Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Does surgical treatment within 4 hours after trauma have an influence on neurological remission in patients with acute spinal cord injury?
Authors Biglari B, Child C, Yildirim TM, Swing T, Reitzel T, Moghaddam A
Received 19 March 2016
Accepted for publication 23 April 2016
Published 31 August 2016 Volume 2016:12 Pages 1339—1346
DOI https://doi.org/10.2147/TCRM.S108856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Bahram Biglari,1 Christopher Child,2 Timur Mert Yildirim,2 Tyler Swing,2 Tim Reitzel,1 Arash Moghaddam2
1Department of Paraplegiology and Technical Orthopedics, BG Trauma Centre, Ludwigshafen, Germany; 2Heidelberg Trauma Research Group, Center for Orthopedics, Trauma Surgery and Spinal Cord injury, Heidelberg University Hospital, Heidelberg, Germany
Background: The proper timing for surgery in patients with acute spinal cord injury is controversial. This study was conducted to detect if there is an advantage in early (within the first 4 hours after trauma) compared to late (between 4 and 24 hours after trauma) surgery on neurological outcome.
Methods: In this single institution prospective cohort study, data were analyzed from 51 spinal cord injured patients with an average age of 43.4 (±19.2) years. The influence of early (29 patients within the first 4 hours) as opposed to late (22 patients between 4 and 24 hours) decompression was evaluated by comparing data for neurological outcome. Patients of the study collectively suffered acute spinal fractures from C2 to L3 (cervical 39.2%, thoracic 29.4%, and lumbal 21.6%) or nonosseous lesions (9.8%). American Spinal Injury Association (ASIA) Impairment Scale (AIS) grades were assessed at time of admission and 6 months after trauma or longer depending on the time of release. Surgical treatment included early stabilization and decompression within 24 hours.
Results: No significant difference between improved neurological function, measured with the AIS, and an early or late surgery time can be seen (P=0.402). Furthermore, binary logistic regression shows no significant difference between sex or age, and AIS improvement as possible confounders.
Conclusion: In our study, all patients with spinal cord injury were treated with spine stabilization and decompression within the first 24 hours after trauma. Surgical decompression within the first 4 hours after trauma was not associated with improved neurological outcome compared to treatment between 4 and 24 hours. In a clinical context, this indicates that there is a time frame of at least 1 day in which optimal care is possible.
Keywords: spinal cord injury, surgery, neurological remission, neurological outcome, AIS
Background
Traumatic spinal cord injury (SCI) often affects young and healthy people and is associated not only with physical disability but also financial, social, and psychological consequences to the individual as well as to those in his social surroundings.1 In addition, this kind of injury involves high costs for insurance companies and the state and thus for the society.2 The incidence of traumatic SCI worldwide is ~29.5 per million inhabitants and the prevalence is ~485 per million inhabitants.2 Currently, there are no causal therapy options for improvement of neurological outcomes after traumatic SCI. All treatment options are related to damage containment and early rehabilitation.
The administration of methylprednisolone sodium succinate is controversial. Cochrane meta-analysis showed evidence supporting motor function recovery in the methylprednisolone sodium succinate group compared to the control group.3 While Hurlbert et al have been consistently against the use of steroids,4 Fehlings et al have insisted that the use of steroids should be considered and left as a treatment option at the discretion of physicians.5 There is need for more randomized trials of pharmacologic therapy for acute SCI.3 The main consensus of opinion in the literature is regarding early mechanical stabilization and decompression of the spinal cord.6 Decompression allows the spinal cord to recover and stops the occurrence of further direct damage to the spinal cord.
Based on pathophysiological criteria, distinctions can be made between the primary phase of injury, which is caused by mechanical force on the spinal cord, and the secondary phase of damage. Edema, necrosis, and ischemia occur in the first few days after trauma as a result of various vascular changes.7 In addition, biochemical signaling cascades are activated, which initiate additional pathological processes.8 Because damage in the primary phase cannot be prevented, all approaches focus on restricting damage in the secondary phase of the injury. Some animal models have suggested that surgical decompression of the spinal cord is accompanied by a reduction of secondary damage, as well as an improvement in motor function.9 Clear evidence for a positive neuroprotective effect of spinal cord decompression and improved clinical outcome is still absent. Also, the proper timing for decompression remains controversial; however, most studies indicate an enhanced neuroprotective effect after early spinal cord decompression.9–12
We pursued the question of whether surgical care within the first 4 hours after trauma has an influence on the patient’s recovery or if later surgical treatment is sufficient.
Materials and methods
Our study is a prospective, monocentric cohort study. Fifty-one patients with acute traumatic SCI were treated in our hospital from 2009 to 2013.
The BG Trauma Center is a level 1 trauma hospital with its own air ambulance. Patient and accident data were collected, such as age, sex, course of events, fracture type according to Arbeitsgemeinschaft Osteosynthese (AO) classification, lesion site, type of paralysis, date and time of alerting the ambulance, and American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade at time of admission and release.
Analysis of prospectively gathered data was done at least a year after discharge from the hospital due to ethical concerns. The persons involved in executing this study, including data analysis, had no influence on initial treatment or on the course of treatment, such as time of surgery or type of surgery. They were simply observers in the process. One should note that the time of hospital discharge was different in patients, making the time interval between the first and second AIS classification variable.
Inclusion criteria were the following: patients with AIS A–D were included in the study according to the AIS guidelines. All patients had traumatic spinal cord damage. Informed consent had to be obtained from all participants or next of kin. Excluded from the study were the following: patients with nontraumatic acute paralysis, pregnant females, vertebral column cancer patients, patients operated on >24 hours after trauma, patients in a life-threatening situation with an immediate surgical contraindication, penetration injury, and preexisting neurological conditions.
Due to available resources, operation after trauma was achievable within 4 hours in many patients. The patient pool was divided into two groups: group 1 (G1) contained all patients who were hospitalized and operated on within the first 4 hours after trauma; group 2 (G2) contained those patients who received treatment after 4 hours but within 24 hours after trauma. The ethics committee of the Chamber of Medicine Rheinland-Pfalz gave their approval to this study (No 837.266.09).
The neurological examination of the SCI was carried out according to standard specifications of the ASIA and injuries were characterized according to the neurological level of injury. The AIS classification system was determined at the time of admission and before discharge over a 6-month follow-up period. Upon arrival, all the patients received both anteroposterior and lateral X-rays as well as a computed tomography (CT) and magnetic resonance imaging (MRI) according to standard procedure in order to illustrate the extent of the fracture and to determine the adequate surgical procedure. A dorsal decompression of the spinal canal was done and the segments were stabilized with various procedures. High-grade fractures were treated with open surgery. If needed, a vertebral body was replaced. In certain circumstances, the cleaning of the spinal canal was necessary. To ensure a safe recovery of the spine, the other patients were treated in two stages in the following 3–4 weeks with ventral stabilization (eg, cage implantation). Because all patients initially received sufficient decompression, the second ventral surgery performed had no further impact on decompression. Within 1 week from the date of surgery, another control CT was performed. Subsequently, patients were divided into two groups according to time of surgery (surgery under or over 4 hours after trauma). After surgical stabilization, all the patients were treated and rehabilitated in a timely manner according to the standard procedure for SCI.
Data analysis
Data analysis was supported by the Institute for Medical Biometrics and IT at the University of Heidelberg, Germany. Statistical analysis for consecutive variables was done with the Student’s t-test. The odds ratio of early and late surgery, age, and sex with AIS improvement were calculated (Table 1). Categorical data between groups were compared with the chi-squared test. Binary logistic regression was applied to analyze the dependence between neurological outcome and early or late surgery (Table 1). The presence or absence of AIS improvement from the initial to final follow-up was set as the outcome variable. The timing of surgery (early or late) was set as the predictor variable. Additionally, sex and age were tested as covariates. Statistical analyses were done with SPSS Software 22.0 (IBM Corporation, Armonk, NY, USA). Figures were created with Sigmaplot Software 11.0 (SPSS Inc., Chicago, Illinois, USA).
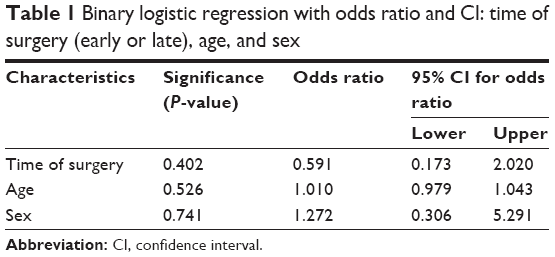 | Table 1 Binary logistic regression with odds ratio and CI: time of surgery (early or late), age, and sex |
Results
In this study, 51 patients were included according to inclusion criteria (initial AIS A–D and compliance of the patient) and relevant data were evaluated statistically.
Table 2 shows the following parameters: age, sex, lesion site, type of injury, AO classification, AIS before and at follow-up, as well as the accident etiology. Dorsal stabilization with decompression of the spinal cord was carried out in all patients no later than 24 hours after arrival. After 3–4 weeks, 45 patients received a second ventral surgical procedure to ensure a safe recovery of the spine. Figure 1 shows pre- and postoperative imaging of two patients. No complications were encountered postoperatively. Neurological improvements were seen in 21 patients from initial to final evaluation. We divided our patient pool in two groups: G1 (n=29) received decompression within the first 4 hours after accident; G2 (n=22) was operated on after 4 hours (Table 2). In both groups, the AIS classification was conducted in awake and responsive patients. After surgery, as well as in the follow-up period, no complications or mortalities were observed.
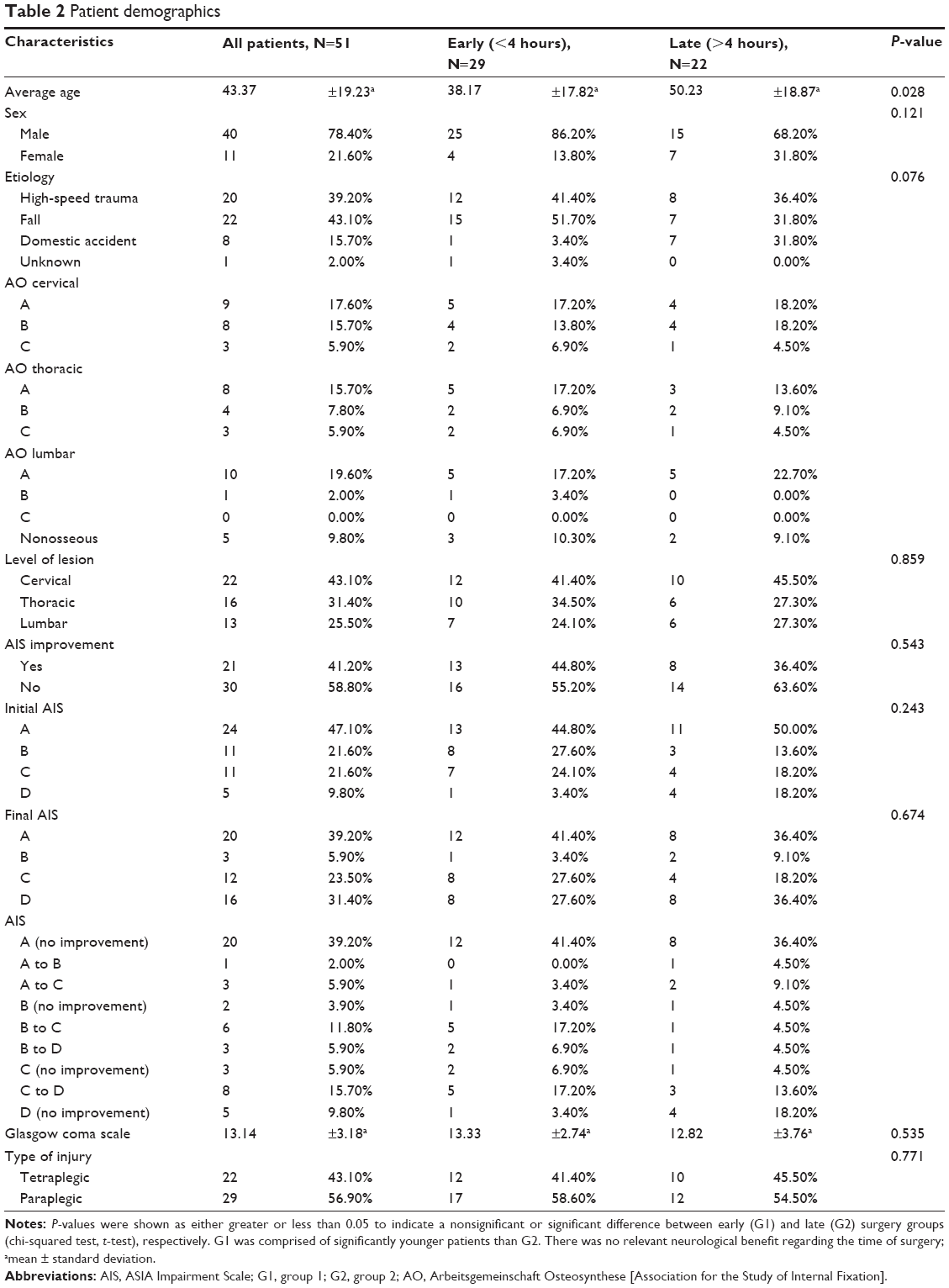 | Table 2 Patient demographics |
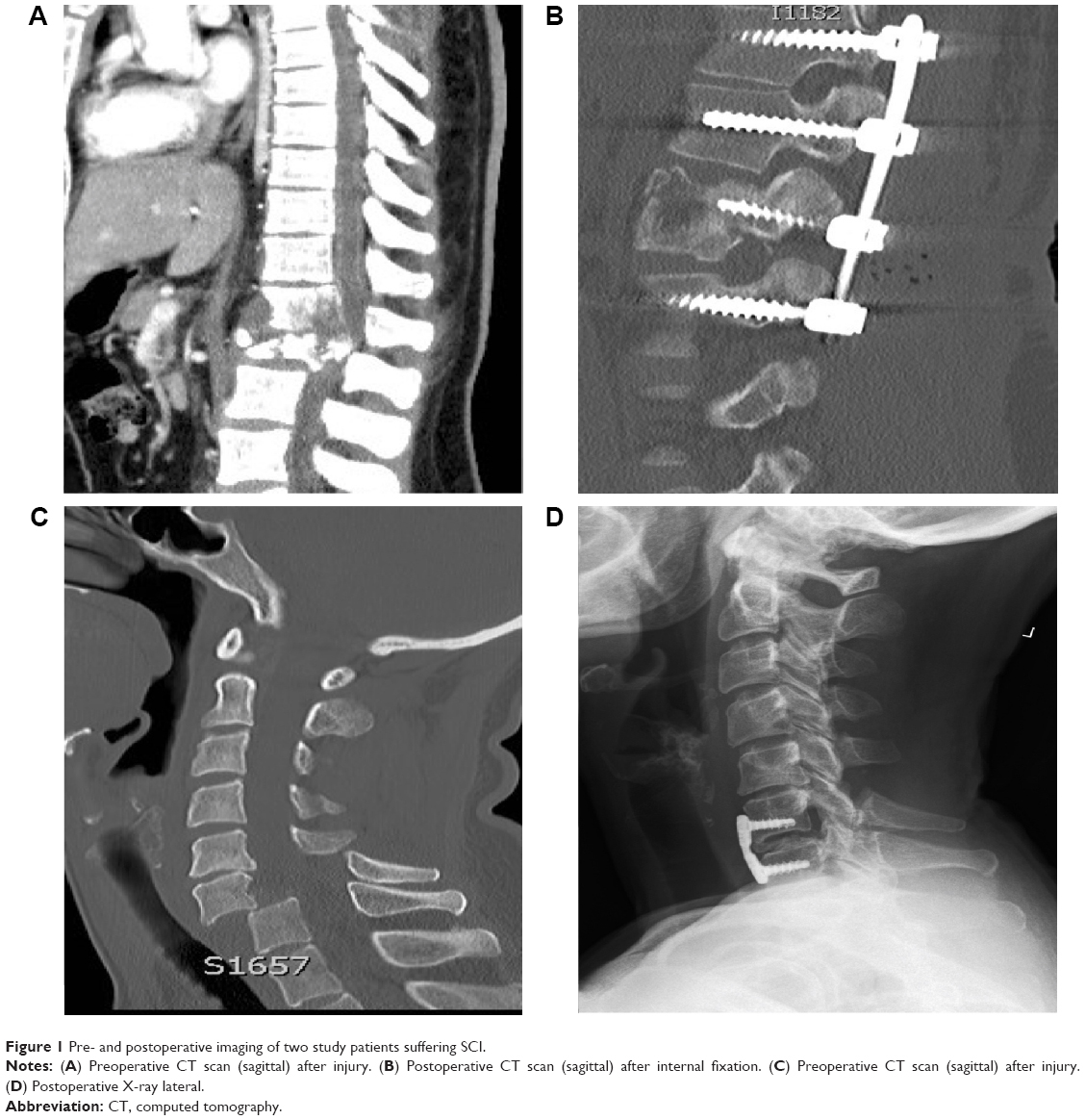 | Figure 1 Pre- and postoperative imaging of two study patients suffering SCI. |
Table 2 gives an overview of the demographics and details of the two groups. G1 had a mean time of 3.2±0.65 hours until surgery and G2 8.2±5.9 hours. The average age of the patients was 43.4±19.2 (15–86) years. Eleven patients were females (21.6%) and 40 males (78.4%). The height of the lesion on the spinal cord was cervical in 22 cases (43.1%), thoracic in 16 (31.4%), lumbar in 13 (25.5%), and there were no sacral cases. There was neurological improvement in 21 (41.2%) over the course of the follow-up study compared to initial AIS grades. There were no significant differences between the distributions of the sex, lesion site, type of fracture, etiology, or Glasgow coma scale between the two groups. However, there was a significant difference in the distribution of average ages between the early and the late surgery groups (P=0.028). In the earlier group, patients tended to be younger.
The classification of fractures was carried out according to the AO classification. A fractures were recorded in 27 (52.9%) cases, B fractures in 13 (25.5%) cases, C fractures in six (11.8%) cases, and nonosseous trauma in five cases (9.8%) (Table 2).
Twenty nine (56.9%) were paraplegic and 22 (43.1%) tetraplegic. The first AIS measurement revealed 24 (47.1%) patients with AIS A, eleven (21.6%) patients with AIS B, eleven (21.6%) patients with AIS C, and five (9.8%) patients with AIS D. The follow-up after 6 months showed AIS score measurements of 20 (38.2%) patients with AIS A, three (5.9%) with AIS B, 12 (23.5%) with AIS C, and 16 (31.4%) with AIS D. AIS E was seen in one patient (1.8%) (Table 2).
According to the results of the National Acute Spinal Cord Injury Study 2 and 3, no patient received methylprednisolone or similar corticoids after surgery or in the clinic.13 Only three patients were administered prednisolone by an emergency physician on location. Blood pressure was taken, and substantial changes in blood pressure were treated without the use of vasopressors.
Neurological improvement
In G1, 13 (44.8%) of 29 patients had an improved neurological outcome and 16 (45.2%) showed no change in AIS grades. In G2, eight (36.4%) of 22 patients had an improved neurological outcome. Fourteen (63.3%) patients showed no neurological improvement in the follow-up (Figure 2).
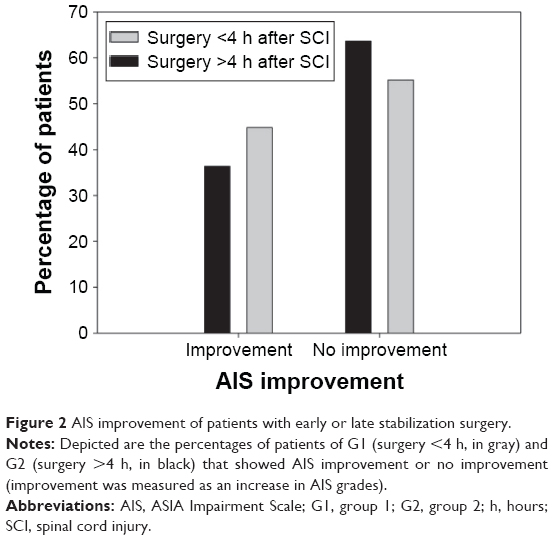 | Figure 2 AIS improvement of patients with early or late stabilization surgery. |
If one considers the binary logistic regression and the odds ratio, no significant difference between the improvement of neurological function and early or late surgery could be seen (P=0.402). There was also no significant difference between sex (P=0.741) or age (P=0.526) and the AIS improvement (Table 1). In order to determine if patient groups compared in this study (ie, early vs late surgery, or absence vs presence of neurological improvement) were similar in terms of other factors, statistical tests were used to compare the groups. When the patients were grouped according to the absence or presence of AIS improvement, no significant differences between groups were found in age (P=0.480), sex (P=0.765), etiology (P=0.329), height of lesion (P=0.666), or Glasgow coma scale (P=0.666) according to the Student’s t-test and chi-squared test. There might have been differences between both groups, although no significant data was found due to the size of the patient pool. Nevertheless, the missing significance between the groups indicates that age, sex, etiology, height of lesion, and Glasgow coma scale had little influence on the neurological outcome.
Finally, with regard to the initial type of AIS, there did appear to be a significant correlation between initial type of AIS and neurological improvement (P<0.001). Overall, 16.7% of AIS-A injuries, 81.8% of AIS-B, 72.7% of AIS-C, and none of AIS-D injuries showed neurological improvement.
Discussion
We conducted a single institution prospective cohort study with data from 51 patients suffering from acute SCI. Our findings led to the conclusion that decompression of SCIs should be performed soon, but not necessarily within the first 4 hours after trauma.
Considering the two groups as a collective, we observed no significant difference in neurological improvement. There was also no significant difference between sex or age and AIS improvement. Still it should be noted that we were limited by the nature of trauma surgery, which did not allow us to divide patients into two equal groups with similar demographics. Patients were operated on as soon as possible and then later grouped during data analysis according to the timing of surgery. In order to provide the proper context in which our results should be interpreted, we listed the demographics according to the two different groups (Table 2). Analysis of preclinical studies supports early decompression after SCI.11 Twenty-two publications based on human data have been published between 1991 and 2009 with varying results and levels of evidence. Levi et al showed in a study from 1991 with 103 patients suffering cervical spine trauma that there were no differences in neurological outcome between early operated patients (<24 hours) and those who received later treatment (>24 hours).14 Mirza et al reported in a study with only 30 patients that those who received early operative treatment (within 3 days) had better motor function, but there was no improvement according to the Frankel grade.15 Duh et al reported in a study using data from the second National Acute Spinal Cord Injury Study that no correlation could be found between a significant improvement in neurological outcome and the time of surgery.16 Chen et al demonstrated that the early (within 4 days) and late (later than 4 days) groups showed similar results in the follow-up using the AIS and the Short Form Health Survey (SF-36).17 Additionally, another large study from 2001 by Croce et al with 291 patients failed to supply conclusive information on neurological improvement and timing of surgery.18 Results of other studies showed a similar tendency.19–21
However, there are also studies that support early decompression. Cengiz et al, for example, showed in a study with 27 patients an improvement in AIS grades in an early group (within 8 hours) and a late group (3–15 days).22 Another recent study with a total number of 69 patients evaluated subaxial cervical spine injuries and concluded that early surgery (within 48 hours) should be considered strongly in view of the lesser complications, early discharge, and reduced mortality.23
The striking differences in the definition of early and late surgery, varying between hours and days, led to problems of comparison between different studies. Early operative care in human studies varied between 8 hours and 4 days after the injury.11 The late care varied between 8 hours and later than 5 days after the injury.11
Due to the possibility of a prompt patient rescue and operative treatment after trauma in many patients, we chose the earliest possible time point to answer the question whether it is necessary to treat the patients surgically at the earliest possible date or it is sufficient to operate within the first 24 hours after trauma.
La Rosa et al showed in a meta-analysis that early surgery within the first 24 hours had a better neurological outcome than after 24 hours or conservative treatment.12 Furthermore, Fehling et al reported in 2012 that surgical stabilization and decompression of the spinal cord are easier within the first 24 hours and can lead to an improvement in neurological outcome.10
Assuming that surgery after 24 hours results in poorer outcome, late decompression was defined as between 4 and 24 hours.
Because adequate surgical care includes both stabilization and decompression, it is difficult to determine whether early stabilization or decompression is mainly responsible for neurological improvements. Therefore, both stabilization and decompression must be taken together and are summarized under the term “early spinal cord surgical treatment” in this study.
The results of our work showed no relevant differences between neurological improvement and early or late surgery. Both groups showed a slight improvement in AIS grades but no significant differences between groups could be detected.
Patients who were admitted with an AIS-D injury are unlikely to regain 100% neurological function due to slight neurological impairment from which most of them will always suffer. AIS-A patients also rarely showed neurological improvement as a consequence of the severity of the injury. In our patient pool, only 16.7% of AIS-A and none of AIS-D showed neurological improvement.
The main strengths of this study were the patient heterogeneity and an almost exact determination of the date of accident and surgery. Furthermore, a follow-up after 6 months was consistently carried out.
In order to compare our study with other literature, we have chosen two different points of time of surgery in our prospective study, one within the first 4 hours and the other between 4 and 24 hours after the accident. All patients were treated only in our clinic during the course of the study. Neurological monitoring and control were carried out through use of the AIS classification.
In comparing the rate of improvement of the AIS grade in our study with other studies, we could show that our results clearly have a better outcome measured in terms of AIS (44.8% in G1 and 36.4% in G2). Fawcett et al, for example, observed a neurological improvement of 15%–25% in patients.24
Our observations did not reveal a significant difference in neurological outcome between the two groups despite the fastest possible surgical decompression and stabilization of the fractured spine segments. According to our findings, we conclude that early operative care within the first 4 hours after trauma does not lead to a significant neurological benefit compared to intervention between 4 and 24 hours after trauma.
Limitations
One limitation of our study is its small sample size. Results could be biased because characteristics of SCI are different among the levels and the levels of injury have not been stratified yet. Furthermore, slight changes in neurological recovery may not be revealed by the AIS grade alone. In future studies, the ASIA motor and sensory scoring system, for example, can be used to detect possible slight differences.
Conclusion
In recent years, quick surgical decompression of the spinal canal and associated neurological remission have been discussed and reported repeatedly. Unfortunately, results and opinions differ too widely to give appropriate recommendations. In our patient pool, we were able to show some evidence that surgery within the first 4 hours after trauma does not lead to better neurological outcome compared to surgery between 4 and 24 hours after trauma. This leads to the conclusion that decompression should be performed soon, but not necessarily within the first few hours after injury.
Acknowledgment
The presented results are part of doctoral theses of Cambiz Firuzabadi and Christopher Child.
Disclosure
The authors report no conflicts of interest in this work.
References
DeVivo MJ. Causes and costs of spinal cord injury in the United States. Spinal Cord. 1997;35(12):809–813. | ||
Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord. 2006;44(9):523–529. | ||
Bracken MB. Steroids for acute spinal cord injury. Cochrane Database Syst Rev. 2012;1:Cd001046. | ||
Hurlbert RJ, Moulton R. Why do you prescribe methylprednisolone for acute spinal cord injury? A Canadian perspective and a position statement. Can J Neurol Sci. 2002;29(3):236–239. | ||
Fehlings MG, Wilson JR, Cho N. Methylprednisolone for the treatment of acute spinal cord injury: counterpoint. Neurosurgery. 2014;61(Suppl 1):36–42. | ||
Fehlings MG, Tighe A. Spinal cord injury: the promise of translational research. Neurosurg Focus. 2008;25(5):E1. | ||
Mortazavi MM, Verma K, Harmon OA, et al. The microanatomy of spinal cord injury: a review. Clin Anat. 2015;28(1):27–36. | ||
Bareyre FM, Schwab ME. Inflammation, degeneration and regeneration in the injured spinal cord: insights from DNA microarrays. Trends Neurosci. 2003;26(10):555–563. | ||
Batchelor PE, Wills TE, Skeers P, et al. Meta-analysis of pre-clinical studies of early decompression in acute spinal cord injury: a battle of time and pressure. PloS One. 2013;8(8):e72659. | ||
Fehlings MG, Vaccaro A, Wilson JR, et al. Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PloS One. 2012;7(2):e32037. | ||
Furlan JC, Noonan V, Cadotte DW, Fehlings MG. Timing of decompressive surgery of spinal cord after traumatic spinal cord injury: an evidence-based examination of pre-clinical and clinical studies. J Neurotrauma. 2011;28(8):1371–1399. | ||
La Rosa G, Conti A, Cardali S, Cacciola F, Tomasello F. Does early decompression improve neurological outcome of spinal cord injured patients? Appraisal of the literature using a meta-analytical approach. Spinal Cord. 2004;42(9):503–512. | ||
Young W. NASCIS. National Acute Spinal Cord Injury Study. J Neurotrauma. 1990;7(3):113–114. | ||
Levi L, Wolf A, Rigamonti D, Ragheb J, Mirvis S, Robinson WL. Anterior decompression in cervical spine trauma: does the timing of surgery affect the outcome? Neurosurgery. 1991;29(2):216–222. | ||
Mirza SK, Krengel WF 3rd, Chapman JR, et al. Early versus delayed surgery for acute cervical spinal cord injury. Clin Orthop Relat Res. 1999;(359):104–114. | ||
Duh MS, Shepard MJ, Wilberger JE, Bracken MB. The effectiveness of surgery on the treatment of acute spinal cord injury and its relation to pharmacological treatment. Neurosurgery. 1994;35(2):240–248. | ||
Chen L, Yang H, Yang T, Xu Y, Bao Z, Tang T. Effectiveness of surgical treatment for traumatic central cord syndrome. J Neurosurg Spine. 2009;10(1):3–8. | ||
Croce MA, Bee TK, Pritchard E, Miller PR, Fabian TC. Does optimal timing for spine fracture fixation exist? Ann Surg. 2001;233(6):851–858. | ||
Vaccaro AR, Daugherty RJ, Sheehan TP, et al. Neurologic outcome of early versus late surgery for cervical spinal cord injury. Spine. 1997;22(22):2609–2613. | ||
Guest J, Eleraky MA, Apostolides PJ, Dickman CA, Sonntag VK. Traumatic central cord syndrome: results of surgical management. J Neurosurg. 2002;97(1 Suppl):25–32. | ||
McKinley W, Meade MA, Kirshblum S, Barnard B. Outcomes of early surgical management versus late or no surgical intervention after acute spinal cord injury. Arch Phys Med Rehabil. 2004;85(11):1818–1825. | ||
Cengiz SL, Kalkan E, Bayir A, Ilik K, Basefer A. Timing of thoracolomber spine stabilization in trauma patients; impact on neurological outcome and clinical course. A real prospective (rct) randomized controlled study. Arch Orthop Trauma Surg. 2008;128(9):959–966. | ||
Gupta DK, Vaghani G, Siddiqui S, et al. Early versus delayed decompression in acute subaxial cervical spinal cord injury: a prospective outcome study at a Level I trauma center from India. Asian J Neurosurg. 2015;10(3):158–165. | ||
Fawcett JW, Curt A, Steeves JD, et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord. 2007;45(3):190–205. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.