Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Digoxin Toxicity at Standard Doses in a Child with Subclinical Elevation of Thyrotrophin: A Case Report
Authors Khorgami M, Dalili M, Karimian B
Received 9 August 2025
Accepted for publication 14 November 2025
Published 23 December 2025 Volume 2025:17 Pages 265—267
DOI https://doi.org/10.2147/DHPS.S553017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hemalkumar B Mehta
Mohammadrafie Khorgami,1 Mohammad Dalili,1 Bahareh Karimian2
1Cardiac Electrophysiology Research Center, Rajaie Cardiovascular Institute, Tehran, Iran; 2Clinical Research Development Unit, Hajar Hospital, Shahrekord University of Medical Sciences, Shahrekord, Iran
Correspondence: Bahareh Karimian, Clinical Research Development Unit, Hajar Hospital, Shahrekord University of Medical Sciences, Shahrekord, Iran, Tel +98-9382726939, Email [email protected]
Abstract: Digoxin toxicity poses a challenge for patients using the drug. Electrolyte disturbances, renal failure, and drug interactions are common predisposing factors. Hypothyroidism can increase the risk of digoxin toxicity primarily. This research reports a 7-year-old boy receiving digoxin 6 μg/kg/day presented with nausea and second-degree atrioventricular block secondary to ongoing digoxin toxicity. Initiation of levothyroxine for subclinical elevation of thyrotrophin resulted in rapid resolution of symptoms and normalization of digoxin levels.
Keywords: digoxin, drug toxicity, subclinical hypothyroidism, children
Introduction
Digoxin is prescribed in selected pediatric patients with congenital or acquired heart disease, yet its narrow therapeutic index makes toxicity a significant concern.1 Reported prevalence of digoxin toxicity is around 1% among treated patients, though pediatric cases are relatively rare and often result from accidental overdose.2–4
Standard pediatric maintenance doses for school-age children typically range from 5–10 μg/kg/day, divided into two doses. Toxicity is usually linked to predisposing factors such as electrolyte abnormalities, renal impairment, or drug–drug interactions (Table 1). Less frequently, thyroid dysfunction has been implicated.5 In hypothyroidism, reduced renal perfusion and altered expression of Na⁺/K⁺-ATPase may influence digoxin clearance and sensitivity, even in subclinical cases where T3/T4 remain normal but TSH is elevated.6
 |
An additional consideration is digoxin-like immunoreactive substances (DLIS), which may cause falsely elevated digoxin levels on immunoassays. However, these typically occur without corresponding symptoms, differentiating them from true digoxin toxicity.9
Here, we present a novel pediatric case of subclinical elevation of thyrotrophin–associated digoxin toxicity occurring at a standard therapeutic dose, underscoring the importance of thyroid screening in patient safety.
Case Report
A 7-year-old boy presented with persistent nausea, vomiting, abdominal pain, lethargy, and arrhythmia. His past history included surgical closure of a ventricular septal defect and tricuspid valve repair. He had been prescribed oral digoxin at 6 μg/kg/day in two divided doses for three months. The day before admission, a serum digoxin test performed elsewhere showed >5 ng/mL, prompting referral.
On admission, his ECG demonstrated 2nd-degree AV block (Mobitz type I) (Figure 1). Laboratory results showed normal electrolytes (Na, K, Mg), and normal renal and hepatic function. A repeat ELISA digoxin assay confirmed >5 ng/mL. Digoxin was discontinued.
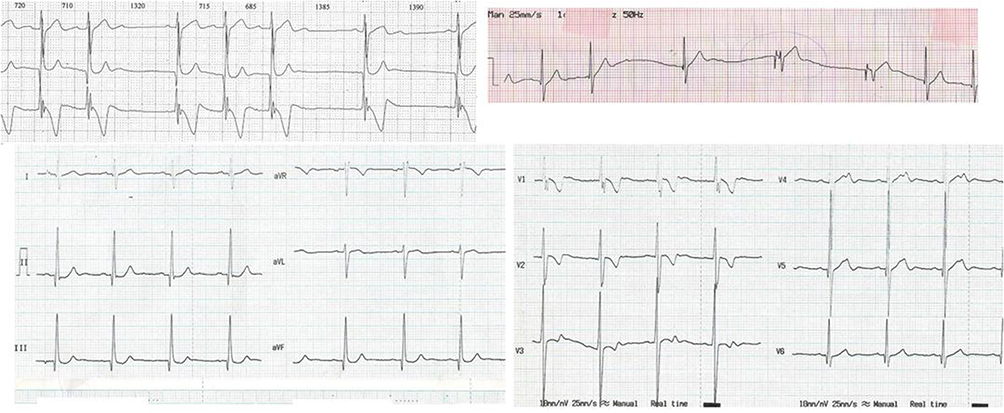 |
Figure 1 Electrocardiogram of the Patient with Digoxin Toxicity. |
During the first hospital night, he developed sinus node dysfunction and bradycardia <30 bpm, requiring a temporary pacemaker. Despite cessation of digoxin, serum levels and clinical symptoms persisted for several days.
On day 7, thyroid function tests revealed TSH 7.9 μIU/mL (ref 0.3–5.1) with normal T3 and T4, consistent with subclinical elevation of thyrotrophin. Pediatric endocrinology-initiated levothyroxine. Within 48 hours, symptoms began improving and digoxin levels decreased; by day 4 post-levothyroxine, serum digoxin was 2.4 ng/mL, and the pacemaker was removed. The patient was discharged on levothyroxine; digoxin was not restarted as it was deemed no longer clinically necessary.
Ethics
Written informed consent, including for publication of ECG and clinical data, was obtained from the patient’s guardian at the Rajaie Cardiovascular Institute. Institutional approval was not required to publish the case details.
Discussion
This case illustrates true digoxin toxicity in a child receiving a standard weight-based dose, with subclinical elevation of thyrotrophin identified as the likely predisposing factor.
Previous studies have suggested elevation of thyrotrophin may reduce digoxin clearance via decreased renal blood flow and altered distribution.5,10,11 Moreover, thyroid hormones regulate Na⁺/K⁺-ATPase, potentially modifying digoxin sensitivity.6 Even mild TSH elevation without overt hypothyroidism may shift the pharmacodynamic balance. The temporal association of levothyroxine initiation with both clinical recovery and biochemical improvement supports a causal role. DLIS interference is an alternative explanation for high serum levels.7,8 However, DLIS typically causes elevated assays without symptoms, unlike our patient who manifested severe bradyarrhythmia. Thus, interference is unlikely. Pediatric digoxin toxicity linked to subclinical elevation of thyrotrophin with normal renal function has rarely been documented. This case highlights the importance of considering endocrine factors in unexplained digoxin toxicity.
One of the limitations of this report is the single-case nature of the study, which limits the possibility of definitively proving a causal relationship between subclinical elevation of thyrotrophin and persistent digoxin toxicity. In addition, there is a possibility of overestimation of serum digoxin levels by ELISA, although the simultaneity of clinical symptoms and rapid improvement after levothyroxine initiation suggests that the increased digoxin levels in this patient represented true toxicity.
Conclusion
Subclinical elevation of thyrotrophin may predispose children to clinically significant digoxin toxicity even at standard therapeutic doses. For patient safety, routine thyroid function testing should be considered in pediatric patients presenting with unexplained digoxin toxicity or persistently elevated serum digoxin levels. Given the limited evidence regarding the influence of thyroid-stimulating hormone on digoxin metabolism, further mechanistic and large multicenter studies are warranted to clarify this association and establish evidence-based screening and monitoring protocols to enhance medication safety in pediatric cardiac care.
Acknowledgments
The authors would like to express their appreciation to the Rajaie Cardiovascular Medical and Research Institute of Tehran, Iran.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Dan AR, Martínez-Rubio A, Buzea CA. Multitarget Autonomic Acting Drugs. In: Antiarrhythmic Drugs. Cham: Springer Nature Switzerland; 2025:197–226.
2. Sheikh S, Munson T, Garvan G, et al. Characterizing utilization and outcomes of digoxin immune fab for digoxin toxicity. Drugs-Real World Outcomes. 2024;11(3):377–388. doi:10.1007/s40801-024-00435-0
3. Zhang H, Huo Q, Jing R, Dong M. Clinical analysis of acute poisoning in children. BMC Pediatric. 2024;24(1):212. doi:10.1186/s12887-024-04697-z
4. Barati L, Vakili M, Mehrpour O, Teimoorian M. Clinical manifestation and laboratory data of illicit drugs versus other substances intoxication in children. Sci Rep. 2025;15(1):802. doi:10.1038/s41598-024-79424-w
5. Rolon L, Akhras A, Nabi S, Ichoa I, Heller D. A case of digoxin toxicity complicated by overt hypothyroidism. Chest. 2024;166(4):A841. doi:10.1016/j.chest.2024.06.567
6. Cordeiro BM, Leite Fontes CF, Meyer-Fernandes JR. Molecular basis of Na, K–ATPase regulation of diseases: hormone and FXYD2 Interactions. Int J Mol Sci. 2024;25(24):13398. doi:10.3390/ijms252413398
7. Naguib R, Elkemary E. Thyroid dysfunction and renal function: a crucial relationship to recognize. Cureus. 2023;15(2). doi:10.7759/cureus.35242
8. Koca HB, Oncu S, Becit-Kizilkaya M, Gokaslan S. Evaluation of therapeutic and toxic levels of serum digoxin concentration: a cross-sectional study from a tertiary hospital. Eur Rev Med Pharmacol Sci. 2024;28(3).
9. Dasgupta A. Challenges In Therapeutic Drug Monitoring Of Digoxin And Other Antiarrhythmic Drugs. In: Therapeutic Drug Monitoring. Academic Press; 2024:163–195.
10. Kalra S, Aggarwal S, Khandelwal D. Thyroid dysfunction and dysmetabolic syndrome: the need for enhanced thyrovigilance strategies. Int J Endocrinol. 2021;2021(1):9641846. doi:10.1155/2021/9641846
11. Gottwald-Hostalek U, Schulte B. Low awareness and under-diagnosis of hypothyroidism. Curr Med Res Opin. 2022;38(1):59–64. doi:10.1080/03007995.2021.1997258
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.