Back to Journals » Risk Management and Healthcare Policy » Volume 13
Drug-Related Problems and Pharmacist Intervention at a General Hospital in the Jazan Region, Saudi Arabia
Authors Babelghaith SD, Wajid S ![]() , Alrabiah Z
, Alrabiah Z ![]() , Othiq MAM, Alghadeer S, Alhossan A
, Othiq MAM, Alghadeer S, Alhossan A ![]() , Al-Arifi M
, Al-Arifi M ![]() , Attafi IM
, Attafi IM
Received 30 January 2020
Accepted for publication 3 April 2020
Published 6 May 2020 Volume 2020:13 Pages 373—378
DOI https://doi.org/10.2147/RMHP.S247686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Salmeen D Babelghaith, 1 Syed Wajid, 1 Ziyad Alrabiah, 1 Mohammed Abdu M Othiq, 2 Sultan Alghadeer, 1 Abdulaziz Alhossan, 1 Mohamed Al-Arifi, 1 Ibraheem M Attafi 3
1Department of Clinical Pharmacy, College of Pharmacy King Saud University, Riyadh, Saudi Arabia; 2Ministry of Health, Sabya General Hospital, General Directorate of Health Affairs, Jazan, Saudi Arabia; 3Poison Control and Medical Forensic Chemistry Center, General Directorate of Health Affairs, Jazan, Saudi Arabia
Correspondence: Syed Wajid
Department of Clinical Pharmacy, College of Pharmacy King Saud University, Riyadh, Saudi Arabia
Email [email protected]
Objective: This study examined the incidence of drug-related problems (DRPs) in different inpatient departments along with the medical team response to pharmacist’s action in addressing DRPs at Jazan Hospital, Saudi Arabia.
Patients and Methods: This retrospective study was conducted among inpatients at Ministry of Health hospital in Jazan, a region in southwestern Saudi Arabia. We collected data for a 2-year period (from 2016 to 2017). For any detected DRP of the ordered medications for dispensing, the inpatient pharmacist is sending report for that particular DRP with recommendation to the medical team which in turn might accept or reject such recommendation. Serious drug–drug interactions, as part of DRP, were assessed by utilizing three different online DDI checkers, including Lexi-Comp, Medscape, and Drugs.com.
Results: The most common type of DRP was serious drug–drug interactions (49%). Over the study period, most incidences of DRPs were decreased. Of the DRPs in 2016 and 2017, antibiotics were the most commonly involved (51% and 69.5%) of cases, respectively, followed by proton pump inhibitors (25.3% and 14.1%) and statins (12.9% and 9.4%). Interestingly, of the 241 interventions for DRPs in 2016, 199 (82.5%) were accepted, resulting in a change in drug therapy (p=0.006). In 2017, 90 (70.3%) interventions out of 128 were accepted by the physician and the drug therapy changed (p=0.029).
Conclusion: Pharmacist interventions appear to decrease the incidence of DRPs, which emphasize the importance of an optimal pharmaceutical care plan for clinical care settings.
Keywords: pharmacist intervention, drug-related problems, inpatient units, Saudi general hospital, Jazan, Saudi Arabia
Introduction
Drug-related problems (DRPs) are the primary clinical concern of pharmaceutical care practitioners. Detecting and resolving them is essential to pharmaceutical practice, as it helps to ensure that patients attain their therapeutic goals and achieve the optimal outcomes of drug therapy.1,2 The American Society of Health-System Pharmacists acknowledges eight types of DRP3 adverse drug reactions, drug errors, drug without indication, failure to receive medication, indicators without drugs, drug interactions, drug noncompliance, and drug poisoning1,3 DRPs are often the result of certain patients’ drug-related issue not being identified and addressed. If they are not identified or addressed, DRPs can lead to clinical complications. They may also increase the number of visits to ambulatory care units or length of hospital stay, and lead to a higher risk of death.3–5 Resolving DRPs requires sound clinical judgement.1
The global prevalence of DRPs among all admissions in ambulatory care settings is about 5.3%, and the incidence of DRPs during hospitalization has ranged from 15.1% to 16.9%.2 Certain health care standards prevent the occurrence of DRP. Several studies investigated the prevalence rates of various types of DRP among different institutions when these institutions failed adherence to such certain healthcare standards. DRPs can originate at any stages of medication processes (ordering/prescribing, transcribing and verifying, dispensing and delivering, administering, and monitoring and reporting).6–8 Many countries have taken measures to improve pharmaceutical care quality and safety in order to prevent DRPs.9 These efforts have principally taken the form of pharmacist interventions, wherein a pharmacist takes action to address non-optimal drug use in order to improve patients’ quality of life and prevent further morbidity or mortality.7,8 Such pharmacist interventions not only positively influence patient care but also reduce unnecessary medical expenditure.10
Few studies have been conducted in the Middle East on DRPs and pharmacists’ role in them. Al Rahbi and his colleagues10 conducted a retrospective study in Oman to evaluate the effect of dispensing pharmacists’ interventions on the number and types of medication errors at an outpatient pharmacy. They found that 688 interventions related to prescribing errors, of which 40.5% were accepted by the medical team. Moreover, 14.9% of the interventions pertained to administrative issues and 8.7% pertained to inappropriate drug therapy. About 8.2% of the interventions focused on drug overdose. Interestingly, pharmacists intervened in 20.8% of cases to prevent complications, 25.1% to explain the treatment, and 7.9% to improve compliance. In Saudi Arabia, a prospective study in 2008 was carried out in Riyadh to assess the role of clinical pharmacists in an intensive care unit (ICU), specifically to what extent they were accepted by physicians, their frequency in the ICU, their clinical significance, and how they influenced targeted patient outcomes. They found that most DRPs that occurred in the ICU involved not giving a drug for a given medical condition (33.2% as shown in Table 1), wrong dosing regimen (28.9%), and no indication for drug use (14.3%).11 In 2013, another study was conducted in central Saudi Arabia to explore the occurrence of adverse drug events (ADEs). The scholars found that pharmacists reported 361 possible events of ADEs, of which around 78% were considered as potential ADEs that, if it reached a patient, it can cause harmful effect.6 More recently, a prospective study was carried out in the Al Ahsa region of Saudi Arabia by Albadr et al to examine the prevalence of DRPs and drug–drug interactions (DDIs) among inpatients of an internal medicine ward. They found a high incidence of DDIs, and noted that polypharmacy, age, and comorbid conditions were the most important factors related to incidence of DDIs.12
 |
Table 1 DRPs According to Drug Class |
However, none of these past studies examined the impact of pharmacist interventions on DRPs in the southern region of Saudi Arabia. Moreover, there remain rather few studies on this topic throughout the country. Therefore, we investigated the incidence of drug-related problems (DRPs) in different inpatient departments along with the medical team response to pharmacist’s action in addressing DRPs at Jazan Hospital, Saudi Arabia.
Patients and Methods
In this retrospective cohort study, we focused on inpatients admitted to a 217-bedded general hospital between 2016 and 2017. This hospital was affiliated with the Ministry of Health and was located in southwestern Saudi Arabia, in the Jazan region.
The hospital inpatient wards were spread across ten departments: medical, surgical and orthopedic, pediatric, obstetric gynecology, delivery, operation room, anesthesiology, recovery room, adult intensive care, and neonatal intensive care. In most of these departments, drug therapy is carried out primarily by physicians and nurses, and there is no clinical or resident pharmacist. Medication orders are written by physicians either using the computer system or manually, after which they are sent to the inpatient pharmacy for dispensing. Any case that important patient information, such as diagnosis, weight, height, allergy status, laboratory data, and daily meals is missing and not included in the patient medication profile (PMP) was excluded from the study.
The hospital employs two pharmacists and one pharmacy technician to assess and dispense ordered medications. Before dispensing, the pharmacist checks the order for DRP that could negatively affect the patient’s health. If any DRP is discovered, the pharmacist begins the intervention by writing a detailed report containing the available patient information, department of admission, the type and details of the DRP, and the plan for its management. Two copies of these written reports are made, one of which remains in the Inpatient Pharmacy Intervention Reports File (IPIRF), while the other is sent to the patient’s original file to be reviewed by the physician who might accept or reject pharmacist’s plan for management of particular DRP. For the aforementioned reasons, the pharmacists focused their intervention efforts on the most common DRPs in hospital inpatient settings: serious DDIs, prolonged antimicrobial use, unnecessary medication orders, inappropriate drug dosage, and unavailable drugs for departments that should have ready access to them. Different intervention strategies were used for each type of DRP. For serious DDIs, pharmacists used three different online DDI checkers, including Lexi-Comp, Medscape, and Drugs.com. When a DDI was classified as serious by ≥2 of these checkers, a DRP report was written by the pharmacy. For prolonged antimicrobial usage, the pharmacists and the pharmacist technician followed the Automatic Stop Order policy created by the Saudi Central Board for Accreditation of Health Institute (CBAHI) for long-term medication use. In the case of prescribing two or more medications known to have therapeutically and/or pharmacologically close effects such as prescribing ceftriaxone with ceftazidime for the same patient, an intervention for unnecessary medication orders was conducted. If the prescribed drug dose was considered inappropriate based on current literature and other resources, the pharmacist issued formal notification of the incorrect dosage. Finally, in the case of prescribing unavailable medication, the pharmacist wrote a report about the unavailability of the medicine and the best available alternative.
Data Collection
We collected data for a 2-year periods (from 2016 to 2017) on the implementation of Inpatient Pharmacy Intervention Reports File (IPIRF). We examined the relation of inpatient pharmacy interventions with the following variables: department in which the DRP occurred; and type of DRP (i.e., prolonged antimicrobial use, unnecessary medication order, inappropriate drug dose, and serous DDI). We also examined physicians’ response to the intervention by examining their written response or actions related to the medication order following the pharmacist recommendation. If they gave no written response and made no other action, they were considered to have issued “no response.”
Statistical Analysis
Descriptive statistics (numbers and percentages) were obtained for variables using SPSS Statistics 25. Chi-square and Fisher exact test was sued to find any association between the variables; a p-value of <0.05 was considered statistically significant.
Results
A total of 369 pharmacist interventions were conducted between 2016 and 2017. The most common type of DRP was serious DDIs (49%), followed by prolonged antimicrobial therapy, and unnecessary medication orders (8.9), as presented in Table 2.
 |
Table 2 Breakdown in the Number of DRPs Across the Two Years (n=369) |
The drug class showing the most DRPs in both 2016 and 2017 were antibiotics (51% and 69.5%, respectively), antiplatelet (25.3% and 14.1%) followed by proton pump inhibitors (25.3% and 14.1%) and statins (12.9% and 9.4%, respectively) See Table 1.
Interestingly, among the 241 interventions in 2016, 199 (82.5%) were accepted by the physicians and the therapy was changed (p=0.006). In 2017, 90 (70.3%) interventions out of 128 (34.7%) were accepted and the therapy was changed (p=0.029) (Table 3). Table 4 shows the extent of physician acceptance according to the hospital ward.
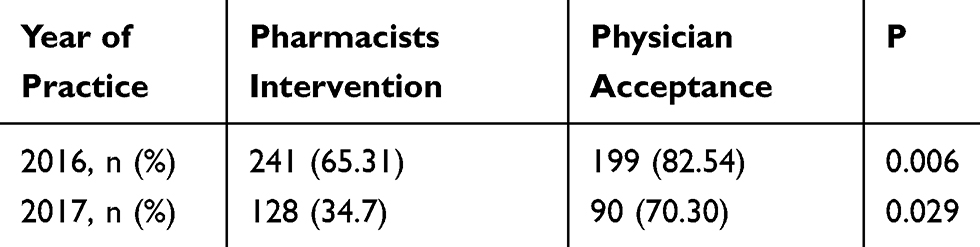 |
Table 3 Acceptance of Interventions by Physicians |
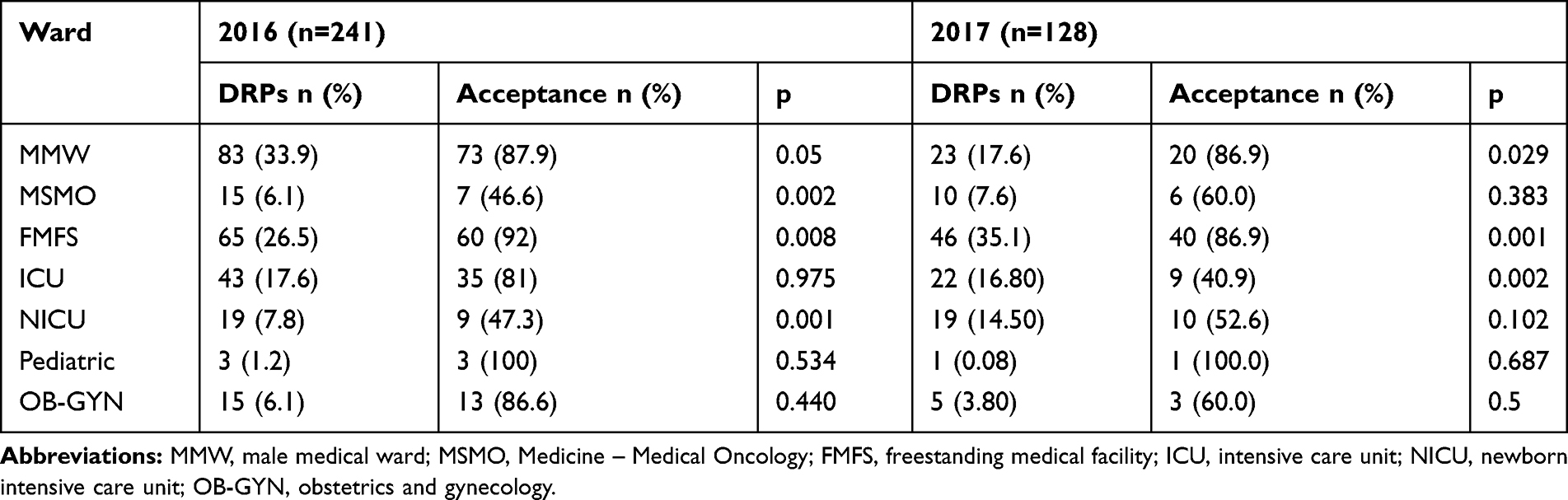 |
Table 4 Acceptance of Interventions According to Hospital Wards |
Discussion
Drugs are therapeutically active substances intended to treat, inhibit, or diagnose infections, diseases, and their symptoms. However, incorrect use of such substances can lead to the disruption of health-related quality of life and increased risk of further morbidity or even mortality.10 Our study showed that pharmacist interventions led to a reduction in DRPs. These results are consistent with both national and international studies showing that pharmacist interventions lead to a decreased incidence of DRPs, suggesting that the pharmacist plays a vital role in improving the health care system.13 A study was carried out in Mecca city, Saudi Arabia, aimed to assess the effectiveness of a pharmacist intervention to decrease the drug error, particularly the use of high-risk abbreviations (HRAs) by specialists.14 The results of this study showed that high prevalence of the use of HRAs in discharge prescriptions and dispensing records (72.7%). However, post-intervention of pharmacists the overall prevalence of HRA was significantly decreased by 52% (p=0.001).14
Surprisingly, the high acceptance rate stated in this study led to a decrease in DRPs, where 289 (78%) of the 369 interventions were accepted by physicians and the patient’s therapy was changed. Similarly, a retrospective study conducted in the outpatient pharmacy department of Khoula Hospital in Muscat, Oman revealed 692 interventions among which 98.2% were accepted by the prescribers.13 Molino et al also had similar findings in a prospective controlled study, reporting that pharmacist interventions were generally accepted by physicians, leading to a change in medication therapy.15 Furthermore, the interventions were well accepted by patients as well, although the compliance with the interventions was not measured.14 These findings suggest that the importance of the pharmacist in healthcare is well recognized by physicians, as is the significance of the pharmaceutical practices in clinical settings. However, the physician acceptance rates for some departments were below 50%. Some barriers to physician acceptance of these pharmacist’s interventions such as specialty, pharmacist gender, and patient gender.16 The most reasons for low physician acceptance of these pharmacist’s interventions included no clinic guidelines requiring doctors’ reaction to pharmacist commendations. The difference between the physicians’ and pharmacists’ knowledge may likewise have added to the low physicians’ acceptance rate of pharmacist commendations. Physicians may consider the advantages of certain drugs outweigh their risks.16
The most common type of DRP in our study was serious DDIs, followed by prolonged antimicrobial therapy, unnecessary medication orders, and inappropriate drug dose. These findings differ somewhat from those found in a previous study in which DRPs commonly involved adverse drug reactions (30.4%) and patient non-compliance (30.4%), followed by untreated indications (10.7%), drug interactions and supratherapeutic/sub-therapeutic doses (7.1% each), improper drug selection (5.4%), and drug use without indication (1.8%).15 Another study was conducted at a private hospital in Riyadh City, Saudi Arabia to investigate the intervention of clinical pharmacist’s services at critical care units. This study reported that the most common DRPs were inappropriate dose (20.05%), followed by drug duplication (11.29%), and unsuitable route (6.87%) and DDIs (1.96%).15 A study conducted in a teaching and research hospital in Istanbul, Turkey, revealed that inappropriate drug selection (44.79%), inappropriate dose selection (27.61%), and inappropriate medication treatment procedures (21.47%) were the most common17,18.
Numerous studies have shown that DDIs are recurrent DRPs10,15,17 which align with our findings. A possible reason that DDIs were the most common DRP in our study is that individual patients may be prescribed a high number of drugs, coupled with a lack of relationship between the prescriber, patient, and pharmacist. Minimizing the total number of medications given to individual patients might help in reducing DDIs.15
Antibiotics were the most common class of drug involved in DRPs, followed by antiplatelet drugs, and proton pump inhibitors. Previous studies in Saudi Arabia identified hypertension, stroke, urinary tract infection (UTI), and community acquired pneumonia, in that order, as the major diagnoses associated with DRPs.16 Studies conducted in other countries showed that DRPs commonly involved patient non-compliance and adverse drug reactions.15,19,20
Scholars have indicated that around 53% of DRPs are preventable.4,15 The current study revealed that the number of DRPs decreased between 2016 and 2017, suggesting that pharmacist involvement leads to significantly more DRPs being identified compared with usual care.21,22 Clinical pharmacists not only can effectively identify, resolve, and prevent clinically significant DRPs and their outcomes on their own, but also can assist multidisciplinary teams in improving treatment adherence and rational drug use, which can further diminish the incidence of DRPs.21–24
Hence, providing education programs on medication safety and appropriateness is needed. Such these programs and workshops to improve patient safety should be delivered frequently to all clinical staff including pharmacists, and should be intended to empower pharmacists specifically to identify and manage DRPs in an interprofessional cooperative health care environment. In addition, an institutional policy that does not just explain the role of pharmacists in the detection and management of DRPs, but also needs prescribers to collaborate with pharmacists in attending to such occurrences should be in place to enable pharmacists to do their expert jobs in guaranteeing patient safety.25
The main limitation of this study was its focus on a single institution, and the fact that it was carried out with two pharmacists and one pharmacy technician. This could have biased the results for DRPs, especially considering that the role of the pharmacist in hospital settings in Saudi Arabia has not yet been fully implemented. This recommends that the number of clinical pharmacy field (residency, master, or even Pharm D), desires to be enlarged to meet the requirements of pharmaceutical care in Saudi Arabia. Future studies are needed to determine interventions that can successfully resolve the DRPs that arise in the hospital setting.
Conclusion
In the present study, serious DDIs and prolonged antimicrobial therapy were the two most common DRPs. DRPs have a serious negative impact on health outcomes, so efforts should be taken to decrease their occurrence. Based on our results, further studies should be conducted to explore DRPs in a larger sample and over a longer period of time. Future studies should also explore pharmacist interventions and the relevant drugs and drug reactions associated with DRPs.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
This cross-sectional study was approved by the Ethics Committee of Jazan Hospital, Saudi Arabia and conducted in accordance with the Declaration of Helsinki.
Consent
Written informed consent was obtained from the participants prior to the study.
Acknowledgment
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through research group no. RG-1440-098.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cipolle RJ, Strand LM, Morley PC. Chapter 5, Drug therapy problems. In: Cipolle RJ, Strand LM, Morley PC, editors. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management Services.
2. Richardson TE, O’Reilly CL, Chen TF. Drug-related problems and the clinical role of pharmacists in inpatient mental health: an insight into practice in Australia. Int J Clin Pharm. 2014;36(5):1077–1086. doi:10.1007/s11096-014-9997-7
3. Alomi YA, Al-Shaibani AS, Alfaisal G, Alasmi NM. Clinical outcomes of drug-related problems in Saudi Arabia: patients’ and healthcare providers’ perspective. J Pharm Pract Commun Med. 2018;4(2):77–82. doi:10.5530/jppcm.2018.2.19
4. Patel P, Zed PJ. Drug related visits to the emergency department: how big is the problem? Pharmacotherapy. 2002;22(7):915–923. doi:10.1592/phco.22.11.915.33630
5. Jatau AI, Aung MM, Kamauzaman TH. Prevalence of drug-related emergency department visits at a teaching hospital in Malaysia. Drugs Real World Outcomes. 2015;2(4):387–395. doi:10.1007/s40801-015-0045-2
6. Aljadhey H, Mahmoud MA, Mayet A, et al. Incidence of adverse drug events in an academic hospital: a prospective cohort study. Int J Qual Health Care. 2013;25(6):648–655. doi:10.1093/intqhc/mzt075
7. Dahal PR, Venkataraman R, Fuloria PC. Assessment of clinical pharmacist intervention in tertiary care teaching hospital of Southern India. Asian J Pharm Clin Res. 2013;6(2):258–261.
8. Viktil KK, Blix HS. The impact of clinical pharmacists on drug-related problems and clinical outcomes. Basic Clin Pharmacol Toxicol. 2008;102(3):275–280. doi:10.1111/j.1742-7843.2007.00206.x
9. Patel I, Balkrishnan R. Medication error management around the globe: an overview. Indian J Pharm Sci. 2010;72(5):539. doi:10.4103/0250-474X.78518
10. Al Rahbi HA, Al-Sabri RM, Chitme HR. Interventions by pharmacists in out-patient pharmaceutical care. Saudi Pharm J. 2014;22(2):101–106. doi:10.1016/j.jsps.2013.04.001
11. Al-Jazairi AS, Al-Agil AA, Asiri YA, Al-Kholi TA, Akhras NS, Horanieh BK. The impact of clinical pharmacist in a cardiac-surgery intensive care unit. Saudi Med J. 2008;29(2):277–281.
12. Albadr Y, Bohassan AK, Ming LC, Khan TM. An exploratory study investigating the potential drug–drug interactions in internal medicine department, Alahsa, Saudi Arabia. J Pharm Health Serv Res. 2014;5(4):237–241. doi:10.1111/jphs.12073
13. Adusumilli PK, Adepu R. Drug related problems: an overview of various classification systems. Asian J Pharm Clin Res. 2014;7:7–10.
14. Haseeb A, Winit-Watjana W, Bakhsh AR, et al. Effectiveness of a pharmacist-led educational intervention to reduce the use of high-risk abbreviations in an acute care setting in Saudi Arabia: a quasi-experimental study. BMJ Open. 2016;6(6):e011401. doi:10.1136/bmjopen-2016-011401
15. Molino CDGRC, Carnevale RC, Rodrigues AT, Visacri MB, Moriel P, Mazzola PG. Impact of pharmacist interventions on drug-related problems and laboratory markers in outpatients with human immunodeficiency virus infection. Ther Clin Risk Manag. 2014;10:631–639. doi:10.2147/TCRM.S61821
16. AL-JUMAILI AA, Jabri AM, Al-Rekabi MD, Abbood SK, Hussein AH. Physician acceptance of pharmacist recommendations about medication prescribing errors in Iraqi hospitals. Inov Pharm. 2016;7(3). doi:10.24926/iip.v7i3.443
17. Al-Arifi M, Abu-Hashem H, Al-Meziny M, Said R, Aljadhey H. Emergency department visits and admissions due to drug related problems at Riyadh military hospital (RMH), Saudi Arabia. Saudi Pharm J. 2014;22(1):17–25. doi:10.1016/j.jsps.2013.01.001
18. Abunahlah N, Elawaisi A, Velibeyoglu FM, Sancar M. Drug related problems identified by clinical pharmacist at the internal medicine ward in Turkey. Int J Clin Pharm. 2018;40(2):360–367. doi:10.1007/s11096-017-0585-5
19. Carcelero E, Tuset M, Martin M, et al. Evaluation of antiretroviral‐related errors and interventions by the clinical pharmacist in hospitalized HIV‐infected patients. HIV Med. 2011;12(8):494–499. doi:10.1111/j.1468-1293.2011.00915.x
20. Mok S, Minson Q. Drug-related problems in hospitalized patients with HIV infection. Am J Health Syst Pharm. 2008;65(1):55–59. doi:10.2146/ajhp070011
21. Al-Olah YH, Al Thiab KM. Admissions through the emergency department due to drug-related problems. Ann Saudi Med. 2008;28(6):426–429. doi:10.5144/0256-4947.2008.426
22. Nelson KM, Talbert RL. Drug‐related hospital admissions. Pharmacotherapy. 1996;16(4):701–707.
23. Geletko SM, Poulakos MN. Pharmaceutical services in an HIV clinic. Am J Health System Pharm. 2002;59(8):709–713. doi:10.1093/ajhp/59.8.709
24. Viktil KK, Blix HS, Moger TA, Reikvam A. Interview of patients by pharmacists contributes significantly to the identification of drug related problems (DRPs). Pharmacoepidemiol Drug Safety. 2006;15(9):667–674. doi:10.1002/pds.1238
25. AlRuthia Y, Alkofide H, Alosaimi FD, et al. Drug-drug interactions and pharmacists’ interventions among psychiatric patients in outpatient clinics of a teaching hospital in Saudi Arabia. Saudi Pharm J. 2019;27(6):798–802. doi:10.1016/j.jsps.2019.05.001
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.