Back to Journals » International Journal of Women's Health » Volume 17
Dosimetric Evaluation of Tangential Arc and Jaw Tracking Techniques in Volumetric Modulated Arc Therapy for Synchronous Bilateral Breast Cancer
Authors Zhang J ![]() , Chen Z, Hong D
, Chen Z, Hong D
Received 16 July 2025
Accepted for publication 10 October 2025
Published 18 October 2025 Volume 2025:17 Pages 3729—3740
DOI https://doi.org/10.2147/IJWH.S554097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jiyong Zhang,1,* Zewei Chen,1,* Danli Hong2
1Department of Radiation Oncology, Cancer Hospital of Shantou University Medical College, Shantou, Guangdong, 515000, People’s Republic of China; 2Department of Endocrinology, The First Affiliated Hospital of Shantou University Medical College, Shantou, Guangdong, 515000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiyong Zhang, Email [email protected]
Purpose: This study presents a dosimetric comparison of volumetric modulated arc therapy (VMAT) treatment plans that employ static jaw, tangential arc, and jaw tracking techniques for patients with synchronous bilateral breast cancer (SBBC).
Methods: VMAT plans employing static jaw (S-VMAT), tangential arc (T-VMAT), and jaw tracking (J-VMAT) techniques were generated for twelve SBBC patients, receiving a prescribed dose of 50 Gy in 25 fractions. All treatment plans had their dosimetric and delivery parameters meticulously recorded and analyzed for comparison. Dosimetric verification was conducted using gamma analysis with 3%/3 mm criteria, based on ArcCHECK phantom measurements.
Results: PTV coverage was comparable among all three techniques, with no statistically significant differences in dose indices, CI, or HI (p > 0.05). In contrast, T-VMAT and J-VMAT showed significant advantages in OARs protection compared to S-VMAT. T-VMAT achieved the lowest lung and heart doses, with the heart Dmean reduced from 11.25 Gy (S-VMAT) to 7.44 Gy, and the heart V5Gy from 86.98% to 36.03%. J-VMAT also demonstrated substantial improvements, reducing heart Dmean to 9.21 Gy and V5Gy to 76.89%. Both techniques also showed lower doses to the liver, esophagus, trachea, and spinal cord compared to S-VMAT. In terms of efficiency, T-VMAT required significantly fewer MUs and achieved a markedly shorter delivery time, with a reduction of over one-third compared to S-VMAT and nearly half compared to J-VMAT. QA pass rates were above 99% for all plans, with no significant differences observed.
Conclusion: T-VMAT and J-VMAT offer superior OAR sparing and efficient treatment delivery compared to S-VMAT. T-VMAT is particularly advantageous in reducing dose and treatment time, while J-VMAT provides a balanced approach between dosimetric quality and delivery accuracy. Both techniques represent promising strategies for optimizing VMAT planning in SBBC.
Keywords: synchronous bilateral breast cancer, volumetric modulated arc therapy, jaw tracking, static jaw, organs at risk
Introduction
Synchronous bilateral breast cancer (SBBC) is a rare subtype of breast cancer, defined by the diagnosis of primary malignant lesions in both breasts within a six-month interval.1–3 Compared to unilateral breast cancer, SBBC presents greater clinical challenges, requiring not only effective treatment for bilateral tumors but also meticulous planning to optimize target coverage while minimizing radiation exposure to surrounding healthy tissues, such as the heart, lungs, spinal cord, and liver. Traditional radiotherapy techniques often lead to uneven dose distribution or excessive radiation to critical organs, increasing the risk of long-term complications such as radiation pneumonitis and cardiotoxicity, which can significantly impact patients’ quality of life. Therefore, the development of more precise and safer radiotherapy strategies has become a crucial focus in the clinical management of SBBC.
Volumetric modulated arc therapy (VMAT) is an advanced radiotherapy technique that achieves highly conformal dose distributions through the dynamic modulation of a multi-leaf collimator (MLC) in coordination with continuous gantry rotation, offering significant advantages in both treatment efficiency and dosimetric precision. It has been increasingly utilized in breast cancer radiotherapy.4–8 However, in SBBC, the symmetrical and adjacent anatomical positioning of bilateral target volumes presents unique challenges. Conventional VMAT is often constrained by static collimator jaw settings during optimization, limiting the movement range of MLC leaves. This restriction can result in dose inhomogeneities, such as “cold spots” or “hot spots” within the target area, while also increasing low-dose exposure to critical organs like the heart and lungs.9,10 Additionally, the complex geometric relationship between bilateral breast targets necessitates steeper dose gradients and enhanced plan deliverability, underscoring the urgent need for technological advancements to overcome these limitations.
Jaw tracking VMAT (J-VMAT) is an advanced optimization mode of VMAT that dynamically synchronizes collimator jaw adjustments with MLC leaf movements. By continuously tracking target projection boundaries in real time, J-VMAT expands the effective modulation range of MLCs, reduces inter-leaf leakage and penumbra regions, and enhances target dose homogeneity while significantly minimizing radiation exposure to adjacent normal tissues. Recent studies have demonstrated the dosimetric advantages of jaw tracking technology in prostate, lung, brain, skin, and head-and-neck cancers.11–13 However, its application in SBBC remains systematically unvalidated. Existing minimal research has predominantly focused on unilateral breast cancer, while the dosimetric characteristics, treatment plan complexity, and clinical feasibility of simultaneous bilateral target irradiation in SBBC patients warrant further investigation.
This study addresses the clinical demands and technical challenges of radiotherapy for SBBC, with the goal of systematically evaluating the clinical value of J-VMAT. By comparing static jaw VMAT (S-VMAT), tangential arc VMAT (T-VMAT), and J-VMAT in terms of target coverage, dose homogeneity, organs at risk (OARs) sparing, and treatment efficiency, we aim to elucidate the potential advantages of T-VMAT and J-VMAT in SBBC radiotherapy. The findings are expected to provide a theoretical foundation for optimizing radiotherapy strategies for bilateral breast cancer, facilitate the clinical implementation of precision radiotherapy in complex anatomical scenarios, and ultimately contribute to improved patient outcomes and quality of life.
Materials and Methods
Patient Selection and Contouring
In this retrospective analysis, twelve patients diagnosed with SBBC between October 2011 and May 2024 were identified and included. Of these, seven underwent bilateral breast conserving surgery (BCS), four had bilateral modified radical mastectomy (MRM), and one received BCS on the left side and MRM on the right. Further details are presented in Table 1. A vacuum bag and wing board were used for immobilization, ensuring stable positioning. Patients were positioned in the supine posture with arms elevated above the head during both scanning and treatment to optimize access to the treatment area. They breathed freely without controlled breathing techniques to replicate natural respiratory patterns. CT images with a 3 mm slice thickness were acquired using a large-aperture CT scanner.
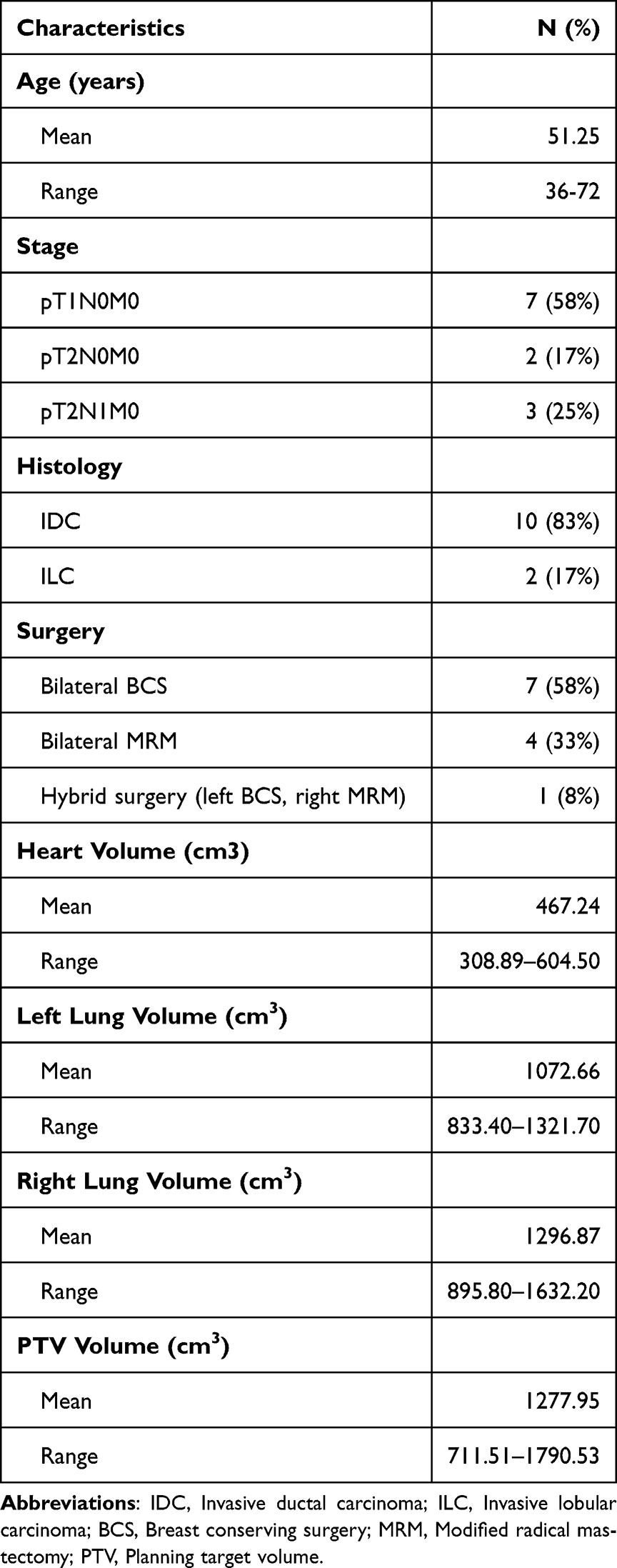 |
Table 1 General Patient Characteristics |
The clinical target volume (CTV) included both whole breasts, with the decision to include or exclude regional lymph node areas based on histological results. The planning target volume (PTV) was defined by expanding the CTV with a 5 mm margin, while excluding the outermost 3 mm below the skin surface. The OARs considered for evaluation were the right lung, left lung, heart, esophagus, trachea, left femoral head, right femoral head, spinal cord, and liver. A radiation oncologist delineated all target volumes and OARs according to the Radiation Therapy Oncology Group (RTOG) guidelines.14
Treatment Planning
For every patient, a novel treatment strategy was developed using S-VMAT, T-VMAT, and J-VMAT approaches. In these plans, 6 MV photon beams were delivered at an operating rate of 600 MU/min. The entire process was carried out on a TrueBeam linear accelerator from Varian Medical Systems, Inc. (Palo Alto, CA, USA), which is outfitted with a 120-leaf Millennium MLC to enable precise beam modulation. Dose distributions were computed using a finely spaced 2.5 mm grid in conjunction with the Anisotropic Analytical Algorithm (AAA) for accurate dosimetry. A total dose of 50 Gy was prescribed, administered in 25 fractions directly to PTV. The treatment design ensured that 95% of the PTV received the full prescribed dose, while the maximum dose was limited to no more than 110% of that value. Furthermore, the dose limitations for OARs were established based on clinical data from patients with unilateral breast cancer and earlier research involving SBBC.15–17 These limitations are as follows: for the lungs, the mean dose (Dmean) should be less than 15 Gy, with volume constraints of V5Gy < 70%, V20Gy < 30%, and V30Gy < 20%; for the heart, Dmean should be below 14 Gy, and the volume constraints are V5Gy < 40%, V20Gy < 15%, and V30Gy < 5%; for the liver, the volume constraints are V20Gy < 20% and V30Gy < 10%; for the esophagus, Dmean should be less than 10 Gy, with V20Gy < 30%; for the humeral heads, Dmean should not exceed 15 Gy; and for the spinal cord, the maximum dose (Dmax) should be kept below 40 Gy. These constraints were carefully selected to minimize radiation exposure to critical structures while optimizing treatment efficacy and maintaining a favorable therapeutic ratio.
In the present study, all three treatment plans utilized a single isocenter, centrally placed beneath the sternum to encompass the entire PTV. For the S-VMAT plans, the treatment plans incorporated two sets of four partial arcs, each covering a total arc span of 260°. To enhance beam delivery and ensure optimal dose distribution, the gantry was carefully rotated within a range of 230° to 130° for all patients (Figure 1a). Considering the mechanical constraints of the Varian linear accelerator, it is advised that the field size in the X direction does not exceed 15 cm, as going beyond this limit may negatively impact the modulation efficiency of the MLC. In addition, to minimize the influence of the tongue-and-groove effect during radiation delivery, the collimator angles were carefully set at either 85° or 95°. To ensure uniform dose coverage across the PTV, the partial arcs were specifically arranged to meet at the isocenter with a 3 cm overlap. This overlap region is crucial for maintaining dose consistency and avoiding underdosed areas within the target volume. The refinement of this overlap was achieved using the auto-feathering function, which effectively smooths the dose transition across the junction, ensuring a seamless integration between arcs. By minimizing dose inconsistencies and enhancing uniformity, this approach significantly improves the overall quality and effectiveness of the treatment plan. Such a systematic and precise planning strategy helps maximize therapeutic benefits while ensuring compliance with established safety and quality standards.
 |
Figure 1 Illustration of dose distributions and beam arrangements for S-VMAT (a) and T-VMAT (b) in synchronous bilateral breast cancer. |
With respect to T-VMAT plans, six tangential arc beams were meticulously designed to provide effective treatment for bilateral breast cancer while ensuring optimal coverage of the target areas. These beams were precisely configured to minimize radiation exposure to critical organs, such as the lungs and heart, thereby reducing potential side effects and improving patient safety. The design of the tangential beams was inspired by the concept of a peeled apple, with layers strategically arranged to conform to the contours of the treatment region and achieve precise dose distribution. To further enhance the accuracy of the radiation delivery, the collimator angle was carefully aligned parallel to the long axis of the target areas, ensuring that the beams precisely matched the shape and orientation of the intended treatment zones. In practice, the jaw positions for the left- and right-sided arcs were individually defined according to the anatomical extent of each breast PTV. The superior and inferior jaws were aligned with the cranio-caudal borders of the target, whereas the medial jaws were confined at the midline to avoid crossing into the contralateral side. The lateral jaws followed the chest wall contour, thereby restricting the irradiation volume and reducing unnecessary exposure to the lungs, heart, and contralateral breast, consistent with the approaches reported by Prokofev et al18 and Zhang et al.19 This configuration allowed the arcs to wrap tangentially around each breast, reproducing the geometry of conventional tangential fields while maintaining the advantages of VMAT modulation. The arc spans were individually tailored to patient anatomy, with the right-sided arcs typically ranging from 220°–260°, 240°–315°, and 315°–0°, and the left-sided arcs from 0°–45°, 45°–125°, and 100°–140° (Figure 1b). This comprehensive approach highlights the importance of both innovative design and precise execution in achieving effective and safe radiation therapy for breast cancer patients.
For the J-VMAT plans, we generated them by duplicating the S-VMAT plan and then enabling the jaw tracking technique. This approach allowed us to maintain consistency with the original S-VMAT plan while introducing the specific modification of jaw tracking. The integration of jaw tracking into the plan aimed to enhance the precision of dose delivery, potentially improving the sparing of surrounding healthy tissues by adjusting the jaws dynamically in response to the tumor’s position during treatment (Figure 2). By making this adjustment, we ensured that the only difference between the two plans was the use of jaw tracking, enabling a clear evaluation of its effects on treatment efficacy and accuracy. Throughout the optimization process, the same dose-volume objectives and constraints were implemented in all three treatment plans to ensure effective target coverage while reducing unnecessary radiation exposure to adjacent healthy tissues. Additionally, the prioritization of critical OARs remained consistent across all three plans, highlighting the need to protect normal tissue function and minimize potential adverse effects. This standardized approach allowed for an objective and equitable assessment of the performance and effectiveness of the S-VMAT, T-VMAT, and J-VMAT techniques.
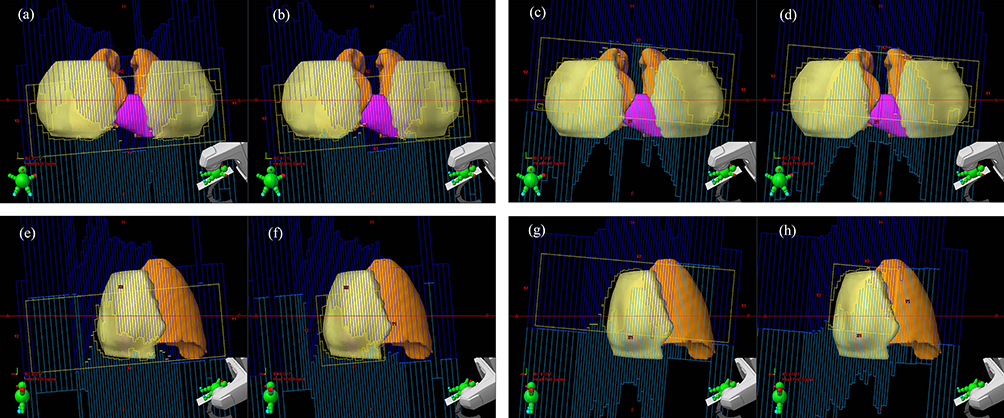 |
Figure 2 Beam’s eye views of a patient in S-VMAT and J-VMAT treatment plans. (a) S-VMAT (static jaw) arc segments at gantry 0° for ARC1. (b) J-VMAT (jaw tracking) arc segments at gantry 0° for ARC1. (c) S-VMAT (static jaw) arc segments at gantry 0° for ARC2. (d) J-VMAT (jaw tracking) arc segments at gantry 0° for ARC2. (e) S-VMAT (static jaw) arc segments at gantry 90° for ARC1. (f) J-VMAT (jaw tracking) arc segments at gantry 90° for ARC1. (g) S-VMAT (static jaw) arc segments at gantry 90° for ARC2. (h) J-VMAT (jaw tracking) arc segments at gantry 90° for ARC2. The yellow region represents the planning target volume; the Orange regions denote the lungs; and the magenta regions correspond to the heart. Orientation marks: L = left; R = right; H = head (superior); F = foot (inferior). Jaw boundaries: X1 and X2 denote the left and right jaw boundaries in the lateral direction; Y1 and Y2 denote the inferior (foot-side) and superior (head-side) jaw boundaries in the longitudinal direction. |
Plan Evaluation
The dose and volume data for the structures were extracted from a dose volume histograms (DVHs) to assess the treatment plans. For the PTV, the parameters assessed included D98%, D2%, D50%, V90%, V95%, V105%, and V110%. D98%, D2%, and D50% represented the doses delivered to 98%, 2%, and 50% of the target volume, respectively, while V90%, V95%, V105%, and V110% indicated the percentages of the target volume receiving 90%, 95%, 105%, and 110% of the prescribed dose. For the OARs, serial tissues were evaluated using the maximum point dose (Dmax) and the maximum volume receiving a specific dose (VxGy). The serial tissues analyzed included the heart, spinal cord, esophagus, trachea, and femoral heads. Parallel tissues, such as the lungs and liver, were assessed based on the maximum volume and mean dose (Dmean).
The conformity index (CI) was used to evaluate the target’s conformity, which is defined as:20
Vref represents the volume covered by the reference dose, VPTV denotes the volume of the PTV, and VPTVref refers to the volume of the PTV encompassed the reference dose. A higher CI indicates better conformity.
The uniformity of the dose distribution within the PTV was assessed using the homogeneity index (HI). The HI is defined as:21

D2%, D98%, and D50% correspond to the doses received by 98%, 2%, and 50% of the target volume, respectively. A lower HI value indicates better dose uniformity.
Delivery Parameters and Dosimetric Verification
The monitor units (MUs) for both treatment plans were quantitatively analyzed. The delivery times were accurately recorded, from the start of the first beam-on to the end of the last beam-off, excluding any time spent on positioning. A comparative analysis of delivery efficiency was performed by assessing the differences in delivery times among the three techniques.
The treatment plans were transferred to the ArcCHECK phantom (Sun Nuclear Corporation, Melbourne, Florida, USA) to measure the dose distributions as part of patient-specific quality assurance (QA). These measured distributions were then compared to the calculated dose distributions to assess the consistency of the dose delivery, using gamma analysis for the comparison. The measurement data were evaluated using gamma criteria of 3% dose difference and 3 mm distance-to-agreement, with a 10% dose threshold.22
Statistical Analysis
One-way analysis of variance (ANOVA) was performed to compare the means among the three techniques. Homogeneity of variances was tested using Levene’s test. If significant differences were found, post hoc multiple comparisons were conducted using Tukey’s test (for equal variances) or Games-Howell test (for unequal variances). A p-value < 0.05 was considered statistically significant. Statistical analysis was conducted using SPSS software (version 22.0, IBM, Chicago, IL).
Results
The evaluation of the treatment plan quantitatively involved analyzing DVHs, which were consistently utilized to assess the optimization of PTV coverage as well as the dose constraints of OARs. Tables 2 and 3 summarize the dosimetric parameters for PTV coverage and OARs dose distribution, respectively, as evaluated using the S-VMAT, T-VMAT, and J-VMAT techniques. Figure 3 illustrates the comparative DVHs for the PTV and OARs derived from the different treatment techniques.
 |
Table 2 Dosimetric Parameter Results for PTV, Treatment Efficiency, and Dosimetric Verification |
 |
Table 3 Comparison of OARs Dosimetric Parameters Using S-VMAT, T-VMAT, and J-VMAT Techniques |
 |
Figure 3 Comparison of DVHs for the PTV and OARs among the S-VMAT, T-VMAT, and J-VMAT techniques. |
PTV Coverage
Table 2 describes the dosimetric parameters for PTV coverage assessed using the S-VMAT, T-VMAT, and J-VMAT techniques. Statistical analysis revealed no significant differences (p > 0.05) among the three techniques in terms of D2%, D50%, D98%, V90%, V95%, V105% and V110%. Likewise, the CI and HI of the PTV showed no significant variation (p > 0.05) across the three approaches.
OARs Dose Distribution
Both T-VMAT and J-VMAT demonstrated significant improvements in OARs sparing compared to S-VMAT, with each showing strengths in different anatomical structures. For the lungs, T-VMAT achieved the lowest low-dose lung exposure, with a whole lung V5Gy of 39.69 ± 4.37%, while J-VMAT also significantly reduced lung dose and showed values closer to T-VMAT than S-VMAT. In terms of cardiac sparing, the reductions were even more pronounced. The heart Dmean was lowered from 11.25 Gy with S-VMAT to 9.21 Gy with J-VMAT and further to 7.44 Gy with T-VMAT. Additionally, the V5Gy to the heart decreased significantly, from 86.98% to 76.89% (J-VMAT) and 36.03% (T-VMAT). In the liver, T-VMAT achieved the greatest dose reduction, while J-VMAT still performed better than S-VMAT in Dmean and V30Gy. For serial organs such as the spinal cord, esophagus, and trachea, T-VMAT achieved the lowest Dmax, especially for the spinal cord. J-VMAT also showed significant reductions in esophageal and tracheal doses compared to S-VMAT.
Treatment Efficiency and Dosimetric Verification
In terms of MUs, T-VMAT also required fewer MUs than J-VMAT (p3 = 0.034), with no significant difference observed between S-VMAT and J-VMAT (p2 = 0.991) (Table 2). T-VMAT demonstrated a clear advantage in delivery efficiency, with a significantly shorter delivery time compared to both S-VMAT and J-VMAT (p1 < 0.001, p2 < 0.001, p3 < 0.001). Specifically, delivery time was reduced by over one-third relative to S-VMAT and by nearly half compared to J-VMAT. Meanwhile, QA pass rates exceeded 99% for all three techniques, with no significant differences detected (p > 0.05).
Discussion
SBBC encompasses a vast target volume and a complex anatomical treatment area. While the bilateral breasts are symmetrically positioned, the natural curvature of the chest wall and post-surgical anatomical changes often lead to irregular target shapes. Furthermore, dose constraints for OARs, including the heart, lung tissue, and liver, add another layer of complexity to treatment planning.23 This study presents a comprehensive comparison of T-VMAT, J-VMAT, and S-VMAT techniques in the treatment of SBBC. The findings illuminate the dosimetric trade-offs between target coverage, OARs sparing, and treatment efficiency, providing valuable insights to guide clinical decision-making.
To enhance clinical efficiency in SBBC treatment, a single isocenter was implemented for the T-VMAT, J-VMAT, and S-VMAT plans. This approach not only reduces patient setup time but also streamlines and optimizes the overall treatment workflow, ultimately enhancing both the precision and effectiveness of the procedure.24,25 In this study, the 100% isodose effectively covered no less than 95% of the target PTV in all plans, ensuring adequate target dose coverage. The absence of significant differences in PTV coverage parameters (D2%, D50%, D98%, V90%, V95%, V105%, HI, and CI) among T-VMAT, J-VMAT, and S-VMAT indicates that all three techniques achieve comparable target coverage and plan homogeneity. Furthermore, these findings confirm that the integration of jaw tracking functionality does not compromise PTV dose distribution. This aligns with previous studies, which demonstrate that jaw tracking technology effectively maintains robust target coverage while optimizing beam shaping.26,27
In reference to the lungs, Marks et al28 indicated that the risk of radiation pneumonitis (RP) could be reduced to below 20% when the Dmean was kept under 20–23 Gy and the V20Gy was restricted to 30–35%. Jiang et al29 confirmed that compliance with the following constraints significantly reduced the incidence of RP: limiting V5Gy to below 65%, restricting V20Gy to under 40%, and maintaining Dmean within the range of 20–22 Gy. Graham et al30 reported that RP did not observed when V20Gy was less than 22%. The findings of this study demonstrated that the lung Dmean, V5Gy, and V20Gy metrics in the T-VMAT, J-VMAT, and S-VMAT plans were considerably lower than those reported in previous research. Moreover, T-VMAT and J-VMAT exhibited superior lung protection, with significantly lower V5Gy values for the left lung, right lung, and whole lung compared to S-VMAT plans. The substantial reductions in V5Gy for both lungs underscore J-VMAT’s effectiveness in minimizing radiation exposure to healthy lung tissue, which is essential for reducing the risk of RP. This finding is in agreement with the results of Jung et al15 who utilized the Jaw tracking VMAT technique in the treatment of unilateral breast tumors.
During the radiotherapy treatment for SBBC, the simultaneous irradiation of bilateral target areas leads to an increased cumulative dose to the heart. Therefore, careful consideration should be given to minimizing cardiac radiation exposure. Numerous authoritative studies consistently underscore a well-documented and significant association between radiotherapy and an increased risk of cardiovascular disease.31–33 According to Darby et al,34 there is a dose-dependent association between heart irradiation and ischemic heart disease risk. The study revealed that a 1 Gy increase in the mean heart dose corresponds to a 7.4% higher probability of major coronary events. Another study reported a 16.5% increase in the cumulative incidence of acute coronary events per gray of mean radiation dose to the heart within the first nine years after treatment.35 The discoveries from their investigation disclosed a direct association between the mean radiation dose delivered to the heart and the probability of coronary artery deterioration. Furthermore, Shi et al36 reported a 1.1 Gy reduction in the mean heart dose with jaw tracking plans compared to static jaw plans. Similarly, Jung et al15 observed a 1.6 Gy decrease in Dmean with jaw tracking plans compared to static jaw plans. In our study, the Dmean of the heart in the J-VMAT plans was reduced from 11.25 Gy to 9.21 Gy, representing a reduction of 2.04 Gy compared to the S-VMAT plans. This decrease suggests that J-VMAT may lower the risk of radiation-induced cardiac complications. Notably, T-VMAT further decreased the heart Dmean to 7.44 Gy, achieving a 3.81 Gy reduction and indicating an even greater potential for cardiac protection. Additionally, other OARs such as the liver, spinal cord, esophagus, trachea, and humeral heads also exhibited notable dose reductions with J-VMAT, while T-VMAT achieved the most pronounced dose sparing in several of these structures, further reinforcing the dosimetric advantages of both advanced techniques.
While J-VMAT demonstrated dosimetric advantages, its longer delivery time compared to S-VMAT (p2 < 0.001) and T-VMAT (p3 < 0.001) warrants consideration. This discrepancy may arise from the increased mechanical complexity of dynamic jaw motion during arc delivery, which could impact clinical workflow and patient throughput. However, the absence of significant differences in MUs among the three techniques suggests that jaw tracking does not introduce any additional burden on dose output from a dose calculation standpoint. Additionally, all three techniques demonstrated high dosimetric accuracy, as evidenced by ArcCHECK verification results with gamma passing rates exceeding 99%. The lack of significant differences in QA outcomes among the techniques further reinforces the reliability of the calculated treatment plans. This observation is consistent with the findings of Yao et al37 and Park et al38 who conducted dosimetric verification studies employing gamma analysis techniques.
Our results show that T-VMAT provides superior OARs sparing and comparable target coverage for SBBC, despite the predefined jaw positions. The tangential arcs follow the natural breast contour, limiting low-dose exposure to lungs, heart, and contralateral breast, while the optimizer modulates beam intensity within the arcs to achieve precise target coverage. This design also reduces overlap and redundancy in beam paths, resulting in substantially fewer monitor units and improved treatment efficiency. These findings highlight the clinical advantage of T-VMAT in balancing OARs protection and delivery efficiency and demonstrate that careful arc geometry combined with VMAT modulation can outperform conventional partial-arc VMAT approaches.
Although variations in surgical procedures may lead to alterations in chest wall anatomy, which could potentially influence the dosimetry of OARs, particularly the heart and lungs, all patients in this study were subjected to uniform contouring protocols and identical planning objectives. Consequently, the dosimetric differences observed among treatment plans are predominantly attributed to the distinct characteristics of the jaw techniques employed, rather than anatomical variations introduced by surgical interventions.
Conclusion
In this study, a comprehensive comparison of S-VMAT, T-VMAT, and J-VMAT techniques was conducted in the context of SBBC radiotherapy. The findings demonstrated that both T-VMAT and J-VMAT significantly improved OARs sparing compared to conventional S-VMAT, particularly in reducing the mean dose to the lungs and heart, which are critical structures in breast cancer treatment. T-VMAT showed the greatest advantage in lowering low-dose exposure and treatment delivery time, while J-VMAT provided a favorable balance between dosimetric performance and delivery accuracy.
Ethics Statement
This study was reviewed and approved by the Ethics Committee of the Cancer Hospital of Shantou University Medical College. The requirement for informed consent was waived as the data were retrospectively collected and anonymized before analysis. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and national research committees and with the principles of the Declaration of Helsinki and its subsequent amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Medical Scientific Research Foundation of Guangdong Province (B2017025) and Shantou Medical Science and Technology Planning Project (no. 2025-96).
Disclosure
The authors declare no competing interests in this work.
References
1. Jiang H, Zhang R, Liu X. Bilateral breast cancer in China: a 10-year single-center retrospective study (2006-2016). Cancer Med. 2021;10(17):6089–6098. doi:10.1002/cam4.4141
2. Schmid SM, Pfefferkorn C, Myrick ME, et al. Prognosis of early-stage synchronous bilateral invasive breast cancer. Eur J Surg Oncol. 2011;37(7):623–628. doi:10.1016/j.ejso.2011.05.006
3. Bhimani F, McEvoy M, Gupta A, et al. Case report: bilateral targeted intraoperative radiotherapy: a safe and effective alternative for synchronous bilateral breast cancer. Front Oncol. 2023;13:1276766. doi:10.3389/fonc.2023.1276766
4. Pasler M, Lutterbach J, Björnsgard M, Reichmann U, Bartelt S, Georg D. VMAT techniques for lymph node-positive left sided breast cancer. Z Med Phys. 2015;25(2):104–111.
5. Karpf D, Sakka M, Metzger M, Grabenbauer GG. Left breast irradiation with tangential intensity modulated radiotherapy (t-IMRT) versus tangential volumetric modulated arc therapy (t-VMAT): trade-offs between secondary cancer induction risk and optimal target coverage. Radiat Oncol. 2019;14(1):156. doi:10.1186/s13014-019-1363-4
6. Kang Z, Chen S, Shi L, He Y, Gao X. Predictors of heart and lung dose in left-sided breast cancer treated with VMAT relative to 3D-CRT: a retrospective study. PLoS One. 2021;16(6):e0252552. doi:10.1371/journal.pone.0252552
7. Kuzba-Kryszak T, Nowakowski S, Winiecki J, Makarewicz R. Comparative analysis of the absorbed dose in the heart and anterior descending branch of the left coronary artery (LAD) in patients with left-sided breast cancer who received radiotherapy using 3D-CRT, IMRT and VMAT techniques. J BUON. 2021;26(3):753–758.
8. Qiu J, Zhang S, Lv B, Zheng X. Cardiac dose control and optimization strategy for left breast cancer radiotherapy with non-uniform VMAT technology. Technol Cancer Res Treat. 2021;20:15330338211053752.
9. Ugurlu BT, Temelli O. The impact of the field width on VMAT plan quality and the assessment of half field method. J Appl Clin Med Phys. 2020;21(3):115–122. doi:10.1002/acm2.12834
10. Nath J, Sarma G. Split X-jaw planning technique of volumetric modulated arc radiotherapy. J Med Phys. 2023;48(4):398–401. doi:10.4103/jmp.jmp_67_23
11. Snyder KC, Wen N, Huang Y, et al. Use of jaw tracking in intensity modulated and volumetric modulated arc radiation therapy for spine stereotactic radiosurgery. Pract Radiat Oncol. 2015;5(3):e155–e162. doi:10.1016/j.prro.2014.09.002
12. Thongsawad S, Khamfongkhruea C, Tannanonta C. Dosimetric effect of jaw tracking in volumetric-modulated arc therapy. J Med Phys. 2018;43(1):52–57. doi:10.4103/jmp.JMP_75_17
13. Sun W, Shi Y, Li Y, et al. Selection strategy of jaw tracking in VMAT planning for lung SBRT. Front Oncol. 2022;12:820632. doi:10.3389/fonc.2022.820632
14. Radiation Therapy Oncology Group. Breast cancer atlas for radiation therapy planning: consensus definitions. Philadelphia, PA: Radiation Therapy Oncology Group; 2016. Available from: https://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx.
15. Jung S, Kim JI, Park JM, Shin KH, Kim JH, Choi CH. Comparison of treatment plans between static jaw and jaw tracking techniques in postmastectomy intensity-modulated radiation therapy. Phys Eng Sci Med. 2022;45(1):181–187. doi:10.1007/s13246-022-01100-y
16. Duan S, Li C, Shi J, et al. Synchronous bilateral breast carcinoma irradiation: a comparative investigation between flattened and unflattened beams. Appl Radiat Isot. 2022;181:110079. doi:10.1016/j.apradiso.2021.110079
17. Gadea J, Ortiz I, Roncero R, et al. Synchronous bilateral breast cancer treated with a 3-week hypofractionated radiotherapy schedule: clinical and dosimetric outcomes. Clin Transl Oncol. 2021;23(9):1915–1922. doi:10.1007/s12094-021-02600-1
18. Prokofev I, Salim N. Off-isocentric VMAT technique for breast cancer: effective dose reduction to organs at risk and its applicability based on patient anatomy. J Appl Clin Med Phys. 2024;25(3):e14237. doi:10.1002/acm2.14237
19. Zhang Y, Fu W, Brandner E, Percinsky S, Moran M, Huq MS. Minimizing normal tissue low dose bath for left breast Volumetric Modulated Arc Therapy (VMAT) using jaw offset. J Appl Clin Med Phys. 2024;25(8):e14365. doi:10.1002/acm2.14365
20. Paddick I. A simple scoring ratio to index the conformity of radiosurgical treatment plans. Technical note. J Neurosurg. 2000;3:219–222.
21. Zhang J, Huang L, Wu F, et al. Tailoring PTV expansion to improve the dosimetry of post modified radical mastectomy intensity-modulated radiotherapy for left-sided breast cancer patients by using 4D CT combined with cone beam CT. J Appl Clin Med Phys. 2021;22(5):139–146. doi:10.1002/acm2.13244
22. Low DA, Harms WB, Mutic S, Purdy JA. A technique for the quantitative evaluation of dose distributions. Med Phys. 1998;25(5):656–661. doi:10.1118/1.598248
23. Djoumessi Zamo FC, Njeh CF, Colliaux A, Blot-Lafond V, Moyo MN. Patient specific quality assurance of volumetric modulated arc therapy of synchronous bilateral breast cancer. Med Dosim. 2024;49(3):177–184. doi:10.1016/j.meddos.2023.11.003
24. Cheng HW, Chang CC, Shiau AC, Wang MH, Tsai JT. Dosimetric comparison of helical tomotherapy, volumetric-modulated arc therapy, intensity-modulated radiotherapy, and field-in-field technique for synchronous bilateral breast cancer. Med Dosim. 2020;45(3):271–277. doi:10.1016/j.meddos.2020.01.006
25. Kang SW, Kang S, Lee B, et al. Evaluation of the dosimetric and radiobiological parameters in four radiotherapy regimens for synchronous bilateral breast cancer. J Appl Clin Med Phys. 2022;23(8):e13706. doi:10.1002/acm2.13706
26. Feng Z, Wu H, Zhang Y, Zhang Y, Cheng J, Su X. Dosimetric comparison between jaw tracking and static jaw techniques in intensity-modulated radiotherapy. Radiat Oncol. 2015;10:28. doi:10.1186/s13014-015-0329-4
27. Pokhrel D, Sanford L, Halfman M, Molloy J. Potential reduction of lung dose via VMAT with jaw tracking in the treatment of single-isocenter/two-lesion lung SBRT. J Appl Clin Med Phys. 2019;20(5):55–63. doi:10.1002/acm2.12580
28. Marks LB, Bentzen SM, Deasy JO, et al. Radiation dose-volume effects in the lung. Int J Radiat Oncol Biol Phys. 2010;76(3 Suppl):091.
29. Jiang Z-Q, Yang K, Komaki R. Long-term clinical outcome of intensity-modulated radiotherapy for inoperable non-small cell lung cancer: the MD Anderson experience. Int J Radiat Oncol Biol Phys. 2012;83(1):332–339. doi:10.1016/j.ijrobp.2011.06.1963
30. Graham MV, Purdy JA, Emami B, et al. Clinical dose-volume histogram analysis for pneumonitis after 3D treatment for non-small cell lung cancer (NSCLC). Int J Radiat Oncol Biol Phys. 1999;45(2):323–329. doi:10.1016/s0360-3016(99)00183-2
31. Taylor CW, Wang Z, Macaulay E, Jagsi R, Duane F, Darby SC. Exposure of the heart in breast cancer radiation therapy: a systematic review of heart doses published during 2003 to 2013. Int J Radiat Oncol Biol Phys. 2015;93(4):845–853. doi:10.1016/j.ijrobp.2015.07.2292
32. Santoro F, Tarantino N, Pellegrino PL. Cardiovascular sequelae of radiation therapy. Clin Res Cardiol. 2014;103(12):955–967. doi:10.1007/s00392-014-0718-y
33. Misra S, Mishra A, Lal P. Cardiac dose reduction using deep inspiratory breath hold (DIBH) in radiation treatment of left sided breast cancer patients with breast conservation surgery and modified radical mastectomy. J Med Imaging Radiat Sci. 2021;52(1):57–67. doi:10.1016/j.jmir.2020.12.004
34. Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–998. doi:10.1056/NEJMoa1209825
35. van den Bogaard VA, Ta BD, van der Schaaf A, et al. Validation and modification of a prediction model for acute cardiac events in patients with breast cancer treated with radiotherapy based on three-dimensional dose distributions to cardiac substructures. J Clin Oncol. 2017;35(11):1171–1178. doi:10.1200/JCO.2016.69.8480
36. Shi L, Lai Y, Chen S, Fu L, Lin Q. Dosimetric superiority of IMRT with jaw tracking technique for whole esophagus and T-shaped field radiotherapy in advanced esophageal cancer. PLoS One. 2018;13(9):e0202628. doi:10.1371/journal.pone.0202628
37. Yao S, Zhang Y, Chen T, et al. Dosimetric comparison between jaw tracking and no jaw tracking in intensity-modulated radiation therapy. Technol Cancer Res Treat. 2019;18:1533033819841061. doi:10.1177/1533033819841061
38. Park SH, Ko H, Choi J. Effect of jaw tracking during volumetric modulated arc therapy for facial non-melanoma skin cancer. In Vivo. 2024;38(2):849–854. doi:10.21873/invivo.13510
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.