Back to Journals » Orthopedic Research and Reviews » Volume 18
Digital Health and Smart Technologies in Shoulder Arthroplasty: Emerging Tools and Clinical Implications
Authors Lazaridou A, Kraus M, Oettl FC, Imiolczyk JP, Back DA, Scheibel M
Received 28 February 2026
Accepted for publication 1 May 2026
Published 12 June 2026 Volume 2026:18 605861
DOI https://doi.org/10.2147/ORR.S605861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qian Chen
Asimina Lazaridou,1,2 Moritz Kraus,1 Felix Conrad Oettl,3 Jan-Philipp Imiolczyk,1,4 David A Back,4 Markus Scheibel1,4 On behalf of DVSE New Technologies Committee
1Department for Shoulder and Elbow Surgery, Schulthess Clinic, Zurich, Switzerland; 2Department of Anesthesiology, Brigham & Women’s Hospital and Harvard Medical School, Boston, MA, USA; 3Department of Orthopedic Surgery, Balgrist University Hospital, University of Zurich, Zurich, Switzerland; 4Department for Shoulder and Elbow Surgery, Center for Musculoskeletal Surgery, Charité University Medicine Berlin, Berlin, Germany
Correspondence: Asimina Lazaridou, Schulthess Clinic, Lengghalde 2, Zurich, CH-8008, Switzerland, Tel +41 44 385 79 77, Email [email protected]
Purpose: Shoulder arthroplasty has evolved substantially in surgical technique, implant design, and indications. Careful coordination across the patient care pathway remains central to optimizing outcomes. Concurrently, rapid advances in digital health, wearable technologies, smart implants, and intraoperative innovations are being explored across orthopedics, with emerging applications in shoulder arthroplasty.
Objective: This narrative review synthesizes current evidence on digital technologies relevant to shoulder arthroplasty, with particular attention to the strength and origin of the available data.
Patients and Methods: A structured review of recent literature was performed, including primary studies in shoulder arthroplasty as well as relevant evidence extrapolated from hip and knee arthroplasty. Areas examined included CT-based 3D planning, navigation, patient-specific instrumentation, robotics, augmented/mixed reality, mobile health (mHealth) platforms, wearable devices, tele-rehabilitation, sensor-enabled implants, and artificial intelligence (AI).
Results: In shoulder arthroplasty, digital planning tools, navigation systems, and patient-specific instrumentation have demonstrated improvements in implant positioning accuracy in selected studies; however, evidence linking these technologies to superior long-term clinical outcomes remains limited. Robotic systems and augmented reality applications are in early investigational phases. Postoperative digital health tools, including tele-rehabilitation and wearable monitoring, have shown non-inferior functional outcomes compared with conventional care in hip and knee arthroplasty, with only preliminary and pilot data currently available in shoulder populations. Sensor-enabled implants and AI-based predictive models represent emerging areas of research, but external validation, workflow integration, and cost-effectiveness analyses remain insufficient.
Conclusion: Digital and smart health technologies in shoulder arthroplasty are evolving and largely investigational. While early findings and extrapolated evidence from other arthroplasty domains suggest potential benefits in planning accuracy, patient engagement, and outcome monitoring, robust shoulder-specific clinical validation is limited. Further prospective studies are required before widespread clinical adoption can be recommended. This narrative review synthesizes emerging evidence in this field, which is currently dominated by feasibility studies, technical reports, and early-phase clinical investigations, with limited high-level outcome data specific to shoulder arthroplasty.
Keywords: telemedicine, mobile applications, wearable electronic devices, telerehabilitation, robotics, augmented reality, biomedical technology
Background
Shoulder arthroplasty has advanced considerably with improvements in surgical techniques and implant design, leading to better outcomes and expanding indications for treatment.1 However, postoperative outcomes remain a critical determinant of long-term success, influencing functional recovery, pain management, and implant longevity. In recent years, rapid innovations in digital health technologies and smart devices have transformed the landscape of orthopedic rehabilitation, especially after shoulder and knee surgeries, and monitoring, offering more personalized, data-driven approaches to care.2
Mobile health (mHealth) applications, wearable devices, remote monitoring systems, and sensor-enabled implants are increasingly integrated into orthopedic care pathways.3,4 mHealth applications, which have been extensively evaluated in hip and knee arthroplasty, offer patient education, rehabilitation instruction, pain monitoring, and secure communication. Studies show that these platforms can achieve outcomes comparable to traditional in-person physiotherapy. In addition, wearable sensors and telemedicine systems enable continuous and objective monitoring of patient activity and recovery, and remote rehabilitation programs have demonstrated high levels of patient engagement and satisfaction after reverse shoulder arthroplasty.5
Beyond patient-facing tools, intraoperative innovations such as robotics, augmented reality, and artificial intelligence (AI) are improving surgical precision, enhancing reproducibility, and laying the foundation for smart, connected surgical ecosystems. Emerging sensor-enabled implants take this a step further, providing real-time data on shoulder implant performance, joint loading, and potential complications before clinical symptoms arise.6
This narrative review focuses on emerging digital and smart technologies in shoulder arthroplasty, drawing primarily from literature published within the past decade and indexed in major medical databases, including PubMed and Embase, supplemented by relevant technical and pilot reports. Given the early maturity of this field, a substantial proportion of the available evidence consists of feasibility studies, pilot trials, and technical reports, with relatively few randomized studies or long-term outcome data specific to shoulder arthroplasty. For example, recent analyses of emerging technologies in shoulder surgery have shown that many studies focus on technical feasibility, surrogate endpoints (eg, implant positioning accuracy), or small patient cohorts, with limited external validation Accordingly, this narrative review aims to synthesize current concepts and emerging technologies in shoulder arthroplasty, with a particular focus on their clinical applicability, level of evidence, and limitations. Specifically, this review seeks to address the following questions: (1) What digital and smart technologies are currently being applied across the perioperative pathway in shoulder arthroplasty? (2) What is the current level of clinical evidence supporting their use? and (3) what are the key challenges and gaps that must be addressed for broader clinical implementation?
Methods
This narrative review was conducted to summarize current evidence on digital and smart technologies in shoulder arthroplasty. A literature search was performed using major medical databases, including PubMed and Embase, covering publications from January 2013 to 2026. Search terms included combinations of “shoulder arthroplasty”, “digital health”, “telemedicine”, “wearable sensors”, “artificial intelligence”, “robotics”, and “augmented reality”. Relevant peer-reviewed articles, including clinical studies, systematic reviews, and selected technical reports, were considered. Priority was given to studies focusing on shoulder arthroplasty; however, where shoulder-specific data were limited, relevant evidence from hip and knee arthroplasty or related orthopaedic fields was included to provide context. Given the narrative nature of this review, no formal systematic selection process or quality scoring was performed. Articles were selected based on relevance to the topic and contribution to current understanding. The included studies were qualitatively categorized according to study design (eg, randomized trials, observational studies, and technical or feasibility reports) to facilitate interpretation of the level of evidence Given the heterogeneity of the literature, emphasis was placed on distinguishing between surrogate endpoints (eg, technical accuracy) and clinically meaningful outcomes (eg, pain, function, implant survivorship) during synthesis Given the narrative nature of this review, no formal quantitative synthesis or meta-analysis was performed. Accordingly, no independent statistical analysis was conducted. The included literature was qualitatively assessed and synthesized to provide an overview of current concepts, evidence levels, and emerging trends (Table 1).
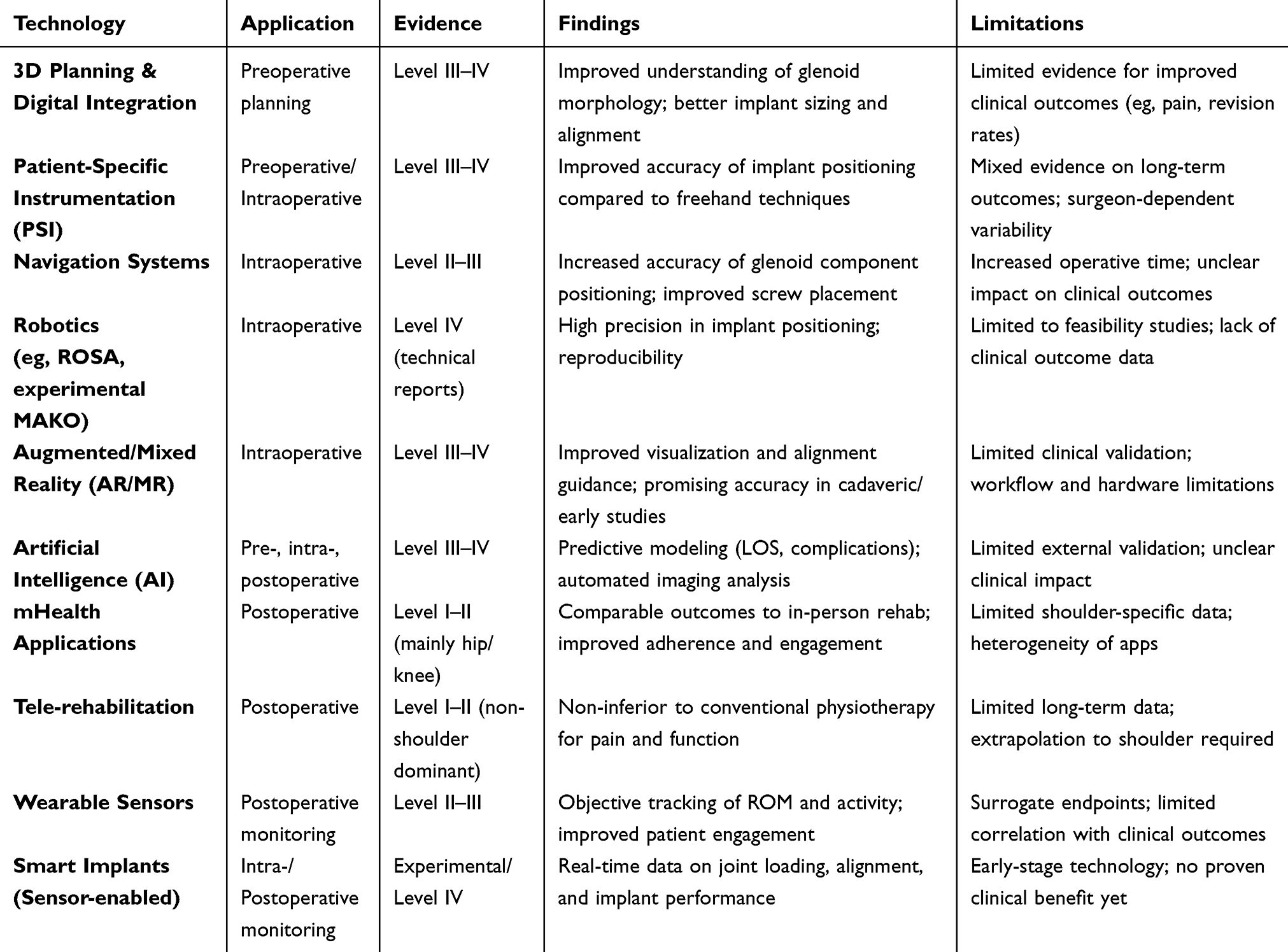 |
Table 1 Summary of Technologies, Clinical Applications, and Evidence in Shoulder Arthroplasty |
Preoperative Digital Assistance
Digital Integration and 3D Planning
Preoperative digital tools have become integral to shoulder arthroplasty, covering planning, intraoperative use, and postoperative evaluation. CT-based 3D reconstructions can already be considered standard practice in the virtual planning of glenoid inclination, version, implant sizes and alignment (especially of the base plate).7 Another aspect is the planning of osseous polyethylene or metallic wedges or even customized 3D printing for drilling templates or even implants for glenoid deformities or substance loss.8 For example, recent studies have demonstrated the use of CT-based 3D planning platforms combined with patient-specific instrumentation (PSI) to optimize glenoid component positioning and improve agreement between planned and achieved implant alignment. In addition, automated planning tools incorporating statistical shape modeling and AI-assisted segmentation have been shown to enhance reproducibility and reduce user-dependent variability in preoperative planning. These approaches allow surgeons to simulate different implant configurations, assess bone stock, and preoperatively optimize fixation strategies in cases of complex deformity or bone loss.7,9–12 Compared with traditional 2D imaging, 3D reconstruction provides a more accurate understanding of glenoid morphology, deformity, and wear patterns. The vault model described by Iannotti et al has been foundational in this regard, enabling improved assessment of glenoid version, inclination, and bone stock relative to the scapular plane. This has helped mitigate known limitations of 2D imaging, which can be misleading and may influence implant selection, component positioning, and anatomic and kinematic considerations. In cases of severe bone loss, 3D planning additionally supports the use of augmented or patient-specific implants, although their role remains controversial and surgeon preference varies.13
Challenges and Implementation Barriers of Technology
Most of the challenges of using digital perioperative solutions are the costs including equipment and licensing costs. Other aspects include the necessary adaptation of workflows with corresponding logistics and learning curves for the application. Head-mounted AR solutions also affect wearing comfort with possible transmission latency compared to navigation. Many digital applications still require clear cost-benefit evidence and evidence of benefit. Evidence on hard clinical endpoints is still limited in some cases or focused on feasibility and cadaver studies.
Among AI applications is eg the documentation with AI scribes for automated speech recognition during operations and following surgical and nursing documentation as well a guidance of logistics with re-ordering of used materials.14 Big data from preoperative 3D planning, intraoperative navigation or robotics with AI-supported image and motion analysis with respective registries will furthermore form the basis for continuous outcome learning and digital twin-supported patient-specific simulations.15 While several studies demonstrate improved implant positioning accuracy and reproducibility with navigation or patient-specific instrumentation, these outcomes represent surrogate technical endpoints. Current evidence remains limited regarding whether enhanced alignment precision translates into improved pain relief, functional outcomes, complication reduction, or long-term implant survivorship.
Current and emerging roles of artificial intelligence (AI) in shoulder surgery, emphasizing its growing impact on clinical practice. Present-day applications include automated imaging analysis for diagnosing rotator cuff tears and other pathologies, surgical planning tools, risk prediction models for complications, and systems for tracking patient outcomes.16 Current research primarily focuses on technical metrics such as classification or object detection rather than clinical outcomes. These findings highlight that while AI has potential to enhance intraoperative decision-making and precision, its integration into surgical practice remains limited, emphasizing the need for standardized frameworks, clinical validation, and careful evaluation of safety and effectiveness.17 Importantly, many reported improvements relate to technical accuracy or process metrics, and should not be interpreted as direct evidence of improved clinical outcomes without prospective validation.
Intraoperative Innovations
Navigation, AR, and Robotics
Intraoperative assistance and robotic technologies are ameliorating modern orthopedic surgery, particularly in shoulder arthroplasty, by aiming to improve surgical precision, reproducibility, and consistency of implant placement.
Emerging technologies including navigation, augmented/mixed reality (AR/MR), and robotics are improving precision and reproducibility. In a recent clinical series on RSA with CT-based planning and additional navigation, similar radiological and functional results were observed compared to standard procedures with fewer screws with longer lengths in the navigated group but also a longer surgical time.18 Commercial digital planning tools are possible for both anatomical and reverse shoulder prostheses. Intraoperative technology plays an increasingly important role in improving the precision and reproducibility of shoulder arthroplasty. Innovations include robotic arm assistance, navigation systems, augmented reality (AR), and intraoperative feedback tools that enhance surgical accuracy and may improve implant longevity.17 Patient-specific implants (PSI) based on digitally 3D-printed drilling templates are useful for glenoid guidance compared to freehand techniques; PSI and custom-made implants are particularly important in cases of complex defects.19,20 Navigation with real-time feedback on drilling directions and implant positioning is highly beneficial. Initial reliable clinical data show more precise version/inclination and more efficient screw placement, especially of the glenoid components in RSA.20,21 Mixed reality and augmented reality systems display planning data in the surgical field of view via head-mounted displays.22 From a clinical perspective, the relevance of these findings depends on whether improvements in technical performance translate into meaningful benefits for patients, including reduced pain, improved function, or lower revision rates. However, these findings are largely based on surrogate endpoints such as implant positioning accuracy or short-term functional measures and should not be assumed to translate into improved patient-reported outcomes or long-term implant survivorship without further validation. Preclinical and clinical studies in shoulder arthroplasty show low deviations between planning and postoperative results, in general, navigation appears to be superior to freehand execution and equal to PSI23 Current preliminary studies also report higher precision for glenoid preparation in RSA compared to manual implantation or PSI.24 However, it must be emphasized that shoulder robotics is still in its very early stages compared to hip and, above all, knee arthroplasty.25 Robotic assistance in shoulder arthroplasty is beginning to move from concept toward clinical reality with data being scarce. One key milestone was the world’s first robotic-assisted shoulder replacement, which was performed at Mayo Clinic by John W. Sperling following FDA 510(k) clearance of the ROSA Shoulder system in 2024 (Zimmer Biomet, Warsaw, Indiana, USA). The ROSA platform designed for both anatomic and reverse shoulder replacement enables preoperative planning, intraoperative feedback, and more precise implantation of glenoid and humeral components. Early reports describing robotic-assisted shoulder arthroplasty, including the ROSA Shoulder system, are primarily technical descriptions and feasibility reports rather than peer-reviewed clinical outcomes studies. These reports demonstrate workflow integration and technical accuracy but do not yet provide robust data on patient-reported outcomes, complication rates, or long-term implant survivorship.26 In parallel, the Mako system (Stryker, Lauderdale by the Sea, Florida, USA) is being adapted experimentally for shoulder procedures, particularly for controlled glenoid preparation using haptic guidance, and has been discussed in the literature as a promising tool to enhance baseplate positioning accuracy.27
However, current evidence remains limited to preclinical studies and technical feasibility reports, without established clinical outcome data in shoulder arthroplasty.
Robotic Arm Assistance, while predominantly utilized in hip and knee arthroplasty, holds significant future potential for optimizing bone preparation and humeral cuts in shoulder surgery, enhancing accuracy in component positioning.14 These systems allow surgeons to execute patient-specific plans with greater consistency. Navigation Systems provide real-time intraoperative guidance and feedback, which has been shown to improve the accuracy of glenoid component positioning, maximize baseplate fixation, and substantially reduce malposition. Systems such as ExactechGPS (Gainesville, Florida),28 for instance, offer dynamic real-time feedback for screw trajectory and length during reverse total shoulder arthroplasty, leading to longer and more effective screw fixation compared to non-navigated procedures.29 Preoperative planning, particularly with 3D computed tomography (CT) images and patient-specific instrumentation, has been demonstrated to significantly enhance the agreement between the ideal planned position and the final implanted position of components. While navigation can increase surgical time, potentially due to a learning curve, studies have reported significantly improved accuracy in glenoid component placement, reducing errors in version from, for example, 10.6 degrees without navigation to 4.4 degrees with navigation.29 However, limitations include higher costs, potential intraoperative malfunctions, and a lack of easy portability.
Augmented Reality and Mixed Reality Applications
Augmented Reality (AR) and Mixed Reality (MR) technologies in shoulder arthroplasty offer an approach, providing improved visualization of anatomy and implant alignment by projecting preoperative plans directly onto head-mounted displays (HUDs) worn by the surgeon.10 This allows surgeons to remain focused on the operative field while receiving real-time information on implant version, inclination, entry point, and reaming depth. AR/MR can address some disadvantages of patient-specific instrumentation and pure navigation by offering real-time feedback with simplified overlay processes. For example, the Microsoft HoloLens has been used in cadaveric shoulder studies to guide glenoid guide-pin placement with high accuracy, demonstrating mean trajectory errors significantly lower than free-hand techniques.6 More advanced systems, like NextAR (Medacta International SA, Castel San Pietro, Switzerland),30 combine MR with intraoperative navigation, providing real-time planned-versus-actual trajectory information for all steps of glenoid component placement. These technologies not only improve accuracy but also hold promise for surgical training and tele-mentoring.
Artificial Intelligence and Predictive Analytics
The broader application of Artificial Intelligence (AI) and Machine Learning (ML) is increasingly evident, leveraging large, complex datasets to support clinical decision-making before, during, and after shoulder surgery.6 AI models can predict length of hospital stay, healthcare costs, clinical outcomes, and complications, thereby personalizing care and optimizing resource allocation. However, these findings are largely based on surrogate endpoints such as prediction accuracy and model performance, and their translation into meaningful improvements in clinical outcomes remains uncertain. In postoperative care and rehabilitation, AI algorithms can analyze continuous data from wearable devices to objectively assess functional recovery and rehabilitation compliance.6 For instance, in patients with adhesive capsulitis, wearable motion sensor devices coupled with mobile applications allowed for personalized home-based exercises and remote supervision, leading to better and faster improvements in shoulder ROM compared to traditional methods.31 AI also enhances surgical robotic systems by improving their ability to recognize complex environments, make predictions, and execute tasks with superior precision and efficiency.32
While these technologies present advantages, including reduced surgical variability, increased consistency of shoulder implant placement, and the potential for improved shoulder implant longevity and functional outcomes, their widespread adoption is tempered by acknowledged limitations such as higher costs, longer operating times, and the necessity for a significant learning curve.24 In addition, recent evidence from machine learning (ML) applications in shoulder arthroplasty suggests that predictive analytics are emerging: a systematic review by Schneller et al identified 25 studies applying ML to total shoulder arthroplasty (TSA), of which ~40% used imaging data and ~60% used tabular clinical data. In those studies, several models achieved fair to good performance in predicting clinical outcomes, yet only three underwent external validation, pointing out challenges in transparency and generalizability.33
Ethical considerations, data security, and privacy also require robust frameworks for successful implementation in clinical settings.34 In addition, improvements in accuracy, precision, and monitoring represent surrogate endpoints and should not be presumed to improve pain, function, or long-term implant survivorship. Current evidence remains mixed regarding whether enhanced measurement translates into better clinical outcomes.
Postoperative Management
Postoperative Rehabilitation and Monitoring
Mobile applications designed for postoperative care can deliver personalized rehabilitation plans, pain-tracking tools, and medication reminders. Studies have shown mHealth apps can improve engagement, adherence, and patient satisfaction in orthopedic populations.35 Apps such as myRehab (My Rehab Pro LLC, Louisville, Kentucky, USA), and custom institution-based tools are increasingly integrated into care pathways for shoulder arthroplasty.36
Smartphone apps are increasingly embedded into perioperative pathways for hip, knee and shoulder procedures. Typical features include education, day-by-day rehab plans with video exercises, medication and wound-care reminders, secure messaging, and symptom/PROMs capture often integrated with the EHR via standards such as FHIR. Early implementation work in knee arthroplasty shows that institution-built apps can streamline education and PROMs collection and are feasible at scale within clinical workflows.37
Tele-Rehabilitation and App-Supported Programs
On effectiveness, a strong body of evidence comes from tele-rehabilitation and app-supported home programs after total knee and hip arthroplasty. Multiple randomized and comparative studies indicate that remote, app-enabled rehabilitation is generally non-inferior to conventional in-person physiotherapy for pain, function, and range of motion. Meta-analyses report small to moderate effect sizes, with standardized mean differences typically ranging from approximately −0.1 to 0.3 across key outcomes, and no clinically meaningful differences between groups. These findings support remote delivery as a viable alternative when appropriately implemented.38
In addition, patient engagement and satisfaction are generally high when content is tailored and reminders are used; orthopedic cohorts report favorable perceptions of app usefulness for recovery monitoring and communication. Apps can also improve completion of patient-reported outcomes by enabling push-prompted submissions outside clinic visits.37 At the same time, multiple reviews caution that clinical impact estimates vary because apps differ widely (content, coaching intensity, sensor use) and studies often have short follow-up or moderate risk of bias. Key implementation risks include digital literacy barriers in older adults, variable adherence once novelty fades, data privacy/security obligations, and the need for interoperability with clinical systems to avoid parallel shadow workflows.39
In postoperative orthopedics, mHealth apps can feasibly deliver personalized rehab plans, track pain and function, and support medication/education tasks while maintaining outcomes comparable to traditional care, especially for knee arthroplasty, provided programs address engagement, equity, and integration.40
Interestingly, to date, there are no definitive clinical mHealth apps targeting postoperative rehabilitation in shoulder arthroplasty. Only one known pilot trial has evaluated a smartphone-based chatbot for postoperative RSA rehabilitation, demonstrating improved adherence and potential functional benefits, while another is currently underway as a multi-center RCT. Additionally, work exists on mobile versions of outcome measures and shoulder pain apps, but not rehabilitation-specific applications.41
Wearables and Objective Functional Monitoring
In addition, the integration of wearable digital tools into rehabilitation after shoulder surgery significantly enhances patient activation, motivation, and engagement.31,42,43 These technologies facilitate continuous tracking of physical activity and joint motion in real-world environments, overcoming the limitations of traditional clinical assessments and yielding objective, quantitative data.44–46 Common device types include motion sensors, such as Inertial Measurement Units (IMUs) and magneto-Inertial Measurement Units (M-IMUs), which incorporate accelerometers, gyroscopes, and often magnetometers to track 3D orientation and shoulder joint angles.47 While research may utilize multiple sensors affixed to the thorax, scapula, and arm to capture detailed kinematics, at-home applications often employ simpler configurations of one or two sensors (eg bracelet-type smartwatch) wearables) to reliably measure shoulder Range of Motion (ROM).48 Smartwatches also employ integrated inertial sensors for exercise recognition and motion monitoring, espespically scapular kinematics.49 Furthermore, EMG-based wristbands measure muscle activation to guide rehabilitation progress.34 In clinical applications, these technologies enable the quantification of range of motion in real-world settings, which is crucial for assessing treatment and rehabilitation outcomes, surpassing the subjectivity of conventional scales although it has to be noted that accuracy is limited and better suited to detect activities rather than exact ROM.43 However, these findings are largely based on surrogate endpoints such as activity levels and range of motion, and do not necessarily reflect improvements in patient-reported outcomes or long-term recovery. This objective motion data complements, the insights gained from conventional patient-reported outcome measures (PROMs), which remain the standard for assessing a patient’s subjective experience of pain and function. Wearables will become instrumental in monitoring compliance with rehabilitation protocols, as mobile applications and online portals empower therapists to remotely track patient progress and enhance adherence.43 The detection of deviations from prescribed exercise routines is augmented by AI and machine learning models that provide real-time feedback and movement analysis, leading to customized treatment plans.31 This capability also facilitates real-time feedback and adjustments by clinicians, allowing them to provide remote guidance to patients and modify exercise programs based on performance.50
Demonstrated efficacy in postoperative shoulder arthroplasty rehabilitation is particularly promising.6 A randomized controlled trial by Marley et al31 showed that gamified exergame therapist-supported therapeutic exercises delivered via motion-tracking games that provide real-time feedback, scoring, and progressive challenges, yielded comparable improvements in active ROM and patient-reported outcomes (Oxford Shoulder Score, DASH-Score) to standard physiotherapy following arthroscopic shoulder surgery. This indicates that a progressive schedule of exergames, prescribed and remotely monitored by a physiotherapist, serves as an effective rehabilitation program. Wearable devices provide insights into postoperative fatigue, pain, and overall recovery by monitoring sleep patterns after rotator cuff repair or total shoulder arthroplasty, with sleep metrics correlating with patient-reported outcomes.46 Despite these benefits, significant challenges remain. Wearable technologies enable objective tracking of motion, activity levels, and rehabilitation adherence. However, these metrics primarily reflect surrogate markers of recovery, and robust evidence linking real-world monitoring data to superior patient-reported outcomes or long-term functional improvement in shoulder arthroplasty is currently lacking. Other key challenges include data privacy concerns, the “digital divide” limiting access for some patients, and a documented tendency for patient compliance to decrease significantly over time.
Smart Implants and Sensor-Enabled Monitoring
Similar, analogous to existing tendencies in knee and hip surgery, smart implants are also gaining importance in shoulder arthroplasty, giving information about instabilities, infections and maybe already intraoperatively, pressure/tension related strength vectors leading to later acromion insufficiency fractures.51
Smart implants with embedded sensors, coupled with advanced intraoperative technologies, are shaping orthopaedic surgery, enabling greater precision, personalization, and improved patient outcomes. These innovations are designed to provide objective, real-time data that augments traditional clinical assessments and surgical techniques.
Smart implants represent a significant leap forward, incorporating embedded sensors directly within prosthetic components to offer both therapeutic and diagnostic capabilities.30 These systems are capable of real-time measurement of crucial parameters such as joint loading, alignment, temperature, range of motion (ROM), pressure, strain, and proximity, with data often transmitted wirelessly to external systems.30 This constant flow of objective, quantitative data provides insights unattainable through other means, enabling physicians to proactively manage treatment, detect complications early, and refine recovery pathways.43
In the area of shoulder arthroplasty, developmental prototypes and early-stage commercial solutions are emerging with the potential to identify complications such as implant loosening, overloading, and mechanical failure even before clinical symptoms manifest.43 For instance, the application of strain gauges for in vivo measurement of shoulder forces during shoulder arthroplasty exemplifies this diagnostic capability. While not all sensor technologies are directly transferable to shoulder arthroplasty, broader orthopaedic applications demonstrate the potential of real-time implant monitoring. Similar advancements extend to hip arthroplasty, where sensors measure joint contact forces and temperature, and inductive proximity sensors detect early implant loosening with high sensitivity.34 In knee arthroplasty, multiaxial force-sensing implants with strain gauges have elucidated peak forces during daily activities, leading to refinements in implant design and postoperative rehabilitation strategies52 Commercial systems like OrthoSensor (ERA-SENSETM) provide real-time intraoperative tibiofemoral force distribution and soft tissue balance data, thereby improving surgical precision and potentially reducing complications. Furthermore, spinal fusion monitoring benefits from implantable sensors that assess fusion progression and measure in vivo loads on vertebral body replacements and internal fixators.52 Temperature-sensing implants are also being explored for early detection of peri-implant infections across various orthopaedic applications. Bergmann et al provided historical proof of concept for in vivo load sensing but are limited by small samples, outdated implant designs, and exclusive use of hemiarthroplasty implants. These studies showed that glenohumeral contact forces can exceed body weight, particularly during lifting and pushing activities, with peak forces reported between 70–170% of body weight.53,54 These data therefore demonstrate feasibility rather than directly supporting current smart implant applications, which require modern validation. Sensor-enabled implants offer the potential for real-time monitoring of implant loading and alignment, yet the clinical relevance of these measurements remains investigational. At present, many digital and smart health innovations in shoulder arthroplasty primarily improve how data are collected, monitored, and analyzed, rather than directly demonstrating improvements in clinical outcomes.
Emerging Evidence and Future Directions
Despite these promising developments, challenges persist. The integration of current sensor technology often necessitates significant modifications to existing implant designs, which can be technically complex, costly, and potentially compromise implant performance. Other limitations include power requirements for wireless sensors, biocompatibility issues, limited data storage capacity in very small implants, and the crucial need for robust data security and privacy measures. The body’s immune response to implanted devices, treating them as foreign bodies, also remains a concern. While groundbreaking, the research was limited by small sample sizes, the use of older implant designs, and measurements taken only in hemiarthroplasty cases, not total shoulder replacements. Additionally, these studies were performed before the introduction of the Medical Device Regulation (MDR), making the data less representative of modern implants. Despite these limitations, these datasets remain the only available in vivo measurements to date and are still referenced by companies such as Orthosensor. Overall, smart implants represent a promising frontier in medical device technology, with potential to improve disease monitoring, reduce invasive follow‐ups, and offer more responsive, personalized care.55
Telemedicine platforms, leveraging data from implants and wearables allow virtual follow-up visits, and integrated remote monitoring systems provide real-time tracking to support timely intervention. Remote rehab programs have shown non-inferiority to in-person care in shoulder surgery populations,56 and systems like ViViRA (Vivira Health Lab GmbH, Berlin, Germany) and Force Therapeutics (Force Therapeutics LLC, New York, NY, USA) have been piloted in shoulder arthroplasty pathways to deliver home-based physical therapy with clinician oversight.57 A recent meta-analysis of 10 randomized trials (n = 497) evaluated telemedicine for rotator cuff–related shoulder disorders; none of the trials involved shoulder arthroplasty. The study found that telemedicine was associated with greater improvements in shoulder function, increased range of motion, and reduced pain compared to conventional in-person care, both immediately after treatment and at follow-up. These findings suggest that telemedicine can be an effective alternative or complement to traditional rehabilitation for rotator cuff conditions, though larger, standardized studies with longer follow-up are needed to confirm long-term benefits.56
Looking ahead, AI has the potential to transform shoulder care by supporting personalized treatment decisions, enhancing surgical precision through integration with robotic systems, and streamlining workflows with predictive analytics. However, challenges remain around data privacy, algorithm bias, validation, and clinical integration. The authors stress the need for rigorous testing and standardization to ensure AI delivers safe, reliable, and equitable improvements in patient care.
Emerging digital health apps bolster this predictive capacity. Akina Cloud (Akina Ltd, Zurich, Switzerland) supports home rehabilitation after shoulder arthroplasty by providing structured exercise programs, real-time feedback via AI motion analysis, and remote therapist oversight to monitor adherence and biomechanics.48 In Korea, groups have applied deep-learning models to intra-operative arthroscopic images and to pre-operative clinical/imaging data to estimate re-tear risk and functional recovery; in one study, a DenseNet model reached ~91% test accuracy (specificity 0.93, sensitivity 0.84).58
Challenges, Costs, and Implementation Barriers
Despite these advances, major implementation gaps remain: heterogeneous sensor hardware and algorithms limit cross-study comparability, data quality and validity in pathological shoulder kinematics require further validation, explanations of ML (“black box” issues) and transparency remain limited, integration into existing clinical workflows and EHRs is nascent, regulatory and data-privacy hurdles are unresolved, and large pragmatic trials demonstrating clinical- and cost-effectiveness in shoulder arthroplasty populations are still scarce. Collectively, remote monitoring systems enriched by AI and outcome prediction models hold substantial promise for shoulder arthroplasty care from preoperative planning, through postoperative rehabilitation to long-term follow-up but realizing this potential will require rigorous external validations, better reporting standards, and alignment with clinical practice.
Conclusion
Collectively, while digital and smart technologies in shoulder arthroplasty demonstrate considerable potential, the current evidence base remains heterogeneous and is largely composed of feasibility studies, technical reports, and small clinical series. High-level evidence demonstrating improvements in patient-centered outcomes, complication rates, or long-term implant survivorship is still limited. As such, the clinical impact of many of these innovations remains to be clearly established. Advances in digital health, smart devices, and intraoperative technologies are poised to reshape the landscape of shoulder arthroplasty care. Mobile health apps and telemedicine platforms have already demonstrated the ability to support education, remote rehabilitation, and patient-reported outcome collection, with strong evidence of effectiveness in hip and knee arthroplasty and emerging pilot studies in shoulder surgery. Wearables and remote monitoring systems provide objective, real-world data on patient activity and recovery, while smart implants offer the potential for continuous, in vivo monitoring of implant performance and early detection of complications. Intraoperative innovations such as robotics, augmented reality, and AI-driven decision support promise to enhance surgical precision and optimize implant longevity. Together, these technologies represent a shift toward personalized, data-driven, and proactive care, but widespread implementation will require rigorous clinical validation, strategies to ensure equity and patient engagement, and seamless integration into healthcare systems to truly realize their transformative potential. An important limitation of the current evidence includes the relative scarcity of shoulder-specific data evaluating digital and smart health technologies across the perioperative pathway. Much of the strongest evidence supporting mHealth platforms, tele-rehabilitation, wearable monitoring, and intraoperative assistive technologies comes from hip and knee arthroplasty, where digital workflows have been implemented and studied at larger scale. This gap underscores the need for prospective, shoulder-focused validation to determine true clinical effectiveness, cost-efficiency, and integration feasibility before widespread adoption.
Nonetheless, emerging technologies, mobile health apps, wearable sensors, remote monitoring, prediction models, and sensor-enabled smart implants are transforming postoperative and intraoperative management in shoulder arthroplasty. The addition of AI-driven prediction tools (eg the ML models reviewed by Schneller et al,33 and app-based systems such as Akina Cloud,48 and ANAPPA,58 suggest a future in which treatment is more personalized, outcome forecasts are more accurate, and patients are more engaged in their recovery. However, achieving this future depends on overcoming challenges of external validation, data standardization, and regulatory oversight, as well as integration into clinical workflows and EHRs. Overall, the integration of digital and smart technologies represents a shift toward more data-driven and personalized care. However, current advances primarily enhance measurement, monitoring, and technical precision rather than directly improving clinical outcomes. Future research should prioritize high-quality, prospective studies with standardized outcome measures to determine whether these technologies translate into meaningful clinical benefit and cost-effectiveness in shoulder arthroplasty.
Abbreviations
AI, artificial intelligence; AR/MR, augmented/mixed reality; CT, computed tomography; EIS, electrical impedance spectroscopy; HUDs, head-mounted displays; IMUs, Inertial Measurement Units; MDR, Medical Device Regulation; mHealth, mobile health; M-IMUs, magneto-Inertial Measurement Units; ML, machine learning; PROMs, patient-reported outcome measures; PSI, Patient-specific implants; ROM, range of motion; TSA, total shoulder arthroplasty.
Acknowledgments
Investigation performed by the New Technology Committee of the German, Austrian, and Swiss Society for Shoulder and Elbow Surgery (DVSE).
Collaborators
The following people are part of the DVSE New Technologies Committee:
Asimina Lazaridou
Moritz Kraus
Felix Conrad Oettl
Jan-Philipp Imiolczyk
David A. Back
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Prof. Dr. David Back reports personal fees from Medacta International, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Berger GK, Garrigues GE, Chalmers PN, Singh A. Shoulder arthroplasty: current evidence and techniques on infection diagnosis and treatment. J Am Acad Orthop Surg. 2025;33(14):e765–13. PubMed PMID: 40344654. doi:10.5435/JAAOS-D-24-00720
2. Baird H, Kodali P, Gallegos M, et al. Artificial intelligence-driven analysis identifies arthroscopic shoulder surgery, meniscus injury and treatment, and total knee arthroplasty design biomechanics as the most commonly published topics in Knee Surgery, Sports Traumatology, Arthroscopy. J Exp Orthop. 2025;12(3):e70341. PubMed PMID: 40655248; PMCID: PMC12255955. doi:10.1002/jeo2.70341
3. Cigolotti A, Biz C, Lerjefors E, de Iudicibus G, Belluzzi E, Ruggieri P. Medium- to long-term clinical and functional outcomes of isolated and combined subscapularis tears repaired arthroscopically. Arch Med Sci. 2021;17(5):1351–1364. PubMed PMID: 34522265; PMCID: PMC8425253. doi:10.5114/aoms.2020.97714
4. Fama G, Tagliapietra J, Belluzzi E, Pozzuoli A, Biz C, Ruggieri P. Mid-term outcomes after arthroscopic “Tear Completion Repair” of partial thickness rotator cuff tears. Medicina. 2021;57(1):74. PubMed PMID: 33477332; PMCID: PMC7829759. doi:10.3390/medicina57010074
5. Crutsen JRW, Heerspink FOL, Kornuijt A, et al. Optimizing recovery after reverse shoulder arthroplasty with a personalised mobile health application compared to generic digital information: a protocol of a multicentre randomised controlled trial. BMC Musculoskelet Disord. 2025;26(1):642. PubMed PMID: 40616068; PMCID: PMC12231299. doi:10.1186/s12891-025-08857-9
6. Kim HG, Kim SC, Park JH, Kim JS, Kim DY, Yoo JC. Artificial intelligence in shoulder arthroplasty: how smart is it? JSES Int. 2025;9(3):988–993. PubMed PMID: 40486793; PMCID: PMC12144956. doi:10.1016/j.jseint.2024.07.002
7. Can Kolac U, Paksoy A, Akgun D. Three-dimensional planning, navigation, patient-specific instrumentation and mixed reality in shoulder arthroplasty: a digital orthopedic renaissance. EFORT Open Rev. 2024;9(6):517–527. PubMed PMID: 38828974; PMCID: PMC11195342. doi:10.1530/EOR-23-0200
8. Yam MGJ, Chao JYY, Leong C, Tan CH. 3D printed patient specific customised surgical jig for reverse shoulder arthroplasty, a cost effective and accurate solution. J Clin Orthop Trauma. 2021;21:101503. PubMed PMID: 34414069; PMCID: PMC8361309. doi:10.1016/j.jcot.2021.101503
9. Iannotti J, Baker J, Rodriguez E, et al. Three-dimensional preoperative planning software and a novel information transfer technology improve glenoid component positioning. J Bone Joint Surg Am. 2014;96(9):e71. PubMed PMID: 24806017. doi:10.2106/JBJS.L.01346
10. Iannotti JP, Weiner S, Rodriguez E, et al. Three-dimensional imaging and templating improve glenoid implant positioning. J Bone Joint Surg Am. 2015;97(8):651–658. PubMed PMID: 25878309. doi:10.2106/JBJS.N.00493
11. Schoch BS, Haupt E, Leonor T, Farmer KW, Wright TW, King JJ. Computer navigation leads to more accurate glenoid targeting during total shoulder arthroplasty compared with 3-dimensional preoperative planning alone. J Shoulder Elbow Surg. 2020;29(11):2257–2263. PubMed PMID: 32586595. doi:10.1016/j.jse.2020.03.014
12. Throckmorton TW, Gulotta LV, Bonnarens FO, et al. Patient-specific targeting guides compared with traditional instrumentation for glenoid component placement in shoulder arthroplasty: a multi-surgeon study in 70 arthritic cadaver specimens. J Shoulder Elbow Surg. 2015;24(6):965–971. PubMed PMID: 25535020. doi:10.1016/j.jse.2014.10.013
13. Scalise JJ, Codsi MJ, Bryan J, Brems JJ, Iannotti JP. The influence of three-dimensional computed tomography images of the shoulder in preoperative planning for total shoulder arthroplasty. J Bone Joint Surg Am. 2008;90(11):2438–2445. PubMed PMID: 18978413. doi:10.2106/JBJS.G.01341
14. Levin JM, Lorentz SG, Hurley ET, et al. Artificial intelligence in shoulder and elbow surgery: overview of current and future applications. J Shoulder Elbow Surg. 2024;33(7):1633–1641. PubMed PMID: 38430978. doi:10.1016/j.jse.2024.01.033
15. Dean MC, Oeding JF, Diniz P, Seil R, Samuelsson K; ESSKA Artificial Intelligence Working Group. Leveraging digital twins for improved orthopaedic evaluation and treatment. J Exp Orthop. 2024;11(4):e70084. PubMed PMID: 39530111; PMCID: PMC11551062. doi:10.1002/jeo2.70084
16. de Marinis R, Marigi EM, Atwan Y, et al. Current clinical applications of artificial intelligence in shoulder surgery: what the busy shoulder surgeon needs to know and what’s coming next. JSES Rev Rep Tech. 2023;3(4):447–453. PubMed PMID: 37928999; PMCID: PMC10625013. doi:10.1016/j.xrrt.2023.07.008
17. Vasey B, Lippert KAN, Khan DZ, et al. Intraoperative applications of artificial intelligence in robotic surgery: a scoping review of current development stages and levels of autonomy. Ann Surg. 2023;278(6):896–903. PubMed PMID: 36177855; PMCID: PMC10631501. doi:10.1097/SLA.0000000000005700
18. Troiano E, Masini A, Colasanti GB, Drago C, Giannotti S, Mondanelli N. 3D CT-based preoperative planning and intraoperative navigation in reverse shoulder arthroplasty: early clinical outcomes. Medicina. 2025;61(4):749. PubMed PMID: 40283040; PMCID: PMC12028824. doi:10.3390/medicina61040749
19. Wesorick BR, Lo EY, Gupta A, Garofalo R, Gall K, Krishnan SG. Current concepts in patient specific implants for reverse shoulder arthroplasty. JSES Int. 2025;9(3):771–778. PubMed PMID: 40486809; PMCID: PMC12145020. doi:10.1016/j.jseint.2024.12.007
20. Dey Hazra RO, Paksoy A, Imiolczyk JP, Gebauer H, Hayta A, Akgun D. Augmented reality-assisted intraoperative navigation increases precision of glenoid inclination in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2025;34(2):577–583. PubMed PMID: 39032685. doi:10.1016/j.jse.2024.05.039
21. Boufadel P, Lopez R, Fares MY, et al. Intraoperative navigation in reverse shoulder arthroplasty: advantages and future prospects. Clin Orthop Surg. 2024;16(5):679–687. PubMed PMID: 39364113; PMCID: PMC11444950. doi:10.4055/cios23407
22. Rojas JT, Menzemer J, Rashid MS, Hayoz A, Ladermann A, Zumstein MA. Navigated augmented reality through a head-mounted display leads to low deviation between planned, intra- and postoperative parameters during glenoid component placement of reverse shoulder arthroplasty: a proof-of-concept case series. J Shoulder Elbow Surg. 2025;34(2):567–576. PubMed PMID: 38942222. doi:10.1016/j.jse.2024.05.006
23. Kopriva JM, McKissack HM, Griswold BG, et al. Mixed-reality improves execution of templated glenoid component positioning in shoulder arthroplasty: a CT imaging analysis. J Shoulder Elbow Surg. 2024;33(8):1789–1798. PubMed PMID: 38320671. doi:10.1016/j.jse.2023.12.019
24. Athwal GS, Nelson A, Antuna S, et al. Glenoid preparation in reverse shoulder arthroplasty: robotic arm-assisted preparation compared to manual preparation and patient-specific guides. J Shoulder Elbow Surg. 2025;34(8):2022–2030. PubMed PMID: 39863156. doi:10.1016/j.jse.2024.12.007
25. Twomey-Kozak J, Hurley E, Levin J, Anakwenze O, Klifto C. Technological innovations in shoulder replacement: current concepts and the future of robotics in total shoulder arthroplasty. J Shoulder Elbow Surg. 2023;32(10):2161–2171. PubMed PMID: 37263482. doi:10.1016/j.jse.2023.04.022
26. Sanchez-Sotelo J. Robot-assisted shoulder arthroplasty. JSES Int. 2025;9(3):974–980. PubMed PMID: 40486788; PMCID: PMC12145009. doi:10.1016/j.jseint.2025.02.004
27. Wang C, Li Y, Chen J, et al. Mako surgical robot could improve the traditional surgical techniques of joint surgery fellows. BMC Med Educ. 2025;25(1):1179. PubMed PMID: 40830952; PMCID: PMC12363048. doi:10.1186/s12909-025-07606-9
28. Reid JJ, Kunkle BF, Greene AT, Eichinger JK, Friedman RJ. Variability and reliability of 2-dimensional vs. 3-dimensional glenoid version measurements with 3-dimensional preoperative planning software. J Shoulder Elbow Surg. 2022;31(2):302–309. PubMed PMID: 34411724. doi:10.1016/j.jse.2021.07.011
29. Lee D, Yoo J, Yoon JP, Oh KS, Chung SW. Comparison of patient-specific instrumentation, navigation, and mixed reality technologies for accurate glenoid positioning in reverse total shoulder arthroplasty: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2025;35:849–863. PubMed PMID: 40902713. doi:10.1016/j.jse.2025.07.019
30. Wang J, Chu J, Song J, Li Z. The application of impantable sensors in the musculoskeletal system: a review. Front Bioeng Biotechnol. 2024;12:1270237. PubMed PMID: 38328442; PMCID: PMC10847584. doi:10.3389/fbioe.2024.1270237
31. Marley WD, Barratt A, Pigott T, Granat M, Wilson JD, Roy B. A multicenter randomized controlled trial comparing gamification with remote monitoring against standard rehabilitation for patients after arthroscopic shoulder surgery. J Shoulder Elbow Surg. 2022;31(1):8–16. PubMed PMID: 34587534. doi:10.1016/j.jse.2021.08.019
32. Kelly CJ, Karthikesalingam A, Suleyman M, Corrado G, King D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019;17(1):195. PubMed PMID: 31665002; PMCID: PMC6821018. doi:10.1186/s12916-019-1426-2
33. Schneller T, Kraus M, Schatz J, Moroder P, Scheibel M, Lazaridou A. Machine learning in shoulder arthroplasty: a systematic review of predictive analytics applications. Bone Jt Open. 2025;6(2):126–134. PubMed PMID: 39900101; PMCID: PMC11790313. doi:10.1302/2633-1462.62.BJO-2024-0234.R1
34. Gaobotse G, Mbunge E, Batani J, Muchemwa B. Non-invasive smart implants in healthcare: redefining healthcare services delivery through sensors and emerging digital health technologies. Sensors Int. 2022;3:100156. doi:10.1016/j.sintl.2022.100156
35. Patel B, Thind A. Usability of mobile health apps for postoperative care: systematic review. JMIR Perioper Med. 2020;3(2):e19099. PubMed PMID: 33393925; PMCID: PMC7709840. doi:10.2196/19099
36. Janela D, Costa F, Molinos M, et al. Asynchronous and tailored digital rehabilitation of chronic shoulder pain: a prospective longitudinal cohort study. J Pain Res. 2022;15:53–66. PubMed PMID: 35035234; PMCID: PMC8755939. doi:10.2147/JPR.S343308
37. Kooner P, Baskaran S, Gibbs V, Wein S, Dimentberg R, Albers A. Commercially available activity monitors such as the fitbit charge and apple watch show poor validity in patients with gait aids after total knee arthroplasty. J Orthop Surg Res. 2024;19(1):404. PubMed PMID: 39004751; PMCID: PMC11247726. doi:10.1186/s13018-024-04892-9
38. Constantinescu D, Pavlis W, Rizzo M, Vanden Berge D, Barnhill S, Hernandez VH. The role of commercially available smartphone apps and wearable devices in monitoring patients after total knee arthroplasty: a systematic review. EFORT Open Rev. 2022;7(7):481–490. PubMed PMID: 35900191; PMCID: PMC9297050. doi:10.1530/EOR-21-0115
39. Wu KA, Kugelman DN, Goel RK, et al. Wearable health technology finds improvements in daily physical activity levels following total knee arthroplasty: a prospective study. Knee Surg Sports Traumatol Arthrosc. 2025;33(9):3218–3227. PubMed PMID: 40221914. doi:10.1002/ksa.12675
40. Gordon AM, Nian P, Baidya J, Scuderi GR, Mont MA. Randomized controlled studies on smartphone applications and wearable devices for postoperative rehabilitation after total knee arthroplasty: a systematic review. J Arthroplasty. 2025;40(8):2204–13e1. PubMed PMID: 39880056. doi:10.1016/j.arth.2025.01.034
41. Blasco JM, Navarro-Bosch M, Aroca-Navarro JE, Hernandez-Guillen D, Puigcerver-Aranda P, Roig-Casasus S. A virtual assistant to guide early postoperative rehabilitation after reverse shoulder arthroplasty: a pilot randomized trial. Bioengineering. 2024;11(2):152. PubMed PMID: 38391638; PMCID: PMC10885890. doi:10.3390/bioengineering11020152
42. Steiner B, Elgert L, Saalfeld B, Wolf KH. Gamification in Rehabilitation of Patients With Musculoskeletal Diseases of the Shoulder: scoping Review. JMIR Serious Games. 2020;8(3):e19914. PubMed PMID: 32840488; PMCID: PMC7479582. doi:10.2196/19914
43. Chen YP, Lin CY, Tsai MJ, Chuang TY, Lee OK. Wearable motion sensor device to facilitate rehabilitation in patients with shoulder adhesive capsulitis: pilot study to assess feasibility. J Med Internet Res. 2020;22(7):e17032. PubMed PMID: 32457026; PMCID: PMC7413285. doi:10.2196/17032
44. Dimo A, Longo UG, D’Hooghe P, et al. 3D-printed wearable sensors for the identification of shoulder movement planes. Sensors. 2025;25(18):5853. PubMed PMID: 41013090; PMCID: PMC12473567. doi:10.3390/s25185853
45. Porciuncula F, Roto AV, Kumar D, et al. Wearable movement sensors for rehabilitation: a focused review of technological and clinical advances. PM R. 2018;10(9 Suppl 2):S220–S32. PubMed PMID: 30269807; PMCID: PMC6700726. doi:10.1016/j.pmrj.2018.06.013
46. Gadangi PV, Lambert BS, Goble H, Harris JD, McCulloch PC. Validated wearable device shows acute postoperative changes in sleep patterns consistent with patient-reported outcomes and progressive decreases in device compliance after shoulder surgery. Arthrosc Sports Med Rehabil. 2023;5(5):100783. PubMed PMID: 37636255; PMCID: PMC10450855. doi:10.1016/j.asmr.2023.100783
47. De Baets L, van der Straaten R, Matheve T, Timmermans A. Shoulder assessment according to the international classification of functioning by means of inertial sensor technologies: a systematic review. Gait Posture. 2017;57:278–294. PubMed PMID: 28683420. doi:10.1016/j.gaitpost.2017.06.025
48. Sassi M, Villa Corta M, Pisani MG, et al. Advanced home-based shoulder rehabilitation: a systematic review of remote monitoring devices and their therapeutic efficacy. Sensors. 2024;24(9):2936. PubMed PMID: 38733040; PMCID: PMC11086333. doi:10.3390/s24092936
49. Antonacci C, Longo UG, Nazarian A, Schena E, Carnevale A. Monitoring scapular kinematics through wearable magneto-inertial measurement units: state of the art and new frontiers. Sensors. 2023;23(15):6940. PubMed PMID: 37571723; PMCID: PMC10422625. doi:10.3390/s23156940
50. Carnevale A, Longo UG, Schena E, et al. Wearable systems for shoulder kinematics assessment: a systematic review. BMC Musculoskelet Disord. 2019;20(1):546. PubMed PMID: 31731893; PMCID: PMC6858749. doi:10.1186/s12891-019-2930-4
51. Caubere A, Rutigliano S, Bourdon S, et al. The effect of humeral tray thickness on glenohumeral loads in a reverse shoulder ‘smart’ implant. Int Orthop. 2024;48(11):2881–2889. PubMed PMID: 39231836. doi:10.1007/s00264-024-06282-6
52. Soares Dos Santos MP, Bernardo RMC. Bioelectronic multifunctional bone implants: recent trends. Bioelectron Med. 2022;8(1):15. PubMed PMID: 36127721; PMCID: PMC9490885. doi:10.1186/s42234-022-00097-9
53. Bergmann G, Graichen F, Bender A, Kaab M, Rohlmann A, Westerhoff P. In vivo glenohumeral contact forces--measurements in the first patient 7 months postoperatively. J Biomech. 2007;40(10):2139–2149. PubMed PMID: 17169364. doi:10.1016/j.jbiomech.2006.10.037
54. Westerhoff P, Graichen F, Bender A, et al. In vivo measurement of shoulder joint loads during activities of daily living. J Biomech. 2009;42(12):1840–1849. PubMed PMID: 19643418. doi:10.1016/j.jbiomech.2009.05.035
55. Abyzova E, Dogadina E, Rodriguez RD, et al. Beyond Tissue replacement: the Emerging role of smart implants in healthcare. Mater Today Bio. 2023;22:100784. PubMed PMID: 37731959; PMCID: PMC10507164. doi:10.1016/j.mtbio.2023.100784
56. Zhang B, Fang Z, Nian K, Sun B, Ji B. The effects of telemedicine on Rotator cuff-related shoulder function and pain symptoms: a meta-analysis of randomized clinical trials. J Orthop Surg Res. 2024;19(1):478. PubMed PMID: 39143625; PMCID: PMC11323625. doi:10.1186/s13018-024-04986-4
57. Schick S, Elphingstone J, Paul K, et al. Home-based physical therapy results in similar outcomes to formal outpatient physical therapy after reverse total shoulder arthroplasty: a randomized controlled trial. J Shoulder Elbow Surg. 2023;32(8):1555–1561. PubMed PMID: 37178958. doi:10.1016/j.jse.2023.03.023
58. Cho SH, Kim YS. Prediction of retear after arthroscopic rotator cuff repair based on intraoperative arthroscopic images using deep learning. Am J Sports Med. 2023;51(11):2824–2830. PubMed PMID: 37565449. doi:10.1177/03635465231189201
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.