Back to Journals » Clinical Ophthalmology » Volume 14
Double-Flanged polypropylene Suture for Scleral Fixation of Cionni Capsule Tension Ring
Authors Samir A ![]() , Abdelrahman Elsayed AM
, Abdelrahman Elsayed AM ![]() , Alyan A, Lotfy A
, Alyan A, Lotfy A ![]()
Received 4 January 2020
Accepted for publication 19 March 2020
Published 20 April 2020 Volume 2020:14 Pages 1055—1058
DOI https://doi.org/10.2147/OPTH.S244751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Double flanged polyprolene suture for fixation of Cionni CTR" [ID 244751]
Views: 1179
Ahmed Samir, Ayman M Abdelrahman Elsayed, Ahmed Alyan, Ayman Lotfy
Ophthalmology Department, Zagazig University, Zagazig, Egypt
Correspondence: Ahmed Samir
Ophthalmology Department, Zagazig University, Zagazig, Egypt
Email [email protected]
Purpose: To describe a new technique for transconjunctival intrascleral fixation of Cionni CTR using double-flanged polypropylens suture.
Methods: This is a prospective interventional case series which included 7 cases with severe (more than 180 degrees) zonular dialysis. Three cases were hereditary lens subluxation (Marfan syndrome), 2 cases with traumatic subluxation and 2 cases with pseudo-exfoliation syndrome.
Results: All cases achieved a good postoperative stable and centered IOL with good visual results. No postoperative complications were recorded apart from PCO in 3 cases and mild bleeding during needle passage in one case.
Conclusion: This described technique is a simple, time sparing and minimally invasive method for achieving good bag centration. It eliminates the need of conjunctival peritomy, subconjunctival vessels cautery and scleral fashioning of a flap, pocket or a groove. The use of 6/0 polypropylene theoretically can achieve better longevity.
Keywords: Cionni ring, lens subluxation, polypropylene suture, scleral fixation
Introduction
The most common causes of zonular insufficiency are pseudoexfoliation syndrome, trauma, previous ocular surgery (eg, filtering surgery or vitrectomy), hypermature cataracts, and increased axial length. Less common causes include Marfan’s syndrome, homocystinuria, Weill–Marchesani syndrome, microspherophakia, retinitis pigmentosa and intraocular neoplasms.1
The Cionni’s modified capsule rings (MCTRs) has an open ring design with one (model I-L or I-R) or two (model 2-L) fixation eyelets attached to the main ring which allows the ring to be fixated to the sclera. This eyelet protrudes 0.25mm forward from the ring and then lays anterior to the anterior capsular rim.1,2
Modified capsule tension rings are sutured to the sclera to give a long-term stability for the capsular bag with severe (more than 180 degree) zonular dialysis. Posterior chamber IOLs can be implanted in the bag after being stabilized and centered.1,2
After passing the sutures through the eyelets, the sutures are externalized, and tied under a scleral flap, tied under a corneoscleral pocket, or tied over episclera according to surgeon preference, as no technique has been definitively proven superior over the other.4–6
This work describes a novel technique to fix the MCTRs to the sclera using a 6/0 polypropylene sutures with double flanges.
Methods
This is a prospective interventional case series which included 7 cases with severe (more than 180 degrees) zonular dialysis. Cases with previous ocular surgeries, glaucoma, posterior segment pathology or corneal opacity were excluded. This work was done according the Declaration of Helsinki and was approved by Alpha Vision center research ethics committee. A written informed consent was obtained from all patients or the parents after explanation of the type of the procedure and the follow up. All cases were done by the same surgeon (A.S).
Surgical technique: (As shown in the supplementary video).
After I/A flexible, iris retractors placed through limbal stab incisions were used to hook the capsulorhexis edge and support the bag during insertion of the MCTR.
The Cionni ring was inserted manually with a McPherson forceps and Sinsky hook was used to guide the trailing end to be placed in the bag.
The Cionni ring was placed so that the eyelet for scleral fixation was placed at the maximum point of subluxation.
A 6/0 polypropylene suture (Prolene®; Ethicon, Somerville, NJ) was introduced through a paracentesis the passes through the eyelet of the ring. A 27-gauge needle was inserted 2 mm behind the limbus transconjunctivally to the sulcus. A microforceps wasused to thread the prolene suture into the lumen of the needle. The needle was withdrawn outside the eye carrying the prolene suture. A hand held ophthalmic cautery (Accu-Temp Cautery; Beaver Visitec, Waltham, MA) wasused to create a flange at the end of the prolene suture at the paracentesis side. To create an adequate sized flange that prevents the suture from passage through the eyelet, more than 5 mm of the suture should be cauterized. The other end of the prolene suture at the scleral side was pulled till the ringwas centered. The suture outside the eye is pulled to the maximum with McPherson forceps in flush with the sclera and the cautery was used to create another bulb then the suture was released till the bulb was totally covered by the conjunctiva and rest in the outer end of the scleral track created by the 27-gauge needle (Figure 1).
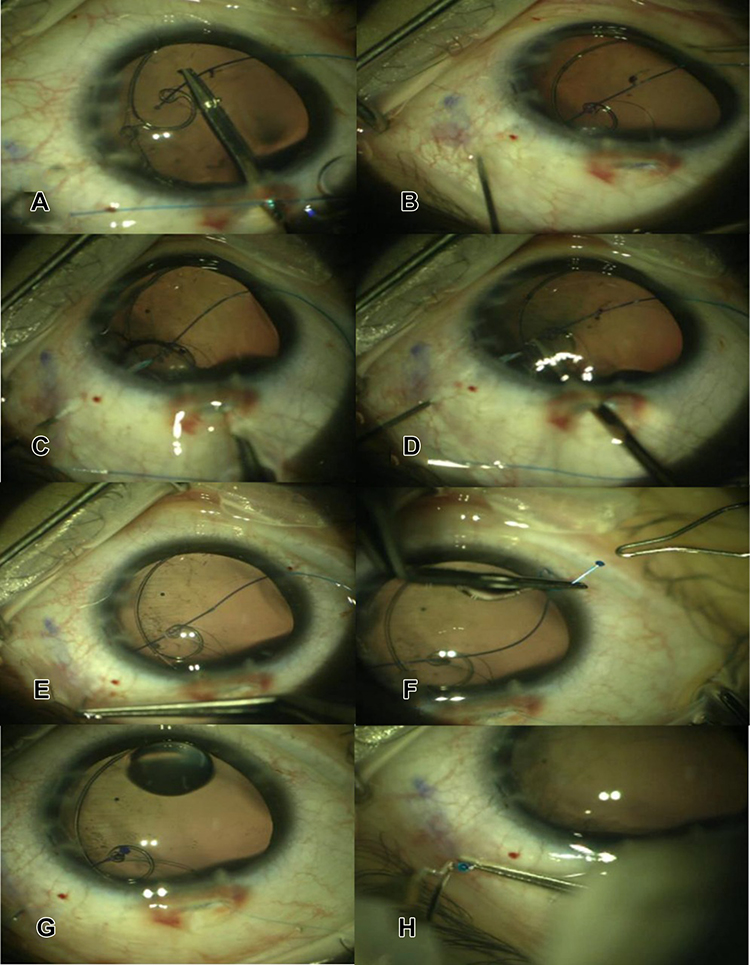 |
Figure 1 (A–H) Shows surgical steps. |
After the bag was well centered by the scleral-fixated MCTR, a single piece IOL was implanted in the bag.
All patients were treated with topical broad spectrum antibiotic drops four times per day and topical prednisolone acetate four times per day. The antibiotic eye drop was stopped after two weeks while the steroid eye drop was tapered over four weeks.
The cases were followed up for at least three months for the best corrected visual acuity, IOP, IOL decentration, and presence of complications as endophthalmitis or intraocular hemorrhage.
Results
The technique was used in 7 cases with severe (more than 180 degrees) zonular dialysis.
Three cases were hereditary lens subluxation (Marfan syndrome), 2 cases with traumatic subluxation and 2 cases with pseudo-exfoliation syndrome.
All cases achieved a good postoperative stable and centered IOL with good visual results. No postoperative complications were recorded apart from PCO in 3 cases and mild bleeding during needle passage in one case (Table 1).
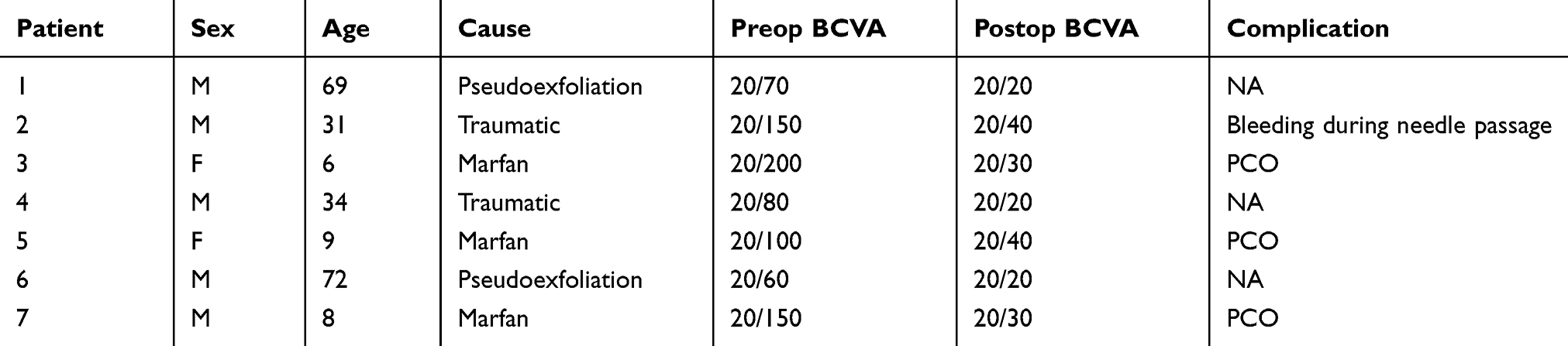 |
Table 1 Preoperative and Postoperative BCVA, Etiology of Lens Subluxation and Postoperative Complications |
Discussion
Capsular tension rings (CTRs) and other endocapsular devices have become well-established tool that allow surgeons to deal with zonular weakness with increased safety. The choice of capsular tension device in a particular surgery depends on the amount of zonular dehiscence as well as the likelihood of progression. CTRs can re-center a mildly subluxated capsular bag, but it will not recenter a severely subluxated capsular bag nor will it cure a progressive zonulopathy. In these situations, a modified CTR (MCTR) or a capsular tension segment (CTS) provides a stable long-term solution through scleral-fixation.2
The standard method of Trans- scleral fixation of Cionni ring for stabilization of capsular bag in cases of zonular dialysis,involves conjunctival peritomy, caurety of subconjunctival vessels, scleral flaps groove or pocket creation which is time consuming and needs along learning curve.5,6
Suture material should be permanent. Polypropylene 10–0 is commonly used but it will hydrolyze over time with a roughly 5- to 10-year survival time. Polypropylene 9–0 should have a longer survival time. The interval before degradation of this suture gauge has not been reported. A polytetrafluoroethylene CV-8 suture has been used for scleral fixation off label and to date has had excellent longevity.3
This described technique is a simple, time sparing and minimally invasive method for achieving good bag centration. It eliminates the need of conjunctival peritomy, subconjunctival vessels cautery and scleral fashioning of a flap, pocket or a groove. The use of 6/0 prolene theoretically can achieve better longevity. However longer period of follow up is required.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Do AT, Holz HA, Cionni RJ. Subluxated cataract lens surgery using sutured segments or rings and implantation of toric intraocular lenses. J Cataract Refract Surg. 2016;42(3):392–398. doi:10.1016/j.jcrs.2015.10.070
2. Thapa BB, Agarwal A, Singh R, Gupta PC, Ram. J. Phacoaspiration with a Cionni ring versus pars plana lensectomy, vitrectomy and sutureless transscleral IOL fixation in pediatric patients with a subluxated lens. Graefes Arch Clin Exp Ophthalmol. 2016;254(5):901–909. doi:10.1007/s00417-016-3297-y
3. Wang Z, Lu Y, Xiao K, et al. Bimanual irrigation-aspiration for ectopia lentis and use of a small incision for 4-point scleral-sutured foldable intraocular lens and anterior vitrectomy in patients with Marfan syndrome. Indian J Ophthalmol. 2019;67(10):1629–1633. doi:10.4103/ijo.IJO_250_19
4. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmol. 2017;124(8):1136–1142. doi:10.1016/j.ophtha.2017.03.036
5. Yavuzer K, Evcimen Y. Sutureless transconjunctival intrascleral intraocular lens fixation: the modified Yamane technique. Arq Bras Oftalmol. 2019;82(5):389–393. doi:10.5935/0004-2749.20190072
6. Dhingra D, Malhotra C, Jakhar V, Rohilla V, Negi A, Jain AK. Combination of capsular tension ring and capsular tension segment for the management of lens coloboma >4 clock hours. Indian J Ophthalmol. 2019;67(10):1684–1687. doi:10.4103/ijo.IJO_1762_18
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.