Back to Journals » Clinical Ophthalmology » Volume 11
Discharge and infection in retinoblastoma post-enucleation sockets
Authors Mourits DL, Hartong DT, Budding AE, Bosscha MI, Tan HS, Moll AC
Received 25 August 2016
Accepted for publication 14 November 2016
Published 1 March 2017 Volume 2017:11 Pages 465—472
DOI https://doi.org/10.2147/OPTH.S120653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Daphne L Mourits,1 Dyonne T Hartong,1 Andries E Budding,2 Machteld I Bosscha,1 H Stevie Tan,1 Annette C Moll1
1Department of Ophthalmology, VU University Medical Center, 2Department of Microbiology, Academic Medical Center, Amsterdam, the Netherlands
Purpose: To investigate the causes and treatment options for socket discharge and infection in patients enucleated for retinoblastoma (Rb).
Methods: A questionnaire was filled out by (parents of) ocular prosthesis-wearing patients with a history of enucleation as treatment for Rb. We collected data on patients’ characteristics, cleaning habits of the prosthesis, frequency of socket irritation, discharge, and infection, and use of antibiotics. With ordinal logistic regression analysis, factors related to the outcome parameters (frequency of irritation, mucoid and purulent discharge) were identified. In a subset of young asymptomatic and symptomatic patients, a swab culture of the socket was performed to determine the presence of microorganisms.
Results: A total of 186 patients or their parents (mean age of the patients: 17.3 years, ranging from 0.8 to 88.3 years) filled out the questionnaire. Irritation, mucoid discharge, and purulent discharge were frequently (once a month or more often) experienced in 75 (39.5%), 127 (66.8%), and 15 (13.2%) sockets, respectively. Younger age was associated with a higher frequency of mucoid and purulent discharge. Radiation therapy, chemotherapy, gender, age at surgery, cleaning frequency, and nocturnal wear were not associated with the outcome parameters. In a subgroup of 26 patients, the sockets were swabbed and cultured. All symptomatic patients had a positive bacterial culture versus 15% (2/13) of the asymptomatic patients (P<0.001). Common cold was correlated with both symptoms and presence of bacteria. Haemophilus influenzae and Staphylococcus aureus were the species most frequently cultured.
Conclusion: Ocular prosthesis-wearing patients often experienced mucoid discharge, and less often irritation and socket infection. These complaints were found to decrease with increasing age, but did not seem to be influenced by cleaning or wearing habits. Symptomatic sockets, with and without discharge, were correlated with the presence of pathogenic bacteria for which local antibiotic treatment seemed effective in most cases.
Keywords: microorganisms, inflammation, prosthesis, cleaning habits
Introduction
Enucleation is performed for several indications: severe trauma, intraocular tumor, and phthisis bulbi. Substitution of the eyeball with a prosthesis resembling the fellow eye may offer psychological acceptation for the patient.
In children, retinoblastoma (Rb) is the main reason for enucleation. Rb has an estimated incidence of one in 15,000 and 20,000 live births, affecting 10–15 children in the Netherlands per year.1 In the past, about 70%–95%2–4 of patients with Rb were treated by enucleation. The mean age at surgery is 1.9 years.5 In recent years, however, more and more globe-sparing methods are employed.6
Toddlers, especially day care attendees, frequently encounter infections and viruses.7–9 In addition to runny noses, parents are often confronted with runny sockets.
Accumulation of discharge from the socket on the prosthesis and eyelids is a common complaint of prosthetic eye wearers. It negatively affects the appearance and is experienced as “dirty” and “annoying”. Discharge from the socket is the second highest concern of enucleated patients after the health of the remaining eye.10 The discharge can be watery, mucoid, or purulent. When the discharge is purulent, the socket often appears red and irritated, and sometimes pain is experienced.
Runny sockets and runny noses are both a result of irritated (or even inflamed) mucosa overproducing mucus. Patients often report an association between common upper respiratory tract viral infections and increased socket discharge. Common colds are not typically treated with (systemic) antibiotics, but we sometimes do administer topical antibiotics for symptomatic sockets. The current study was designed to describe potential causes and characteristics of socket problems, and to address the question whether the use of antimicrobial agents is justified in the treatment of inflamed sockets.
Methods
This study was approved by the local ethics committee of the VU University Medical Center (VUmc) and performed in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from the participants and from the parents of younger participants.
The study population consisted of patients wearing an ocular prosthesis and with a history of enucleation as treatment for Rb, who were seen during regular Rb follow-up consultations between April 2013 and May 2015. A questionnaire was filled out by (the parents of) the patients to investigate their characteristics, cleaning habits of the prosthesis, frequency of socket irritation, discharge, and infection, and use of topical antibiotics.
The results of the questionnaire were compiled. Outcomes of irritation and mucoid and purulent discharge in relation to age at surgery and age at time of examination, gender, material of prosthesis, cleaning frequency, nocturnal wear, and history of radiation therapy and/or systemic chemotherapy were analyzed using ordinal logistic regression.
In a subset of the study population, a comparative swab study was performed. Consecutive young patients (0–4 years) visiting the hospital for routine exam and/or treatment for Rb under general anesthesia and patients (5–10 years) with complaints of excessive discharge at routine exam (without general anesthesia) were included. During physical examination, the sockets were judged on discharge and color of conjunctiva, and a swab (eSwab™; Copan Italia, Brescia, Italy) was taken on which bacterial culture of the conjunctival socket was performed.
Patients were classified as “symptomatic” when parents mentioned an irritated socket and/or complaints of increased discharge in the questionnaire and when the socket appeared diffusely hyperemic with or without mucoid or purulent discharge at physical examination. Patients without complaints and a pale-to-mild hyperemic socket with or without discharge at examination were categorized as “asymptomatic”.
Inclusion was complete when both groups, symptomatic and asymptomatic, were represented by a similar number of patients (both groups should contain minimal ten patients). Patients were excluded when local or systemic antibiotics were used at the time of examination and up to 2 weeks before. All symptomatic patients were treated with topical Ofloxacin (Trafloxal®) ointment or eyedrops three times a day for 2 weeks.
Two weeks after examination, a follow-up consultation was conducted by telephone. If symptoms persisted at follow-up, antibiotic treatment was prolonged (with instructions: washing hands and removing the prosthesis when applying the antibiotics) for 2 weeks. If symptoms persisted after these 2 weeks, an additional physical examination was conducted.
Main outcome of the swab study was the presence of bacteria in the socket. Characteristic differences between the groups were compared with Mann–Whitney U test. The Mantel–Haenszel method was used for the common odds ratio. A chi square test was performed to compare main outcome in both groups.
Results
A total of 186 patients or their parents filled out the questionnaire for patients treated for Rb by unilateral enucleation (N=182) or bilateral enucleation (N=4). Thirty-six patients (and 38 sockets) had a history of treatment with external-beam radiation therapy (EBRT). Mean age at the time of enucleation was 22.1 months, and at the time of examination was 17.3 years.
The outcome of the questionnaire is summarized in Table 1.
 | Table 1 Overview of questionnaire |
Key findings of the questionnaire were the following: frequent (once a month or more often) experience of irritation was reported in 75 (39.5%) sockets; mucoid discharge was reported in 127 (66.8%) sockets and purulent discharge in 15 (13.2%); the majority (137, 72%) slept with the prosthesis in situ, and most patients cleaned the prosthesis daily with tap water.
An ordinal logistic regression model was used to identify factors related to the outcome parameters: frequency of irritation, and mucoid and purulent discharge. Factors included in the model were radiation therapy, chemotherapy, gender, age at examination, age at surgery, material of prosthesis, cleaning frequency, and nocturnal wear. With forward stepwise regression, nonsignificant factors were excluded from the model. The age at the time of examination demonstrated a significant relation to the outcomes of irritation and mucoid and purulent discharge. In the model for irritation also, the variable prosthesis material demonstrated significant influence. The frequency of irritation, and mucoid and purulent discharge decreased with increasing age (Table 2).
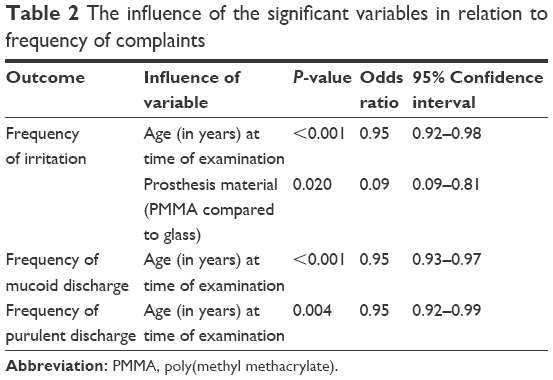 | Table 2 The influence of the significant variables in relation to frequency of complaints |
Comparative swab study
A total of 26 Rb patients with unilateral post-enucleation sockets were included in the comparative swab study. This comprised 24 patients examined under general anesthesia and two slightly older patients (age 5 and 7) examined without general anesthesia. The latter were included because of complaints of excessive discharge.
Thirteen patients were classified as symptomatic, and 13 as asymptomatic. Mean age at examination was 39.4 months (median 38.2, range 9–90 months), and mean age at enucleation was 16.1 months (median 10.2, range 1.9–40 months). These characteristics did not significantly differ between the two groups.
In the symptomatic group, 12 sockets were diffuse hyperemic with purulent discharge. One patient was classified symptomatic because of increased complaints; however, at examination, only minor features of inflammation were present (mild hyperemia and mucoid discharge). In this particular case, the treating physician opted for a watchful waiting policy and did not prescribe antibiotics. Within 2 weeks, symptoms did increase, and on request of the parents, this patient also received topical antibiotic treatment.
In the asymptomatic group, 11 sockets were pale without evident discharge. Two sockets showed mild hyperemia without discharge. No parents reported increased discharge or an irritated socket. In this group, no antibiotics were prescribed.
Fifteen patients had a positive socket culture. Most of the sockets harbored a single bacterial species, and some contained two species (Table 3). In Table 4, the antibiotic sensitivity is demonstrated. The positive cultures corresponded with 13 (100%) of the symptomatic patients and two (15%) of the asymptomatic patients. Nine patients had common cold (with runny noses): seven of the symptomatic and two of the asymptomatic group (these latter two did not harbor bacteria).
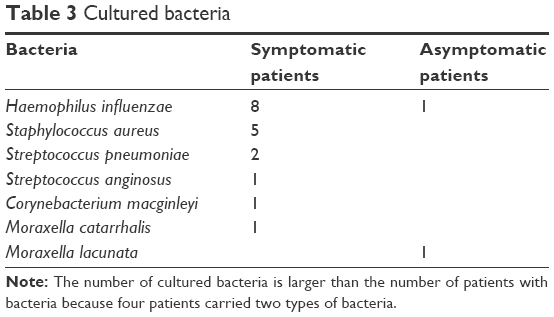 | Table 3 Cultured bacteria |
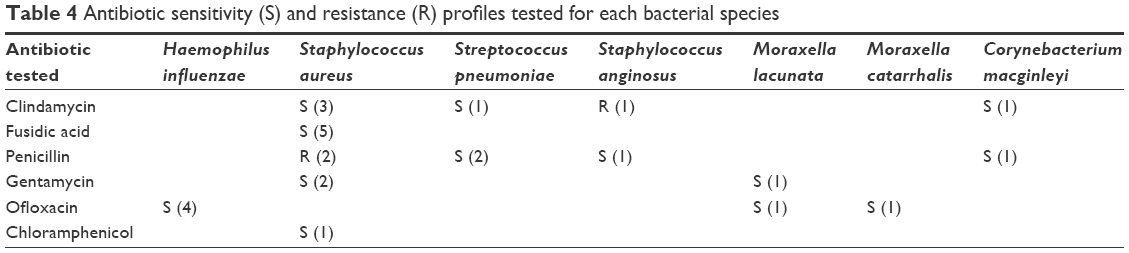 | Table 4 Antibiotic sensitivity (S) and resistance (R) profiles tested for each bacterial species |
Culture results proved a strong association between the presence of symptoms and a positive socket culture: χ2(1) =19.067, P<0.001; with the presence of common cold: P=0.018; without the presence of common cold: P=0.011 (Fisher exact).
All but three patients responded within 2 weeks to the antibiotics. In one, the mother administered the antibiotics at the front surface of the prosthesis. After prolonged treatment and instructions to remove the prosthesis at time of application of the ointment, the symptoms disappeared.
The two other patients did not show any response to (prolonged) antibiotic treatment. Repeated cultures from their sockets showed different bacteria. Systemic antibiotics (sulfamethoxazol and trimethoprim) were administered in one of these patients (age 2) because of a respiratory infection combined with neutropenia. During this treatment, the patient was free of socket symptoms. At that time, a socket culture proved negative. After termination of this treatment, symptoms returned. In the second case (age 7), the same systemic treatment was given, but this had only a minor effect. As the persistent infection was caused by Staphylococcus aureus, and the patient was a nasal S. aureus carrier, eradication therapy was initiated (Table S1). Indeed, this initially eradicated carriage and infection, but it returned after 3 months.
In these two patients, the bad response to the antibiotics was not a result of insensitivity to the administered agent nor resistance (both tested). Repeated cultures demonstrated different bacteria. Possibly, the chronic superficial socket infection in both patients could have been due to anatomic deviations of the socket: a complete ptosis in one and contraction and entropion (with the lashes stuck to the prosthesis) in the other patient. Both were recommended surgery.
Discussion
Excessive discharge in anophthalmic sockets of prosthetic-eye-wearing patients occurs commonly and is a burden for patients who suffer from this.10 In our current study, regular complaints of socket discharge were reported by 66.8% of patients. Dirty sockets are disfiguring and can negatively influence psychosocial well-being and social interaction. The discharge may cause physical discomfort, makes the prosthesis opaque, and may interfere with the motility of the prosthesis.11
Pine et al12 surveyed 429 prosthetic eye wearers and found an association between cleaning regime and frequency, volume, and viscosity of discharge: more severe discharge was reported with a more frequent cleaning regimen. According to a three-phase homeostasis model and staining tests with different prosthesis-cleaning frequencies,13 they advised that the best cleaning frequency lies within maximally once a month and minimally once every 6 months. We did not find a relation between cleaning habits of the patients and symptoms of socket discharge or irritation. In addition, subjective experience with different cleaning regimens within one individual did not alter discharge.
We did find a significant relation between younger age and increased frequency of discharge and irritation of the socket. In their study, Pine et al12 did not find an association between age and discharge severity. In that study, however, the ages of the survey responders were not reported. It is possible that we have been studying different age groups.
In our clinic, patients report complaints of increased discharge to be associated with common colds. This was also demonstrated in our study results. Common colds increase the amount of discharge, which in turn may cause bacterial overgrowth. The current study demonstrates a strong correlation between symptomatic sockets and the presence of bacteria in these sockets. Haemophilus influenzae was most prevalent, followed by S. aureus. In the study of Vasquez and Linberg,14 Staphylococcus epidermidis and Corynebacterium xerosis were most prevalent; in the study of Krishna,15 Streptococcus pyogenes, Aspergillus spp., and Penicillium spp. were common. The ages of their study populations are not mentioned. Age may be related to prevalence of specific bacteria which could explain the different findings in these studies. For patients suffering from a red irritated socket with increased discharge, we recommend prescription of topical broad-spectrum antibiotics such as Ofloxacin. In this study, 11 of 13 patients were symptom-free after this antibiotic treatment. The two cases that were not cured with antibiotic treatment suffered from chronic complaints. In chronic cases, underlying causes need to be addressed.
In Figure S1, we present an overview of potential underlying causes of chronic discharge with resulting problems and their specific reason coupled to an adequate advice for treatment. This diagram can be used as a protocol for patients with chronic discharge.
A bad prosthesis fit due to anatomical distortion or simply due to a bad custom fit may result in dead space. In this dead space, a coagulum of proteinaceous debris can form a sequester in which bacterial colonization easily takes place.16 This in turn causes inflammation, resulting in further increase of discharge leading to a vicious circle. In case of a bad custom fit combined with normal anatomy of the socket, a new prosthesis can be fitted. However, if an anatomical distortion causes the bad fit, rehabilitation of the socket can be attempted.
Lack of an adequate tearfilm increases the foreign body sensation and induces crusting of the mucus at the prosthesis, which in turn leads to additional irritation and increase of mucus production. Allen et al17 demonstrated that tear production in anophthalmic sockets was reduced as compared to normal eyes and that people with complaints had only half the tear secretion quantity compared to patients without complaints. They postulated that the absence of a cornea eliminates the stimulus for tear production. We noticed that patients with lagophthalmos did not differ in frequency of irritation and discharge complaints compared to those with adequate eyelid closure.
In addition to decreased lacrimal gland stimulation, three other factors may play a role: a damaged lacrimal gland system, bad quality of the tearfilm (unbalanced aqueous, mucous, and oily components), and the hydrophobic property of the acrylic prosthesis resulting in dispersion of the tearfilm. Glass prostheses have hydrophilic properties; in the ordinal regression model, the material of the prosthesis did only reach statistical significance for the outcome “frequency of irritation”. Glass prostheses were however worn by a small number of patients, mostly elderly patients. Potential benefits of the hydrophilic properties should be prospectively tested in a matched population or within one patient.
Among patients enucleated for the treatment of Rb, damage to the excretory lacrimal system is potentially a contributing factor to discharge problems in those who were additionally treated with EBRT.18–20 In our current study, we found no relation between radiation therapy and complaints of discharge. Also, chemotherapy did not significantly contribute to experienced problems.
In conclusion, many Rb patients wearing ocular prostheses experience discharge, irritation, and infection of their socket. The cleaning regime has no influence on these complaints. Symptomatic hyperemic sockets are often caused by pathogenic bacteria for which topical antibiotics are effective. Patients with infection who do not respond to antibiotic therapy should be examined for underlying causes such as lacrimal problems, bad prosthetic fit, allergy to material, or anatomical distortion of the socket and/or eyelids.
Acknowledgments
The authors thank Birgit Witte (VUmc) for her statistical advice. This study was funded by ODAS Foundation, Delft, the Netherlands. The sponsor or funding organization had no role in the design or conduct of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
Moll AC, Kuik DJ, Bouter LM, et al. Incidence and survival of retinoblastoma in the Netherlands: a register based study 1862–1995. Br J Ophthalmol. 1997;81(7):559–562. | ||
Berman EL, Donaldson CE, Giblin M, Martin FJ. Outcomes in retinoblastoma, 1974–2005: the Children’s Hospital, Westmead. Clin Exp Ophthalmol. 2007;35(1):5–12. | ||
Lumbroso-Le Rouic L, Savignoni A, Levy-Gabriel C, et al. Treatment of retinoblastoma: the Institut Curie experience on a series of 730 patients (1995 to 2009). J Fr Ophtalmol. 2015;38(6):535–541. | ||
Othman IS. Retinoblastoma major review with updates on Middle East management protocols. Saudi J Ophthalmol. 2012;26(2):163–175. | ||
Mourits DL, Moll AC, Bosscha MI, Tan HS, Hartong DT. Orbital implants in retinoblastoma patients: 23 years of experience and a review of the literature. Acta Ophthalmol. 2016;94(2):165–174. | ||
Grossniklaus HE. Retinoblastoma. Fifty years of progress. The LXXI Edward Jackson Memorial Lecture. Am J Ophthalmol. 2014;158(5):875–891. | ||
Enserink R, Ypma R, Donker GA, Smit HA, van Pelt W. Infectious disease burden related to child day care in the Netherlands. Pediatr Infect Dis J. 2013;32(8):e334–e340. | ||
Fleming DW, Cochi SL, Hightower AW, Broome CV. Childhood upper respiratory tract infections: to what degree is incidence affected by day-care attendance? Pediatrics. 1987;79(1):55–60. | ||
Louhiala PJ, Jaakkola N, Ruotsalainen R, Jaakkola JJ. Form of day care and respiratory infections among Finnish children. Am J Public Health. 1995;85(8 Pt 1):1109–1112. | ||
Pine K, Sloan B, Stewart J, Jacobs RJ. Concerns of anophthalmic patients wearing artificial eyes. Clin Exp Ophthalmol. 2011;39(1):47–52. | ||
Goldfarb HJ, Turtz AI. A detergent-lubricant solution for artificial eyes. Am J Ophthalmol. 1966;61(6):1502–1505. | ||
Pine K, Sloan B, Stewart J, Jacobs RJ. A survey of prosthetic eye wearers to investigate mucoid discharge. Clin Ophthalmol. 2012;6:707–713. | ||
Pine KR, Sloan B, Jacobs RJ. Deposit buildup on prosthetic eyes and implications for conjunctival inflammation and mucoid discharge. Clin Ophthalmol. 2012;6:1755–1762. | ||
Vasquez RJ, Linberg JV. The anophthalmic socket and the prosthetic eye – a clinical and bacteriologic study. Ophthal Plast Reconstr Surg. 1989;5(4):277–280. | ||
Krishna G. Contracted sockets – I (aetiology and types). Indian J Ophthalmol. 1980;28(3):117–120. | ||
Rose GE. The giant fornix syndrome: an unrecognized cause of chronic, relapsing, grossly purulent conjunctivitis. Ophthalmology. 2004;111(8):1539–1545. | ||
Allen L, Kolder HE, Bulgarelli EM, Bulgarelli DM. Artificial eyes and tear measurements. Ophthalmology. 1980;87(2):155–157. | ||
Imhof SM, Hofman P, Tan KE. Quantification of lacrimal function after D-shaped field irradiation for retinoblastoma. Br J Ophthalmol. 1993;77(8):482–484. | ||
Karp LA, Streeten BW, Cogan DG. Radiation-induced atrophy of the Meibomian gland. Arch Ophthalmol. 1979;97(2):303–305. | ||
Macfaul PA, Bedford MA. Ocular complications after therapeutic irradiation. Br J Ophthalmol. 1970;54(4):237–247. |
Supplementary materials
 | Table S1 Staphylococcus aureus eradication protocol |
 | Figure S1 Overview of potential underlying causes of chronic discharge. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.