Back to Journals » Clinical Interventions in Aging » Volume 21
Dynamic versus Static Metabolic Models for Predicting ECG-Defined Cardiovascular Risk in Elderly MAFLD: A Three-Year Cohort Study
Authors Liu Z ![]() , Liu Y
, Liu Y ![]() , Liu B
, Liu B ![]() , Zhao M, Lu Y
, Zhao M, Lu Y ![]() , Zhang X
, Zhang X ![]()
Received 14 September 2025
Accepted for publication 23 December 2025
Published 5 February 2026 Volume 2026:21 567520
DOI https://doi.org/10.2147/CIA.S567520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Nandu Goswami
Zhangyi Liu,1 Yongli Liu,2 Bintao Liu,3 Mei Zhao,1 Yu Lu,4,* Xiaoqing Zhang1,*
1School of Life Sciences, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Physical Examination Department, Weifang Kuiwen Hengkang Hospital, Weifang, Shandong, People’s Republic of China; 3College of Architecture and Landscape, Peking University, Beijing, People’s Republic of China; 4Institute of Information on Traditional Chinese Medicine, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqing Zhang, School of Life Sciences, Beijing University of Chinese Medicine, Beijing, People’s Republic of China, Tel +86 10 53912159, Email [email protected] Yu Lu, Institute of Information on Traditional Chinese Medicine, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China, Tel +86 10 64089578, Email [email protected]
Purpose: Given the high and rising prevalence of metabolic dysfunction-associated fatty liver disease (MAFLD) among the aging population and its established link to cardiovascular risk, this study aimed to evaluate the predictive value of dynamic metabolic trajectories for ECG-defined cardiovascular risk in elderly patients with MAFLD.
Patients and Methods: This three-year longitudinal study enrolled 1086 elderly patients with MAFLD from Weifang City, Shandong Province, China. Group-based trajectory modeling (GBTM) was applied to identify dynamic changes in 12 metabolic indicators. The predictive performance of the metabolic trajectory model was compared with that of the cross-sectional model using 5-fold cross-validation. Multivariable logistic regression was employed to evaluate the independent associations between specific metabolic trajectories and ECG-defined cardiovascular risk.
Results: During follow-up, 877 participants (80.76%) developed new ECG abnormalities. The trajectory model demonstrated a modest but statistically significant improvement in discrimination over the cross-sectional model (ΔAUC = 0.054). Specific progressively worsening metabolic trajectories were strongly associated with increased risk: the “Obesity-Increasing” BMI, “Moderate Hypertension-Increasing” SBP, and “High Level-Increasing” TC trajectories. Notably, a “legacy effect” of liver injury was evident: patients whose elevated AST later declined (“High-Decreasing” trajectory) still faced substantially elevated cardiovascular risk (aOR = 4.15; aRR = 1.20). Conversely, the “Moderate Diabetes-Decreasing” FPG trajectory (aOR = 0.49; aRR = 0.82) and adherence to a predominantly vegetarian diet (aOR = 0.22; aRR = 0.61) were associated with significantly lower risk. Advanced age remained a strong independent risk factor.
Conclusion: Dynamic metabolic trajectories offer incremental predictive value over static measures in predicting ECG-defined cardiovascular risk in elderly MAFLD patients. Clinical management should shift from state-based to trend-based intervention, focusing on early control of adverse trends, long-term vigilance for patients with a history of liver injury, and active improvement of reversible risk factors. Tailored dietary interventions are also recommended. These findings provide an evidence-based foundation for developing precise and proactive risk prevention strategies in this high-risk population.
Plain Language Summary: Why was the study done?
Heart disease is common in older adults with MAFLD. Current risk assessments often use single measurements, which may miss important health trends over time. We conducted this study to see whether tracking metabolic changes over several years could better predict heart risk.
What did the researchers do and find?
We followed 1086 older adults with MAFLD for three years. We identified patterns in how 12 metabolic indicators changed over time, grouping people based on improving, worsening, or stable trends. We then tested whether these trend-based groups predicted future heart risk (measured by ECG changes) better than a single measurement.
We found that the trajectory-based model predicted CVD risk much better than one-time measurements. Patients with worsening groups—especially increasing obesity, rising blood pressure, or climbing cholesterol—faced the highest risk. Even after liver enzyme levels normalized, those with past liver injury were linked to a lasting higher risk. Conversely, people who improved their blood sugar or mostly ate vegetarian foods had much lower risk.
What do these results mean?
For elderly patients with MAFLD, tracking health trends over time provides a clearer picture of future heart risk than a single check. This approach enables earlier and more personalized care—like helping patients avoid worsening trends, offering long-term monitoring for those with past liver issues, and promoting beneficial diets. These steps can prevent disease, improve well-being, and use healthcare resources more effectively.
Keywords: group-based trajectory modeling, electrocardiography, risk prediction, precision prevention, geriatrics
Introduction
The accelerating pace of global population aging has positioned the prevention and management of age-related diseases as one of the most pressing public health challenges worldwide.1,2 Among these conditions, metabolic dysfunction-associated fatty liver disease (MAFLD)—characterized by hepatic steatosis in the context of metabolic dysregulation—has garnered increasing attention.3,4 In 2024, the Chinese Society of Hepatology introduced updated diagnostic criteria tailored to national conditions, defining MAFLD as a positive diagnosis based on imaging or histological evidence of hepatic steatosis along with the presence of at least one component of metabolic syndrome, thereby superseding the traditional exclusion-based concept of non-alcoholic fatty liver disease (NAFLD).5 Epidemiological evidence further underscores the urgency of the issue. The global prevalence of MAFLD has risen from 25.26% in 1990–2006 to 38.00% in 2016–2019,6 with affected individuals in the Asia-Pacific region aged 65–89 exceeding 120 million in 2019.7 A synthesis of previous studies indicates that the prevalence among Chinese adults over the past two decades reaches 29.6%,8 while a 2021 ultrasonographic screening of 347,000 community-dwelling elderly in Shenzhen revealed a fatty liver prevalence of 33.25%, with both prevalence and risk of complications significantly increasing with age.9 Consequently, clinical guidelines emphasize that lifestyle intervention should form the foundation of MAFLD management in the elderly, alongside comprehensive control of metabolic disorders and vigilant monitoring of multisystem extrahepatic complications.5
MAFLD is now recognized not as an isolated hepatic disorder but as a multisystem condition, with clinical manifestations extending to a range of extrahepatic complications, including chronic kidney disease, type 2 diabetes, and certain extrahepatic malignancies.4 Foremost among these is cardiovascular disease (CVD), a leading cause of mortality in elderly patients with MAFLD.10,11 This elevated CVD risk is largely mediated by shared pathophysiological pathways. Specifically, progressive worsening of metabolic abnormalities—such as obesity, dyslipidemia, and hepatic injury—can exacerbate lipotoxicity, chronic systemic inflammation, and insulin resistance, which concurrently drive both hepatic steatosis and vascular endothelial dysfunction, thereby accelerating atherosclerosis.4,12,13 Notably, the dynamic history of these metabolic parameters may hold greater prognostic value than their static, cross-sectional levels. This concept aligns with the “metabolic memory” phenomenon observed in other diseases, wherein past dysregulation can impart enduring effects.14 We therefore hypothesize a potential “legacy effect” in MAFLD, whereby the cumulative burden of past metabolic disturbances induces a persistent adverse cardiovascular milieu—likely driven by mechanisms such as entrenched pro-inflammatory signaling or epigenetic reprogramming—that may not be fully reversed by subsequent biochemical improvement. However, most previous studies are ill-equipped to investigate this hypothesis, as they have predominantly relied on cross-sectional or single-time-point measurements, failing to capture dynamic risk trajectories, and have focused on hard clinical endpoints such as myocardial infarction, with limited attention to early subclinical cardiovascular damage.
To address these limitations, we conducted a three-year prospective longitudinal study in Weifang City, Shandong Province, China, enrolling 1086 elderly patients with MAFLD. Electrocardiogram (ECG) abnormalities defined according to AHA/ESC guidelines were employed as an early marker of subclinical cardiovascular risk,15 with the primary endpoint being the occurrence of new ECG abnormalities during the follow-up period. The analysis set was restricted to participants who completed the entire three-year follow-up; individuals who withdrew due to death, loss to follow-up, or reasons unrelated to cardiovascular events were excluded. Our statistical analysis proceeded in two stages. First, group-based trajectory modeling (GBTM) was applied to identify distinct dynamic patterns in key metabolic indicators. This method is particularly suitable for identifying subgroups of individuals exhibiting similar trajectories over time, which aligns with our objective of classifying patients based on clinically interpretable metabolic trajectory phenotypes.16 Subsequently, machine learning techniques were employed to systematically evaluate the incremental predictive value of these trajectory-based indicators compared to conventional static measures. To our knowledge, this is the first longitudinal study in a dedicated elderly MAFLD cohort that integrates metabolic trajectories with early cardiovascular risk, aiming to establish a novel dynamic risk assessment framework for this high-risk population. This integrated approach seeks to identify trajectory patterns associated with cardiovascular complications, thereby offering targeted insights for cardiovascular disease prevention in elderly patients with MAFLD.
Materials and Methods
Participant Characteristics
This three-year longitudinal cohort study was conducted from April 2021 to April 2023. The study population comprised elderly patients with MAFLD who were permanent residents of Weifang City, Shandong Province. Standardized assessments were conducted annually in April.
The diagnosis of MAFLD was based on established international consensus criteria,4,5 requiring the presence of hepatic steatosis identified by abdominal ultrasonography in addition to at least one of the following three criteria: overweight or obesity, type 2 diabetes mellitus (T2DM), or evidence of metabolic dysregulation.
Inclusion criteria were: (1) age ≥ 65 years; (2) confirmed MAFLD diagnosis based on international guidelines;9 and (3) absence of CVD history at baseline. Exclusion criteria included: (1) severe comorbidities, including concurrent liver diseases (eg, significant liver dysfunction, cirrhosis, or hepatocellular carcinoma), other chronic systemic diseases (eg, chronic kidney disease, severe chronic obstructive pulmonary disease, autoimmune disorders, or active malignancy), or severe neuropsychiatric disorders (eg, schizophrenia or severe cognitive impairment); or (2) inability to complete the three-year follow-up due to death, loss to follow-up, or non-cardiovascular-related reasons, or having insufficient clinical data for analysis.
The flow of participant screening, enrollment, and follow-up is summarized in Figure 1.
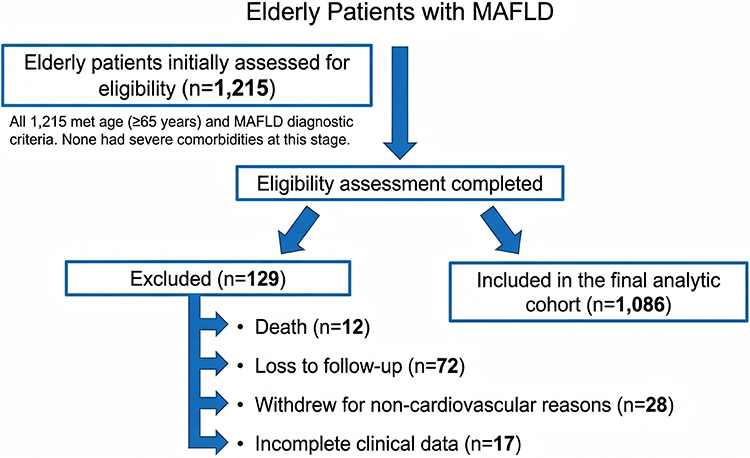 |
Figure 1 The flowchart summarizes the process of participant screening, enrollment, and follow-up in the cohort of elderly patients with MAFLD. |
This investigation was conducted as a substudy of a collaborative project between our research team and the Department of Cardiology, Dongzhimen Hospital, Beijing University of Chinese Medicine. The study protocol was designed in accordance with the ethical principles outlined in the Declaration of Helsinki246. Ethical approval was obtained from the Institutional Ethics Committee of Dongzhimen Hospital (Approval No.: 2023DZMEC-228-02). Written informed consent was secured from all participants prior to their enrollment in the study.
Definitions
Demographic and Clinical Baseline Data
Demographic and clinical baseline data were assessed through a combination of standardized questionnaires and electronic medical records. Information collected included demographic characteristics (sex, age), lifestyle factors (physical activity frequency, dietary patterns), and clinical history (smoking status, alcohol use, and family history of cardiovascular disease). All data were collected at enrollment and updated during the two subsequent annual follow-ups, yielding three complete data points per participant over the three-year study period.
Data collection was performed by qualified personnel based on their expertise: standardized questionnaires and electronic medical records were managed by postgraduate researchers and residents under the supervision of attending physicians, while physical examinations and biosample collection were conducted by trained hospital nurses following standardized operating procedures.
Metabolic Parameters
The following metabolic indicators were evaluated: obesity-related measures (body mass index, BMI and waist circumference), blood pressure (systolic blood pressure, SBP, and diastolic blood pressure, DBP), fasting plasma glucose (FPG), lipid profile (total cholesterol, TC, triglycerides, TG, low-density lipoprotein cholesterol, LDL-C, and high-density lipoprotein cholesterol, HDL-C), and liver function markers (aspartate aminotransferase, AST, alanine aminotransferase, ALT, and total bilirubin, TBIL). All measurements were conducted in accordance with standardized protocols using calibrated equipment and automated analyzers. Specifically, blood pressure was measured using a Yuwell YE670CR electronic sphygmomanometer (Jiangsu Yuyue Medical Equipment & Supply Co., Ltd., Jiangsu, China), and the biochemical analyses for FPG, TC, TG, LDL-C, HDL-C, AST, and ALT were performed using a Seamaty SD1 fully automated dry biochemical analyzer (Chengdu Seamaty Technology Co., Ltd., Sichuan, China). Specific measurement methods for all indicators are presented in Table 1.
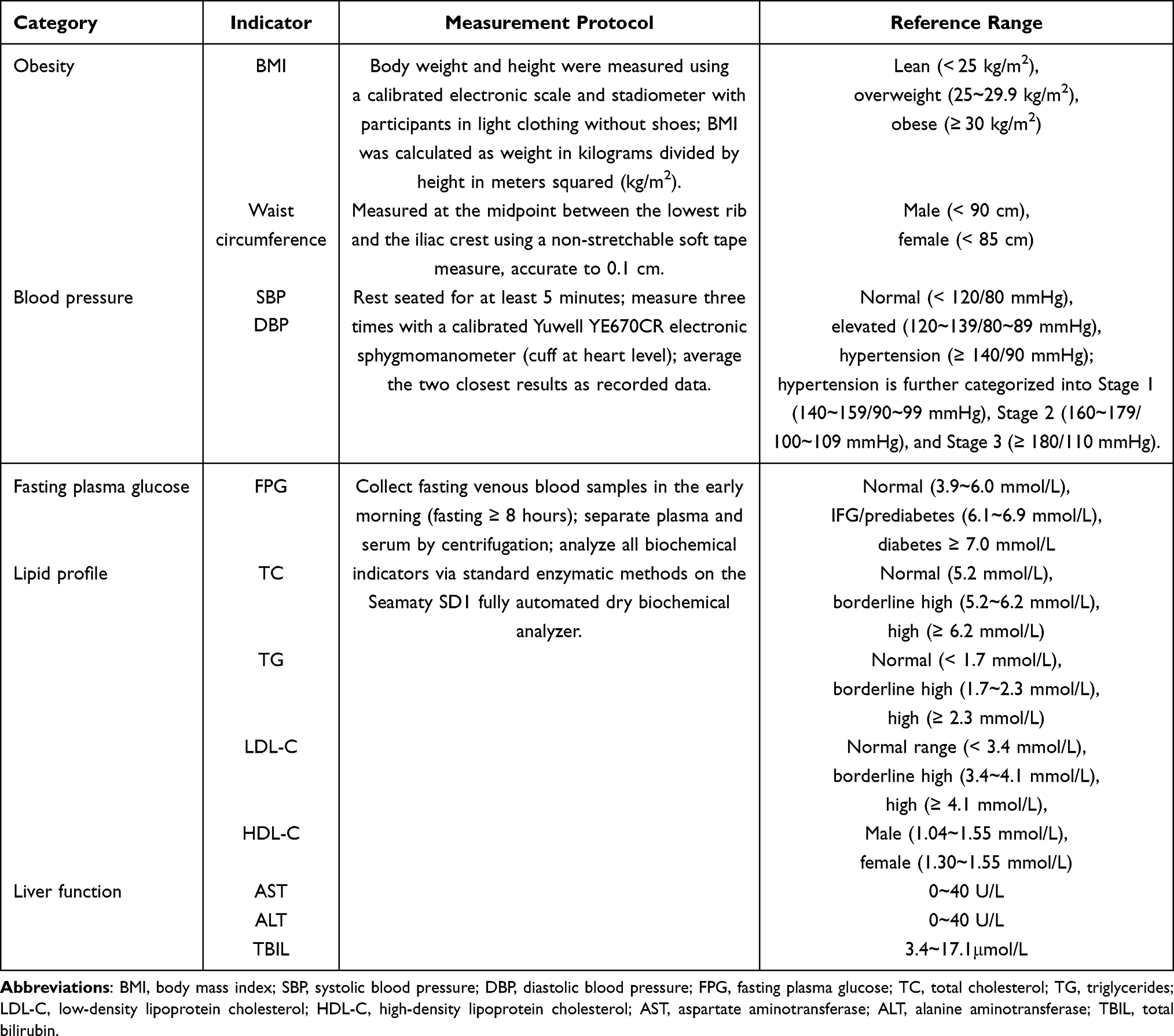 |
Table 1 Measurement Protocols and Analytical Methods of Metabolic Parameters |
Electrocardiogram Acquisition
Standard 12-lead ECGs were acquired with a GE MAC5500 HD electrocardiograph (GE Healthcare, USA). With the patient in a supine position at rest, the four limb electrodes and six precordial electrodes were placed in accordance with standard anatomical locations. Signal quality and lead connection integrity were verified using the device’s integrated “Hookup Advisor” feature. Participants were instructed to remain still and breathe normally during the recording. ECG signals were then collected at a sampling rate of 16,000 samples per second. All acquired tracings were stored electronically for centralized archiving and subsequent analysis.
Outcome Definition and Adjudication
ECG is a non-invasive modality that provides a direct representation of cardiac electrophysiological activity, enabling the detection of rhythm disorders and morphological abnormalities. In this study, we employed specific ECG anomalies as markers of subclinical cardiovascular risk, defined as an elevated susceptibility to future clinical events in asymptomatic individuals without a prior CVD diagnosis.15,17 These ECG patterns are established indicators of underlying cardiovascular pathology that can manifest before overt symptoms arise. All ECG interpretations were performed independently by two certified cardiologists. Any discrepancies in initial readings were resolved through adjudication by a third senior cardiologist. Based on American Heart Association (AHA) guidelines, high cardiovascular risk was defined as the presence of one or more of the following confirmed abnormalities: ① myocardial ischemia/injury, ② repolarization abnormality, ③ myocardial necrosis, ④ conduction disturbance, ⑤ arrhythmia.
Statistical Analysis
Analysis of Baseline Characteristics and Confounding Factor Selection
All analyses were performed on a complete-case basis. Baseline data were analyzed using SPSS 22.0. Categorical variables were summarized as frequencies and percentages. Certain continuous variables, such as age, were categorized based on established clinical cut-points and analyzed as categorical variables. Group differences between patients with and without incident ECG risk were assessed using chi-square tests. Covariates for adjustment in multivariable models were selected through a two-step process: first, sex and age were included a priori based on established clinical relevance. Second, lifestyle and clinical history variables (including dietary habits, exercise frequency, smoking history, alcohol consumption, and family history of CVD) that demonstrated a significant association (p < 0.05) in univariate analysis were retained as mandatory adjustments to control for potential confounding. Data on specific medication use were not systematically collected or included as covariates, as the metabolic trajectory groups are considered to integrate the net effect of both underlying pathophysiology and any concomitant pharmacological management.
Modeling of Metabolic Trajectories
To identify heterogeneous trajectories of metabolic indicators over time, this study employed GBTM, implemented using the traj plugin in STATA 17.0. For each indicator, models with 3 to 5 trajectory groups were fitted, examining linear, quadratic, and cubic functional forms. Parameters were estimated via maximum likelihood estimation, and non-significant terms were iteratively pruned to simplify the model. Final model selection was based on the following criteria: (1) goodness-of-fit, with the Bayesian Information Criterion (BIC) serving as the primary criterion—models with smaller BIC values were preferred; (2) classification reliability, requiring an average posterior probability (AvePP) > 0.7 for each trajectory subgroup to ensure robust individual classification; and (3) clinical interpretability, ensuring that trajectory subgroups were clinically meaningful and each accounted for at least 5% of the sample. Based on these criteria, trajectory group labels were generated for all 12 metabolic indicators and included as key predictor variables in subsequent analyses.
Validation of Predictive Model Performance
To evaluate the clinical utility of the metabolic trajectory framework, this study constructed both a cross-sectional model and a trajectory-enhanced model. All analyses were implemented in Python 3.12, leveraging the scikit-learn and XGBoost libraries. The cross-sectional model employed L1-regularized logistic regression, with input features consisting of baseline covariates and the three-year average values of metabolic indicators. The trajectory-based model was built using the gradient boosting machine (GBM) algorithm, incorporating baseline covariates and trajectory group labels derived from GBTM as input features. Model performance was evaluated using a nested 5-fold cross-validation framework, which consisted of an outer loop for performance estimation and an inner loop for model selection: In the outer loop, the dataset was randomly partitioned into five mutually exclusive subsets. Each subset served as the test set once, while the remaining four were used as the training set, resulting in five independent training-test splits. Within each training set of the outer loop, an inner 5-fold cross-validation was performed to optimize the hyperparameters of the GBM model via grid search, maximizing the mean area under the curve (AUC). This nested design ensured that hyperparameter tuning was conducted without exposure to the outer-loop test set, thereby preventing information leakage. After completing all five outer folds, predictions from each test set were aggregated, and the average values of performance metrics—including the AUC, Brier score, integrated discrimination improvement (IDI), and net reclassification improvement (NRI)—were calculated. This comprehensive comparison was designed to determine whether dynamic metabolic trajectories provide statistically significant incremental predictive value over conventional static metabolic indicators.
Assessment of the Impact of Metabolic Trajectories on CVD Risk
This analysis aimed to identify metabolic trajectories associated with the three-year cumulative cardiovascular risk. Given the annual assessment schedule, the exact timing of ECG abnormality onset was interval-censored. Therefore, multivariable logistic regression was employed as the standard and most appropriate method, as it is designed to model the probability of a binary outcome over a fixed period. This approach aligns with both the data structure and the research objective, as it does not require precise time-to-event data.
To evaluate the independent associations, an initial model incorporating all trajectory groups and pre-selected covariates was constructed. Significant trajectory variables were identified using backward elimination (removal threshold p > 0.10) to obtain a parsimonious model that yields clinically interpretable odds ratios (ORs) with 95% confidence intervals (CIs). The final model retained all variables with p < 0.05.
Results
Baseline Characteristics
The cohort comprised 1086 elderly patients diagnosed with MAFLD. During the follow-up period, 877 patients (80.76%) developed new-onset ECG abnormalities, while 209 patients (19.24%) remained free of such events until the study endpoint. Comparison of baseline characteristics between groups revealed expected differences in sex and age distributions. A significant difference was observed in dietary patterns: patients in the non-CVD group were nearly twice as likely to report a predominantly vegetarian diet (15.31%) compared to those in the CVD group (7.75%). No statistically significant differences were found between groups regarding exercise frequency, smoking history, alcohol consumption, or family history of cardiovascular disease (Table 2).
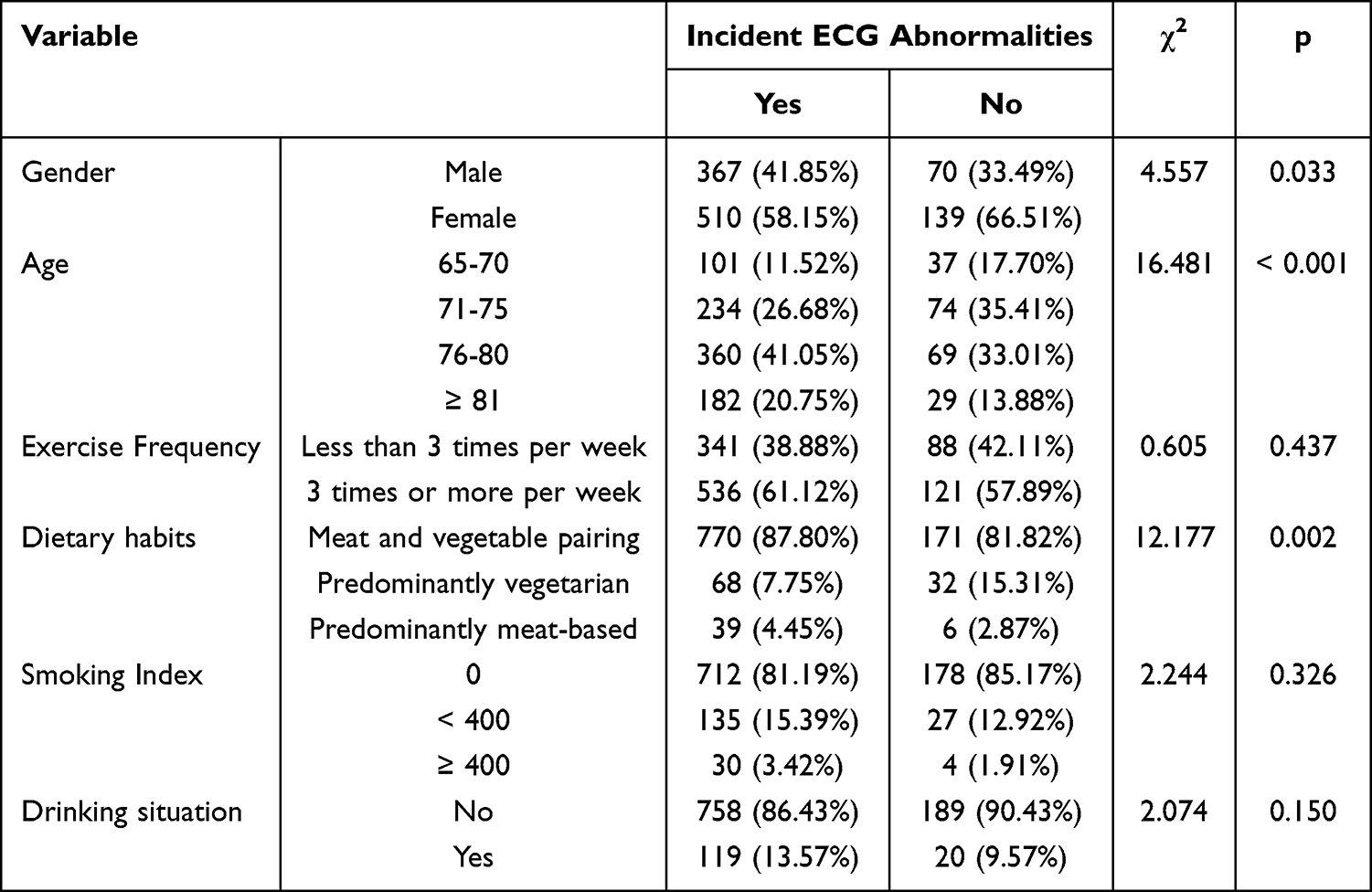 |
Table 2 Baseline Characteristics and Stratification by ECG-Defined Cardiovascular Risk According to Demographic and Lifestyle Factors |
Model Fit and Trajectory Group Characteristics
GBTM was applied to characterize the longitudinal patterns of key metabolic indicators, including obesity, blood pressure, fasting plasma glucose, lipid profile, and liver function parameters. All identified trajectory groups demonstrated a good fit to the data, with AvePP exceeding 0.7, which confirms appropriate classification reliability and model adequacy. The defining characteristics and detailed data for each trajectory subgroup are presented in Table 3, while the shapes of the trajectories are illustrated in Figure 2.
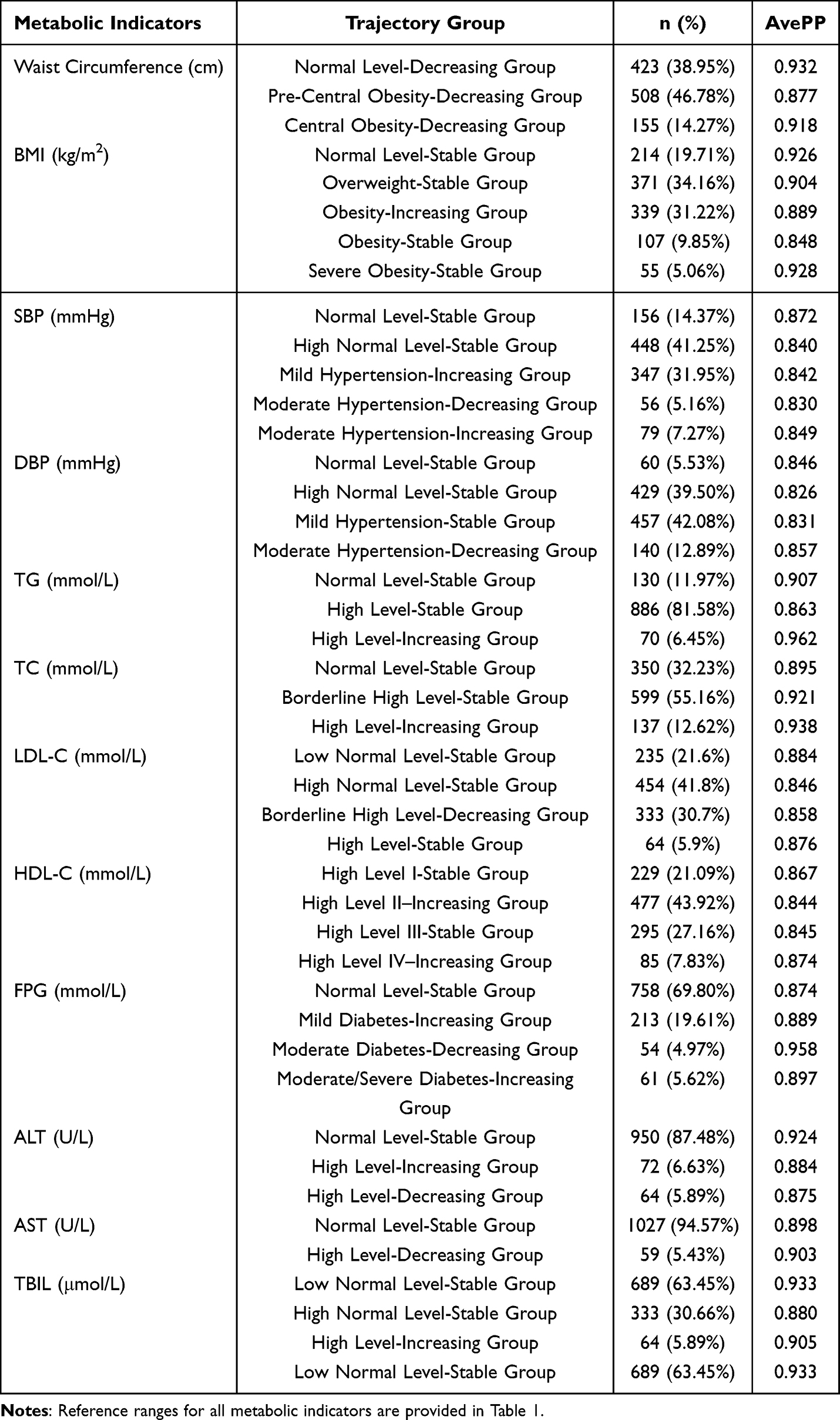 |
Table 3 Longitudinal Trajectory Patterns of Key Metabolic Indicators |
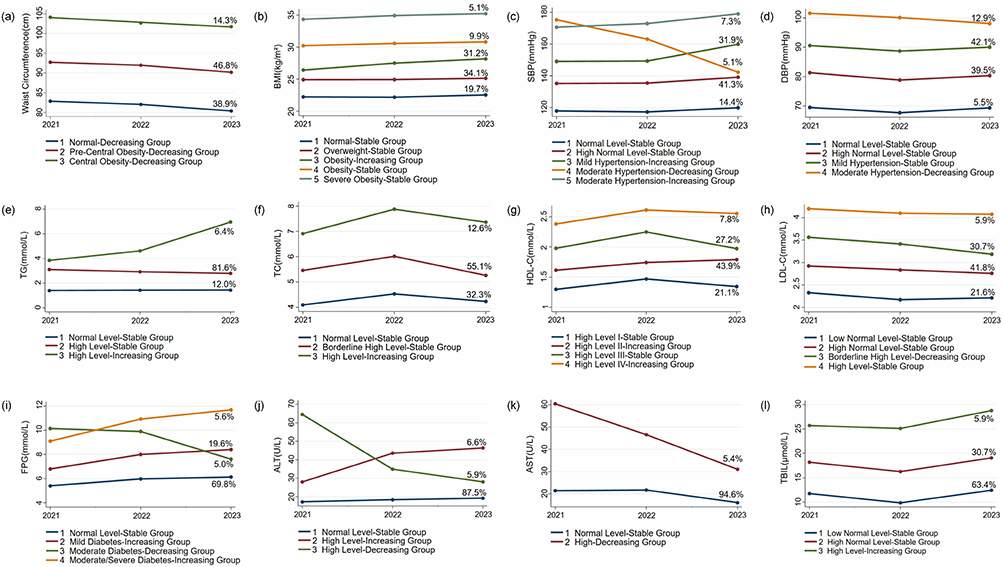 |
Figure 2 Longitudinal trajectories of key metabolic indicators derived from GBTM in elderly MAFLD patients during a three-year follow-up period. Notes: (a) Waist Circumference (cm); (b) body mass index (BMI, kg/m2); (c) systolic blood pressure (SBP, mmHg); (d) diastolic blood pressure (DBP, mmHg); (e) triglycerides (TG, mmol/L); (f) total cholesterol (TC, mmol/L); (g) high-density lipoprotein cholesterol (HDL-C, mmol/L); (h) low-density lipoprotein cholesterol (LDL-C, mmol/L); (i) fasting plasma glucose (FPG, mmol/L); (j) alanine aminotransferase (ALT, U/L); (k) aspartate aminotransferase (AST, U/L); (l) total bilirubin (TBIL, μmol/L). The X-axis spans annual time points (2021 to 2023). The Y-axis scales reflect measurement ranges of respective indicators. |
Comparative Predictive Performance of Dynamic Metabolic Trajectory Models
After adjustment for potential confounders including sex, age, and dietary habits, a systematic comparison was conducted between the dynamic trajectory model and the conventional cross-sectional model in predicting cardiovascular risk among elderly MAFLD patients. The results demonstrated superior performance of the trajectory-based approach (Table 4).
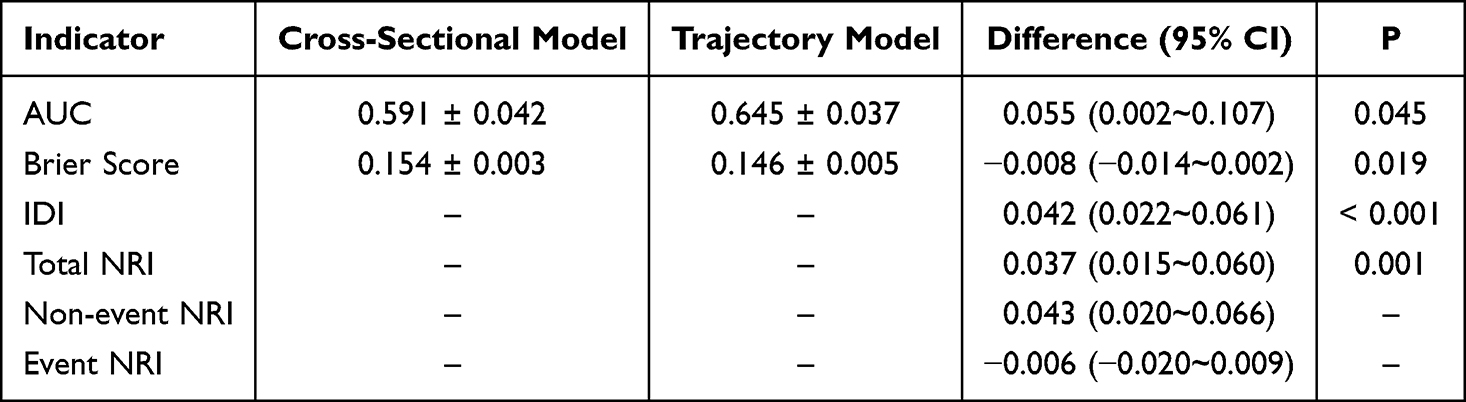 |
Table 4 Comparison of Predictive Performance Between the Trajectory-Based Model and Cross-Sectional Model |
Comparison of ROC curves (Figure 3) indicated that the dynamic trajectory model exhibited a statistically significant improvement in discriminatory accuracy over the cross-sectional model (ΔAUC = 0.054, P = 0.045). The trajectory model’s ROC curve consistently lay above that of the cross-sectional model across the entire range of specificities, indicating uniformly higher sensitivity. A reduction in the Brier score (Δ = −0.008, P = 0.019) suggested that the predicted probabilities generated by the trajectory model were closer to the actual observed outcomes with smaller overall error. Improvement in integrated discrimination index (IDI = 0.042, P < 0.001) further confirmed enhanced overall discriminatory ability of the trajectory model. Analysis of the NRI indicated that the trajectory model correctly reclassified an additional 3.74% of the patients (total NRI = 0.037, P = 0.001). This improvement was primarily driven by enhanced identification of low-risk individuals (non-event NRI = 0.043), whereas classification accuracy for high-risk subjects showed minimal change (event NRI = −0.006), indicating potential for further refinement in this subgroup. Finally, the distribution of predicted probabilities (Figure 4) demonstrated that the trajectory model achieved more effective risk stratification, with reduced distributional overlap between the CVD and non-CVD groups.
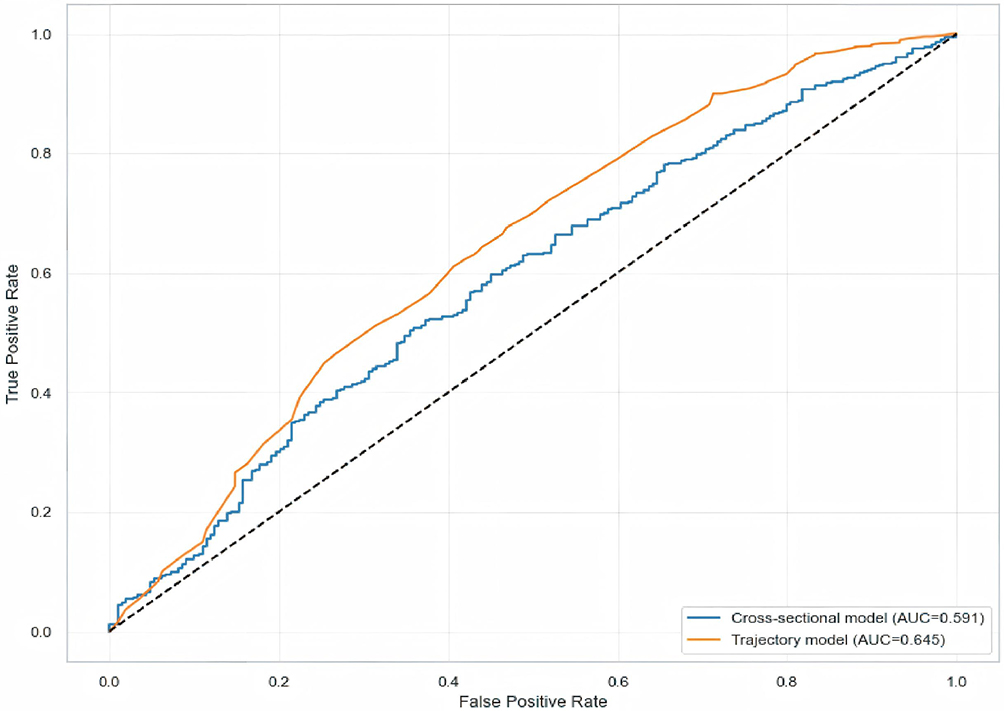 |
Figure 3 The trajectory model demonstrates superior discriminative performance for ECG-defined cardiovascular risk prediction compared to the cross-sectional model in elderly MAFLD patients. Notes: The yellow line represents the trajectory model (Area Under the Curve, AUC = 0.645), and the blue line represents the cross-sectional model (AUC = 0.591). The diagonal grey line indicates reference performance equivalent to random chance (AUC = 0.5). The X-axis spans the False Positive Rate (1 - Specificity) from 0.0 to 1.0. The Y-axis spans the True Positive Rate (Sensitivity) from 0.0 to 1.0. |
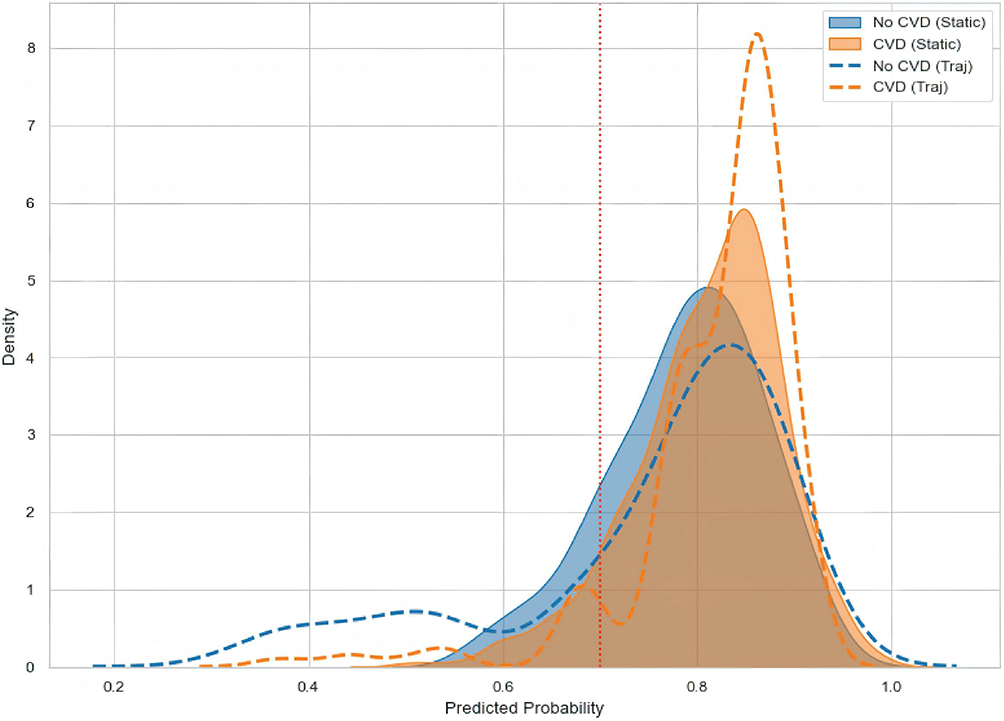 |
Figure 4 The trajectory model shows improved separation of predicted ECG-defined cardiovascular risk between patients with and without events compared to the cross-sectional approach. Notes: Density curves illustrate the separation of predicted probabilities between patients who developed CVD (yellow) and those who did not (blue) under the static model (solid lines) and the trajectory-based model (dashed lines). The trajectory model demonstrates improved risk stratification, with less overlap between the CVD and non-CVD groups compared to the static model, indicating its enhanced ability to discriminate high-risk from low-risk individuals. The X-axis spans the predicted probability of cardiovascular risk from 0.0 to 1.0. The Y-axis represents the probability density. Greater separation between the No CVD and CVD density curves for a given model indicates better discriminative ability in risk stratification. The trajectory model shows improved separation compared to the cross-sectional model. |
Assessment of the Impact of Metabolic Trajectories on Subclinical Cardiovascular Risk
To further evaluate the predictive utility of the trajectory model, multivariable logistic regression was used to quantify the specific effects of distinct metabolic trajectories on ECG-defined cardiovascular risk (Table 5). In light of the high outcome incidence, adjusted relative risks (aRR) are presented alongside adjusted odds ratios (aOR) to facilitate a more direct clinical interpretation of the effect sizes.
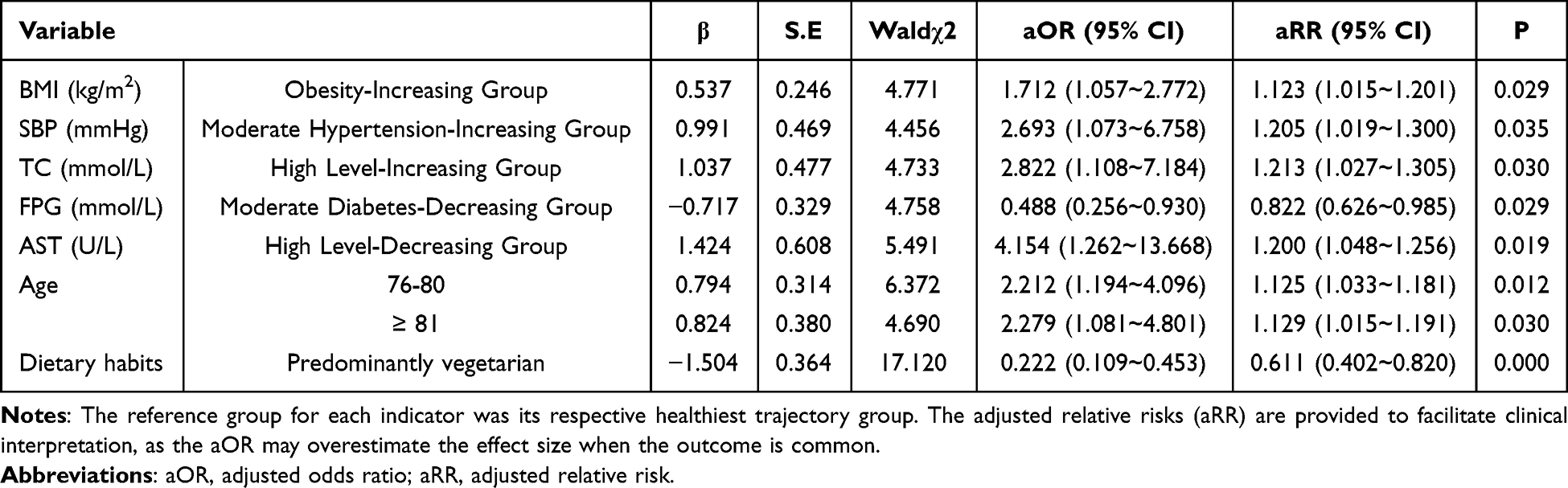 |
Table 5 Factors Associated with ECG-Defined Cardiovascular Risk in Elderly MAFLD Patients: Results from Multivariable Logistic Regression Analysis |
Participants in the “Obesity-Increasing” BMI trajectory exhibited significantly elevated ECG-defined cardiovascular risk (aOR = 1.71, 95% CI: 1.06~2.77; aRR = 1.12, 95% CI: 1.02~1.20), corresponding to a 12% increase in absolute risk compared to the “Normal-Stable” reference group. Similarly, the “Moderate Hypertension-Increasing” SBP trajectory was associated with substantially higher risk (aOR = 2.69, 95% CI: 1.07~6.76; aRR = 1.21, 95% CI: 1.02~1.30), representing a 21% increase in absolute risk. The “High Level-Increasing” TC trajectory also demonstrated a strong association (aOR = 2.82, 95% CI: 1.11~7.18; aRR = 1.21, 95% CI: 1.03~1.31), indicating a 21% increase in absolute risk. Conversely, the “Moderate Diabetes-Decreasing” trajectory group showed a significantly reduced ECG-defined cardiovascular risk (aOR = 0.49, 95% CI: 0.26~0.93; aRR = 0.82, 95% CI: 0.63~0.99), representing a 18% reduction in absolute risk. Notably, even when AST levels showed a declining trend, patients in the “High Level-Decreasing” AST trajectory maintained substantially elevated risk (aOR = 4.15, 95% CI: 1.26~13.67; aRR = 1.20, 95% CI: 1.05~1.26), indicating a 20% increase in absolute risk compared to those with persistently normal liver function.
Regarding non-metabolic factors, participants aged 76–80 years (aOR = 2.21, 95% CI: 1.19~4.10; aRR = 1.13, 95% CI: 1.03~1.18) and ≥ 81 years (aOR = 2.28, 95% CI: 1.08~4.80; aRR = 1.13, 95% CI: 1.02~1.19) showed a 13% increase in ECG-defined cardiovascular risk compared to the 65–70-year reference group. In contrast, adherence to a predominantly vegetarian diet was associated with markedly lower risk (aOR = 0.22, 95% CI: 0.11~0.45; aRR = 0.61, 95% CI: 0.40~0.82), representing a 39% reduction in absolute risk.
To assess the potential impact of participants excluded due to incomplete follow-up (n = 129) on the primary findings, we conducted a sensitivity analysis under two extreme scenarios. The magnitude, direction, and statistical significance of the key associations presented in Table 5 remained substantially unchanged under both scenarios, confirming the robustness of our conclusions regarding the independent associations between specific metabolic trajectories and ECG-defined cardiovascular risk.
Discussion
This three-year longitudinal study provides the first systematic investigation into the value of dynamic trajectories of metabolic indicators for predicting subclinical cardiovascular risk in elderly patients with MAFLD. The key findings reveal several clinically relevant insights: First, a prediction model incorporating dynamic metabolic trajectories demonstrated significantly improved performance compared to conventional models based on static mean values. Second, adverse metabolic trajectories—including progressive obesity, persistent hypertension and hypercholesterolemia, and the legacy effect of liver injury—were identified as strong independent risk factors for CVD. Conversely, trajectories indicating metabolic improvement, such as effective glycemic control in diabetes, were associated with a protective effect. Third, advanced age emerged as an important risk factor, while a vegetarian diet was correlated with significant cardiovascular protection. These findings offer new theoretical support and potential interventional strategies for personalized CVD risk management in older adults with MAFLD.
Strengths of this study lie in its novel methodological framework and shifted clinical perspective. First, we introduce and validate a systematic, dynamic risk-assessment framework based on longitudinal metabolic trajectories. This operable and scalable framework advances the clinical management paradigm for elderly MAFLD patients from a focus on “static parameter control” to proactive “dynamic trend intervention”. Second, beyond methodological innovation, our analysis has preliminarily identified several metabolic trajectory patterns with distinct clinical implications. These empirical patterns offer novel, hypothesis-generating insights for future mechanistic research into the temporal dynamics of metabolic dysregulation and cardiovascular damage. Third, by employing ECG-defined subclinical cardiovascular risk as the primary endpoint, our study shifts focus toward earlier, pre-symptomatic risk identification. This approach provides a finer-grained lens for stratifying and managing cardiovascular risk in this growing, high-risk elderly population, where the probability of comorbid events is substantial and outcomes are severe.
The most significant finding of this study is that the metabolic trajectory model demonstrated statistically superior predictive performance for subclinical cardiovascular risk compared to the conventional cross-sectional model. The key result is not the model’s absolute discriminatory ability (AUC = 0.645)—which remains moderate—but the consistent and measurable improvement achieved by integrating trajectory information (ΔAUC = 0.054, IDI = 0.042, NRI = 0.037). This confirms that the “trend” of metabolic indicators provides incremental prognostic information beyond a single “state” measurement when assessing risk in elderly MAFLD patients. The underlying mechanism may lie in the fact that dynamic trajectories more accurately reflect the persistent dysregulation of metabolic homeostasis—that is, the cumulative effect of metabolic burden on the organism.18
From a clinical interpretation perspective, the metabolic trajectories identified in this study should be understood as underlying physiological trends and the effects of clinical management, including pharmacological interventions. For instance, trajectories showing an improving trend likely reflect effective therapeutic interventions. This integration, however, does not compromise the reliability of our findings but rather enhances their clinical utility. In real-world patient management, the achieved metabolic status—whether improved through lifestyle modifications or medication—is what ultimately determines cardiovascular risk. Thus, these trajectories function as composite prognostic indicators, whose primary utility lies in identifying patients in whom overall management has effectively reduced risk.
The AHA has emphasized that both the severity and duration of obesity are critically linked with CVD risk.19 Our study extends this concept by quantifying it specifically in an elderly MAFLD population. The “Obesity-Increasing” trajectory was associated with a 12% increase in ECG-defined cardiovascular risk (aRR = 1.12), underscoring that it is not merely the state of obesity, but rather the biologically active process of continuing weight gain that amplifies cardiovascular risk. This process exacerbates lipotoxicity and pro-inflammatory responses from adipose tissue, which concurrently affect both the liver and vascular system via the portal and systemic circulation.20,21 Similarly, the “Moderate Hypertension-Increasing” trajectory, which conveys a 21% risk increase (aRR = 1.21), highlights the peril of dynamic deterioration. It captures active disease progression in individuals with pre-existing hypertension, reflecting progressive hemodynamic stress and decompensated vascular regulation.22 This dynamic worsening itself constitutes an independent risk signal that cannot be discerned from single-point blood pressure measurements. This is especially consequential in elderly individuals, whose vascular systems are more vulnerable due to age-related arteriosclerosis and reduced elasticity.23 When superimposed on the pro-hypertensive environment characteristic of MAFLD, the effect of steadily rising blood pressure is further amplified, thereby underscoring the prognostic value of monitoring dynamic trajectory patterns. The “High Level-Increasing” TC trajectory, also corresponding to a 21% risk increase (aRR = 1.21), further emphasizes the necessity of dynamic monitoring in cholesterol management. MAFLD-related liver dysfunction and systemic inflammation readily foster a pro-atherogenic environment, leading to progressive accumulation of cholesterol within the vascular endothelium.24 Identifying a steadily rising TC trajectory is therefore equivalent to detecting an active phase of this vicious cycle.
For elderly MAFLD patients, the principal cardiovascular risk stems not only from isolated metabolic abnormalities at a single time point, but more critically from a sustained dysregulation of metabolic control—reflecting a pronounced decline in the ability to maintain physiological homeostasis. This implies that management strategies must shift from “parameter control” to proactive “trajectory intervention”. Consequently, clinical practice should advance beyond asking, “Are current blood pressure, weight, or cholesterol levels at target?” to also inquiring, “How has this parameter changed over recent years—has it remained stable, improved, or worsened?” Interventions should therefore be initiated earlier in the disease continuum—focusing not only on treating manifest disease but also on identifying and actively reversing adverse trajectories.
Our study found that even after AST levels normalized, patients in the “High-Level-Decreasing” trajectory still exhibited a significantly elevated risk of ECG-defined cardiovascular events (aRR = 1.20) compared to those with persistently normal liver function. This observation aligns with the concept of “metabolic memory”.14 This theory posits that past metabolic disturbances can induce long-term complications through lasting biological alterations, such as epigenetic reprogramming.14 These changes can sustain abnormal gene expression and a pro-inflammatory state even after the initial insult has resolved—a phenomenon well-documented in conditions like diabetes.25 Thus, we hypothesize that early liver injury in MAFLD may similarly activate a persistent “memory” program, entrenching pro-inflammatory features within hepatic and systemic immune cells. This process could continuously fuel vascular inflammation and accelerate atherosclerosis, leading to a prolonged increase in cardiovascular risk.26 Although our study did not directly measure these molecular markers, this theoretical framework provides a plausible mechanistic direction for understanding the long-term cardiovascular sequelae of liver injury. This finding implies that for MAFLD patients with a history of liver injury, cardiovascular risk management must look beyond the mere “normalization” of current biochemical markers and adopt a more proactive, long-term strategy.
One of the most instructive findings was the significant cardiovascular protection associated with the “Moderate Diabetes-Decreasing” trajectory (aRR = 0.82). This seemingly paradoxical result underscores that the direction of metabolic change holds greater prognostic value than static levels. It strongly aligns with the established glycemic “legacy effect”, wherein early improvement in glucose control yields long-term cardiovascular benefits that persist for decades.27 Successful reduction of blood glucose—whether achieved through lifestyle or pharmacological intervention—likely indicates a broad improvement in systemic metabolic health beyond glycemia alone.28 Our findings collectively reveal two contrasting faces of metabolic memory in MAFLD. On one hand, liver injury may leave irreversible “metabolic scars” that perpetuate CVD risk. On the other hand, glucose regulation exhibits high plasticity; its active reversal, as shown here, can initiate a durable protective state, yielding a substantial “metabolic dividend”. Thus, for elderly MAFLD patients with diabetes, actively reversing dysglycemia is not merely about immediate control but a critical step to establish a long-term protective trajectory and alter future cardiovascular risk.
This study also highlights the importance of non-metabolic factors. Even within this elderly cohort, advancing age demonstrated a significant gradient effect on cardiovascular risk.29 Participants aged 76–80 and ≥ 81 years showed a 13% increase in absolute risk (aRR = 1.13) compared to those aged 65–70, indicating a synergistic interaction between physiological aging and metabolic aging in patients with MAFLD. Aging inherently involves a progressive decline in physiological reserve and irreversible vascular senescence.30 In the context of MAFLD, the aging process forms a vicious cycle with hepatic metabolic dysfunction and chronic low-grade inflammation, collectively accelerating atherosclerosis. Advanced age thus serves as a biological amplifier of cumulative damage rather than merely a demographic trait. Furthermore, the sociological dimensions of aging cannot be overlooked. Advanced age is often accompanied by social isolation, cognitive decline, and polypharmacy, which may indirectly elevate CVD risk by affecting self-management behaviors.31 In contrast, adherence to a predominantly vegetarian diet was associated with a 39% reduction in ECG-defined cardiovascular risk (aRR = 0.61). We interpret this finding as preliminary, hypothesis-generating evidence that supports the potential value of plant-based diets in this specific population, while explicitly acknowledging that residual confounding and the observational design preclude causal inference. The observed association aligns with the established cardioprotective properties of plant-based foods, which are rich in fiber, antioxidants, and unsaturated fatty acids—nutrients known to improve lipid profiles and attenuate inflammatory pathways.32 Furthermore, in the local context of Weifang, such a dietary pattern may confer benefit not only by reducing the intake of high-salt preserved foods but also by potentially increasing the consumption of potassium-rich vegetables (eg, green radish) and, given regional dietary staples, whole grains and diversified flour-based foods.33 Future studies with detailed dietary quantification and objective biomarkers are warranted to clarify the precise role and optimal composition of plant-based diets in this high-risk population.34 Ultimately, any dietary modification for elderly patients with complex conditions like MAFLD should be undertaken with individualized guidance from healthcare professionals.35
In summary, our findings suggest that cardiovascular risk management in elderly patients with MAFLD requires a paradigm shift from static parameter control toward dynamic and individualized trend intervention. Particularly for those with a history of liver injury, while they should be regarded as a long-term high-risk population, it is crucial to carefully avoid potential over-medicalization and psychological burden in this elderly group.36 Therefore, we emphasize that any long-term monitoring and intervention strategy must adhere to the core principles of “individualization” and “risk stratification”. Specifically, a focused periodic assessment plan (eg, annual ECG, liver and kidney function, and basic metabolic panels) should be formulated based on the patient’s overall health status, comorbidities, functional capacity, and personal preferences, rather than conducting frequent and ineffective screenings. Implementing a “shared decision-making” process to fully communicate the rationale and goals of ongoing monitoring with patients is essential for alleviating psychological burden and achieving precise prevention with maximal benefit and minimal burden.
Limitations
The interpretations of our findings should be considered in the context of several limitations. First, while the use of ECG abnormalities as an outcome measure allowed efficient early screening of subclinical cardiovascular risk, it lacks the specificity to differentiate distinct disease subtypes—unlike hard clinical endpoints such as myocardial infarction or stroke. Second, the categorical assessment of several baseline characteristics, though pragmatic for data collection in this elderly community-based cohort, limits analytical granularity. For instance, dietary pattern was classified simply as vegetarian, meat-based, or mixed, lacking quantification of specific nutrients, caloric intake, or socioeconomic correlates. This approach, coupled with the single-region (Weifang) design and reliance on self-reporting, may introduce regional specificity, measurement error, and recall bias. Third, the annual follow-up design meant that the exact timing of ECG abnormality onset could not be determined, resulting in interval-censored data. This precluded the use of survival analysis to investigate how metabolic trajectories influence the time to event. Future studies with more frequent assessments are needed to explore these temporal dynamics. Fourth, although the primary aim was to demonstrate the incremental value of dynamic trajectories rather than to develop a clinical prediction model, we acknowledge that the absolute predictive performance of the combined baseline-trajectory model remains moderate. To develop a tool with sufficient discriminative power for direct clinical application, future studies should integrate dynamic trajectories with a broader array of biomarkers. Fifth, our application of group-based trajectory modeling, while suitable for identifying longitudinal patterns, has inherent methodological limitations. These include the potential for trajectory misclassification, the influence of regression to the mean, and a degree of dependence on the frequency and timing of measurements. Sixth, a related and important translational challenge is determining the clinically actionable threshold for what constitutes a significant “trend” warranting intervention. Our study identifies high-risk trajectories but does not establish precise thresholds for when a trend should trigger clinical action, which is a key step for translating this framework into practical protocols. Seventh, this study did not systematically collect or adjust for the use of specific medications. Although the identified metabolic trajectories can be regarded as valid composite predictors of cardiovascular risk, it remains challenging to distinguish to what degree these trajectory changes are attributable to the natural disease course versus therapeutic intervention. Eighth, baseline liver disease severity was not quantitatively assessed, primarily due to ethical and resource constraints. Although exclusion criteria controlled for advanced disease, the lack of direct adjustment for fibrosis or steatosis severity remains a limitation. Ninth, and finally, our study cohort consisted exclusively of elderly patients with MAFLD from a single region in China, and our models have not yet been externally validated. Consequently, while the core finding—that dynamic metabolic trajectories outperform static measures—is likely generalizable, the specific trajectory patterns and risk thresholds identified here may not be directly applicable to populations with differing genetic backgrounds, dietary habits, or healthcare systems. Future research should prioritize the validation and refinement of these models in independent, multi-center, and more diverse cohorts.
Notwithstanding these limitations, the dynamic trajectory assessment framework proposed in this study offers a valuable new perspective for identifying and managing cardiovascular risk at a subclinical stage in elderly patients with MAFLD.
Conclusion
This study demonstrates the significant value of dynamic metabolic trajectory in predicting cardiovascular risk among elderly patients with MAFLD, using longitudinal trajectory modeling. Our findings advocate a shift in clinical management strategies from “static parameter control” toward “dynamic trend intervention”. Trajectories of ongoing deterioration in indicators such as obesity, blood pressure, and cholesterol were identified as strong early warning signals for cardiovascular events, highlighting the need for heightened vigilance and early intervention in progressively worsening metabolic abnormalities. Notably, even when liver enzyme levels later normalized, baseline liver injury continued to confer a persistently elevated cardiovascular risk. This “legacy effect” suggests that early hepatic insults may incur lasting risk, potentially through mechanisms such as entrenched low-grade inflammation, underscoring the need for long-term vigilance beyond biochemical normalization. On the other hand, indicators with high metabolic plasticity—such as blood glucose—can yield substantial cardiovascular benefits through active intervention and reversal. Furthermore, a predominantly vegetarian diet was associated with significant risk reduction, supporting its consideration within tailored dietary strategies; however, this observational finding requires individual assessment and may be influenced by unmeasured lifestyle or socioeconomic factors. Importantly, advancing age acts as an independent amplifier of cardiovascular risk. For older adults, any long-term monitoring strategy must be individualized and risk-stratified to carefully balance prevention benefits against the potential for over-medicalization and psychological burden. In summary, these findings extend the current risk prediction model by integrating the dimension of time, offering a novel, proactive framework for cardiovascular prevention in this high-risk aging population.
Author Contribution
Zhangyi Liu: Conceptualization, Methodology, Formal analysis, Investigation, Writing – Original Draft, Writing – Review & Editing, Visualization, Project administration. Yongli Liu: Conceptualization, Investigation, Resources, Data Curation, Writing – Review & Editing. Bintao Liu: Conceptualization, Formal analysis, Writing – Review & Editing, Visualization. Mei Zhao: Formal analysis, Investigation, Writing – Original Draft. Yu Lu: Methodology, Formal analysis, Data Curation, Writing – Review & Editing, Supervision, Project administration. Xiaoqing Zhang: Conceptualization, Methodology, Writing – Review & Editing, Supervision, Project administration, Funding acquisition. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Data Sharing Statement
The data analyzed during the current study are not publicly available due to ethical restrictions but are available from the first author, Zhangyi Liu ([email protected]), upon reasonable request.
Ethics Approval
The study protocol adhered to the ethical principles outlined in the Declaration of Helsinki and received approval from the Institutional Ethics Committee of Dongzhimen Hospital (Approval No. 2023DZMEC-228-02). Written informed consent was secured from all participants before study enrollment.
Acknowledgments
We gratefully acknowledge the cardiovascular specialists at Dongzhimen Hospital, Beijing University of Chinese Medicine and Weifang Kuiwen Hengkang Hospital for their professional guidance in clinical protocol development and data interpretation. We also sincerely thank Qiong Wu and Chao Wang from the Institute of Basic Theory of Traditional Chinese Medicine, China Academy of Chinese Medical Sciences for their valuable assistance in study design and for their insightful suggestions during manuscript revision in response to reviewers’ comments.
Funding
This work was supported by the National Key Research and Development Program of China (No. 2022YFC3502301), the Beijing Natural Science Foundation Youth Project (No. 7262206, 7264389), the Traditional Chinese Medicine Monitoring and Statistical Research Project (No. 2025JCTJE9), the Special Funding Program of Beijing University of Chinese Medicine (No. BZY-BZX-2022-04), and the Funding of the China Academy of Chinese Medical Sciences (No. ZZ19-YQ-065, ZZSYS-1903-02CZ)
Disclosure
The authors report no conflicts of interest in this work.
References
1. Partridge L, Deelen J, Slagboom PE. Facing up to the global challenges of ageing. Nature. 2018;561(7721):45–17. doi:10.1038/s41586-018-0457-8
2. Ferrucci L, Wilson DM 3rd, Donega S, Montano M. Enabling translational geroscience by broadening the scope of geriatric care. Aging Cell. 2024;23(1):e14034. doi:10.1111/acel.14034
3. Guo Z, Wu D, Mao R, Yao Z, Wu Q, Lv W. Global burden of MAFLD, MAFLD related cirrhosis and MASH related liver cancer from 1990 to 2021. Sci Rep. 2025;15(1):7083. doi:10.1038/s41598-025-91312-5
4. Eslam M, Fan JG, Yu ML, et al. The Asian Pacific association for the study of the liver clinical practice guidelines for the diagnosis and management of metabolic dysfunction-associated fatty liver disease. Hepatol Int. 2025;19(2):261–301.
5. Fan J, Xu X, Nan Y, et al. Guidelines for the prevention and treatment of metabolic-associated (non-alcoholic) fatty liver disease (2024 edition). J Pract Hepatol. 2024;27(4):494–510.
6. Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–1347. doi:10.1097/HEP.0000000000000004
7. Danpanichkul P, Kongarin S, Permpatdechakul S, et al. The surreptitious burden of nonalcoholic fatty liver disease in the elderly in the asia-pacific region: an insight from the global burden of disease study 2019. J Clin Med. 2023;12(20):6456. doi:10.3390/jcm12206456
8. Zhou J, Zhou F, Wang W, et al. Epidemiological features of NAFLD from 1999 to 2018 in China. Hepatology. 2020;71(5):1851–1864. doi:10.1002/hep.31150
9. Ni W, Yuan X, Zhang Y, Zhang H, Zheng Y, Xu J. Sociodemographic and lifestyle determinants of multimorbidity among community-dwelling older adults: findings from 346,760 SHARE participants. BMC Geriatr. 2023;23(1):419. doi:10.1186/s12877-023-04128-1
10. Lei F, Qin JJ, Song X, et al. The prevalence of MAFLD and its association with atrial fibrillation in a nationwide health check-up population in China. Front Endocrinol. 2022;13:1007171. doi:10.3389/fendo.2022.1007171
11. Zhou XD, Targher G, Byrne CD, et al. An international multidisciplinary consensus statement on MAFLD and the risk of CVD. Hepatol Int. 2023;17(4):773–791. doi:10.1007/s12072-023-10543-8
12. Zhou XD, Cai J, Targher G, et al. Metabolic dysfunction-associated fatty liver disease and implications for cardiovascular risk and disease prevention. Cardiovasc Diabetol. 2022;21(1):270. doi:10.1186/s12933-022-01697-0
13. Yang K, Song M. New insights into the pathogenesis of metabolic-associated fatty liver disease (MAFLD): gut-liver-heart crosstalk. Nutrients. 2023;15(18):3970. doi:10.3390/nu15183970
14. Dong H, Sun Y, Nie L, et al. Metabolic memory: mechanisms and diseases. Signal Transduct Target Ther. 2024;9(1):38. doi:10.1038/s41392-024-01755-x
15. Yagi R, Mori Y, Goto S, Iwami T, Inoue K. Routine electrocardiogram screening and cardiovascular disease events in adults. JAMA Intern Med. 2024;184(9):1035–1044. doi:10.1001/jamainternmed.2024.2270
16. Nagin DS, Jones BL, Elmer J. Recent advances in group-based trajectory modeling for clinical research. Annu Rev Clin Psychol. 2024;20(1):285–305. doi:10.1146/annurev-clinpsy-081122-012416
17. Krist AH. Screening ECGs for cardiovascular risk assessment. JAMA Intern Med. 2024;184(9):1044–1045. doi:10.1001/jamainternmed.2024.2279
18. Malekpour MR, Abbasi-Kangevari M, Ghamari SH, et al. The burden of metabolic risk factors in North Africa and the Middle East, 1990-2019: findings from the Global Burden of Disease Study. EClinicalMedicine. 2023;60:102022. doi:10.1016/j.eclinm.2023.102022
19. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;143(21):e984–e1010. doi:10.1161/CIR.0000000000000973
20. Azzu V, Vacca M, Virtue S, Allison M, Vidal-Puig A. Adipose tissue-liver cross talk in the control of whole-body metabolism: implications in nonalcoholic fatty liver disease. Gastroenterology. 2020;158(7):1899–1912. doi:10.1053/j.gastro.2019.12.054
21. Peng H, Zhao Z, Gong J, He K. BMI trajectories are associated with NAFLD and advanced fibrosis via aging-inflammation mediation. BMC Public Health. 2025;25(1):147. doi:10.1186/s12889-025-21322-5
22. Liu S, Zhao D, Wang M, et al. Association between cumulative blood pressure and long-term risk of cardiovascular disease: findings from the 26-year Chinese Multi-provincial Cohort Study-Beijing Project. Chin Med J. 2021;134(8):920–926. doi:10.1097/CM9.0000000000001383
23. Chatzis DG, Magounaki K, Pantazopoulos I, Beltsios ET, Katsi V, Tsioufis KP. Current management of hypertension in older adults. Drugs Aging. 2023;40(5):407–416. doi:10.1007/s40266-023-01013-9
24. Pipitone RM, Ciccioli C, Infantino G, et al. MAFLD: a multisystem disease. Ther Adv Endocrinol Metab. 2023;14:20420188221145549. doi:10.1177/20420188221145549
25. Bhattacharya S, Kalra S, Nagendra L, Dutta D. Forty-four years of the UK prospective diabetes study: legacy effect and beyond. touchREV Endocrinol. 2025;21(1):2–3. doi:10.17925/EE.2025.21.1.8
26. Kunutsor SK, Bakker SJ, Kootstra-Ros JE, Blokzijl H, Gansevoort RT, Dullaart RP. Inverse linear associations between liver aminotransferases and incident cardiovascular disease risk: the PREVEND study. Atherosclerosis. 2015;243(1):138–147. doi:10.1016/j.atherosclerosis.2015.09.006
27. Prattichizzo F, Ceriello A. The legacy effect of hyperglycaemia in type 2 diabetes. Lancet. 2025;405(10472):28. doi:10.1016/S0140-6736(24)02382-1
28. Jackson MA, Ahmann A, Shah VN. Type 2 diabetes and the use of real-time continuous glucose monitoring. Diabetes Technol Ther. 2021;23(S1):S27–S34. doi:10.1089/dia.2021.0007
29. Donato AJ, Machin DR, Lesniewski LA. Mechanisms of dysfunction in the aging vasculature and role in age-related disease. Circ Res. 2018;123(7):825–848. doi:10.1161/CIRCRESAHA.118.312563
30. Paneni F, Diaz Cañestro C, Libby P, Lüscher TF, Camici GG. The aging cardiovascular system: understanding it at the cellular and clinical levels. J Am Coll Cardiol. 2017;69(15):1952–1967. doi:10.1016/j.jacc.2017.01.064
31. Li X, Zhao C, Liu M, Zhao W, Pan H, Wang D. Sociodemographic index-age differences in the global prevalence of cardiovascular diseases, 1990-2019: a population-based study. Arch Public Health. 2025;83(1):2. doi:10.1186/s13690-024-01454-7
32. Threapleton DE, Greenwood DC, Evans CE, et al. Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis. BMJ. 2013;347:f6879.
33. Li Y, Wang L, Liu X, et al. Household food-consumption structure and characteristics of rural residents in Shandong Province based on in-home tracking surveys. J Nat Res. 2018;33(6):978–991.
34. Wang T, Masedunskas A, Willett WC, Fontana L. Vegetarian and vegan diets: benefits and drawbacks. Eur Heart J. 2023;44(36):3423–3439. doi:10.1093/eurheartj/ehad436
35. Petersen KS, Kris-Etherton PM. Diet quality assessment and the relationship between diet quality and cardiovascular disease risk. Nutrients. 2021;13(12):4305. doi:10.3390/nu13124305
36. Chen L, Huang Z, Jiang C, et al. Illness perception, coping and psychological distress among patients with metabolic dysfunction-associated fatty liver disease (MAFLD) in China. BMC Public Health. 2025;25(1):541. doi:10.1186/s12889-024-21260-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.