Back to Journals » Psychology Research and Behavior Management » Volume 14
Does Psychological Capital Mediate Between Workplace Violence and Depressive Symptoms Among Doctors and Nurses in Chinese General Hospitals?
Received 25 November 2020
Accepted for publication 19 January 2021
Published 19 February 2021 Volume 2021:14 Pages 199—206
DOI https://doi.org/10.2147/PRBM.S293843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xiaomeng Li,1,2 Huazhang Wu1
1Department of Health Service Management, China Medical University, Shenyang, Liaoning, 110122, People’s Republic of China; 2Liaoning Academy of Social Sciences, Shenyang, Liaoning, 110032, People’s Republic of China
Correspondence: Huazhang Wu Tel +86-13694129862
Email [email protected]
Background: Depressive symptoms related to workplace violence (WPV) have been studied and are the main causes of lower psychological and physical well-being and work motivation. Our study aims to examine the prevalence of depressive symptoms and to explore whether psychological capital (PsyCap) mediates the effect of WPV on depressive symptoms in doctors and nurses.
Methods: Participants were recruited from general hospitals in Liaoning, China in 2018. Out of 1218 participants, 1062 (87.2%) completed self-reported questionnaires. Depressive symptoms, WPV and PsyCap were measured by Epidemiologic Studies Depression Scale (CES-D), Workplace Violence Scale (WVS) and Psychological Capital Questionnaire (PCQ), respectively. The related factors of depressive symptoms were investigated by using hierarchical multiple regression in both doctors and nurses.
Results: The mean scores of depressive symptoms were 23.09 ± 8.38 in doctors and 22.33 ± 8.95 in nurses, and there was no significant difference between the scores of these two groups. WPV was positively associated with depressive symptoms (doctors: β=0.349, P< 0.001; nurses: β=0.317, P< 0.001) while PsyCap was negatively associated with depressive symptoms (doctors: β=− 0.101, P< 0.001; nurses: β=− 0.230, P< 0.001). In addition, PsyCap acted as a mediating role between WPV and depressive symptoms in both doctors and nurses.
Conclusion: Both doctors and nurses had serious depressive symptoms. WPV could aggravate depressive symptoms, while PsyCap could aggravate against depressive symptoms. When PsyCap acted as a mediator, WPV had a negative impact on PsyCap, which could increase doctors’ and nurses’ depressive symptoms.
Keywords: doctors, nurses, workplace violence, depressive symptoms, psychological capital
Introduction
Workplace violence (WPV) has been in the limelight all walks of life, particularly, health care settings. WHO reported that there were 8–38% of medical personnel who have suffered from workplace violence including verbal abuse, threat and physical violence in 2017.1 In China, WPV is common in healthcare sectors, and a previous study indicated that more than half of doctors and nurses have been the victims of WPV in medical sectors.2 WPV has an adverse impact on the psychological and physical well-being of medical personnel,3,4 and decreases doctors' and nurses’ job motivation,5,6 which is unacceptable. Consequently, this violence places medical staff at risk and compromises the quality of medical service, which causes enormous medical resources loss in the healthcare settings.
WPV is defined as the psychological and physical harm that doctors and nurses often are confronted with when providing medical service.7,8 WPV consists of threat, physical assault, verbal sexual harassment, emotional abuse and sexual assault. Several studies have indicated that WPV significantly and negatively affected medical staff’s mental health, and even led to serious mental illnesses like depressive symptoms.9,10 One study found that 36.3% of medical personnel who had suffered from WPV in hospital reported mild to moderate depressive symptoms, and 16% presented probable major depressive symptoms.4 Besides, depressive symptoms have an adverse effect on psychological and physical well-being, work performance and job satisfaction, which leads to negative attitudes towards performing medical services. From a long-term point of view, this environment can result in the immense loss of medical human resources, and the serious decline of the quality of health service.11 It was reported that nurses were at higher risk of being exposed to WPV than doctors in general hospitals.9 Therefore, our study hypothesized nurses would be more vulnerable to suffer from mental problems than doctors, and examined the impact of WPV on depressive symptoms among doctors and nurses in Chinese general hospitals.
Psychological capital (PsyCap) has been reported as a protective factor for mental illness like depressive symptoms.12,13 PsyCap exhibits a positive state of mind in the process of individual growth and development.14 PsyCap includes four core elements, namely, resilience, self-efficacy, hope and optimism.15 These four elements are defined as important capacities to combat negative emotions and burnouts in the occupational population when they are confronted with difficulties and challenges. According to the theory of systemic assessment of depressive symptoms among registered nurses (SAD-RN),12 Ross et al proposed that when the nurses perceive stressors (eg, WPV), those who do not possess positive belief and resources (eg, PsyCap) may fail to deal with negative responses caused by stressors and are more likely to develop depressive symptoms. This suggests that PsyCap may relieve the adverse effect of WPV on depressive symptoms in health care workers. In addition, other studies found that PsyCap could mediate and moderate the effect of work-family conflict on depressive symptoms in Chinese female nurses.13 In other words, it was believed that PsyCap may be a mediating factor between WPV and depressive symptoms in doctors and nurses.
Therefore, the aims of this study were to 1) examine the prevalence of depressive symptoms and to evaluate its related factors in doctors and nurses, respectively, 2) explore the effect of WPV on depressive symptoms, 3) explore the association of PsyCap and depressive symptoms, and whether psychological capital mediates the effect of WPV on depressive symptoms.
Methods
Design and Procedures
This cross-sectional survey was conducted from June to October of 2018 in Liaoning province, China. Random sampling method was applied in our study. According to the geographical distribution, our study randomly selected three cities in Liaoning province, and two general hospitals were randomly selected from each city. The inclusion criteria are that the doctors or nurses should have worked over one year in the general hospitals. After writing the informed consent, each subject would receive a self-administered questionnaire and the study complied with the declaration of Helsinki. The questionnaires were sent to 744 doctors and 474 nurses, and 644 (86.6%) doctors and 418 (88.2%) nurses were selected as the final subjects.
Measurement of Depressive Symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D) was used to measure depressive symptoms among doctors and nurses in this study.16 This scale has 20 items, and each item was applied with a 4-point Likert scale from 0 (rarely) to 3 (most or all of the time). The total score of this scale is 0–60, with a higher score indicating severer depressive symptoms. Participants who had 16–19 CES-D score were defined as “mild to moderate depressive symptoms” group, and >19 means “possibility of major depression” group.16 The CES-D scale has been widely used among medical staff in Chinese hospitals.17 The Cronbach’s alpha coefficient for CES-D was 0.872 (doctors: 0.870, nurses: 0.875) in this study.
Measurement of Workplace Violence
The frequency of WPV experienced by doctors and nurses was assessed by using the Chinese version of workplace violence scale (WVS).18 The Chinese version of WVS was originated from Schat version and developed by Wang.19 The WVS includes five dimensions: verbal sexual harassment, emotional abuse, physical assault, threat, and sexual assault, and each dimension includes one item. Each item uses a 4-point Likert scale from 0 (never) to 3 (≥4 times). The total score of this scale is 0–15, and a higher score indicates a higher frequency of experiencing workplace violence. Several studies that employed this scale have been reported to have good validity and reliability in the occupational population.20 The internal reliability for WVS was 0.942 (doctors: 0.945, nurses: 0.934) in this study.
Measurement of Psychological Capital
The level of PsyCap was measured with the Chinese version of the Psychological Capital Questionnaire (PCQ).21 This scale consists of 24-item and has four core elements, including resilience optimism self-efficacy and hope.22 Each element has six items, and each item uses a 6-point Likert scale from 1 (strongly disagree) to 6 (strongly agree). This scale has been proved to show good reliability and construct validity in Chinese occupational population.23,24 The internal reliability coefficient for this scale was 0.943 (doctors: 0.936, nurses: 0.952) in the present study.
Besides, this study included six demographic variables which are marital status, gender, monthly income, weekly working time (hrs), education, and the number of exercises practiced weekly. Gender was categorized as male and female. Marital status included divorced/widowed/separated, unmarried and married/cohabitation. Weekly working time (hrs) was classified as <40 and ≥40. Monthly income (RMB) comprised <3000, 3000–5000 and ≥5000. Education background contained junior college or lower, bachelor college and master college or higher. The number of exercises weekly was classified as 0, 1, 2–3 and ≥4.
Statistical Analysis
The data were analyzed using SPSS statistical package version 20.0. One-way ANOVAs or T-tests were used to test the distribution of dimensions of depressive symptoms in demographic variables. Also, depressive symptom differences between doctors and nurses were examined by T-tests. Correlation coefficients among depressive symptoms, WPV and PsyCap were examined by Pearson’s correlation. Hierarchical multiple regression analysis was used to explore related influencing factors of depressive symptoms. Besides age and gender, other demographic variables that were associated with depressive symptoms in univariate analysis (P<0.05) were entered in the regression model. In step 1, age, gender, weekly work time and number of exercises weekly were added; in step 2, WPV was entered; in step 3, PsyCap was added. There was a partially mediating effect of PsyCap on the association between WPV and depressive symptoms if the regression coefficient (β) of WPV in step 3 was smaller than that in step 2 with P < 0.05.25 PsyCap completely mediated the impact of WPV on depressive symptoms if the regression coefficient (β) of WPV in step 3 was smaller than that in step 2 with P > 0.05.25
Two-tail P < 0.05 was defined as statistically significant in this study.
Results
Demographic Characteristics
Table 1 shows the demographics of doctors and nurses, and the distributions of depressive symptoms. In this study, 644 doctors and 418 nurses participated. The mean age was 33.38 (8.58) and 33.48 (9.35) for doctors and nurses, respectively. More than half of doctors were male. About 73.8% of doctors and 67.0% of nurses were married or cohabited. Approximately half of doctors and nurses hold a bachelor's degree. More than half of doctors' and nurses’ monthly income were between 3000 and 5000 (RMB). Weekly work time and the number of exercise practices weekly were related to depressive symptoms in doctors (P<0.05), and a number of exercises weekly were associated with depressive symptoms in nurses (P<0.05).
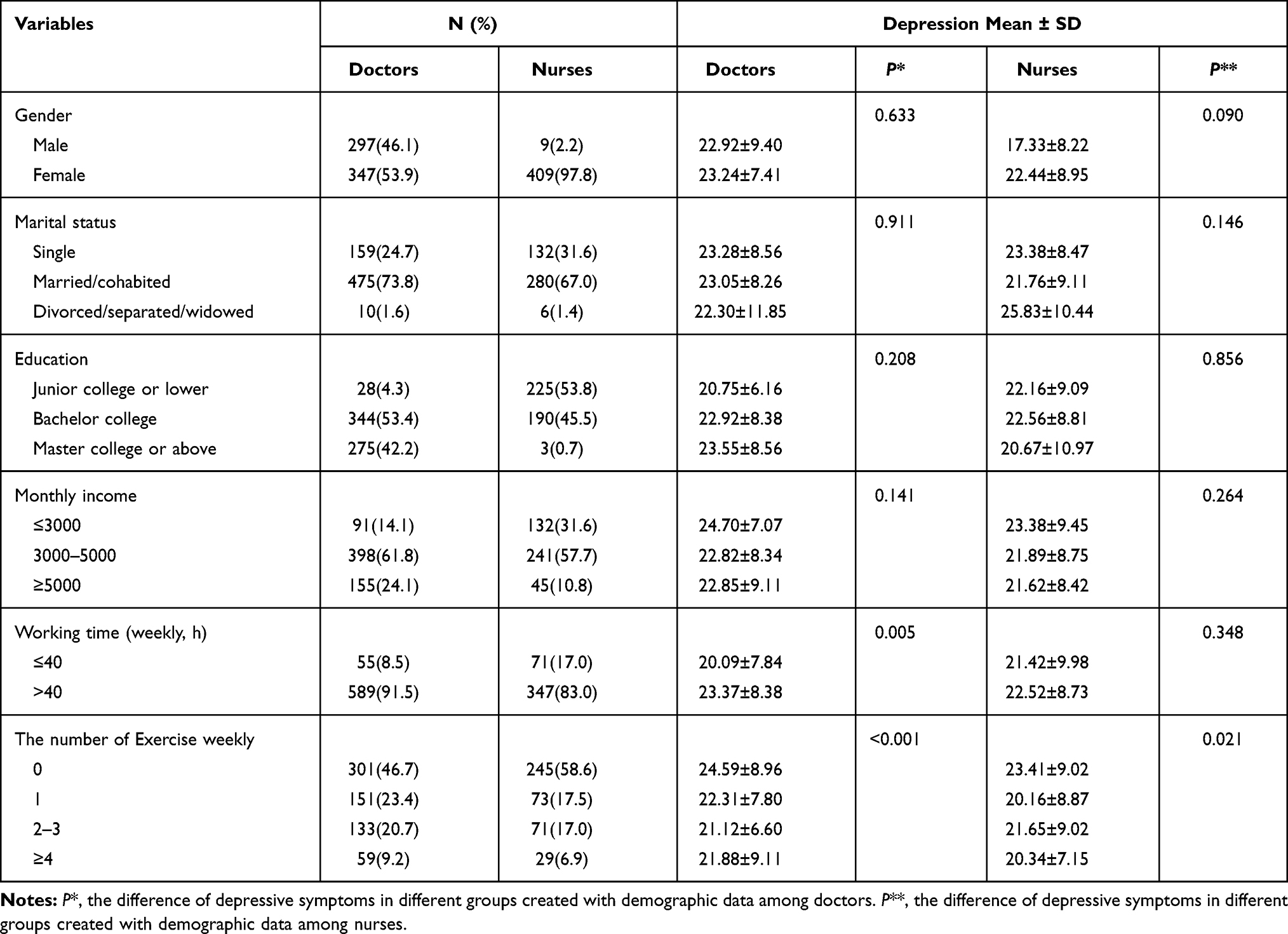 |
Table 1 Demographic Characteristics of Participants and Results of Univariate Analysis |
Correlations Between Study Variables
Table 2 presents the correlation between depressive symptoms, WPV, and PsyCap. WPV was positively associated with depressive symptoms for both doctors (r = 0.346, P<0.01) and nurses (r=0.362, P<0.01), whereas PsyCap was negatively associated with depressive symptoms both doctors (r=−0.166, P<0.01) and nurses (r=−0.299, P<0.01).
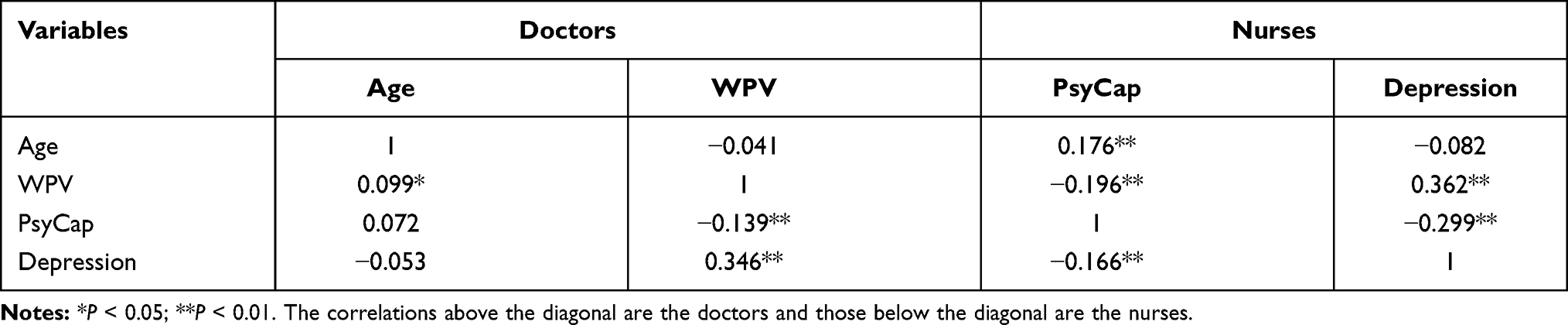 |
Table 2 Correlations Analysis Between WPV, PsyCap and Depression Among Doctors and Nurses |
Comparison of Depressive Symptoms Between Doctors and Nurses
Table 3 reports a comparison of depressive symptoms between doctors and nurses. The mean scores of depressive symptoms were 23.09 ± 8.38 for doctors and 22.33 ± 8.95 for nurses. In total, 530 (mild to moderate depressive symptoms: 14.6%; major depressive symptoms: 66.7%) doctors and 336 (mild to moderate depressive symptoms: 14.1%; major depressive symptoms: 66.3%) nurses had shown depressive symptoms. Also, the numbers did not show the difference in depressive symptoms between doctors and nurses (P>0.05).
 |
Table 3 Difference of Doctors and Nurses on Depressive Symptoms |
Hierarchical Regression Analysis
Table 4 shows that the results of hierarchical multiple regression in doctors. After controlling demographic variables, WPV was positively associated with depressive symptoms (β=0.364, P<0.001) in step 2. PsyCap was negatively associated with depressive symptoms (β=−0.101, P<0.001) in step 3 while the effect of WPV on depressive symptoms (β=0.349, P<0.001) was smaller compared with that in step 2, which indicated that WPV could become a partial mediator on the association of WPV with depressive symptoms.
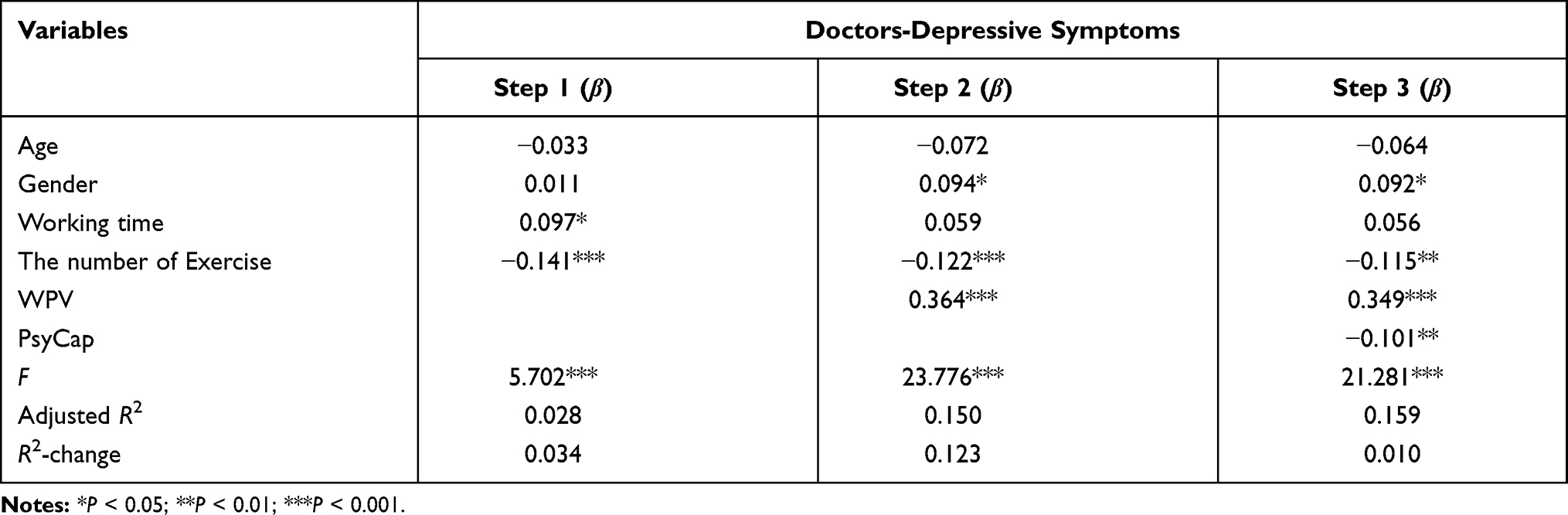 |
Table 4 The Linear Regression Analysis Among Doctors |
Table 5 shows that the results of hierarchical multiple regression in nurses. WPV was positively associated with depressive symptoms (β=0.359, P<0.001) in step 2 after controlling those two demographic variables. PsyCap was negatively associated with depressive symptoms (β=−0.230, P<0.001) in step 3, but the effect of WPV on depressive symptoms (β=0.317, P<0.001) was smaller compared with that in step 3. Thus, PsyCap may mediate the effect of WPV on depressive symptoms in nurses.
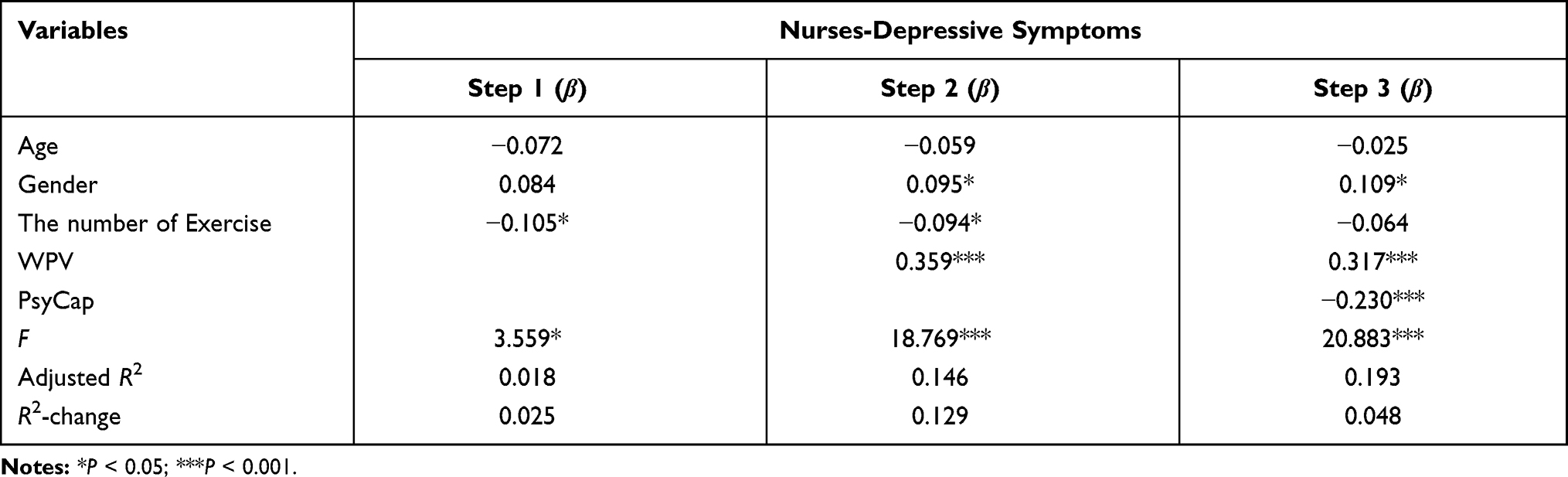 |
Table 5 The Linear Regression Analysis Among Nurses |
Discussion
The results from this study did not show a significant difference between doctors (mild to moderate depressive symptoms: 14.6%; major depressive symptoms: 66.7%) and nurses (mild to moderate depressive symptoms: 14.1%; major depressive symptoms: 66.3%) on depressive symptoms, which failed to support our hypothesis (nurses would be more vulnerable to suffer from mental problems than doctors). One of the reasons could be that although both doctors and nurses are medical staff, doctors tend to suffer from a higher level of stress because their work is more directly correlated with patients’ health.13,26 In practice, doctors take more responsibility for the right diagnosis, proper prescription and effective operation; thus, they need to learn the latest medical knowledge and sophisticated medical technologies, and to spend more time communicating with patients and studying their diseases. However, these results were significantly higher than the rates in previous studies which studied approximately 45.3% to 47.2% of healthcare personnel in China.27,28 In addition, Da Silva et al reported that medical staff in primary care had 52.3% (intermediate depressive symptoms: 36.3%; major depressive symptoms: 16%) depressive symptoms in Brazil.4 Therefore, we can still conclude that doctors and nurses in Chinese general hospitals are suffering from serious mental problems, and our next priority is to find out the influencing factors of mental health in medical staff.
Our results suggested that WPV was positively correlated with depressive symptoms, which were similar to the previous findings.29–31 In other words, doctors and nurses who suffered from WPV were more likely to develop depressive symptoms, because they confront with violent situations more often, from which they may feel being treated disrespectfully about their dedications and professional knowledge; hence, depressive symptoms may be triggered. Besides, these violent environments would result in heavy stress and burnout.32–34 Norman et al reported that individuals who suffered WPV would be vulnerable to negative emotions such as fear, anger, and irritability.35 In addition, another study confirmed that WPV was positively associated with depressive symptoms.36 In nature, the occurrence of WPV may affect the mental and physical health of doctors and nurses and impair their professional performance, which results in a negative impact on patient’s health, eventually.11,37,38 Therefore, it is time to carry out intervention strategies to prevent violent incidents in healthcare settings; for non-emergency medical settings, interventions to prevent violence against health workers should focus on better managing violent patients and high-risk visitors; for emergency medical settings, interventions should focus on ensuring the physical security of health-care facilities.
Doctors and nurses suffering from WPV may feel angrier and more fearful than they usually do, so they need resources to cope with the negative emotions. Coping resources from individuals include self-efficacy, hope, resilience and optimism, which are called PsyCap for releasing WPV-related stress. In our study, we found that PsyCap could mediate the association between WPV and depressive symptoms among medical staff. Namely, psychological capital were protective factors against developing depressive symptoms for assaulted doctors and nurses in Chinese general hospitals. Psychological capital could effectively prevent the development of depressive symptoms, or decrease its adverse impact on mental health. The previous survey has conformed these findings.39,40 Increasingly studies presented that individuals who possessed higher PsyCap may have more self-confidence to achieve the pre-set goals, to bravely embrace difficulties, and to take a positive attitude towards adversity or personal setbacks.41–43 Hao et al reported a similar finding that PsyCap could attenuate the adverse impact of negative factors on depressive symptoms in medical staff.13 Given the characteristics of PsyCap that it can be effectively developed and managed, intervention strategies concerning PsyCap should be carried out to increase the level of PsyCap in both doctors and nurses to prevent depressive symptoms.
However, there are some limitations in this study. Firstly, a cross-sectional design was employed in this study, which cannot draw causal conclusions between theses variables. Therefore, casual relationships should be confirmed by Longitudinal studies in the future. Secondly, self-reported questionnaires were used to collect data in the present study. Thus, recall bias could have been introduced. Finally, although this study examined the relationships between WPV, PsyCap, and depressive symptoms, some important information was not collected in this study, including the number of children and the elderly, and spouse occupation, which might influence the results. Therefore, these possible risk factors should be taken into account in further studies.
Conclusion
Our findings revealed that both doctors and nurses had serious depressive symptoms, and more than half of them had suffered from WPV, including verbal sexual harassment or physical assault. WPV was positively associated with depressive symptoms, while PsyCap was protective factors against developing depressive symptoms. Besides, PsyCap could mediate the effect of WPV on depressive symptoms among both doctors and nurses. In other words, doctors and nurses with high levels of psychological capital are adaptable to changing demands and demonstrate emotional stability when faced with WPV. Therefore, a safer work environment and psychological capital development based on resilience, hope, self-efficacy and optimism may be considered in prevention and treatment strategies for reducing depressive symptoms.
Ethical Approval
The study was approved by the Ethics Committee on Human Experimentation of China Medical University and complied with the Declaration of Helsinki.
Acknowledgments
All authors would like to gratitude the research fellows who participated in data collection, management and analysis of the study. All authors read and approved the final manuscript.
Funding
There was no funding support.
Disclosure
All authors declared that there are no conflicts of interest in this work.
References
1. WHO. Violence against health workers. Available from: http://www.who.int/violence_injury_prevention/violence/workplace/en/.
2. Chen ZH, Wang SY. Psychiatric hospital and general hospital workplace violence study comparison. Chin Public Health. 2004;20:40–41.
3. Hegney D, Eley R, Plank A, Buikstra E, Parker V. Workplace violence in Queensland, Australia: the results of a comparative study. Int J Nurs Pract. 2006;12(4):220–231. doi:10.1111/j.1440-172X.2006.00571.x
4. Da Silva AT, Peres MF, Lopes CS, et al. Violence at work and depressive symptoms in primary health care teams: a cross-sectional study in Brazil. Soc Psychiatry Psychiatr. 2015;50:1347–1355.
5. Zhao S, Liu H, Ma H, et al. Coping with workplace violence in healthcare settings: social support and strategies. Int J Environ Res Public Health. 2015;12(11):14429–14444. doi:10.3390/ijerph121114429
6. Farrell GA, Bobrowski C, Bobrowski P. Scoping workplace aggression in nursing: findings from an Australian study. J Adv Nurs. 2006;55(6):778–787. doi:10.1111/j.1365-2648.2006.03956.x
7. ILO, WHO. Framework Guidelines for Addressing Workplace Violence in the Health Sector. Geneva, Switzerland: International Labour Office; 2002.
8. Simpson KR. Incivility, bullying, and workplace violence: new recommendations for nurses and their employers from the American nurses association. MCN Am J Matern Child Nurs. 2016;41(1):68. doi:10.1097/NMC.0000000000000206
9. Ferri P, Silvestri M, Artoni C, et al. Workplace violence in different settings and among various health professionals in an Italian general hospital: a cross-sectional study. Psychol Res Behav Manag. 2016;9:263–275. doi:10.2147/PRBM.S114870
10. Zhao S, Qu L, Liu H, et al. Coping with workplace violence against general practitioners and nurses in heilongjiang province, china: social supports and prevention strategies. PLoS One. 2016;(2016)(11):e0157897. doi:10.1371/journal.pone.0157897
11. Fang H, Zhao X, Yang H, et al. Depressive symptoms and workplace-violence-related risk factors among otorhinolaryngology nurses and physicians in Northern China: a cross-sectional study. BMJ Open. 2018;8(1):e019514. doi:10.1136/bmjopen-2017-019514
12. Ross R, Letvak S, Sheppard F, Jenkins M, Almotairy M. Systemic assessment of depressive symptoms among registered nurses: a new situation-specific theory. Nurs Outlook. 2020;68(2):207–219. doi:10.1016/j.outlook.2019.08.007
13. Hao J, Wu D, Liu L, et al. Association between work-family conflict and depressive symptoms among Chinese female nurses: the mediating and moderating role of psychological capital. Int J Environ Res Public Health. 2015;12(6):6682–6699. doi:10.3390/ijerph120606682
14. Luthans F, Youssef-Morgan CM, Avolio BJ. Psychological capital: developing the human competitive edge. J Asian Econ. 2007;8:315–332.
15. Youssef-Morgan CM, Luthans F. Psychological capital and well-being. Stress Health. 2015;31(3):180–188. doi:10.1002/smi.2623
16. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
17. Yang L, Jia CX, Qin P. Reliability and validity of the center for epidemiologic studies depression scale (CES-D) among suicide attempters and comparison residents in rural China. BMC Psychiatry. 2015;15(1):76. doi:10.1186/s12888-015-0458-1
18. Wang PX, Wang MZ, Bai Q, et al. Path analysis on workplace violence affecting work ability, job satisfaction and turnover intent in health professionals in Shangqiu City. J Hyg Res. 2006;35:785–788.
19. Schat AC, Kelloway EK. Reducing the adverse consequences of workplace aggression and violence: the buffering effects of organizational support. J Occup Health Psychol. 2003;8(2):110–122. doi:10.1037/1076-8998.8.2.110
20. Lin WQ, Wu J, Yuan LX, et al. Workplace violence and job performance among community healthcare workers in china: the mediator role of quality of life. Int J Environ Res Public Health. 2015;12:14872–14886. doi:10.3390/ijerph121114872
21. Luthans F, Avolio BJ, Avey JB, Norman SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. 2007;60(3):541–572. doi:10.1111/j.1744-6570.2007.00083.x
22. Luthans F, Norman SM, Avolio BJ, Avey JB. The mediating role of psychological capital in the supportive organizational climate-employee performance relationship. J Organ Behav. 2008;29(2):219–238. doi:10.1002/job.507
23. Li X, Kan D, Liu L, et al. The mediating role of psychological capital on the association between occupational stress and job burnout among bank employees in China. Int J Environ Res Public Health. 2015;12(3):2984–3001. doi:10.3390/ijerph120302984
24. Peng J, Jiang X, Zhang J, et al. The impact of psychological capital on job burnout of Chinese nurses: the mediator role of organizational commitment. PLoS One. 2013;8(12):e84193. doi:10.1371/journal.pone.0084193
25. Wen ZL, Zhang L, Hou JT, Liu HY. The procedure of mediating effect test and its application. Acta Psychol Sin. 2004;36(5):614–620.
26. Steiner-Hofbauer V, Schrank B, Holzinger A. What is a good doctor? Wien Med Wochenschr. 2018;168(15–16):398–405. doi:10.1007/s10354-017-0597-8
27. Yang X, Hu S. Related study between social support and coping style, and anxiety and depression of nurse. Chin J Health Psychol. 2011;19:300–301.
28. Ji Y, He L, He L, Hao J, Kuang G. Correlation study of occupational stress and mental health among medical staff. Occup Health. 2015;31:3393–3395.
29. Jung PK, Won JU, Roh J, et al. Workplace violence experienced by substitute (daeri) drivers and its relationship to depression in Korea. J Korean Med Sci. 2015;30(12):1748–1753. doi:10.3346/jkms.2015.30.12.1748
30. Kelly EL, Subica AM, Fulginiti A, et al. A cross-sectional survey of factors related to inpatient assault of staff in a forensic psychiatric hospital. J Adv Nurs. 2015;71(5):1110–1122. doi:10.1111/jan.12609
31. Hsieh H, Wang H, Shen S, Li Y-C. Predictors of depressive symptoms among psychiatric nurses who suffered from workplace violence. J Adv Nurs. 2017;74(1):425–432. doi:10.1111/jan.13451
32. Laeeque SH, Bilal A, Babar S, et al. How patient-perpetrated workplace violence leads to turnover intention among nurses: the mediating mechanism of occupational stress and burnout. J Aggress Maltreat Trauma. 2018;27(1):96–118. doi:10.1080/10926771.2017.1410751
33. Itzhaki M, Bluvstein I, Bortz AP, et al. Mental health nurse’s exposure to workplace violence leads to job stress, which leads to reduced professional quality of life. Front Psychol. 2018;9. doi:10.3389/fpsyt.2018.00059
34. Duan X, Ni X, Shi L, et al. The impact of workplace violence on job satisfaction, job burnout, and turnover intention: the mediating role of social support. Health Qual Life Outcomes. 2019;17(1). doi:10.1186/s12955-019-1164-3.
35. Norman ID, Aikins M, Binka FN. Faith-based organizations: sexual harassment and health in accra-tema metropolis. Sex Cult. 2013;17(1):100–112. doi:10.1007/s12119-012-9141-6
36. Street AE, Gradus JL, Stafford J, Kelly K. Gender differences in experiences of sexual harassment: data from a male-dominated environment. J Consult Clin Psychol. 2007;75(3):464–474. doi:10.1037/0022-006X.75.3.464
37. Mento C, Catena SM, Bruno A, et al. Workplace violence against healthcare professionals: a systematic review. Aggress Violent Behav. 2020;51:1–8. doi:10.1016/j.avb.2020.101381
38. Gillespie GL, Gates DM, Miller M, et al. Workplace violence in healthcare settings. Work. 2015;51(1):3–4. doi:10.3233/WOR-152017
39. Liu L, Chang Y, Fu J, et al. The mediating role of psychological capital on the association between occupational stress and depressive symptoms among Chinese physicians: a cross-sectional study. BMC Public Health. 2012;12(1):219–226. doi:10.1186/1471-2458-12-219
40. Bakker DJ, Lyons ST, Conlon PD. An exploration of the relationship between psychological capital and depression among first-year doctor of veterinary medicine students. J Vet Med Educ. 2017;44(1):50–62. doi:10.3138/jvme.0116-006R
41. Wang Z, Liu H, Yu H, Wu Y, Chang S, Wang L. Associations between occupational stress, burnout and well-being among manufacturing workers: mediating roles of psychological capital and self-esteem. BMC Psychiatry. 2017;17(1):1–10. doi:10.1186/s12888-017-1533-6
42. Liu L, Pang R, Sun W, et al. Functional social support, psychological capital, and depressive and anxiety symptoms among people living with HIV/AIDS employed fulltime. BMC Psychiatry. 2013;13.
43. Tan-Kristanto S, Kiropoulos LA. Resilience, self-efficacy, coping styles and depressive and anxiety symptoms in those newly diagnosed with multiple sclerosis. Psychol Health Med. 2015;20(6):635–645. doi:10.1080/13548506.2014.999810
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.