Back to Journals » Orthopedic Research and Reviews » Volume 18
Does Anteroposterior Cage Position and Screw Orientation Influence Clinical/Radiographic Outcomes and Complications After Oblique Lumbar Interbody Fusion with Lateral Plate Fixation?
Authors Li Y ![]() , Shi X, Lu S, Liu J
, Shi X, Lu S, Liu J
Received 23 March 2026
Accepted for publication 16 June 2026
Published 23 June 2026 Volume 2026:18 611380
DOI https://doi.org/10.2147/ORR.S611380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qian Chen
Yachen Li,1– 3,* Xin Shi,1– 3,* Sheng Lu,1– 3 Jie Liu1– 3
1Department of Orthopaedics, The First People’s Hospital of Yunnan Province.The Affiliated Hospital of Kunming University of Science and Technology, Kunming, People’s Republic of China; 2Yunnan Provincial Spinal Cord Disease Clinical Medical Centre, Kunming, People’s Republic of China; 3Yunnan Key Laboratory of Digital Orthopedics, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Sheng Lu, Department of Orthopaedics, The First People’s Hospital of Yunnan Province. The Affiliated Hospital of Kunming University of Science and Technology, No. 175 Jinbi Road, Xishan District, Kunming, Yunnan, People’s Republic of China, Email [email protected] Jie Liu, Department of Orthopaedics, the First People’s Hospital of Yunnan Province. The Affiliated Hospital of Kunming University of Science and Technology, No. 175 Jinbi Road, Xishan District, Kunming, Yunnan, People’s Republic of China, Email [email protected]
Objective: The objective of this study was to evaluate the influence of cage anteroposterior position and angulation, as well as plate and screw trajectory, in oblique lumbar interbody fusion with lateral plate fixation, on clinical and radiographic outcomes along with associated perioperative complications.
Methods: A total of 47 patients undergoing OLIF-LP surgery were enrolled. Cases were divided into the anterior position group (APG) or the posterior position group (PPG) based on whether the cage was positioned anterior or posterior to the midline. Data were collected preoperatively and at 3 days, 3 months, and 12 months postoperatively. Radiographic parameters measured included LL, FSL, DH, and FH. Implant-related measurements comprised cage-device angle (CDA), superior screw to endplate angle (SSEA), and inferior screw to endplate angle (ISEA). Clinical outcomes included Back-VAS, Leg-VAS, ODI scores, and perioperative complications, to evaluate the impact of cage position on radiographic and clinical outcomes at different time points.
Results: No significant differences were found in clinical outcomes between the groups at any point. Radiographically, the APG showed greater improvement in FSL than the PPG (4.37± 3.56° vs. 1.75± 3.16°, p=0.012). The APG also had greater loss of FH during follow-up (p=0.024). Thigh/inguinal numbness was the most common complication (38.3%), and was more frequent in the PPG. SSEA positively correlated with FSL at final follow-up (r=0.408, p=0.004).
Conclusion: When employing a lateral plate for fixation in OLIF, an anteriorly positioned cage yields superior improvement in FSL, whereas posterior placement more effectively maintains FH, albeit with an increased risk of perioperative neurological complications. Moreover, a larger SSEA was positively associated with improvement in long-term FSL.
Keywords: lumbar interbody fusion, lordosis, OLIF, cage position, complications, lateral plate fixation
Introduction
Oblique Lumbar Interbody Fusion (OLIF), first reported by Silvestre et al in 2012,1 has emerged as a mainstream surgical approach for degenerative disc disease, spondylolisthesis, and spinal stenosis. Its oblique lateral retroperitoneal access effectively circumvents vascular complications associated with traditional anterior approaches while avoiding posterior muscular dissection. This technique offers distinct advantages including minimized surgical trauma, reduced intraoperative bleeding, and lower neurological complication rates, significantly accelerating postoperative recovery. When performed within appropriate indications,2 OLIF achieves thorough disc space release, optimal intervertebral height restoration, and sagittal balance correction, yielding favorable clinical outcomes.
Nevertheless, standalone OLIF (SA-OLIF) configurations face significant challenges with cage subsidence,3 frequently leading to complications such as disc height loss and pseudarthrosis that substantially compromise long-term efficacy. To enhance segmental stability, contemporary OLIF procedures commonly incorporate supplemental fixation techniques including lateral plates (LP), lateral screws (LS), and posterior bilateral/unilateral pedicle screw instrumentation (BPS/UPS).4,5 Among these, OLIF with lateral plate fixation (OLIF-LP) has gained prominence due to its single-incision and single-position advantages, establishing itself as a prevalent surgical option.
Current international consensus recommends placing the cage in zones II and III of the intervertebral space, primarily based on anatomical safety considerations to avoid vascular injury with anterior placement or neural injury with posterior placement.6 While studies have investigated cage position in PLIF, TLIF, and OLIF/LLIF procedures with bilateral posterior pedicle screw fixation,7–10 there is a lack of research focusing on implant positioning (including cage, plate, and screws) in OLIF combined with lateral plate fixation. Different surgical approaches and fixation techniques exhibit variations in biomechanics and long-term outcomes.11–13 In clinical practice, cage placement is frequently subject to positional deviation or angular inclination due to limited surgical exposure, morphological variations of the endplates, or iliac crest obstruction. Simultaneously, substantial operational heterogeneity exists in the screw insertion direction (cephalad/caudal angulation) of the lateral plate. Moreover, the addition of a lateral plate may potentially influence the lateral spinal structures. Notably, whether these variations affect the overall stability of the “cage-plate construct” and consequently lead to differences in radiographic and clinical outcomes remains unexplored.
This study pioneers the comprehensive analysis of how critical technical parameters—cage positional shift (anterior/posterior displacement), cage angular deviation, and plate screw trajectories—influence postoperative functional outcomes, radiographic parameters, and complication profiles in OLIF-LP procedures. Our findings will establish evidence-based guidance for optimizing precision execution of OLIF-LP.
Materials and Methods
Patient Population
This study received ethical approval from the Institutional Review Board of The First People’s Hospital of Yunnan Province (Approval No.KHLL2025-KY132). Written informed consent for research participation and publication was obtained from all participants.
Between April 2022 and January 2024, 86 consecutive patients underwent single-surgeon OLIF-LP procedures at The First People’s Hospital of Yunnan Province. All patients were diagnosed with lumbar spinal stenosis, degenerative spondylolisthesis, segmental instability, or adjacent segment disease (ASD), with complete minimum 12-month follow-up documentation. Exclusion criteria comprised: (1) Utilization of alternative fixation methods or standalone OLIF constructs. (2) History of abdominal or spinal surgeries. (3) Severe spinal stenosis, high-grade degenerative spondylolisthesis, spinal infections, traumatic injuries, or neoplasms. (4) Incomplete pre- or postoperative clinical/radiological documentation. Baseline demographic parameters were meticulously documented: gender, chronological age, standing height, body weight, comorbidities, symptom duration, smoking status, and cage material specifications. After implementing these selection criteria, 47 OLIF-LP patients were ultimately included in the final cohort.
Surgical Procedure
All patients underwent comprehensive preoperative evaluations including lumbar MRI, three-dimensional CT scans, and standard anteroposterior/lateral radiographs with dynamic flexion-extension views. Preoperative assessment specifically evaluated psoas major-vascular corridor stenosis, osseous spinal canal narrowing, and facet joint fusion. All procedures were performed by a single experienced spine surgeon. Patients were positioned in the lateral decubitus position. Under C-arm fluoroscopic guidance, skin markings were made at the target disc center. Following abdominal muscle incision and dissection, the retroperitoneal space was accessed to approach the psoas major. Careful psoas retraction exposed the disc space, enabling insertion of a localization needle. Repeat fluoroscopy confirmed the disc midpoint, facilitating placement of a tubular retractor. Annulotomy, complete discectomy, and bilateral endplate preparation were subsequently performed. Blunt contralateral annulus dissection ensured adequate traversal of the disc space by the interbody cage. An 18 mm-wide, 6° lordotic cage packed with allogeneic bone graft was inserted, with trial spacers confirming appropriate sizing. Posterior and lateral fluoroscopy verified cage positioning within Knight zones II–III on lateral imaging. Intraoperatively, the target was to position the cage at the midpoint of the endplate; however, the final cage center point varied between zones II and III on postoperative imaging. A length-appropriate lateral plate (pre-locked to the cage) was positioned in the same region, followed by freehand placement of 5.5 mm-diameter screws into the cephalad and caudal vertebral bodies under fluoroscopic confirmation of proper screw length and maintained zone II–III positioning. For two-level procedures, skin markings centered on the intermediate vertebral body under C-arm guidance enabled single-incision completion. Postoperatively, all patients wore lumbosacral orthoses for three months.
Data Collection
Clinical outcomes were evaluated using the Back Pain Visual Analog Scale (Back-VAS), Leg Pain Visual Analog Scale (Leg-VAS), and Oswestry Disability Index (ODI) preoperatively and at postoperative day 3, month 3, and month 12. Perioperative complications, symptomatic events, hospitalization duration, operative time, and intraoperative blood loss were systematically documented.
Identical timepoints (preoperative, postoperative day 3, month 3, month 12) were employed for lateral radiographic parameter measurement: (1) Disc Height (DH): Mean value of anterior and posterior disc space heights; (2) Foraminal Height (FH): Maximum distance between the inferior vertebral notch of the cephalad vertebra and superior vertebral notch of the caudal vertebra; (3) Fused Segment Lordosis (FSL): Angle between lines connecting the superior endplate of the upper vertebra and inferior endplate of the lower vertebra; (4) Lumbar Lordosis (LL): Angle between the superior endplates of L1 and S1; (5) Cage Subsidence Grading: Assessed on 12-month lateral radiographs using the Luis Marchi et al14 classification (Grade 0–3), with Grade ≥1 defined as subsidence. Postoperative day 3 lumbar three-dimensional CT scans facilitated implant-related measurements: (1) Cage Deviation Angle (CDA): Angle between the cage’s longitudinal axis and posterior vertebral margin horizontal line on axial CT;15 (2) Cage Position (CP): Cage center point location relative to the vertebral midline (anterior/posterior) on axial CT; (3) Screw Trajectory Angles: Superior Screw to Endplate Angle (SSEA): Coronal CT angle between superior screw and cephalad endplate; Inferior Screw to Endplate Angle (ISEA): Coronal CT angle between inferior screw and caudal endplate. All radiographic parameters underwent independent measurement by two spinal surgeons each possessing over five years of specialized experience. The measurement methods of relevant parameters are shown in Figure 1.
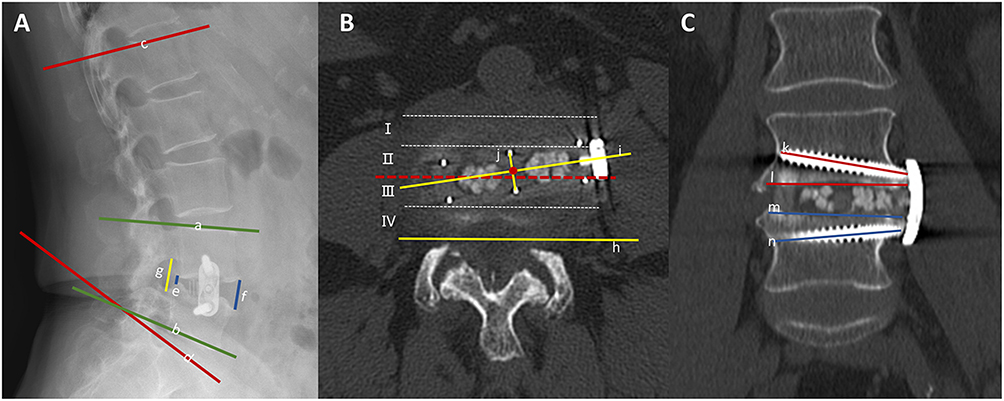 |
Figure 1 Radiographic measurement parameters. (A) Measurements on sagittal radiographs, the angle between line a and b was FSL; the angle between line c and d was the LL; the average length of line e and f was DH; the length of line g was FH; (B) Measurements on axial CT scans 3 days postoperatively, line j and i were the mutually perpendicular central dividing lines of the cage, with the intersection point of the two lines located anterior or posterior to the midline to determine cage position; the angle between line i and h was CDA; (C) Measurements on coronal CT scans 3 days postoperatively, the angle between line k and l was the SSEA, and the angle between line m and n was ISEA. |
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics version 27.0 (IBM Corp). Continuous variables are presented as mean ± standard deviation, while categorical variables are presented as frequencies (proportions). Inter-rater reliability was assessed via the intraclass correlation coefficient (ICC), calculated using a two-way random-effects model with absolute agreement specification. Normality of continuous data was assessed using the Shapiro–Wilk test. For between-group comparisons, continuous variables with normal distribution were analyzed using independent samples t-tests, while those with non-normal distribution were analyzed using Mann–Whitney U-tests. Categorical variables were analyzed using chi-square or Fisher’s exact tests. Correlations were evaluated using Pearson’s correlation coefficient for normally distributed continuous variables and Spearman’s rank correlation coefficient for non-normally distributed continuous variables or ordinal categorical variables. Statistical significance was defined as p < 0.05.
Results
A total of 47 patients meeting inclusion/exclusion criteria were enrolled. The cohort comprised 17 males and 30 females, with a mean age of 58.1 ± 8.1 years (range: 40–74 years), all completing >12-month follow-up. Postoperative measurements confirmed all cages were positioned within zones II–III. Patients with cage center points anterior to the disc space midpoint constituted the Anterior Position Group (APG), while those posterior formed the Posterior Position Group (PPG):27 patients (57.4%) comprised the APG (M: F=8:19; mean age 56.40 ± 6.96 years; BMI 24.16 ± 3.44 kg/m2), whereas 20 patients (42.6%) were allocated to the PPG (M: F=9:11; mean age 60.30 ± 9.04 years; BMI 25.55 ± 3.09 kg/m2). Smoking history included 4 APG and 7 PPG patients.
No significant intergroup differences existed in preoperative primary diagnoses or comorbidities. Both groups utilized two material types of 18 mm-wide, 6° lordotic cages without intergroup variation. The PPG cohort comprised 16 single-level and 4 two-level procedures, while the APG included 25 single-level and 2 two-level interventions. Collectively addressing 53 surgical levels (L3/4:16; L4/5:37), no significant intergroup disparities were observed in operative time, intraoperative blood loss, or hospitalization duration (Table 1).
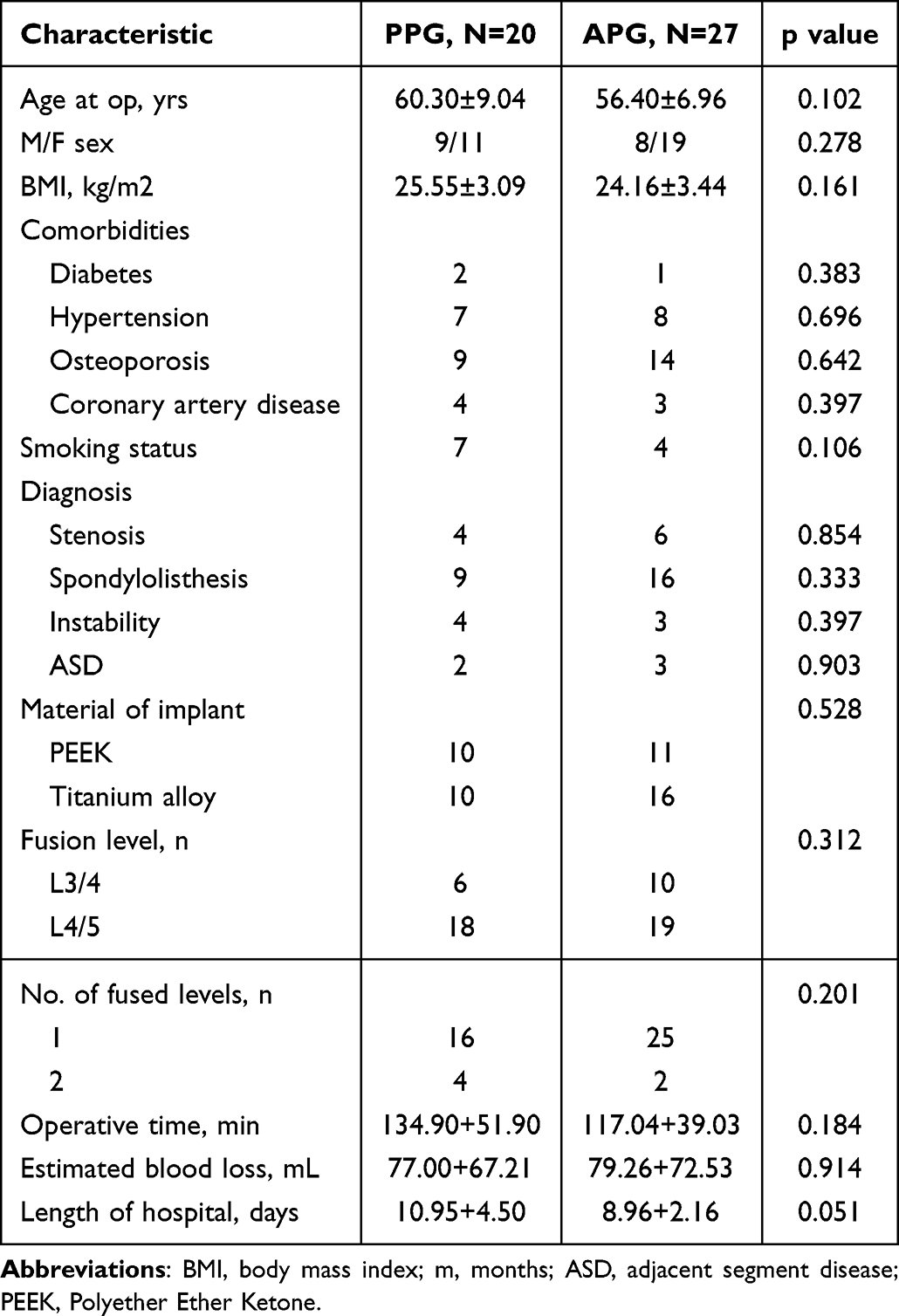 |
Table 1 Demographic and Clinical Data of Patients |
Both groups demonstrated significant clinical improvement compared with baseline, which was maintained through final follow-up. Comparative analysis revealed no significant differences in ODI, Back-VAS, or Leg-VAS scores between PPG and APG at any time point (Table 2).
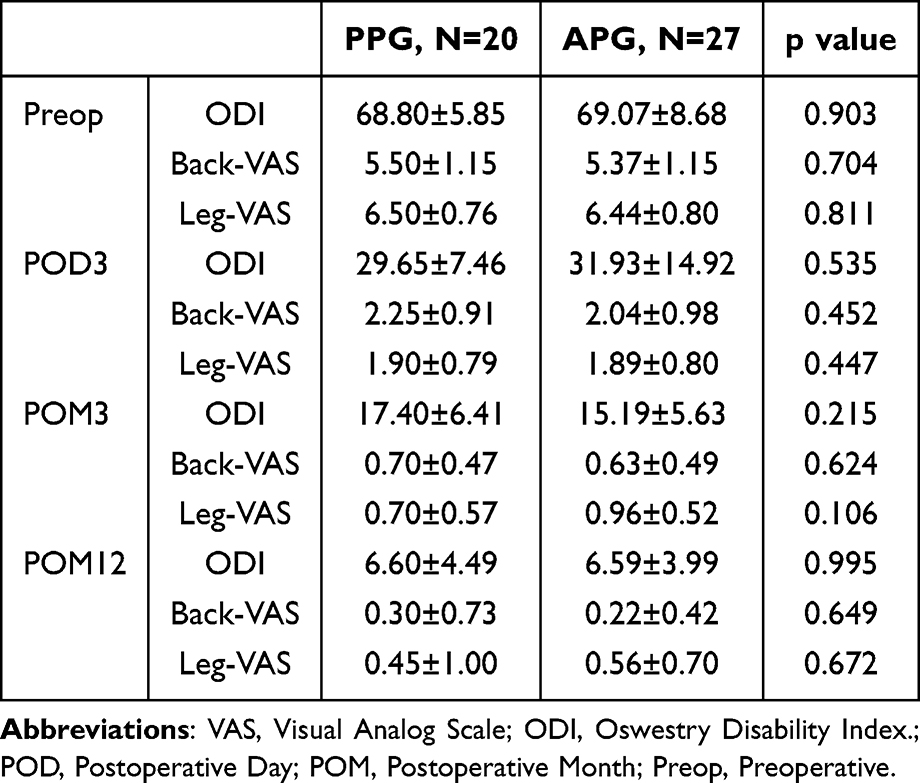 |
Table 2 Clinical Results |
Radiographically, both groups exhibited substantial improvements in DH and LL that were sustained throughout follow-up, with no significant intergroup differences. Notably, independent-samples t-test showed that APG achieved superior restoration of FSL compared with PPG postoperatively (4.37±3.56° vs. 1.75±3.16°, p=0.012). Although no significant differences in FH were observed between groups at baseline or on postoperative day 3, APG exhibited significantly greater FH loss at 3- and 12-month follow-ups compared with PPG (p=0.024 and p=0.033, respectively) (Table 3).
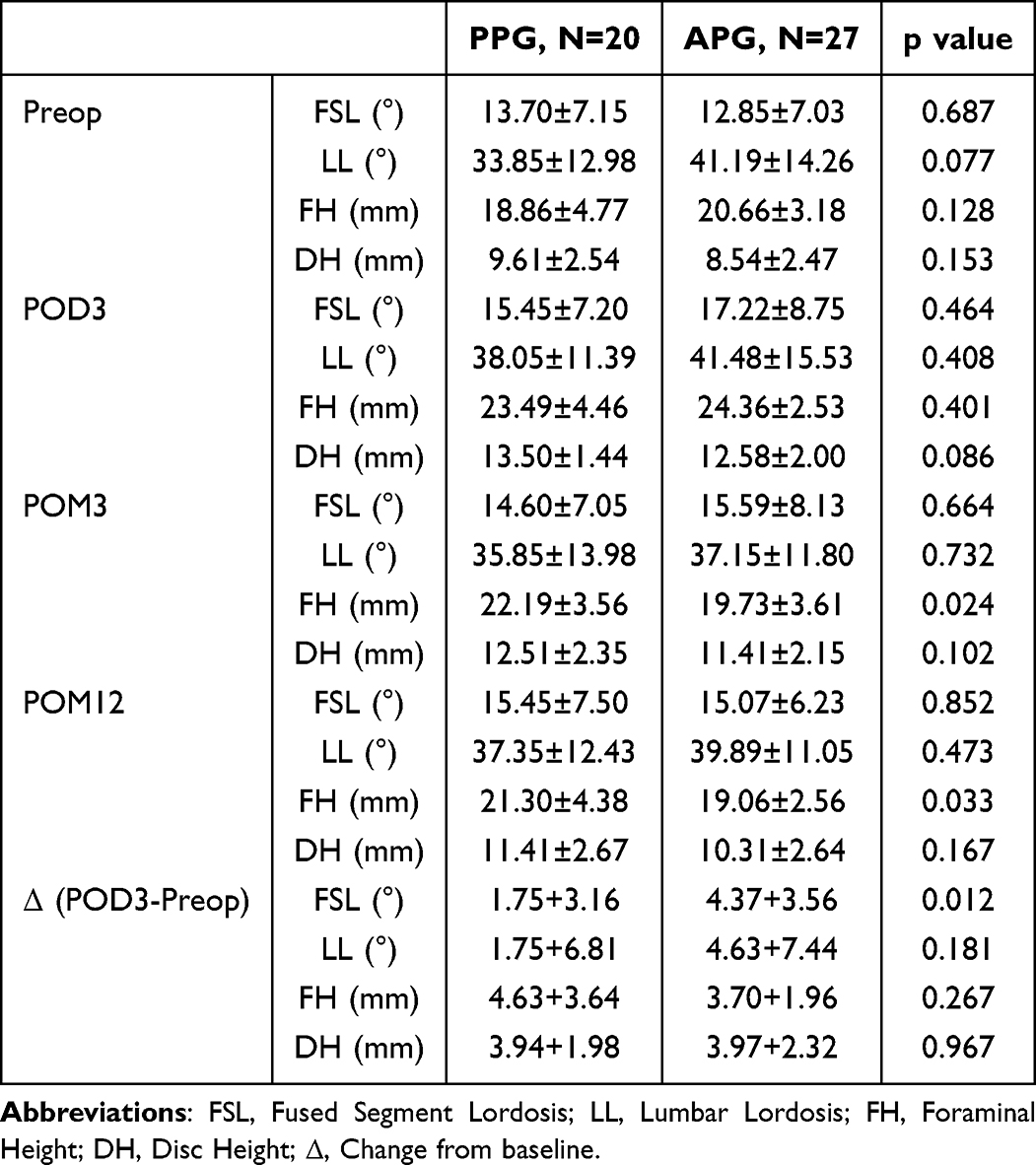 |
Table 3 Radiographic Results |
Postoperative complications/symptoms occurred in twenty-three patients, comprising eight with single manifestations and fifteen with multiple occurrences. Cage subsidence occurred in 29.8% of patients, but no statistically significant difference was observed between the groups. Transient symptoms—including hip weakness, thigh/inguinal numbness, thigh pain, abdominal distension, and constipation—resolved completely by the 3-month follow-up without long-term sequelae. Notably, thigh numbness emerged as the most prevalent complication (38.3% overall incidence), demonstrating significantly higher frequency in the PPG cohort (p<0.05) (Table 4). Spearman correlation analysis of implant-related parameters (SSEA=8.74±4.40°; ISEA=12.00±3.70°; CDA=5.11±5.01°) revealed no significant associations between SSEA/ISEA/CDA and long-term clinical outcomes or cage subsidence, except for a positive correlation between SSEA and 12-month FSL (ρ=0.408, p=0.004) (Table 5).
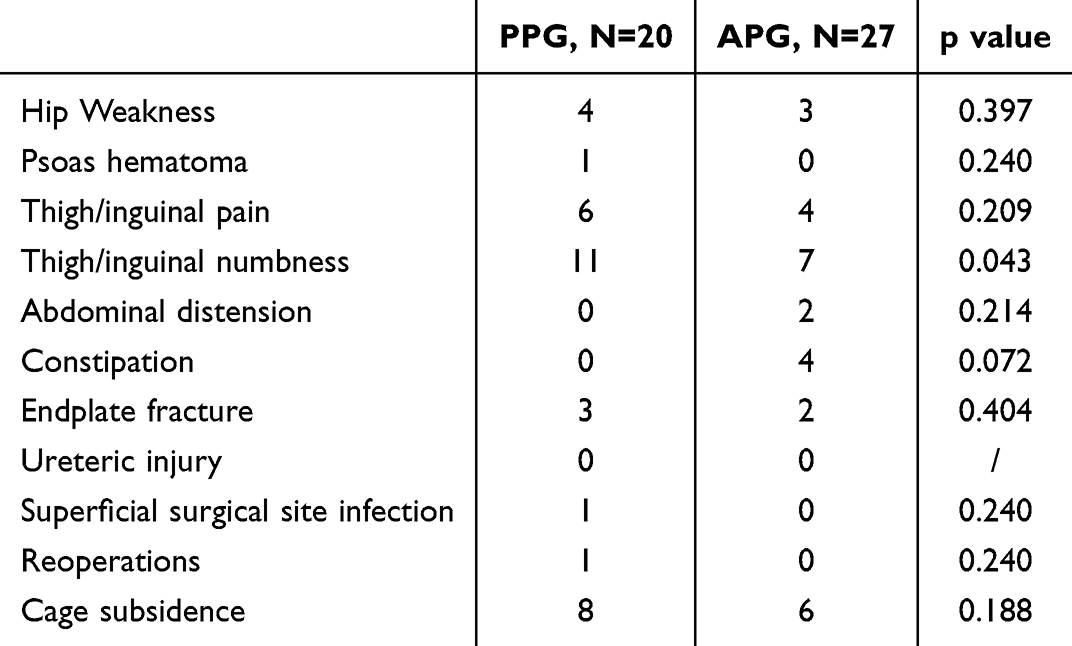 |
Table 4 Comparison of Perioperative Complications Between PPG and APG Groups |
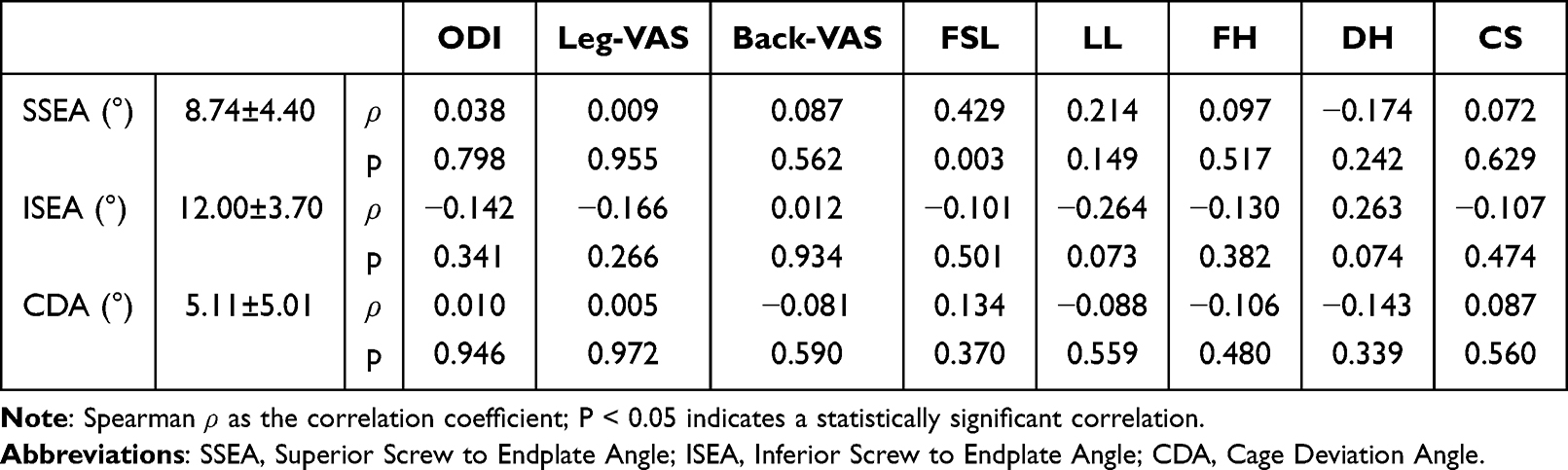 |
Table 5 Spearman Correlation Analysis Between Implant-Related Measurements and 12-Month Postoperative Clinical Outcomes (n=47) |
Discussion
OLIF achieves indirect decompression and restores lumbar alignment by inserting an interbody cage to distract annular fibers and ligaments.16 Compared to traditional TLIF and PLIF techniques, OLIF preserves the posterior musculoligamentous complex and facet joint structures, enabling these preserved posterior elements to provide greater segmental stability. This characteristic obviates the universal necessity for supplemental rigid pedicle screw fixation.17 When supplemented with LP, OLIF delivers superior stability versus standalone constructs18,19 while eliminating requirements for intraoperative positional changes or additional incisions.20,21
In PLIF and TLIF procedures, alterations in cage center position can influence adjacent segment facet joint degeneration and lumbar lordosis, where restoring or maintaining lordosis constitutes a critical determinant for optimizing clinical outcomes.8,22,23 Furthermore, multiple studies demonstrate anterior cage placement in PLIF/TLIF facilitates increased anterior disc height and compresses the posterior disc space to achieve spinal lordosis.7,24–26 For OLIF techniques, in vitro studies confirm OLIF-BPS constructs provide biomechanical stability comparable to PLIF.27 Regarding OLIF-BPS or LLIF-BPS procedures, Park et al recommend positioning cages in the anterior 1/3 of the disc space as the optimal location for LLIF, as successful indirect decompression better restores FSL.28 Qiao et al also reported cages located at the anterior 1/3 with better SLA improvement than those at the posterior 2/3 (2.8° versus 0.8°) in LLIF. However, research evaluating cage position in OLIF-LP—an anterolateral fixation construct—remains absent. Our findings demonstrate that with lateral plate augmentation, anterior cage positioning yields significantly greater FSL improvement versus posterior placement (4.37±3.56° vs 1.75±3.16°, p=0.012), with sustained correction throughout follow-up. The PPG demonstrated comparable FH to the APG at postoperative day 3, but exhibited significantly better FH maintenance during follow-up. This outcome may stem from the cage’s role as a shifting pivot point within the disc space: when positioned anteriorly, it may predispose to posterior disc height loss, thereby increasing FSL; conversely, posterior placement may better preserve posterior disc height, maintaining FH (Figure 2). However, this mechanism awaits biomechanical validation. Notably, these radiographic variations did not translate to clinical outcome differences within the 1-year follow-up period. Moreover, posterior placement may limit segmental lordosis restoration, which could theoretically lead to suboptimal sagittal alignment and persistent back pain despite successful fusion, although such long-term functional effects were not observed within our 1-year follow-up.
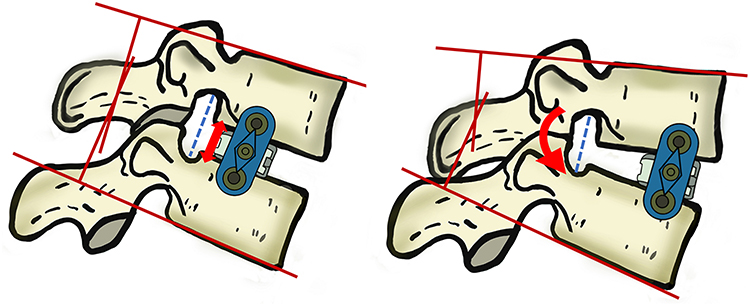 |
Figure 2 The left panel illustrates that when the cage is positioned posteriorly within the intervertebral space, it better maintains posterior disc height and FH. The right panel demonstrates that anterior cage placement allows the posterior structures to compress using the cage as a pivot point, thereby improving FSL. |
Numerous studies have substantiated the short-term clinical efficacy and functional outcomes of OLIF-LP; however, perioperative complications associated with this technique remain understudied. Crucially, local complication profiles may exhibit distinct characteristics when lateral supplemental instrumentation is employed compared to traditional posterior fixation approaches. While the OLIF approach inherently mitigates risks of intraspinal neurological injury, perioperative neurological complications still occur in 8%–35% of cases, including thigh numbness, hip/leg pain, and lower extremity weakness.29–32 In this study, 48.9% of patients developed new-onset postoperative symptoms or complications. Among all complications, inguinal/thigh numbness demonstrated the highest incidence (38.3%). All cases of inguinal/thigh numbness, constipation, abdominal distension, and hip weakness proved transient, with complete resolution by the 3-month follow-up. The PPG cohort demonstrated a significantly higher incidence of inguinal/thigh numbness compared to the APG group—representing the only perioperative symptom exhibiting intergroup disparity based on cage position. Anatomically, the OLIF procedure’s operational safety window resides between the lumbar plexus and sympathetic trunk;33 All surgical interventions in this series targeted exclusively the L3/4 or L4/5 spinal segments, with L4/5 constituting the majority (69.8%) of treated levels. At L3–4, all nerve roots consistently occupied Zone IV, including the L2 division contributing to the lumbar plexus, L3 root, and lateral femoral cutaneous nerve (L2–L3). The genitofemoral nerve consistently resided within Zone I. At L4–5, neural elements within Zones III and IV comprised: (1) lumbar plexus branches contributing to the femoral nerve (L2–L3 divisions and L4 root), (2) intrinsic psoas muscle branches, and (3) obturator nerve pathways. The genitofemoral nerve consistently coursed along the psoas’ anterior surface in Zone I.6 In the anatomical study by Davis, T.T., et al, at the L4/5 level, the femoral nerve traversed Zone II in 1 of 18 specimens and was positioned posterior to the disc space in 5 specimens, with the remainder located in Zones III or IV. Critically, surgical dissection at L4/5 risks encountering the main femoral nerve trunk rather than solely its branches.34 These results align with our findings. Using an expandable retractor for intraoperative distraction after posterior cage placement generates compressive forces between the device and the transverse processes. These forces may compress neural structures in zones III or IV, potentially causing physiological and structural nerve damage. The resulting pathological changes may lead to functional impairments of varying severity. However, it should be acknowledged that postoperative thigh/inguinal numbness may also be influenced by other unmeasured surgical and anatomical factors, such as individual variations in nerve root anatomy, retraction force magnitude, and retraction duration. Therefore, a definitive causal relationship between posterior cage placement and neurological complications cannot be established from the current data.
CS after OLIF is a common complication. Mild CS is often asymptomatic; however, as CS progresses, it may lead to pain, spinal deformity, neurological injury, or even surgical failure.32,35,36 Although supplemental internal fixation is theoretically expected to stabilize the OLIF construct and reduce CS risk, some studies suggest that LP fixation does not significantly lower CS incidence compared with SA constructs. In severe CS cases, LP fixation may even result in plate or screw displacement.37 Notably, no plate displacement was observed in LP-fixed patients in our cohort. Cheng et al38 reported that anterior cage positioning in OLIF-BPS fixation markedly reduced CS incidence (1.8% vs. 28.9%, P < 0.05). They hypothesized that anterior placement allows the cage to span the denser anterior apophyseal ring rather than the comparatively softer central endplate region. Conversely, Yu et al39 found no correlation between cage-endplate contact variables and anteroposterior cage position. Our data similarly showed no statistically significant difference in CS rates between anterior and posterior cage placements. These discrepancies may reflect variations in fixation methodologies across studies.
In the present study, a positive correlation was identified between SSEA and FSL at 12 months postoperatively (r=0.408, p=0.004). Previous studies have demonstrated that OLIF-LP achieves comparable stability to BPS or UPS fixation during lateral bending, but exhibits inferior stability in flexion-extension and axial rotation.11–13,40,41 OLIF-LP fails to effectively restrict motion in the facet joints and posterior lumbar structures.42 However, the mechanism underlying this correlation remains unclear, and causality should not be inferred. While theoretical possibilities exist—such as differential endplate loading or altered segmental kinematics—these speculations require direct biomechanical validation. However, there is currently no direct evidence or clear rationale to explain why the size of the SSEA correlates with FSL at 12 months postoperatively. Current research has predominantly focused on biomechanical comparisons among different fixation methods, while neglecting the critical variable of screw trajectory in LP fixation. Future studies should establish finite element models of LP fixation with varying screw angles to quantitatively analyze endplate stress distribution and screw load characteristics. Additionally, cadaveric experiments should be conducted to evaluate range of motion (ROM) and failure load under different screw trajectories. Such investigations would facilitate a comprehensive understanding of this clinical phenomenon.
This study has several limitations. First, as a single-center retrospective investigation, the stratification of patients by cage position and screw angle was not prospectively controlled. Factors such as intraoperative patient positioning and iliac crest shadowing may have led to deviations in cage placement and screw trajectory. Moreover, the modest sample size (n=47) precluded adjustment for multiple comparisons and multivariable analyses, and cage position was assessed categorically rather than continuously. Therefore, the statistically significant findings should be interpreted as hypothesis‑generating rather than confirmatory. A multicenter study with a larger sample size would help mitigate these inherent biases. Second, the retrospective design limited access to comprehensive clinical data, including cage height, bone graft material composition, and screw length, all of which could influence clinical outcomes. Although this study assessed clinical and radiographic outcomes at 12 months post-OLIF-LP, it cannot adequately determine long-term endpoints such as fusion rates, implant failure, or adjacent segment disease. Finally, additional biomechanical investigations are warranted to validate the correlations between cage/screw placement configurations and clinical outcomes or complication rates. Future prospective multicenter studies consolidating comprehensive datasets are needed to precisely define the roles of cage positioning and plate-screw orientation in OLIF-LP procedures.
Conclusions
In OLIF-LP procedures, cage position, cage deviation angle, and screw trajectory do not appear to affect patients’ long-term symptomatic outcomes. Anteriorly placed cages demonstrate superior improvement in FSL, whereas posteriorly positioned cages better maintain FH but may increase perioperative neurological risk. Additionally, posterior placement may limit segmental lordosis restoration, which could theoretically affect long-term sagittal balance and functional outcomes, though this was not observed within the 1-year follow-up. Consequently, for patients with symptomatic foraminal stenosis, posterior cage placement (Zone III) may be a reasonable option, while anterior positioning (Zone II) could be considered for other clinical indications. Moreover, a larger SSEA was positively associated with long-term FSL improvement.
Abbreviations
APG, anterior position group; ASD, adjacent segment disease; BMI, body mass index; BPS, bilateral pedicle screw; CDA, cage deviation angle; CT, computed tomography; DH, disc height; FH, foraminal height; FSL, fused segment lordosis; ISEA, inferior screw to endplate angle; LL, lumbar lordosis; LLIF, lateral lumbar interbody fusion; LP, lateral plate; MRI, magnetic resonance imaging; ODI, Oswestry Disability Index; OLIF, oblique lumbar interbody fusion; PLIF, posterior lumbar interbody fusion; PPG, posterior position group; ROM, range of motion; SA, standalone; SSEA, superior screw to endplate angle; TLIF, transforaminal lumbar interbody fusion; UPS, unilateral pedicle screw; VAS, Visual Analog Scale.
Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of The First People’s Hospital of Yunnan Province (Approval No.KHLL2025-KY132).
Informed Consent Statement
All patients included in the study signed informed consent for the conduct of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Yunnan Provincial Science and Technology Department/Kunming Medical University Joint Project of Basic Research (202401AC070862), Yunnan Provincial Spinal Cord Disease Clinical Medical Centre (ZX2022000101), and Yunnan Province Clinical Research Center for Orthopaedic and Athletic Rehabilitation(202102AA310068).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Silvestre C, Mac-Thiong JM, Hilmi R, Roussouly P. Complications and morbidities of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lumbar interbody fusion in 179 patients. Asian Spine J. 2012;6(2):89–11. doi:10.4184/asj.2012.6.2.89
2. Sato J, Ohtori S, Orita S, et al. Radiographic evaluation of indirect decompression of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lateral interbody fusion for degenerated lumbar spondylolisthesis. Eur Spine J. 2017;26(3):671–678. doi:10.1007/s00586-015-4170-0
3. Shen S, You X, Ren Y, Ye S. Risk factors of cage subsidence following oblique lumbar interbody fusion: a meta-analysis and systematic review. World Neurosurg. 2024;183:180–186. doi:10.1016/j.wneu.2023.12.110
4. Fogel GR, Parikh RD, Ryu SI, Turner AW. Biomechanics of lateral lumbar interbody fusion constructs with lateral and posterior plate fixation: laboratory investigation. J. Neurosurg. Spine. 2014;20(3):291–297. doi:10.3171/2013.11.SPINE13617
5. Phan K, Maharaj M, Assem Y, Mobbs RJ. Review of early clinical results and complications associated with oblique lumbar interbody fusion (OLIF). J Clin Neurosci. 2016;31:23–29. doi:10.1016/j.jocn.2016.02.030
6. Uribe JS, Arredondo N, Dakwar E, Vale FL. Defining the safe working zones using the minimally invasive lateral retroperitoneal transpsoas approach: an anatomical study. J. Neurosurg. Spine. 2010;13(2):260–266. doi:10.3171/2010.3.SPINE09766
7. Landham PR, Don AS, Robertson PA. Do position and size matter? An analysis of cage and placement variables for optimum lordosis in PLIF reconstruction. Eur Spine J. 2017;26(11):2843–2850. doi:10.1007/s00586-017-5170-z
8. Li F, Zhan X, Xi X, et al. Do the positioning variables of the cage contribute to adjacent facet joint degeneration? Radiological and clinical analysis following intervertebral fusion. Ann Translat Med. 2021;9(9):776. doi:10.21037/atm-20-7718
9. Qiao G, Feng M, Liu J, et al. Does the position of cage affect the clinical outcome of lateral interbody fusion in lumbar spinal stenosis? Glob Spine J. 2022;12(2):204–208. doi:10.1177/2192568220948029
10. Issa TZ, Lee Y, Lambrechts MJ, et al. The impact of cage positioning on lumbar lordosis and disc space restoration following minimally invasive lateral lumbar interbody fusion. Neurosurg. Focus. 2023;54(1):E7. doi:10.3171/2022.10.FOCUS22607
11. Cai XY, Bian HM, Chen C, Ma XL, Yang Q. Biomechanical study of oblique lumbar interbody fusion (OLIF) augmented with different types of instrumentation: a finite element analysis. J Orthopaedic Surg Res. 2022;17(1):269. doi:10.1186/s13018-022-03143-z
12. Hao J, Tang X, Jiang N, Wang H, Jiang J. Biomechanical stability of oblique lateral interbody fusion combined with four types of internal fixations: finite element analysis. Front Bioeng Biotechnol. 2023;11:1260693. doi:10.3389/fbioe.2023.1260693
13. Reis MT, Reyes PM, Bse B, et al. Biomechanical evaluation of lateral lumbar interbody fusion with secondary augmentation. J. Neurosurg. Spine. 2016;25(6):720–726. doi:10.3171/2016.4.SPINE151386
14. Marchi L, Abdala N, Oliveira L, Amaral R, Coutinho E, Pimenta L. Radiographic and clinical evaluation of cage subsidence after stand-alone lateral interbody fusion. J. Neurosurg. Spine. 2013;19(1):110–118. doi:10.3171/2013.4.SPINE12319
15. Chen L, Han Z, Wei J, et al. Accuracy of the cage placement in oblique lumbar interbody fusion and its effects on the radiological outcome in lumbar degenerative disease. Glob Spine J. 2025;15(1):127–135. doi:10.1177/21925682241226956
16. Spiker WR, Goz V, Brodke DS. Lumbar interbody fusions for degenerative spondylolisthesis: review of techniques, indications, and outcomes. Global Spine J. 2018;9(1):77–84. doi:10.1177/2192568217712494
17. Ziino C, Konopka JA, Ajiboye RM, Ledesma JB, Koltsov JCB, Cheng I. Single position versus lateral-then-prone positioning for lateral interbody fusion and pedicle screw fixation. J Spine Surg. 2018;4(4):717–724. doi:10.21037/jss.2018.12.03
18. Fan K, Zhang D, Xue R, et al. Biomechanical Analysis of Double-Level Oblique Lumbar Fusion with Different Types of Fixation: a Finite Element-Based Study. Ortho Surg. 2023;15(5):1357–1365. doi:10.1111/os.13703
19. Zhang S, Liu Z, Lu C, et al. Oblique lateral interbody fusion combined with different internal fixations for the treatment of degenerative lumbar spine disease: a finite element analysis. BMC Musculoskelet Disord. 2022;23(1):206. doi:10.1186/s12891-022-05150-x
20. Cappuccino A, Cornwall GB, Turner AW, et al. Biomechanical analysis and review of lateral lumbar fusion constructs. Spine. 2010;35(26 Suppl):S361–7. doi:10.1097/BRS.0b013e318202308b
21. Laws CJ, Coughlin DG, Lotz JC, Serhan HA, Hu SS. Direct lateral approach to lumbar fusion is a biomechanically equivalent alternative to the anterior approach: an in vitro study. Spine. 2012;37(10):819–825. doi:10.1097/BRS.0b013e31823551aa
22. Hsu HT, Yang SS, Chen TY. The correlation between restoration of lumbar lordosis and surgical outcome in the treatment of low-grade lumbar degenerative spondylolisthesis with spinal fusion. Clin Spine Surg. 2016;29(1):E16–20. doi:10.1097/BSD.0000000000000061
23. Schwab F, Lafage V, Patel A, Farcy JP. Sagittal plane considerations and the pelvis in the adult patient. Spine. 2009;34(17):1828–1833. doi:10.1097/BRS.0b013e3181a13c08
24. Ding Q, Tang X, Zhang R, Wu H, Liu C. Do radiographic results of transforaminal lumbar interbody fusion vary with cage position in patients with degenerative lumbar diseases? Ortho Surg. 2022;14(4):730–741. doi:10.1111/os.13224
25. Matos TD, Fleury RBC, Teixeira KO, Romero V, Defino HLA. Changes in the lumbar vertebral segment related to the cage position in Tlif technique. Acta Ortop. Bras. 2020;28(2):92–96. doi:10.1590/1413-785220202802224215
26. Otsuki B, Fujibayashi S, Takemoto M, et al. Analysis of the factors affecting lumbar segmental lordosis after lateral lumbar interbody fusion. Spine. 2020;45(14):E839–e846. doi:10.1097/BRS.0000000000003432
27. Godzik J, Martinez-Del-Campo E, Newcomb A, et al. Biomechanical stability afforded by unilateral versus bilateral pedicle screw fixation with and without interbody support using lateral lumbar interbody fusion. World Neurosurg. 2018;113:e439–e445. doi:10.1016/j.wneu.2018.02.053
28. Park SJ, Lee CS, Chung SS, Kang SS, Park HJ, Kim SH. The ideal cage position for achieving both indirect neural decompression and segmental angle restoration in Lateral Lumbar Interbody Fusion (LLIF). Clin Spine Surg. 2017;30(6):E784–e790. doi:10.1097/BSD.0000000000000406
29. Cheng C, Wang K, Zhang C, Wu H, Jian F. Clinical results and complications associated with oblique lumbar interbody fusion technique. Ann Translat Med. 2021;9(1):16. doi:10.21037/atm-20-2159
30. Johnson AT, Kumar G, Mohapatra B, Mahajan R. Perioperative Complications of Oblique Lumbar Interbody Fusion (OLIF): 5 Years of Experience with OLIF. Asian J. Neurosurg. 2024;19(4):721–727. doi:10.1055/s-0044-1790515
31. Ricciardi L, Piazza A, Capobianco M, et al. Lumbar interbody fusion using oblique (OLIF) and lateral (LLIF) approaches for degenerative spine disorders: a meta-analysis of the comparative studies. Eur J Orthop Surg Traumatol. 2023;33(1):1–7. doi:10.1007/s00590-021-03172-0
32. Zeng ZY, Xu ZW, He DW, et al. Complications and prevention strategies of oblique lateral interbody fusion technique. Ortho Surg. 2018;10(2):98–106. doi:10.1111/os.12380
33. Gu Y, Ebraheim NA, Xu R, Rezcallah AT, Yeasting RA. Anatomic considerations of the posterolateral lumbar disk region. Orthopedics. 2001;24(1):56–58. doi:10.3928/0147-7447-20010101-20
34. Davis TT, Bae HW, Mok JM, Rasouli A, Delamarter RB. Lumbar plexus anatomy within the psoas muscle: implications for the transpsoas lateral approach to the L4-L5 disc. J Bone Joint Surgery-Am Volume. 2011;93(16):1482–1487. doi:10.2106/JBJS.J.00962
35. Quillo-Olvera J, Lin GX, Jo HJ, Kim JS. Complications on minimally invasive oblique lumbar interbody fusion at L2-L5 levels: a review of the literature and surgical strategies. Ann Translat Med. 2018;6(6):101. doi:10.21037/atm.2018.01.22
36. Xi Z, Mummaneni PV, Wang M, et al. The association between lower Hounsfield units on computed tomography and cage subsidence after lateral lumbar interbody fusion. Neurosurg. Focus. 2020;49(2):E8. doi:10.3171/2020.5.FOCUS20169
37. Ge T, Ao J, Li G, Lang Z, Sun Y. Additional lateral plate fixation has no effect to prevent cage subsidence in oblique lumbar interbody fusion. J Orthopaedic Surg Res. 2021;16(1):584. doi:10.1186/s13018-021-02725-7
38. Gong K, Lin Y, Wang Z, Li F, Xiong W. Restoration and maintenance of segment lordosis in oblique lumbar interbody fusion. BMC Musculoskelet Disord. 2022;23(1):914. doi:10.1186/s12891-022-05855-z
39. Yu Y, Robinson DL, Ackland DC, Yang Y, Lee PVS. The influence of lumbar vertebra and cage related factors on cage-endplate contact after lumbar interbody fusion: an in-vitro experimental study. J Mech Behav Biomed Mater. 2024;160:106754. doi:10.1016/j.jmbbm.2024.106754
40. DenHaese R, Gandhi A, Ferry C, Farmer S, Porter R. An in vitro biomechanical evaluation of a lateral lumbar interbody fusion device with integrated lateral modular plate fixation. Glob Spine J. 2021;11(3):351–358. doi:10.1177/2192568220905611
41. Wang Z, Yang W, Liu X, et al. An in vitro biomechanical evaluation of integrated lateral plate combined with oblique lateral interbody fusion in different bone conditions. Sci Rep. 2024;14(1):29432. doi:10.1038/s41598-024-80631-8
42. Cai Z, Ma R, Zhang J, et al. Evaluation of the stability of a novel lateral plate internal fixation: an in vitro biomechanical study. World Neurosurg. 2022;158:e237–e244. doi:10.1016/j.wneu.2021.10.164
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.