Back to Journals » Cancer Management and Research » Volume 11
Distribution Of Brain Metastasis From Lung Cancer
Authors Wang G, Xu J, Qi Y, Xiu J, Li R ![]() , Han M
, Han M
Received 12 July 2019
Accepted for publication 15 October 2019
Published 1 November 2019 Volume 2019:11 Pages 9331—9338
DOI https://doi.org/10.2147/CMAR.S222920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Guangyu Wang, Jiying Xu, Yana Qi, Jianjun Xiu, Ranran Li, Mingyong Han
Cancer Therapy and Research Center, Shandong Provincial Hospital Affiliated to Shandong University, Jinan 250021, People’s Republic of China
Correspondence: Mingyong Han
Cancer Therapy and Research Center, Shandong Provincial Hospital Affiliated to Shandong University, 324 Jingwuweiqi Road, Jinan 250021, People’s Republic of China
Tel +86 531 6877 2825
Fax +86 531 6877 2825
Email [email protected]
Purpose: The prognosis of lung cancer with brain metastasis is poor. The purpose of this study was to investigate the distribution of brain metastasis and explore its relationship with pathology and genetic mutations.
Patients and methods: Between June 2015 and July 2018, 335 patients from Shandong Provincial Hospital affiliated to Shandong University who had been firstly diagnosed with brain metastasis from lung cancer were retrospectively reviewed. All metastatic lesions were detected in the corresponding area using magnetic resonance imaging (MRI).
Results: A total of 2046 metastatic lesions were found. Of the 335 patients, 21.2% (71/335) had a single brain metastasis and 78.8% (264/335) had multiple lesions. The cerebellum (56%; 189/335), right parietal lobe (54%; 182/335), right frontal lobe (47%; 157/335), and left frontal lobe (45%; 152/335) were the regions with the highest incidence of brain metastasis. The different pathological types of lung cancer showed different distribution of brain metastasis. In lung adenocarcinoma, the left frontal lobe (53%; 111/208), right frontal lobe (48%; 100/208) and cerebellum (56%; 116/208) exhibited higher brain metastases, while the cerebellum (61%; 45/74) and the right frontal lobe (46%; 34/74) had the highest incidence of brain metastasis from small-cell carcinoma. For lung squamous cell carcinoma, the cerebellum (70%; 14/20) was the most common site for metastasis. Adenocarcinoma was the most common pathological type in patients regardless of the number of lesions (ie, single or multiple brain metastases). Comparison of 37 cases with epidermal growth factor receptor (EGFR) gene mutation versus 26 cases without mutations showed that there was no correlation between the distribution of brain metastasis and gene mutation.
Conclusion: The different pathological types of lung cancer demonstrate different distribution of brain metastasis. These findings may have significant implications in the diagnosis and treatment of brain metastasis from lung cancer.
Keywords: epidermal growth factor receptor, magnetic resonance imaging, pathology, gene mutations
Introduction
Brain metastases are the most common intracranial tumors in adults and are an important cause of unfavorable outcomes in patients.1,2 Of the patients with malignant tumors, 40% are prone to intracranial metastasis in the course of disease development. Lung cancer accounts for the vast majority of these metastases.3–5 Despite the current standard treatment for brain metastasis (eg, resection, whole brain radiotherapy, microsurgery and stereotactic radiosurgery), metastasis from lung cancer continues to be associated with a poor prognosis.6–8
Lung cancer can be divided into non-small cell lung cancer (NSCLC) and small-cell lung cancer (SCLC) according to the different pathological types. In conventional studies, patients with SCLC had a high risk of brain metastasis.9 However, owing to the continuous improvement of therapeutic measures and prolonged patient survival, the rate of NSCLC metastasis to the brain is also significantly increased. Prophylactic cranial irradiation is becoming crucial in the treatment of lung cancer. Thus, understanding the accurate distribution of brain metastasis of lung cancer is instructive to the regulation of the dosage of prophylactic cranial irradiation, and could be helpful in the diagnosis of minimal lesions.
In the early years, differences were found in the distribution of brain metastases through computed tomography (CT) or autopsies.10–12 However, limited by the imaging techniques available at that time, it was not possible to thoroughly divide brain regions. At present, based on the potential ability of magnetic resonance imaging (MRI) to noninvasively assess the characteristics of brain tissue, studies have upheld the heterogeneity of brain metastasis.13,14 However, few studies have investigated the specific distribution of brain metastases from lung cancer, especially in relation to pathology and genetic mutations. Herein, we analyzed the distribution of metastases and clinical information of 335 patients with brain metastasis from lung cancer.
Materials And Methods
Patients
Between June 2015 and July 2018, we retrospectively analyzed patients who were firstly diagnosed with brain metastases using MRI, and 380 patients were initially identified. Patients who had multiple primary lung cancers (MPLC) or combined with a second primary cancer were excluded from the study. We only reviewed those with brain metastasis from lung cancer, leaving 335 patients (88.1% of the initial cohort) in the final cohort for analysis. A few patients were diagnosed with brain and leptomeningeal metastases. This study focused on the distribution of lung cancer in the brain parenchyma; thus, we did not record the distribution of leptomeningeal metastases. A total of 71 patients underwent the gene detection technique. The diagnosis of all primary lesions was supported by pathological or imaging examination according to the criteria of the World Health Organization (WHO) for primary cancer, while the detection of metastasis was based on brain MRI.
This study was approved by the Medical Committee of Shandong Provincial Hospital affiliated to Shandong University (Jinan, People’s Republic of China), and written informed consent was obtained from all patients when they were in the hospital. All study was carried out in compliance with the Declaration of Helsinki.
MRI Examinations And Gene Detection Technique
All patients underwent conventional MRI examination using a 3.0T MR scanner (Philips Medical Systems Nederland BV) equipped with an eight-channel head and neck coil. The conventional MRI sequences collected were: sagittal, coronal, and axial T2-weighted and T1-weighted images, fluid-attenuated inversion recovery sequence (FLAIR) images, diffusion-weighted images (DWI) and apparent diffusion coefficient (ADC) and T1-weighted enhanced images. All the results were confirmed by experienced imaging doctors in Shandong Provincial Hospital affiliated to Shandong University. A total of 71 patients underwent the gene detection technique, using amplification refractory mutation system-polymerase chain reaction (ARMS-PCR) and next-generation sequencing technology (NGS). Of those, 43 patients had gene mutations, including epidermal growth factor receptor (EGFR) gene mutations and anaplastic lymphoma kinase (ALK) gene mutations.
Clinical Characteristics
Age, sex, time from the diagnosis of the tumor to brain metastasis (for patients in whom the primary lesions were found due to clinical manifestations of brain metastasis, this was recorded as 0 months), pathology, extracerebral metastasis, drinking, smoking, Karnofsky Performance Scores (KPS), and the site of metastasis were recorded in this study.
Metastatic Regions
The distribution of brain metastasis was recorded according to the different regions of the brain. We divided the brain metastasis regions into the frontal lobe, parietal lobe, temporal lobe, occipital lobe, insular lobe, basal nuclei, thalamus (above areas distinguish between left and right), cerebellum, brainstem, and cingulate gyrus.
Statistical Analysis
Contrast-enhanced MRI is more sensitive for detecting small brain metastases. Hence, the number and size of metastatic lesions varied between different regions; there may be numerous metastatic lesions in a particular region. When we compared the distribution of brain metastases, we recorded one metastasis per region, regardless of the number of metastases occurring in that area. Therefore, we focused on the incidence of brain metastases in a region, rather than the number of brain metastases. Statistical analysis was performed using the SPSS statistical software package (version 20.0; IBM Corp., Armonk, NY, USA). We adopted a uniform distribution of brain metastases as null hypothesis. Chi-squared or Fisher’s exact tests were used to compare categorical variables. P-values <0.05 denoted statistical significance.
Results
Proportion Of Brain Metastases From Lung Cancer
Between June 2015 and July 2018, 380 patients with cancer and brain metastasis who met our inclusion criteria were retrospectively reviewed. The type of primary cancer is shown in Table 1. Among these patients, the incidence of brain metastasis was highest for lung cancer (88%; 335 patients).
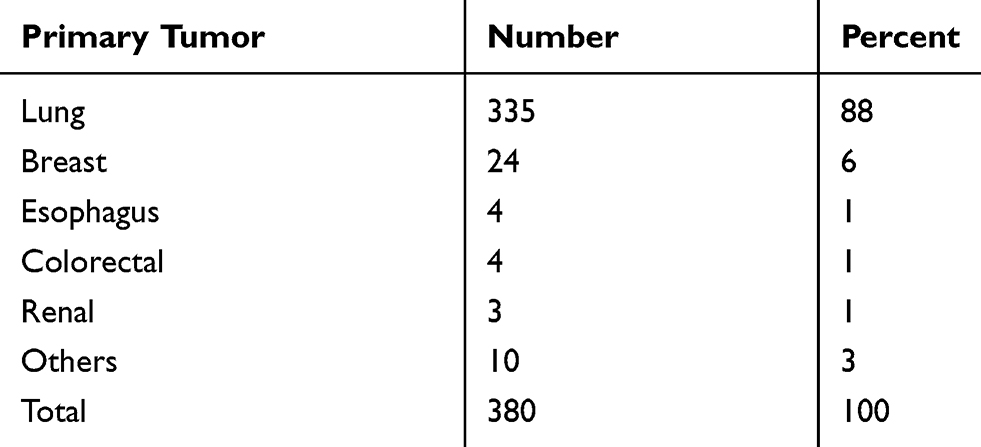 |
Table 1 Primary Tumor In Patients With Brain Metastasis |
Clinical Characteristics Of Patients With Lung Cancer
Table 2 summarizes the clinical characteristics of patients with brain metastases from lung cancer. The median age at diagnosis of brain metastasis was 60 years (range: 28–98 years). A total of 195 men and 140 women were enrolled in the groups. Adenocarcinoma was the most common pathological type (62%; 208 patients), while large cell carcinoma was the least common (1%; two patients). The median time to metastasis, defined as the period from the diagnosis of lung cancer to brain metastasis, was 2 months. There were differences in the time to brain metastasis among the different pathological types, namely 2 months for lung adenocarcinoma, 3.5 months for lung squamous cell carcinoma, and 6 months for small-cell lung cancer. Most of the patients did not consume alcohol, and the proportions of smokers and non-smokers were equal.
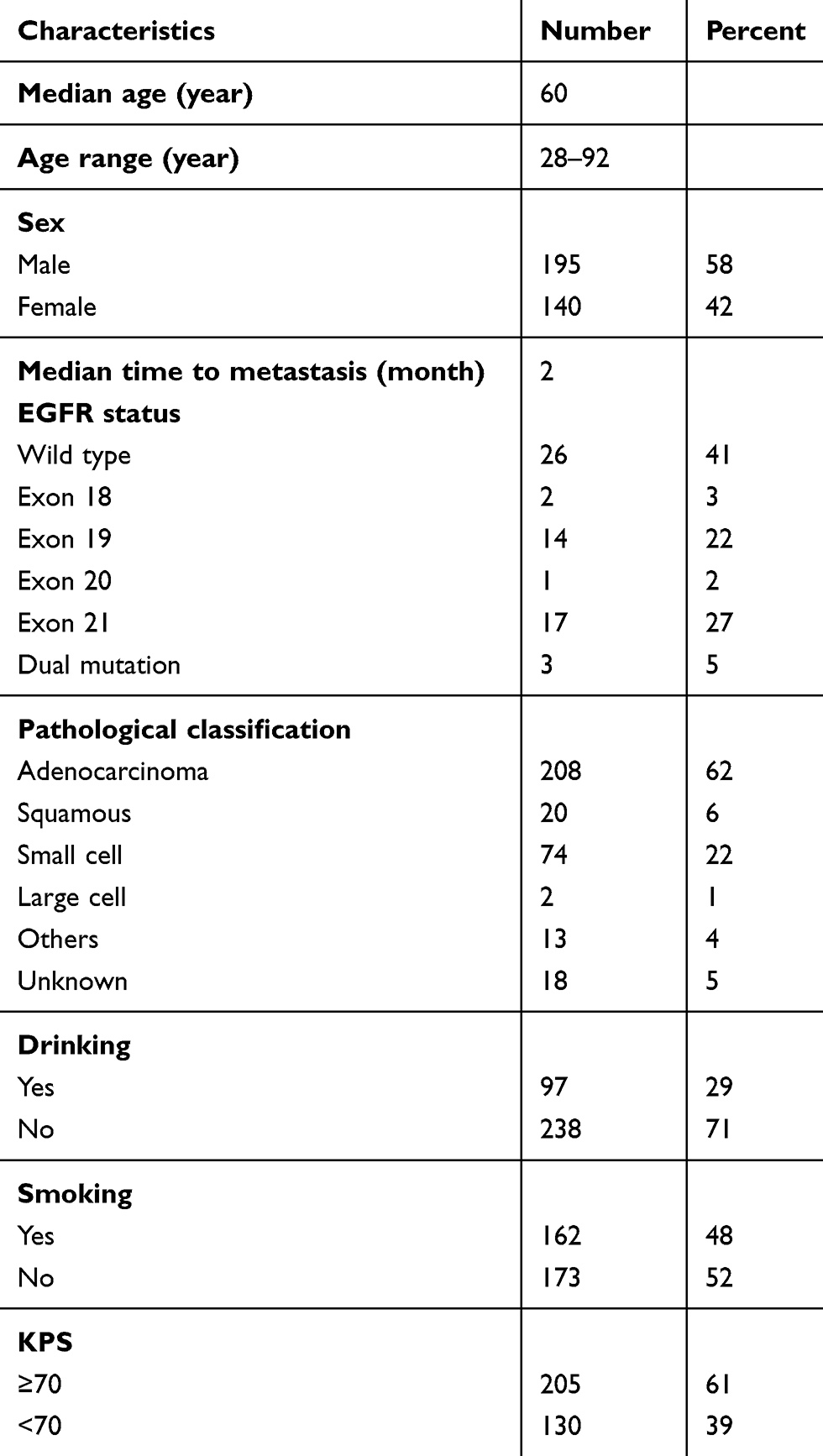 |
Table 2 Clinical Characteristics |
Gene Mutation Status
Among the 43 patients with a mutated gene, 37 patients had EGFR gene mutations and four patients had ALK gene mutations. Among those with mutated EGFR, two patients had mutations at exon 18; 14 patients at exon 19; one patient at exon 20; 17 patients at exon 21; and three patients had dual mutations (one at exon 18 and 20; one at exons 19 and 20; and one at exons 19 and 21).
Extracerebral Metastasis Findings
Most patients developed extracerebral metastases in parallel with brain metastases (91%; 305 patients). These organs include lymph nodes, bones, lungs, pleura, liver, adrenal gland, pancreas, kidneys, and spleen. The most common extracerebral metastatic organs were the lymph nodes (273/335 patients; P<0.05), followed by bone (115/335 patients), and intrapulmonary metastases (93/335 patients) which had no statistical difference in pairings (P>0.05).
Distribution Of Brain Metastases
The number of metastases is shown in Table 3. The distribution of brain metastasis is presented in Figure 1. A total of 2046 metastatic lesions were found in 335 patients. Of those, 21.2% (71/335 patients) had single brain metastasis and 78.8% (264/335 patients) had multiple lesions. Lung adenocarcinoma accounted for the highest proportion of single metastasis (55%; 39/71 patients). Among the single metastatic lesions, cerebellar metastasis exhibited the highest incidence (35%; 25/71 patients; P<0.05). Compared with other sites, the cerebellum (56%; 189/335 patients), right parietal lobe (54%; 182/335 patients), right frontal lobe (47%; 157/335 patients), and left frontal lobe (45%; 152/335 patients) had the highest rate of metastasis (P<0.05), and there was no statistical difference in metastasis between these four regions (P>0.05). For lung adenocarcinoma, the left frontal lobe (53%; 111/208), right frontal lobe (48%; 100/208) and cerebellum (56%; 116/208) exhibited the higher rate of metastasis, and there was no significant difference in metastasis between these three regions (P>0.05). Notably, the cerebellum (61%; 45/74 patients) and the right frontal lobe (46%; 34/74 patients) had the highest incidence of brain metastasis from small-cell carcinoma (P<0.05). For lung squamous cell carcinoma, the cerebellum (70%; 14/20 patients) was the most common site for metastasis (P<0.05).
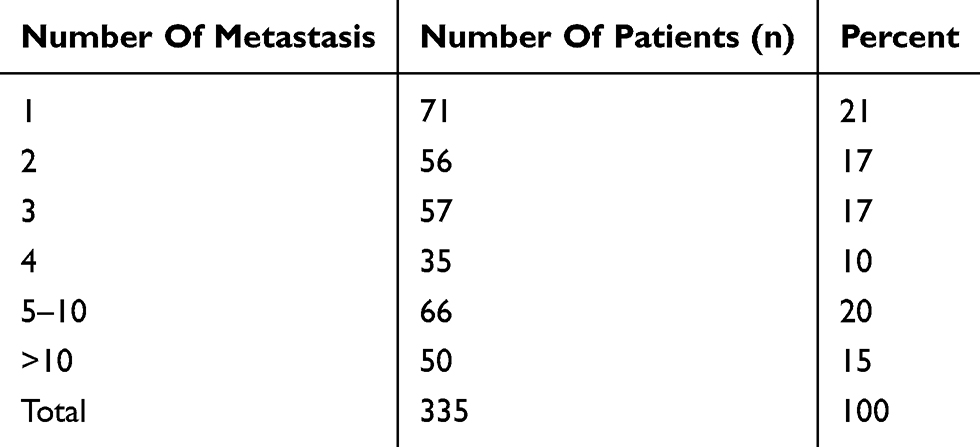 |
Table 3 Number Of Metastasis |
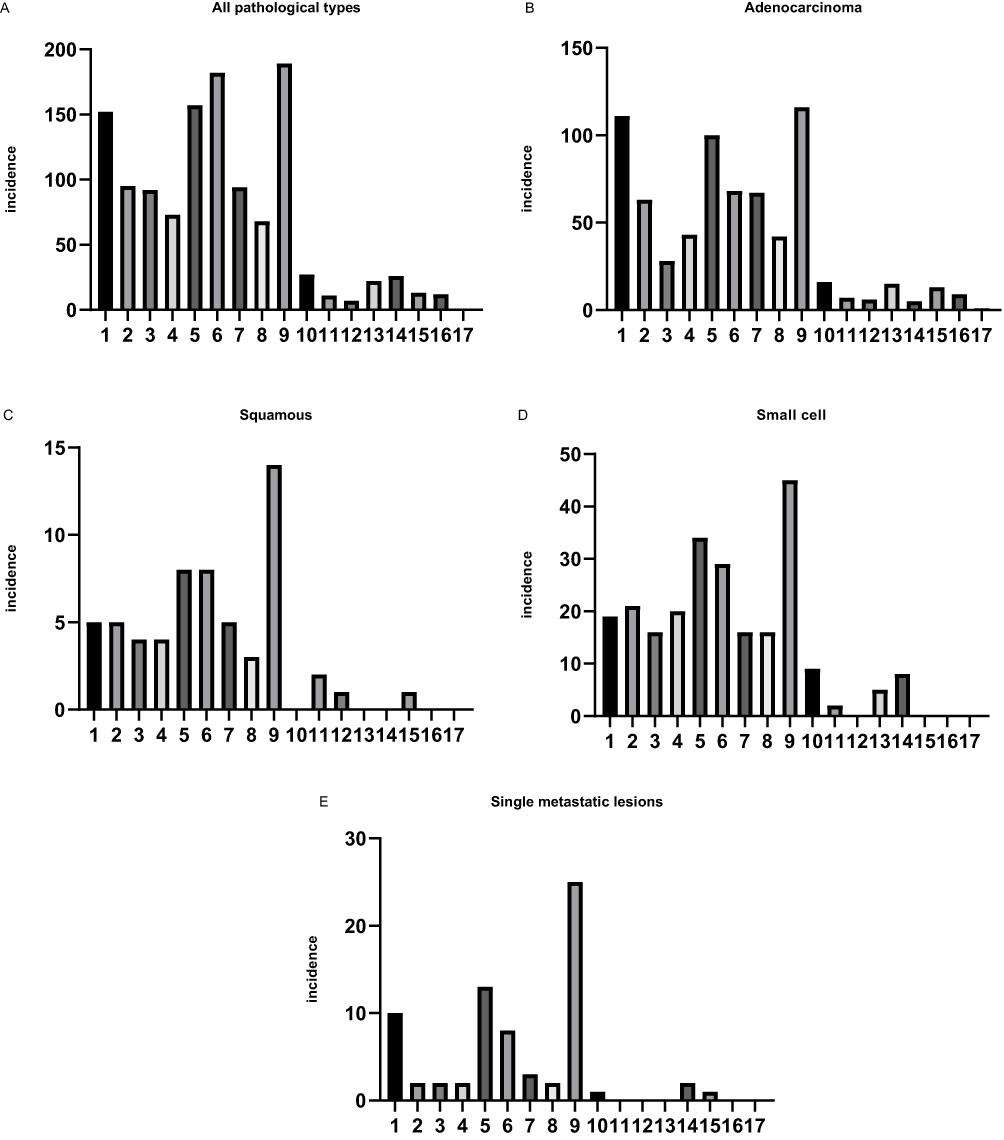 |
Figure 1 Histogram shows the distribution of brain metastasis. (A–E) for Figure 1 represent the incidence of brain metastases in all pathological types, adenocarcinoma, squamous cell carcinoma, small-cell carcinoma and single metastatic lesions cases. Transverse coordinates numbers from left to right represent left frontal lobe, left parietal lobe, left temporal lobe, left occipital lobe, right frontal lobe, right parietal lobe, right temporal lobe, right occipital lobe, cerebellum, brainstem, left insular lobe, right insular lobe, left basal nuclei, right basal nuclei, left thalamus, right thalamus and cingulate gyrus. The vertical coordinates in the histogram represent the incidence of metastasis. |
The distribution of brain metastasis associated with gene mutations is suggested in Figure 2. In patients with EGFR gene mutations, the left frontal lobe (62%; 23/37 patients), right frontal lobe (62%; 23/37 patients) and cerebellum (57%; 21/37 patients) had the highest rate of metastasis. However, there was no statistically significant difference (P=0.998>0.05) between patients with EGFR gene mutations and those with wild-type EGFR (26 patients). The highest incidence of metastasis with ALK gene mutations was reported in the right parietal lobe (75%; 3/4 patients) and right frontal lobe (75%; 3/4 patients). However, the small number of cases (only four patients) did not permit statistical analysis.
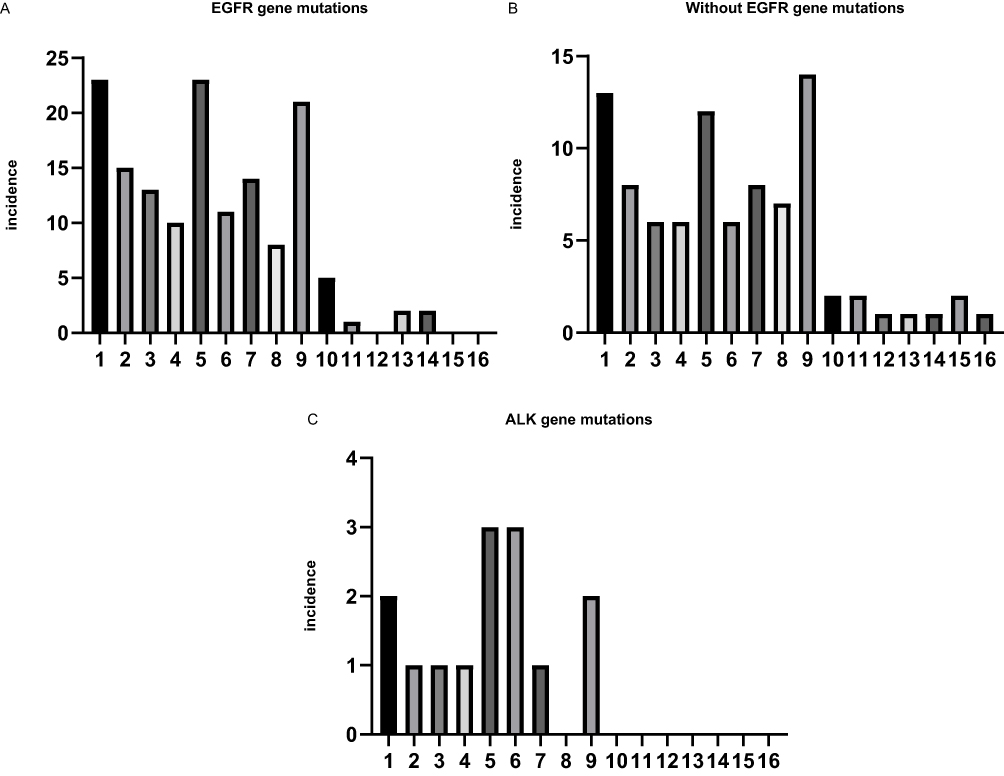 |
Figure 2 Histogram shows the distribution of brain metastasis. (A–C) for Figure 2 represent the incidence of brain metastases in EGFR gene mutations, without EGFR gene mutations and ALK gene mutations cases. Transverse coordinates numbers from left to right represent left frontal lobe, left parietal lobe, left temporal lobe, left occipital lobe, right frontal lobe, right parietal lobe, right temporal lobe, right occipital lobe, cerebellum, brainstem, left insular lobe, right insular lobe, left basal nuclei, right basal nuclei left thalamus and right thalamus. The vertical coordinates in the histogram represent the incidence of metastasis. |
Discussion
In our study, we explored the distribution of brain metastasis from lung cancer by analyzing 335 patients firstly diagnosed with brain metastases between June 2015 and July 2018. Among all patients with brain metastasis, those with lung cancer showed the highest proportion of brain metastases. This was consistent with previously reported data regarding the propensity of lung cancer to metastasize to the brain.3,4,15 In patients with brain metastasis from lung cancer, adenocarcinoma accounts for the vast majority of cases. This can be explained by the aggressive biological behavior of this type of tumor, wide application of molecule-targeted drugs, and continuous improvement of awareness regarding the management of lung adenocarcinoma. These factors can reduce the size of the lesion and prolong patient survival, leading to an increase in the probability of brain metastasis.16–18
According to previous studies and literature, there is a relationship between brain anatomy and brain metastasis; the cerebellum, gray-white matter junction, and watershed areas are preferentially involved.10–13 However, these studies did not perform a detailed division of the brain. Our results showed that metastases in the cerebellum (56%; 189/335 patients), right parietal lobe (54%; 182/335 patients), right frontal lobe (47%; 157/335 patients), and left frontal lobe (45%; 152/335 patients) are most frequent (P<0.05) in patients with lung cancer. These findings are similar to those reported by Wu et al: frontal lobe (31.6%), parietal lobe (18.3%), and cerebellum (18.1%)19 However, they did not divide the brain (left and right areas), and compared the number of lesions (rather than the incidence) for the analysis of brain metastasis.
The “Paget’s theory” or “seed and soil theory” has been previously used to explain the specific sites of brain metastases: the microenvironment provides fertile “soil” for the growth of malignant cells under the specific conditions20 The microenvironment of the cerebellum, parietal lobe, and frontal lobe sites provides appropriate conditions for the development of brain metastasis. Another potential explanation may be the high blood perfusion in these regions. A high blood volume and long perfusion time provide favorable conditions for metastasis, homing, colonization, and outgrowth of tumor cells in the brain parenchyma.21–23
In addition, we investigated the relationship between brain metastasis and pathology, revealing that the various pathological types exhibit different distributions. For lung adenocarcinoma, the left frontal lobe, right frontal lobe, and cerebellum had the higher incidence of brain metastasis. The cerebellum and right frontal lobe had the highest rate of brain metastasis from small-cell carcinoma. For lung squamous cell carcinoma, the cerebellum was most common site of metastasis. The difference in these distributions may be closely related to the biological behavior of different pathological types of lung cancer cells. Adenocarcinoma shows infiltrating growth and often invades the bronchus. After destroying the wall of the tube, the tumor cells can spread hematogenously through the anastomotic branches between the pulmonary vessels and the vertebral veins. Small-cell carcinoma exhibits the characteristics of high malignancy and rapid growth; thus, it is easy to metastasize. As a result, adenocarcinoma and small-cell carcinoma tend to be associated with extensive brain metastases. In most cases of squamous cell carcinoma, exophytic growth is slow, only invading the blood vessels in the advanced phases of the disease. Thus, the distribution of brain metastasis in squamous cell carcinoma is more limited.
Recently, an increasing number of research studies have explored brain metastasis at the molecular level. In lung cancer, patients with mutant EGFR had a higher frequency of brain metastasis than those with wild-type EGFR24 Furthermore, among patients with EGFR mutations, the incidence of brain metastasis was significantly higher in patients with mutation at exon 19 than in those with mutation at other sites.25 Takano et al reported that brain metastasis from lung cancer in patients with an EGFR L858R mutation occurred more often in the caudate nucleus, cerebellum, and temporal lobe than those with an EGFR exon 19 deletion.13 Thus, we suggest that the distribution of brain metastasis differs according to the genetic composition of lung cancer. Similar to other reports, in our study, mutations occurred most commonly at exons 19 and 21.25–27 However, our results showed that there was no statistical significance in the distribution of brain metastasis between patients with EGFR gene mutations and those without mutations (P=0.998). A possible explanation for this difference is that Takano et al compared various types of EGFR mutations, while we compared mutated and wild-type subgroups. In addition, it is possible that the small sample size of the two studies investigating gene mutations may have led to differences. It is undeniable that the molecular mechanism of preferential areas of brain metastasis and the correlation between the EGFR status and risk of brain metastasis remain unclear. The roles of molecules related to the EGFR mutation status will be studied further in the near future.
The results of our research are useful to clinicians for the diagnosis of brain metastasis, especially in the analysis of the different pathological types of lung cancer, in which small lesions can be found. Meanwhile, these findings also provide a reference for the regulation of the dosage of prophylactic cranial irradiation.
Our study had several limitations. Firstly, this was a single-center retrospective analysis. Thus, it is inevitable that patients have regional characteristics, leading to bias. Nonetheless, our sample size was sufficiently large versus analogous studies, and the results were similar between studies. Secondly, we only compared patients with EGFR gene mutations, while those with ALK gene mutations were not analyzed due to the small sample size.
Conclusion
This analysis revealed the distribution of brain metastasis, especially its relationship with pathology. Furthermore, we did not find a relationship between the distribution of brain metastasis and gene mutations. These findings provide theoretical bases for the diagnosis and management of brain metastasis from lung cancer and provide guidance for further research.
Abbreviations
MRI, magnetic resonance imaging; NSCLC, non-small cell lung cancer; SCLC, small-cell lung cancer; CT, Computed Tomography; MPLC, multiple primary lung cancers; WHO, World Health Organization; DWI, diffusion-weighted images; ADC, apparent diffusion coefficient; ARMS-PCR, amplification refractory mutation system-polymerase chain reaction; NGS, next-generation sequencing technology; EGFR, epidermal growth factor receptor; ALK, anaplastic lymphoma kinase; KPS, Karnofsky Performance Scores.
Acknowledgment
The general programs of the National Natural Science Foundation of China (81272351) supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Riihimaki M, Hemminki A, Fallah M, et al. Metastatic sites and survival in lung cancer. Lung Cancer. 2014;86(1):78–84. doi:10.1016/j.lungcan.2014.07.020
2. Fox BD, Cheung VJ, Patel AJ, Suki D, Rao G. Epidemiology of metastatic brain tumors. Neurosurg Clin N Am. 2011;22(1):1–6. doi:10.1016/j.nec.2010.08.007
3. Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75(1):5–14. doi:10.1007/s11060-004-8093-6
4. Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004;22(14):2865–2872. doi:10.1200/JCO.2004.12.149
5. Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol. 2002;249(10):1357–1369. doi:10.1007/s00415-002-0870-6
6. Kotecha R, Gondi V, Ahluwalia MS, Brastianos PK, Mehta MP. Recent advances in managing brain metastasis. F1000Research. 2018;7. doi:10.12688/f1000research.15903.1
7. Saito EY, Viani GA, Ferrigno R, et al. Whole brain radiation therapy in management of brain metastasis: results and prognostic factors. Radiat Oncol. 2006;1:20. doi:10.1186/1748-717X-1-20
8. Thon N, Kreth FW, Tonn JC. The role of surgery for brain metastases from solid tumors. Handb Clin Neurol. 2018;149:113–121.
9. Schild SE, Sio TT, Daniels TB, Chun SG, Rades D. Prophylactic cranial irradiation for extensive small-cell lung cancer. J Oncol Pract. 2017;13(11):732–738. doi:10.1200/JOP.2017.026765
10. Delattre JY, Krol G, Thaler HT, Posner JB. Distribution of brain metastases. Arch Neurol. 1988;45(7):741–744. doi:10.1001/archneur.1988.00520310047016
11. Kindt GW. The pattern of location of cerebral metastatic tumors. J Neurosurg. 1964;21:54–57. doi:10.3171/jns.1964.21.1.0054
12. Ask-Upmark E. Metastatic tumours of the brain and their localization. Acta Med Scand. 1956;154(1):1–9. doi:10.1111/j.0954-6820.1956.tb14295.x
13. Takano K, Kinoshita M, Takagaki M, et al. Different spatial distributions of brain metastases from lung cancer by histological subtype and mutation status of epidermal growth factor receptor. Neuro Oncol. 2016;18(5):716–724. doi:10.1093/neuonc/nov266
14. Kyeong S, Cha YJ, Ahn SG, Suh SH, Son EJ, Ahn SJ. Subtypes of breast cancer show different spatial distributions of brain metastases. PLoS One. 2017;12(11):e0188542. doi:10.1371/journal.pone.0188542
15. Ekici K, Temelli O, Dikilitas M, Halil Dursun I, Bozdag Kaplan N, Kekilli E. Survival and prognostic factors in patients with brain metastasis: single center experience. J Buon. 2016;21(4):958–963.
16. Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. doi:10.1056/NEJMoa0810699
17. Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239–246.
18. Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31(27):3327–3334. doi:10.1200/JCO.2012.44.2806
19. Wu SG, Rao MY, Zhou J, et al. Distribution of metastatic disease in the brain in relation to the hippocampus: a retrospective single-center analysis of 6064 metastases in 632 patients. Oncotarget. 2015;6(41):44030–44036. doi:10.18632/oncotarget.5828
20. Ribatti D, Mangialardi G, Vacca A. Stephen Paget and the ‘seed and soil’ theory of metastatic dissemination. Clin Exp Med. 2006;6(4):145–149. doi:10.1007/s10238-006-0117-4
21. van Laar PJ, Hendrikse J, Golay X, Lu H, van Osch MJP, van der Grond J. In vivo flow territory mapping of major brain feeding arteries. NeuroImage. 2006;29(1):136–144. doi:10.1016/j.neuroimage.2005.07.011
22. Weidle UH, Birzele F, Kollmorgen G, Ruger R. Dissection of the process of brain metastasis reveals targets and mechanisms for molecular-based intervention. Cancer Genomics Proteomics. 2016;13(4):245–258.
23. Hendrikse J, van der Grond J, Lu H, van Zijl PC, Golay X. Flow territory mapping of the cerebral arteries with regional perfusion MRI. Stroke. 2004;35(4):882–887. doi:10.1161/01.STR.0000120312.26163.EC
24. Ge M, Zhuang Y, Zhou X, Huang R, Liang X, Zhan Q. High probability and frequency of EGFR mutations in non-small cell lung cancer with brain metastases. J Neurooncol. 2013;31(27):413–418. doi:10.1007/s11060-017-2590-x
25. Li B, Sun SZ, Yang M, et al. The correlation between EGFR mutation status and the risk of brain metastasis in patients with lung adenocarcinoma. J Neurooncol. 2015;124(1):79–85. doi:10.1007/s11060-015-1776-3
26. Shigematsu H, Gazdar AF. Somatic mutations of epidermal growth factor receptor signaling pathway in lung cancers. Int J Cancer. 2006;118(2):257–262. doi:10.1002/(ISSN)1097-0215
27. Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–2388. doi:10.1056/NEJMoa0909530
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.