Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 7
Different T cells' distribution and activation degree of Th17 CD4+ cells in peripheral blood in patients with osteoarthritis, rheumatoid arthritis, and healthy donors: preliminary results of the MAGENTA CLICAO study
Authors Lurati AM, Laria A, Gatti A, Brando B, Scarpellini M
Received 30 January 2015
Accepted for publication 20 April 2015
Published 16 October 2015 Volume 2015:7 Pages 63—68
DOI https://doi.org/10.2147/OARRR.S81905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Alfredomaria Lurati,1 Antonella Laria,1 Arianna Gatti,2 Bruno Brando,2 Magda Scarpellini1
1Rheumatology Unit, Fornaroli Hospital, Magenta, Italy; 2Transfusional Centre, Legnano Hospital, Legnano, Italy
Objective: To determine distribution of T cells and activation degree of Th CD4+ cells in peripheral blood of patients with osteoarthritis (OA), rheumatoid arthritis (RA), and healthy donors.
Methods: Patients with established diagnosis of RA according to American College of Rheumatology/European League Against Rheumatism 2010 criteria, knee or hip OA according to American College of Rheumatology criteria, and healthy blood donor volunteers were eligible. Multi-channel flow cytometry and monoclonal antibodies against CD3, CD4, CD8, CCR6, CD38, CXCR3, and HLA DR were used to distinguish and evaluate T cells' subpopulation.
Results: We analyzed blood samples of 15 patients with well-defined RA, 56 with hip or knee OA, and 20 healthy age matched controls. Blood samples from RA patients showed significantly higher counts of CD4+ CD38+ DR+ (activated CD4 T cells) and Th17 (CCR6+ CXCR3-) cells as compared to OA patients and control group (P<0.01). Furthermore the samples from the OA patients showed a higher percentage of activated CD4 T cells and Th17 cells as compared to control group (P<0.05). Interestingly there was no difference between Th1 (CD4+ CXCR3+ CCR6-) and Th2 (CD4+ CXCR3- CCR6-) between the three groups (P>0.1).
Conclusion: According to the latest view of OA disease pathogenesis, our preliminary results support the hypothesis that OA may also be a disease with an immunological/inflammatory involvement like RA. It seems that there is a quantitative but non-qualitative difference in Th17 cells' profile, including the expression of activation markers, between RA and OA.
Keywords: Th17, flow cytometry, osteoarthritis
Introduction
Osteoarthritis (OA) is a chronic, painful, disabling condition affecting the whole joint (bone, synovia, and cartilage), well defined clinically and radiologically, but its etiology is largely poorly understood.1–4 In a pro-inflammatory milieu, chondrocytes become metabolically active and initiate inflammatory processes that secrete several inflammatory cytokines that work synergistically to stimulate synthesis of enzymes that break down cartilage. Immunohistochemical studies have confirmed that mononuclear cell infiltration, lymphocytes and macrophages, and production of pro-inflammatory cytokines and mediators of joint damage are common synovial membrane (SM) characteristics in patients with OA.5–7 The study of OA synovial fluid (SF) has rendered similar findings.8–13 Mononuclear cell infiltrates in synovial tissues (ST) have been reported in OA8,10 and have been shown to contain primarily CD3+ T cells.14 The Th1 subset of T cells was found to be approximately five times more than Th2 cells and higher levels of Th1 cytokines, IL2, and INF-gamma, were detected in most OA patients.15,16 Data from literature show that CD4+/CD8+ ratio in OA ST is approximately 5:1 compared to normal ST where the ratio is 2:1 and the higher ratio is comparable to rheumatoid arthritis (RA) ST.16,17 Furthermore, T cells’ CD4+ levels are higher in early OA compared to late stage OA.17 Studies on IL-1 levels in SF specimens from different arthropathies, including OA, have shown that the range of IL-1 levels in OA are similar than in RA, a chronic inflammatory disease known to be characterized by the presence of a prominent cellular infiltrate in the SM and the SF.5,11,15 T lymphocytes represent the most important cell type for immune functions and are responsible for specific immunity involved in the arthritic process. T cell populations are not homogenous and consist of different subgroups, each with a specific function and structure. In addition to common surface antigens (CD) found in all T lymphocytes (such as CD2, CD3, and CD5), other surface molecules also exist that are used to discriminate between different T lymphocyte subgroups (such as CD61, CCR6, CCR4, CXCR3). CD4+ Th cells are activated by the antigenic stimulation of T cell receptors and differentiated into different subsets of effector Th cells.15 Among these cells, INF-gamma-producing Th1 cells are predominant in RA. Recent reports have suggested that IL-17-producing Th17 cells are a new subset of cells critical to the pathogenesis of RA. IL-17 induces the production of inflammatory cytokines such as IL-1, IL-6, IL-8, and TNF-α and it has been detected in the serum, SF, and synovium of patients with RA.18,19 Beyond Th17 and Th1 cells, there is a third pathogenetic Th cell population in RA, namely Th17/1 cells. This population expresses a cytokine phenotype intermediate between Th17 and Th1.20 On their surface, Th17/1 cells express CCR6 and CD61, suggesting a common origin of Th17 lymphocytes. However, Th17/1 are CCR4 negative, different from Th17. This intermediate population is CXCR3 and T-bet positive (like Th1 cells) and produce both IL-17and INF-gamma.20 On the other hand, reports about T cell subtypes in OA SM or SF are scarce. In particular, CD4+ T lymphocytes and their cytokines play a major role in the initiation of inflammation in this disease. The objective of this study was to analyze, by means of various CD markers’ expression, the means level and activation degree of T cells particularly Th17 lymphocytes in peripheral blood samples from OA patients and to compare them with samples from patients with RA and healthy controls.
Methods
Patients with established diagnosis of RA according to American College of Rheumatology/European League Against Rheumatism 2010 criteria, knee or hip OA according to American College of Rheumatology criteria, and healthy blood donor volunteers were eligible. Other inclusion criteria were: DAS28 (disease activity score based on 28 joints) between 3.2 and 5.1 or a Western Ontario and McMaster Universities Arthritis Index (WOMAC) score of more than 50 respectively in patients with RA or OA, age between 40 and 60 years old, a Kellgren Lawrence index of 2–3. Patients with RA were naïve to disease-modifying antirheumatic drugs therapy including methotrexate and steroids. Patients with OA were naïve to treatment with nonsteroidal anti-inflammatory drugs and disease-modifying osteoarthritis drugs. Exclusion criteria were the presence of other autoimmune diseases, tumors or secondary OA. Finally no intra-articular treatment with steroids or hyaluronic acid was allowed from 3 months before enrollment. Multichannel flow cytometry and monoclonal antibodies against CD3, CD4, CD8, CCR6, CD38, CXCR3, and HLA DR were used to distinguish between and evaluate T cells’ subpopulation. Participants were informed about the aim of the project and gave their written consent. A second sample to confirm the results was obtained 1 month later and the same analysis was performed. The Fornaroli Hospital Local Ethics Committee approved the project. All patients signed informed consent to participate in the study. We collected blood samples from February 2014 to November 2014.
Statistical analysis
The Shapiro-Wilk test was used to study the normality of variables. Data are displayed as mean and standard deviation. In view of non-normal distribution, variables were compared using the Mann–Whitney test for two groups and the Kruskal–Wallis test for multiple groups. Values less than 0.05 were considered significant. SPSS version 14 for Windows was used.
Flow cytometry
Freshly drawn ethylenediaminetetraacetic acid blood samples were analyzed by 8-color flow cytometry (FACSCanto II; BD, Franklin Lakes, NJ, USA) with the following conjugated antibody panel: CD45-FITC; CXCR3-PE; CD4-PerCP-Cy5.5; CCR6-PE-Cy7; CD38-Alexa 647; CD8-APC-H7; CD3-V450; HLA DR-V500 at the appropriate concentrations (all from BD, manufacturer’s recommended concentrations). After 20-minute staining in the dark, 2 mL of ammonium chloride lysing was added for 10 minutes. After centrifugation at 1,500 rpm for 7 minutes, the pellet was re-suspended in 200 microliters of cold phosphate buffered saline and immediately analyzed. At least 50,000 lymphocytes (defined as CD45+++, SSClow cells) were acquired. The gating strategy included the parallel capture of CD4+/CD3+ and CD8+/CD3+ cells in two separate downstream hierarchies. Each parent subset was then further dissected into functional subpopulations, namely CD4+ T cells as Th1 cells (CD4+ CXCR3+ CCR6−), Th2 cells (CD4+ CXCR3− CCR6−) and Th17 cells (CD4+ CXCR3− CCR6+), respectively according to Maecker et al.21 Both CD4+ and CD8+ cells were divided into quiescent (CD38− HLADR−) or activated elements (CD38+ and/or HLADR+). Functional subset percentages were calculated over the total lymphocyte population and over the parent CD4+ or CD8+ subsets, respectively, and all values were also recorded as absolute levels per microliter on the basis of total lymphocyte count (DXH800; Beckman Coulter, Brea, CA, USA).
Results
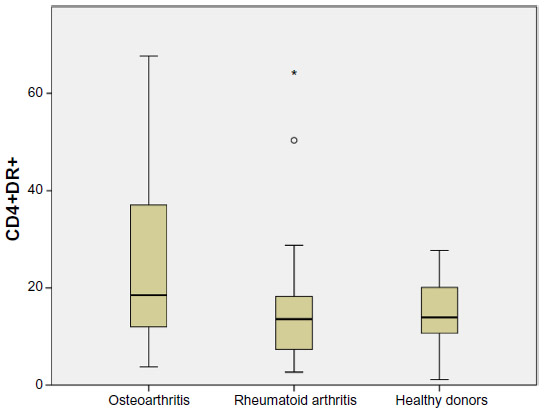
We analyzed blood samples of 91 subjects (75 females, 16 males): 15 patients with well-defined RA, 56 with hip or knee OA, and 20 healthy age matched controls. Median age was 43 (range 34–52) years old (P>0.05 between groups). The median duration of disease in OA and RA patients was 3.8 (range 3.1–5.7) and 3.1 (range 2.8–4.5) years respectively (P>0.05). Blood samples from the RA patients had a significantly higher count of CD4+ CD38+ DR+ (activated CD4 T cells) and Th17 (CCR6+ CXCR3−) cells as compared to OA patients and control group (P<0.01). Furthermore the samples from the OA patients had a higher percentage of activated CD4 T cells as compared to control group (P<0.05) (Figures 1–6). Interestingly there was no difference between Th1 (CD4+ CXCR3+ CCR6−), Th2 (CD4+ CXCR3- CCR6−), and Th17 levels between the three groups (P>0.1). Analog results were obtained in the second sample performed 1 month later, with no significant variations between groups (P>0.05).
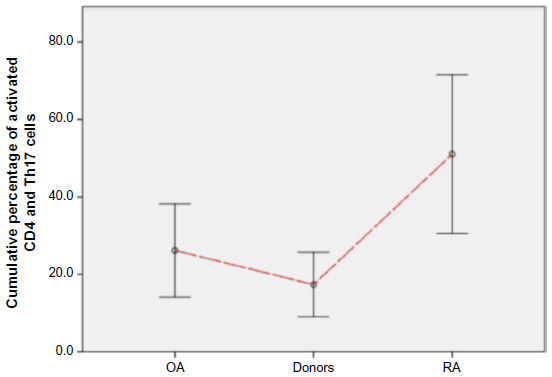 | Figure 1 Percentage of activated CD4 T cells and Th17 cells from the samples of the OA patients compared to control group. |
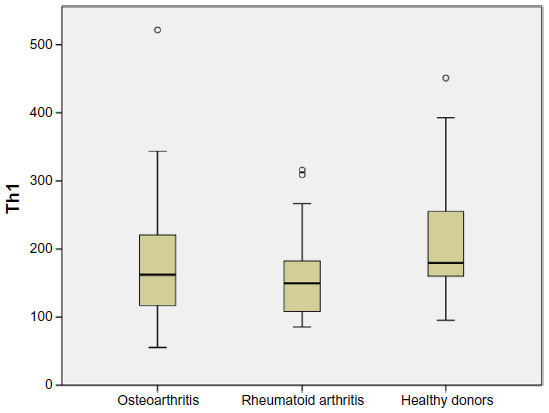 | Figure 2 Th1 levels in each subgroup (median with range and outlier values are shown). |
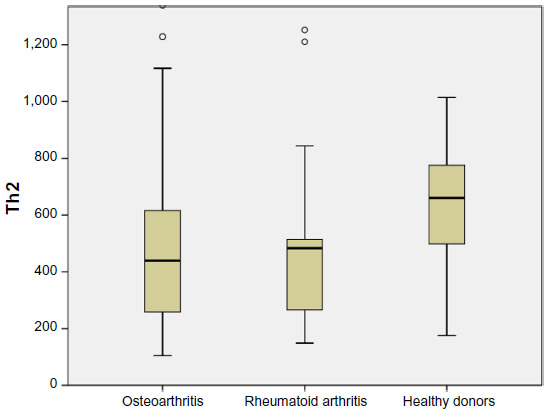 | Figure 3 Th2 levels in each subgroup (median with range and outlier values are shown). |
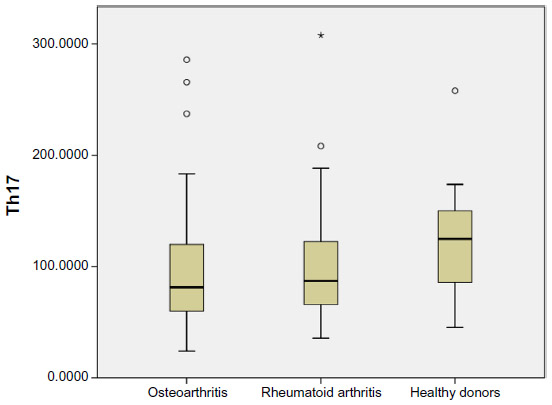 | Figure 4 Th17 levels in each subgroup (median with range and outlier values are shown). |
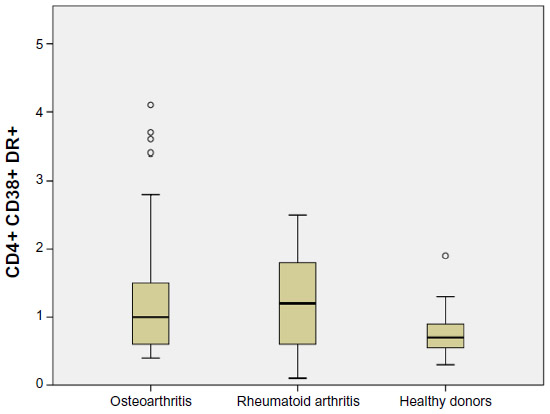 | Figure 5 Th cell activated (CD38+ and DR+) levels in each subgroup (median with range and outlier values are shown). |
 | Figure 6 Th cell activated (CD38+) levels in each subgroup (median with range and outlier values are shown). |
Discussion
Circulating markers of inflammation, such as CRP, may be elevated in OA compared with control populations without disease.22–24 Histological examination of synovia frequently demonstrates inflammatory cell infiltration, involving macrophages and lymphocytes, increased cell turnover and angiogenesis.25,26 CD4+ Th cells are activated by the antigenic stimulation of T cell receptors and differentiated into different subsets of effector Th cells.18 It is well known that RA has been characterized by a Th1 response. Among these cells, INF-gamma-producing Th1 cells are predominant in RA. However, the etiopathogenetic role in RA of a new Th subset (Th17) has appeared to be very important in the last years. These Th17 cells and Th17/1 are more important than Th1 in the contribution to pathogenesis in early RA.27,28 IL-17 induces the production of inflammatory cytokines such as IL-1, IL-6, IL-8, and TNF-α and it has been detected in the serum, SF, and synovium of patients with RA and OA.18 Previous reports including tissue samples from patients with OA and RA had demonstrated infiltrating mononuclear cells and pro-inflammatory cytokines in both diseases but consistently less abundant in OA. Gallelli et al recently described levels of IL-6, TNF-α, and VEGF in SF of patients with knee OA.29–33 The pro-inflammatory cytokine IL-17 is implicated in both the induction of local inflammation and the joint destruction that characterize the ST of RA. IL-17 is able to stimulate fibroblast-like synoviocytes, macrophages, chondrocytes, and osteoclasts.34,35 IL-17 is present at increased concentrations in serum, SF, and synovium samples from patients with RA and has been shown to induce and perpetuate chronic inflammation, cartilage damage, and bone erosion. In RA, the number of Th17 cells in peripheral blood correlates with disease activity.36 Many studies have demonstrated the Th17 cell heterogeneity, high degree of phenotypic instability and plasticity, responsible for induction of a Th1-like phenotype.36–38 Ghoreschi et al demonstrated that Th17 cells can be divided into pathogenic and non-pathogenic phenotype according to their different cytokine secretion. In particular, IL-17, IL-21, IL-22, IL-2, and IFN-gamma are secreted by pathogenic cells (including Th17/1); while non-pathogenic Th17 release IL-17, IL-21, IL-9, and IL-10. According to cytokine milieu, Th17 can induce differentiation in Th17/1 lymphocytes or into Th1 phenotype, in the presence of IL-12 or IL-23 in the absence of TGF-beta in vitro, respectively.37–40 Th17/1 cells secrete IL-17 and INF-gamma while Th1 cells do not release IL-17 but only INF-gamma. OA shares several characteristics with RA, including joint destruction and synovitis. It can be assumed that tissue damage in OA is responsible for the chemotaxis of inflammatory cells, while in RA joint destruction is considered to be a consequence of inflammation. In addition, IL-17 has been shown to be present in SF from patients with OA. However, in literature there are few data about Th17/1 in OA, today.41 In this report, we showed that patients with OA have a different expression of activated Th cells, with a marked tendency of higher expression than healthy controls. There was no significant qualitative evidence but only quantitative differences between RA and OA Th sub-populations thus indicating that lymphocytes in OA and RA exhibited a similar Th phenotype with evident activation and involving the same pro-inflammatory cytokines. In particular, we found the same levels in the OA and RA subgroups of Th1 cells, Th2 cells, and Th17 cells. Also, the levels of CD38+ DR+ and DR+ cells were similar in OA and RA subgroups, significantly higher than in the healthy control group. These results indicate that, despite a mechanical contribution to its pathophysiology, OA might be characterized as a low-grade inflammatory condition, similar to other rheumatic diseases with a well-known inflammatory etiology such as RA.
Disclosure
The authors have no conflicts of interest to disclose.
References
Lories RJ, Luyten FP. The bone-cartilage unit in osteoarthritis. Nat Rev Rheumatol. 2011;7(1):43–49. | |
Egloff C, Hügle T, Valderrabano V. Biomechanics and pathomechanisms of osteoarthritis. Swiss Med Wkly. 2012;142:w13583. | |
Smith MD, Triantafillou S, Parker A, Youssef PP, Coleman M. Synovial membrane inflammation and cytokine production in patients with early osteoarthritis. J Rheumatol. 1997;24(2):365–371. | |
Berembaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage. 2013;21(1):16–21. | |
Revell PA, Mayston V, Lalor P, Mapp P. The synovial membrane in osteoarthritis: a histological study including the characterization of the cellular infiltrate present in inflammatory osteoarthritis using monoclonal antibodies. Ann Rheum Dis. 1988;47(4):300–307. | |
Ayral X, Pickering EH, Woodworth TG, Mackillop N, Dougados M. Synovitis: a potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis results of a year longitudinal arthroscopic study in 422 patients. Osteoarthritis Cartilage. 2005;13(5):361–367. | |
Hill CL, Hunter DJ, Niu J, et al. Synovitis detected on magnetic resonance imaging and its relation to pain and cartilage loss in knee osteoarthritis. Ann Rheum Dis. 2007;66(12):1599–1603. | |
Haraoui B, Pelletier JP, Cloutier JM, Faure MP, Martel-Pelletier J. Synovial membrane histology and immunopathology in rheumatoid arthritis and osteoarthritis. II. In vivo effects of antirheumatic drugs. Arthritis Rheum. 1991;34(2):153–163. | |
Kennedy ID, Plater-Zyberk C, Partridge TA, Woodrow DF, Maini RN. Morphometric comparison of synovium from patients with osteoarthritis and rheumatoid arthritis. J Clin Pathol. 1988;41(8):847–852. | |
Lindblad S, Hedfors E. Arthroscopic and immunohistologic characterization of knee joint synovitis in osteoarthritis. Arthritis Rheum. 1987;30(10):1081–1088. | |
Myers SL, Brandt KD, Ehlich JW, et al. Synovial inflammation in patients with early osteoarthritis of the knee. J Rheumatol. 1990;17(12):1662–1669. | |
Orita S, Koshi T, Mitsuka T, et al. Associations between proinflammatory cytokines in the synovial fluid and radiographic grading and pain-related scores in 47 consecutive patients with osteoarthritis of the knee. BMC Musculoskelet Disord. 2011;12:144. | |
Lùrati A, Laria A, Mazzocchi D, Re KA, Marrazza M, Scarpellini M. Effects of hyaluronic acid (HA) viscosupplementation on peripheral Th cells in knee and hip osteoarthritis. Osteoarthritis Cartilage. 2015;23(1):88–93. | |
Ishii H, Tanaka H, Katoh K, Nakamura H, Nagashima M, Yoshino S. Characterization of infiltrating T cells and Th1/Th2 type cytokines in the synovium pf patients with osteoarthritis. Osteoarthritis Cartilage. 2002;10(4):277–281. | |
Sakkas LI, Scanzello C, Johanson N, et al. T cells and T cell cytokine transcripts in the synovial membrane in patients with osteoarthritis. Clin Diagn Lab Immunol. 1988;5(4):430–437. | |
Saito I, Koshino T, Nakashima K, Uesugi M, Saito T. Increased cellular infiltrate in inflammatory synovia of osteoarthritic knees. Osteoarthritis Cartilage. 2002;10(2):156–162. | |
De Lange-Brokaar BJ, Ioan-Facsinay A, van Osch GJ, et al. Synovial inflammation, immune cells and their cytokines in osteoarthritis: a review. Osteoarthritis Cartilage. 2012;20(12):1484–1499. | |
Kuryliszyn-Moskal A. Comparison of blood and synovial fluid lymphocyte subsets in rheumatoid arthritis and osteoarthritis. Clin Rheumatol. 1995;14(1):43–50. | |
Hussein MR, Fathi NA, El-Din AM, et al. Alterations of the CD4(+), CD8(+) T cell subsets, interleukins-1beta, IL-10, IL-17, tumor necrosis factor-alpha and soluble intercellular adhesion molecule-1 in rheumatoid arthritis and osteoarthritis: preliminary observations. Pathol Oncol Res. 2008;14(3):321–328. | |
Nistala K, Adams S, Cambrook H, et al. Th17 plasticity in human autoimmune arthritis is driven by the inflammatory environment. Proc Natl Acad Sci U S A. 2010;107(33):14751–14756. | |
Maecker HT, McCoy JP, Nussenblatt R. Standardizing immunophenotyping for the Human Immunology Project. Nat Rev Immunol 2012. Feb 17;12(3):191–200. | |
Conrozier T, Chappuis-Cellier C, Richard M, Mathieu P, Richard S, Vignon E. Increased serum C-reactive protein levels by immunonephelometry in patients with rapidly destructive hip osteoarthritis. Rev Rhum Engl Ed. 1998;65(12):759–765. | |
Spector TD, Hart DJ, Nandra D, et al. Low-level increases in serum C-reactive protein are present in early osteoarthritis of the knee and predict progressive disease. Arthritis Rheum. 1997;40(4):723–727. | |
Sharif M, Elson CJ, Dieppe PA, Kirwan JR. Elevated serum C-reactive protein levels in osteoarthritis. Br J Rheumatol. 1997;36(1):140–141. | |
Wolfe F. The C-reactive protein but not erythrocyte sedimentation rate is associated with clinical severity in patients with osteoarthritis of the knee or hip. J Rheumatol. 1997;24(8):1486–1488. | |
Haywood L, McWilliams DF, Pearson CI, et al. Inflammation and angiogenesis in osteoarthritis. Arthritis Rheum. 2003;48(8):2173–2177. | |
Dong W, Zhu P. Functional niche of inflamed synovium for Th17 cell expansion and activation in rheumatoid arthritis:implication to clinical therapeutics. Autoimmun Rev. 2012;11(12):844–851. | |
Jimeno R, Gomariz RP, Garín M, et al. The pathogenic Th profile of human activated memory Th cells in early rheumatoid arthritis can be modulated by VIP. J Mol Med (Berl). 2015;93(4):457–467. | |
Gallelli L, Galasso O, Falcone D, et al. The effects of non-steroidal anti-inflammatory drugs on clinical outcomes, synovial fluid cytokine concentration and signal transduction pathways in knee osteoarthritis. A randomized open label trial. Osteoarthritis Cartilage. 2013;21(9):1400–1408. | |
Farahat MN, Yanni G, Poston R, Panayi GS. Cytokine expression in synovial membranes of patients with rheumatoid arthritis and osteoarthritis. Ann Rheum Dis. 1993;52(12):870–887. | |
Bianchi M, Broggini M, Balzarini P, Franchi S, Sacerdote P. Effects of nimesulide on pain and on synovial fluid concentrations of substance P, interleukin-6 and interleukin-8 in patients with knee osteoarthritis: comparison with celecoxib. Int J Clin Pract. 2007;61(8):1270–1277. | |
Schumacher HR Jr, Meng Z, Sieck M, et al. Effect of a nonsteroidal anti-inflammatory drug on synovial fluid in osteoarthritis. J Rheumatol. 1996;23(10):1774–1777. | |
Alvarez-Soria MA, Largo R, Santillana J, et al. Long term NSAID treatment inhibits COX-2 synthesis in the knee synovial membrane of patients with osteoarthritis: differential pro-inflammatory cytokine profile between celecoxib and aceclofenac. Ann Rheum Dis. 2006;65(8):998–1005. | |
Lubberts E, Koenders MI, Oppers-Walgrenn B, et al. Treatment with a neutralizing anti-murine interleukin-17 antibody after the onset of collagen-induced arthritis reduces joint inflammation, cartilage destruction, and bone erosion. Arthritis Rheum. 2004;50(2):650–659. | |
Benedetti G, Miossec P. Interleukin 17 contributes to the chronicity of inflammatory diseases such as rheumatoid arthritis. Eur J Immunol. 2014;44(2):339–347. | |
Kim J, Kang S, Kim JK, Kwon G, Koo S. Elevated levels of T helper 17 cells are associated with disease activity in patients with rheumatoid arthritis. Ann Lab Med. 2013;33(1):52–59. | |
Ghoreschi K, Laurence A, Yang XP, Hirahara K, O’Shea JJ. T helper 17 cell heterogeneity and pathogenicity in autoimmune disease. Trends Immunol. 2011;39(9):395–401. | |
Lexberg MH, Taubner A, Albrecht I, et al. IFNγ and IL-12 synergize to convert in vivo generated Th17 into Th1/Th17 cells. Eur J Immunol. 2010;40(11):3017–3027. | |
Annunziato F, Cosmi L, Santarlasci V, et al. Phenotypic and functional features of human Th17 cells. J Exp Med. 2007;204(8):1849–1861. | |
Lee YK, Turner H, Maynard CL, et al. Late developmental plasticity in the T helper 17 lineage. Immunity. 2009;30(1):92–107. | |
Honorati MC, Bovara M, Cattini L, Piacentini A, Facchini A. Contribution of interleukin 17 to human cartilage degradation and synovial inflammation in osteoarthritis. Osteoarthritis Cartilage. 2002; 10(10):799–807. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.