Back to Journals » Clinical Ophthalmology » Volume 20
Discontinuing Anti-VEGF Therapy in Patients with Neovascular Age-Related Macular Degeneration That Remains Inactive with Treatment at the Maximum Injection Interval
Authors Şatırtav G ![]() , Lövestam-Adrian MK, Chang W, Charles M, Chen LJ, Cheung CMG, Kodjikian L, Ohji M, Zinkernagel M, Wolf S
, Lövestam-Adrian MK, Chang W, Charles M, Chen LJ, Cheung CMG, Kodjikian L, Ohji M, Zinkernagel M, Wolf S
Received 11 December 2025
Accepted for publication 16 May 2026
Published 26 June 2026 Volume 2026:20 587803
DOI https://doi.org/10.2147/OPTH.S587803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Günhal Şatırtav,1 Monica Karin Lövestam-Adrian,2 Woohyok Chang,3 Martín Charles,4 Lee-Jen Chen,5 Chui Ming Gemmy Cheung,6,7 Laurent Kodjikian,8,9 Masahito Ohji,10 Martin Zinkernagel,11 Sebastian Wolf11
1Department of Ophthalmology, Meram Faculty of Medicine, Necmettin Erbakan University, Konya, Turkey; 2Department of Ophthalmology, Lund University Hospital, Lund, Sweden; 3Chang’s Retina Center, Daegu, South Korea; 4Charles Centro Oftalmológico, Buenos Aires, Argentina; 5Department of Ophthalmology, Mackay Memorial Hospital, Taipei, Taiwan; 6Singapore Eye Research Institute, Singapore National Eye Centre, Singapore, Singapore; 7Duke-NUS Medical School, National University of Singapore, Singapore, Singapore; 8Department of Ophthalmology, Croix-Rousse University Hospital, Hospices Civils de Lyon, Lyon, France; 9University of Lyon 1, UMR5510 MATEIS, CNRS, INSA Lyon, Villeurbanne, France; 10Department of Ophthalmology, Shiga University of Medical Science, Otsu, Japan; 11Department of Ophthalmology, Inselspital, University of Bern, Bern, Switzerland
Correspondence: Günhal Şatırtav, Department of Ophthalmology, Meram Faculty of Medicine, Necmettin Erbakan University, Konya, Turkey, Email [email protected]
Abstract: This review aims to provide guidance on the management of patients with neovascular age-related macular degeneration (nAMD) whose disease becomes inactive on anti-vascular endothelial growth factor (VEGF) treatment. The Vision Academy’s membership of international retinal disease experts reviewed the literature and developed consensus recommendations and an algorithm to determine the appropriate timing of treatment suspension and a post-treatment follow-up strategy for appropriate patients with nAMD who achieve a good response to anti-VEGF therapy. Patients with inactive disease (defined as absence of both intraretinal and subretinal fluid, absence of deterioration in vision, and absence of new retinal hemorrhage) for at least three consecutive maximum treatment intervals as outlined in the clinic’s protocol may be considered for treatment exit. However, in patients with stable disease that remains active and those with only one good seeing eye and a history of disease recurrence, treatment continuation may be preferred. An appropriate interval for continued monitoring with optical coherence tomography and visual acuity testing should be decided following discussion with the patient and consideration of patient-specific factors. This article presents consensus guidelines for nAMD management in patients who respond well to anti-VEGF therapy, and for the discontinuation of treatment in cases of success.
Keywords: intravitreal injections, inactive disease, treatment discontinuation, treatment success
Introduction
Neovascular age-related macular degeneration (nAMD) is a condition that causes significant and progressive vision loss.1,2 Monthly or bi-monthly anti-vascular endothelial growth factor (VEGF) injections have been proven to improve functional and anatomical results in patients with nAMD in pivotal studies.3–5 However, there are large, inter-individual variations in anti-VEGF drug response, in terms of both functional and morphological characteristics.6 Anti-VEGF therapeutic response has been shown to be influenced by a number of parameters, including patient age, lesion features, lesion duration, baseline visual acuity, and the existence of certain genetic risk alleles.6 To alleviate the treatment burden, customized treatment regimens were designed to minimize the number of required clinic visits and injections.5,7 In personalized approaches where treatment is largely of a dry retina, there may be uncertainty over whether disease is considered stable or inactive and hence whether anti-VEGF medication should be discontinued in cases of functional and morphological stability.
The Vision Academy previously established guidelines for the suspension of anti-VEGF medication in cases of futility, where patients with nAMD do not respond well to anti-VEGF treatment.8 The purpose of the present article is to examine the rationale for discontinuing anti-VEGF medication in patients who have responded favorably to treatment, and to provide guidelines for case selection and strategies for monitoring after discontinuation of therapy.
Methods
This article is based on a review of the literature and consensus among retinal experts from the Vision Academy. The Vision Academy comprises an international group of over 80 retinal physicians who work together to share skills and knowledge and to provide recommendations, based on their collective clinical expertise, on clinical challenges in areas where there is a lack of conclusive evidence in the literature (www.visionacademy.org).
Two comprehensive literature searches were performed using the PubMed database (from December 22, 2008, to March 17, 2026) to identify articles published in English that investigated exit from intravitreal anti-VEGF treatment regimens in patients with nAMD who had responded well to therapy. The search strategy is summarized in Table 1. A single reviewer (GS) screened titles and abstracts for eligibility. Articles discussing studies with treatment discontinuation were selected for review. An algorithm including criteria for the suspension of anti-VEGF treatment in patients with nAMD with successful outcomes (Figure 1) was developed based on the findings of the literature search and the collective expertise of the authors. The recommendations contained within the algorithm were subsequently reviewed, commented upon, and endorsed by a majority of the Vision Academy membership before finalization. Vision Academy members were asked to rate their agreement with the proposed recommendations using the options “strongly agree”, “agree”, “neither agree nor disagree”, “disagree”, and “strongly disagree”. Responses from more than 50% of members were required for the survey to be valid. Respondents were also asked for the reimbursement status of treatment in their country of practice (ie, mostly reimbursed or mostly out of pocket) to determine whether this may have influenced their responses. Biases were assessed using χ2. Endorsement was considered “strong” if 75% or more of respondents indicated that they agreed or strongly agreed with a recommendation. The list of Vision Academy members who contributed to the recommendations is provided at the end of the article.
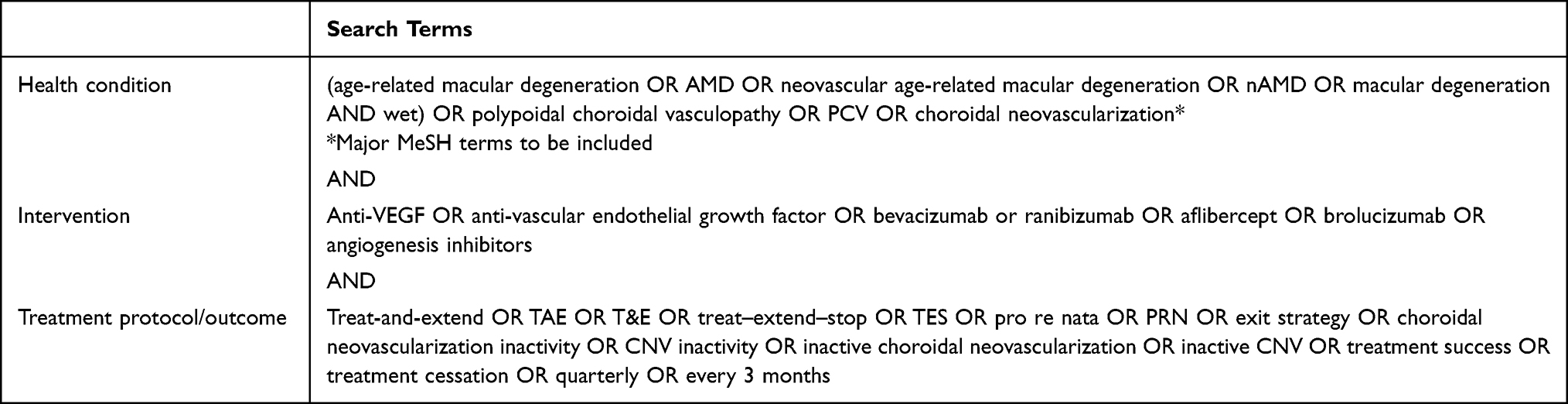 |
Table 1 Search Terms and Search Strategy |
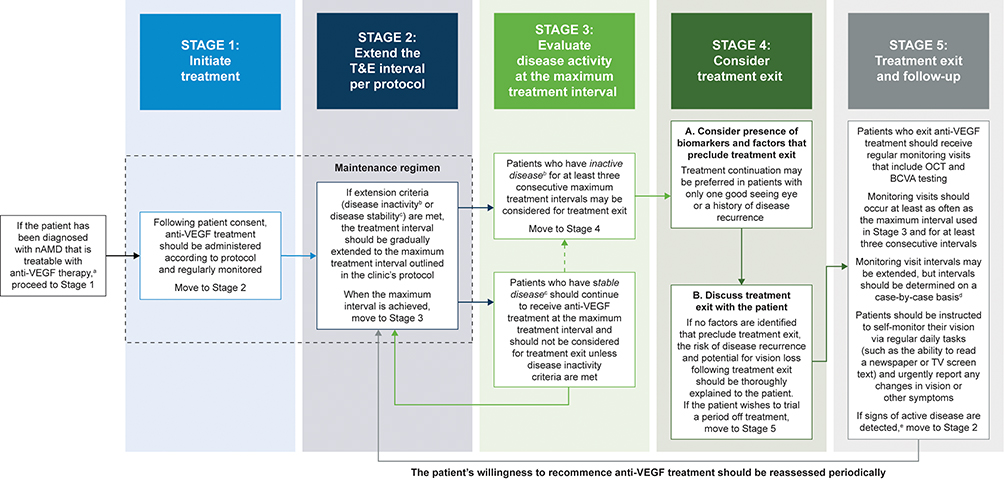 |
Figure 1 Algorithm for considering treatment exit in patients with nAMD who respond well to anti-VEGF therapy. Abbreviations: BCVA, best corrected visual acuity; IRF, intraretinal fluid; MNV, macular neovascularization; nAMD, neovascular age-related macular degeneration; OCT, optical coherence tomography; SRF, subretinal fluid; T&E, treat-and-extend; VEGF, vascular endothelial growth factor. Note: aThe patient must have unilateral or bilateral nAMD in the eye in question; bDisease inactivity is defined as the absence of IRF and SRF attributable to VEGF activity, absence of deterioration in vision attributable to MNV activity, and absence of new retinal hemorrhage attributable to MNV activity; cDisease stability is defined as no fluid or a small amount of persistent residual SRF without a further decrease, despite adequate regular injections, until maximal anatomic effect (with at least an initial three monthly injections during the induction phase). In this case, and only in the absence of any other signs of disease activity, the disease can be considered stable and the treatment interval maintained or cautiously increased; dAn appropriate interval for continued monitoring should be decided after careful discussion of risk profile and visual potential of the affected eye and the fellow eye, at the physician’s discretion; eDisease activity is defined as the presence of IRF and/or SRF attributable to VEGF activity, deterioration in vision attributable to MNV activity, presence of new retinal hemorrhage attributable to MNV activity, and/or an increasing amount of SRF/IRF despite regular injections. |
Results
The optimal exit strategy for suspending treatment in patients with inactive nAMD is unclear. In this article, the Vision Academy aims to provide guidance for treatment exit with a preplanned follow-up strategy in patients with successful treatment responses in order to prevent potentially unnecessary lifelong treatment. Response to treatment is generally considered good if the disease is inactive, as defined in the “Disease activity, stability, and inactivity criteria” section below.
Disease Activity, Stability, and Inactivity Criteria
Anti-VEGF treatments are beneficial in nAMD; however, not all patients benefit in the same way in terms of functional and morphological results. Measurement of treatment response using both visual function and morphological indicators assessed with optical coherence tomography has been used in pivotal studies.6,7,9,10
The Vision Academy has recently published recommendations on how to define disease activity, stability, and inactivity that take account of evidence from large clinical trials regarding the impact of different types of residual retinal fluid on treatment outcomes (Table 2). According to these recommendations, inactive disease is defined as the absence of all of the following: intraretinal fluid and subretinal fluid attributable to VEGF activity; deterioration in vision attributable to macular neovascularization activity; and new retinal hemorrhage attributable to macular neovascularization activity.11 Treatment exit should be considered only in cases of inactive age-related macular degeneration, with treatment continuation being advised in cases of stable disease.12–14
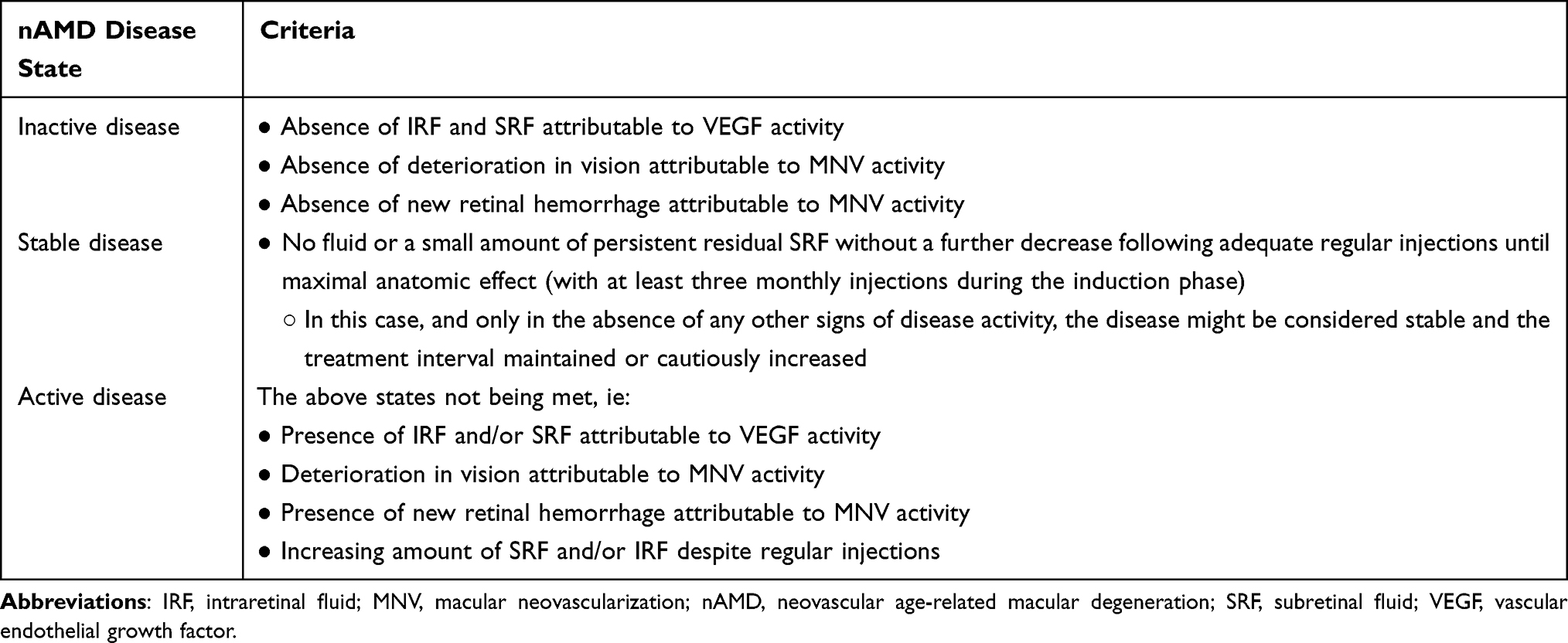 |
Table 2 Vision Academy Definitions of nAMD Disease States11 |
Treatment Regimens, Maximum Re-Treatment Intervals, and Exit Criteria
While the extension and reduction of treatment intervals are clearly characterized in published research, there is much controversy regarding the maximum treatment interval, and evidence of the effects of exit strategies when treating patients using a treat-and-extend (T&E) protocol is limited. In pro re nata (PRN; “as needed”) trials, the number of injections required in a particular period of time varied significantly among patients.5,9 Different maximum treatment intervals and treatment protocols have been used for stability requirements in investigations where a treatment exit was envisaged (Table 3). Several studies used disease stability at three consecutive 12- or 16-week treatment intervals as the criterion for discontinuing anti-VEGF treatment (Table 3).12,15–17
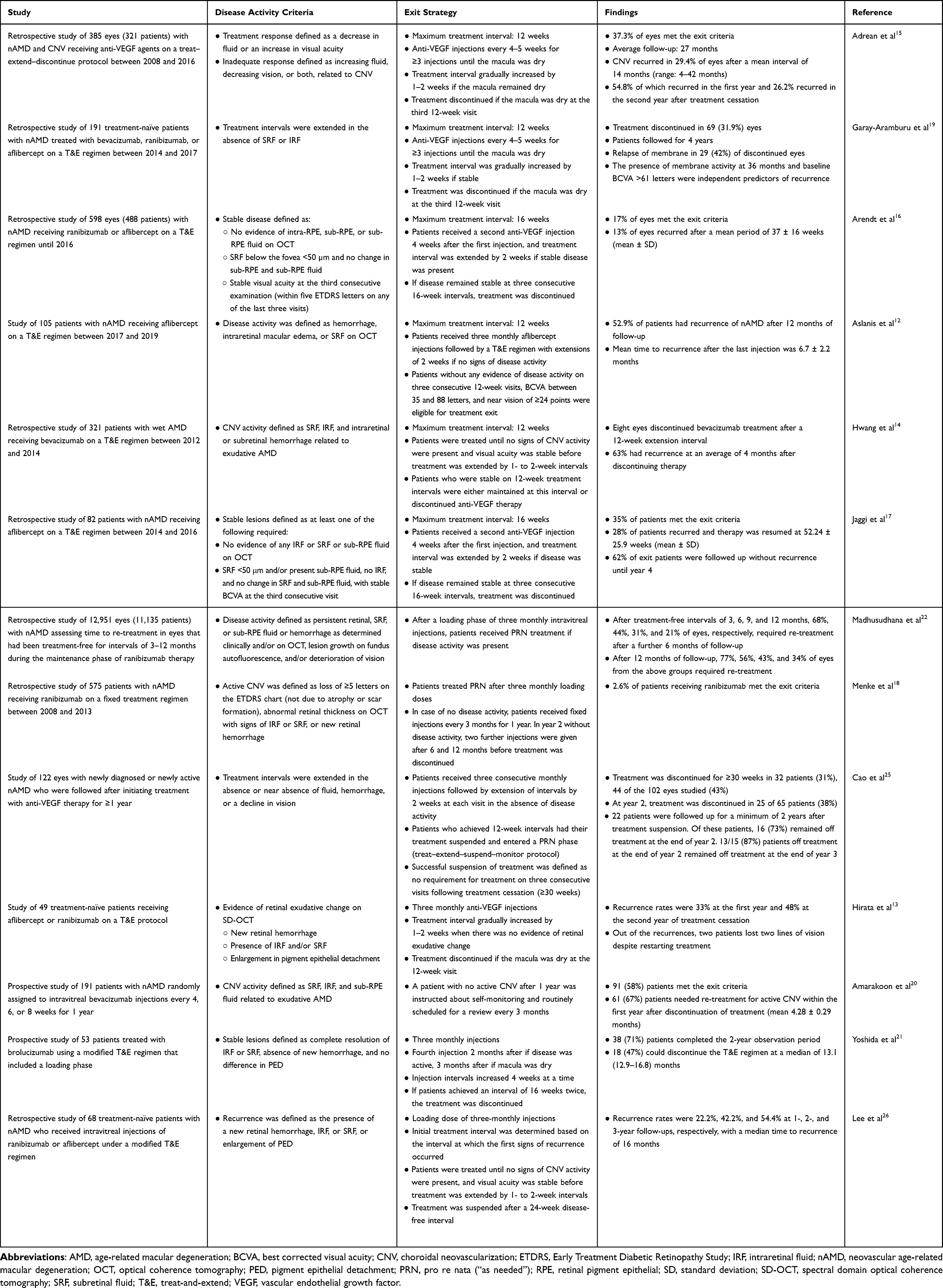 |
Table 3 Exit Criteria and Outcomes in Studies Where Anti-VEGF Treatment for nAMD Was Discontinued |
Menke et al18 reported the outcome of patients with exudative age-related macular degeneration who met the exit criteria of the Bern treatment regime. Patients with no disease activity after the loading phase received fixed injections every 3 months for the first year of follow-up, then fixed injections at 6 and 12 months in the second year of follow-up, before therapy was stopped (Table 3).
Several studies have investigated anti-VEGF treatment exit following T&E regimens in patients with nAMD (Table 3). Adrean et al15 found that 37.3% of eyes met the criteria for discontinuing therapy (a dry macula at three consecutive 12-week visits) after an average of 27 months of follow-up, while disease recurrence was reported in 29.4% of eyes after an average of 14 months (range: 4–42 months). Similarly, Garay-Aramburu et al19 discontinued therapy in 31.9% of their patients after inactivity following three consecutive 12-week injections. They have observed relapse of the membrane in 42% of these patients in a 4-year follow-up. Arendt et al16 and Jaggi et al17 gradually extended the treatment interval in patients who were stable after a loading dose, and reported that patients met the exit requirements at three consecutive 16-week intervals, with disease recurrences observed in 13% and 28%, respectively. Amarakoon et al20 evaluated recurrence rates at 1 year after treatment cessation in patients who had been treated with fixed-interval dosing (4, 6, or 8 weeks), finding an overall reactivation rate of 67% with a mean time to recurrence of 4.28 ± 0.29 months, regardless of the previous injection frequency. The patients included in these studies were treated with bevacizumab, ranibizumab, or aflibercept, and the maximum treatment interval or treatment cycle was not determined by the specific agent used.15–17 In the era of second-generation anti-VEGF agents, a 2-year prospective study by Yoshida et al21 showed that 47% of eyes discontinued treatment after reaching a 16-week interval twice and a recurrence rate of 5.6% was observed during the 1-year follow-up period. Thus, between-study variations in the rates of disease recurrence may not be attributable solely to differences in maximal treatment intervals, with other factors potentially also playing a role.
Exit criteria and outcomes in studies where anti-VEGF treatment for nAMD was stopped are listed in Table 3. With most of the studies following a T&E protocol, only two have followed or incorporated a PRN regime. A retrospective study by Madhusudhana et al22 followed a PRN protocol and reported that a high proportion of patients required re-treatment after treatment cessation, and a study by Menke et al18 used a capped PRN protocol and reported a low proportion of patients meeting exit criteria. A study by Arendt et al,16 employing a T&E regimen, observed a higher proportion of patients achieving the exit criteria (Table 3) compared to the findings from Menke et al.18 Arendt et al suggested that this difference between the T&E and PRN studies may have been due to possible undertreatment in the PRN study with more disease recurrences; this, in turn, may have resulted in a lower likelihood of patients on a PRN regimen reaching the predefined exit criteria. However, Liu et al23 reported no significant disparity in the rates of long-term remission or the incidence of recurrence between patients managed with PRN vs. T&E protocols.
Biomarkers to Guide Treatment Exit
Studies have been reported of several morphological and demographic prognostic indicators that can predict response to therapy in nAMD.24 Patients with posterior vitreous detachment require significantly fewer injections than those with vitreomacular adhesion, and also meet the treatment exit criteria more frequently. Also, patients with an epiretinal membrane have a lower likelihood of achieving treatment-free disease stability than patients without an epiretinal membrane27 (Table 4).
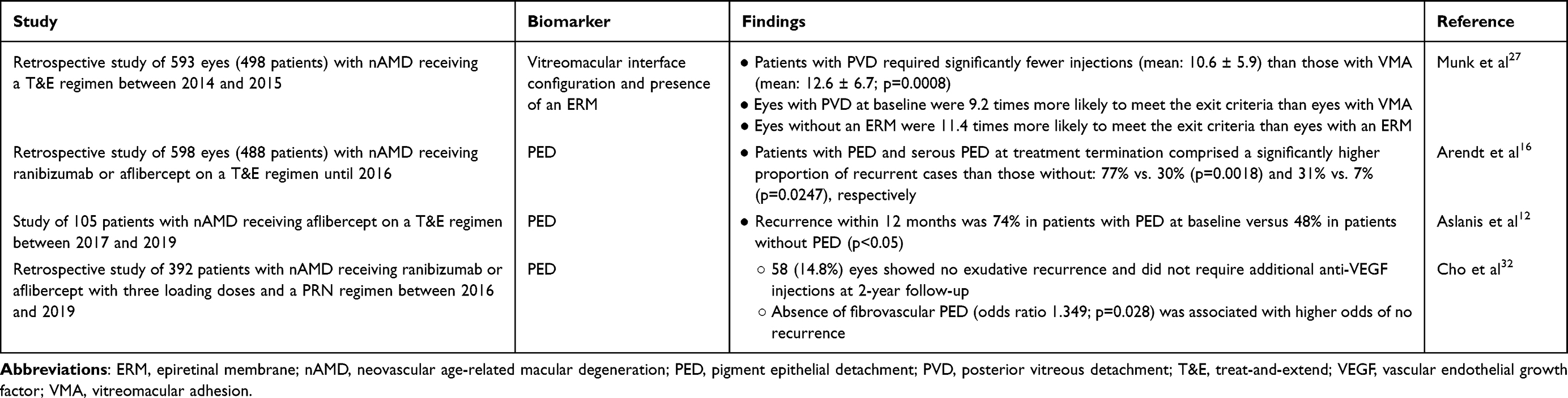 |
Table 4 Biomarkers for Anti-VEGF Treatment Exit and Disease Recurrence |
In a post hoc analysis of the results of the VIEW 1 and VIEW 2 studies, patients with baseline pigment epithelial detachment were less likely to achieve improvement in visual acuity from baseline, and were more likely to experience disease reactivation when switched from a fixed-dose regimen to a flexible-dose regimen.28,29 Several studies have also implicated the presence of serous pigment epithelial detachment in increased risk of disease recurrence in patients exiting anti-VEGF treatment (Table 4), suggesting that serous pigment epithelial detachment may be a helpful imaging marker for risk stratification when considering discontinuation of anti-VEGF treatment.12,16
Post-Exit Follow-Up and Recurrence
In cases of planned suspension of a treatment regimen, the follow-up approach should be properly managed, with the goal of detecting any prospective recurrences in a timely manner while limiting unnecessary visits. Numerous studies have examined the rates of recurrence of disease in patients with nAMD following stabilization across maximum treatment intervals (Table 3).
In a study by Hwang et al,14 patients were offered the option of continuing bevacizumab maintenance treatment at 12-week intervals or undergoing a trial off treatment. Recurrence was evident in 63% of eyes after an average of 4 months (16 weeks) since discontinuing maintenance therapy (Table 3).
Aslanis et al12 reported evidence of nAMD recurrence in 52.9% of patients who discontinued T&E aflibercept injections on achieving disease stability (Table 3), with a mean time to recurrence of 6.7 ± 2.2 months. In 85.2% of these patients, the recurrence occurred during the first 8 months of follow-up.12 Hirata et al13 reported nAMD recurrence rates of 33% in the first year and 48% in the second year after cessation of treatment with aflibercept or ranibizumab in patients receiving treatment under a T&E protocol where treatment intervals were extended to over 12 weeks (Table 3).
A study using a national UK database assessed time to re-treatment in eyes with nAMD treated with ranibizumab.22 Following the treatment-free intervals of 3, 6, 9, or 12 months and a further 6 months of follow-up, 68%, 44%, 31%, and 21% of eyes, respectively, needed re-treatment.22
Adrean et al15 investigated the disease recurrence rates in a treat–extend–discontinue paradigm where therapy was discontinued at the third 12-week visit until recurrence, which was reported in 29.4% of eyes after a mean interval of 14 months (range: 4–42 months; Table 3). Arendt et al16 and Jaggi et al17 established a 16-week maximum treatment interval following a T&E regimen and permitted patients to discontinue therapy after three consecutive injections at the maximum interval. Disease recurrence was reported in 13% of eyes after 37 ± 16 weeks (mean ± standard deviation) in the study by Arendt et al, and in 28% of patients after 52.24 ± 25.9 weeks in the study by Jaggi et al, respectively (Table 3). In a long-term real-world analysis with a mean follow-up of 8.1 ± 3.4 years, Cho et al30 reported that while 66% of eyes eventually met the criteria for treatment discontinuation, 66.8% of those eyes with initial stable responses subsequently experienced disease recurrence. Although the median time to reactivation was 3.3 years, late-onset recurrences were observed up to 10 years after treatment cessation. In a study by Lee et al26 recurrence rates at 1, 2, and 3 years of follow-up were 22.2%, 42.2%, and 54.4%, respectively, after a T&E protocol with a maximum treatment interval of 24 weeks. While disparities in recurrence rates cannot be directly linked to differences in maximum treatment intervals, they should be taken into account.
In two of the trials with a defined exit strategy, a follow-up time of 3–4 months was designated following the cessation of medication.16,27 Adrean et al15 used a more stepwise follow-up technique with patients followed up for 4 weeks after discontinuation and examined again in a progressive method, extending the follow-up duration by 2 weeks at a time until it reached 12 weeks. Patients were then followed up at 3-monthly intervals.15 In a study by Garweg et al,31 patients with stable disease opted to either continue treatment at intervals of 12–14 weeks or discontinue treatment and attend follow-up visits every 8–12 weeks. Recurrent disease was observed in both groups, with the time from the achievement of stable disease to recurrence being comparable between the two strategies.31
Other Considerations for Treatment Exit
Numerous papers demonstrate an increased risk of intraocular hemorrhagic consequences in individuals with nAMD who are using antiplatelet or anticoagulant medicines. Kiernan et al33 reported an annual incidence of combined subretinal and vitreous hemorrhage of 0.009% in patients receiving daily antiplatelet or anticoagulant drugs and 0.001% in patients not receiving them. Additionally, Kuhli-Hattenbach et al34 reported that patients receiving antithrombotic medication had considerably greater subretinal hemorrhages (mean: 9.71-disc areas) than those who did not. While the evidence is limited concerning possible complications of antiplatelet or anticoagulant medications in patients with nAMD, their risks should be considered before treatment exit.
Treatment continuation may be preferred in patients with the only eye that is being treated, especially if the vision loss of the contralateral eye has been secondary to undertreatment or subretinal fibrosis.
Discussion and Vision Academy Recommendations
There is a lack of guidance on the criteria for determining when discontinuation of anti-VEGF treatment should be considered for patients with nAMD who have responded favorably to therapy. Based on a review of the published literature and our collective experience, we propose a five-stage algorithm to assist ophthalmologists in identifying patients who may be candidates for treatment discontinuation (Figure 1).
The recommendations listed below were formulated by the authors and submitted to the entire Vision Academy membership for endorsement; 72 responses (including from the authors) were received. Overall, the recommendations were endorsed by 92.4% of the respondents (a response of “agree” or “strongly agree”), with the level of endorsement for each individual recommendation ranging from 84.7% to 98.6%. The mean rate of non-endorsement was 7.72% (1.4–31.9%) for a response of either “disagree” or “strongly disagree” and 3.24% (0–5.6%) for a response of “neither agree nor disagree”. One recommendation was not endorsed (<75% of respondents selected “agree” or “strongly agree”) and was subsequently revised based on the feedback and submitted to the authors and the Vision Academy Steering Committee for re-endorsement. It should be noted that these recommendations represent the ideal scenario, and full implementation may not be possible in all clinics.
Stage 1: Initiate treatment after obtaining the patient’s consent to intravitreal injections of anti-VEGF therapy in accordance with the protocol, and regularly monitor to assess nAMD activity as defined in Table 2 and reassess periodically the patient’s willingness to receive anti-VEGF treatment.
Stage 2: Extend the T&E interval per protocol. If disease inactivity or disease stability is achieved based on both functional and morphological changes, extend the T&E interval per protocol (Table 2). The T&E interval should be gradually extended, per protocol, to the maximum treatment interval outlined in the clinic’s protocol.
Stage 3: Evaluate disease activity at the maximum treatment interval. Patients who have inactive disease (Table 2) for at least three consecutive maximum intervals or for a predefined period of time may be considered for treatment exit. Patients who have stable disease (Table 2) should continue receiving anti-VEGF treatment at the maximum treatment interval and should not be considered for treatment exit unless the disease inactivity criteria are met. If the disease inactivity criteria are not met, patients should continue to receive anti-VEGF treatment.
Stage 4: Consider treatment exit. Consider the presence of factors that may preclude treatment exit. Treatment continuation may be preferred in patients with only one good seeing eye or in those with a history of disease recurrence. Discuss treatment exit with the patient and thoroughly explain the risk of disease recurrence and potential for vision loss following treatment exit. If no factors are identified that preclude treatment exit, discuss with the patient whether they wish to trial a period off treatment.
Stage 5: Treatment exit and follow-up. Patients who wish to trial a period off anti-VEGF treatment should attend regular monitoring visits that include optical coherence tomography and best corrected visual acuity testing. Monitoring visits should occur at least as often as the maximum treatment interval used in Stage 3, and for at least three consecutive intervals. Monitoring visits may be extended, but intervals should be determined on a case-by-case basis after careful discussion of risk profile and visual potential of the affected and the fellow eye, at the physician’s discretion. Patients should be instructed to self-monitor their vision via regular daily tasks (such as the ability to read a newspaper or TV screen text) and urgently report any changes in vision or other symptoms, without waiting for the next appointment. Patients should be made aware of the significance of monitoring both eyes separately and adhering to follow-up appointments in order to prevent potential recurrences in the treated eyes and potential activation of nAMD in the untreated eyes. If signs of active disease are detected (Table 2), treatment should be reinitiated. While earlier reports raised concerns about VEGF suppression and macular atrophy, more recent data from the RIVAL and TREX-AMD studies35,36 indicate that macular atrophy reflects the natural history of the underlying disease rather than a treatment side effect. Nevertheless, Stage 5 facilitates a transition to monitoring in inactive cases, ensuring anatomical stability while avoiding unnecessary treatment.
Beyond clinical outcomes, the sustainability of lifelong anti-VEGF therapy is a growing concern. In practice, “indefinite” treatment often leads to clinic overcrowding, which can delay care for new patients or cases with active lesions. Our algorithm provides a clear exit strategy that helps reclaim outpatient capacity, ensuring limited medical resources are focused where they are most needed and making nAMD management more sustainable for both the clinic and the healthcare system.
Future Perspectives
The management of nAMD is transitioning towards higher-durability therapies that allow for more rapid extension of treatment intervals. In the PULSAR trial, aflibercept 8 mg demonstrated substantial durability; by Week 96, 53% of patients maintained dosing intervals of 20 weeks or longer, and 31% reached a 24-week interval.37 Similarly, 2-year data from the TENAYA and LUCERNE trials showed that 59–67% of patients treated with faricimab remained on a 16-week schedule, with post hoc analyses suggesting that a specific subset could extend to 20-week intervals.38,39 These clinical trial findings are supported by real-world evidence, such as the “treat, extend, and stop” protocol used with brolucizumab, where patients successfully discontinued therapy after remaining stable through two consecutive 16-week intervals.21
Future strategies are expected to incorporate sustained-release platforms, such as tyrosine kinase inhibitor implants (eg, OTX-TKI, EYP-1901) and port delivery systems, to maintain continuous VEGF inhibition over extended periods.40 Furthermore, the development of gene therapy (eg, RGX-314) represents a significant frontier, aiming to provide a single-administration approach by enabling the retina to continuously produce therapeutic proteins, potentially eliminating the need for regular injections.41 Combining these long-acting delivery systems with routine genomic profiling – specifically identifying patients at lower risk of recurrence, such as those lacking the ARMS2 A69S risk allele – may establish a structured and safer strategy for discontinuation of therapy.42,43 Overall, the enhanced durability of these next-generation agents is expected to better support successful treatment discontinuation by maintaining longer periods of disease inactivity.
Conclusion
This article provides guidelines for the management of patients with nAMD who respond well to anti-VEGF medication. We present a treatment success algorithm using predetermined treatment protocols, a variety of biomarkers, and clinical indications, to help practitioners distinguish patients with nAMD with a good response to anti-VEGF treatment, who may be candidates for treatment exit. Additionally, the algorithm includes a post-treatment follow-up strategy to aid detection of prospective disease recurrences and avoid the need for late intervention.
Abbreviations
AMD, age-related macular degeneration; BCVA, best corrected visual acuity; CNV, choroidal neovascularization; ERM, epiretinal membrane; ETDRS, Early Treatment Diabetic Retinopathy Study; IRF, intraretinal fluid; MNV, macular neovascularization; nAMD, neovascular age-related macular degeneration; OCT, optical coherence tomography; PED, pigment epithelial detachment; PRN, pro re nata (“as needed”); PVD, posterior vitreous detachment; RPE, retinal pigment epithelial; SD, standard deviation; SD-OCT, spectral domain optical coherence tomography; SRF, subretinal fluid; T&E, treat-and-extend; VEGF, vascular endothelial growth factor; VMA, vitreomacular adhesion.
Acknowledgments
The authors would like to thank the members of the Vision Academy who aided the development of the Vision Academy recommendations. The following Vision Academy members and mentees reviewed and commented on the original recommendations drafted by the authors, thereby significantly contributing to the development and finalization of the recommendations presented in this article: Archana Airody, Winfried Amoaku, Jennifer Arnold, Tariq Aslam, Stéphanie Baillif, Vilma Jūratė Balčiūnienė, Francesco Bandello, Daniel Barthelmes, Francine Behar-Cohen, Sophie Bonnin, Claudia Brockmann, Ângela Maria Veloso Guimarães Carneiro, Irini Chatziralli, Shih-Jen Chen, Catherine Creuzot-Garcher, Alan Cruess, José Cunha-Vaz, Carla Danese, Corinne Dot, Bora Eldem, Claudia Virgínia Louro Farinha, Luisa Frizziero, Kenneth Fong, Richard Gale, Robyn Guymer, Horst Helbig, Polona Jaki Mekjavić, Keiko Kataoka, Adrian Koh, Mineo Kondo, Jean-François Korobelnik, Anthony Kwan, Timothy Lai, Paolo Lanzetta, Xiaoxin Li, Anat Loewenstein, Thibaud Mathis, Hemal Mehta, Marion Munk, Toshinori Murata, Annabelle Okada, Mali Okada, Daniel Pauleikhoff, Cynthia Qian, Francisco Rodríguez, Paisan Ruamviboonsuk, Figen Şermet, Sobha Sivaprasad, Giovanni Staurenghi, Anastasios Stavrakakis, Simon Szeto, Kelvin Yi Chong Teo, Sarah Touhami, Miltiadis Tsilimbaris, Akitaka Tsujikawa, Patricia Udaondo, Aistė Varoniukaitė, Francesco Viola, Sebastian Waldstein, Peter van Wijngaardenm, Tien Yin Wong, Lihteh Wu, Young Hee Yoon, Javier Zarranz-Ventura, and Dinah Zur. Medical writing support, under the direction of the authors, was provided by Hollie Robinson, PhD, and Macha Aldighieri, PhD, of the Publications Division of Omnicom Health Medical Communications, funded by Bayer Consumer Care AG, Pharmaceuticals Division, Basel, Switzerland, in accordance with Good Publication Practice (GPP 2022) guidelines. Editorial support was provided by Rebecca Fletcher, BA (Hons), and Rachel Fairbanks, BA (Hons), of the Publications Division of Omnicom Health Medical Communications, funded by Bayer Consumer Care AG, Pharmaceuticals Division, Basel, Switzerland.
Author Contributions
All authors: made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical writing and editorial assistance was funded by Bayer Consumer Care AG, Pharmaceuticals Division, Basel, Switzerland, in accordance with Good Publication Practice (GPP 2022) guidelines.
Disclosure
GŞ: Funding: AbbVie. Honoraria: Bayer. MLA: Consultant: AbbVie, Bayer, Novartis, Roche. Funding: Bayer. WC: Consultant: Alcon, Bayer, Roche. Honoraria: AbbVie, Alcon, Bayer, Roche. MC: Consultant: Alcon, Bayer, Roche. LJC: Consultant: Bayer, Novartis, Roche. Honoraria: Bayer, Roche. CMGC: Consultant: Astellas, Bayer, Boehringer Ingelheim, Novartis, Roche, Zeiss. Funding: Bayer, Boehringer Ingelheim, Novartis, Roche. Honoraria: Bayer, Roche, Zeiss. LK: Consultant: AbbVie, Alcon, Alimera-Horus, Bayer, Horus, Novartis, Roche, Théa. MO: Consultant: Chugai. Funding: Alcon Japan, Bayer, Nikon, Otsuka, Santen, Senju. Honoraria: AMO, Chugai, Jonan Medical, Otsuka, Santen, Senju. MZ: Consultant: Alcon, Annexon, Bayer, BCNPeptides, Janssen, Novartis, Oculis, PeriVision, Roche. Funding: Bayer, Boehringer Ingelheim, Heidelberg Engineering. SW: Consultant: Bayer, Celltrion, Heidelberg Engineering, La Science, Novartis, Ocular Therapeutix, Oculis, Roche, Zeiss. Honoraria: Bayer. The authors report no other conflicts of interest in this work.
References
1. Coleman HR, Chan CC, Ferris FL, et al. Age-related macular degeneration. Lancet. 2008;372(9652):1835–13. doi:10.1016/s0140-6736(08)61759-6
2. Lim JH, Wickremasinghe SS, Xie J, et al. Delay to treatment and visual outcomes in patients treated with anti-vascular endothelial growth factor for age-related macular degeneration. Am J Ophthalmol. 2012;153(4):678–686.e1–2. doi:10.1016/j.ajo.2011.09.013
3. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57–65. doi:10.1016/j.ophtha.2008.10.018
4. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
5. Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO study. Am J Ophthalmol. 2009;148(1):43–58. doi:10.1016/j.ajo.2009.01.024
6. Amoaku WM, Chakravarthy U, Gale R, et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye. 2015;29(6):721–731. doi:10.1038/eye.2015.48
7. Wykoff CC, Croft DE, Brown DM, et al. Prospective trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: TREX-AMD 1-year results. Ophthalmology. 2015;122(12):2514–2522. doi:10.1016/j.ophtha.2015.08.009
8. Wong DT, Lambrou GN, Loewenstein A, et al. Suspending treatment of neovascular age-related macular degeneration in cases of futility. Retina. 2020;40(6):1010–1020. doi:10.1097/IAE.0000000000002713
9. Fung AE, Lalwani GA, Rosenfeld PJ, et al. An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol. 2007;143(4):566–583. doi:10.1016/j.ajo.2007.01.028
10. Berg K, Pedersen TR, Sandvik L, et al. Comparison of ranibizumab and bevacizumab for neovascular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology. 2015;122(1):146–152. doi:10.1016/j.ophtha.2014.07.041
11. Zur D, Guymer R, Korobelnik JF, et al. Impact of residual retinal fluid on treatment outcomes in neovascular age-related macular degeneration. Br J Ophthalmol. 2025;109:307–315. doi:10.1136/bjo-2024-325640
12. Aslanis S, Amrén U, Lindberg C, et al. Recurrent neovascular age-related macular degeneration after discontinuation of vascular endothelial growth factor inhibitors managed in a treat-and-extend regimen. Ophthalmol Retina. 2022;6(1):15–20. doi:10.1016/j.oret.2021.03.010
13. Hirata Y, Oishi A, Maekawa Y, et al. Recurrence of neovascular age-related macular degeneration after cessation of treat and extend regimen. Sci Rep. 2022;12:14768. doi:10.1038/s41598-022-19062-2
14. Hwang RY, Santos D, Oliver SCN. Rates of exudative recurrence for eyes with inactivated wet age-related macular degeneration on 12-week interval dosing with bevacizumab therapy. Retina. 2020;40(4):679–685. doi:10.1097/iae.0000000000002446
15. Adrean SD, Chaili S, Grant S, et al. Recurrence rate of choroidal neovascularization in neovascular age-related macular degeneration managed with a treat–extend–stop protocol. Ophthalmol Retina. 2018;2(3):225–230. doi:10.1016/j.oret.2017.07.009
16. Arendt P, Yu S, Munk MR, et al. Exit strategy in a treat-and-extend regimen for exudative age-related macular degeneration. Retina. 2019;39(1):27–33. doi:10.1097/iae.0000000000001923
17. Jaggi D, Nagamany T, Ebneter A, et al. Aflibercept for age-related macular degeneration: 4-year outcomes of a ‘treat-and-extend’ regimen with exit-strategy. Br J Ophthalmol. 2022;106(2):246–250. doi:10.1136/bjophthalmol-2020-316514
18. Menke MN, Zinkernagel MS, Ebneter A, et al. Functional and anatomical outcome of eyes with neovascular age-related macular degeneration treated with intravitreal ranibizumab following an exit strategy regimen. Br J Ophthalmol. 2014;98(9):1197–1200. doi:10.1136/bjophthalmol-2013-304775
19. Garay-Aramburu G, Rodriguez-Feijoo D, Aldazabal-Echeveste M, et al. Predictors of stoppage and recurrence of choroidal neovascularization with a treat-extend-stop protocol: 4-year follow-up. J Fr Ophtalmol. 2023;46(10):1204–1211. doi:10.1016/j.jfo.2023.02.021
20. Amarakoon S, Martinez-Ciriano JP, Baarsma S, et al. Reactivation of CNV after discontinuation of bevacizumab treatment of age-related macular degeneration. Ophthalmologica. 2021;244(3):200–207. doi:10.1159/000514539
21. Yoshida H, Inoda S, Takahashi H, et al. Two-year outcomes of intravitreal brolucizumab for neovascular age-related macular degeneration: treat, extend, and stop-protocol. Graefes Arch Clin Exp Ophthalmol. 2024;262(12):3815–3823. doi:10.1007/s00417-024-06577-9
22. Madhusudhana KC, Lee AY, Keane PA, et al. UK neovascular age-related macular degeneration database. Report 6: time to retreatment after a pause in therapy. Outcomes from 92 976 intravitreal ranibizumab injections. Br J Ophthalmol. 2016;100(12):1617–1622. doi:10.1136/bjophthalmol-2015-308077
23. Liu JY, Cheng CK, Bai CH, et al. Long-term remission and incidence of recurrence of neovascularization in intravitreal injection treated exudative age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2025;263(9):2541–2550. doi:10.1007/s00417-025-06885-8
24. Ashraf M, Souka A, Adelman RA. Age-related macular degeneration: using morphological predictors to modify current treatment protocols. Acta Ophthalmol. 2018;96(2):120–133. doi:10.1111/aos.13565
25. Cao X, Sanchez JC, Dinabandhu A, et al. Aqueous proteins help predict the response of patients with neovascular age-related macular degeneration to anti-VEGF therapy. J Clin Invest. 2022;132(2):e144469. doi:10.1172/JCI144469
26. Lee J, Choi J, Yu SY, et al. Recurrence of neovascular age-related macular degeneration after discontinuation of modified treat and extend treatment. Sci Rep. 2025;15:8952. doi:10.1038/s41598-025-92832-w
27. Munk MR, Arendt P, Yu S, et al. The impact of the vitreomacular interface in neovascular age-related macular degeneration in a treat-and-extend regimen with exit strategy. Ophthalmol Retina. 2018;2(4):288–294. doi:10.1016/j.oret.2017.07.010
28. Waldstein SM, Simader C, Staurenghi G, et al. Morphology and visual acuity in aflibercept and ranibizumab therapy for neovascular age-related macular degeneration in the VIEW trials. Ophthalmology. 2016;123(7):1521–1529. doi:10.1016/j.ophtha.2016.03.037
29. Schmidt-Erfurth U, Waldstein SM, Deak GG, et al. Pigment epithelial detachment followed by retinal cystoid degeneration leads to vision loss in treatment of neovascular age-related macular degeneration. Ophthalmology. 2015;122(4):822–832. doi:10.1016/j.ophtha.2014.11.017
30. Cho SC, Park KH, Park SJ, et al. Discontinuation of treatment and retreatment of neovascular age-related macular degeneration in the real-world: bundang AMD cohort study report 5. Front Med. 2023;10:1204026. doi:10.3389/fmed.2023.1204026
31. Garweg JG, Traine PG, Garweg RA, et al. Continued anti-VEGF treatment does not prevent recurrences in eyes with stable neovascular age-related macular degeneration using a treat-and-extend regimen: a retrospective case series. Eye. 2022;36(4):862–868. doi:10.1038/s41433-021-01562-6
32. Cho HJ, Jeon YJ, Yoon W, et al. Neovascular age-related macular degeneration without exudative recurrence over 24 months after initial remission. Sci Rep. 2022;12(1):15662.
33. Kiernan DF, Hariprasad SM, Rusu IM, et al. Epidemiology of the association between anticoagulants and intraocular hemorrhage in patients with neovascular age-related macular degeneration. Retina. 2010;30(10):1573–1578. doi:10.1097/IAE.0b013e3181e2266d
34. Kuhli-Hattenbach C, Fischer IB, Schalnus R, et al. Subretinal hemorrhages associated with age-related macular degeneration in patients receiving anticoagulation or antiplatelet therapy. Am J Ophthalmol. 2010;149(2):316–321. doi:10.1016/j.ajo.2009.08.033
35. Gillies MC, Hunyor AP, Arnold JJ, et al. Macular atrophy in neovascular age-related macular degeneration: a randomized clinical trial comparing ranibizumab and aflibercept (RIVAL study). Ophthalmology. 2020;127(2):198–210. doi:10.1016/j.ophtha.2019.08.023
36. Abdelfattah NS, Al-Sheikh M, Pitetta S, et al. Macular atrophy in neovascular age-related macular degeneration with monthly versus treat-and-extend ranibizumab: findings from the TREX-AMD trial. Ophthalmology. 2017;124(2):215–223. doi:10.1016/j.ophtha.2016.10.002
37. Korobelnik JF, Lanzetta P, Leal S, et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration: ninety-six-week results from the randomized Phase 3 PULSAR trial. Ophthalmology. 2026;133(1):39–50. doi:10.1016/j.ophtha.2025.08.022
38. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926. doi:10.1016/j.ophtha.2024.02.014
39. Ambresin A, Chaudhary V, Gale R, et al. Potential 20-week faricimab dosing in wet age-related macular degeneration. Ophthalmol Retina. 2026;10(5):573–575. doi:10.1016/j.oret.2026.02.001
40. Dhoot DS. Treatment of retinal/choroidal vascular diseases by sustained delivery of vascular endothelial growth factor receptor tyrosine kinase inhibitors. Am J Ophthalmol. 2025;277:570–579. doi:10.1016/j.ajo.2025.06.010
41. Khanani AM, Aziz AA, Khanani ZA, et al. Subretinal gene therapy for treatment of retinal and choroidal vascular diseases. Am J Ophthalmol. 2025;277:512–517. doi:10.1016/j.ajo.2024.12.002
42. Kikushima W, Sakurada Y, Fukuda Y, et al. Incidence and characteristics of neovascular age-related macular with over a 12-month remission after three monthly aflibercept administration: 60 months results of a pro re nata regimen. Retina. 2024;44(3):498–505. doi:10.1097/IAE.0000000000003994
43. Kikushima W, Sakurada Y, Fukuda Y, et al. Brolucizumab versus aflibercept in treating exudative age-related macular degeneration: a 12-month pro re nata regimen. Sci Rep. 2026;16:4739. doi:10.1038/s41598-026-34984-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.