Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Differential expression of Wnt5a and β-Catenin in Keratoacanthoma, Verrucous Carcinoma and Well-Differentiated Squamous Cell Carcinoma
Authors Zhang Y, Bai X, Ning X, Ren J
Received 4 January 2026
Accepted for publication 6 March 2026
Published 16 March 2026 Volume 2026:19 586819
DOI https://doi.org/10.2147/CCID.S586819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Yanfei Zhang,1 Xuanjiang Bai,2 Xiaoying Ning,1 Jianwen Ren1
1Department of Dermatology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Clinical Medicine, Nanchang University Queen Mary School, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Yanfei Zhang, Department of Dermatology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, 710004, People’s Republic of China, Email [email protected]
Background: Verrucous carcinoma (VC) are always considered to be a variant of well-differentiated squamous cell carcinoma (SCC). If Keratoacanthoma (KA) is a variant of well-differentiated SCC, it is controversial currently. Both β-catenin and Wnt5a are key factors in the classical and non-classical Wnt signaling pathways, which are often used in the differential diagnosis of benign and malignant tumors. However, the expression of these two factors in these three diseases remains unclear. The goal of the current study was to explore the expression of β-catenin and Wnt5a in KA, VC, and well-differentiated SCC and to determine their value in differential diagnosis.
Methods: Twenty samples were collected from VC lesions, 30 from KA lesions, and 30 from cutaneous well-differentiated SCC lesions. The expression of Wnt5a and β-catenin in paraffin-embedded tissue sections was analyzed by immunohistochemistry. The histo (H) score was used to evaluate positive cases.
Results: There were no statistically significant differences in sex or age between KA, VC, and well-differentiated SCC patients (P-value> 0.05). Immunohistochemical analysis showed that β-catenin was expressed in all tissues. For Wnt5a and β-catenin staining intensity, H score and H-score category, there were significant differences between the well-differentiated SCC and KA groups, as well as VC and KA groups (P-value< 0.01 for all). However, there were no differences between the well-differentiated SCC and VC groups (P-value> 0.05).
Conclusion: In this study, the differential expression of Wnt5a and β-catenin suggests that the benign tumor KA and well-differentiated SCC may be two distinct entities. We identified that Wnt5a and β-catenin could be used as adjuvant immunohistochemical markers for the differential diagnosis of KA from well-differentiated SCC.
Keywords: Wnt5a, β-catenin, keratoacanthoma, verrucous carcinoma, well-differentiated squamous cell carcinoma
Introduction
Keratoacanthoma (KA) is an unusual and often controversial skin disease.1 Some scholars believe that KA is a self-resolving benign lesion characterized by rapid growth within a few weeks, followed by spontaneous regression in the next few months. KA is considered by many researchers to be a benign behavioral variant of squamous cell carcinoma (SCC), a self-resolving tumor similar to well-differentiated SCC in histopathology.2,3 Although different hypotheses have been proposed to explain the mechanisms of KA tumor degeneration, we still lack a clear understanding of the signals and cellular mechanisms that drive its spontaneous degeneration.
Squamous cell carcinoma (SCC) is a common skin malignancy that can develop from actinic keratosis (AK). Distinguishing between keratoacanthoma and well-differentiated SCC remains a challenge in the diagnosis of skin pathology.
Verrucous carcinoma (VC) is a low-grade, slow-growing, well-differentiated tumor with very low metastatic potential. It is a rare variant of well-differentiated SCC.4 Usually due to high levels of UVB exposure, and mainly affects exposed areas, such as the face, neck, arms, and hands.5
Wnts is a large family of secretory glycoproteins rich in cysteine, which plays an important role in the development and physiological process of many tissues.6 As a key factor of classical and non classical Wnt pathway, β-catenin and Wnt5a regulates inflammatory response and various functions of tumor cells by activating cascade signaling pathways, including cell proliferation, differentiation, apoptosis, survival, and cell polarity. The expression of β-catenin and Wnt5a are often used for the differential diagnosis of benign and malignant tumors.7,8
If KA is a variation of well-differentiated SCC, if not, what is the difference between KA and well-differentiated SCC, and if so, are there some similarities between KA and VC (low-grade, slow-growing, well-differentiated SCC)? In this study, we investigated β-catenin and Wnt5a expression levels in KA, VC, and well-differentiated SCC. We expect to answer these questions to a certain extent.
Materials and Methods
Samples
This is a retrospective case study. Patients with KA, VC, and well-differentiated SCC confirmed by histopathology from January 2020 to December 2023 were selected as research subjects (clinical diagnosis was required to be consistent with histopathology. The histological diagnosis of KA and cutaneous SCC was met the criteria described by Richard Carr9). Inclusion criteria including: 1. The patient had no history of hypertension, diabetes, or other chronic diseases. 2. None of the recruited patients were administered any systemic drugs within 2 months or topical drugs in the previous 2 weeks. 3. No treatment was administered to the lesion. Exclusion criteria were as follows: 1. Patients who were not histopathologically confirmed or refused to participate in the study. 2. KA during the regression phase. 3. The patient had other tumors, such as lung and oral SCC. 4. Moderately and poorly differentiated SCC and secondary SCC such as SCC secondary to psoriatic plaque lesions. 5. Actinic keratosis and Bowen disease. 5. Other related inflammatory or immune-mediated conditions may affect the Wnt pathway (such as hypertension, diabetes, psoriasis, lichen planus, alopecia areata, or rheumatoid arthritis). Written informed consent was obtained from all participants. Biopsies were performed under local anesthesia. All experimental protocols were approved by the Institutional Review Board of Xi’an Jiaotong University (No:2019–1098) and performed according to the guidelines governing ethics care in China. This study was performed in accordance with the Declaration of Helsinki guidelines.
Immunohistochemical Analysis
Immunohistochemical analyses of all specimens derived from patient biopsies were formalin-fixed and paraffin embedded. Detection was performed using the avidin-biotin-peroxidase method. The negative control group was treated saline instead of primary antibody. The specimen sections were incubated with rabbit polyclonal to Wnt5a primary antibody (ab229200; final dilution 1:200) and rabbit polyclonal anti-β-catenin primary antibody (ab616051; final dilution 1:500) overnight at 4°C, followed by incubation with an appropriate biotinylated streptavidin-horseradish peroxidase-conjugated secondary antibody (ZSGB-BIO, Beijing, China), counterstaining with hematoxylin, and visualization with 3’-diaminobenzidine (ZSGB-BIO, Beijing, China). All histopathological and immunohistochemical analysis was performed by dermatopathologists.
Immunohistochemical Results Interpretation
Stained sections were examined using Nanozoomer digital pathology (Hamamatsu, Japan). For positive cases, the percentage of positive cells and intensity of staining (0, no staining; 1, weak; 2, moderate; and 3, strong staining) were recorded. The consistency among observers was always>95%. Each experiment was performed thrice in duplicate. All analyses were conducted independently by two investigators. The histo (H) score was used to evaluate the positive cases, and the intensity and percentage were calculated using the following formula: H score=3× (percentage of strong intensity) + 2× (percentage of moderate intensity) +1× (percentage of mild intensity). The scores ranged from 0 to 300 and were divided into two categories: low (< 150) and high (≥ 150).10
Statistical Analysis
All data were processed using SPSS20.0 statistical analysis software (SPSS Inc., Chicago, IL, USA). Results are presented as the mean± standard deviation (SD). The chi-square test, unpaired T test for two groups, and one-way ANOVA for multiple group comparisons were used to analyze differences. Spearman correlation coefficients were used for the correlation analysis. Statistical significance was set at P <0.05.
Results
The Characteristics of the Study Population
As shown in Table 1, patients with VC (13 males and 7 females; mean age: 61.35 ± 15.31 years; age range: 32–83 years) and well-differentiated SCC (19 males and 11 females; mean age: 63.22 ± 13.28 years; age range: 35–86 years) were more common in male. But KA cases (12 males and 18 females; mean age: 61.33 ± 12.41years; age range: 36–77 years) was more common in female. The head and neck are the most affected areas. The genital area is also involved in VC and well-differentiated SCC. The average disease duration was the shortest in patients with KA and the longest in patients with well-differentiated SCC. There were no significant differences in age or sex between patients with KA, VC, or well-differentiated SCC (P-value>0.05).
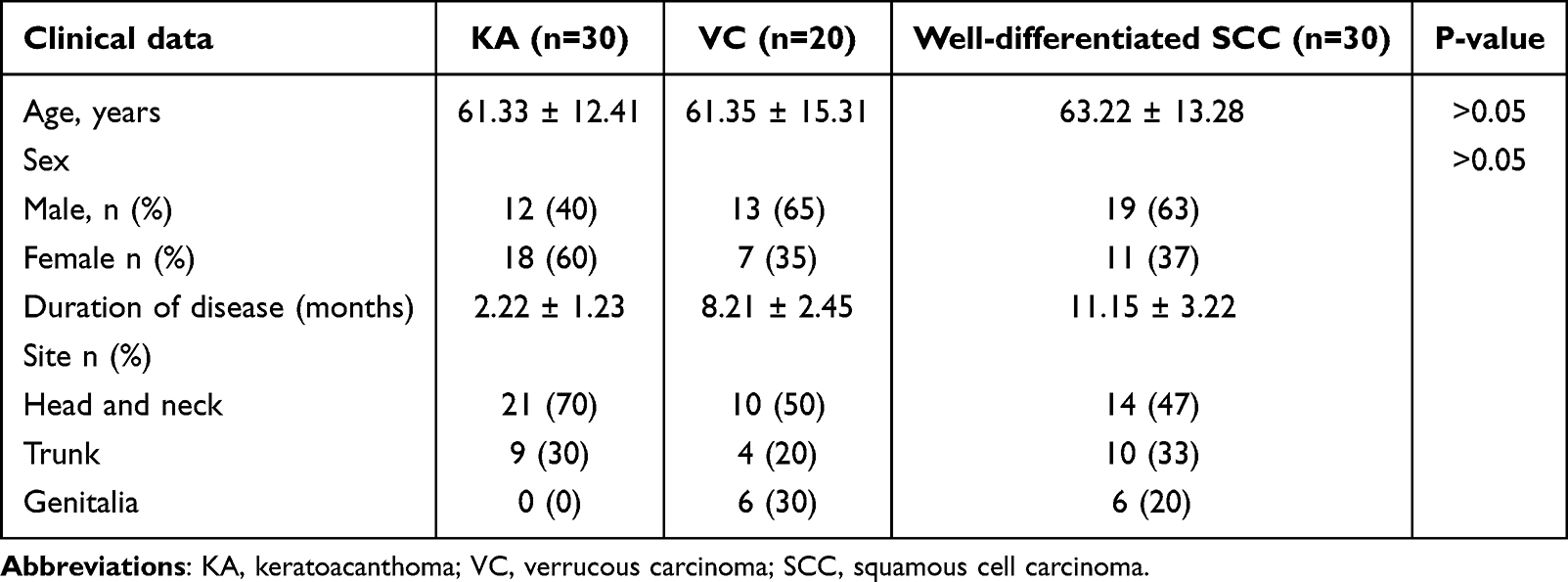 |
Table 1 The Characteristics of Study Population |
Immunohistochemical Expression of Wnt5a in Lesions of KA, VC and Well-Differentiated SCC
Immunohistochemical staining showed that Wnt5a was highly expressed in well-differentiated SCC and VC lesions (Figure 1a and b). As shown in Table 2, for SCC, mild staining intensity was observed in six cases (20%), moderate staining in 14 (47%), and strong staining in 10 (33%). The H score was 193.32 ± 28.77. The H-score category was high in 24 cases (80%) and low in 6 cases (20%). In VC cases, staining intensity was rated as mild in 3 cases (15%), moderate in 11 (55%) and strong in 6 (30%), The H score was 186.86 ± 23.03. The H-score category was high in 17 cases (85%) and low in 3 cases (15%). However, in KA, mild staining intensity was observed in 23 cases (77%), moderate staining in five (17%), and strong staining in two (6%). The positive cells were distributed only at the edge of the tumor (Figure 1c). The H score was 98.29 ± 19.73. The H-score category was high in seven cases (23%) and low in 23 cases (77%). For Wnt5a staining intensity, H score and H-score category, there were significant differences between the well-differentiated SCC and KA groups, as well as VC and KA groups (P-value<0.01 for all). However, there was no significant difference between the well-differentiated SCC and VC groups (P-value>0.05). (Table 2).
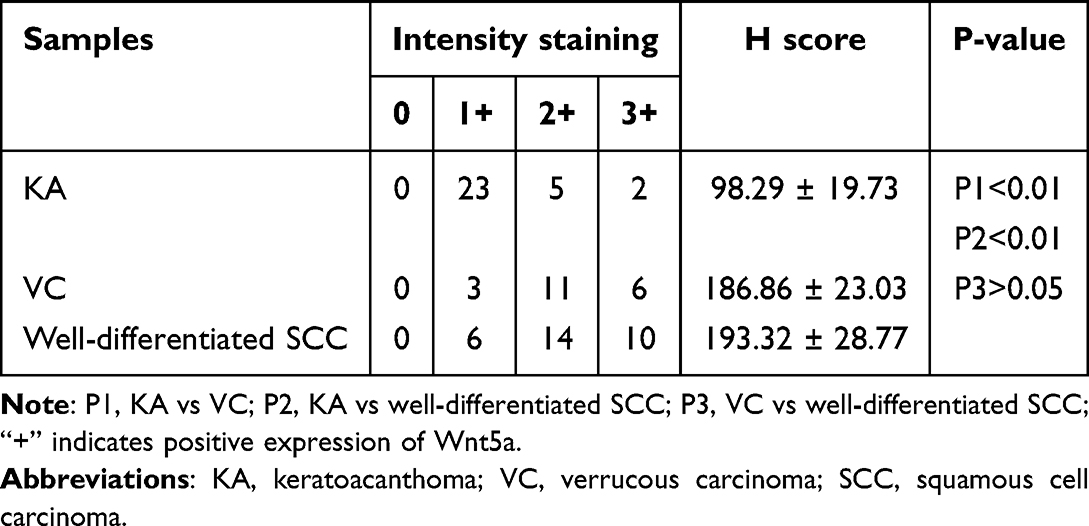 |
Table 2 The Expression of Wnt5a in KA, VC and Well-Differentiated SCC |
 |
Figure 1 Immunohistochemical of Wnt5a expression in well-differentiated SCC, VC and KA. (a) moderate to strong diffuse expression in well-differentiated SCC. (b) moderate to strong diffuse expression in VC. (c) only mild expression in the leading edge of KA tumor. Magnification (a–c) ×20. |
Immunohistochemical Expression of β-Catenin in Lesions of KA, VC and Well-Differentiated SCC
Accumulation of β-catenin in the nucleus or cytoplasm indicated active β-catenin signaling.6 As shown in Table 3 and Table 4, all tissues showed membrane expression of β-catenin. In well-differentiated SCC, 22/30 (73%) cases showed positive β-catenin expression (Figure 2a), mild intensity staining in 7 cases (32%), moderate in 7 (32%) and strong in 8 (36%). The H score was 156.95 ± 18.65, H-score category was high in 15 (68%) case and low in 7 cases (32%). There were 14/20 (70%) cases showing positive β-catenin expression in the VC (Figure 2b), mild staining intensity in 3 cases (21%), moderate staining in 5 cases (36%), and strong staining in 6 cases (43%). The H score was 153.14 ± 18.63, and the H-score category was high in 11 cases (79%) and low in 3 cases (21%). For KA, 7/30 (23%) cases showed positive β-catenin expression (Figure 2c), mild staining intensity in 5 cases (71%), moderate staining in 1 case (14.5%), and strong staining in 1 case (14.5%). The H score was 103.29 ± 30.43, H-score category was high in 2 cases (50%) and low in 5 cases (50%). For β-catenin staining intensity, H score, and H-score category, there were significant differences between the well-differentiated SCC and KA groups, as well as between the VC and KA groups (P-value<0.01 all). However, there were no differences between the well-differentiated SCC and VC groups (P-value>0.05). (Table 4).
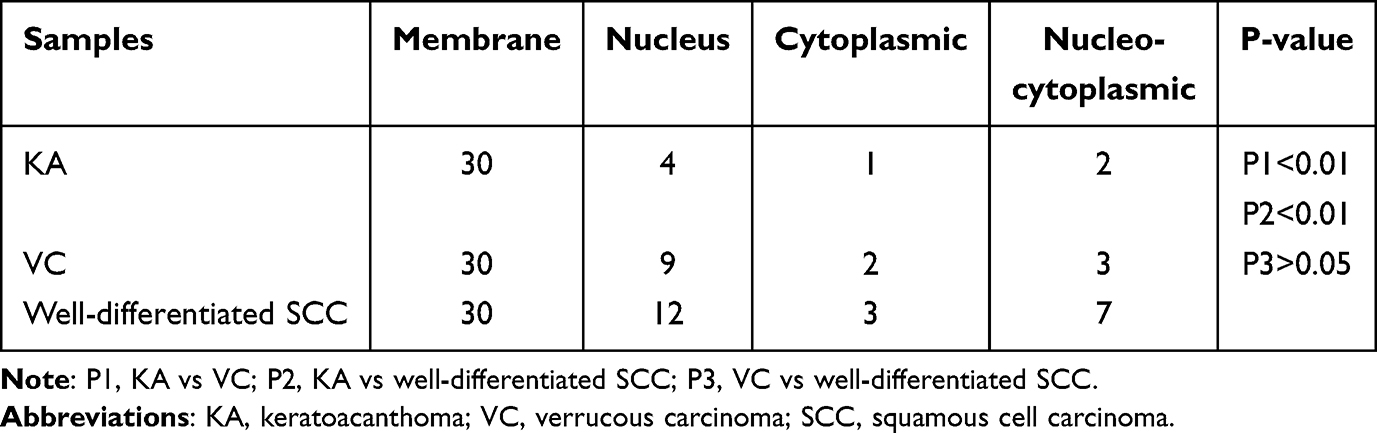 |
Table 3 The Pattern of β-Catenin Expression in KA, VC and Well-Differentiated SCC |
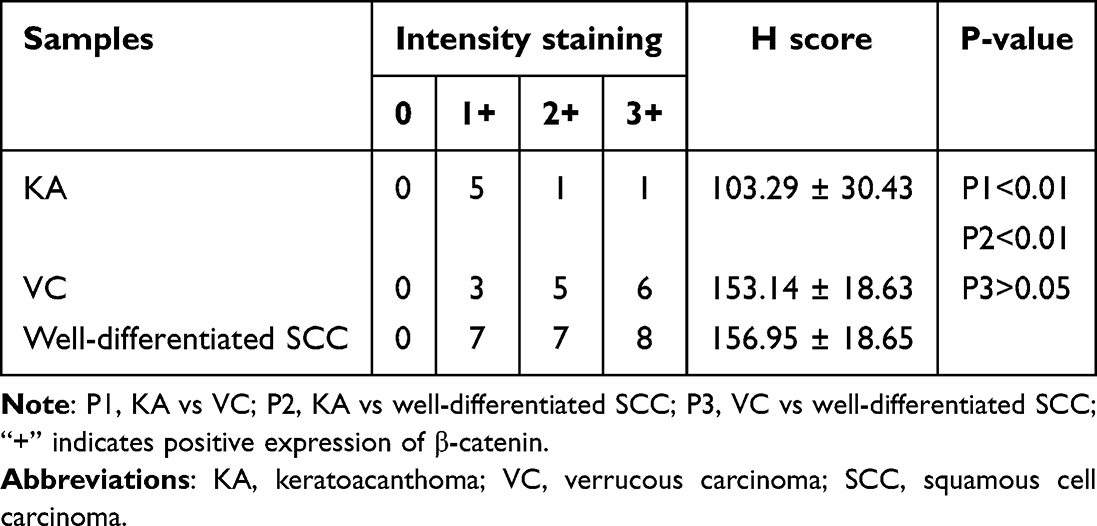 |
Table 4 The Expression of β-Catenin in KA, VC and Well-Differentiated SCC |
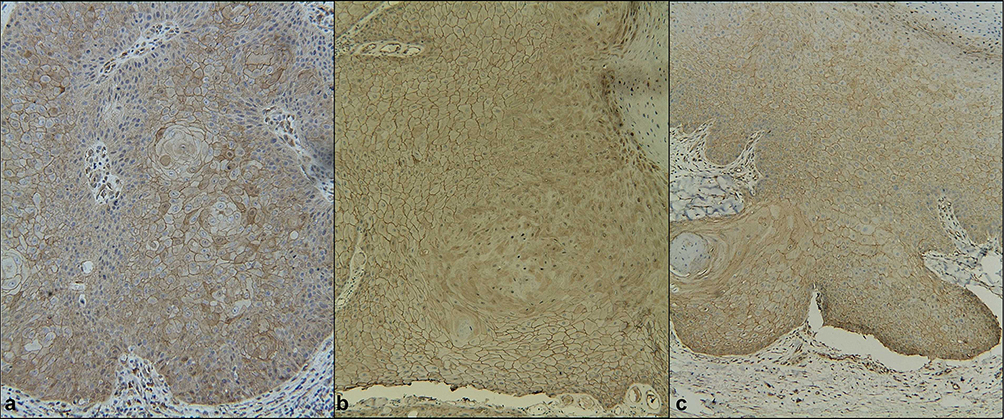 |
Figure 2 Immunohistochemical analysis of β-catenin expression in well-differentiated SCC, VC, and KA. (a) Moderate-to-strong cytoplasmic or nuclear expression in well-differentiated SCC. (b) Moderate to strong cytoplasmic or nuclear expression in VC. (c) Almost all membrane expressions in KA. Magnification: (a–c) ×40. |
Correlation Between the Expression Levels of Wnt5a and β-Catenin in KA, VC and Well-Differentiated SCC
Spearman correlation coefficient analysis showed no correlation between Wnt5a and β-catenin in KA (r=0.22, P-value>0.05) (Figure 3a). There were significant positive correlations between Wnt5a and β-catenin in the VC (r=0.85, P-value<0.01) and well-differentiated SCC (R = 0.75, P < 0.01) (Figure 3b and c).
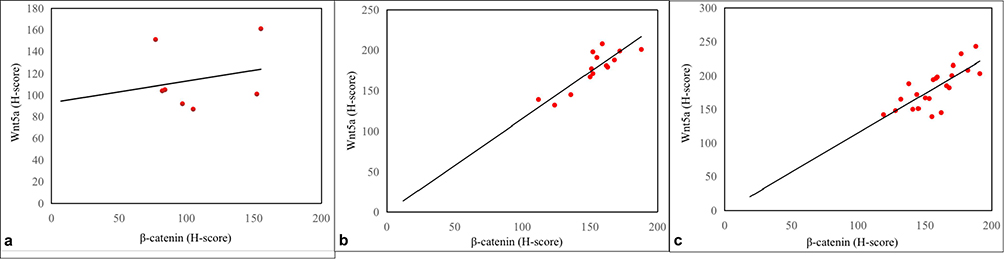 |
Figure 3 Correlation between Wnt5a and β-catenin expression in KA, VC, and well-differentiated SCC tissues (a) No correlation in KA. (b) Positive correlations in VC. (c) Positive correlation in well-differentiated SCC. |
Discussion
KA is a benign skin tumor. Some isolated KA resolve spontaneously, leaving a faint scar, while others require routine resection if KA with 4 mm margins. Aggressive large KA that are greater than 2 cm in cosmetically sensitive areas require tissue sparing and should consider Mohs micrographic surgery.11 It is difficult to distinguish KA from well-differentiated SCC clinically and histologically (particularly with perforated biopsy). However, it has been reported that they exhibit different gene expression profiles.12 But, study found KA typically characterized by a short clinical course and a predilection for sites other than the head and neck. Compared with cutaneous SCC (cSCC), KA generally lacks expression of p16, p53, and Ki-67, whereas cSCC frequently exhibits abnormalities in these markers. This research results are of great value in distinguishing between these two diseases.9 Researchers have shown the nuclear expression of β-catenin increases during the KA growth phase.13 On the contrary, in our and other studies, we found that the membrane staining of β-catenin was visible in all KA cells, but most KA did not show nuclear or cytoplasmic β-catenin staining.14
However, in VC and well-differentiated SCC, most tissues showed nuclear or cytoplasmic β-catenin staining. This is consistent with findings in oral SCC and cutaneous SCC.15,16 Partial or complete deletion of β-catenin membrane staining and an increase in β-catenin cytoplasmic and nuclear staining are associated with less differentiated and more aggressive clinical behavior in SCC.15
Here, we report that Wnt5a was upregulated in well-differentiated SCC and VC, but in KA, Wnt5a was only localized at the leading edge of the tumors in KA. Previously, Wnt5a have been reported to induce tumor invasion aggressive in oral SCC.17 And in vitro, Wnt5a can promote β-catenin cytoplasmic and nuclear transcription, further promote the proliferation of tumor cells.18 In addition, immunohistochemical analysis of SCC specimens of the tongue suggests that high expression of Wnt5a is associated with a poor prognosis.19
In our study, KA showed β-catenin membrane expression with little nuclear or cytoplasmic staining. Wnt5a is expressed only in cells at the tumor edge. This may explain its noninvasive and regressive characteristics. Low Wnt5a and β-catenin expression levels may reach a balanced state. The expression of Wnt5a is not sufficient to promote tumor proliferation, and the membrane expression of β-catenin can stabilize cell connections, which is not conducive to metastasis and the further deterioration of KA.
Several studies have shown that Wnt5a and β-catenin play important roles in cancer invasion. However, the role of Wnt5a and β-catenin in cancer remains controversial. Some reports have indicated that Wnt5a and β-catenin may play tumor suppressor roles. However, both can promote the occurrence and development of tumors. However, in our study, the expression of Wnt5a and β-catenin increased in well-differentiated SCC and VC. Correlation analysis showed that the expression of Wnt5a was positive correlated with β-catenin expression in VC and well-differentiated SCC. We believe that the upregulation of Wnt5a leads to β-catenin signal transduction, and that both Wnt5a and β-catenin synergistically promote tumor invasion and proliferation. Further studies are required to confirm this hypothesis.
In fact, upregulation of the Wnt/β-catenin signaling pathway is associated with carcinogenesis in various tissues, including colorectal cancer, gastric cancer, prostate cancer, and carcinoma of the skin.20,21 The Wnt/β-catenin signaling pathway influences the proliferation and apoptosis of tumor cells by regulating downstream target genes.22
Therefore, our study found that KA and well-differentiated SCC may be distinct entities: KA and VC. However, VC and well-differentiated SCC are different types of the same disease. Reliably distinguishing between cutaneous SCC and KA will shift the management strategy of KA to minimally invasive treatments, prevent unnecessary surgical complications, and potentially reduce associated healthcare costs. To date, no definitive KA deaths have been reported, although the death rate from cutaneous SCC is approximately 1.5%. There is some evidence that KA is a benign lesion that differs from cutaneous SCC.12,23,24
Interestingly, our study found no significant differences in age or sex between patients with KA, VC, or well-differentiated SCC, which differs from findings reported in other studies.9,25 This may be due to the small sample size and all patients from a single center, there may had a biases.
Our study has some limitations: 1. KA in the regression stage and SCC with poor differentiation were excluded from the study. 2. Other downstream factors of the Wnt pathway have not been identified. 3. We only performed immunohistochemical analysis and did not perform mRNA or Western blot analyses. 4. The sample size of this study was not sufficiently large. Further experiments will be conducted in the future.
Conclusion
In conclusion, the presented data provide some evidence to prove that KA and well-differentiated SCC may be two distinct entities, and a couple of markers may help in the differential diagnosis of KA and well-differentiated SCC on pathology.
Financial support: This study was supported by the National Natural Science Foundation of China (No. 81703129).
Disclosure
The authors declare no competing interests in this work.
References
1. Kwiek B, Schwartz RA. Keratoacanthoma (KA): an update and review. J Am Acad Dermatol. 2016;74(6):1220–8. doi:10.1016/j.jaad.2015.11.033
2. Nagarajan P. Differentiating keratoacanthoma from squamous cell carcinoma in quest of the holy grail. J Cutan Pathol. 2020;47(4):418–420. doi:10.1111/cup.13640
3. Mandrell JC, Santa CD. Keratoacanthoma: hyperplasia, benign neoplasm, or squamous cell carcinoma. Semin Diagn Pathol. 2009;26(3):150–156. doi:10.1053/j.semdp.2009.09.003
4. Fawaz B, Vieira C, Decker A, et al. Surgical treatment of verrucous carcinoma: a review. J DermatolTreat. 2022;33(4):1811–1815. doi:10.1080/09546634.2021.1914312
5. Akrish S, Eskander-Hashoul L, Rachmiel A, et al. Clinicopathological analysis of verrucous hyperplasia, verrucous carcinoma, and squamous cell carcinoma as part of the clinicopathologic spectrum of oral proliferative verrucous leukoplakia: a literature review and analysis. Pathol Res Pract. 2019;215(12):152670. doi:10.1016/j.prp.2019.152670
6. Steinhart Z, Angers S. Wnt signaling in development and tissue homeostasis. Development. 2018;145(11):dev146589. doi:10.1242/dev.146589
7. Zhan T, Rindtorff N, Boutros M. Wnt signaling in cancer. Oncogene. 2017;36(11):1461–1473. doi:10.1038/onc.2016.304
8. Lopez-Bergami P, Barbero G. The emerging role of Wnt5a in the promotion of pro-inflammatory and immunosuppressive tumor microenvironment. Cancer Metastasis Rev. 2020;39(3):933–952. doi:10.1007/s10555-020-09878
9. Carr RA, Mesiano D, Heffron C, et al. Aberrant p16, p53 and Ki-67 immunohistochemistry staining patterns can distinguish solitary keratoacanthoma from cutaneous squamous cell carcinoma. Pathology. 2023;55(6):772–784. doi:10.1016/j.pathol.2023.07.001
10. Bilalovic N, Sandstad B, Golouh R, et al. CD10 protein expression in malignant melanoma and stromal cells is associated with tumor progression. Mod Pathol. 2004;17(10):1251–1258. doi:10.1038/modpathol.3800174
11. Zito PM, Scharf R. Keratoacanthoma. In: StatPearls. StatPearls Publishing: Treasure Island (FL); 2025.
12. Ra SH, Su A, Li X, et al. Keratoacanthoma and squamous cell carcinoma are distinct from the molecular perspective. Mod Pathol. 2015;28(6):799–806. doi:10.1038/modpathol.2015.5
13. Zito G, Saotome I, Liu Z, et al. Spontaneous tumor regression in keratoacanthomas is driven by crosstalk between Wnt/retinoic acid signalling. Nat Commun. 2014;5(1):3543. doi:10.1038/ncomms4543
14. Joshi S, De Angelis PM, Zucknick M, et al. Role of the Wnt signaling pathway in keratoacanthoma. Cancer Rep. 2020;3(2):e1219. doi:10.1002/cnr2.1219
15. Laxmidevi LB, Angadi PV, Pillai RK, et al. Aberrant β-catenin expression during the histological differentiation of oral squamous cell carcinoma and verrucous carcinoma: an immunohistochemical study. J Oral Sci. 2010;52(4):633–640. doi:10.2334/josnusd.52.633
16. Lan YJ, Chen H, Chen JQ, et al. Immunolocalization of vimentin, keratin 17, Ki-67, involucrin, β-catenin, and E-cadherin in cutaneous squamous cell carcinoma. Pathol Oncol Res. 2014;20(2):263–266. doi:10.1007/s12253-013-9690-5
17. Prgomet Z, Axelsson L, Lindberg P, et al. Migration and invasion of oral squamous carcinoma cells is promoted by WNT 5A, a regulator of cancer progression. J Oral Pathol Med. 2015;44(10):776–784. doi:10.1111/jop.12292
18. Pramanik KK, Nagini S, Singh AK, et al. Glycogen synthase kinase-3beta mediated regulation of matrix metalloproteinase-9 and its involvement in oral squamous cell carcinoma progression and invasion. Cell Oncol. 2018;41(1):47–60. doi:10.1007/s13402-017-0358-0
19. Sakamoto T, Kawano S, Matsubara R, et al. Critical roles of Wnt5a-Ror2 signaling in the aggressiveness of tongue squamous cell carcinoma and production of matrix metalloproteinase-2 via deltaNp63beta-mediated epithelial- mesenchymal transition. Oral Oncol. 2017;69:15–25. doi:10.1016/j.oraloncology.2017.03.019
20. Parsons MJ, Tammela T, Dow LE. WNT as a driver and dependency in Cancer. Cancer Discov. 2021;11(10):2413–2429. doi:10.1158/2159-8290.CD-21-0190
21. Kervarrec T, Cheok Lei K, Sohier P, et al. Wnt/beta-catenin-activated nonpilomatrical carcinoma of the skin: a case series. Mod Pathol. 2024;37(11):100586. doi:10.1016/j.modpat.2024.100586
22. Song P, Gao Z, Bao Y, et al. Wnt/beta-catenin signaling pathway in carcinogenesis and cancer therapy. J Hematol Oncol. 2024;17(1):46. doi:10.1186/s13045-024-01563-4
23. Gleich T, Chiticariu E, Huber M, et al. Keratoacanthoma: a distinct entity. Exp Dermatol. 2016;25(2):85–91. doi:10.1111/exd.12880
24. Tisack A, Fotouhi A, Fidai C, et al. Clinical and biological review of keratoacanthomas. Br J Dermatol. 2021;185(3):487–498. doi:10.1111/bjd.20389
25. Kolmodin A, Pandeya NP, Olsen CM, et al. Patient and tumour characteristics of keratoacanthoma in a large, community-based cohort study from Queensland, Australia. Acta Derm Venereol. 2021;101(6):adv00469. doi:10.2340/00015555-3824
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.