Back to Journals » Risk Management and Healthcare Policy » Volume 16
Disaster Preparedness Amongst Emergency Pharmacists for the FIFA World Cup Qatar 2022™: A Cross-Sectional Survey
Authors Isleem N ![]() , Naseralallah L
, Naseralallah L ![]() , Koraysh S
, Koraysh S ![]() , Abu Ghalyoun A
, Abu Ghalyoun A ![]() , Alnaimi S, Pallivalapila A, Al Hail M
, Alnaimi S, Pallivalapila A, Al Hail M
Received 4 February 2023
Accepted for publication 28 March 2023
Published 4 April 2023 Volume 2023:16 Pages 573—583
DOI https://doi.org/10.2147/RMHP.S404367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Nour Isleem,1,* Lina Naseralallah,1,2,* Somaya Koraysh,1 Ahmad Abu Ghalyoun,1 Shaikha Alnaimi,1 Abdulrouf Pallivalapila,1 Moza Al Hail1
1Pharmacy Department, Hamad Medical Corporation, Doha, Qatar; 2School of Pharmacy, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK
*These authors contributed equally to this work
Correspondence: Nour Isleem, Pharmacy Department, Hamad Medical Corporation, P.O.Box 42, Doha, Qatar, Tel +974 3100 3071, Email [email protected]
Purpose: The aim of this study is to assess the level of preparedness of pharmacists working in the emergency department at Hamad Medical Corporation (HMC) for any emergency disasters that may take place during the FIFA World Cup Qatar 2022™ by evaluating their awareness (A), attitude (A), and readiness (R).
Methods: A cross-sectional quantitative observational study was conducted through a web-based survey. The survey was distributed among emergency pharmacists working in general hospitals under HMC. The questionnaire was composed of three major domains assessing awareness, attitude, readiness, as well as an additional domain to collect the participants’ demographics. Student’s t-test, analysis of variance, Pearson’s correlation, and linear regression were used with an alpha level of 0.05.
Results: Most pharmacists working in the emergency departments at HMC had high levels of awareness (76.9%), attitude (92%), and readiness (53.8%) for any emergency disasters that may occur during the FIFA World Cup 2022. Nonetheless, almost half of the respondents reported moderate level of readiness for emergency events. Pharmacists with > 10 years’ practice experience had significantly higher AAR score compared to those with < 5 years’ experience (P = 0.002). Significant direct positive correlations were found among the 3 AAR parameters (P < 0.05). Attitude was found to be a significant predictor of readiness (P < 0.05). A model composed of attitude and awareness could predict 12% of readiness score.
Conclusion: Emergency pharmacists at HMC have high level of preparedness for any emergency disaster event during the World Cup. Future research should focus on the development of theory-based action framework for pharmacy departments during mass gathering events.
Keywords: disaster preparedness, disaster management, emergency medicine, pharmacist, mass gathering, FIFA World Cup
Introduction
Emergency situation has been defined by the Federal Emergency Management Agency (FEMA) as “any situation, whether caused by nature, technology, or people that calls for responsive action to save lives or protect property”.1 Emergency disasters are more likely to happen when small countries host huge populations. Events involving mass gathering could often increase the workload on local hospitals and emergency services.2–5 According to the World Health Organization (WHO), mass gathering is an event with more than 1000 person in a specific location for a specific purpose for a defined period of time.6
In the past few years, Qatar held a variety of mass gathering events such as the 2006 Asian Games, the 2019 World Athletics Championships and the 2021 Arab Cup. Fortunately, no disasters have happened during these events; according to the INFORM 2023 Risk Index,7 which assess the risk of humanitarian crises and disasters of a country, Qatar has an index of 1.4 indicating that Qatar is at a very low risk for disasters. However, the World Cup is one of the biggest sports events in the world. Over 1.4 million tourists from all over the globe visited Qatar between 20 November and 18 December.8 This large number of attendees had the potential to impose a hefty burden on public health and response capabilities. The preparedness of the healthcare system was key to guarantee the timely and effective provision of healthcare. Additionally, the Qatar Olympic Committee (QOC) announced that Qatar will host 81 sport mass gathering events in 2023 including 14 international events.9
During mass gathering events, healthcare systems are expected to provide support and guidance. Therefore, in preparation for the 2022 FIFA World Cup Qatar™, Hamad Medical Corporation (HMC) had implemented multiple initiatives to ensure the provision of optimal healthcare to visitors while assuring the sustainability of care delivered to citizens and residents. HMC is the primary public healthcare provider in the State of Qatar. It oversees 12 hospitals (nine specialized and three general community hospitals).10 As part of HMC preparedness efforts, the pharmacy department has launched many strategies to prepare emergency pharmacists. This includes well-organized high-tech pharmaceutical services. Other medication-related issues have also been addressed including chain supply management and adding new drugs to the formulary to handle issues related to doping.11
Pharmacy workforce is a crucial part of the healthcare system. In recent years, the scope of pharmacist’s job has been expanding to adapt new practice roles such as providing direct patient care, integrating into public health, and performing frontline duties. The latter was particularly evident during the coronavirus disease (COVID-19) pandemic when pharmacists promptly adapted new roles and effectively contributed to the health sector response.12 The American Society of Health-System Pharmacists (ASHP) strongly advised that members of the pharmacy workforce exercise their responsibilities in anticipating and responding to emergencies.13 Regardless, finding from previous research showed that pharmacists have an unsatisfactory level of preparedness.14,15 Although previous research has looked into the preparedness of the pharmacy workforce for emergency disasters,16–19 there is paucity of research on the preparedness of pharmacists for mass gathering events.
Therefore, the aim of this cross-sectional quantitative study is to assess the level of preparedness of pharmacists working in the emergency department at HMC for any emergency disasters that may take place during the FIFA World Cup Qatar 2022™ by evaluating their awareness (A), attitude (A), and readiness (R). Measuring the preparedness of emergency pharmacists is imperative to ensure the visitors safety and to reduce the long-term effects of emergencies. It also will enable policy makers to determine the need for further instructional support and emergency management plan implementation for any future mass gathering events.
Methods
Study Design
A cross-sectional, quantitative, observational study was conducted using web-based piloted survey.
Ethical Considerations
This study was approved by the Medical Research Center (MRC), Hamad Medical Corporation in 2022 (MRC-0122-680). The consent form was attached to the distributed surveys, and a respondent returning the survey indicated his or her agreement to participate in the study.
Study Population and Setting
The targeted population was pharmacists working in the emergency departments in the three general hospitals under HMC, which are Hamad General Hospital, Al-Khor Hospital and Al-Wakra Hospital. Of a total population of 80 emergency pharmacists, a sample size of 61 pharmacists was needed. The required sample size was calculated based on a margin of error of 5%, a 95% confidence level, and an 80% response distribution. Raosoft® was used to perform this calculation.20 Pharmacists were recruited based on random sampling through sending an e-mail to the pharmacists who met the inclusion criteria. All pharmacists and clinical pharmacists working in the emergency department in HMC were included in the study with no restrictions on age, gender, time of work, and training history. Pharmacy students and residents were excluded, as were pharmacists who participated in the pilot phase.
Outcome Measures
The primary outcome of the study was the assessment of AAR levels amongst emergency pharmacists in HMC. For the purpose of this study, awareness was defined as the knowledge and understanding that something is happening or exists;21 attitude was defined as a way of behaving that is caused by experiences of our opinions about disaster;22 and readiness was defined as a state of preparation and willingness to practice if a disaster were to occur.23
Questionnaire Development and Validation
A self-administered questionnaire was developed based on an extensive review of the literature and was adopted with few modifications to fit the context of this study.17,24–26 The questionnaire was comprised of three major sections assessing awareness (A), attitude (A), and readiness (R), as well as an additional section related to the demographic profile of the respondents. Awareness section has a total of 11 yes/no questions and had a maximum score of 11 points. To categorize the scores, cut-off points were set as follows: below 4 points was considered low (25th quartile), 4–8 points was moderate (more than the 25th quartile and less than the 75th quartile), and above 8 points was high (75th quartile). A 5-point Likert scale (from strongly agree to strongly disagree) was utilized to elicit the attitude which contains 15 items with a maximum of 75 possible points. A score between 25 points and 50 points is considered moderate, below this is low and above it is high. Readiness-related options (9 items) were given a score from 1 to 5 whereby the “strongly agree” option was assigned a score of 5 and “strongly disagree” was assigned a score of 1 with a maximum score of 45 points. A score below 15 points is considered low, between 15 and 30 points is moderate, while above 30 points is high.
The questionnaire was evaluated for face and content validity by three purposively selected experts (one associate director of the research center of the pharmacy department and two faculty members from the College of Pharmacy at Qatar University, all of which are doctorate holders) with extensive experience in disaster medicine and survey instrument development. Appropriate minor modifications of the survey instrument were undertaken based on the experts’ opinions to fit the scope of the study and to remove confusing and leading questions. The readability, clarity and completion time of the questionnaire was determined by piloting among five emergency pharmacists.
Data Collection Procedure
The data were collected through an anonymous, self-administered questionnaire through a web-link at SurveyMonkey® (Survey Monkey Inc., SanMateo, California, USA). The link was distributed through the hospital official e-mail system to the emergency pharmacists from the three general hospitals. A detailed description of the study (eg, objectives, data collection procedure, confidentiality and anonymity measures, and voluntary nature of participation) was provided. The completion of the questionnaire implied an informed consent to participate.
Data Analysis
The collected data were analyzed using IBM Statistical Package for Social Sciences (IBM SPSS Statistics, Version 22.0; IBM Corp, Armonk, NY). Descriptive analyses were reported as frequency (%) for categorical data or mean (±SD) for numerical data. Shapiro–Wilk test was used to test the normality of collected data. For difference between gender and AAR scores, independent T-test or Mann–Whitney were used for parametric and non-parametric data, respectively. One-way ANOVA or Kruskal–Wallis analysis were used to study the effect of location and experience years on AAR scores, followed by post-hoc analysis using Bonferroni test. Pearson’s correlation was utilized to establish the strength of relation amongst the 3 AAR parameters. Finally, linear regression was performed to predict the readiness (R) from Awareness (A) and Attitude (A2).
Results
Pharmacists working in the emergency department of three general hospitals participated in this survey with a response rate of 81.25% (65/80). Participant demographics are summarized in Table 1. Around 54% of respondents were male. The majority of pharmacists practiced in Hamad General Hospital (49.2%), followed by Al-Khor Hospital (30.8%) and Al-Wakra Hospital (20%). Most participants had less than 5 years of experience (41.5%), while 33.8% had more than 10 years of experience.
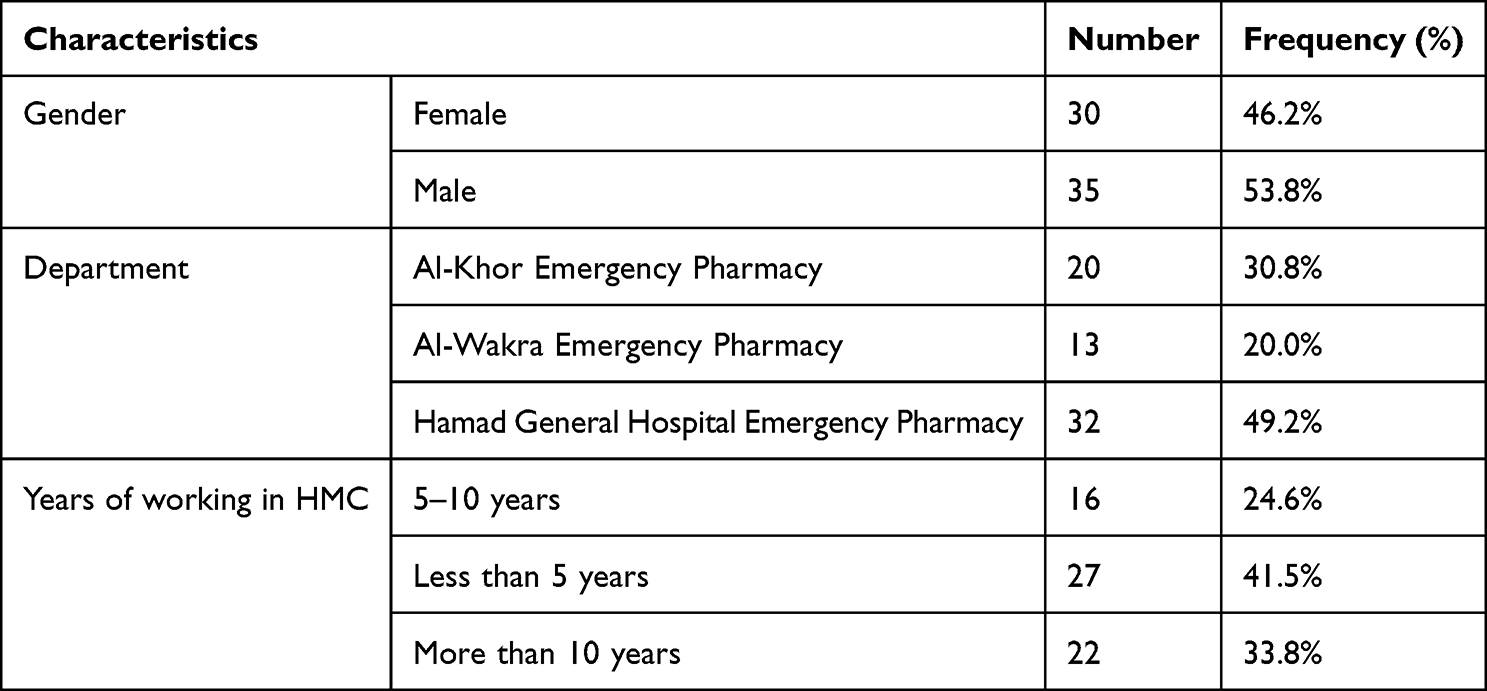 |
Table 1 Respondents’ Demographics |
Figure 1 illustrates the preparedness level of pharmacists in terms of awareness, attitude, and readiness. The survey results showed that majority of respondents have high levels of awareness (76.9%), attitude (92%), and readiness (53.8%) for emergency disasters during the FIFA World Cup. The findings also illustrated that 20% and 7.7% of participants had a moderate level of awareness and attitude respectively, while almost half of the respondents (46.2%) indicated moderate level of readiness for emergency disaster events. Only 3.1% of respondents’ responses demonstrated a low level of awareness.
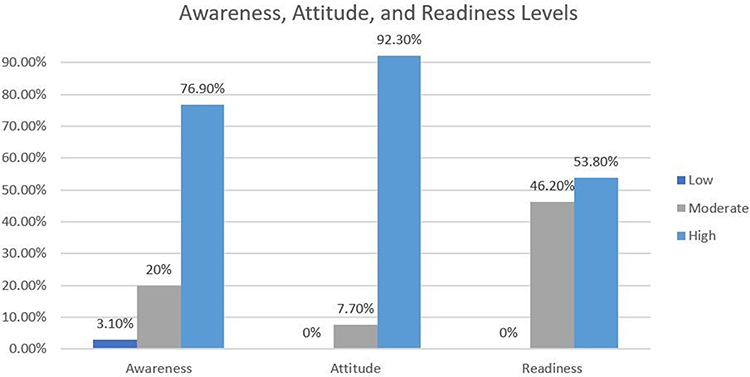 |
Figure 1 Respondents’ level of awareness, attitude, and readiness. |
Normality testing illustrated normally distributed data (P > 0.05) for all outcome measures except for awareness (P < 0.0001) (Supplementary Table 1). Table 2 represents the results obtained from analyzing the association between the respondents’ characteristics and their AAR parameters. The results indicated no significant difference between pharmacists from different locations on AAR parameters or total scores. Additionally, results showed no significant differences in attitude, readiness, and total scores based on gender; however, male participants showed a significantly higher awareness level on disaster medicine for FIFA World Cup as compared to female pharmacists (MD 1.79, 95% CI 0.63–2.95; P = 0.006).
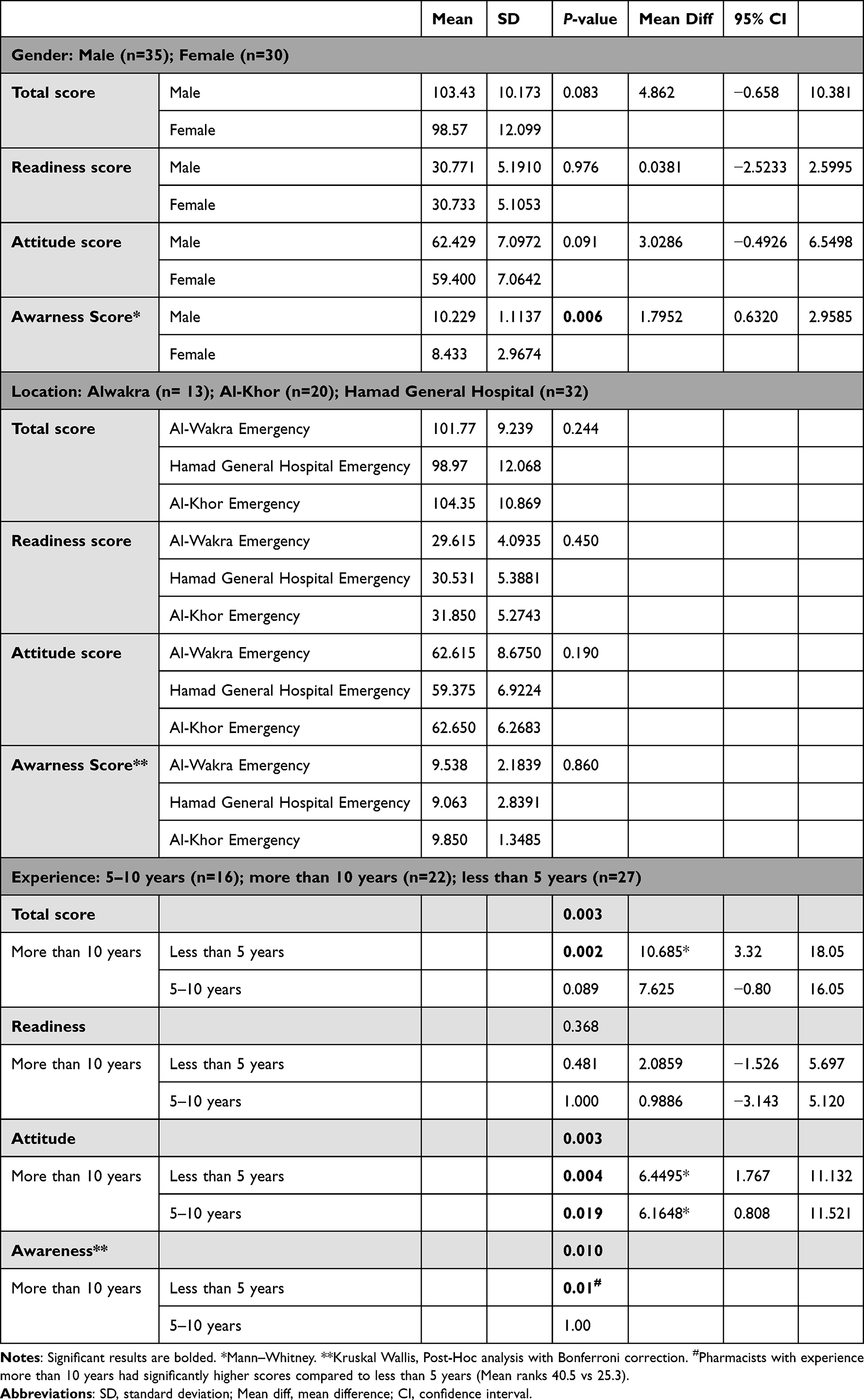 |
Table 2 Awareness, Attitude, Readiness, and Total Scores Based on Respondents’ Demographics |
Moreover, results indicated that pharmacists with more than 10 years of experience have significantly higher AAR total scores compared to pharmacists with less than 5 years of experience (MD 10.86, 95% CI 3.32–18.05, P = 0.003). Specifically, post-hoc analysis showed a significant difference among the said groups in awareness (P = 0.01) and attitude (P = 0.004), but not readiness (P = 0.481).
A significant positive correlation (P < 0.05) was noted between total AAR scores and each individual parameters (A; moderate, A2; strong, R; strong). Moreover, the pharmacist’s awareness scores were moderately correlated with their attitude scores (P = 0.004). Pharmacist’s readiness was moderately correlated with their attitude (P = 0.05), but weakly-to-moderately correlated with their awareness (P = 0.023) (Table 3). A regression analysis produced a model that predicts 12% of the respondents’ readiness scores based on awareness and attitude (P = 0.007).

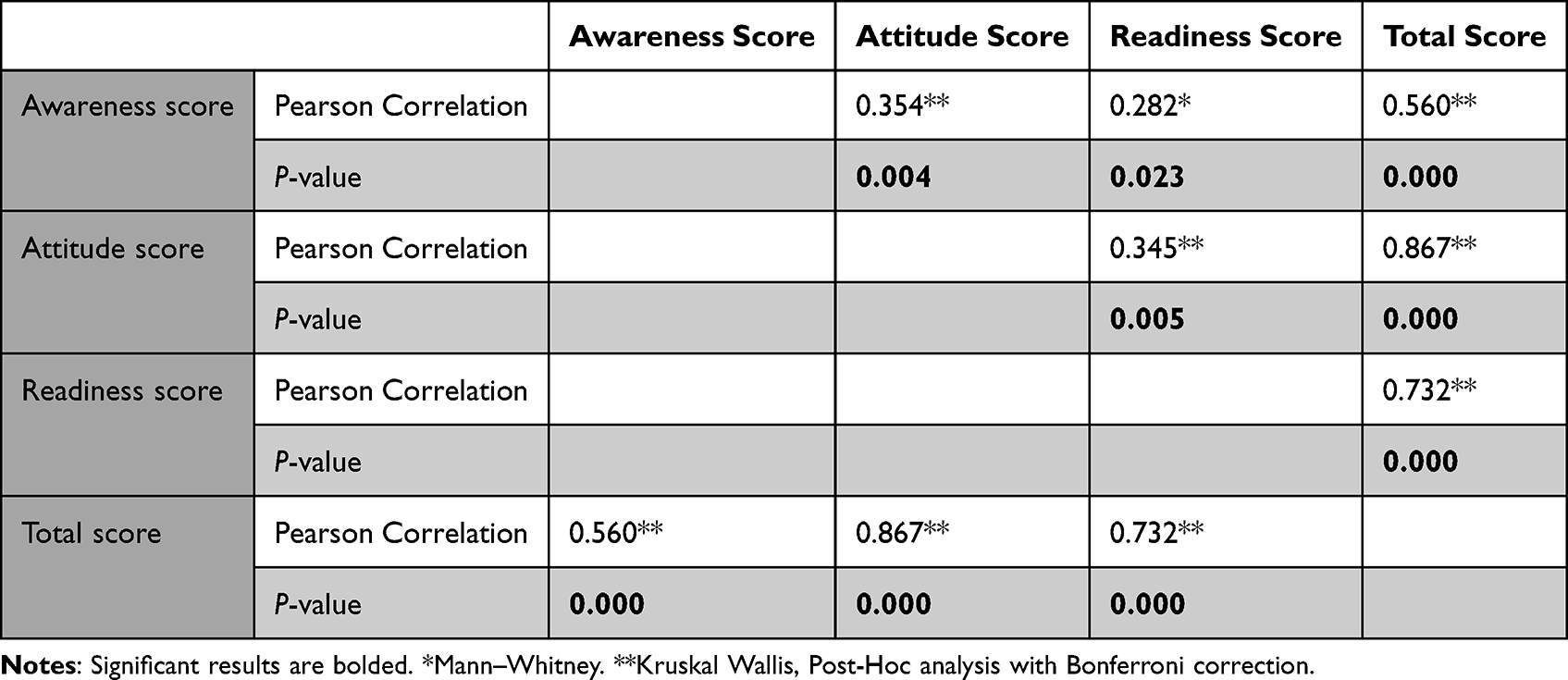 |
Table 3 Correlation Between Awareness, Attitude, and Readiness Among Respondents |
Discussion
Statement of Key Findings
The findings from this questionnaire-based study highlighted that most pharmacists working in the emergency departments at HMC had high levels of awareness (76.9%), attitude (92%), and readiness (53.8%) for any emergency disasters during the FIFA World Cup 2022. Nevertheless, almost half of the respondents reported moderate level of readiness for emergency disaster events. Low scores were only noted for awareness in 3.1% of respondents. Pharmacists with more than ten years of experience had significantly higher AAR scores compared to those with less than five years (P = 0.002). A significant direct positive correlation was seen amongst all AAR parameters (P < 0.05). Attitude was found to be moderately correlated to readiness, while awareness and readiness were weakly correlated.
Interpretation of Findings
According to the INFORM 2023 Risk Index,7 which assesses the risk of humanitarian crises and disasters of a country, Qatar has an index of 1.4 (vs Saudi Arabia: 3.5, Oman: 2.6, Kuwait: 1.8, United Arab Emirates: 1.7, and Bahrain: 1.2). This indicates that Qatar is at a very low risk for disasters. However, Qatar is hosting the FIFA World Cup 2022 which exposes the country to an array of risks that are associated with mass gathering events. Mass gathering events are known to pose a substantial burden and serious challenges on healthcare systems. Previous research showed that such events increase the workload especially for emergency medical services.2,27–29 They also could lead to delayed emergency responses and strain the resources of local emergency services.30 Hence, implementing preparedness measures and action plans as well as ensuring resource planning and staff preparedness for any unexpected events is imperative.
Disaster medicine is a discipline that incorporates emergency medicine and disaster management. It provides healthcare to the most victims possible of both natural and human-made disasters.31 Healthcare workers should have the willingness and the competency to respond to disasters and need to be engaged in the different phases of the disaster cycle.31,32 Preparedness is one of the four phases of the disaster cycle alongside mitigation, response, and recovery.31 For healthcare providers to be competent and willing to respond to disasters, disaster medicine preparedness should be an integral component of the undergraduate curriculum, continuous professional development activities, as well as the pre-planning efforts for mass gathering events.17,28
A plethora of studies from different countries across the globe, including one paper from Qatar, have looked into the emergency preparedness and the disaster management of the pharmacy workforce and pharmacy students. Findings showed that pharmacists and pharmacy students had significant areas of deficiencies such as the lack of well-identified role and the limited training related to disaster situations.16–19 Additionally, a recent systematic review of six studies demonstrated that pharmacists and pharmacy students had poor to moderate preparedness for emergency disasters.15 This situation is particularly dire in mass gathering events as previous studies have highlighted the lack of pharmacy-based strategic action plans for such events.33–35 A scoping literature search revealed that, although action plans may exist for other departments or for healthcare systems in general, less attention has been given to preparation measures specific to pharmacy departments.33–35 Planning pharmaceutical needs, including aspects of health risk assessment and economic assessment, has an integral role in the overall preparedness of the healthcare system. This will ensure the continuity of supply of pharmaceutical products and the provision of pharmacy-based services, as well as ensure the preparedness of the pharmacy workforce for any emergencies during such events.33–35
The pharmacy department in HMC has recognized the importance of having preparedness measures and action plans, hence a wide range of educational and training opportunities were implemented to prepare the staff for any unexpected disaster emergencies that may take place during the tournament. The beneficial outcomes of these measures have been reflected in our findings which, in contrast to previous research, showed that pharmacists working in emergency departments across HMC were at high level of awareness and attitude. Nonetheless, in line with previous work, their readiness level was still moderate to high. The latter could be due to variety of reasons including the training delivery mode and the lack of pharmacy-based professional pathways amongst others. For example, studies showed that high-fidelity simulation training and practice drills could increase the self-confidence of healthcare providers as compared to traditional training methods, which could subsequently improve their self-reported readiness for medical emergencies.36–38 Additionally, on an international level, there is lack of guidelines and advisories for pharmacy professionals to guide workflow and optimize services during emergencies; resulting in lacunae in the proper and effective integration of pharmacists into public health and emergency preparedness and response, which could negatively impact their response capabilities and readiness.39
It is worth noting that only few publications have explored the level of preparedness for previous World Cup tournaments. The focus of these papers was the hospital preparedness rather than staff with no mention for the role of the pharmacy department. For instance, a paper from Germany that focused on the emergency medical preparedness showed that the implemented measures were effective.40 Other studies from South Africa and Brazil indicated that although the overall levels of planning and performance were good, improvements were required in relation to surge capacity, communications and public relations; which emphasizes on the importance of exploring the workforce preparedness and integration of the pharmacy department.41 Lastly, a paper from Qatar that included physicians and nurses working in the emergency department showed that they had a satisfactory level of knowledge and attitude pertaining to the risk of communicable diseases during mass gathering events.42 The latter did not include pharmacist nor focused on the World Cup; however, it supports our findings that healthcare providers in Qatar have received sufficient training for mass gathering events.
Although findings from the current study indicated a moderate correlation between attitude and readiness, the correlation between awareness and readiness was found to be weak. This could be due to multiple factors such as the short-term experience and the lack of disaster experience as most participants had an experience of less than five years. Experience is a complex variable that involves both direct and indirect personal experiences. An example of indirect experience could be an experience of small hazard events that did not impact individuals directly.43 Pharmacists with more than 10 years of experience in Qatar could have an indirect experience with emergency disaster as they were working during previous mass gathering events hosted by the country such as the 2006 Asian Games. This was also emphasized in the post-hoc analysis that showed that pharmacists with longer experience had significantly higher AAR scores as compared to pharmacists with shorter experience. Similarly, a cross-sectional, Europe-wide survey study showed that pharmacists who experienced disasters were more likely to develop standard operating procedures for future events which made them more prepared for and emergency disaster.16
Strengths and Limitations
To our knowledge, this is the first study to investigate the level of preparedness of pharmacists for any mass gathering event such as the FIFA World Cup. The study also has a high response rate of more than 80%. In addition, the study was multi-center as it included three general hospitals in three different cities in the State of Qatar.
The study was limited by the inclusion of emergency departments in general hospitals only. For example, emergency departments in the Heart Hospital were excluded. This could limit the generalizability of our findings. Furthermore, the study relied on self-reported data through a survey which might increase the potential for bias.
Implication for Practice and Research
The role of the pharmacist has been transforming and expanding in recent years. A myriad of studies and systematic reviews has explored the impact of pharmacy-based interventions on patient-related outcomes. Findings from these studies were encouraging as pharmacist-led services were mostly associated with favorable outcomes.44–47 The beneficial influence of pharmacists has also been proven in emergent situation particularly the recent COVID-19 pandemic where pharmacists undertook additional clinical roles and initiated novel pandemic-driven services.12,48 This proves that pharmacists are capable of expanding their pharmaceutical care activities in emergency situations and supports the efforts for embracing new roles for pharmacists. Hence, it is pivotal to involve the pharmacists in disaster management strategies to harness the full potential of their expertise. This is of particular importance in the pre-planning for mass gathering events as their role is seldom examined. Thus, we recommend that future research investigates the potential role for pharmacists in such events in order to shape their roles and propose action frameworks. The roles of community pharmacists should also be explored in further studies because they are the most accessible healthcare providers. This should be followed by an assessment of the feasibility and scalability of such roles in real-world settings. We also recommend utilizing theoretical frameworks in developing such interventions and services as they provide an in-depth understanding of the structural and psychological determinants of behavior at different levels (ie individual, interpersonal, organizational, community, and societal levels). This enables theoretically informed interventions to create a sustainable behavior change.49
Additionally, we encourage healthcare authorities to assess the preparedness of healthcare workforces including pharmacists prior to any mass gathering event. The survey utilized in this study could be used as a reference for future managers and policy makers who are interested in assessing the preparedness of their staff.
Our findings suggested that despite the high awareness and attitude scores, readiness was still moderate to high. This finding should be further investigated in future qualitative studies (eg focus groups) with the same participants as this study design will offer a better understanding of the determinants of causality which could be tackled in future educational and training sessions. It was also noted that the scores were higher in pharmacists with longer experience. This suggests that simulation training and practice drills could probably enhance the readiness of the pharmacy workforce for future mass gathering events in Qatar and worldwide. We encourage policy makers to conduct a learning needs assessment before undertaking educational and training initiatives as this will ensure that the sessions are tailored to the needs of the audience.50
Conclusion
This cross-sectional survey study showed that the majority of emergency pharmacists at HMC have high levels of awareness and attitude for any emergency disaster event during the World Cup; yet only around half of the participants showed high level of readiness. The results of this research can be used as a basis for involving pharmaceutical staff in policy making and training on disaster response which is recognized as a main component of the professional development for frontliners. Future research should focus on the development of theory-based action framework for pharmacy departments to adopt during mass gathering events.
Acknowledgment
Open Access funding provided by the Qatar National Library.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Research Center (MRC) at Hamad Medical Corporation (HMC), grant number (MRC-0122-680).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Federal Emergency Management Agency. Glossary; 2022. Available from: https://training.fema.gov/programs/emischool/el361toolkit/glossary.htm.
2. Zeitz K, Bolton S, Dippy SSR, et al. Measuring emergency services workloads at mass gathering events. Aust J Emerg Manag. 2007;22:23–30.
3. Ranse J, Hutton A, Keene T, et al. Health service impact from mass gatherings: a systematic literature review. Prehosp Disaster Med. 2017;32(1):71–77. doi:10.1017/S1049023X16001199
4. Chhabra N, Gimbar RP, Walla LM, et al. Emergency department patient burden from an electronic dance music festival. J Emerg Med. 2018;54(4):435–439. doi:10.1016/j.jemermed.2017.10.007
5. Saari K. Crowd situations and their policing from the perspective of Finnish police officers—a case study of Finnish police knowledge. J Scand Stud Criminol Crime Prev. 2009;10(2):102–119. doi:10.1080/14043850903320370
6. World Health Organization. Communicable Disease Alert and Response for Mass Gatherings: Technical Workshop. Geneva: World Health Organization; 2008.
7. PreventionWeb. Disaster Risk Management Knowledge Centre (DRMKC) - INFORM: European Commission; 2023. Available from: https://drmkc.jrc.ec.europa.eu/inform-index/INFORM-Risk/Results-and-data/moduleId/1782/id/453/controller/Admin/action/Results.
8. Hamad Medical Corporation. Our accreditations; 2023. Available from: https://www.hamad.qa/EN/About-Us/Our-Accreditations/Pages/default.aspx.
9. Qatar Olympic Committee. Qatar Olympic committee announces, sport events calendar; 2023. Available from: https://www.olympic.qa/media-center/qatar-olympic-committee-announces-2023-sport-events-calendar.
10. Hamad Medical Corporation. Our organization; 2023. Available from: https://www.hamad.qa/EN/About-Us/Our-Organization/Pages/default.aspx.
11. Qatar Tribune. HMC prepares pharmacists for 2022 FIFA World Cup in Qatar; 2023. Available from: https://www.qatar-tribune.com/article/110432/NATION/HMC-prepares-pharmacists-for-2022-FIFA-World-Cup-in-Qatar.
12. Isleem N, Shoshaa S, AbuGhalyoun A, et al. Critical care tele-pharmacy services during COVID-19 pandemic: a qualitative exploration of healthcare practitioners’ perceptions. J Clin Pharm Ther. 2022;47(10):1591–1599. doi:10.1111/jcpt.13709
13. Corrigan M, MacDonald NC, Musselman M, et al. ASHP statement on the role of the pharmacy workforce in emergency preparedness. Am J Health Syst Pharm. 2022;79(23):2185–2189. doi:10.1093/ajhp/zxac226
14. Ford H, Trent S, Wickizer S. An assessment of state board of pharmacy legal documents for public health emergency preparedness. Am J Pharm Educ. 2016;80(2):20. doi:10.5688/ajpe80220
15. McCourt E, Singleton J, Tippett V, et al. Disaster preparedness amongst pharmacists and pharmacy students: a systematic literature review. Int J Pharm Pract. 2021;29(1):12–20. doi:10.1111/ijpp.12669
16. Schumacher L, Bonnabry P, Widmer N. Emergency and disaster preparedness of European hospital pharmacists: a survey. Disaster Med Public Health Prep. 2021;15(1):25–33. doi:10.1017/dmp.2019.112
17. Al-Ziftawi NH, Elamin FM, Mohamed Ibrahim MI. Assessment of knowledge, attitudes, and readiness to practice regarding disaster medicine and preparedness among university health students. Disaster Med Public Health Prep. 2021;15(3):316–324. doi:10.1017/dmp.2019.157
18. Ahmad Suleiman M, Magaji MG, Mohammed S. Evaluation of pharmacists’ knowledge in emergency preparedness and disaster management. Int J Pharm Pract. 2022;30(4):348–353. doi:10.1093/ijpp/riac049
19. Aljabri A, Bakhsh H, Baageel A, et al. Hospital pharmacy preparedness and pharmacist role during disaster in Saudi Arabia. Risk Manag Healthc Policy. 2021;14:5039–5046. doi:10.2147/RMHP.S343789
20. Raosoft, Inc. Sample size calculator; 2022. Available from: http://www.raosoft.com/samplesize.html.
21. Merriam-Webster. Awareness definition; 2022. Available from: https://www.merriam-webster.com/dictionary/awareness#:~:text=noun.something%20is%20happening%20or%20exists.
22. Merriam-Webster. Attitude definition; 2022. Available from: https://www.merriam-webster.com/dictionary/attitude.
23. Merriam-Webster. Readiness definition; 2022. Available from: https://www.merriam-webster.com/dictionary/readiness#:~:text=noun,%3A%20a%20state%20of%20preparation.
24. Gillani AH, Mohamed Ibrahim MI, Akbar J, et al. Evaluation of disaster medicine preparedness among healthcare profession students: a cross-sectional study in Pakistan. Int J Environ Res Public Health. 2020;17:6.
25. Naser WN, Saleem HB. Emergency and disaster management training; knowledge and attitude of Yemeni health professionals- a cross-sectional study. BMC Emerg Med. 2018;18(1):23. doi:10.1186/s12873-018-0174-5
26. Wunderlich R, Ragazzoni L, Ingrassia PL, et al. Self-perception of medical students’ knowledge and interest in disaster medicine: nine years after the approval of the curriculum in German universities. Prehosp Disaster Med. 2017;32(4):374–381. doi:10.1017/S1049023X17000280
27. Sabra JP, Cabañas JG, Bedolla J, et al. Medical support at a large-scale motorsports mass-gathering event: the inaugural formula one United States grand prix in Austin, Texas. Prehosp Disaster Med. 2014;29(4):392–398. doi:10.1017/S1049023X14000636
28. Koski A, Kouvonen A, Sumanen H. Preparedness for mass gatherings: factors to consider according to the rescue authorities. Int J Environ Res Public Health. 2020;17(4):1361. doi:10.3390/ijerph17041361
29. Arbon P. Planning medical coverage for mass gatherings in Australia: what we currently know. J Emerg Nurs. 2005;31(4):346–350. doi:10.1016/j.jen.2005.03.002
30. Koski A, Pappinen J, Kouvonen A, et al. Preparedness for mass gatherings: rescue and emergency medical services’ workloads during mass gathering events. Scand J Trauma Resusc Emerg Med. 2022;30(1):15. doi:10.1186/s13049-022-01003-7
31. Ciottone G. Introduction to disaster medicine. Ciottones Disaster Med. 2016;2016:2–5.
32. Shoaf KI, Rottman SJ. The role of public health in disaster preparedness, mitigation, response, and recovery. Prehosp Disaster Med. 2000;15(4):144–146. doi:10.1017/S1049023X00025243
33. Cecchi A, Carchietti E. A planning model of pharmaceutical needs for mass gatherings at public special events. Pharm Regul Aff. 2013;2(1):2–3.
34. Alomi Y. National mass gathering pharmaceutical care program at MOH in Saudi Arabia. J Pharm Pract Res Comm Med. 2016;2:102–103. doi:10.5530/jppcm.2016.3.9
35. Alomi Y, Alhennawi K, Khayayt N. Pharmacy workload and workforce requirements at moh hospitals during ten years mass gathering hajj (2006–2015) in Makkah Region, Saudi Arabia. J Pharm Pract Res Comm Med. 2017;3:s75–s83. doi:10.5530/jppcm.2017.4s.52
36. Thompson Bastin ML, Cook AM, Flannery AH. Use of simulation training to prepare pharmacy residents for medical emergencies. Am J Health Syst Pharm. 2017;74(6):424–429. doi:10.2146/ajhp160129
37. Mercuzot C, Debien B, Riviere É, et al. Impact of a simulation-based training on the experience of the beginning of residency. Rev Med Interne. 2021;42(11):756–763. doi:10.1016/j.revmed.2021.07.002
38. Shin S, Park JH, Kim JH. Effectiveness of patient simulation in nursing education: meta-analysis. Nurse Educ Today. 2015;35(1):176–182. doi:10.1016/j.nedt.2014.09.009
39. Aruru M, Truong HA, Clark S. Pharmacy Emergency Preparedness and Response (PEPR): a proposed framework for expanding pharmacy professionals’ roles and contributions to emergency preparedness and response during the COVID-19 pandemic and beyond. Res Social Adm Pharm. 2021;17(1):1967–1977. doi:10.1016/j.sapharm.2020.04.002
40. Betlehem J, Schaefer J. Emergency medical preparedness during the 2006 World Cup in Frankfurt, Germany. Disasters. 2010;34(1):155–163. doi:10.1111/j.1467-7717.2009.01119.x
41. Valesky W, Silverberg M, Gillett B, et al. Assessment of hospital disaster preparedness for the 2010 FIFA World Cup using an internet-based, long-distance tabletop drill. Prehosp Disaster Med. 2011;26(3):192–195. doi:10.1017/S1049023X11006443
42. Al-Romaihi H, Al-Dahshan A, Kehyayan V, et al. Knowledge, attitude, and training of health-care workers and preparedness of hospital emergency departments for the threat of communicable diseases at mass gathering events in Qatar: a cross-sectional study. Disaster Med Public Health Prep. 2021;2021:1–5.
43. Becker JS, Paton D, Johnston DM, et al. The role of prior experience in informing and motivating earthquake preparedness. Int J Disaster Risk Reduct. 2017;22:179–193. doi:10.1016/j.ijdrr.2017.03.006
44. El-Awaisi A, Al-Shaibi S, Al-Ansari R, et al. A systematic review on the impact of pharmacist-provided services on patients’ health outcomes in Arab countries. J Clin Pharm Ther. 2022;47(7):879–896. doi:10.1111/jcpt.13633
45. Jaam M, Naseralallah LM, Hussain TA, et al. Pharmacist-led educational interventions provided to healthcare providers to reduce medication errors: a systematic review and meta-analysis. PLoS One. 2021;16(6):e0253588. doi:10.1371/journal.pone.0253588
46. Naseralallah LM, Hussain TA, Jaam M, et al. Impact of pharmacist interventions on medication errors in hospitalized pediatric patients: a systematic review and meta-analysis. Int J Clin Pharm. 2020;42(4):979–994. doi:10.1007/s11096-020-01034-z
47. Al-Qahtani S, Jalal Z, Paudyal V, et al. The role of pharmacists in providing pharmaceutical care in primary and secondary prevention of stroke: a systematic review and meta-analysis. Healthcare. 2022;10:11. doi:10.3390/healthcare10112315
48. Ahmed A, Tanveer M, Shrestha S, et al. Interventions and impact of pharmacist-delivered services for people infected with COVID-19: a systematic review. Healthcare. 2022;10:9. doi:10.3390/healthcare10091630
49. Naseralallah L, Stewart D, Azfar Ali R, et al. An umbrella review of systematic reviews on contributory factors to medication errors in health-care settings. Expert Opin Drug Saf. 2022;21(11):1379–1399. doi:10.1080/14740338.2022.2147921
50. Al-Ismail MS, Naseralallah LM, Hussain TA, et al. Learning needs assessments in continuing professional development: a scoping review. Med Teach. 2022;2022:1–9.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.