workers
Introduction
The implementation of pre-exposure prophylaxis (PrEP) services among members of key and vulnerable populations will contribute to ending the HIV epidemic by 2030. It is estimated that the wide use of PrEP services is likely to reduce HIV incidence at the population level by up to 40%.1 Nevertheless, the effectiveness of PrEP is primarily determined by adherence, which is influenced by the retention in PrEP services.2 To achieve a high level of impact of PrEP at the population level, retention in PrEP services among people at high risk of HIV is of paramount importance.1,3,4 However, it has been reported that less than half of initiators are retained in PrEP services within 6 months after initiation3,5,6 with Sub-Saharan Africa having the lowest retention rate (47.5%) than other world regions.6 Low retention in PrEP services deters the overall benefits of PrEP in reducing HIV incidences.
Low retention in PrEP care is linked to operational, clinical, behavioral, and social-demographic factors such as high cost, healthcare providers’ negative attitudes toward PrEP, mobility for sex work, high stigma, perceived low HIV risk, young age and place of residence among others.7–17 The knowledge about these factors has mainly been generated from studies among transgender, bisexuals, and men who have sex with men, with limited data from female sex workers.15–17 Retention in PrEP care outcomes and their associated factors have been well studied in the context of clinical trials and demonstration projects but remain understudied in real-world settings among female sex workers. There have been some real-life studies, including one in Rwanda, which reported a 12-month retention of 53.4% and cited inconsistent condom use as a factor of discontinuing PrEP care.18
In 2018, the Ministry of Health in Tanzania rolled out PrEP as a small-scale intervention, and the following year, it updated the HIV management guideline to include PrEP and then scaled up PrEP services in 2021.19 An estimated 515,410 members of key and vulnerable populations are eligible for PrEP, and 24% of these are female sex workers.20 According to the Global PrEP Tracker (AVAC: (prepwatch.org)), from 2018 to the first quarter of 2024, Tanzania has an estimated cumulative total of 334,432 PrEP initiators. Nevertheless, the retention rates and associated factors among initiators are poorly understood in these settings. Therefore, our study aimed to determine the retention in PrEP care outcomes and the associated factors among female sex workers in Tanzania. The findings are intended to inform work aiming to improve retention in PrEP care among female sex workers.
Methods
Study Design, Setting, Recruitment, and Follow-Up Procedures
We conducted observational longitudinal analysis of data from the control group nested within a pragmatic quasi-experimental trial for HIV pre-exposure prophylaxis rollout in Tanzania (PREPTA), which was conducted from March 2021 to June 2023.21–23 Study participants (n=470) in the intervention arm (in the city of Dar es Salaam) received a mHealth intervention, ie they were given a smartphone app intended to support them in adhering to PrEP and remaining in PrEP care. The control group (in the city of Tanga) received standard PrEP care (n=313). Our analyses in this paper focus on the latter cohort of female sex workers. They followed all the procedures for PrEP use as per routine clinical practice in Tanzania including eligibility criteria, attendance schedules for PrEP refill, and counseling on PrEP use and harm reduction;20 participants were prescribed monthly PrEP pills (30 tablets containing 200 mg of emtricitabine and 300 mg of Tenofovir Disoproxil Fumarate) and were required to return for refill visits every month after initiation. The only differences when compared to routine PrEP clients were that the clinic files of the study participants had unique identification numbers (so that their clinic attendance could be traced) and that they were contacted (by peer educators) and asked to attend interviews (about PrEP use and sexual behavior) at month 1, 6, and 12 (and were compensated for their fare in connection with these interviews). After 12 months, participants were followed up for another 4 months to document their attendance at the PrEP clinic. Therefore, this paper presents analysis from the observational longitudinal data among female sex workers who were followed up for 16 months to understand the retention patterns to facility-based PrEP care as described in Figure 1. To better understand the retention in facility-based PrEP care and its factors, we utilized Health Belief Model (HBM) constructs which are useful in explaining and predicting health behavior as well as studying preventive behavior and service utilization.24
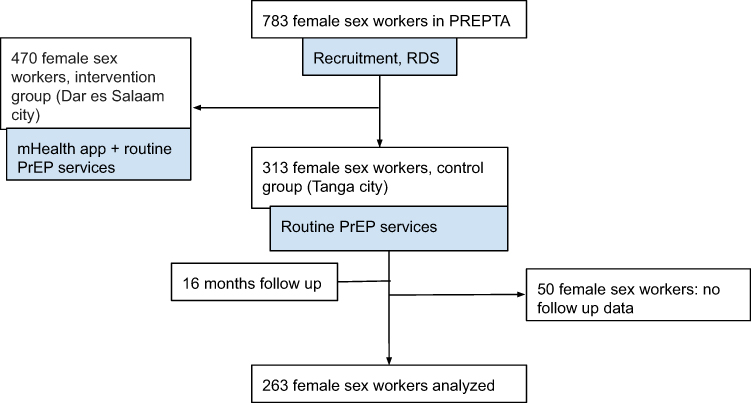 |
Figure 1 Study flow. Abbreviations: mHealth app, mobile health application; PrEP, HIV pre-exposure prophylaxis; RDS, Respondent-driven sampling; PREPTA, Pragmatic Trial for HIV Pre-Exposure Prophylaxis Roll-Out in Tanzania. |
Study Population, Sampling Technique, and Study Power
The details of the study population and sampling technique population have been published.21,22 Briefly, we recruited women who had sold sex during the 3 last months preceding the study, were aged 18 years or older, had been living in the city of Tanga for at least 6 months, met the criteria for PrEP use as per the Tanzanian guidelines, and consented to take part in the study. In this analysis, we included 263 female sex workers who made up the control group of the PREPTA study. They had been recruited through respondent-driven sampling. The sample size in the PREPTA project was obtained by adopting respondent-driven sampling for cohort studies as described by Kirkwood.25 The final sample size of 263 gave a statistical power of 80%, assuming a 15% change in retention rates from initiation and a 20% attrition rate with a 95% confidence interval.
Data Collection
Trained research assistants collected data using online Swahili questionnaires. The collected data were directly sent to Tjenester for Sensitive Data (Norwegian for “Services for Sensitive Data” and abbreviated TSD), an electronic system hosted by the University of Oslo. There were three types of questionnaires: The first was used at month 1 and collected information related to PrEP initiation. The second questionnaire was used at months 6 and 12 and was used to collect information on sexual behaviour, clinical, and PrEP use. The third was a data extraction form used to collect data from clinical files about monthly PrEP refill visits from initiation up to 16 months. The refill questionnaire contained sections on dates for PrEP initiation, PrEP refill appointment, actual presentation at the clinic and date of next appointment, HIV test results, and estimated glomerular filtration rate (estimated using serum creatinine clearance). It also contained information on the status of PrEP use (either continuing, stopped/discontinued, or restarted), reason(s) for stopping/discontinuing, and number of pills dispensed.
Outcome Variables
The primary study outcome was retention in PrEP care outcomes categorized as early and long-term retention in PrEP care. We defined early retention as attending 2 or more PrEP refill visits in the first 6 months after initiation. Long-term retention in PrEP care was defined as the cumulative proportion of participants attending three or more PrEP refill visits in the first 16 months after PrEP initiation, more specifically: attending 2 or more refill visits in the first 6 months and at least one additional visit between 6 and 16 months after PrEP initiation. Participants were considered to have dropped out from PrEP care if they did not attend the clinic during the first 6 months after PrEP initiation or if they did not return to the clinic during the 10-month window (6–16 months) or if self-reported stopping using PrEP. Both the early and long-term retentions were documented as binary outcomes, ie. retained versus non-retained. These definitions were informed by real-world practice in our settings and other studies15,26 considering changes in patterns of risky sexual behaviour of female sex workers.15,26 We observed that female sex workers were not at all-time high risk as more than half had less than 30 sexual clients per month (54.5%), and of these 25% had less than 10 sexual clients. This means they were not practising sex work on other days of the month. We also noted that those who did not have sex or used condoms never used the PrEP pill: 90.3% of follow-up participants were still using the previous PrEP pills. Additionally, we determined the timing of PrEP refill visits, reasons for delayed attendance of scheduled PrEP refill visits, and factors influencing early and long-term retention in PrEP care. This approach was chosen deliberately to reflect the programmatic reality of facility-based PrEP delivery in a pragmatic trial setting, where visit timing is often irregular and influenced by mobility, service access, and structural barriers. Our refill-based definition therefore captures engagement with PrEP services over time, rather than strict adherence to scheduled visit dates.
Exposure Variables
The HBM constructs guided the selection of exposure variables. i) Self-perceived susceptibility to HIV acquisition was categorized as “high”, “moderate”, and “low or no” HIV risk. ii) Perceived barriers to remaining in PrEP care: Social support, sex work stigma, PrEP stigma, migration for sex work, and source of income. iii) PrEP self-efficacy was categorized as “high” if scored >18 and “low” if scored ≤18. iv) Sociodemographic and structural variables: Age, PrEP knowledge, education level, and living arrangements. Alcohol use was assessed using the Alcohol Use Disorder Identification Test (AUDIT) scores; categorized as “low risk” (score ≤7), “harmful” or “hazardous” (score 8–14), and “dependence” (score >14). We assessed social support using the Duke-UNC Functional Social Support Questionnaire (FSSQ, α=0.88). A score <32 denoted inadequate social support (score <32), while adequate social support included a score ≥32. Knowledge of PrEP was assessed using true or false questions and participants with a score above 75% were considered to have adequate knowledge. Perceived PrEP stigma (α=0.88) was categorized as low if scored ≤30 and high if otherwise. Sex work stigma (α=0.84) was classified as either low (scores ≤26); moderate (scores 27–38), or high (scores ≥39).27
Data Analysis
We conducted a descriptive analysis of sociodemographic and structural factors, self-perceived HIV risk, PrEP self-efficacy, perceived barriers against PrEP use, and visits to PrEP refill services. We reported these as proportions and frequencies for categorical variables and medians with a 25%–75% interquartile range (IQR) for continuous variables.
The number of days from PrEP initiation until the person presented at the clinic for the PrEP follow-up visit was used to calculate the time (in months) and to categorize study participants as either being retained in care or discontinued from care as per the definition of retention mentioned above. The delay in follow-up visits was calculated as the number of days from the scheduled appointment date to the presentation date at the PrEP clinic. For each exposure-outcome pair, the log-binomial regression model with the clustered robust standard error was used to determine the factors associated with the retention in PrEP services at a 95% confidence interval (CI) and a p-value <0.05. The model with the lowest Akaike Information Criterion value was considered optimal. All models converged without warning ie, convergence was achieved within the default iteration limits. The regression analysis was not conducted for the effect of PrEP self-efficacy on retention in PrEP care due to few observations in the low category (2/312, 0.6%): only variables with >10 observations were included in the analysis. To avoid multivariable model misinterpretation, only the primary exposure–outcome relations were presented. Notably, the multivariable analysis had small sample size, so we conducted this analysis as exploratory, with the aim of identifying factors associated with long-term PrEP retention. The analysis used STATA version 18 (Stata Corp., College Station, TX).
Confounders
The confounders were determined using a directed acyclic graph (DAG). We determined the confounders for each exposure-outcome pair using dagitty.net.28 Some of the exposures were confounders for other exposure-outcome pairs. Age was the confounder for all pairs and was adjusted as a continuous variable. We adjusted for any condom use (during vaginal or anal sex). Any experience of physical violence was considered gender-based violence. The set of confounders was adjusted for the total effect of exposure on the outcome.
Handling of Missing Data
Missing data for covariates were minimal and were handled using complete-case analysis. Participants who did not attend a given interview were not excluded from the study but contributed data at other time points where available.
Patient and Public Involvement
The public was involved in the design or conduct of the study or reporting or dissemination plans of our research.
Results
Participant Characteristics
A total of 263 female sex workers were and included in the analysis with mean (SD) age of 28.6 (6.1) years. Of all participants (n=263), 119 (45.2%) had completed primary education. Most were not married 171/263 (65.0%) and were living with family 205/263 (77.9%). Of women who reported alcohol use (n=256), about three-quarters 198 (77.3%) were classified as alcohol dependent, and 190/263 (72.2%) were self-perceived to be at high risk of HIV. Participants who reported social support (n=250), 134 (53.6%) said that they had adequate social support. One hundred and sixty-three of 255 women (63.9%) reported that they experienced “moderate” sex work stigma, and 106/260 (40.8%) reported that they had experienced physical violence during sex work. The majority 206/257 (80.2%) were classified as experiencing “low” degrees of PrEP stigma. Of all participants (n=263), 124 (47.1%) did not use condoms at the previous vaginal sex with a client. Among participants who reported anal sex (n=194), 130 (67.0%) had had condomless sex the last time they had anal sex with a client. As for the number of sex clients per month (n=263), 118 (44.9%) had more than thirty (≥30). Female sex workers (n=263), 118 (41.1%) reported to have experienced financial difficulties to spend on health. More than half 148/263 (56.3%) reported having travelled for sex work in the last 6 months. The PrEP knowledge was classified as inadequate for 170/263 (64.6%) of the study participants, and PrEP self-efficacy was high 260/261 (99.4%). The socio-demographic and sexual behaviour of study participants are described in Table 1.
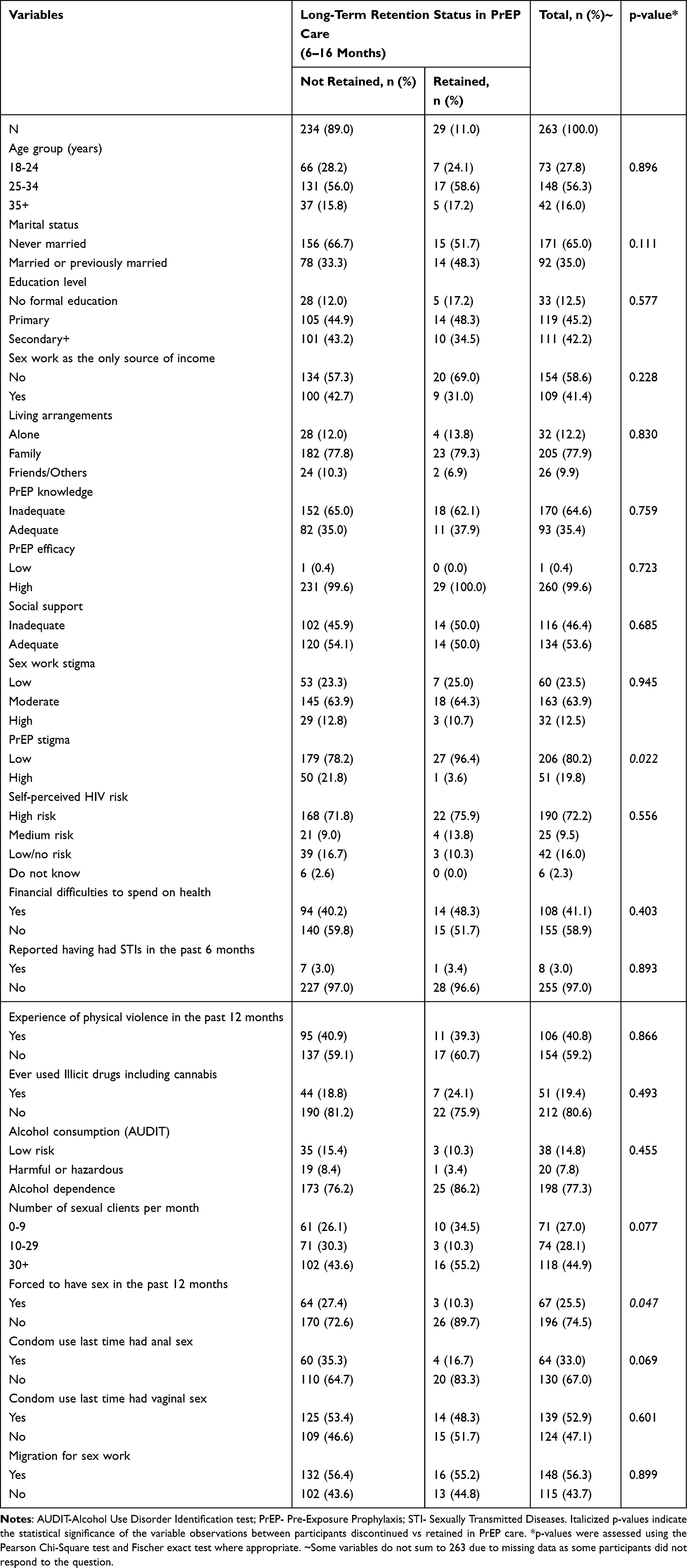 |
Table 1 Distribution of Socio-Demographic and Sexual Behaviour Characteristics by Long-Term Retention Status in PrEP Care Among Female Sex Workers in the City of Tanga, Tanzania (N=263) |
Of 263 participants who reported the primary place for sex work, 210 (79.9%) said they do sex work in a bar/pub/club or disco, 37 (14.1%) via online platforms (such as telephones), 7 (2.7%) through guesthouses/hotels/rented rooms, 4 (1.5%) in a brothel, and 5 (1.9%) in other places (did not prefer to mention). At baseline (n=263), 8 (3.0%) had a history of STIs, and 3 (1.1%) participants had a positive test for hepatitis B virus (HBsAg+). During follow-up (n=263), 1 (0.4%) of the study participants became HIV infected.
Factors Associated with Early Retention
The early retention in care (ie. the proportion who remained in care after 6 months) was 100/263 (38.0%; 95% CI: 33.25–43.04). Participants who had sex work as the only source of income had a 42% lower risk of being retained in PrEP care 6 months after initiation compared to those who had alternative sources of income (aRR 0.58, 95% CI: 0.36–0.94, p = 0.028). Female sex workers who self-perceived to have a “medium” risk of acquiring HIV were 64% more likely to be retained than those who self-perceived to have a “high” HIV risk (aRR 1.64, 95% CI: 1.12–2.41, p=0.011). Participants who had from 10 to 29 sex clients per month were 34% less likely to remain in PrEP care after 6 months than those who had less than 10 clients per month (aRR 0.66, 95% CI: 0.47–0.92, p=0.014). Table 2
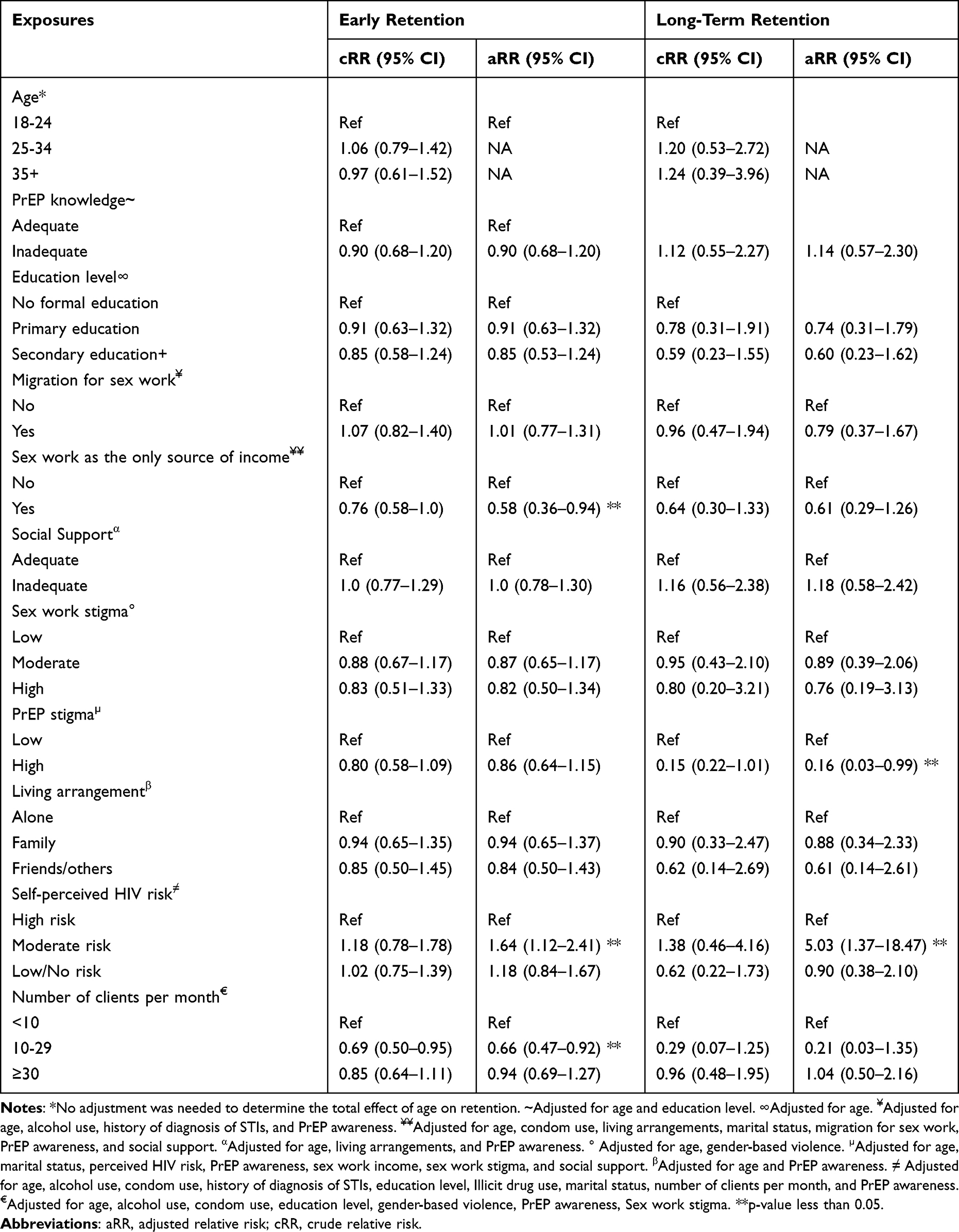 |
Table 2 Log-Binomial Regression Analysis of Independent Factors Associated with Early and Long-Term Retention in Facility-Based PrEP Care Among Female Sex Workers in the City of Tanga, Tanzania |
Factors Associated with Long-Term Retention
The long-term retention in facility-based PrEP care, defined as retention between 6 and 16 months, was 29/263 (11.0%; 95% CI: 7.67–15.61). Female sex workers who experienced high PrEP stigma were 84% less likely to be retained in PrEP care in the longer term than those who experienced low PrEP stigma (aRR 0.16, 95% CI: 0.03–0.99, p=0.049). Female sex workers who self-perceived to have a medium risk of acquiring HIV were five times more likely to be retained in facility-based PrEP care than those who self-perceived to have a high HIV risk (aRR 5.03, 95% CI: 1.37–18.47, p=0.015). Table 2
There was a delay in attending scheduled PrEP refill visits of 71 days (IQR: 7–144). Participants attended the first PrEP refill visit at a median of 88 days after PrEP initiation. The highest delay pertained to the 2nd visit, with 98 days (IQR: 11–144) followed by the first visit, with a delay of 58 days (IQR: 7–147) from the scheduled date (Table S1). Of all participants (n=263), 9 (3.4%) attended from 1 to 8 days earlier than the scheduled date, and 24/263 (9.2%) attended exactly as expected.
Reasons for Missing Scheduled PrEP Refill Clinic Visits
Overall, 175/255 (68.6%) women reported having scheduled appointments on first PrEP refill. Of 175 women who had scheduled refill appointments, 126 (72.0%) did not attend as scheduled. The common reasons for missing the scheduled PrEP refill visits were being out of the city (50.4%), having busy schedules with work or family matters (29.6%), and forgetting the appointment (12.8%). Figure 2
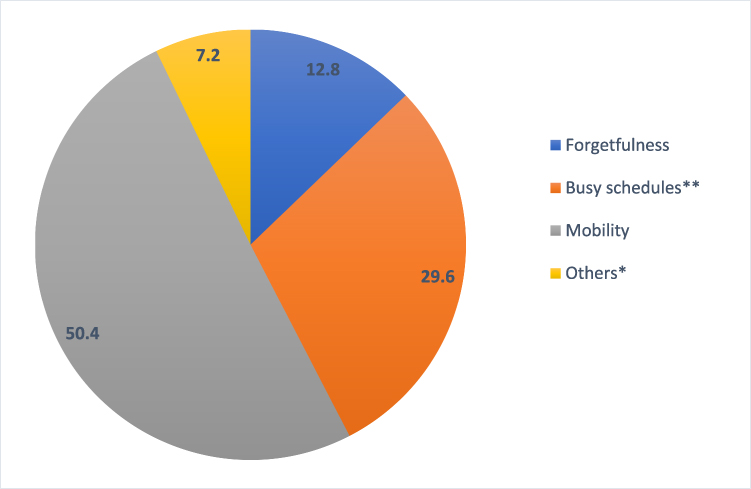 |
Figure 2 The proportion of reasons for missing scheduled PrEP refill appointments among female sex workers in the City of Tanga, Tanzania. *Frequency of other reasons: clinic was far (n=1), not sure needed to continue using PrEP (n=1), was sick (n=4), not used the PrEP pill (n=1), stopped by husband (n=1) and did not know the place to attend for refill (n=1). ** Busy with work or family matters. |
Discussion
We evaluated the early and long-term retention, as well as the associated factors, in facility-based PrEP care among female sex workers in the city of Tanga, Tanzania. The retention rate after 6 and 6–16 months was 38.0% and 11.0%, respectively. The factors that negatively influenced early retention were having sex work as the only source of income and having between 10 and 30 sex clients per month, whereas having a self-perceived moderate HIV risk was positively associated with early retention in PrEP care. Self-perceived high PrEP stigma negatively affected long-term retention and self-perceived moderate HIV risk positively affected retention in PrEP care among female sex workers.
The retention in PrEP care in our study was lower than in demonstration projects in sub-Saharan Africa involving female sex workers. For instance, the retention rate in Senegal at 6 and 12 months was 79.9% and 73.4%, respectively,16 and in Benin, it was 73.8%, 53.8%, and 54.7% at 6, 15 and 18 months,29 respectively. In the Democratic Republic of Congo, the 6-month retention rate was 86.6%.30 In these studies, researchers actively followed up PrEP users by sending reminders for their clinic appointments and, in some cases, conducting follow-up visits at the client’s homes or workplaces which may present pseudo-retention. In contrast, in our study, participants were not contacted in connection with clinical follow-up/refill visits (they were only contacted to return for face-to-face interviews, which were conducted independently of the clinical visits). Creating artificial conditions, such as active follow-up to promote clinical visits, payment of transport fares, or other incentives to attend clinics, as commonly done in clinical trials, can inflate retention rates and lead to what is known as pseudo-retention. Nevertheless, our study participants were recruited through RDS. They did not make an independent decision to start PrEP entirely on their own but were encouraged to enroll in the study. We may, therefore, have recruited women who were not so motivated to use PrEP at the outset, which may explain the low retention rates in the six months after PrEP initiation. Thus, differences in design could be the reason for the differences in retention rates between our study and the others mentioned. The lower retention rates in our study provide insights into the PrEP care implementation gap in Tanzania, which needs to be addressed to optimize retention.
Nevertheless, we found reduced rates of retention among female sex workers who self-perceived high PrEP stigma, similar to previous studies.7,31 PrEP use has been linked to HIV treatment due to the resemblance of the pills and packages to antiretroviral therapy pills.32 Also, PrEP services in Tanzania are provided at the Care and Treatment Clinics for people living with HIV, which may result in the misconception of PrEP users as HIV-positive, leading to stigma. Sometimes, female sex workers might not have individually experienced PrEP stigma, but they are aware of its existence in the community leading to fear of anticipated stigma, which interferes with retention in facility-based PrEP services.7,32 Thus, addressing PrEP stigma is crucial in optimizing retention in PrEP care among female sex workers.
Understanding the HIV risk and the desire to remain negative could be the reason for the high retention rate among those who self-perceived to have a moderate HIV risk. Self-perceived HIV risk is a known factor that influences the uptake and retention in PrEP care.31 We found that most participants self-perceived to have a moderate-to-high risk of HIV, implying an understanding of their substantial risk of HIV. Although there are no published findings on the link between number of sexual clients and self perceived HIV risk, we hypothesize the low PrEP retention rate among female sex workers who had few sexual clients (10–29) was due to self-perceiving at low risk. These participants had on average less than one sexual client per day per month which is considered a low number for them to perceive at high risk of HIV. It has been reported that members of key populations remain in PrEP care if they self-perceive high risk of HIV and discontinue if otherwise.33,34 This is in line with the HBM by which female sex workers perceived HIV as severe and felt more susceptible to HIV infection than the general population; these motivated them to be retained in PrEP care. However, due to the dynamic nature and seasonality of the risky behaviour of female sex workers, it is recommended to regularly assess HIV risk coupled with STI, hepatitis B, and HIV testing services during PrEP implementation.19,35,36 HIV risk assessment is encouraged to be routinely done during PrEP refill visits and determines the need to continue using PrEP.
Participants whose sex work was the only source of income had a high risk of not being retained in PrEP services. Financial factors such as out-of-pocket PrEP services and transportation costs have been found to adversely affect the retention in PrEP services.37 Hence, female sex workers may be discontinuing PrEP service to reduce costs associated with PrEP refill attendance. The PrEP initiators require transport fares and in other countries, are required to pay for the PrEP services, this is viewed as a barrier to retention in PrEP care.37 In Tanzania, PrEP care is provided free of charge and to overcome cost as a barrier it also implements community outreach programs for initiation and PrEP refills in line with the facility-based PrEP services, yet the retention is still low. Thus, factors that affect retention are multifaceted and require multiple approaches to overcome.
According to the guidelines, eligible PrEP clients in Tanzania are given a 3-month prescription but are required to pick up the pills every month at the facility and are considered to have discontinued PrEP care if they delay scheduled appointments for more than 90 days.20 We observed consistent delays in the scheduled visits, with the longest delay occurring on the second visit. A study conducted among men who have sex with men and transgender women in the US reported wide variability in days between the scheduled date and actual presentation to the PrEP care.15 There is a lack of published literature on the reasons for delayed presentation to PrEP care; however, we found that mobility, busy schedules, and forgetfulness are the most common reasons for missing scheduled PrEP refills. Also, alternative explanations for missing scheduled PrEP refill visits could be short refill dates which made female sex workers fail to attend clinics as expected. This calls for assessing the feasibility of 3-monthly PrEP pill dispensation at initiation, contrary to the current practice of monthly dispensation and refill visits.
Limitations
Our analysis was limited to female sex workers; therefore, generalizability may not apply to other members of key and vulnerable populations, including people who inject drugs, and men who have sex with men. The small sample size used in the multivariable analysis could have led to underpowered and unstable estimates affecting the generalizability of the study findings in the same population; therefore, findings should be interpreted with caution. Since this study was part of the trial, it could have affected the outcomes, as participants were paid compensation for attending interviews at months 1, 6, and 12. We did not accurately measure the exact discontinuation date due to cessation of risk versus discontinuation despite the ongoing risk of the confounders used in the model mentioned are time-varying confounders; however, the regression model used considers them as static (ie, condom use, and exposure to physical violence). Therefore, the findings should be interpreted with caution. The qualitative analysis of the interviews with those who discontinued and were indicated for PrEP is not in the scope of this paper.38 We used HBM constructs to select exposure variables. However, it primarily addresses individual perceptions and may not fully capture social, structural, or temporal factors influencing PrEP retention. Additionally, it assumes rational decision-making and does not account for dynamic interactions between constructs, which should be considered when interpreting the findings. The definitions of early and long-term retention are not based on exact visit timing but rather on the number of PrEP refills obtained within predefined follow-up intervals. However, strict time-based definitions would likely overestimate discontinuation and underestimate real-world PrEP retention in this highly mobile population. More granular visit and dispensing data in future studies would better distinguish continuous use from intermittent gaps.
Conclusion and Recommendation
The early- and long-term retention in facility-based PrEP services among female sex workers was low. Having sex work as the only source of income, self-perceiving “high” PrEP stigma and having 10–29 sexual clients per month negatively influenced retention in PrEP care. Female sex workers who perceived themselves to be at moderate risk of HIV were more likely to continue attending facility-based PrEP services. Our study highlights the need to establish a client-centred approach by identifying services that should be provided during PrEP care. Approaches to address PrEP stigma and enhancing understanding of the HIV risk among female sex workers are crucial to optimize retention in facility-based PrEP services delivery. Interventions to increase retention in PrEP care should consider the reasons for missing appointments. This was an exploratory analysis and studies with larger samples conducted outside of clinical trials are needed to confirm findings.
Abbreviations
HIV, Human Immunodeficiency Virus; PrEP, Pre-Exposure Prophylaxis; PREPTA, Pragmatic Trial for HIV Pre-Exposure Prophylaxis Roll-Out in Tanzania.
Data Sharing Statement
All data are available upon reasonable request. The request for data can be sent to the PREPTA principal investigator: Prof. Elia J Mmbaga; Email: [email protected].
Ethics Approval and Consent to Participate
Participants consented freely without coercion using the Swahili language (Tanzania National language). The refund of costs in connection with travel was given for transport fare only. Considering that sex work is a criminal act in Tanzania, protection of highly sensitive data, privacy, and confidentiality was employed to prevent divulging which could result in legal action being taken. The project had ethical clearance from MUHAS (MUHAS-REC-10-2019-057) and the National Institute for Medical Research (NIMR) (NIMR/HQ/R.8a/Vol.IX/3454). The project was funded by the Norwegian Research Council and hence, received ethical clearance in Norway by the “Regional Ethical Committee (REC)”. The study was conducted according to the Helsinki Declaration. All the information obtained from this study was used for research purposes only and not shared with anyone without the participants’ consent. Participants gave written informed consent to participate in the study.
Acknowledgments
We thank all the female sex workers who agreed to participate in the study. Thanks to the research assistant team, who tirelessly supported data collection from baseline to the follow-up stages. Special thanks to Dr. Christopher Mbotwa, a biostatistician, for his statistical assistance and guidance during data analysis.
Funding
The Research Council of Norway funded the PREPTA project through the Global Health and Vaccination Programme (GLOBVAC), project number 285361. The project is also part of the European & Developing Countries Clinical Trials Partnership (EDCTP2) program supported by the European Union. Also, the Norwegian Programme for Capacity Development in Higher Education and Research for Development (NORAD) funded the implementation of a project entitled “Strengthening Doctoral Education for Health in Tanzania (DOCEHTA)” through which the corresponding author was sponsored. The HIS project through an NIH D43 grant partly funded the study on the follow-up stage post-12 months.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pyra MN, Haberer JE, Hasen N, Reed J, Mugo NR, Baeten JM. Global implementation of PrEP for HIV prevention: setting expectations for impact. J Int AIDS Soc. 2019;22(8):1–13. doi:10.1002/jia2.25370
2. Chan PA, Mena L, Patel R, et al. Retention in care outcomes for HIV pre-exposure prophylaxis implementation programmes among men who have sex with men in three US cities. J Int AIDS Soc. 2016;19(1):1–8. doi:10.7448/IAS.19.1.20903
3. Bavinton BR, Grulich AE. HIV pre-exposure prophylaxis: scaling up for impact now and in the future. Lancet Public Heal. 2021;6(7):e528–e533. doi:10.1016/S2468-2667(21)00112-2
4. Wu L, Schumacher C, Chandran A, et al. Patterns of PrEP retention among HIV pre-exposure prophylaxis users in Baltimore City, Maryland. J Acquir Immune Defic Syndr. 2020;85(5):593–600. doi:10.1097/QAI.0000000000002506
5. Delany-Moretlwe S, Chersich M, Harvey S, et al. Empowerment clubs did not increase PrEP continuation among adolescent girls and young women in South Africa and Tanzania-results from the EMPOWER randomised trial. In:
6. Zhang J, Li C, Xu J, et al. Discontinuation, suboptimal adherence, and reinitiation of oral HIV pre-exposure prophylaxis: a global systematic review and meta-analysis. Lancet HIV. 2022;9(4):e254–e268. doi:10.1016/S2352-3018(22)00030-3
7. Arnold T, Brinkley-Rubinstein L, Chan PA, et al. Social, structural, behavioral and clinical factors influencing retention in pre-exposure prophylaxis (PrEP) care in Mississippi. PLoS One. 2017;12(2):e0172354. doi:10.1371/journal.pone.0172354
8. Marks SJ, Merchant RC, Clark MA, et al. Potential healthcare insurance and provider barriers to pre-exposure prophylaxis utilization among young men who have sex with men. AIDS Patient Care STDS. 2017;31(11):470–478. doi:10.1089/apc.2017.0171
9. Brooks RA, Allen VC, Regan R, Mutchler MG, Cervantes-Tadeo R, Lee SJ. HIV/AIDS conspiracy beliefs and intention to adopt preexposure prophylaxis among black men who have sex with men in Los Angeles. Int J STD AIDS. 2018;29(4):375–381. doi:10.1177/0956462417727691
10. Schwartz J, Grimm J. Stigma communication surrounding PrEP: the experiences of a sample of men who have sex with men. Health Commun. 2019;34(1):84–90. doi:10.1080/10410236.2017.1384430
11. Gallagher T, Link L, Ramos M, Bottger E, Aberg J, Daskalakis D. Self-perception of HIV risk and candidacy for pre-exposure prophylaxis among men who have sex with men testing for HIV at commercial sex venues in New York City. LGBT Heal. 2014;1(3):218–224. doi:10.1089/lgbt.2013.0046
12. Lelutiu-Weinberger C, Golub SA. Enhancing PrEP access for black and latino men who have sex with men. J Acquired Immun Deficiency Syndr. 2016;73(5):547–555. doi:10.1097/QAI.0000000000001140
13. Petroll AE, Walsh JL, Owczarzak JL, McAuliffe TL, Bogart LM, Kelly JA. PrEP awareness, familiarity, comfort, and prescribing experience among US primary care providers and HIV specialists. AIDS Behav. 2017;21(5):1256–1267. doi:10.1007/s10461-016-1625-1
14. Franks J, Hirsch-Moverman Y, Loquere AS, et al. Sex, PrEP, and stigma: experiences with HIV pre-exposure prophylaxis among New York City MSM participating in the HPTN 067/ADAPT study. AIDS Behav. 2018;22(4):1139–1149. doi:10.1007/s10461-017-1964-6
15. Chan PA, Patel RR, Mena L, et al. Long-term retention in pre-exposure prophylaxis care among men who have sex with men and transgender women in the United States. J Int AIDS Soc. 2019;22(8):1–9. doi:10.1002/jia2.25385
16. Sarr M, Gueye D, Mboup A, et al. Uptake, retention, and outcomes in a demonstration project of pre-exposure prophylaxis among female sex workers in public health centers in Senegal. Int J STD AIDS. 2020;31(11):1063–1072. doi:10.1177/0956462420943704
17. Kagaayi J, Batte J, Nakawooya H, et al. Uptake and retention on HIV pre-exposure prophylaxis among key and priority populations in South-Central Uganda. J Int AIDS Soc. 2020;23(8). doi:10.1002/jia2.25588
18. Mubezi S, Rwibasira GN, Uwineza J, et al. Factors associated with retention on pre-exposure prophylaxis among female sex workers in Kigali, Rwanda. PLOS Glob Public Heal. 2023;3(11):e0002524. doi:10.1371/journal.pgph.0002524
19. Tanzania Ministry of Health. National guidelines for the management of HIV and AIDS. 2020.
20. United Republic of Tanzania Ministry of Health, Community Development, National Aids Control. Program implementation framework for pre-exposure prophylaxis of HIV in Tanzania Mainland. Minist Health Commun Dev Gender Elder Child. 2021;(May):10–15.
21. Mbotwa C, Kazaura M, Moen K, et al. Predictors of mHealth use in promoting adherence to pre-exposure prophylaxis among female sex workers: an evaluation of the Jichunge intervention in Dar es Salaam, Tanzania. BMC Health Serv Res. 2022;22(1):1–12. doi:10.1186/s12913-022-08245-2
22. Lichtwarck HO, Mbotwa CH, Kazaura MR, Moen K, Mmbaga EJ. Early disengagement from HIV pre-exposure prophylaxis services and associated factors among female sex workers in Dar es Salaam, Tanzania: a socioecological approach. BMJ Glob Heal. 2023;8(12):e013662. doi:10.1136/bmjgh-2023-013662
23. Haaland I, Metta E, Moen K. The use of PrEP among men who have sex with men and transgender women as biomedical prevention work: a conceptual framework. Soc Sci Med. 2023;333(November 2022):116147. doi:10.1016/j.socscimed.2023.116147
24. Rejeski WJ, Fanning J. Models and theories of health behavior and clinical interventions in aging: a contemporary, integrative approach. Clin Interv Aging. 2019;14:1007–1019. doi:10.2147/CIA.S206974
25. Kirkwood BR, Sterne JA. Essential Medical Statistics, 2nd Edition.
26. Burns CM, Borges M, Frye J, et al. Understanding retention in pre-exposure prophylaxis care in the South: insights from an academic HIV prevention clinic. AIDS Res Hum Retroviruses. 2022;38(4):306–312. doi:10.1089/aid.2021.0177
27. Mikomangwa WP, Moen K, Mmbaga EJ, et al. HIV pre-exposure prophylaxis use during periods of unprotected sex among female sex workers in Tanga city, Tanzania: a control arm analysis of the pragmatic quasi-experimental trial. Front Public Health. 2024;12(July):1–12. doi:10.3389/fpubh.2024.1405765
28. Textor J, Hardt J, Knüppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology. 2011;22(5):745. doi:10.1097/EDE.0b013e318225c2be
29. Mboup A, Béhanzin L, Guédou FA, et al. Early antiretroviral therapy and daily pre-exposure prophylaxis for HIV prevention among female sex workers in Cotonou, Benin: a prospective observational demonstration study. J Int AIDS Soc. 2018;21(11):1–11. doi:10.1002/jia2.25208
30. Franks J, Teasdale C, Olsen H, et al. PrEP for key populations: results from the first PrEP demonstration project in the Democratic Republic of the Congo. AIDS Care. 2022;34(3):359–362. doi:10.1080/09540121.2021.1969332
31. Pillay D, Stankevitz K, Lanham M, et al. Factors influencing uptake, continuation, and discontinuation of oral PrEP among clients at sex worker and MSM facilities in South Africa. PLoS One. 2020;15(4):1–19. doi:10.1371/journal.pone.0228620
32. Calabrese SK. Understanding, contextualizing, and addressing PrEP stigma to enhance PrEP implementation. Curr HIV/AIDS Rep. 2020;17(6):579–588. doi:10.1007/s11904-020-00533-y
33. Guure C, Afagbedzi S, Torpey K, Chaurasia A. Willingness to take and ever use of pre-exposure prophylaxis among female sex workers in Ghana. Med. 2022;101(5):28798. doi:10.1097/MD.0000000000028798
34. Muhumuza R, Ssemata AS, Kakande A, et al. Exploring perceived barriers and facilitators of PrEP uptake among young people in Uganda, Zimbabwe, and South Africa. Arch Sex Behav. 2021;50(4):1729–1742. doi:10.1007/s10508-020-01880-y
35. Elsesser SA, Oldenburg CE, Biello KB, et al. Seasons of risk: anticipated behavior on vacation and interest in episodic antiretroviral pre-exposure prophylaxis (PrEP) among a large national sample of U.S. men who have sex with men (MSM). AIDS Behav. 2016;20(7):1400–1407. doi:10.1007/s10461-015-1238-0
36. Centers for Disease Control and Prevention: U.S. Public Health Service. Preexoposure prophylaxis for the prevention of HIV infection in the United States – 2021 update. 2021. Available from: https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf.
37. Rogers BG, Sosnowy C, Chan PA, et al. Factors associated with suboptimal retention in HIV pre-exposure prophylaxis care among men who have sex with men. AIDS Care. 2023;35(4):495–508. doi:10.1080/09540121.2022.2129036
38. Mikomangwa WP, Metta E, Moen K, et al. “I stopped to prove them wrong:” reasons for discontinuing daily oral HIV pre-exposure prophylaxis among women at high risk of HIV in Tanzania—a convergent mixed methods study. AIDS Behav. 2026;30:355–367. doi:10.1007/s10461-025-04879-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retention in HIV Pre-Exposure Prophylaxis Among Men Who Have Sex with Men in Tanga, Tanzania
Kiondo F, Metta E, Mmbaga EJ, Leshabari MT, Swai C, Mbotwa CH, Moen K
HIV/AIDS - Research and Palliative Care 2025, 17:185-194
Published Date: 11 July 2025
The HIV Epidemic in the United States – Epidemiological Projections and Public Economic Impact of Achieving Zero Transmission Goals
Copeland C, Martins R, Thaliffdeen R, Kotsopoulos N, Jarrett J, Chaudhari P, Mordi U, Postma MJ
ClinicoEconomics and Outcomes Research 2025, 17:755-769
Published Date: 23 October 2025