Back to Journals » Clinical Ophthalmology » Volume 19
Early Adoption and Utilization of Perfluorohexyloctane for Dry Eye Disease in the United States
Authors Shen Lee B ![]() , Pizzicato L
, Pizzicato L ![]() , Langford E, Shi L, Divino V, Alexander A, Nair AA
, Langford E, Shi L, Divino V, Alexander A, Nair AA ![]()
Received 7 May 2025
Accepted for publication 18 July 2025
Published 31 July 2025 Volume 2025:19 Pages 2529—2540
DOI https://doi.org/10.2147/OPTH.S529837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bridgitte Shen Lee,1 Lia Pizzicato,2 Elizabeth Langford,2 Liucheng Shi,2 Victoria Divino,2 Adam Alexander,3 Abhishek A Nair4
1Vision Optique, Houston, TX, USA; 2Real World Solutions, IQVIA, Falls Church, VA, USA; 3Medical Affairs, Bausch + Lomb Pharmaceuticals. Inc, Bridgewater, NJ, USA; 4Global Health Economics and Outcomes Research, Bausch + Lomb Pharmaceuticals. Inc, Bridgewater, NJ, USA
Correspondence: Abhishek A Nair, Bausch + Lomb Somerset Corporate Center, 400 Somerset Corporate Blvd, Bridgewater, NJ, 08807, USA, Email [email protected]
Purpose: To characterize early adopters of perfluorohexyloctane (PFHO) and 90-day refill rates after the first prescription, overall and compared to a cohort initiating cyclosporine ophthalmic emulsion 0.05% (CsA).
Patients and Methods: Patients ≥ 18 years newly initiating PFHO or CsA between September and November 2023 were identified in IQVIA open-source medical and pharmacy claims databases (date of first claim = index date). Demographics, index prescription characteristics, 12-month baseline clinical characteristics, and 90-day refill rates were descriptively compared between cohorts. A multivariable logistic regression model was developed to evaluate factors associated with the adjusted odds of 90-day refill of the respective index therapy.
Results: The final sample included 7,209 PFHO and 75,871 CsA patients (mean age: 60.6 and 66.6 years; 79.9% and 80.4% female; 67.0% and 39.4% third party payer; respectively). In total, 75.9% of PFHO patients received their prescription through the mail while 92.2% of CsA patients received it through the retail setting. Only 38.5% of PFHO and 33.3% of CsA patients had a diagnosis of dry eye disease (DED) over the 12-month baseline period. Nearly half (46.6%) of PFHO patients used at least one different DED medication over the 12-month baseline compared to 8.1% of CsA patients. Over the 90-day follow-up, most (72.0%) PFHO patients refilled the prescription for their index therapy compared to 37.4% of CsA patients. In the multivariable logistic regression model, PFHO patients had 72% higher likelihood of refilling their index prescription within 90-days compared to CsA patients (adjusted odds ratio: 1.72; 95% confidence interval: 1.60– 1.86).
Conclusion: High DED medication use among PFHO patients in the 12-month period prior to treatment initiation suggests that prior medication may not have resolved their DED symptoms. The higher 90-day refill rate for PFHO versus CsA indicates a higher degree of patient satisfaction with this new, first-in-class treatment for DED.
Keywords: cyclosporine ophthalmic emulsion, prescription refill, administrative claims, evaporative dry eye disease, meibomian gland dysfunction
Introduction
Dry eye disease (DED) is a chronic, multifactorial disease characterized by inflammation of the ocular surface and reductions in the quality and quantity of tears.1 Symptoms of DED vary between individuals and can include ocular pain, discomfort, dryness, fatigue, and visual disturbances such as blurry or fluctuating vision.1 This can result in reduced quality of life and affect worker productivity by impacting activities such as driving, reading, or use of a computer.1 In the United States (US), it is estimated that over 16 million adults have DED with increasing prevalence with age and among women.2 Furthermore, DED imposes a substantial economic burden estimated at $3.8 billion in health care expenditures and $55 billion in societal costs (eg, reduced productivity and indirect costs) annually in the US (reported in 2008 US dollars).3
DED is broadly classified as aqueous-deficient dry eye, evaporative dry eye, or a combination of the two.1 Aqueous-deficient dry eye is characterized by decreased lacrimal gland tear secretion, while evaporative dry eye results from excessive evaporation of tear fluid from the eye surface. It is estimated that most DED patients (>85%) have an evaporative component, while only between 3.5% and 14.6% of DED patients have standalone aqueous-deficient dry eye.4–6 Treatment decisions for DED are guided by the underlying cause (eg, aqueous deficiency, excessive tear evaporation) and severity of disease.7 Historically, most prescription medications for DED have primarily focused on enhancing tear volume or quality and reducing inflammation.7 Until recently, the available treatments did not target the excessive tear evaporation that occurs for most patients.8
In May 2023, the US Food and Drug Administration (FDA) approved perfluorohexyloctane ophthalmic solution (PFHO; Miebo™; Bausch + Lomb) for the treatment of the signs and symptoms of DED, and it became commercially available through a prescription in September 2023.9,10 PFHO is the first and only FDA-approved prescription eye drop for DED that directly targets tear evaporation. In two Phase 3 randomized clinical trials, PFHO met both primary sign and symptom efficacy endpoints of change in total corneal fluorescein staining and eye dryness Visual Analog Scale.11,12
The purpose of this study was to characterize the early adoption of PFHO in real-world clinical practice in the US. A multitude of sociodemographic and clinical factors can impact successful adoption of a novel first-in-class treatment; however, successful early adoption is a sign of positive patient response to a new therapy. This study used open-source medical and pharmacy claims data to describe demographic and clinical characteristics of early adopters of PFHO and initial refill rates after their first prescription. Initiators of cyclosporine ophthalmic emulsion 0.05% (CsA, inclusive of generic CsA, Restasis® and Restasis MultiDose®; Allergan Inc., an AbbVie Company13,14), a well-established commercially available prescription medication indicated to increase tear production in DED, were characterized as the reference comparator group. While the mechanism of action of CsA and PFHO differ, both agents are prescribed for patients with DED and represent important therapeutic options in clinical practice. Furthermore, in the US, both are available through prescription only. As such, CsA serves as a pragmatic and relevant therapeutic benchmark for evaluating patient characteristics and refill patterns among patients initiated on PFHO.
Materials and Methods
Study Overview
This was a retrospective database study utilizing linked data from IQVIA’s Longitudinal Prescription Claims (LRx) and Professional Fee Claims (Dx) databases from September 1, 2022, to February 29, 2024 (the “study period”). The study sample included adult patients initiating PFHO and a comparator cohort initiating CsA between September 1, 2023, and November 30, 2023 (the “selection window”).
Data Sources
The LRx database includes more than 1.6 billion retail or mail order prescription claims, representing dispensed prescriptions for approximately 85% of all pharmacies. The Dx database includes approximately 1 billion professional fee claims per year, representing over 870,000 practitioners per month. Data elements include diagnoses, procedures and office administered drugs. The databases are de-identified and Health Insurance Portability and Accountability Act (HIPAA) compliant. The data are open-source and not limited to any one type of health insurance payer. Patients are linked between databases through a unique IQVIA patient ID, created using a deterministic matching algorithm and actual patient information.
Patient Selection
Patients with ≥1 prescription claim for PFHO or CsA in LRx between September 1, 2023, and November 30, 2023, (the “selection window”) were identified. A hierarchical approach was taken, and the first PFHO claim during the selection window, if any, was identified first to maximize the PFHO sample. The date of the first observed claim for PFHO (if any) or CsA was termed the “index date”, and the drug determined the index therapy. Eligible patients had linkage to Dx, a 12-month baseline period (the “baseline” period), a 90-day post-index period (the “follow-up” period) and were ≥18 years of age at index (Figure 1). Patients were excluded if they had ≥1 prescription claim for the index therapy during the baseline period or invalid data (eg, missing or invalid gender or region or with data supplier issue).
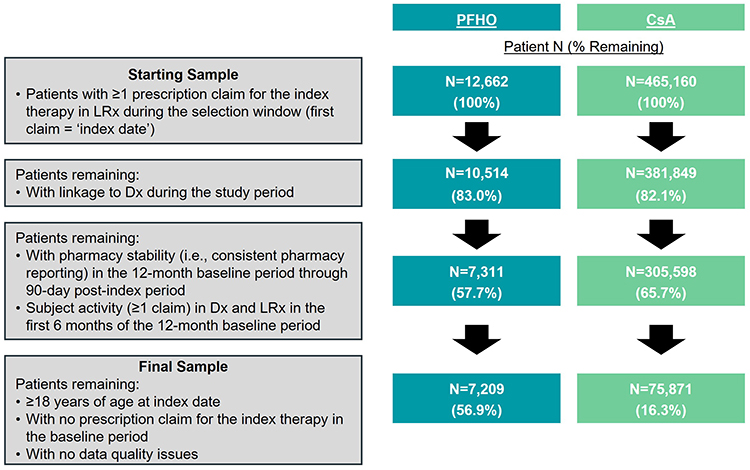 |
Figure 1 Patient Selection. Abbreviations: CsA, cyclosporine ophthalmic emulsion 0.05%; Dx, Professional Fee Claims; LRx, Longitudinal Prescription Claims; PFHO, perfluorohexyloctane. Notes: A hierarchical approach was taken, and PFHO patients were identified first in the selection window. |
Study Measures
Baseline demographics (eg, age, gender, region, payer type) and index prescription characteristics (eg, prescribing specialty, prescription channel, days’ supply) were assessed on the index date. Clinical characteristics (eg, Charlson Comorbidity Index [CCI]; type of DED diagnosis [Supplemental Table 1], ocular and non-ocular comorbidities, DED medication use, relevant ophthalmic procedures) were assessed over the 12-month baseline period.
Initial refill rates in the 90-day period following the index date were assessed, defined as the proportion of patients with ≥1 prescription for the index therapy within 90 days after the index date. Among patients with refill, the time from index date to first refill was also reported. In a secondary analysis, refill rates were also reported among the subset of patients with index days’ supply ≤30 to provide a more equal comparison between the therapy cohorts.
Analyses
Descriptive statistics were produced for all relevant study measures previously described, overall. Categorical measures were presented using frequency (number of patients [n]) and percentage (%) of total study patients observed in each category. Continuous and count variables were presented as the mean and standard deviation (SD). As relevant, continuous variables were also categorized into intervals. Analyses were conducted on the observed data using SAS® 9.4 M8 (SAS Institute Inc., Cary, NC). Baseline characteristics and initial refill rates were assessed and descriptively compared between the PFHO and CsA cohorts without any formal comparison.
A multivariable logistic regression model was developed to evaluate the factors associated with the adjusted odds of 90-day refill of the respective index therapy among PFHO and CsA initiators. Covariates included in the model were demographics (age, gender, region, payer type), index prescription characteristics (prescriber specialty, days’ supply, prescription channel), and baseline clinical characteristics (DED diagnosis, ocular and non-ocular comorbidities, DED medication use, and ophthalmic procedures). The model covariates were also evaluated for multicollinearity. A p-value <0.05 was considered statistically significant.
Results
Patient Sample
The initial sample comprised 12,662 patients with ≥1 prescription claim for PFHO and 465,160 patients with ≥1 claim for CsA following the hierarchical approach (Figure 1). The final sample was composed of 7,209 PFHO patients (56.9% of the initial sample) and 75,871 CsA patients (16.3%) in the comparator cohort.
Patient Baseline Characteristics
Demographics
PFHO patients were younger than CsA patients, with mean (SD) age of 60.6 (14.3) years and 66.6 (13.3) years, 14.4% and 7.4% with age <45 years, and 41.1% and 63.4% with age 65+ years, respectively (Table 1). The vast majority of PFHO and CsA patients were female (79.9–80.4%). The majority (66.1%) of PFHO patients had a third party payer while over half (55.4%) of CsA patients had Medicare. Patients from both cohorts were most often located in the South (37.9–41.5%). Over half (55.2%) of PFHO patients had index month of November while CsA patients most often had index month of October (35.3%) given that PFHO was new to the market.
 |
Table 1 Demographics of PFHO and CsA Cohorts |
Index Prescription Characteristics
More than half (54.7%) of PFHO patients received their index prescription from an optometrist (54.7%), whereas CsA patients most often received their index prescription from an ophthalmologist (47.5%) (Table 2). Mean (SD) days’ supply was lower for the PFHO cohort compared to the CsA cohort (29.9 [14.3] days and 54.6 [29.7] days), and almost all (93.1%) PFHO patients received days’ supply ≤30 days compared to 56.9% of CsA patients. The vast majority (75.9%) of PFHO patients received their prescription through a mail order pharmacy while most (92.2%) CsA patients received their prescription through the retail pharmacy setting.
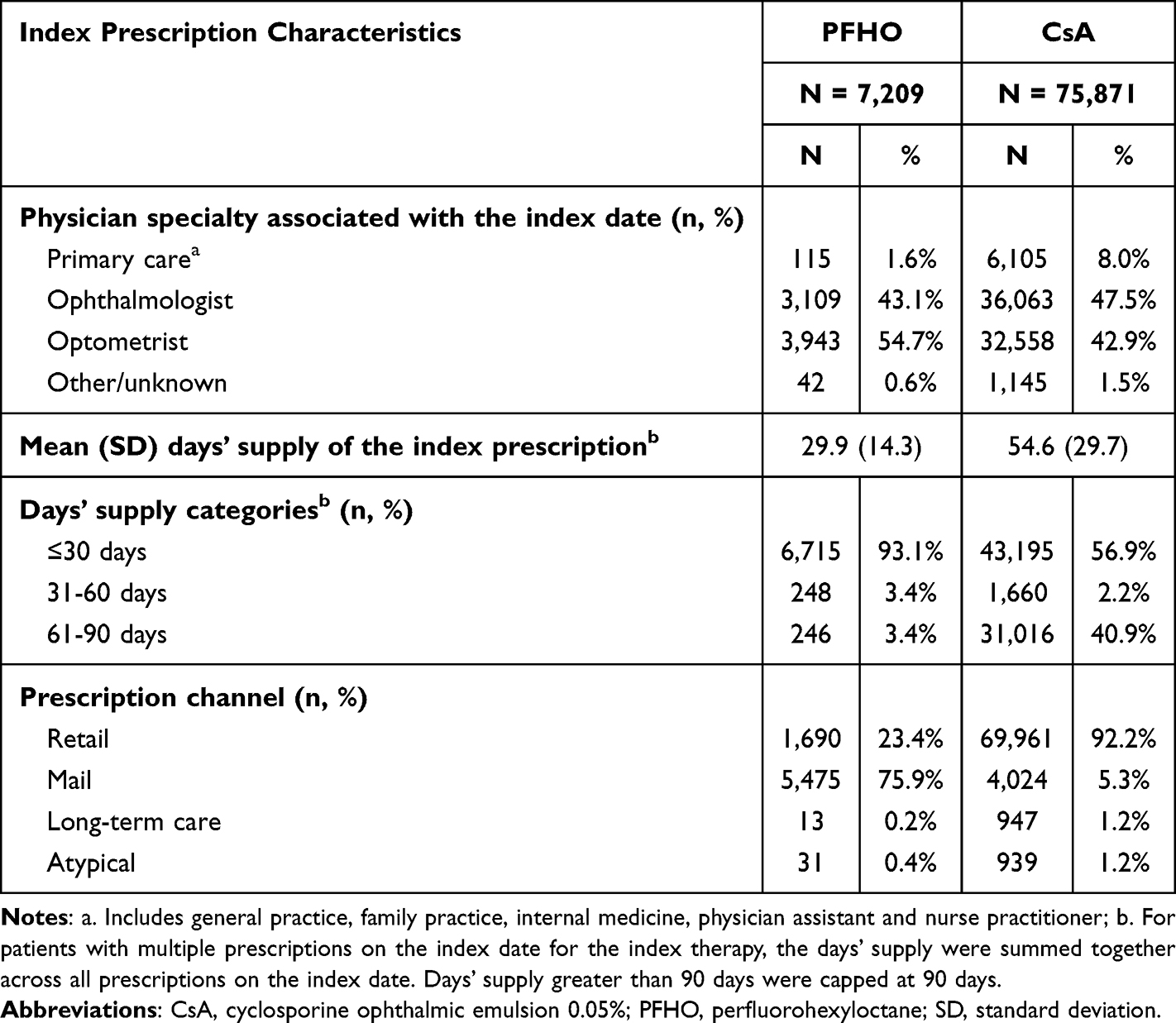 |
Table 2 Index Prescription Characteristics of PFHO and CsA Cohorts |
Clinical Characteristics
Diagnosis of DED over the 12-month baseline period or the index date was relatively infrequent, but higher among PFHO patients (38.5%) than CsA (33.3%) patients (Table 3). Aqueous-deficient DED diagnosis was most commonly observed (28.7% and 24.4%, respectively). Notably, evaporative dry eye was more frequently observed among PFHO patients compared to CsA patients (11.3% and 5.5%, respectively).
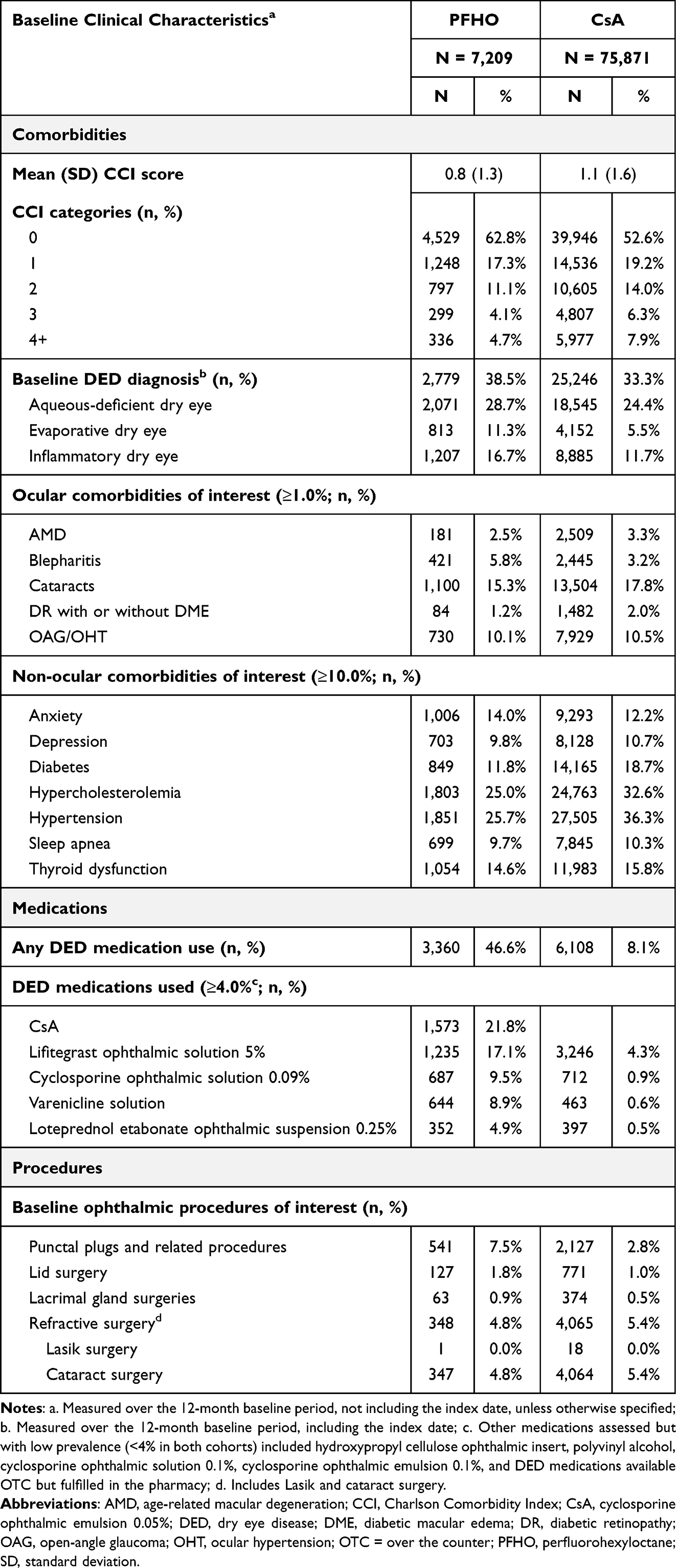 |
Table 3 Baseline Clinical Characteristics of PFHO and CsA Cohorts |
Baseline comorbidities were generally higher among CsA patients, likely related to their older age. Mean (SD) CCI score was lower among the PFHO cohort compared to the CsA cohort (0.8 [1.3] and 1.1 [1.6]), and a higher proportion of PFHO patients had a CCI score of 0 (62.8% and 52.6%, respectively). Proportion with diabetes, hypercholesterolemia, and hypertension were higher in the CsA cohort while proportion with anxiety, depression, sleep apnea, and thyroid dysfunction were similar between PFHO and CsA patients. Proportion with ocular comorbidities of interest was generally similar (eg, blepharitis, cataracts, and open-angle glaucoma/ocular hypertension) between cohorts.
Nearly half (46.6%) of PFHO patients used any DED medication over the 12-month baseline period compared to only 8.1% of CsA patients. Proportion with baseline punctal plugs and related procedures was also higher among PFHO patients (7.5% and 2.8%, respectively). Proportion with refractive surgery was generally similar (4.8–5.4%).
90-Day Post-Index Refill Rates
In the 90-days post-index, overall, the majority (72.0%) of PFHO patients refilled a prescription for their index therapy compared to over one-third (37.4%) of CsA patients (Figure 2a). Among patients with refill, the mean (SD) time from index date to first refill was 31.5 (14.7) days for PFHO and 45.9 (24.8) days for CsA.
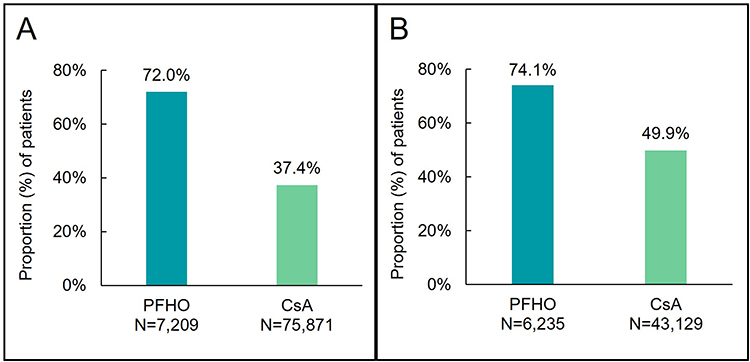 |
Figure 2 90-day Refill Rates of PFHO and CsA Cohorts (A) Overall, (B) Secondary Analysisa. Abbreviations: CsA, cyclosporine ophthalmic emulsion 0.05%; PFHO, perfluorohexyloctane. Notes: a. Among the subset of patients with index days’ supply ≤30 days. |
In the secondary analysis, 6,235 PFHO patients (86.5% of the final sample) and 43,129 CsA patients (56.8%) had ≤30 days’ supply on the index date and only one index therapy claim on the index date. Of these patients, the majority (74.1%) of PFHO patients continued to refill within 90-days post-index, compared to half (49.9%) of CsA patients (Figure 2b). Notably, in this secondary analysis, 90-day refill rates for CsA increased compared to the overall analysis, while PFHO rates increased marginally.
Predictors of 90-Day Post-Index Refill
In the multivariable logistic regression model, patients initiating PFHO were associated with 72.2% higher likelihood of refilling their index prescription compared to patients initiating CsA over the 90-day follow-up period (adjusted odds ratio [aOR]: 1.72; 95% confidence interval [CI]: 1.60–1.86) (Table 4). The c-statistic for this model was 0.710 indicating a good fit. Several other covariates were significantly (p < 0.001) associated with odds of refilling within 90 days after their index prescription. Patients aged 45–64 years were associated with higher odds of refilling compared to patients aged 65+ years (aOR: 1.29; 95% CI: 1.24–1.35). Patients located in the Northeast (aOR: 1.20; 95% CI: 1.15–1.24) and West (aOR: 1.32; 95% CI: 1.27–1.37) had higher odds of refilling compared to patients located in the South. Patients with Medicaid were associated with higher odds of refilling as compared to patients with a third party payer (aOR: 1.45; 95% CI: 1.36–1.54). Patients with an ophthalmologist associated with the index prescription had higher odds of refilling compared to those associated with an optometrist (aOR: 1.09; 95% CI: 1.05–1.13). Compared to patients with ≤30 days’ supply of the index prescription, those with days’ supply of 31–60 days (aOR: 0.59; 95% CI: 0.53–0.65) and 61–90 days (aOR: 0.25; 95% CI: 0.24–0.26) had lower odds of refilling. Patients with a history of DED medication use were associated with higher odds of refilling their index prescription compared to those without a history of DED medication use (aOR: 1.52; 95% CI: 1.44–1.60).
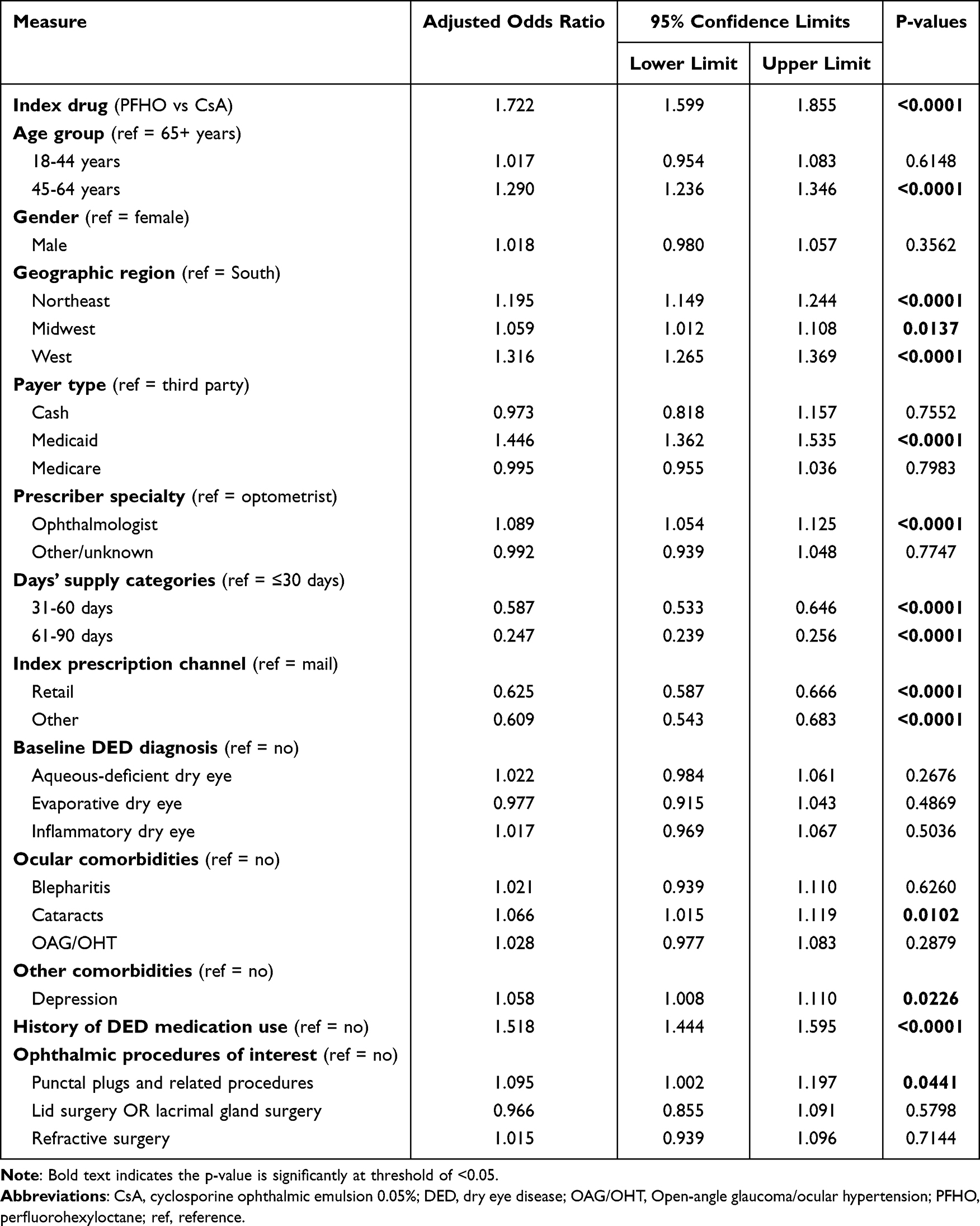 |
Table 4 Predictors of 90-Refill from Logistic Regression Model for Odds of Refill of the Index Therapy Within 90 Days Post-Index (c-Statistic = 0.710) |
Discussion
This study examined demographic and clinical characteristics of patients who were early adopters of PFHO leveraging recent real-world data. PFHO patients were younger than CsA patients but had a similar distribution by gender and geographic region of residence. Most PFHO patients had a commercial payer and received their index prescription from a mail order pharmacy while most CsA patients had a Medicare payer and received their index prescription from a retail pharmacy. For both cohorts, DED diagnosis appeared to be under-recorded in the claims data as less than two-thirds of patients in both groups had at least one diagnosis of DED in the 12-month baseline period. Furthermore, our study identified a comparatively higher proportion of patients with baseline DED medication use and prior punctal plug procedure among those treated with PFHO than those treated with CsA. Descriptively, a higher proportion of PFHO patients refilled their prescription within 90-days after initiation compared to CsA patients in both the main and secondary analysis. After adjusting for differences in baseline demographic, clinical, and index prescription characteristics, PFHO patients were associated with a higher likelihood of 90-day prescription refill compared to CsA patients.
Meibomian gland dysfunction has been noted as the primary cause of evaporative DED, wherein the quality and quantity of lipid secretion is impacted, leading to increased evaporative aqueous tear loss.11 PFHO is a novel therapy with amphiphilic properties that is thought to form a monolayer at the air-tear interface to inhibit tear evaporation.12 This unique proposed mechanism of action allows PFHO to address the driver of the disease itself and potentially help promote tear film stability and homeostasis.12 Studies examining DED etiology have suggested that the vast majority of patients with DED have an underlying evaporative component, indicating most patients with DED could benefit from PFHO therapy.4,6
The refill rates among CsA patients in the present study were low which is consistent with previous research that has reported high rates of discontinuation among patients initiating CsA treatment.15 This may suggest that there is an unmet need and CsA may not be effectively addressing symptoms among these patients with DED. There may be several drivers of the observed lower refill rates among CsA patients in the present study. First, patients may refill CsA prescriptions at lower rates due to adverse reactions. For instance, in clinical trials for CsA, the most common adverse event was ocular burning reported in 17% of patients while this adverse event was only present in 0.5% of patients in PFHO clinical trials.11–13 Furthermore, one prior chart review study found that 60.0% of patients reported discontinuing CsA treatment due to burning or stinging associated with its use while a separate satisfaction survey study noted that 21% of CsA patients reported “usually” or “always” experiencing “burning sensation upon instillation.”16,17 Another reason for discontinuation may be related to the reported time required to be on CsA treatment (>3 months) before the experience of clinical benefits.15,18 In a cross-sectional study, 29% of patients currently using CsA reported dissatisfaction with the time to onset of effect.16 On the other hand, clinical trials for PFHO showed reductions in the signs and symptoms of DED as early as 2 weeks with continued improvements observed through week 8.11,12,19 In the present study, PFHO patients had high DED medication use in the 12-month period prior to treatment initiation, which may suggest that prior therapies were unsuccessful in resolving their DED symptoms. Importantly, discontinuation of treatment resulting from failure to refill medications can lead to disease progression and symptom worsening.20 Further research is needed to fully understand reasons for the differences in refill rates between patients initiating CsA and PFHO; however, experience with adverse events and the lag time between treatment initiation and symptomatic relief may be key drivers.
In this analysis, DED appeared to be under-recorded in the data, as approximately two-thirds of both PFHO and CsA patients received the index prescription despite not having a recorded DED diagnosis. Previous studies that have examined real-world treatment patterns of patients initiating CsA similarly found that less than one-third of patients had a recorded DED diagnosis.15,21 Of the DED conditions captured in the present study, aqueous-deficient dry eye was seen most frequently (PFHO: 28.7%; CsA: 24.4%), while evaporative dry eye was seen in 11.3% of PFHO patients and only 5.5% in CsA patients. This is different than the distribution reported in the literature from site-based studies, which suggests 85.5–94% of patients have an evaporative dry eye component.4–6 Although DED diagnoses are under-reported on claims in the present study, PFHO targets the evaporative dry eye etiology, which is likely driving the higher prevalence of evaporative dry eye observed in the data for PHFO-treated patients compared to CsA-treated patients.10 Importantly, the distribution of DED diagnosis codes in the present study may differ from the literature as the specific diagnosis code included on the claim may be potentially driven by health insurance reimbursement requirements.4,22
The study is subject to several limitations. First, claims data are collected for administrative purposes, not research, and may not reflect true diagnoses and treatment as coding issues may occur. Second, there are limitations related to the use of open-source claims databases. Data is utilized as available from a patient but is not considered comprehensive. Data is obtained from pharmacies and offices that participate in and contribute to the databases, and there is no insight into activity at pharmacies or offices that do not contribute to the data. Nevertheless, LRx and Dx coverage in the US is relatively high. We applied proxies for continuous enrollment based on patient activity and pharmacy reporting to provide greater assurance that patient healthcare activity within these databases is captured during the study period. In addition, while filled prescriptions are identified through the claims data, a prescription fill is not an indicator of medication utilization by the patient. Furthermore, these data do not include DED medications purchased over-the-counter without a prescription like artificial tear eye drops. Finally, the study included limited follow-up time to allow for an early view into early adopters of PFHO.
Conclusion
Despite these limitations, our study had key strengths. This is one of the first real-world studies to characterize early initiators of PFHO, leveraging recent data from large, national claims databases in the US that are inclusive of all payers. After adjusting for baseline differences, early adopters of PFHO were more likely to refill their prescription within 90 days than CsA patients. These findings provide important evidence regarding initial refill rates among patients with DED receiving PFHO and CsA. Once additional longer-term data is available, further research comprehensively examining refill rates, other treatment patterns such as adherence and persistence, DED diagnosis patterns, clinical outcomes, and medication cost will help to inform optimal treatment decisions for patients with DED.
Data Sharing Statement
Original de-identified data used in this analysis were obtained from and are the property of IQVIA. IQVIA has restrictions prohibiting the authors from making the dataset publicly available. Interested researchers may contact IQVIA to apply to gain access to the study’s data in the same way the authors obtained the data (https://www.iqvia.com/contact/sf).
Ethics Statement
This study involved use of IQVIA de-identified data. Data were de-identified by IQVIA and comply with the Health Insurance Portability and Accountability Act and the Helsinki Declaration of 1964 and its later amendments or comparable ethical standards. The US Department of Health and Human Services does not consider analysis of de-identified secondary data to meet the definition for human subject research. Therefore, this study was exempt from federal regulations and did not require patient consent or institutional review board review.
Consent for Publication
All authors provide consent for the article to be published.
Acknowledgments
Some details and results of the study were presented at the following conferences: 127th Annual AOA Congress & 56th Annual AOSA Conference: Optometry’s Meeting (Nashville, TN; June 19–22, 2024; DOI: 10.13140/RG.2.2.27302.02884); Women in Ophthalmology (WIO) 2024 Summer Symposium (Carlsbad, CA; August 22, 2024–August 25, 2024; DOI: 10.13140/RG.2.2.34012.91529); 10th International Tear Film and Ocular Surface Society (TFOS) Conferences (Venice, Italy; October 30–November 2, 2024; DOI: 10.13140/RG.2.2.10174.60485); 2025 Caribbean Eye Meeting (San Jose del Cabo, Mexico; January 31-February 5, 2025); World Cornea Congress 2025 (Washington, DC; March 20–22, 2025; DOI: 10.13140/RG.2.2.21554.72640); American Society of Cataract and Refractive Surgery (ASCRS) 2025 (Los Angeles, CA; April 25–28, 2025); Association for Research in Vision and Ophthalmology (ARVO) 2025 (Salt Lake City, UT; May 4–8, 2025; https://iovs.arvojournals.org/article.aspx?articleid=2809143); and the 128th Annual AOA Congress & 57th Annual AOSA Conference: Optometry’s Meeting (Minneapolis, MN; June 25–28, 2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Bausch + Lomb (Bridgewater, NJ, USA). The Article Processing Fee was also funded by Bausch + Lomb. The sponsor participated in the design of the study, interpretation of the data, and review and approval of the manuscript.
Disclosure
BSL reports receiving consulting/speaker fees from Bausch + Lomb, CooperVision, Dompe, LENZ Therapeutics, Sun Pharmaceutical Industries, Inc., Tarsus Pharmaceuticals, and Carl Zeiss Meditec, Inc.; and research support from Johnson and Johnson Vision, SightGlass Vision, Tarsus Pharmaceuticals, and Viatris Inc. VD, EL, LP, and LS are employees of IQVIA which received funding for this study from Bausch & Lomb Americas. AA and AAN are employees and stockholders of Bausch & Lomb Americas. The authors report no other conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Farrand KF, Fridman M, Stillman I, Schaumberg DA. Prevalence of diagnosed dry eye disease in the United States among adults aged 18 years and older. Am J Ophthalmol. 2017;182:90–98. doi:10.1016/j.ajo.2017.06.033
3. Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. doi:10.1097/ICO.0b013e3181f7f363
4. Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472–478. doi:10.1097/ICO.0b013e318225415a
5. Tong L, Chaurasia SS, Mehta JS, Beuerman RW. Screening for meibomian gland disease: its relation to dry eye subtypes and symptoms in a tertiary referral clinic in Singapore. Invest Ophthalmol Vis Sci. 2010;51(7):3449–3454. doi:10.1167/iovs.09-4445
6. Badian RA, Utheim TP, Chen X, et al. Meibomian gland dysfunction is highly prevalent among first-time visitors at a Norwegian dry eye specialist clinic. Sci Rep. 2021;11(1):23412. doi:10.1038/s41598-021-02738-6.
7. Clayton JA. Dry Eye. N Engl J Med. 2018;378(23):2212–2223. doi:10.1056/NEJMra1407936
8. Sheppard JD, Evans DG, Protzko EE. A review of the first anti-evaporative prescription treatment for dry eye disease: perfluorohexyloctane ophthalmic solution. Am J Manag Care. 2023;29(14 Suppl):S251–s259. doi:10.37765/ajmc.2023.89464
9. Bausch + Lomb. Bausch + Lomb and Novaliq announce FDA approval of MIEBO™ (Perfluorohexyloctane Ophthalmic Solution) for the Treatment of the signs and symptoms of dry eye disease. Available from: https://ir.bausch.com/press-releases/bausch-lomb-and-novaliq-announce-fda-approval-miebotm-perfluorohexyloctane.
10. Miebo [Package Insert. Bridgewater, NJ: Bausch & Lomb Americas Inc; 2023.
11. Tauber J, Berdy GJ, Wirta DL, Krösser S, Vittitow JL. NOV03 for dry eye disease associated with meibomian gland dysfunction: results of the randomized phase 3 GOBI study. Ophthalmology. 2023;130(5):516–524. doi:10.1016/j.ophtha.2022.12.021
12. Sheppard JD, Kurata F, Epitropoulos AT, Krösser S, Vittitow JL. NOV03 for signs and symptoms of dry eye disease associated with meibomian gland dysfunction: the randomized phase 3 MOJAVE study. Am J Ophthalmol. 2023;252:265–274. doi:10.1016/j.ajo.2023.03.008
13. Restasis [Package Insert]. Irvine, CA: Allergan, Inc; 2012.
14. Restasis Multidose [Package Insert]. Irvine, CA: Allergan, Inc; 2024.
15. White DE, Zhao Y, Ogundele A, et al. Real-world treatment patterns of cyclosporine ophthalmic emulsion and lifitegrast ophthalmic solution among patients with dry eye. Clin Ophthalmol. 2019;13:2285–2292. doi:10.2147/opth.S226168
16. White DE, Zhao Y, Jayapalan H, Machiraju P, Periyasamy R, Ogundele A. Treatment satisfaction among patients using anti-inflammatory topical medications for dry eye disease. Clin Ophthalmol. 2020;14:875–883. doi:10.2147/opth.S233194
17. Mah F, Milner M, Yiu S, Donnenfeld E, Conway TM, Hollander DA. PERSIST: physician’s Evaluation of Restasis(®) Satisfaction in Second Trial of topical cyclosporine ophthalmic emulsion 0.05% for dry eye: a retrospective review. Clin Ophthalmol. 2012;6:1971–1976. doi:10.2147/opth.S30261
18. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003
19. Tauber J, Wirta DL, Sall K, Majmudar PA, Willen D, Krösser S. A randomized clinical study (SEECASE) to assess efficacy, safety, and tolerability of NOV03 for treatment of dry eye disease. Cornea. 2021;40(9):1132–1140. doi:10.1097/ico.0000000000002622
20. Rao SN. Reversibility of dry eye deceleration after topical cyclosporine 0.05% withdrawal. J Ocul Pharmacol Ther. 2011;27(6):603–609. doi:10.1089/jop.2011.0073
21. Karpecki P, Barghout V, Schenkel B, et al. Real-world treatment patterns of OTX-101 ophthalmic solution, cyclosporine ophthalmic emulsion, and lifitegrast ophthalmic solution in patients with dry eye disease: a retrospective analysis. BMC Ophthalmol. 2023;23(1):443. doi:10.1186/s12886-023-03174-y
22. Sun Opthalmics. Cequa: prior authorization, billing, and coding. Available from: https://www.cequapro.com/prior-authorization-billing-coding.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.