Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Dual Bronchodilator in the Era of Triple Therapy
Authors Papaioannou AI ![]() , Loukides S
, Loukides S ![]() , Bakakos P
, Bakakos P ![]() , Kosmas EN, Rovina N
, Kosmas EN, Rovina N ![]() , Steiropoulos P
, Steiropoulos P ![]() , Fouka E
, Fouka E ![]() , Hillas G, Patentalakis G, Kouvela M
, Hillas G, Patentalakis G, Kouvela M ![]() , Tzanakis N
, Tzanakis N
Received 30 July 2020
Accepted for publication 23 September 2020
Published 28 October 2020 Volume 2020:15 Pages 2695—2705
DOI https://doi.org/10.2147/COPD.S273987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Richard Russell
Andriana I Papaioannou,1 Stelios Loukides,1 Petros Bakakos,2 Epameinondas N Kosmas,3 Nikoletta Rovina,2 Paschalis Steiropoulos,4 Evangellia Fouka,5 Georgios Hillas,6 Georgios Patentalakis,7 Marousa Kouvela,7 Nikos Tzanakis8
1 2nd Respiratory Medicine Department, University of Athens, “Attikon” University Hospital, Athens, Greece; 2 1st Respiratory Medicine Department, University of Athens, “Sotiria” Chest Hospital, Athens, Greece; 3PNOH Pulmonary Clinic, Metropolitan Hospital, Athens, Greece; 4Department of Respiratory Medicine, Medical School, Democritus University of Thrace, Alexandroupolis, Greece; 5Respiratory Medicine Department, Aristotle University of Thessaloniki, G Papanikolaou Hospital, Thessaloniki, Greece; 6 5th Respiratory Medicine Department, Sotiria Chest Hospital, Athens, Greece; 7 3rd Department of Medicine, Athens Medical School, Athens, Greece; 8Department of Thoracic Medicine, Faculty of Medicine, University of Crete, Crete, Greece
Correspondence: Andriana I Papaioannou 2nd Respiratory Medicine Department
University of Athens, “Attikon” University Hospital, Chaidari, Athens, Greece
Tel +302105831163
Email [email protected]
Abstract: Pharmacological medications used for the treatment of COPD patients have increased significantly. Long-acting bronchodilators have been recognized as the mainstay of the treatment of stable COPD, while ICS are usually added in patients with COPD who experience exacerbations, despite bronchodilator treatment. In the latest years, several studies have been published showing the beneficial effect of adding ICS on dual bronchodilation in patients suffering from more severe disease comparing triple therapy with several therapeutic regiments including dual bronchodilation and providing a message that this triple therapy might be more appropriate for COPD patients. However, not all COPD patients have a desirable response to ICS treatment while long-term ICS use in COPD is associated with several side effects. In this report, we aimed to provide a review of the current knowledge on the importance of dual bronchodilation on COPD patients and to compare its use with triple therapy, by covering a wide spectrum of topics. Finally, we propose an algorithm on performing treatment step up from dual bronchodilation to triple therapy and step down from triple to double bronchodilation considering the current evidence.
Keywords: chronic obstructive pulmonary disease, dual bronchodilation, inhaled corticosteroids, triple therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the commonest diseases worldwide, with an increasing burden related to the ageing of the global population and to continued exposure to risk factors.1 During the last two decades, the number of the available inhaled medications used for the treatment of COPD patients increased significantly with the development of new agents that are more potent, have a longer duration of action and are delivered with improved inhalation devices compared to the older compounds.2 Long-acting bronchodilators have been recognized as the mainstay of COPD treatment, and long-acting β2 agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) are currently the main treatment for stable chronic obstructive pulmonary disease (COPD).1 LAMAs and LABAs achieve bronchodilation through different but complementary mechanisms and previous studies have shown that their combination improves pulmonary function as expressed by forced expiratory volume in 1 second (FEV1), dyspnoea and quality of life, and reduces the rate of acute COPD exacerbations (AECOPD).3–16
During the past two decades, ICS/LABA combinations were broadly used for the treatment of COPD. Their use was based on large studies showing that this therapeutic scheme was more effective compared to placebo and to LABA monotherapy on the reduction of COPD exacerbations and on the improvement of lung function and health-related quality of life.14,17–20 However, ICS/LABA combinations have been shown to be inferior compared to the combination of two bronchodilators (LABA/LAMA) regarding lung function and health status21–26 improvements and exacerbation reduction.26
Although the use of LABA/LAMA/ICS with different inhalation devices, mostly as LABA/ICS plus LAMA and infrequently as LABA/LAMA plus ICS, was an option, nowadays the so-called triple therapy represents the combination of a LABA, a LAMA and an inhaled corticosteroid (ICS) in a single inhalation device. The different clinical trials available for three fixed combinations showed both better efficacy and safety compared to mono-components and dual combinations.27 Interestingly, the implementation of this new treatment strategy remains a real challenge for the physician since it is often difficult to clarify the population who really needs to be treated with triple therapy and to avoid overtreatment.
In this report, we aimed to provide a review of the current knowledge on the importance of dual bronchodilation on COPD patients and to compare its use with triple therapy, by covering a wide spectrum of topics. Thus, we present an overview of the evidence regarding fixed triple therapy as a therapeutic option and we summarize and compare available data, focusing on its efficacy against LABA/LAMA combinations. In cases in which direct comparisons do not exist, we interpreted in light of our combined expertise. Our main goal at the end of this review was to eliminate any overtreatment approaches and to clarify some issues which are mainly related to aspects not directly assessed by all the studies. Finally, in order to optimize pharmacotherapy in stable COPD, we propose an algorithm on performing step-up of therapy from dual bronchodilation to triple therapy and step down from triple to double bronchodilation taking into account the extremely heterogeneous population of COPD patients.
Studies of Fixed Triple Therapy Studies
Currently, three different triple combinations are been studied for the treatment of stable COPD: Glycopyronium/Formoterol fumarate/Beclomethasone dipropionate (GFB), Fluticasone furoate/Vilanterol/Umeclidinium (FVU) and Budesonide/Glycopyrrolate/Formoterol fumarate (BGF).
The main studies of GFB, been the first tiple fixed dose combination (FDC) approved for COPD treatment, have performed its comparison with the main available therapeutic schemes used for COPD: ICS/LABA,28 LABA/LAMA,29 LAMA monotherapy,30 and open triple (ie ICS/LABA FDC plus LAMA).30
Trilogy was a 52-week study which randomized 1367 patients to compare fixed triple combination GFB with an ICS/LABA [beclomethasone/formoterol (BF)].28 The primary outcomes were pre-dose FEV1, 2-h post-dose FEV1 and dyspnea, according to the Transition Dyspnea Index (TDI) at 26 weeks. The study has shown that at week 26, GFB significantly improved pre-dose FEV1 and 2-h post-dose FEV1 compared to BF. However, the study failed to show a statistically significant difference in the improvement of TDI. Similarly, tribute randomized 1532 patients comparing fixed triple with GFB with LABA/LAMA Indacaterol/Glycopyronium in a fixed dose 110/50 once-daily31 having as a primary outcome the annual rate of moderate to severe exacerbations. The study has shown that moderate-to-severe exacerbation rates were significantly lower in the arm of the fixed triple therapy, compared to dual bronchodilation. However, in this study, triple therapy failed to show superiority regarding the rates of moderate exacerbations and severe exacerbations analyzed separately, as well as to time to first moderate or severe exacerbation. A non-significant difference was also observed in terms of FEV1 and health-related quality of life (HRQoL) assessed by the Saint George Respiratory Questionnaire (SGRQ) total score change from baseline at both week 26 and 52, the changes in COPD assessment test (CAT) and the use of rescue medication. Finally, TRINITY was a 52-week study which randomized 2690 patients to compare fixed triple combination GFB with tiotropium (LAMA) monotherapy alone and to open triple (BF plus tiotropium administered with two different devices).30 The primary outcome was again the annualized rate of moderate to severe exacerbations, and fixed triple therapy has been superior to tiotropium but not to open triple therapy.
A number of trials are also available for the second fixed triple therapy regimen containing Fluticasone furoate, Vilanterol and Umeclidinium (FVU). In the “FULFIL” trial 1810 patients were randomized to receive either FVU or budesonide/formoterol and the two co-primary outcomes included changes in trough FEV1 and HRQoL at week 24.32 The study has shown a statistically significant difference in favor of fixed triple therapy for both co-primary outcomes. In a second trial,33 a non-inferiority approach was used and 1055 patients were randomized to receive either fixed triple therapy with FVU or an open triple of the same compounds using two separate devices one containing the ICS/LABA FDC and the second the LAMA. The primary endpoint of this study was the change in trough FEV1 at week 24. The results confirmed the non-inferiority in terms of various aspects including the primary endpoint of trough FEV1. Finally, “IMPACT” trial,34 which is the leading trial for this fixed triple combination randomized 10,355 patients in three treatment arms: one arm received triple therapy with FVU, the second received a LABA/LAMA combination (Vilanterol/Umeclidinium) and the third received ICS/LABA FDC (Fluticasone furoate/Vilanterol). The primary outcome of this study was the annual rate of moderate or severe exacerbations. Eligible patients had symptomatic COPD with CAT score ≥10, post-bronchodilator FEV1 of less than 50%, at least one moderate or severe COPD exacerbation in the previous 12 months or an FEV1 of 50–80% predicted and at least two moderate exacerbations or one severe exacerbation in the previous year. IMPACT trial reached its primary outcome in favor of fixed triple (FVU) therapy since the rate of moderate or severe exacerbations was significantly lower with FVU compared to Fluticasone furoate/Vilanterol or Umeclidinium/Vilanterol. FEV1 and SGRQ total score significantly differed in favor of fixed triple therapy. Interestingly, mortality rates were lower with FVU compared to other regimes.
Regarding the third fixed triple therapy, BGF to date two large studies have been completed (KRONOS and ETHOS).35,36 The KRONOS study35 randomized 1902 patients in a 2:2:1:1 manner to receive Budesonide/Glycopyrrolate/Formoterol fumarate metered-dose inhaler (BGF), Glycopyrrolate/Formoterol fumarate metered-dose inhaler (GF), Budesonide/Formoterol fumarate metered-dose inhaler (BF MDI) or open-label Budesonide/Formoterol fumarate dry-powder inhaler (BF DPI). This study included COPD patients who remained symptomatic despite receiving at least two maintenance inhaled therapies. Interestingly, most of the study subjects were lacking an exacerbation history. The Primary endpoint was FEV1 area under the curve from 0 to 4 h (AUC0–4) at 24 weeks and change from baseline in morning pre-dose trough FEV1 at the same time period. The results showed that at week 24 fixed triple therapy significantly improved the FEV1 AUC0–4 compared BF MDI. No significant difference was observed for trough pre-dose FEV1. Rates of moderate or severe exacerbations were significantly lower during treatment with BGF versus GF. BGF significantly improved TDI focal score versus BF DPI, but not versus GF and BF MDI. Significant improvements in SGRQ total score were observed in favor of BGF vs GF. There was no significant difference between groups in the average puffs per day of daily rescue medication.
The ETHOS study36 was a randomized controlled study including 8509 patients to receive twice-daily inhaled doses of triple therapy (320 μg or 160 μg of Budesonide, 18 μg Glycopyrrolate, and 9.6 μg Formoterol) or one of two dual therapies (18 μg Glycopyrrolate plus 9.6 μg Formoterol or 320 μg Budesonide plus 9.6 μg Formoterol). Inclusion criteria included symptomatic COPD patients despite receiving at least two maintenance inhaled therapies, with postbronchodilator FEV1 of 25% to 65%pred, smoking history of at least 10 pack-years, and at least one moderate or severe COPD exacerbation (in patients with FEV1 <50%pred) or at least two moderate or at least one severe COPD exacerbation (in patients with FEV1 ≥50%pred) in the preceding year. Interestingly, in this study, most of the study participants were lacking an exacerbation history. The primary endpoint was the annual rate of moderate or severe COPD exacerbations. The study has shown that exacerbation rate was significantly lower in patients receiving 320-μg–Budesonide triple therapy than with Glycopyrrolate/Formoterol (24% lower: rate ratio (RR), 0.76; 95% confidence interval [CI], 0.69 to 0.83; p<0.001) or Budesonide/Formoterol (13% lower: RR, 0.87; 95% CI, 0.79 to 0.95; p = 0.003). Similarly, the rate was significantly lower with 160-μg–Budesonide triple therapy than with Glycopyrrolate/Formoterol (25% lower: RR, 0.75; 95% CI, 0.69 to 0.83; p<0.001) or Budesonide/Formoterol (14% lower: RR, 0.86; 95% CI, 0.79 to 0.95; p = 0.002).
The aforementioned encouraging results regarding the efficacy of triple therapy in patients with COPD pose a great risk for the treating physician of selecting this therapy for all COPD patients, in a “one size fits all” manner. However, having in mind that overtreatment might increase the risk of adverse events without providing a clear benefit to the patient it is important to specify the exact reasons and patient characteristics that would make triple therapy a reasonable choice.
Exacerbations
Bronchodilators act by altering the airway smooth muscle tone and thus improving FEV1 but equally or even more importantly reducing dynamic hyperinflation at rest and during exercise.37–39 However, although lung function and everyday symptoms are important features of COPD, the most important aspects of the disease are exacerbations, which are characterized by symptom worsening and lung function decline and are often caused by a viral/bacterial infection.40 Studies on COPD therapy focus on the reduction or avoidance of exacerbations which lead to worsening of quality of life, deterioration of lung function and increased risk of death.40
Although in the previous years, ICS/LABA FDC was believed to be the main regimen for exacerbation reduction,17–19 nowadays there is increasing evidence that dual bronchodilation can significantly reduce COPD exacerbations compared to LABA/ICS FDC.25,26 Similarly, ICS discontinuation was not associated with an increase in exacerbation risk when patients continued to be treated with dual bronchodilation.41 A recent meta-analysis including trials of patients with moderate to very severe COPD has shown that dual bronchodilation has a greater efficacy for COPD exacerbations reduction compared to either LAMA monotherapy or LABA/ICS FDC. According to the aforementioned evidence we can come to the conclusion that dual bronchodilation is an effective therapeutic option for exacerbation reduction at least for some COPD patients. This effect of the LABA/LAMA combinations in reducing exacerbation risk is believed to be related to their ability to reduce hyperinflation and symptom severity, and to ameliorate mucociliary clearance.42
Regarding severe exacerbations (defined such as exacerbations requiring hospital admission) no significant benefit was observed between triple therapy and dual bronchodilation in both ETHOS36 and TRIBUTE31 [RR 0.84 95% CI (0.69–1.03) p=0.009, and 0.787 (0.551–1.125), p=0.189, respectively,]. However, a significant difference was observed in the IMPACT34 study in which triple therapy was more effective to reduce severe exacerbations compared to LABA/LAMA [RR 0.66 (0.56–0.78), p<0.001]. However, the IMPACT has been criticized for not excluding patients with a previous diagnosis of asthma, and thus this result must be interpreted with caution. Similarly, a recent real-life study comparing triple therapy with dual bronchodilation has not shown any significant difference in the prevention of severe COPD exacerbations [HR 1.04 (95% CI 0.79–1.37)] between the two treatments.43 Considering that severe exacerbations have an independent negative impact on patient prognosis and are even more related to mortality,44,45 this lack of statistically significant difference in the large RCTs and real life comparing triple combinations with dual bronchodilation also suggests that triple therapy should be preserved for those patients who will definitely benefit from their use.
Lung Function, Symptoms, and Health-Related Quality of Life
Dual bronchodilation can result in greater improvements in lung function (including both trough and peak FEV1) in COPD patients compared to LABA/ICS.24,26,46,47 However, the beneficial effects on lung function by adding an ICS in regimens with dual bronchodilation remain controversial. Previous studies have shown significantly higher improvements on trough and/or peak FEV1 in COPD patients receiving triple therapy compared to dual bronchodilation.27,31,34,35 However, triple therapy was not superior to dual bronchodilation in terms of FEV1 response (defined as change from baseline in pre-dose FEV1≥ 100 mL),31 while these lung function improvements, although statistically significant, were always below 100 mL which has been accepted as the limit of clinical significance.31,34 These observations probably reduce the importance of lung function improvements with triple therapy compared to dual bronchodilation.
Interestingly, it seems that ICS discontinuation in COPD patients previously receiving triple therapy results in a more rapid lung function decline (measured by FEV1) compared to patients who remained on triple therapy especially those with a higher number of blood eosinophils.41,48,49 Nevertheless, these differences on FEV1 were also below the limit of clinical significance and thus these observations regarding differences in lung function and lung function decline might not be an appropriate reason for choosing the addition of an ICS in a patient currently on dual therapy who otherwise seem to be stable, controlled and non-exacerbating.
Whether triple therapy is more effective in reducing COPD-related symptoms and especially dyspnea, this remains debatable since different studies have provided controversial results. IMPACT and ETHOS have reported that patients on triple therapy had a greater improvement in dyspnea compared to dual bronchodilation.34,36 However, other studies failed to provide significant differences in the level of respiratory symptoms and the use of rescue medication for patients receiving triple therapy compared with dual bronchodilation.31,35
In regard to HRQoL, studies comparing triple therapies with dual bronchodilation report a greater improvement in the Saint George’s Respiratory Questionnaire (SGRQ) compared to dual bronchodilation.27,31,34,35 However, again these changes although statistically significant are below the limit of 4 units known to represent clinically significant alterations of HRQoL measured with this questionnaire.50 Furthermore, when patients were examined as responders (defined as decrease from baseline in SGRQ total score ≥4 units) the results are controversial with one study not providing statistically significant differences between triple therapy and dual bronchodilation31 while others show statistically significant differences in favor of triple therapy.34–36
ICS-Associated Pneumonia
The addition of ICS in the therapeutic schemes of patients with COPD is under question since it can reduce the risk of future exacerbations of the disease at the expense of increasing the risk of pneumonia,17,26,51–53 accompanied by an excess risk for hospitalization due to pneumonia.54 Patients at higher risk of pneumonia are those of ≥55 years of age, current smokers, low BMI, severe dyspnea, severe airflow limitation, a prior medical history of pneumonia and low <2% blood eosinophil count.55–57 However, besides this increased pneumonia risk, the benefit ICS are offering on the reduction of exacerbation rate seems to rival the possible harm.28,30,31,34 Furthermore, it has been reported that the increased incidence of ICS-associated pneumonia is not accompanied by an increased rate of pneumonia-related mortality or overall mortality.58 Newer publications showed increased pneumonia risk also on COPD patients treated with ICS other than Fluticasone propionate (such as Beclomethasone, Fluticasone furoate).28,30,31,34,55 However, Janson C and coauthors59 found that Fluticasone propionate was associated with 43–78% increased risk of pneumonia, while only slightly increased risk or no risk was found for Budesonide. Similarly, a previous Cochrane meta-analysis60 has shown that Fluticasone propionate increased non-fatal serious adverse pneumonia events requiring hospitalization (odds ratio (OR) 1.78, 95% confidence interval (CI) 1.50 to 2.12; 18 more per 1000 treated over 18 months; high quality) while budesonide also increased non-fatal serious adverse pneumonia events compared with placebo, but the effect was less precise and was based on shorter trials (OR 1.62, 95% CI 1.00 to 2.62; six more per 1000 treated over 9 months; moderate quality). The risk of any pneumonia event (ie less serious cases treated in the community) was higher with fluticasone than with budesonide (OR 1.86, 95% CI 1.04 to 3.34), and this was the only significant difference reported between the two drugs. These findings should be interpreted with caution because of possible differences in the assignment of pneumonia diagnosis, and because no trials directly compared the two drugs.
Since dual bronchodilation significantly improves symptoms and is effective on exacerbation reduction, when ICS must be added in a patient’s regiment, it is meaningful to identify whether this patient is more vulnerable to develop pneumonia associated with ICS. Vulnerable COPD patients seem to be those with concomitant bronchiectasis combined with chronic bacterial infection and low (<100 cells/μL) number of blood eosinophils61 and those with BMI<25 kg/m2.62
The Importance of Blood Eosinophils
Eosinophilic airway inflammation is often present in patients with stable COPD.63–65 More than 10 years ago, a randomized study has reported the effectiveness of ICS in COPD exacerbation reduction of COPD based on the number of eosinophils.66 According to this study, when ICS use was guided by the number of sputum eosinophils, it resulted in a significant reduction of severe COPD exacerbations. Studies in COPD patients have shown a significant correlation between blood and sputum eosinophils67–69 while patients with elevated numbers of blood eosinophils are at increased risk of COPD exacerbations70 and approximately 64% of frequent exacerbators have blood eosinophils count ≥150cells/μL.71 Since blood eosinophil count is much more accessible compared to sputum eosinophils, it can be more easily used as an indicator of eosinophilic inflammation. Although it is not clear how eosinophilic inflammation contributes to exacerbations, it is believed to be a result of the development of oedema, airway remodeling and mucus production.72 According to these observations, it seems that blood eosinophils might serve as a useful biomarker to guide the use of ICS as add on therapy for the prevention of exacerbations in patients with stable COPD and a recent guideline has been published by the European Respiratory society, suggesting against ICS withdrawal in COPD patients who have a blood eosinophil count >300 eosinophils·μL−1, with or without a history of frequent exacerbations.73
The use of ICS in COPD patients is known to be related to several adverse events (such as oral and oropharyngeal candidiasis, hoarseness, hyperglycemia in patients with diabetes mellitus, cataracts, osteoporosis and osteoporotic fractures)74 and an increased risk of pneumonia.17,60,75 This fact in combination with the evidence which shows that dual bronchodilation is effective in the reduction of COPD exacerbations, the use of ICS as an add-on therapy to maximal bronchodilation should be limited to patients who are more likely to benefit.
Evidence from several studies in stable COPD shows that the number of blood eosinophils can predict response to ICS.29,35,49,76–81 The addition of ICS to a LABA results in COPD exacerbation reduction which is greater as the number of blood eosinophils increases.76,77 Furthermore, the addition of ICS to LABA monotherapy in reducing clinical important deterioration in COPD patients was positively associated with the blood eosinophil count.82 The cut-off point of the number of blood eosinophils seems to be as low as 100 cells/μL and patients with blood eosinophils above this value, if treated with LABA/ICS combination, have a 25% reduced risk of exacerbations compared to those treated with LABA alone.83 Similarly, in a study that has shown the superiority of dual bronchodilation compared to LABA/ICS in exacerbation reduction,26 this superiority was limited at lower levels of blood eosinophils while in patients with ≥300 cells/μL both treatments provided similar efficacy.29,78
Triple therapy also seems to be more effective for the reduction of AECOPD compared to dual bronchodilation and to LAMA monotherapy in patients with higher levels of blood eosinophils30,31 and this reduction on the risk of exacerbations compared to dual bronchodilation is significant at a value of ≥150 cells/μL, although it can already be observed in patients with 100–150cells/μL.34,35,81,84 Similarly, step down from triple therapy to dual bronchodilation in COPD patients with ≥300 blood eosinophils/μL and a history of more than 2 AECOPD in the previous year seems to be related to an increased risk of AECOPD.85 According to these data, it is obvious that it is not easy to identify a definite cut-off point of blood eosinophils guiding the addition of ICS in the treatment of COPD patients, while it should be always kept in mind that the predictive value of blood eosinophil counts seems to interact with the frequency of exacerbations in the previous year. Furthermore, half-life of blood eosinophils is short and its number varies significantly presenting a diurnal variation (with a peak during the evening)67,69,86–88 while it is affected by several parameters such as exercise, and smoking.89,90 However, the number of blood eosinophils does not seem to be influenced by the use of ICS.91 All aforementioned observations lead to the conclusion that a single measurement of blood eosinophils might not be enough to guide the inclusion of an ICS in the therapeutic scheme of a COPD patient.
Finally, eosinophil levels in COPD patients seem to predict not only the response to ICS but also the risk of pneumonia which is related to their use. This risk seems to be lower in COPD patients with higher eosinophil levels57 and increases when blood eosinophils are <100 cells/μL ICS.61 This observation probably means that in COPD patients with eosinophilic inflammation the use of ICS in their therapeutic scheme as an add-on therapy might be a safe choice.
Since data from most clinical trial populations show that blood eosinophil counts impact the effect of ICS regarding the prevention of COPD exacerbations,92 it seems that blood eosinophil count might serve as a potential and useful biomarker for the prognosis and guidance of treatment with ICS as an add-on therapy, in patients with stable COPD. However, further research is still needed in order to define specific cut-off points and conditions of measurement of blood eosinophil levels, as well as disease characteristics, the combination of which will allow the potential of a more personalized treatment of our patients.
Discussion
The most recent GOLD report recommends the use of ICS as part of initial treatment in patients of Group D who have concurrent asthma or blood eosinophils more than 300/μL.1 On re-evaluation, the addition of ICS to dual bronchodilation is suggested in patients that continue to exacerbate despite this treatment and have more than 100 eosinophils in peripheral blood since patients with fewer blood eosinophils are unlikely to benefit from the addition of an ICS in their regimens. However, this approach does not provide specific guidelines on the escalation from dual bronchodilation to triple therapy and de-escalation from triple therapy to dual bronchodilation. Unfortunately, in real life, even patients with mild or moderate COPD severity are treated with triple therapy, regardless of the risk of COPD exacerbations, and this not only by general practitioners93 but also by specialists.94 For these reasons, a clearer approach is needed in order to provide to the physicians a specific algorithm on how to perform escalation from dual bronchodilation to triple therapy as well as de-escalation from triple to dual bronchodilation when the ICS does not provide any benefit in disease control.
Considering the evidence presented above, double bronchodilation should be the cornerstone of the treatment of COPD patients. Triple therapy seems to provide modest clinical benefit in the general COPD population; however, it could be used in patients who still exacerbate especially if they have a higher number of circulating eosinophils, have poor HRQoL related to symptoms and patients who are still very symptomatic while already on LABA/LAMA combination. On the other hand, ICS should be discontinued and de-escalation from triple therapy to double bronchodilation should be attempted in patients who do not seem to benefit from ICS treatment and this subgroup includes patients who continue to exacerbate on triple therapy, are at increased risk of ICS-associated pneumonia (have low numbers of circulating eosinophils, low BMI, concomitant bronchiectasis and chronic bacterial colonization) and in those experiencing adverse events related with ICS use. Finally, in patients receiving triple therapy who have not exacerbated for a long period of time (ie more than 12 months), ICS withdrawal might be performed with close monitoring, for the early recognition of those who might deteriorate after ICS withdrawal (Figure 1).
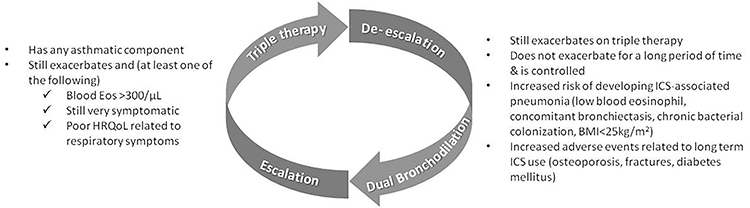 |
Figure 1 Algorithm of escalating to and de-escalating from triple therapy.Notes: Consider escalation/de-escalation if the patient has any of the characteristics shown in this Figure. |
In conclusion, dual bronchodilation is a therapeutic option related to the improvement of symptoms, lung function and health-related quality of life and exacerbation reduction in the great majority of patients with COPD. ICS do not seem to have any beneficial effect in patients with mild to moderate disease who do not exacerbate and thus should not be a therapeutic option for these groups of patients. However, in cases in which symptoms remain uncontrolled and exacerbations continue to occur, the treating physician should adjust therapy by adding an ICS, to help the patient and control the disease. Although there is evidence indicating which patients would benefit more from each therapeutic combination, the final decision should include not only the step up but also the step-down option. It must be made on a patient-to-patient basis weighing any potential impact on lung function, symptoms, and exacerbation risk as well versus the risk of adverse events.
Acknowledgments
Medical writing assistance was supported financially by Boehringer Ingelheim and provided by Hedwig Stals of HD consultancy, under the authors’ conceptual direction and based on feedback from the authors.
Author Contributions
The authors take full responsibility for the scope, direction, content of, and editorial decisions relating to the manuscript. They were involved in all stages of development and have approved the submitted manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
AIP has received Fees and honoraria from Menarini, GSK, Novartis, Elpen, Boehringer Ingelheim, AstraZeneca and Chiesi. SL has received Fees and honoraria from Novartis, AstraZeneca, Sanofi, Menarini, Chiesi, Elpen, Boehringer Ingelheim and GSK. PB has received Fees and Honorara from GSK, AstraZeneca, Novartis, Elpen, Chiesi, Boehringer Ingelheim and Sanofi. EK has received Speaker fees, advisory board honoraria, travel expenses, and fees for clinical trials from AstraZeneca, Angelini, Novartis, GSK, Boehringer Ingelheim, CSL Behring, Chiesi, Elpen, Menarini, Vocate, and Resmed. NR has received honoraria from GSK, AstraZeneca, Chiesi, Elpen, Boehringer Ingelheim, and Novartis. PS has received Fees and Honoraria from Menarini, Boehringer Ingelheim, Elpen, AstraZeneca, Chiesi, GSK and Novartis. EF has received Fees and Honoraria from Chiesi, GSK, Menarini, Novartis, AstraZeneca, Boehringer and Elpen. GH has received Fees and Honoraria from Pharmathen, AstraZeneca, Boehringer Ingelheim, GSK, CSL Behring, Elpen, Chiesi, Innovis, Menarini, Novartis, and UCB. GP is a Boehringer Ingelheim employee. MK has received honoraria from Sanofi, Boehringer Ingelheim and BMS. NT has received Fees and honoraria from Pharmathen, AstraZeneca, GSK, Menarini, Pfizer, Elpen, Chiesi, Boehringer Ingelheim, Novartis, and Inovis. The authors report no other conflicts of interest in this work.
References
1. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2020. Available from: http://www.goldcopd.org.
2. Celli BR. Pharmacological therapy of COPD: reasons for optimism. Chest. 2018;154(6):1404–1415. doi:10.1016/j.chest.2018.07.005
3. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5). doi:10.1183/13993003.00164-2019.
4. Calverley PMA, Anzueto AR, Carter K, et al. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): a double-blind, randomised, parallel-group, active-controlled trial. Lancet Respir Med. 2018;6(5):337–344. doi:10.1016/S2213-2600(18)30102-4
5. Celli B, Crater G, Kilbride S, et al. Once-daily umeclidinium/vilanterol 125/25 mcg in COPD: a randomized, controlled study. Chest. 2014;145(5):981–991. doi:10.1378/chest.13-1579
6. Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respir Med. 2013;107(10):1538–1546. doi:10.1016/j.rmed.2013.06.001
7. Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2(6):472–486. doi:10.1016/S2213-2600(14)70065-7
8. Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. doi:10.1016/j.rmed.2014.10.002
9. Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. doi:10.1183/09031936.00136014
10. Martinez FJ, Rabe KF, Ferguson GT, et al. Efficacy and safety of glycopyrrolate/formoterol metered dose inhaler formulated using co-suspension delivery technology in patients with COPD. Chest. 2017;151(2):340–357. doi:10.1016/j.chest.2016.11.028
11. Hanania NA, Tashkin DP, Kerwin EM, et al. Long-term safety and efficacy of glycopyrrolate/formoterol metered dose inhaler using novel co-suspension delivery technology in patients with chronic obstructive pulmonary disease. Respir Med. 2017;126:105–115. doi:10.1016/j.rmed.2017.03.015
12. Mahler DA, Kerwin E, Ayers T, et al. FLIGHT1 and FLIGHT2: efficacy and safety of QVA149 (indacaterol/glycopyrrolate) versus its monocomponents and placebo in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(9):1068–1079. doi:10.1164/rccm.201505-1048OC
13. Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. doi:10.1183/09031936.00200212
14. Ferguson GT, Taylor AF, Thach C, et al. Long-term maintenance bronchodilation with indacaterol/glycopyrrolate versus indacaterol in moderate-to-severe COPD patients: the FLIGHT 3 study. Chronic Obstr Pulm Dis. 2016;3(4):716–728.
15. Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med. 2013;1(3):199–209. doi:10.1016/S2213-2600(13)70052-3
16. Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;18(14):178. doi:10.1186/1471-2466-14-178
17. Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. doi:10.1056/NEJMoa063070
18. Calverley P, Pauwels R, Vestbo J, et al. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2003;361(9356):449–456. doi:10.1016/S0140-6736(03)12459-2
19. Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(6):912–919. doi:10.1183/09031936.03.00027003
20. Szafranski W, Cukier A, Ramirez A, et al. Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease. Eur Respir J. 2003;21(1):74–81. doi:10.1183/09031936.03.00031402
21. Donohue JF, Worsley S, Zhu CQ, Hardaker L, Church A. Improvements in lung function with umeclidinium/vilanterol versus fluticasone propionate/salmeterol in patients with moderate-to-severe COPD and infrequent exacerbations. Respir Med. 2015;109(7):870–881. doi:10.1016/j.rmed.2015.04.018
22. Rodrigo GJ, Plaza V. Efficacy and safety of a fixed-dose combination of indacaterol and glycopyrronium for the treatment of COPD: a systematic review. Chest. 2014;146(2):309–317. doi:10.1378/chest.13-2807
23. Singh D, Worsley S, Zhu CQ, Hardaker L, Church A. Umeclidinium/vilanterol versus fluticasone propionate/salmeterol in COPD: a randomised trial. BMC Pulm Med. 2015;19(15):91. doi:10.1186/s12890-015-0092-1
24. Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group study. Lancet Respir Med. 2013;1(1):51–60. doi:10.1016/S2213-2600(12)70052-8
25. Zhong N, Wang C, Zhou X, et al. LANTERN: a randomized study of QVA149 versus salmeterol/fluticasone combination in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:1015–1026.
26. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. doi:10.1056/NEJMoa1516385
27. Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: a systematic review and meta-analysis. Eur Respir J. 2018;52(6). doi:10.1183/13993003.01586-2018
28. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388(10048):963–973. doi:10.1016/S0140-6736(16)31354-X
29. Papi A, Kostikas K, Wedzicha JA, et al. Dual bronchodilation response by exacerbation history and eosinophilia in the FLAME study. Am J Respir Crit Care Med. 2018;197(9):1223–1226. doi:10.1164/rccm.201709-1822LE
30. Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389(10082):1919–1929. doi:10.1016/S0140-6736(17)30188-5
31. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
32. Lipson DA, Barnacle H, Birk R, et al. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(4):438–446. doi:10.1164/rccm.201703-0449OC
33. Bremner PR, Birk R, Brealey N, Ismaila AS, Zhu CQ, Lipson DA. Single-inhaler fluticasone furoate/umeclidinium/vilanterol versus fluticasone furoate/vilanterol plus umeclidinium using two inhalers for chronic obstructive pulmonary disease: a randomized non-inferiority study. Respir Res. 2018;19(1):19. doi:10.1186/s12931-018-0724-0
34. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
35. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, Phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758.
36. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;24.
37. O’Donnell DE, Flüge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832–840. doi:10.1183/09031936.04.00116004
38. O’Donnell DE, Sciurba F, Celli B, et al. Effect of fluticasone propionate/salmeterol on lung hyperinflation and exercise endurance in COPD. Chest. 2006;130(3):647–656. doi:10.1378/chest.130.3.647
39. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi:10.1056/NEJMoa0805800
40. Donaldson GC, Wedzicha JA. COPD exacerbations.1: epidemiology. Thorax. 2006;61(2):164–168. doi:10.1136/thx.2005.041806
41. Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. doi:10.1056/NEJMoa1407154
42. Beeh KM, Burgel PR, Franssen FME, et al. How do dual long-acting bronchodilators prevent exacerbations of chronic obstructive pulmonary disease? Am J Respir Crit Care Med. 2017;196(2):139–149. doi:10.1164/rccm.201609-1794CI
43. Suissa S, Dell’Aniello S, Ernst P. Comparative effects of LAMA-LABA-ICS vs LAMA-LABA for COPD: cohort study in real-world clinical practice. Chest. 2020;157(4):846–855. doi:10.1016/j.chest.2019.11.007
44. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
45. Fuso L, Incalzi RA, Pistelli R, et al. Predicting mortality of patients hospitalized for acutely exacerbated chronic obstructive pulmonary disease. Am J Med. 1995;98(3):272–277. doi:10.1016/S0002-9343(99)80374-X
46. Beeh KM, Derom E, Echave-Sustaeta J, et al. The lung function profile of once-daily tiotropium and olodaterol via respimat(®) is superior to that of twice-daily salmeterol and fluticasone propionate via accuhaler(®) (ENERGITO(®) study. Int J Chron Obstruct Pulmon Dis. 2016;11:193–205. doi:10.2147/COPD.S95055
47. Vogelmeier C, Paggiaro PL, Dorca J, et al. Efficacy and safety of aclidinium/formoterol versus salmeterol/fluticasone: a phase 3 COPD study. Eur Respir J. 2016;48(4):1030–1039. doi:10.1183/13993003.00216-2016
48. Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198(3):329–339. doi:10.1164/rccm.201803-0405OC
49. Watz H, Tetzlaff K, Wouters EF, et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled corticosteroids: a post-hoc analysis of the WISDOM trial. Lancet Respir Med. 2016;4(5):390–398. doi:10.1016/S2213-2600(16)00100-4
50. Jones PW. Health status measurement in chronic obstructive pulmonary disease. Thorax. 2001;56(11):880–887. doi:10.1136/thorax.56.11.880
51. Crim C, Calverley PM, Anderson JA, et al. Pneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study results. Eur Respir J. 2009;34(3):641–647. doi:10.1183/09031936.00193908
52. Drummond MB, Dasenbrook EC, Pitz MW, Murphy DJ, Fan E. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(20):2407–2416. doi:10.1001/jama.2008.717
53. Morjaria JB, Rigby A, Morice AH. Inhaled corticosteroid use and the risk of pneumonia and COPD exacerbations in the UPLIFT study. Lung. 2017;195(3):281–288. doi:10.1007/s00408-017-9990-8
54. Ernst P, Gonzalez AV, Brassard P, Suissa S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am J Respir Crit Care Med. 2007;176(2):162–166.
55. Crim C, Calverley PMA, Anderson JA, et al. Pneumonia risk with inhaled fluticasone furoate and vilanterol in COPD patients with moderate airflow limitation: the SUMMIT trial. Respir Med. 2017;131:27–34. doi:10.1016/j.rmed.2017.07.060
56. Crim C, Dransfield MT, Bourbeau J, et al. Pneumonia risk with inhaled fluticasone furoate and vilanterol compared with vilanterol alone in patients with COPD. Ann Am Thorac Soc. 2015;12(1):27–34. doi:10.1513/AnnalsATS.201409-413OC
57. Pavord ID, Lettis S, Anzueto A, Barnes N. Blood eosinophil count and pneumonia risk in patients with chronic obstructive pulmonary disease: a patient-level meta-analysis. Lancet Respir Med. 2016;4(9):731–741. doi:10.1016/S2213-2600(16)30148-5
58. Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219–229. doi:10.1001/archinternmed.2008.550
59. Janson C, Stratelis G, Miller-Larsson A, Harrison TW, Larsson K. Scientific rationale for the possible inhaled corticosteroid intraclass difference in the risk of pneumonia in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:3055–3064. doi:10.2147/COPD.S143656
60. Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;10(3):CD010115.
61. Martinez-Garcia MA, Faner R, Oscullo G, et al. Inhaled steroids, circulating eosinophils, chronic airway infection and pneumonia risk in chronic obstructive pulmonary disease: a network analysis. Am J Respir Crit Care Med. 2020;201(9):1078–1085. doi:10.1164/rccm.201908-1550OC
62. Hartley BF, Barnes NC, Lettis S, Compton CH, Papi A, Jones P. Risk factors for exacerbations and pneumonia in patients with chronic obstructive pulmonary disease: a pooled analysis. Respir Res. 2020;21(1):5. doi:10.1186/s12931-019-1262-0
63. Balbi B, Aufiero A, Pesci A, et al. Lower respiratory tract inflammation in chronic bronchitis. Evaluation by bronchoalveolar lavage and changes associated with treatment with immucytal, a biological response modifier. Chest. 1994;106(3):819–826. doi:10.1378/chest.106.3.819
64. Keatings VM, Barnes PJ. Granulocyte activation markers in induced sputum: comparison between chronic obstructive pulmonary disease, asthma, and normal subjects. Am J Respir Crit Care Med. 1997;155(2):449–453. doi:10.1164/ajrccm.155.2.9032177
65. Papi A, Romagnoli M, Baraldo S, et al. Partial reversibility of airflow limitation and increased exhaled NO and sputum eosinophilia in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;162(5):1773–1777. doi:10.1164/ajrccm.162.5.9910112
66. Siva R, Green RH, Brightling CE, et al. Eosinophilic airway inflammation and exacerbations of COPD: a randomised controlled trial. Eur Respir J. 2007;29(5):906–913. doi:10.1183/09031936.00146306
67. Negewo NA, McDonald VM, Baines KJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:1495–1504. doi:10.2147/COPD.S100338
68. Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(12):956–967. doi:10.1016/S2213-2600(17)30432-0
69. Singh D, Kolsum U, Brightling CE, Locantore N, Agusti A, Tal-Singer R. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697–1700. doi:10.1183/09031936.00162414
70. Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The copenhagen general population study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
71. Vogelmeier CF, Kostikas K, Fang J, et al. Evaluation of exacerbations and blood eosinophils in UK and US COPD populations. Respir Res. 2019;20(1):178. doi:10.1186/s12931-019-1130-y
72. Eltboli O, Brightling CE. Eosinophils as diagnostic tools in chronic lung disease. Expert Rev Respir Med. 2013;7(1):33–42.
73. Chalmers JD, Laska IF, Franssen FME, et al. Withdrawal of inhaled corticosteroids in COPD: a European respiratory society guideline. Eur Respir J. 2020;55(6):2000351. doi:10.1183/13993003.00351-2020
74. Matera MG, Cardaci V, Cazzola M, Rogliani P. Safety of inhaled corticosteroids for treating chronic obstructive pulmonary disease. Expert Opin Drug Saf. 2015;14(4):533–541. doi:10.1517/14740338.2015.1001363
75. Suissa S, Patenaude V, Lapi F, Ernst P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68(11):1029–1036. doi:10.1136/thoraxjnl-2012-202872
76. Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
77. Siddiqui SH, Guasconi A, Vestbo J, et al. Blood eosinophils: a biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(4):523–525. doi:10.1164/rccm.201502-0235LE
78. Roche N, Chapman KR, Vogelmeier CF, et al. Blood eosinophils and response to maintenance chronic obstructive pulmonary disease treatment. Am J Respir Crit Care Med. 2017;195(9):1189–1197. doi:10.1164/rccm.201701-0193OC
79. Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC
80. Hinds DR, DiSantostefano RL, Le HV, Pascoe S. Identification of responders to inhaled corticosteroids in a chronic obstructive pulmonary disease population using cluster analysis. BMJ Open. 2016;6(6):e010099. doi:10.1136/bmjopen-2015-010099
81. Ferguson GT, Papi A, Anzueto A, et al. Budesonide/formoterol MDI with co-suspension delivery technology in COPD: the TELOS study. Eur Respir J. 2018;52(3):1801334. doi:10.1183/13993003.01334-2018
82. Bafadhel M, Singh D, Jenkins C, et al. Reduced risk of clinically important deteriorations by ICS in COPD is eosinophil dependent: a pooled post-hoc analysis. Respir Res. 2020;21(1):17. doi:10.1186/s12931-020-1280-y
83. Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117–126. doi:10.1016/S2213-2600(18)30006-7
84. Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756.
85. Calverley PMA, Tetzlaff K, Vogelmeier C, et al. Eosinophilia, frequent exacerbations, and steroid response in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(9):1219–1221. doi:10.1164/rccm.201612-2525LE
86. Winkel P, Statland BE, Saunders AM, Osborn H, Kupperman H. Within-day physiologic variation of leukocyte types in healthy subjects as assayed by two automated leukocyte differential analyzers. Am J Clin Pathol. 1981;75(5):693–700. doi:10.1093/ajcp/75.5.693
87. Schumann DM, Tamm M, Kostikas K, Stolz D. Stability of the blood eosinophilic phenotype in stable and exacerbated COPD. Chest. 2019;29.
88. Oshagbemi OA, Burden AM, Braeken DCW, et al. Stability of blood eosinophils in patients with chronic obstructive pulmonary disease and in control subjects, and the impact of sex, age, smoking, and baseline counts. Am J Respir Crit Care Med. 2017;195(10):1402–1404. doi:10.1164/rccm.201701-0009LE
89. Mensinga TT, Schouten JP, Weiss ST, Van der Lende R. Relationship of skin test reactivity and eosinophilia to level of pulmonary function in a community-based population study. Am Rev Respir Dis. 1992;146(3):638–643. doi:10.1164/ajrccm/146.3.638
90. Landis SH, Suruki R, Hilton E, Compton C, Galwey NW. Stability of blood eosinophil count in patients with COPD in the UK clinical practice research datalink. COPD. 2017;14(4):382–388. doi:10.1080/15412555.2017.1313827
91. Kreindler JL, Watkins ML, Lettis S, Tal-Singer R, Locantore N. Effect of inhaled corticosteroids on blood eosinophil count in steroid-naive patients with COPD. BMJ Open Respir Res. 2016;3(1):e000151. doi:10.1136/bmjresp-2016-000151
92. Calverley PMA. A light in the darkness? The FLAME trial, blood eosinophils, and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(9):1125–1127. doi:10.1164/rccm.201703-0560ED
93. Bloom CI, Elkin SL, Quint JK. Changes in COPD inhaler prescriptions in the United Kingdom, 2000 to 2016. Int J Chron Obstruct Pulmon Dis. 2019;14:279–287. doi:10.2147/COPD.S190086
94. Corrado A, Rossi A. How far is real life from COPD therapy guidelines? An Italian observational study. Respir Med. 2012;106(7):989–997. doi:10.1016/j.rmed.2012.03.008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.