Back to Journals » Patient Preference and Adherence » Volume 11
Does information form matter when giving tailored risk information to patients in clinical settings? A review of patients’ preferences and responses
Authors Harris R, Noble C, Lowers V
Received 24 October 2016
Accepted for publication 20 December 2016
Published 1 March 2017 Volume 2017:11 Pages 389—400
DOI https://doi.org/10.2147/PPA.S125613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Rebecca Harris, Claire Noble, Victoria Lowers
Institute of Psychology, Health and Society, University of Liverpool, Liverpool, UK
Abstract: Neoliberal emphasis on “responsibility” has colonized many aspects of public life, including how health care is provided. Clinical risk assessment of patients based on a range of data concerned with lifestyle, behavior, and health status has assumed a growing importance in many health systems. It is a mechanism whereby responsibility for self (preventive) care can be shifted to patients, provided that risk assessment data is communicated to patients in a way which is engaging and motivates change. This study aimed to look at whether the form in which tailored risk information was presented in a clinical setting (for example, using photographs, online data, diagrams etc.), was associated with differences in patients’ responses and preferences to the material presented. We undertook a systematic review using electronic searching of nine databases, along with handsearching specialist journals and backward and forward citation searching. We identified eleven studies (eight with a randomized controlled trial design). Seven studies involved the use of computerized health risk assessments in primary care. Beneficial effects were relatively modest, even in studies merely aiming to enhance patient–clinician communication or to modify patients’ risk perceptions. In our paper, we discuss the apparent importance of the accompanying discourse between patient and clinician, which appears to be necessary in order to impart meaning to information on “risk,” irrespective of whether the material is personalized, or even presented in a vivid way. Thus, while expanding computer technologies might be able to generate a highly personalized account of patients’ risk in a time efficient way, the need for face-to-face interactions to impart meaning to the data means that these new technologies cannot fully address the resource issues attendant with this type of approach.
Keywords: risk, patient communication, personalisation, information, behavior change, health education
Introduction
Risk communication is something that most clinicians do every day.1 This is because, first, patients’ risk perception (belief about the likelihood of personal harm from a behavior), and how this balances with benefits, lies at the heart of helping patients make informed choices between treatment options and, second, because self-care and self-management behavior is underpinned by how patients perceive threats to their health.2,3 Risk communication is also the concern of public health practitioners, where it is seen as crucial to the prevention and cooperative management of health risks, and “at least equally essential to outbreak control as epidemiological training and laboratory analysis”.4 Literature on health risk communication is, therefore, understandably prolific – embracing a range of disciplines and theories that explore the complexities of how individuals are influenced by such information.4
There is a general consensus that tailoring of information is beneficial,5–7 and so we set aside “mass” programs concerned with risk communication and focus here on communicating individualized information. Individualized health communication can range from personalized generic communication (for example using someone’s name to personalize the message), to targeted communication (composing the message with a particular group or segment of the population in mind – an approach that is the basis of many public health education and social marketing campaigns), through to truly personalized communication that provides information based on characteristics unique to a person (as in brief counseling interventions, for example). These latter approaches involve tailoring based on characteristics beyond broad demographic categories such as age or gender, and therefore depend on some sort of individual assessment; although with the advent of computer-based tailoring, their population reach can still be wide.8,9
A common aim of tailoring used in health education messages is to increase attention and therefore message comprehension – both cognitive preconditions for the processing of information, which lead to a change in behavior.6 It is also thought that tailoring works by way of peripheral or emotional processing; for example, “the sender understands me”; which enhances source credibility and the following of recommendations with little critical analysis.6 Some even argue that patients’ assessment of risk is primarily determined not by facts but by emotions,10 for the more risk information evokes an emotional response, the greater the perceived chance of the threat occurring.11
Studies show that visual displays enhance people’s understanding of risk, particularly holding attention when they are given in a vivid way;12,13 and emotional responses to information portrayed say in pictures or videos influence whether people increase or decrease certain health behaviors.12 So, although much previous attention has been focused on the way risk messages are framed and presented (comparing gain-framed with lost-framed messages and various numerical and graphical formats),1,14 the actual form in which the risk information is presented (verbal, written leaflet with or without diagrams, video, computer, photograph) is an important additional feature that may influence people’s engagement and responses to the material. With current expansion in possibilities of tailored risk communication by means of intelligent interactive systems,15 it is important to consider both patient preferences and their responses to risk information when presented in different forms. Our aim was therefore to undertake a systematic review of patients’ preferences and responses to personally tailored information given in different forms, limiting this to clinical settings (“patient communication”), although the work may inform wider public health education efforts too. After presenting the results of the review, we go on to discuss what this means in modern times where computer and mobile phone capabilities make it possible to issue a wealth of feedback on lifestyle and clinical information to patients against a background where health policies increasingly advocate efficiencies of care delivery and patients’ responsibility for their own health.
Methods
Literature searching was limited to all types of study design, including qualitative work and protocols, concerned with adult patients receiving tailored risk information as part of their care in clinical settings. Intervention studies were only included where the study involved comparing delivery of tailored risk information in one form with either usual care, verbal risk messages, or with a different form of risk information so that a comparison regarding differing information forms could be made (Table 1 shows full inclusion and exclusion criteria). Since studies show that lay concepts of “risk” tend to be more aligned with a dichotomous model of risk presentation (“I am a likely/unlikely candidate for illness”), than a model involving graduations along a probability spectrum (“I am at a 30% higher risk of being ill than someone else of my age”),16 we included studies involving giving tailored information about individuals’ levels of health with reference to likely negative consequences as well as those involving “risk” terminology and health outcome probabilities.
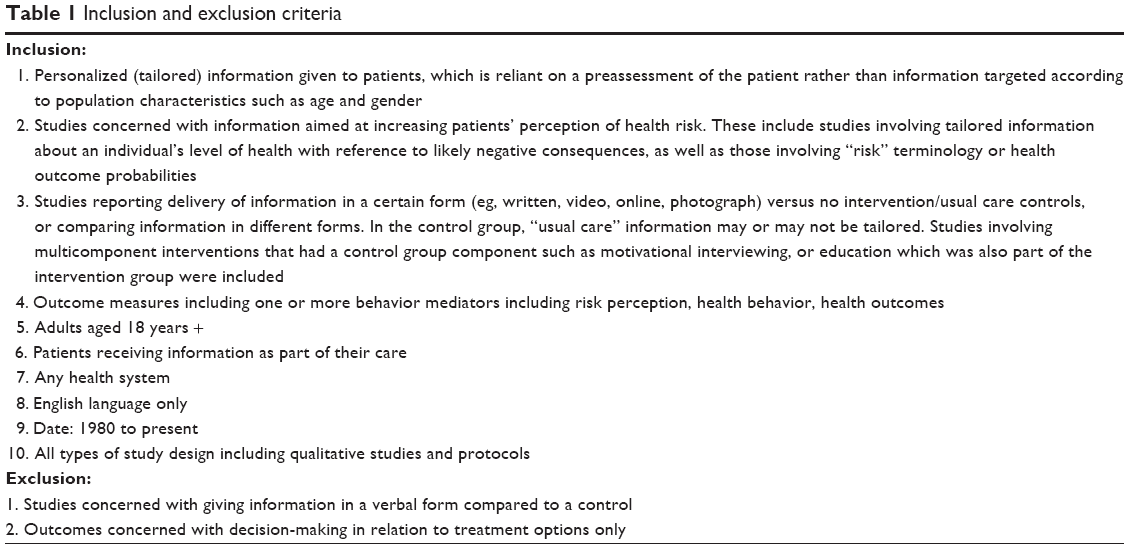 | Table 1 Inclusion and exclusion criteria |
We adopted an iterative search strategy that involved electronic literature searching of nine databases (including gray literature and dissertation databases) and handsearching eight specialist journals (Supplementary material Table S1). To strike a balance between literature search sensitivity (finding all articles in the topic area) and precision (finding only relevant articles), we initially developed electronic search terms using Automatic Term Recognition software (TerMine), applying this to 35 papers previously retrieved through pilot searches undertaken in Google Scholar.17 We then broadened out the search strategy with general topic search terms (eg, health education) as is customary to systematic review methods.18 We also used forward and backward citation searches, that is, reviewing references cited in articles identified earlier in the review process and searching for publications which cited papers that met study inclusion criteria. Quality assessment of included randomized controlled trials (RCTs) was undertaken using Cochrane risk of bias methodology.19
Results
Electronic and handsearching identified 10,682 papers, of which 1,673 were duplicates. A further 100 papers were identified through backward and forward citation chasing. Screening by two independent reviewers identified 624 relevant papers. Full-paper screening by two reviewers left eleven included papers,20–30 (Figure 1). The most common reason for paper exclusion (309) was because the risk information presented was not fully personalized as set out in our inclusion criteria (requiring a patient assessment prior to receiving the information, Table 1). In the majority of these excluded papers, risk information was formulated using broad population characteristics such as age. Another 51 papers were excluded because they involved considering only one form of presenting information to patients, rather than a comparison between two different forms or comparing a certain form of information (eg, photographs) with verbal information or usual care. Full reasons for exclusion are given in Figure 1.
 | Figure 1 PRISMA diagram. |
Details of included papers indicate that this is a relatively new research area (Table 2). Eight of the eleven papers were published in the last 5 years. No studies were found that made comparisons between different information forms, with most included studies comparing particular forms of communicating risk information with usual care. Heterogeneity in study design and outcomes of included studies meant that a meta-analysis was not undertaken. Where data from reviews are insufficient to merit pooling of included studies because of the very wide range of interventions covered, a “narrative synthesis” is recommended.31 Narrative synthesis involves summarizing the main features of different studies and important characteristics (such as similarities and differences between studies) and identifying patterns of results in the data.31
 | Table 2 Included papers: study design and main findings |
Summary of included studies
Five studies concerned cardiovascular risk information,23,24,26–28 one concerned asthma risk information,29 and the rest covered broader “healthy life check” information. Three studies involved information for Type 2 diabetes patients.24,28,30 Although eight studies used an RCT design, two were feasibility studies23,26 and two were pilot RCTs.25,27 Of the three remaining publications, one was an intervention description,30 one a protocol,27 and the other an uncontrolled prospective study.28 Quality assessment of included RCTs indicates that some of the RCTs had a low risk of bias in many domains, apart from intervention and outcome assessment blinding (Table 3).
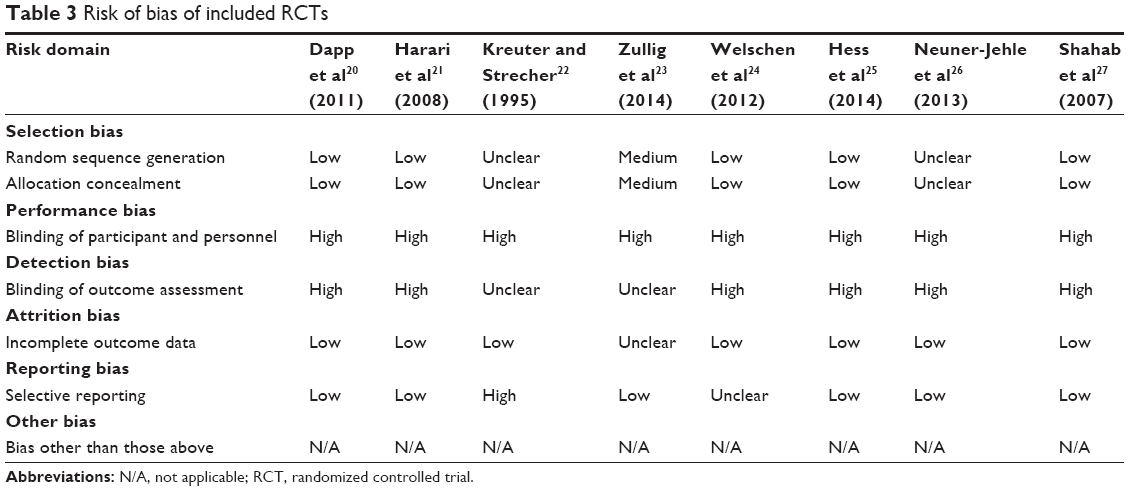 | Table 3 Risk of bias of included RCTs |
Computer generated individualized written feedback on health risk
Seven articles concerned personalized risk information presented on computer.20–23,25,29,30 Developments in information technology have made it possible to combine health behavior change theory, communication theory, social marketing principles, and computer-based programs and algorithms to produce personally relevant health messages for individuals. Information from participants’ survey data can be assembled to generate customized messages, to the extent that it includes elements such as an individuals’ health literacy, locus of control, internet experience, attitude to self-care, decision preferences, and current health knowledge.30 Computer technology allows incorporation of several hundred text files, graphics, and photographs which can potentially correspond with each survey question selected for tailoring and its possible response option combinations.32 By personalizing messages and the language in the interactive dialogue (for example, contextualizing according to the user’s viewpoint eg, “as you said before … ”), attention and impact is thought to be increased.
Most of the randomized controlled trials within our included studies involved computer-generated health risk appraisals (HRA), although results were generally disappointing. An RCT of a web-based intervention delivering personalized cardiovascular risk information to patients was found to be ineffective, with no significant differences in health outcomes or behavior between intervention and control groups after 3 months.23 Even a study of computerized HRA where the outcome of interest was set relatively modestly at changes in risk perception found that adjustments in optimistic and pessimistic bias only occurred in some of the disease domains studied22 (Table 2).
Two included studies reported randomized controlled trials of computerized HRAs administered in a general medical practice setting.20,21 Both involved older adults. The earliest of these integrated computerized HRAs into practice-based information technology systems and generated individualized feedback to both patients and general practitioners who had been trained on current care and behavior recommendations relating to the risk domains covered. It was, however, left to the discretion of doctors and patients as to how any issues identified were addressed in consultations, if at all.21 Results were relatively disappointing, with minimal improvement in patients’ health behavior or uptake of preventive care across the domains studied21 (Table 2). Intervention group participants reported slightly higher pneumococcal vaccination uptake (odds ratio [OR]: 1.7, confidence interval [CI]: 1.4–2.1) and some improvement in physical activity levels compared with controls (OR: 2.0, CI: 1.6–2.6). However, no significant differences were observed for any other of the 14 categories of health behavior or types of preventive health service use at the 12 month follow-up.21
A later study, this time undertaken in medical practices in Hamburg, Germany, offered additional message reinforcement as well as the HRA information for patients and practitioners (again with a training of the general practitioners involved).20 Overall, results were slightly better (Table 2). While there were still no differences between intervention and controls in mortality, hospital admissions, and the frequency of visits to a doctor, there were small but statistically significant shifts in self-reported health behaviors.20 After 1 year, the proportion of 9 types of preventive service use (such as dental check-ups) was an average of 75% in the intervention group and 68% in controls (OR: 6.1, CI: 4.3–7.9).20 Likewise, out of six possible health behaviors (such as three or more moderate to strenuous physical activities per week), 64% of these behaviors were reported by the intervention group, versus 60% in the controls (OR: 3.7, CI: 2.0–5.4).20 Of the 804 participants in the HRA intervention group, 503 opted to take up some group session reinforcement, 77 opted for home visit reinforcement, and 224 did not take up the reinforcement offer. This allowed for a subgroup analysis to explore the efficacy of the reinforcement component within this complex intervention. Findings indicate that a reinforcement component is needed if the intervention is to be effective. The “difference” in reported preventive service use between intervention and controls was 7.1% (CI: 5.2%–9.0%; P<0.001) for those receiving the full HRA intervention, including some kind of reinforcement, but only 2.0% (CI: −2.2 to 6.3, P>0.1) where intervention participants received the HRA only.20 The same pattern was seen in other self-reported health behavior outcomes.20
Although authors suggest that computerized HRAs in clinical settings are best used to complement face-to-face consultations with clinicians, making them “more efficient and satisfying for both sides” by “increasing patients knowledge and power to enable them to be active partners in their care”,30 an RCT using computer-generated risk information on tablet PCs just prior to a doctor’s appointment does not support this.25 Little increase in both patients’ and doctors’ reports of discussion on various health topics for patients with prior access to their HRA was found.25 Harari et al21 also reported no HRA effect on patients’ self-efficacy related to patient/doctor interactions (Table 2). In summary, therefore, several studies come to the same conclusion: that although computerization makes tailoring of risk information possible, and enables simple and visual representation of complex risk information, additional input is needed to interpret and discuss the feedback – in other words, some sort of face-to-face component to HRA interventions appears to be needed if beneficial effects are to be seen.20–23
Risk information presented by way of diagrams, charts, and photographs
These small or non-significant findings are not limited to risk information presented on computers. Studies in the clinical setting presenting risk information by way of population diagrams,24,28 colored charts,26 or photographs27 come to similar conclusions – that risk information presented in this way alone is insufficient to prompt patients to adopt healthier lifestyles or to enhance clinical communication (Table 2). The only effect found was a short-term increase in risk perception.24,27 Welschen et al24 conclude that risk communication is insufficient on its own, but should be a first stage in a more complex lifestyle intervention.
The RCT by Shahab et al27 using ultrasound scans showing the extent of blockage in carotid arteries allows some insight into the processes involved. They theorized that visual imagery such as scans of partially blocked carotid arteries span the conscious–unconscious continuum more readily than language, with the result that patients experience less filtering out of the information by the “conscious critical apparatus”, which usually serves to disengage the individual from beliefs which derogate the threat message. Their study collected behavior mediator variables based on the Extended Parallel Process model and was able to offer an explanation as to why some individuals were able to ignore the threat message even when it was presented in such a vivid way. Results showed that positive responses to the threat message presented were dependent on individuals having high self-efficacy beliefs (feeling able to make positive changes in the necessary behavior).27 A more recent study by Saver et al28 supports the hypothesis that individuals are able to distance themselves from computer-generated risk information, even when it is presented in an personally tailored way. Participants professed that “the computer model is wrong about me … I know my health better … than some statistics”. Almost 80% reported that they felt the data did not apply to them personally. Instead, 75% described “knowing myself” as an important way they understood their risks “because I know myself better than I think some statistics show .... ” Embodiment of risk was described, although interestingly, the doctor was identified as someone who was the next best placed person to make risk judgments: “ .... that’s why I go by my body experiences, besides the doctor, you are the one who knows how your body functions”.28
Discussion
As is the case in all systematic reviews, despite carefully constructing electronic search strategies, some literature may have been missed if articles were poorly indexed. We recognize this as a possible limitation of the review. Systematic review search term filters are usually determined in a trade-off between sensitivity (ability to detect all possible publications on the topic, knowing that this will throw up a lot of papers not meeting inclusion criteria) and precision (ability to deliver a search identifying a high proportion of relevant papers).33 We attempted to balance these two considerations by undertaking text mining of sample papers, and then subsequently broadening the search to increase sensitivity, supplementing this with handsearching of specialist journals. However, it is possible that by using text mining to design a precise search, we may have limited its sensitivity somewhat, and so some relevant publications were missed.
Nevertheless, it is striking how little literature there is on how tailored risk information is received by patients in clinical settings, bearing in mind the emphasis on personal responsibility for health and providing personal health and lifestyle risk factor advice to patients which is the basis of current health policy in many countries.34 For example, in both medical and dental care in the UK, growing attention is paid to collecting a range of “life check” information using personal health and lifestyle risk assessment tools with the intention that this is linked to personalized advice to patients.34,35 This is in contrast to a wealth of studies contrasting whether people’s risk perception is best informed using various different types of numerical and diagrammatical representations.14 The expansion of technology that allows extensive personalization of risk information makes translation into the clinical setting tempting. Certainly, computer technology which allows a range of information to be incorporated into patients’ assessments on the face of it appears to offer some assistance to clinicians. However, our study indicates these approaches may be insufficiently meaningful for patients, to make this worthwhile on their own.
Results remind us that the very notion of “risk” itself differs substantially when approached from different standpoints. Scientific medicine defines “risk” in terms of an objective reality that can be measured, controlled, and managed.36 Although this approach tends to dominate thinking in this area of health care, and leads on to approaches which quantify risk, for example, with elaborate computer modeling of lifestyle data, our results indicate these may lack sufficient meaning for patients. In other words “risk” is something of a “trans-scientific” topic in that issues can be raised but not completely answered by science.37
Lindell et al38 identify that important differences exist when communicating risk information to individuals (in clinical settings) as opposed to populations. Science-based notions of risk which are based on mathematically expressed probabilities are only meaningful at the level of a population. Although this type of data represents objective, anonymized knowledge, at the level of individuals, the information becomes potentially emotionally charged and anxiety inducing.38 Lindell et al38 also observe that when talking to individuals about “risk”, it becomes concretized, almost “reified”, as if it was something “carried” by the patient in her own body – a conclusion which resonates with the qualitative data reported in Saver et al’s study.28
And so it is up to clinicians to “recontextualize” the information to make it meaningful at a truly personal level.38 Often data involving percentages are recast into an “all or nothing” scenario (“Will I get sick or not?”).16 And so we observe that clinicians naturally simplify risk information when talking to patients, to a relatively dichotomous model through the use of verbal qualifiers (“Your risk is high” or “This is not good for your health”).39 Misselbrook and Armstrong agree that when talking to individuals rather than populations, a high/low risk model is a better fit because it “provides the patient with a map to enable them to function and cope in an uncertain world”.40
A common theme across our included studies, which were limited to those undertaken in a clinical setting, is that “discourse” (in some sort of face-to-face interaction) is a necessary way in which meaning is imparted to risk information, making it possible to move from scientifically based risk representations relevant at a population level to notions of risk relevant to individuals. Our results indicate that this is still necessary with scientific data, even where this has been “personally tailored” to individuals. Faisal et al41 terms the process as “internalization of externalized data” (externalized data such as visual representations of data on computer-supported tools) and argue that “sense-making” is a necessary process of finding meaning from information. So, while risk information may be helpful in assisting people to perceive and make sense of their health status and medical condition, the process of sense-making concerns not just the data, but their own life experiences.42 The study by Dapp et al20 is particularly interesting because discourse on HRA data took place in groups or at home, and not in the medical practice with a doctor. These discursive practices help to define “who and what is normal, standard, and acceptable”.43 They help to challenge what was once “taken for granted”. It is after destabilizing current meaning that the information forms a basis for change.
Conclusion
Although presenting personalized information on health risk to patients is increasingly expected as part of a general health policy approach that emphasizes patients’ contribution for their health by adhering to health education advice, our review reveals that relatively little empirical work has been done that compares the relative impact of communicating information on risk to patients using different forms. Most work has been done in the growing field of presenting computerized health risk appraisals to patients. Findings suggest, however, that the impact of this information format is limited because there remains a need for discourse between patient and clinician (or even between patients) in order to impart personal meaning to the information sufficient to prompt a change in behavior. More work is needed to explore this further.
Acknowledgments
This project was funded by the National Institute for Health Research Health Services and Delivery Research Program (Project number 13/33/45). The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the HS&DR Program, NIHR, NHS, or the Department of Health. We also acknowledge the work by Andy Pennington and Eleanor Kotas in assisting in formulating the electronic search strategy.
Disclosure
The authors report no conflicts of interest in this work.
References
Ahmed A, Nail G, Willoughby H, Edwards AG. Communicating risk. BMJ. 2012;344:1–7. | ||
Becker MH. The Health Belief Model and Personal Health Behaviour. San Francisco, CA: Society for Public Health Education; 1974. | ||
Witte K, Meyer G, Martell D. Effective Health Risk Messages: A Step-by Step Guide. Thousand Oaks, CA: Sage; 2001. | ||
European Centre for Disease Prevention and Control. A literature review on effective risk communication for the prevention and control of communicable diseases in Europe: insights into health communication. Technical Report; 2013. Available from: http://ecdc.europa.eu/en/healthtopics/health_communication/health-communication-topics/pages/risk-communication.aspx. Accessed October 14, 2016. | ||
Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behaviour change interventions. Psychol Bull. 2007;133(4):673–693. | ||
Hawkins RP, Kreuter M, Resnicow K, Fishbein M, Dijkstra A. Understanding tailoring in communicating about health. Health Educ Res. 2008;23(3):454–466. | ||
Edwards AG, Naik G, Ahmed H, et al. Personalised risk communication for informed decision making about taking screening tests. Cochrane Database Syst Rev. 2013;2:CD001865. | ||
Abrams DB, Mills S, Bulger D. Challenges and future directions for tailored communication research. Ann Behav Med. 1999;21(4):299–306. | ||
Lustria ML, Noar SM, Cortese J, Van Stee SK, Glueckauf RL, Lee J. A meta-analysis of web-delivered tailored health behaviour change interventions. J Health Commun. 2013(9);18:1039–1069. | ||
Paling J. Strategies to help patients understand risks. BMJ. 2003;327(7417):745–748. | ||
Timmermans DRM, Ockhuysen-Vermey CF, Henneman L. Presenting health information in different formats: the effect on participants’ cognitive and emotional evaluation and decisions. Patient Educ Couns. 2008;73(3):443–447. | ||
Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication. Patient Educ Couns. 2006;61(2):173–190. | ||
Rothman AJ, Kiviniemi MT. Treating people with information: an analysis and review of approaches to communicating health risk information. J Natl Cancer Inst Monogr. 1999;25:44–51. | ||
Lipkus IM, Hollands JG. The visual communication of risk. J Natl Cancer Inst Monogr. 1999;25:149–163. | ||
Buchanan BG, Moore JD, Forsythe DE, Carenini G, Ohlsson S, Banks G. An intelligent interactive system for delivering individualised information to patients. J Artif Intell Med. 1995;7:117–154. | ||
Davidson C, Davey Smith G, Frankel S. Lay epidemiology and the prevention paradox: the implications of coronary candidacy for health education. Sociol Health Illness. 1991;13(1):1–19. | ||
Lefebvre CJ, Glanville J, Wieland LS, Weightman A. Methodological developments in searching for systematic reviews: past. Present and future? Syst Rev. 2013;2:78. | ||
Effective Practice and Organisation of Care (EPOC). How to develop a search strategy. EPOC Resources for review authors. Oslo, Norway: Norwegian Knowledge Centre for the Health Services; 2014. Available from: http://epoc.cochrane.org/epoc-specific-resources-review-authors. Accessed October 14, 2016. | ||
Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 [updated March, 2011]. The Cochrane Collaboration; 2011. Available from: http://www.handbook.cochrane.org. Accessed October 14, 2016. | ||
Dapp U, Anders JAM, von Renteln-Kruse W, et al; PRO-AGE Study Group. A randomized trial of effects of health risk appraisal combined with group sessions or home visits on preventive behaviours in older adults. J Gerontol A Biol Sci Med Sci. 2011;66(5):597–598. | ||
Harari D, Iliffe S, Kharicha K, et al. Promotion of health in older people: a randomised controlled trial of health risk appraisal in British general practice. Age Ageing. 2008;37(5):565–571. | ||
Kreuter MW, Strecher VJ. Changing inaccurate perceptions of health risk: results from randomised trial. Health Psychol. 1995;14(1):56–63. | ||
Zullig LL, Sanders LL, Shaw RJ, McCant F, Danus S, Bosworth HB. A randomised controlled trial of providing personalised cardiovascular risk information to modify health behaviour. J Telemed Telecare. 2014;20(3):147–152. | ||
Welschen LM, Bot SD, Kostense PJ, et al. Effects of cardiovascular disease risk communication for patients with type 2 diabetes on risk perception in a randomized controlled trial. Diabetes Care. 2012;35(12):2485–2492. | ||
Hess R, Tindle H, Conroy MB, Clark S, Yablonsky E, Hays RD. A randomized controlled pilot trial of the functional assessment screening tablet to engage patients at the point of care. J Gen Intern Med. 2014;29(12):1641–1649. | ||
Neuner-Jehle S, Knecht MI, Stey-Steurer C, Senn O. Acceptance and practicability of a visual communication tool in smoking cessation counselling: a randomised controlled trial. Prim Care Respir J. 2013;22(4):412–416. | ||
Shahab L, Hall S, Marteau T. Showing smokers with vascular disease images of their arteries to motivate cessation: a pilot study. Br J Health Psychol. 2007;12:275–283. | ||
Saver BG, Mazor K, Hargraves JL, Hayes M. Inaccurate risk perceptions and individualized risk estimates by patients with type 2 diabetes. J Am Board Fam Med. 2014;27(4):510–519. | ||
Ahmed S, Bartlett, SJ, Ernst P, et al. Effect of a web-based chronic disease management system on asthma control and health-related quality of life: study protocol for a randomized controlled trial. Trials. 2011;12:260. | ||
Weyman N, Harter M, Petrak F, Dirmaier J. Health information, behaviour change, and decision support for patients with type 2 diabetes: development of a tailored, preference-sensitive health communication application. Patient Prefer Adherence. 2013;7:1091–1099. | ||
Ryan R; Cochrane Consumers and Communication Review Group. Cochrane Consumers and Communication Review Group: data synthesis and analysis. Available from: http://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/AnalysisRestyled.pdf. Accessed December 5, 2016. | ||
Campbell MK, Carr C, DeVellis B, et al. A randomised trial of tailoring and motivational interviewing to promote fruit and vegetable consumption for cancer prevention and control. Ann Behav Med. 2009;38(2):71–85. | ||
Boluyt N, Tiosyold L, Lefebvre C, Klassen TP, Offringa M. Usefulness of systematic review search strategies in finding child health systematic reviews in MEDLINE. Arch Pediatr Adolesc Med. 2008;162(2):111–116. | ||
Department of Health. Government White paper Cm 6737. Our health, our care, our say: a new direction for community services. London, UK: DOH; 2006. Available from: https://www.dh.gov.uk. Accessed May 31, 2016. | ||
Department of Health. Guidance: Dental contract reform: prototypes: patient information. London, UK: DOH; 2015. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/556110/Patient_information_16_17.pdf. Accessed October 14, 2016. | ||
Althaus CE. A disciplinary perspective on the epistemological status of risk. Risk Analysis. 2005;25(3):567–588. | ||
Kasperson RE. The Social Amplification of Risk: Progress in Developing an Integrative Framework. Westport, CT: Praeger; 1995:157. | ||
Lindell P, Adelsward V, Sachs L, Bredmar M, LindStedt U. Expert talk in medical contexts: explicit and implicit orientation to risks. Res Lang Soc Interact. 2002;35:195–218. | ||
Neuner-Jehle S, Senn O, Wegwarth O, Rosemann T, Steurer J. How do family physicians communicate about cardiovascular risk? Frequencies and determinants of different communication formats. BMC Fam Pract. 2011;12:15–24. | ||
Misselbrook D, Armstrong D. Thinking about risk. Can doctors and patients talk the same language? Fam Pract. 2002;19:1–12. | ||
Faisal S, Blandford A, Potts HWW. Making sense of personal information: challenges for information visualisation. Health Inform J. 2013;19(3):198–217. | ||
Lupton D. Introduction: risk and sociocultural theory. In: Lupton D, editor. Risk and Sociocultural Theory: New Directions and Perspectives. Cambridge, UK: Cambridge University Press; 1999. | ||
Macguire S, Hardy C. Organising processes and the construction of risk: a discursive approach. Acad Manage J. 2013;56(1):231–255. |
Supplementary material
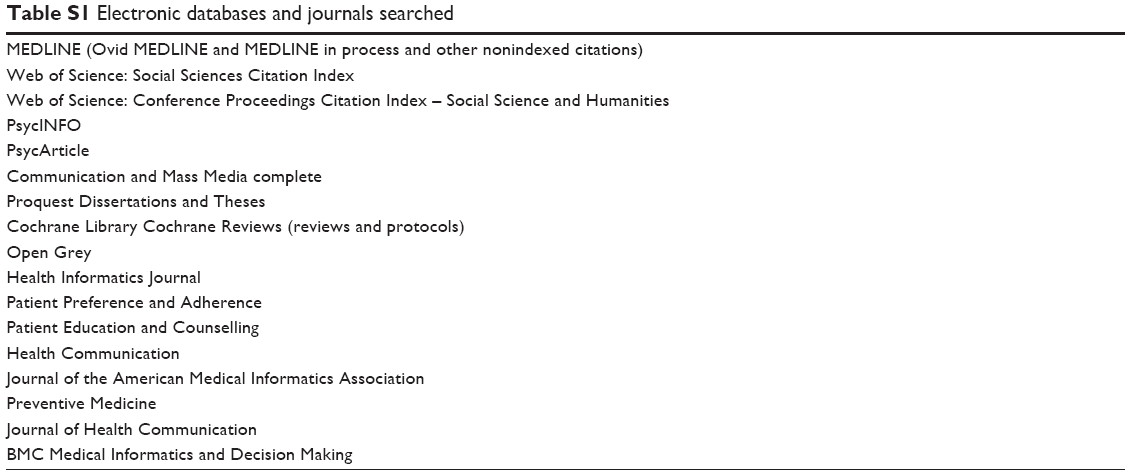 | Table S1 Electronic databases and journals searched |
 © 2017 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2017 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.