Back to Journals » Risk Management and Healthcare Policy » Volume 14
Dual Contraceptive Utilization and Associated Factors Among Reproductive-Age Women on Anti-Retroviral Therapy at Hospitals in Central Ethiopia
Authors Tilahun Y, Bala ET ![]() , Bulto GA
, Bulto GA ![]() , Roga EY
, Roga EY ![]()
Received 4 November 2020
Accepted for publication 6 February 2021
Published 15 February 2021 Volume 2021:14 Pages 619—627
DOI https://doi.org/10.2147/RMHP.S290362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Yohannes Tilahun,1 Elias Teferi Bala,2 Gizachew Abdissa Bulto,3 Ephrem Yohannes Roga3
1Disease Prevention and Control Division, Addis Ababa Health Bureau, Addis Ababa, Ethiopia; 2Department of Public Health, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 3Department of Midwifery, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia
Correspondence: Gizachew Abdissa Bulto Email [email protected]
Background: Ethiopia is one of the Sub-Saharan African countries with an increasingly risky sexual practice and mostly affected by the Human Immunodeficiency Virus (HIV) epidemic. Dual protection is an important preventive approach which can prevent both unwanted pregnancy and sexually transmitted infections including HIV/AIDS. Therefore, this study aimed to assess the dual contraceptive utilization and associated factors among reproductive-age women on Anti-Retroviral Therapy (ART) in central Ethiopia.
Methods: An-institution based cross-sectional study was conducted among 311 women on ART at public hospitals of West Shewa Zone from June to September 2019. A systematic random sampling technique was used to select the study participants. A pretested structured interviewer-administered questionnaire was used for data collection. The data were entered into Epi data version 3.1 and exported to IBM SPSS statistical software version 25 for analysis. Bivariate and multivariable logistic regression analysis were computed. Odds ratio along with 95% confidence interval was computed to ascertain the association.
Results: The prevalence of dual contraceptive utilization among women on ART was 21.4% (95% CI: 16.8– 25.9). Age of respondents between 15 and 24 years [AOR=8.35, (95% CI: 3.12– 17.78)], living in urban [AOR=2.59, 95% CI: 1.15– 4.22], separated women [AOR=2.28, 95% CI (1.26– 5.04)], had post-diagnosis counselling on family planning [AOR=5.33, 95% CI: 1.52– 18.68], disclosed HIV status [AOR=5.98, 95% CI: 1.63– 21.93], freely discuss with their husband [AOR=4.22, 95% CI, 1.84– 12.36], have no fertility desire [AOR=2.46, (95% CI: 1.34– 6.44)] were significantly associated with dual contraceptive utilization.
Conclusion and Recommendation: The overall magnitude of dual contraceptive utilization among women on ART was found to be low. Factors like age, residence, marital status, post-diagnosis counselling, disclosure of HIV status, and free discussion with husband were significantly associated with dual contraceptive method utilization. Therefore, it is necessary to expand the range of strategies and tools available to married and single women’s for protecting themselves from being infected with other strains and pregnancy. The concerned stakeholders also should emphatically consider those identified factors for intervention.
Keywords: dual contraceptives, utilization, HIV, central Ethiopia
Background
Dual contraceptive utilization is the utilization of barrier contraceptive (ie Condoms), associated with another modern contraceptive method (oral Contraceptive pills, Jadelle, Depo Provera, Intra-uterine device) which can reduce transmission of STIs, and unintended pregnancy.1,2 By the end of 2030, the study predicted the number of mothers living with HIV worldwide to be 1.5 million.3 The 2015 United Nations Program on HIV and AIDS (UNAIDS) data, covering 160 countries showed that the annual AIDS-related mortality was reduced by 43%.4 UNAIDs report on HIV in 2017 indicated that 36 million people were infected with HIV worldwide, most new HIV infections were from Sub-Saharan Africa (SSA) with 43% women and 2 million children.5
Studies showed that more than 2 million women live with HIV become pregnant every year due to poor dual contraceptive method utilization and unsafe sexual practices.6 The occurrence of unintended pregnancies was due to either using ineffective contraceptive methods or lack access to family planning services.7 The growing epidemics of HIV/AIDS and a spectrum of other Sexually Transmitted Infections (STIs) was significantly higher in HIV positive women (20.7%) as compared to HIV free mothers (13.5%).8 Evidences indicated that more than half of unintended pregnancy occurred among adolescent mothers were end with unsafe abortion.9,10
Most of the incidence of HIV infection in children (90% of cases) were attributable to Mother to Child Transmission.11 Some studies recommended that, unless appropriate care has taken in sexual activity and desire to have children, the chance of transmitting the infection to their partner are higher, considering the high population momentum. Therefore, one of the pillars of the world health organization (WHO) global effort to prevent Mother to Child Transmission of HIV (MTCT) was the prevention of unwanted pregnancy in HIV infected women.12 HIV/AIDS continues to have disastrous medical, economic, social, and physical impacts on individuals, their communities and the nations of the world.13
In HIV care and treatment programs, medication adherence counselling provides a unique window of opportunity to address preventive health recommendations, including family planning and STI prevention.14 To avoid unintended pregnancy and vertical transmission of HIV from mothers to child dual contraceptive utilization was taken as the better strategy.15
Sub-Saharan Africa was at the epicenter of the epidemic and continues to carry the full brunt of its health and socioeconomic impact due to resistance to condom use that was found to be strongly related to STIs (including HIV/AIDS).16 Condom use in such relationships may be seen as a clear sign of infidelity. These attitudes represent a major obstacle to the use of condoms as a dual method of protection.17 Ethiopia was one of the SSA countries that mostly affected by the HIV epidemic.5 Though many people are living with HIV AIDS in the country, ART enables them a return to normal life including a resumption of sexual activity and desire for children.13 Evidence from the UNAIDs report revealed that Ethiopia was one of the sub-Saharan countries with an increasingly risky sexual practice.5 Different studies done in Ethiopia indicated that the utilization of dual method contraception was found to be low.15,18,19 This is quite unexpected in a country where contraceptive services are virtually for free. The Ethiopian Demographic and Health Survey of 2016 revealed that 8% of pregnancy in Ethiopia was not wanted, and also 17% of pregnancy was mistimed. Moreover, the finding from this survey indicated that HIV prevalence among women of reproductive age group was 1.2%, which is seven times higher in urban than in rural areas.20 Most of the studies conducted previously were focused on contraceptive method utilization; however, studies conducted on dual contraceptive utilization were limited. Therefore, this study aimed to assess how people are protecting themselves from the dual risks of unintended pregnancy and sexually transmitted diseases in marital or cohabitating and other types of relationships; because in this country the dual risk of unintended pregnancy and HIV was very high and results in extensive morbidity and mortality.
Methods
Study Design, Period and Setting
An institutional-based cross-sectional study design was conducted at ART clinics of public hospitals in the West Shewa Zone, Oromia region, Ethiopia from June to September 2019. West Shewa Zone is one of the zones of Oromia Region in Ethiopia. Ambo town which is the capital of the zone is located 114 kilometers to the West of Addis Ababa, the capital of the country. According to 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), the total population of the West Shewa Zone was 2,058,676, of whom 1,028,501 are men and 1,030,175 women with the growth rate of 2.9. The zone covers an area of 14,788.78 square kilometers. The Health System of the zone consists of one Teaching Referral hospital, 3 General hospitals, 4 primary hospitals, 89 health centers and 447 health posts with 93% of potential health service coverage. There are 8 public Hospitals namely Ambo University Referral Hospital, Ambo general Hospital, Gedo Hospital, Jaldu Hospital, Inchini Hospital, Gindeberet Hospital, Guder Hospital and Bako Hospital, and also 18 other health centers which are currently providing ART services for the clients in West Shewa Zone. The total numbers of people enrolled to ART in West Shewa Zone were 9319.21
All sampled women of reproductive age (15 to 49 years) living with HIV and had follow-ups at ART clinics in public hospitals of the West Shewa Zone during the study period were our study population. All reproductive age women who were living with HIV and who were pregnant or known to be infecund or who were critically sick and unable to respond to an interview were excluded.
Sample Size Determination and Sampling Technique
The sample size was determined using single population proportion formula, considering the proportion of women with dual contraceptive utilization of 32% (P=0.32)22 that was taken from the study conducted at Fitche Hospital, with 95% confidence interval, 5% (α = 0.05) level of significance, Z α/2 = 1.96 and 5% marginal error. Accordingly, the total sample size was 334. Since the source populations (1856) were less than 10,000, correction formula was used to determine the final sample size that yields 311 by considering 10% for non-response rate.
All hospitals found in the West Shewa zone were included in the study. The study subjects were allocated based on proportional population size on ART through multiplying the number of women on ART with the sample of 311 and dividing with the total available women of reproductive age on ART (1856) at those public hospitals in the West Shewa zone. Then after taking lists of individual women of reproductive age’s Pre-ART registration number from each hospital as a sampling frame. A systematic random sampling technique was applied to select the study subjects. Furthermore, the study subjects were selected every 5th interval dividing the total number women of reproductive age who have a follow-up at ART clinics of public hospitals in West Shewa Zone.
Data Collection Tools and Procedure
The structured pretested questionnaire was used to collect the required data through a face-to-face interview. The questionnaire was prepared first in English and translated into Afan Oromo (the local language), then back to English to check for consistency. The Afan Oromo version of the questionnaire was used to collect the data. Five Bachelor degree nurses who can speak the local language and have experience in data collection were recruited as data collectors. The data collection process was supervised by two MSc in Maternity and Reproductive Health.
Data Analysis
The data were coded, cleaned and entered into the Epi DATA 3.1 software and exported to SPSS version 25 for the final analysis. In this study dual contraceptive utilization was considered if the women used any of hormonal, Non-hormonal or permanent contraceptive method along with male or female condom for six months.22 The data were presented using tables, percentages, graphs and mean values for descriptive analysis. Bivariate and multivariable logistic regressions were done to identify associations between the dependent and independent variables. All explanatory variables with p-value less than 0.25 in bivariate analyses were entered into the multivariable logistic regression analysis and finally, the significance was declared based on the adjusted odds ratio with 95% confidence interval and a p-value less than 0.05.
Data Quality Assurance
Data collectors were trained for two days before the data collection period. The training was given on the objectives of the study, how to retrieve clients, keeping the confidentiality of the clients and how to complete the questionnaire. The questionnaire was developed from other studies and adopted to make it suitable to the local context. A pretest was conducted in Tullu Bollo Hospital located outside the study area on 5% of women of the reproductive age group who were on ART follow up. The questionnaire was checked for its clarity, understandability and simplicity. After pre-tested, the questionnaire was reformatted based on the inputs and comments generated. The quality of the collected data was checked daily by supervisors.
Ethical Approval
The study was conducted according to the Declaration of Helsinki. Ethical approval was obtained from Ambo University, College of Medicine and Health Sciences research review and ethics committee. Finally, informed written consent was obtained from each study participant after fully explaining the objective of the study and the procedures for the study participants as it is attached in the information sheet. For those who are under eighteen years, written consent was taken from either their partner or parents, which is also approved by the ethics committee. The anonymously collected data from the study participants were also kept confidential.
Result
Socio-Demographic Characteristics
Among the 311 sampled respondents, 304 responded to the interview completely, yielding a response rate of 97.7%. The mean age of the respondents was 29.5 with the standard deviation of 9.3 years. One-third of respondents, 105 (34.5%) were in the age group less than or equal to 24 years. The majority of the respondents 236 (77.6%) belong to the Oromo ethnic group and 177 (58.2%) were protestant religion followers. Nearly half of the respondents, 148 (48.7%) were married and 167 (55%) attended formal education. Almost one-third of the respondents, 98 (32.2%) were Farmers. Two-third 201 (66.1%) of them were from urban residence (Table 1).
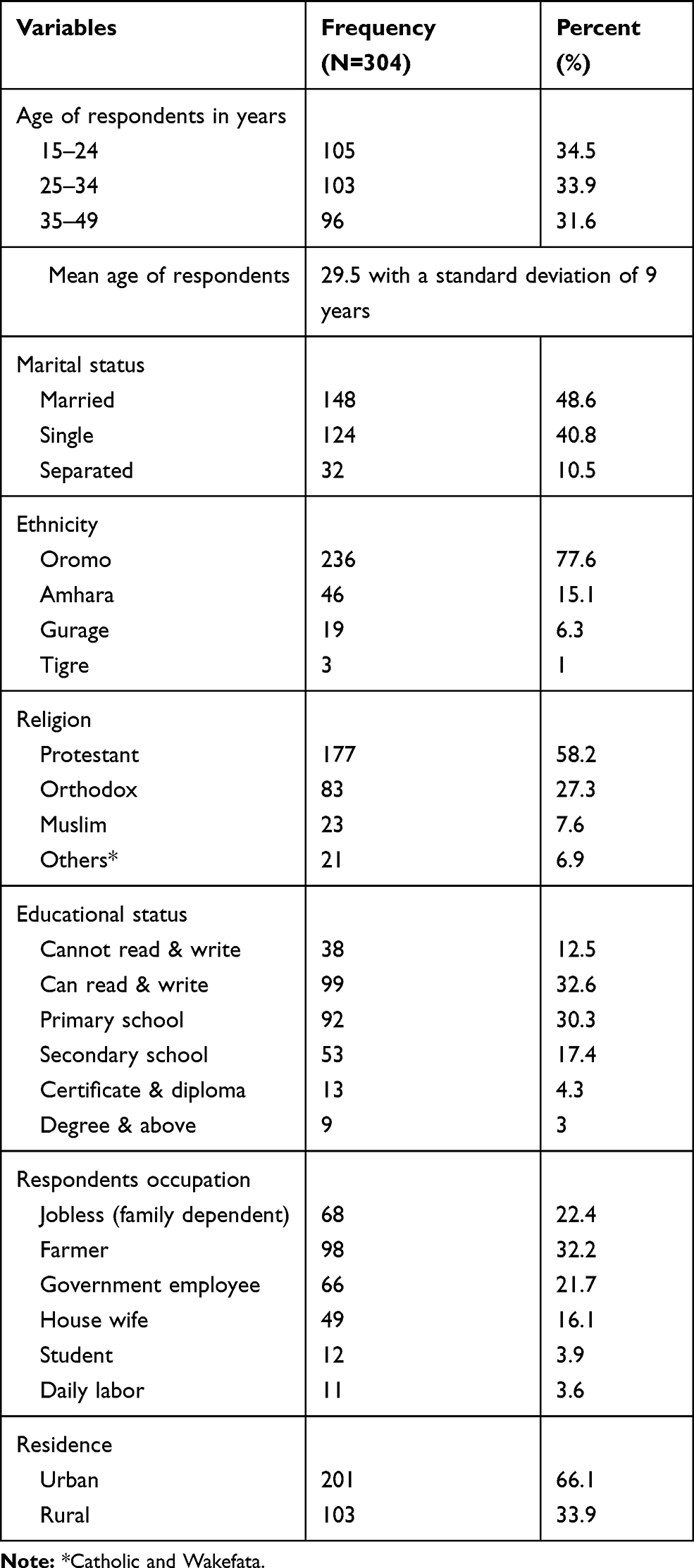 |
Table 1 Sociodemographic Characteristics of Women Living with HIV Attending ART Clinic at Public Hospitals in West Shewa Zone, Ethiopia 2020 |
Awareness on Dual Contraceptive Use, Risk Prevention and Fertility Desire
Majority 188 (61.8%) of respondents have not heard about dual contraceptive methods, and only 116 (38.2%) of them heard from health professionals. Regarding the importance of using a dual contraceptive method, 86 (74.1%) of the respondents think it is useful for the prevention of unwanted pregnancy. Only a few respondents 44 (14.5%) got approval from their religious fathers to use modern contraceptives. Three fifth 176 (57.9%) of them decides jointly on use of family planning methods with their partners.
Most of the respondents, 223 (73.4%) had never used condom in the past six months prior to the study period. The main reported reasons for not using a condom were; slipping of condom in 68 (30.5%), and partner’s refusal 58 (26%). Nearly three-fifth 178 (58.6%) of women living with HIV did not get post-diagnosis counselling on family planning. Half of the women living with HIV, 155 (51%) had ever experienced sexual violence (Table 2).
 |
Table 2 Awareness on Dual Contraceptive Use and Risk Prevention Practice Among Women Living with HIV Attending ART at Public Hospitals in West Shewa Zone, Central Ethiopia 2020 |
Majority, 211 (69.4%) of the women had reported a history of pregnancy at least once in their lifetime. From those who had a history of pregnancy in 149 (70.6%) of them their recent pregnancy was wanted of which in 55 (26%) of respondents their pregnancy was terminated or induced. Half of the respondents, 154 (50.7%) do not want to have more children in the future.
Dual Contraceptive Utilization Among Women Living with HIV
Only one fifth 65 (21.4%) of women were consistently using dual contraception methods (95% CI: 16.8–25.9%) (Figure 1). The most common form of the dual method reported was condom combined with injectable 40 (61.5%). Almost all 227 (97.8%) of the respondents chose the method they are using. Regarding the reason for using a dual contraceptive method, 44 (67.7%) of them responded to prevent STI. Majority of respondents 206 (67.8%) were sexually active in the last six months (Table 3).
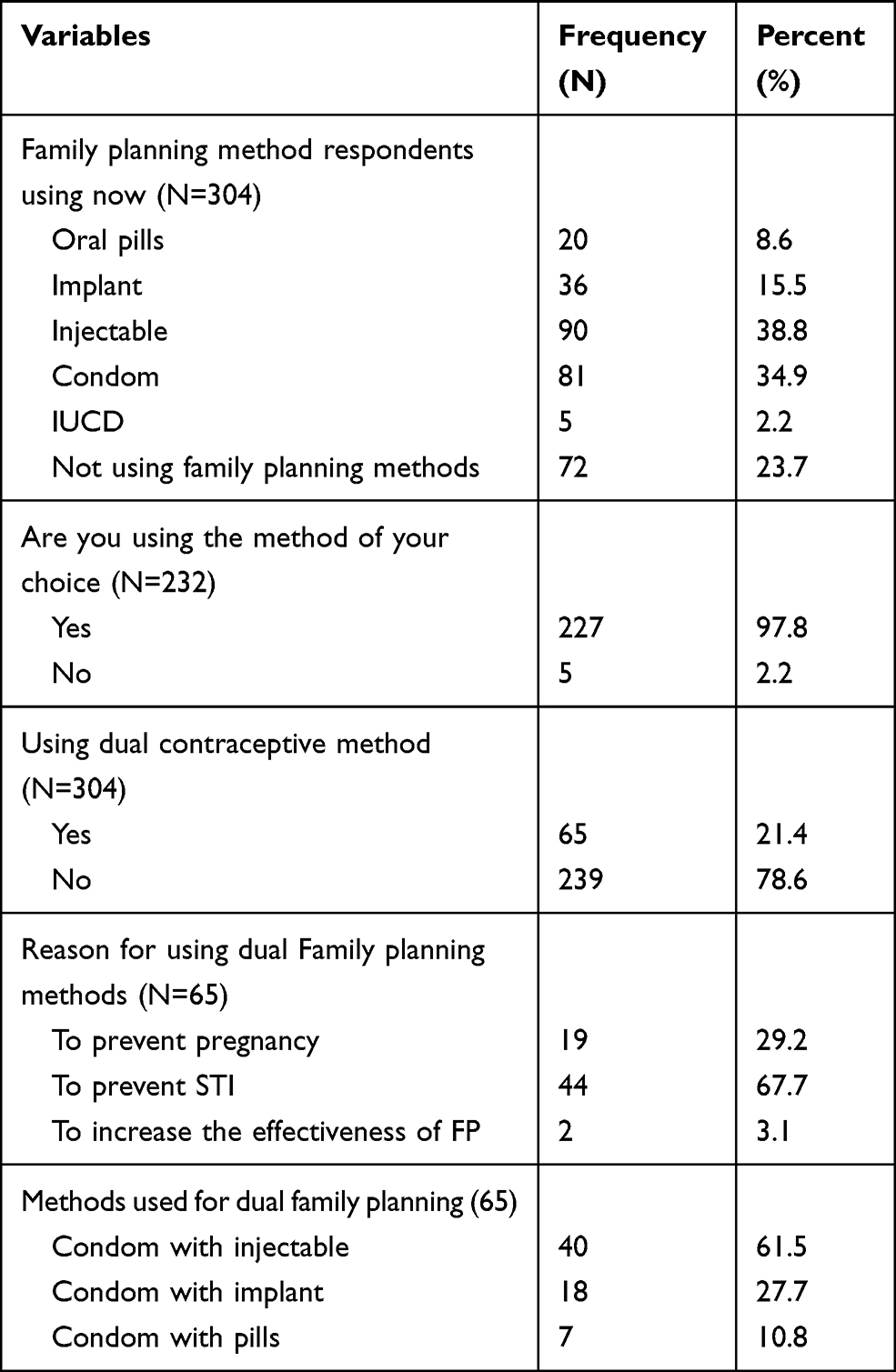 |
Table 3 Dual Contraceptive Method Utilization Among Women Living with HIV Attending ART Clinic at Public Hospitals in West Shewa Zone, Central Ethiopia 2020 |
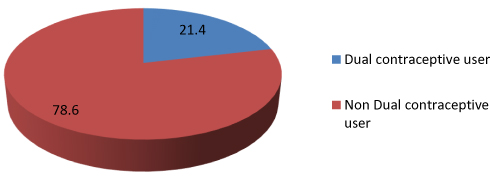 |
Figure 1 Proportion of dual contraceptive utilization among WLHIVs among women living with HIV in West Shewa Hospitals, 2020. |
HIV Status Disclosure and Decision-Making Status
From the total respondents, only 134 (44.1%) of them had disclosed their HIV status for others. Most of the respondents 94 (70.1%) disclosed their HIV status to their partner or family, while 29 (21.6%) disclosed to their sexual partner and 11 (8.2%) disclosed their status for the public voluntarily. Regarding the reason for not disclosing HIV status, most of the participants, 118 (69.4%) were due to lack of trust, 52 (30.6%) were due to fear of stigma and discrimination. Regarding the decision making on women sexual and reproductive health, 128 (42.1%) of respondents reported that they decided by themselves, 126 (41.4%) of them made a joint decision or together, and 50 (16.4%) revealed that all decisions has been solely done by their husbands.
Factors Associated with Dual Contraceptive Utilization Among WLHIV
Factors associated with dual contraceptive utilization among WLHIV on bivariate analysis at P-value of less than 0.25 were included in the final regression model. Multivariable logistic regression analysis was carried out for controlling the possible effect of confounders, and finally, the variables which have significant association were identified based on AOR, with 95% CI and P-value less than 0.05.
A multivariable logistic regression analysis indicates that respondents of age between 15 and 24 years were 8.35 times (AOR=8.35, 95% CI: 3.12–17.78) more likely to utilize dual contraceptive methods as compared to age greater than 35 years old. Separated women used dual contraceptive 2.28 times more likely than married women living with HIV (AOR=2.28, 95% CI: 1.26–5.04). WLHIV who can freely discuss with their husbands were 4.22 times (AOR=4.22, 95% CI: 1.84–12.36) more likely to utilize dual contraceptive methods as compared to those who did not have an open discussion with their husbands. Women living in urban area were 2.59 times more likely to utilize dual contraceptive methods than their rural counterparts’ rural area (AOR=2.59, 95% CI: 1.15–4.22). Women who had been counselled about family planning services were five times more likely to use a dual contraceptive method more than those who did not receive counselling (AOR=5.33, 95% CI 1.52–18.68). WLHIV who had no fertility desire were 2.46 times (AOR=2.46, 95% CI: 1.34–6.44) more likely to utilize dual contraceptive methods as compared to those who had a fertility desire (Table 4).
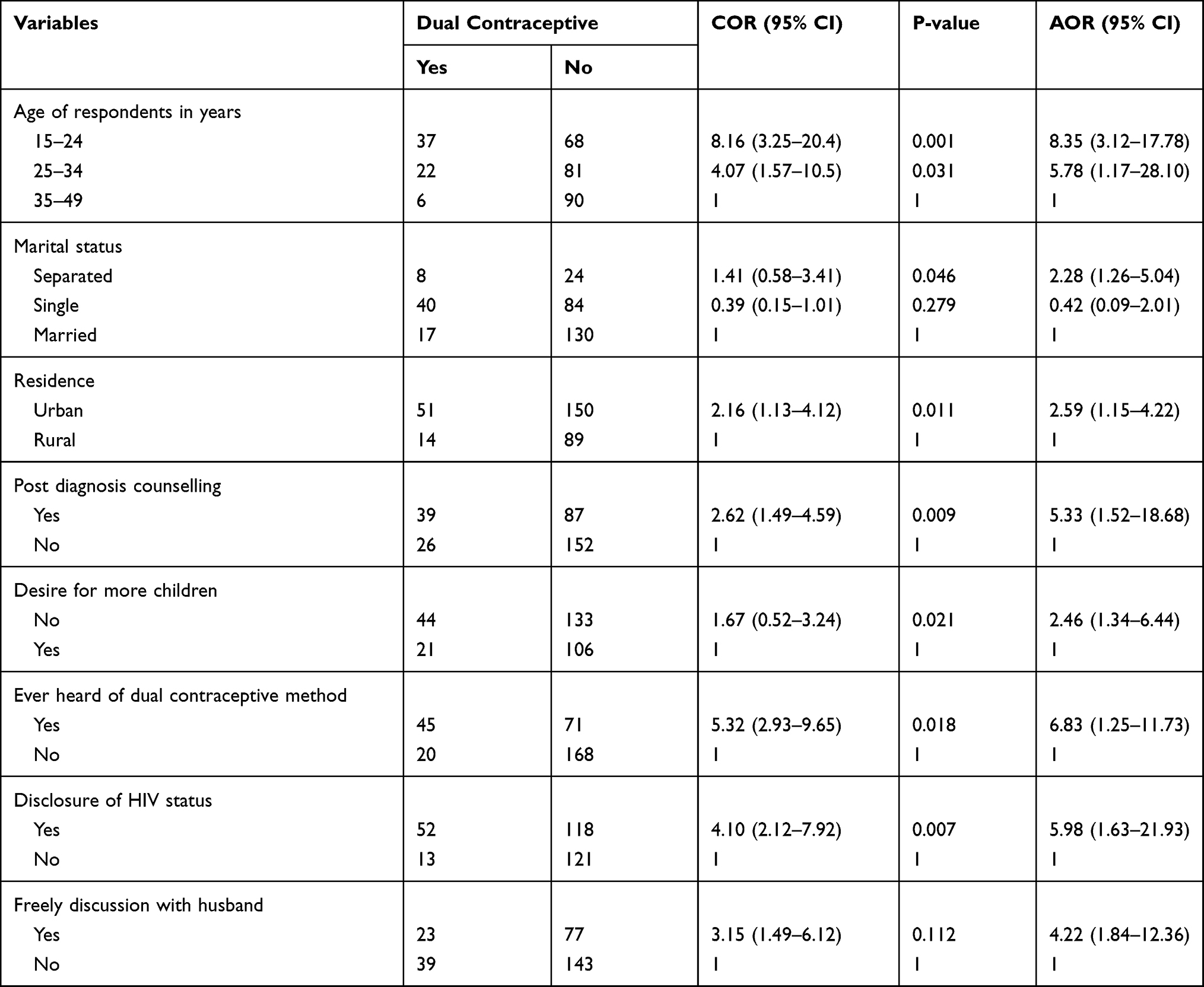 |
Table 4 Factors Associated with Dual Contraceptive Utilization Among Women Living with HIV Attending ART Clinic at Public Hospitals in West Shewa Zone, Central Ethiopia 2020 |
Discussion
The current study revealed that the prevalence of dual contraceptive utilization was found to be 21.4% (95% CI: 16.8–25.9). This finding was almost similar to the study conducted in Southern Ethiopia (19.8%) and Lusaka Zambia (17.7%). This finding was less than the study conducted in South Africa (33%), Tigray (45%)19 and Fitche, Ethiopia (32%).22–25 The possible explanation for this difference might be partly due to variation in socio-demographic characteristics and sample size. The current finding was higher than a study conducted in Tigray (15.7%)18 and Addis Ababa (14.7%).26 This could be because of the study done in Tigray region includes men, and men may have under-reported hormonal contraceptive use among their wives because the men might not directly control dual contraceptive method.
The current study revealed that respondents of age between 15 and 25 years were more likely to utilize the dual contraceptive method than respondents of age greater than 35 years old. This finding was supported by the study conducted in South West Ethiopia.25 However, this finding was different from a study done in Zambia in which women of age greater than or equal to 35 years old were more likely utilized dual contraceptive greater than those 15–24 years old respondents.24 The difference may be linked to the difference in Socioeconomic background and health policy of both countries. In Ethiopia, the younger community has exposure to better information and services regarding dual protection than the older community.
This study showed that HIV positive women who were living in urban were more likely to use dual contraceptive methods as compared to those living in rural areas. This study was in line with a study conducted in Southern Ethiopia.25 The possible explanation for this might be because of the variation in accessing information and services related to this area. The urban women were more easily accessed the important information and services related to dual contraceptive utilization through different sources like; social media and also from their daily social interpersonal relationships.
Finding from this study indicated that those respondents who were separated from their partners were more likely utilized dual contraceptive methods as compared to married women. This evidence was supported by the study conducted in Addis Ababa, Ethiopia.26 This might be due to the fact that husbands may resist the use of condoms in marital and steady relationships because sex needs to be natural and based on trust. The other possible reason might be because; separated women may have multiple sexual partners and do not want to be pregnant, and for this matter they can utilize dual protection.
In this study HIV positive women who had no fertility desire were more likely to utilize dual contraceptive as compared to those who have fertility desire. This finding was similar to a study conducted in Fitche Hospital, Oromia region on people living with HIV.22 Due to the fact that, there are many complications related to pregnancy and STIs. This can, directly and indirectly, affect the respondent’s immunity. Therefore, they are expected to utilize dual contraceptive methods than others.
This study indicated that respondents who received post-diagnosis counselling on family planning were more likely utilized dual contraceptive methods. This finding is in line with a study from India27 that reported receiving post-diagnosis counselling as a significant factor. This could have happened because it is important to understand the more, they got information about the benefit of utilization of the dual contraceptive method, the more they can utilize it.
The current study also showed that women living with HIV who had disclosed their HIV status were more likely to use dual contraceptive methods than those who failed to disclose. This finding was supported with the study done in Addis Ababa, Ethiopia.26 This could be after disclosing their secret and they can use dual protection freely. This could lessen the fear of social stigma and discrimination. This will help them to have a free discussion regarding sexual matters.28 But those who failed to disclose their status might be scared of exposing the secret they are hiding. Another finding of the present study was that women who heard of dual contraceptive showed better use of dual contraceptive method than their counterparts. The result was in line with the studies conducted in Tigray and Addis Ababa, Ethiopia.26 This might be because those women are expected to have more information and awareness on dual contraceptive utilization.
Despite the great contribution of this study, this study may not be generalizable to all women living with HIV who have their follow-ups at health centers and HIV positive but have no follow-up. Furthermore, this study may not be free from social desirability bias.
Conclusion
The proportion of dual contraceptive methods utilization among women living with HIV was found to be Low. Respondent’s age, residence, marital status, post-diagnosis counselling, disclosure of HIV status, and freely discussing with husband were found to be significantly associated with dual contraceptive method utilization.
Therefore, the stakeholders have to give greater attention for the integration of dual contraceptive methods, or family planning with ART units and emphatically consider those identified factors for intervention. It is necessary to expand the range of strategies and tools available to married and single women’s for protecting themselves from being infected with other strains and pregnancy.
Abbreviations
AIDS, Acquired Immunodeficiency Syndrome; ART, Anti-Retroviral Therapy; HIV, Human Immunodeficiency Virus; STI, Sexually Transmitted Infections; SNNP, Southern Nation Nationalities and Peoples; UNAIDS, United Nations Program on HIV and AIDS; WLHIV, Women Living with Human Immunodeficiency Virus.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Acknowledgment
We would like to thank Ambo University, College of Medicine and Health Sciences, Department of Public Health for providing us with the opportunity to conduct the study. We would like to thank West Shewa zonal Health Office, study participants, data collectors and supervisors for their cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the current study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Wilson TE, Koenig LJ, Walter E, Fernandez I, Ethier K. Dual contraceptive method use for pregnancy and disease prevention among HIV-infected and HIV-uninfected women: the importance of an event-level focus for promoting safer sexual behaviors. Sex Transm Dis. 2003;30(11):809–812. doi:10.1097/01.OLQ.0000086617.41012.14
2. World Health Organization. WHO recommendations on adolescent sexual and reproductive health and rights; 2018.
3. UNICEF. Children, HIV and AIDS: the world today and in 2030. Available from: https://data.unicef.org/resources/children-hiv-and-aids-2030/.
4. UNAIDS. UNAIDS reports on the global AIDS epidemic 2013. Geneva: UNAIDS; 2013:201. Available from: https://www.who.int/hiv/pub/me/unaids_global_report/en/.
5. UNAIDS. Joint United Nations Programme on HIV/AIDS (UNAIDS). Geneva, Switzerland; 2017. Available from: https://www.unaids.org/en/resources/documents/2017/2017_data_book.
6. Collins L, Doupe A. Preventing HIV and Unintended Pregnancies: Strategic Framework 2011–2015. UNFPA publication; 2012.
7. Osuafor GN, Maputle SM. Dual protection and contraceptive method use among women in heterosexual relationships in Mahikeng, South Africa. Afr J Reprod Health. 2017;21(1):64–72. doi:10.29063/ajrh2017/v21i1.5
8. Muyindike W, Fatch R, Steinfield R, et al. Contraceptive use and associated factors among women enrolling into HIV care in southwestern Uganda. Infect Dis Obstet Gynecol. 2012;2012:1–9. doi:10.1155/2012/340782
9. Darroch J, Woog V, Bankole A, Ashford L. Adding It Up: Costs and Benefits of Meeting the Contraceptive Needs of Adolescents. New York: New York Guttmacher Institute; 2016.
10. Chandra-Mouli V, Ferguson BJ, Plesons M, et al. The political, research, programmatic, and social responses to adolescent sexual and reproductive health and rights in the 25 years since the International Conference on Population and Development. J Adolesc Health. 2019;65(6):S16–S40. doi:10.1016/j.jadohealth.2019.09.011
11. Melaku YA, Zeleke EG. Contraceptive utilization and associated factors among HIV positive women on chronic follow up care in Tigray Region, Northern Ethiopia: a cross sectional study. PLoS One. 2014;9(4):e94682. doi:10.1371/journal.pone.0094682
12. King R, Khana K, Nakayiwa S, et al. ‘Pregnancy comes accidentally-like it did with me’: reproductive decisions among women on ART and their partners in rural Uganda. BMC Public Health. 2011;11(1):530. doi:10.1186/1471-2458-11-530
13. Federal Democratic Republic of Ethiopia. Country progress response report on the HIV/AIDS response. Addis Ababa: HIV/AIDS, Prevention and Control Office (HAPCO); 2014.
14. Nattabi B, Li J, Thompson SC, Orach CG, Earnest J. Family planning among people living with HIV in post-conflict Northern Uganda: a mixed methods study. Confl Health. 2011;5(1):18. doi:10.1186/1752-1505-5-18
15. Abay F, Yeshita HY, Mekonnen FA, Sisay M. Dual contraception method utilization and associated factors among sexually active women on antiretroviral therapy in Gondar City, northwest, Ethiopia: a cross sectional study. BMC Women’s Health. 2020;20(1):26. doi:10.1186/s12905-020-0890-3
16. Bowring AL, Schwartz S, Lyons C, et al. Unmet need for family planning and experience of unintended pregnancy among female sex workers in urban Cameroon: results from a national cross-sectional study. Glob Health Sci Pract. 2020;8(1):82–99.
17. Coombe J, Anderson AE, Townsend N, et al. Factors influencing contraceptive use or non-use among Aboriginal and Torres Strait Islander people: a systematic review and narrative synthesis. Reprod Health. 2020;17(1):1–17. doi:10.1186/s12978-020-01004-8
18. Gebrehiwot SW, Azeze GA, Robles CC, Adinew YM. Utilization of dual contraception method among reproductive age women on antiretroviral therapy in selected public hospitals of Northern Ethiopia. Reprod Health. 2017;14(1):125. doi:10.1186/s12978-017-0390-6
19. Kalayu H Dual contraceptive use and associated factors among HIV positive women on art follow up in Mekelle Town Tigray, Ethiopia; 2017.
20. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016: key Indicators Report, CSA and ICF, Addis Ababa, Ethiopia, and Rockville, MD, USA; 2016.
21. West Shoa Zone Health Office. West Shoa Zonal Office: health management information system general report Ethiopia; 2018.
22. Demissie DB, Girma T, Abdissa G. Dual contraceptive utilization and associated factors among people living with HIV attending ART clinic in Fitche Hospital, Ethiopia. J Health Med Nurs. 2015;2015:20.
23. Chibwesha CJ, Li MS, Matoba CK, et al. Modern contraceptive and dual method use among HIV-infected women in Lusaka, Zambia. Infect Dis Obstet Gynecol. 2011;2011:1–8. doi:10.1155/2011/261453
24. Kaida A, Laher F, Strathdee SA, et al. Contraceptive use and method preference among women in Soweto, South Africa: the influence of expanding access to HIV care and treatment services. PLoS One. 2010;5(11):e13868. doi:10.1371/journal.pone.0013868
25. Erashi M, Tesso F, Beyene T. Dual-contraceptive method utilization and associated factors among HIV positive women attending art clinic in Gebretsadik Shawo Hospital, SNNPR, South West Ethiopia. Women’s Health Care. 2015;4:6.
26. Asfaw HM, Gashe FE. Contraceptive use and method preference among HIV positive women in Addis Ababa, Ethiopia: a cross sectional survey. BMC Public Health. 2014;14(1):566. doi:10.1186/1471-2458-14-566
27. Chakrapani V, Kershaw T, Shunmugam M, Newman PA, Cornman DH, Dubrow R. Prevalence of and barriers to dual-contraceptive methods use among married men and women living with HIV in India. Infect Dis Obstet Gynecol. 2011;2011:1–8. doi:10.1155/2011/376432
28. Saeieh SE, Nasrabadi AN, Ebadi A, et al. Contraception use among Iranian women with HIV: a qualitative study. Glob J Health Sci. 2016;8(1):199. doi:10.5539/gjhs.v8n1p199
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.