Back to Journals » International Journal of Women's Health » Volume 17
Differences in Pelvic Organ Prolapse and Diastasis Recti Abdominis Between Primiparous and Age-Matched second-Parous Females After Vaginal Delivery: A Retrospective Cohort Study
Authors Lin T, Lou W, Chien JH, Zhang X, Wei H, Fan G, Zhu L ![]()
Received 15 November 2024
Accepted for publication 27 February 2025
Published 3 March 2025 Volume 2025:17 Pages 585—595
DOI https://doi.org/10.2147/IJWH.S506821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Tangdi Lin,1 Wenjia Lou,1 Jung hung Chien,2 Xue Zhang,1 Huanhuan Wei,1 Guorong Fan,1 Lan Zhu3
1Department of Obstetrics and Gynecology, National Clinical Research Center for Obstetric & Gynecologic Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Department of Health & Rehabilitation Science, College of Allied Health Professions, University of Nebraska Medical Center, Omaha, NE, USA; 3Department of Obstetrics and Gynecology, National Clinical Research Center for Obstetric & Gynecologic Diseases, State Key Laboratory of Common Mechanism Research for Major Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China
Correspondence: Lan Zhu, Department of Obstetrics and Gynecology, National Clinical Research Center for Obstetric & Gynecologic Diseases, State Key Laboratory of Common Mechanism Research for Major Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China, Email [email protected]
Purpose: This study aims to investigate the differences in pelvic floor dysfunction (PFD) and diastasis recti abdominis (DRA) between primiparous and second-parous females with known risk factors controlled.
Patients and Methods: 49 primiparous and 49 age-matched second-parous postpartum after spontaneous vaginal delivery were included between October and December 2023. Independent variables include weight, height, body mass index (BMI), fetal weight, gestational weight gain (GWG). Main outcome measurements include vaginal resting pressure (VRP) and maximum voluntary contraction pressure (MVCP) indicating pelvic floor muscle strength, the stage of anterior (APOP) and posterior pelvic organ prolapse (PPOP) and inter-recti distance (IRD) indicating DRA. Independent t-test and Chi-square test of independence were used to analyze differences between two groups for continuous and categorical variables, respectively.
Results: No significant differences were found in terms of vaginal pressure measurements between two groups (VRP: t (96) = 0.07, p = 0.942; MVCP: t (96) = 0.40, p = 0.689). Second-parous group showed significantly more severe DRA with larger IRD than primiparous group (t (96) = − 2.405, p = 0.018). No significant association was found between parity and APOP stage (χ2(1) = 2.67, p = 0.102) in this current study; however, second-parous females demonstrated greater PPOP stage than primiparous females (χ2(1) = 5.24, p = 0.022).
Conclusion: Second-parous females at similar age are more likely to experience PPOP than primiparous group after spontaneous vaginal delivery. Greater public attention with plausible actions should be taken for second-parous female group to prevent more severe postpartum pelvic floor dysfunction.
Keywords: pelvic floor dysfunction, postpartum, second-parous females, pelvic floor muscle strength, pelvic organ prolapse, diastasis recti abdominis
Introduction
Pelvic floor dysfunction (PFD) includes, but is not limited to, bladder and bowel dysfunction, pelvic organ prolapse, sexual dysfunction, and pelvic pain.1 During the past three decades, PFD has remained a major health concern, particularly in low- and middle-income areas.1,2 The prevalence of PFD worldwide ranges from 25% to 46.5%,3–7 reaching its peak in the 70–74 age group for females.8 PFD has a substantial negative impact on females’ quality of life, including physical, psychological, social, and emotional aspects.9 Based on available research, treatment costs for persons with PFD account for approximately 50% of their weekly income in some low-income areas.2 According to another study, PFD either increases the burden of caretaking on families or contributes to social isolation and mental health issues.9 Therefore, detecting PFD at an early stage is highly recommended.
Currently, clinical assessments of pelvic organ prolapse (POP),10–12 pelvic floor muscle (PFM) strength,13–15 and diastasis recti abdominis (DRA)15,16 have been used to provide a comprehensive understanding of female postpartum pelvic floor dysfunction. The most frequently used clinical assessments of POP and DRA are the Pelvic Organ Prolapse Quantification System (POP-Q)17 and digital measurements of the inter-recti distance (IRD),18 respectively. As reliable assessments, both tools have been validated by researchers and are widely used in clinical settings due to their convenience.18,19 As for PFM, it is important to note that there is no gold standard for measuring the muscle strength and endurance as of yet.20 Multiple assessment tools are used in conjunction with each other to gain a full picture of pelvic floor muscle strength and endurance in clinical practice, including manual muscle testing,21 manometry,22,23 electromyography,22,23 and imaging techniques.24,25 Due to its simplicity and non-invasive nature, manometry is one of several methods that has been used widely to assess PFM strength objectively. Additionally, the reliability and validity of manometry have been demonstrated in previous clinical studies.26–28 To effectively control the co-contraction of lower transverse abdominals as one of the observed compensation strategies during pelvic floor contractions, the authors of the study by Bo er al.29 highlighted the significance of the observation of the balloon catheter during the test since the inward movement of the balloon catheter is only apparent during correct contraction with an elevated PFM.
It has been well established by existing literature that pelvic floor and abdominal muscles are highly correlated to explain female postpartum pelvic floor function. Together with diaphragm, pelvic floor and abdominal muscles play essential roles in the maintenance of intra-abdominal pressure and core stability.30 PFM relaxes and contracts during inhalation and exhalation as the abdomen expands or rests in pace with the diaphragm.31 DRA, a direct clinical indicator of abdominal weakness, can result in improper trunk posture, such as anterior pelvic tilt. Consequently, this may alter the length of PFM and diminish its capacity to regulate intra-abdominal pressure.32,33 PFM tends to manage increased intra-abdominal pressure with excessive tightness, known as elevated muscle tone, limiting its ability to contract and relax and ultimately contributing to pelvic floor dysfunction. A study by Zhang et al34 has explored the correlation between IRD and PFM function and discovered that females with DRA demonstrated weakened PFM endurance, particularly in the urethral sphincter and external anal sphincter muscles. Both two muscles are important superficial components of PFM while the abnormal function of them may affect the urogenital hiatus and weaken the support of pelvic floor organs, leading to POP eventually.
POP, DRA combined with decreased PFM strength are all known potential postnatal consequences.3,35,36 There are several risk factors associated with PFD after childbirth, including maternal age,37 delivery mode,26 and parity.16,38 Previous research work has shown that females over the age of 35 years old are more likely to experience adverse maternal outcomes39 and postnatal PFD.40 As a result of considering multiple factors, including hormone changes during pregnancy and overstretching of connective tissue during delivery,41 researchers found that neither vaginal nor cesarean delivery can protect females from postnatal PFD.41–44 Therefore, it is reasonable to control these influential factors to make groups more comparable in the study. In terms of parity, Elenskaia et al28 found there is a significant increase in the prevalence of different types of PFD after the first pregnancy and increases further with subsequent pregnancies. To investigate how childbirth relates to PFD, current studies often categorized females into nulliparous, primiparous, and multiparous groups. Blomquist et al45 reported that multiparous females who have had at least one vaginal delivery are more likely to demonstrate weaker PFM strength, which is associated with a greater risk of PFD but females who have delivered all children by cesarean delivery showed no such association. However, there is lacking evidence suggesting how pelvic floor function changes specifically after each childbirth with maternal age and delivery mode controlled. Therefore, the purpose of this study is (1) to investigate how PFM strength differs after second childbirth compared to the first childbirth between age-matched and delivery mode-controlled group, and (2) to explore the incidence of postpartum POP and DRA among primiparous and second-parous females after controlling maternal age and delivery mode. We hypothesized that PFM strength would decrease with more severe stage of prolapse and an increased incidence of IRD in the second-parous group.
Materials and Methods
Study Design and Population
A retrospective single-center cohort study was conducted at Peking Union Medical College Hospital from October 2023 to December 2023 on 77 second-parous and 227 primiparous women who attended postpartum pelvic floor evaluation in the Department of Obstetrics and Gynecology. The inclusion criteria include primiparous or second-parous females who were 6 to 12 weeks postpartum with spontaneous vaginal delivery and seen by the same pelvic floor physical therapist. Participants were excluded if they underwent caesarean section or instrumental vaginal delivery, suffered from severe pregnancy complications, had missing data in their medical records, or had enrolled in any kind of PFM rehabilitation following this current childbirth. Finally, 49 second-parous females and 49 age-matched primiparous females remain in this study. All data were collected from a computerized medical record system including data concerning basic individual information, obstetric history, and pregnancy outcomes. Independent variables include weight, height, body mass index (BMI), fetal weight, gestational weight gain (GWG) (Table 1). In terms of GWG, the data collected in our study was the participant’s weight at the last prenatal visit minus that at the first one. Primary outcomes included vaginal resting pressure (VRP), maximum voluntary contraction pressure (MVCP), anterior (APOP) or posterior pelvic organ prolapse (PPOP) stages, and DRA postpartum. Vaginal pressure was measured using manometry as the catheter balloon was placed with the middle of the balloon 3.5 cm inside the introitus vagina, and a simultaneous inward movement of the vaginal catheter should be observed to ensure the correct PFM contraction.29 VRP represents the original pressure value before contractions, and MVCP represents the difference between the peak vaginal pressure and the resting vaginal pressure during maximum voluntary contraction,13 which is proportional to the force of PFM and is widely used as an indicator of the strength of the PFM.46,47 Participants were placed in dorsal lithotomy positions, and the degree of prolapse was assessed during the Valsalva maneuver. Stages of POP-Q system measurements were utilized with the hymen as the reference point. Stage 0 is defined as no prolapse is demonstrated. Stage 1 is defined as the most distal portion of the prolapse is more than 1 cm above the level of the hymen. Stage 2 is defined as the most distal portion of the prolapse is 1 cm or less proximal or distal to the hymenal plane.17 DRA refers to the separation of the rectus abdominis muscle, which is quantified by the IRD.48 IRD was measured with palpation at the level of the umbilicus by measuring the number of fingers that fit between the medial borders of the rectus abdominis muscles. DRA is defined as an IRD that is larger than two finger widths.18 There have been previous studies that have shown the validity of both methods of assessing prolapse and DRA.18,19
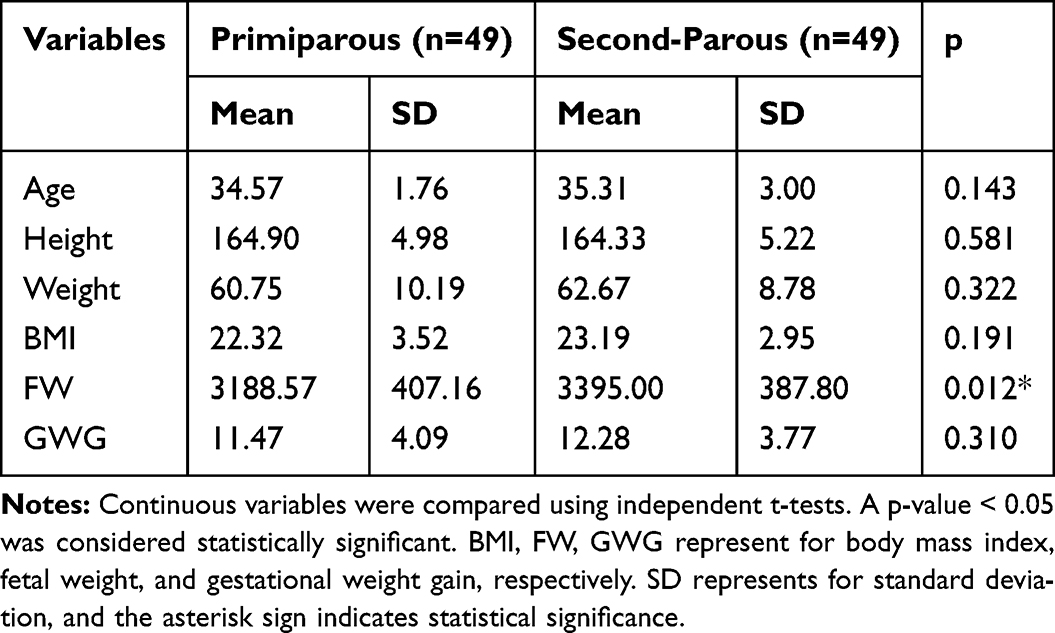 |
Table 1 Basic Characteristics Between Primiparous and second-Parous Females |
Statistical Analysis
Continuous and categorical variables are expressed as the mean ± standard deviation and percentages, respectively. Continuous variables were compared using the independent t-test, and categorical variables were compared using the chi-square test. For the primary outcomes, chi-square tests were used to compare categorical variables such as APOP stages, PPOP stages, and DRA between groups, and independent t-tests were used to determine whether there was a difference between groups for VRP, MVCP, and IRD. To make the Chi-square test results valid with no observed cell numbers less than 5, APOP and PPOP stages were both eventually combined into 2 groups. Group 1 of APOP stages include APOP stage 0 and stage 1 while group 2 include only stage 2. Group 1 of PPOP stages include only PPOP stage 0 and group 2 of PPOP stages include stage 1 and 2. A statistical analysis was conducted using SPSS 22.0 (IBM, Armonk, NY, USA). A p-value < 0.05 was considered statistically significant. To evaluate the achieved power of this study, a post-hoc power analysis using G*Power (Version 3.1) has been conducted. Cohen’s d (for the independent t-test) and Cramér’s V (for the Chi-square test) were set at 0.5 and 0.3, respectively, to reflect a moderate effect size. These values were based on previous research studies demonstrating a moderate effect of parity on pelvic floor dysfunction and diastasis recti abdominis.49–51 With an alpha level of 0.05, and a total sample size of 98 (49 primiparous and 49 second-parous participants), the calculated power was 0.98 for the Chi-square test and 0.99 for the independent t-test, which demonstrated that the sample size was sufficient to detect statistically significant differences between two groups. The study was approved by Peking Union Medical College Hospital Ethics Committee (IRB Number: I-24PJ0428).
Results
There were no significant differences found between two groups considering both VRP (t (96) = 0.07, p = 0.942) and MVCP (t (96) = 0.40, p = 0.689) after childbirth (Table 2). The IRD of women who had a second pregnancy (1.89 cm x 1.17 cm) was significantly higher than that of primiparous women (1.31 cm x 1.22 cm) (t (96) = −2.405, p = 0.018), with an average difference of 0.58 cm (95% CI, 0.10 ±1.1) cm (Table 2 and Figure 1). The effect size was moderate, Cohen’s d = −0.486 (95% CI, −0.887,-0.083), further underscoring the substantial impact of a second pregnancy on the widening of the IRD. Significant difference was found between two groups when considering DRA (χ2(1) = 4.10, p = 0.043) (Table 3). The current incidence of APOP was 42.9%% (group 1) and 57.1% (group 2) and that of PPOP was 26.5% (group 1) and 73.5% (group 2) respectively, regardless of parity (Table 3 and Figure 2). The association between parity and postpartum APOP, however, does not appear to be significant (χ2(1) = 2.67, p = 0.102). Second-parous females were significantly more likely to experience PPOP than primiparous females (χ2(1) = 5.24, p = 0.022). The effect size was moderate, Cramér’s V = 0.23, suggesting that parity is a meaningful predictor of posterior pelvic organ prolapse.
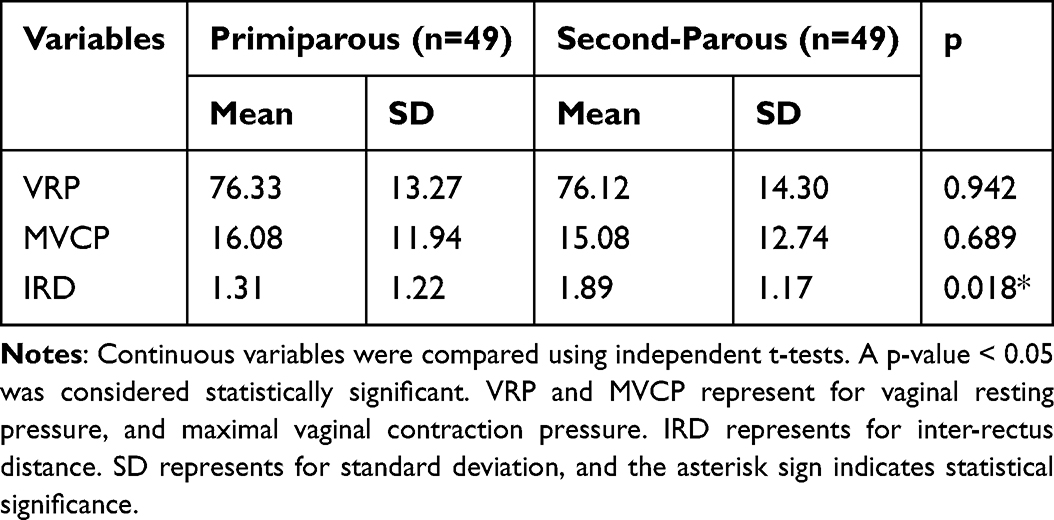 |
Table 2 The Analysis of Continuous Outcome Variables Between Primiparous and second-Parous Groups |
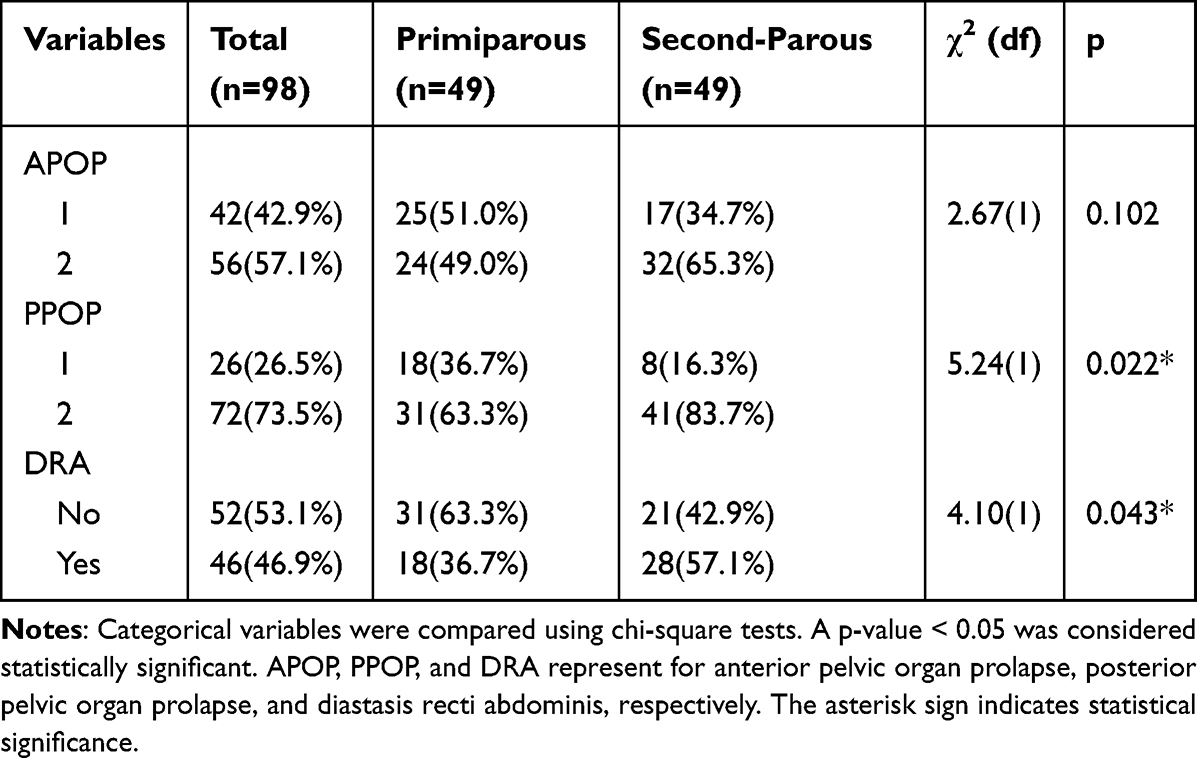 |
Table 3 The Analysis of Categorical Outcome Variables Between Primiparous and second-Parous Groups |
 |
Figure 1 The difference of inter-recti distance (IRD) between primiparous and second-parous groups. The grey and white violin plots represent IRD in primiparous and second-parous groups, respectively. The solid diamond represents the difference between the means of two groups, while the error bar indicates the standard deviation. Y-axis units are centimeters. |
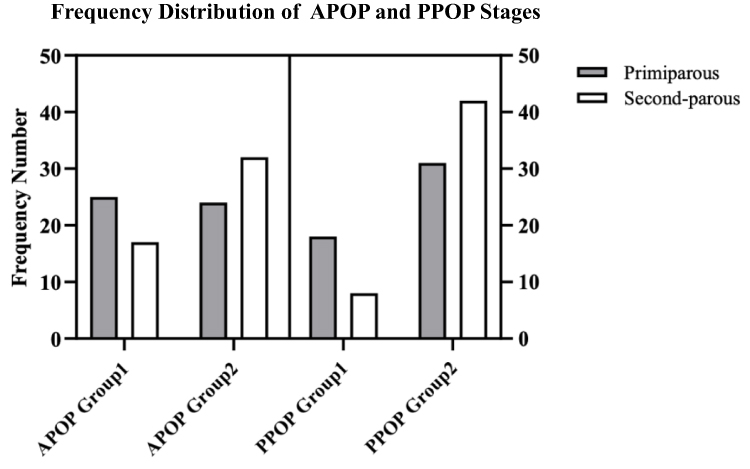 |
Figure 2 Frequency distribution of anterior (APOP) and pelvic organ prolapse (PPOP) groups between primiparous and second-parous population. Bar charts show the frequency distribution of APOP and PPOP groups. The grey and white bars represent primiparous and second-parous groups, respectively. |
Discussion
This study examined whether second-parous women are more likely to experience postpartum dysfunctions compared to primiparous women. Importantly, the age and delivery mode were controlled between these two groups. It was found that second-parous women have an increased risk of PPOP and a greater IRD than primiparous women. In spite of this, there was no significant difference between the two groups in terms of vaginal pressure.
The findings of this study align with previous studies indicating a strong association between parity and postpartum pelvic floor disorders.8,28,52 However, a notable distinction of this study is its reliance on objective assessments of pelvic floor dysfunction, as opposed to the subjective reports used in existing literature. Despite the focus on Chinese postpartum females, the results were consistent with studies conducted in Western countries,8,52 suggesting broad clinical relevance. This study also added a new dimension by isolating primiparous and second-parous groups aiming to differentiate the progression of pelvic floor dysfunction following each subsequent childbirth, a distinction not fully addressed by previous work. The findings have significant implications for future pelvic floor clinical practice, particularly for second-parous females. The study underscores the need for heightened medical awareness among healthcare providers regarding the increased risk of prolapse in the vaginal posterior compartment among this second-parous population. It suggested that tailored evaluations and interventions should be developed for this population. Additionally, future research could explore the progression or regression of posterior pelvic organ prolapse in multiparous groups following each childbirth, further informing pelvic floor rehabilitation practice.
Second-Parous Females Demonstrated Greater IRD Than Primiparous Females
As a major finding of this study, second-parous females demonstrated greater IRD, indicating higher incidence of DRA, than primiparous females. According to an epidemiological cohort study, there is a positive correlation between the number of pregnancies and IRD among Finnish women.53 It was worth noting that the average IRD in this previous study for primiparous and multiparous females were 2.36 ± 0.83 cm and 2.55 ± 1.09 cm respectively, which both were greater than the ones in our current findings. The level of statistical significance between primiparous and multiparous females was not reached in this previous study. Several rationales could be made. The first reason was the racial difference between the Finnish and Chinese populations. An IRD measurement conducted 3 cm above the umbilicus by Qu et al54 revealed that Chinese nulliparous females had an IRD of 0.62 ± 0.56 cm, whereas Beer et al55 reported a value of 1.30 ± 0.07 cm for nulliparous females from eastern countries at the same location. The second reason is that IRD measurement is not standardized. Previous studies measuring IRD used different locations as a reference, resulting in incompatibility between the results. Moreover, the focus of this previous study was on primiparous and multiparous females, but not on primiparous and second-parous females. Liaw et al56 also included multiparous women in their study and confirmed that parous females were capable of recovering their IRD from 7 weeks to 6 months but continued to have a significant greater IRD than nulliparous women; however, their study did not compare IRD between primiparous and multiparous women. Our study compared the difference in IRD between primiparous and second-parous females and confirmed that second-parous females demonstrated significantly larger IRD with a difference of 0.58 cm than primiparous females.
PPOP is More Popular Among second-Parous Females Than Primiparous Females, but APOP is More Popular Than PPOP Among Parous Females with More Severe Stages
According to the current study, PPOP was more commonly seen among second-parous women than primiparous women. Possibly, increased weight of vaginally delivered fetuses can be explained by a correlation between posterior prolapse and fetal weight,57,58 as shown by the fact that the second-parous group in the current study had a significantly greater fetal weight. Research has shown that increased fetal weight is associated with increased fetal head circumference,59 which may result in an overstretching of tissues in the posterior vaginal wall.60 Most pelvic floor muscles are only able to tolerate stretch to a certain extent due to the single-direction alignment of their fibers. Existing literature using finite element method has supported the above-mentioned hypotheses, revealing that a higher risk of pelvic floor muscle injury along with a corresponding PFD may be evident as soon as the permissible stretch reaches a certain level. For instance, Parente et al61 measured the stretches and deformations on pelvic floor muscles induced by the passage of the fetus during the vaginal delivery. The stretch ratio, defined as the ratio between the current tissue length to the original tissue length, is a key metric in assess tissue strain. Initial investigation into contraction-induced injury identified a maximal non-injurious stretch value of 1.5.62 The maximal stretch ratio obtained in this study was 1.63 for a vertical displacement of the fetal head of approximately 60 mm, which indicates a higher risk of pelvic floor muscle injury during the second stage of labor with larger fetal head circumferences at this vertical level. Thus, it is hypothesized that once the fetal weight or head circumference exceeds a certain number, the posterior vaginal wall will be traumatically overstretched, leading to PPOP.
It is somewhat of a surprise that we did not find significant difference in APOP stages between two groups, but only PPOP stages. However, the findings of our study are still consistent with previous research that APOP is more popular than PPOP in parous females with more severe stages.10,15 To date, no research has revealed why postpartum APOP is more commonly seen than PPOP. Yagi et al63 conducted magnetic resonance imaging evaluation on pelvic floor structures with 3 reference lines (pubo-coccygeal line, pubo-rectal line, and the M line) to determine their changes are linked to prolapse. Pubo-rectal line represents the distance from pubic symphysis to the most cranial portion of the posterior anal canal while the M line was defined as the vertical line from dorsal edge of the pubo-rectal line to pubo-coccygeal line, which represents the descent of the hiatus. The study results revealed that in comparison to non-POP population, POP patients are more likely to recover their lengthened pubo-rectal line, but not completely and accumulatively lengthen the M line with no recovery. Further research study may focus on investigating how pubo-rectal and the M lines differentiate between patients with APOP and PPOP to uncover the mechanism behind the different types of POP.
Neither VRP nor MVCP Were Found Significantly Different Between Two Groups
The current study found no significant difference in VRP and MVCP between two groups. To explain our findings, we speculated that the second-parous women had lower antepartum pressure values than primiparous women. With previous childbirth experiences, second-parous females showed faster body recovery and returned to their antepartum values within 3 months. Primiparous females, however, were only able to recover to the level of second-female antepartum status during this short period of time; thus, no difference in pressure values was detected in the current study. Our hypothesis was supported by a previous study conducted by Peschers et al,25 which determined that multiparous women already had lower antepartum pressure values than primiparous women. Moreover, multiparous females have already recovered to their antepartum vaginal pressure values 6 to 10 weeks postpartum, but no full recovery was observed among primiparous groups; however, no statistical analysis was conducted to determine the differences between the two groups. Another study from Bø et al27 also found that primiparous females did not fully recover to their pressure values even 12 months postpartum; however, no second- or multiparous females were included in this study and no follow-ups of these primiparous females to investigate their PFM strength and endurance changes during their subsequent pregnancies were conducted.
Limitations
The current study has some limitations. First of all, given its retrospective study design, the study is subject to selection bias. To reduce bias, we were able to control some potential confounders, including age and delivery mode. Another limitation of the current study is the small sample size. We have conducted a post-hoc power analysis and shown that the chi-square and independent t-tests have acceptable power with values of 0.98 and 0.99, respectively. In addition, this study relies on medical records of women who attended postpartum pelvic floor evaluations. These females may demonstrate greater health awareness or more severe symptoms, which could limit the generalizability of this study results and potentially overestimate the severity of pelvic floor dysfunction in the targeted group. Furthermore, this study only evaluates women within a short postpartum window (6–12 weeks postpartum). It is possible that their symptoms of PFD and DRA could continue to progress or regress over time. Therefore, future research could focus on a longer timeframe to capture the full extent of the long-term differences between primiparous and second-parous females in terms of PFM function. Additionally, due to the lack of medical records, this study cannot exclude second-parous females who may have undergone postnatal pelvic floor rehabilitation following their first childbirth. This highlights the need for future studies to account for prior rehabilitation history when examining the impact of parity on pelvic floor health. Lastly, due to the retrospective nature of the study design, this current study lacks pre-pregnancy or pre-delivery measurements of PFM strength and endurance, which are critical for assessing changes attributable to childbirth. A prospective longitudinal study would be recommended to track changes in PFM strength and endurance from pre-pregnancy through postpartum periods to allow for a clearer understanding of how childbirth and parity impact pelvic floor function over time.
Conclusion
This current retrospective cohort study supports the notion that second-parous females may be at greater risk of developing PPOP with increased IRD than primiparous females. There is a higher incidence of APOP among parous females than PPOP with more severe stages. There was no significant difference found in vaginal pressure values such as VRP and MVCP to detect pelvic floor muscle strength difference between primiparous and second-parous females.
Abbreviations
PFD, pelvic floor dysfunction; POP, pelvic organ prolapse; APOP, anterior pelvic organ prolapse; PPOP, posterior pelvic organ prolapse; DRA, diastasis recti abdominis; PFM, pelvic floor muscle; IRD, inter-recti distance; BMI, body mass index; GWG, gestational weight gain; VRP, vaginal resting pressure; MVCP, maximum voluntary contraction pressure; POP-Q, Pelvic Organ Prolapse Quantification System; PFDI, Pelvic Floor Distress Inventory; PFIQ-SF, Pelvic Floor Impact Questionnaire Short Form.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. The study has been approved by Peking Union Medical College Hospital Ethics Committee and the IRB number of this study is I-24PJ0428. Informed consent for study participation was obtained from all participants.
Acknowledgment
We thank all participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Our study was funded by National Key Research and Development Program of China (2021YFC2701300).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang B, Chen Y, Zhu X, et al. Global burden and trends of pelvic organ prolapse associated with aging women: an observational trend study from 1990 to 2019. 2023. (2296-2565 (Electronic)).
2. Zillioux J, Yeaman C, Desai R, Sharma D, Balkrishnan R, Rapp D. Economic impact of urinary incontinence and pelvic organ prolapse in women in Belize. IJS Global Health. 2023;6(5). doi:10.1097/GH9.0000000000000271
3. Bozkurt M, Yumru AE, Şahin L. Pelvic floor dysfunction, and effects of pregnancy and mode of delivery on pelvic floor. Taiwanese J Obstetrics Gynecol. 2014;53(4):452–458. (1875-6263 (Electronic)). doi:10.1016/j.tjog.2014.08.001
4. Peinado-Molina RA-O, Hernández-Martínez A, Martínez-Vázquez S, Rodríguez-Almagro J, Martínez-Galiano JM. Pelvic floor dysfunction: prevalence and associated factors. BMC Public Health. 2023;23(1). (1471-2458 (Electronic)). doi:10.1186/s12889-023-16901-3
5. Dheresa M, Worku A, Oljira L, Mengiste B, Assefa N, Berhane Y. One in five women suffer from pelvic floor disorders in Kersa district Eastern Ethiopia: a community-based study. BMC Women’s Health. 2018;18(1):95. doi:10.1186/s12905-018-0585-1
6. Sawai M, Yuno C, Shogenji MA-O, et al. Prevalence of symptoms of pelvic floor dysfunction and related factors among Japanese female healthcare workers. LUTS. 2022;14(5):380–386. (1757-5672 (Electronic)). doi:10.1111/luts.12455
7. Zhang L, Zhu L, Xu T, et al. A population-based survey of the prevalence, potential risk factors, and symptom-specific bother of lower urinary tract symptoms in adult Chinese women. 2015. (1873-7560 (Electronic)).
8. MacLennan AH, Taylor AW, Wilson DH, Wilson D. The prevalence of pelvic floor disorders and their relationship to gender, age, parity and mode of delivery. BJOG. 2000;107(12):1460–1470. doi:10.1111/j.1471-0528.2000.tb11669.x
9. Peinado Molina RA, Hernández Martínez A, Martínez Vázquez S, Martínez Galiano JM. Influence of pelvic floor disorders on quality of life in women. Front Public Health. 2023;11. (2296-2565 (Electronic)). doi:10.3389/fpubh.2023.1180907
10. Trutnovsky G, Kamisan Atan I, Martin A, Dietz HP. Delivery mode and pelvic organ prolapse: a retrospective observational study. BJOG. 2016;123(9):1551–1556. doi:10.1111/1471-0528.13692
11. Sigurdardottir TA-O, Bø K, Steingrimsdottir T, Halldorsson TI, Aspelund T, Geirsson RT. Cross-sectional study of early postpartum pelvic floor dysfunction and related bother in primiparous women 6-10 weeks postpartum. Int Urogynecol J. 2021;32(7):1847–1855. (1433-3023 (Electronic)). doi:10.1007/s00192-021-04813-y
12. Saucedo AM, Richter HE, Gregory WT, et al. Intrapartum risk factors associated with pelvic organ prolapse at 6 months postpartum. Am J Obstetrics Gynecol MFM. 2022;4(6):100692. (2589-9333 (Electronic)). doi:10.1016/j.ajogmf.2022.100692
13. Sun ZJ, Tian Z, Xu T, et al. Pelvic floor muscle strength and influencing factors based on vaginal manometry among healthy women at different life stages: a multicentre cross-sectional study. 2023. (1471-0528 (Electronic)). doi:10.1111/1471-0528.17736.
14. Driusso PA-O, Beleza ACS, Mira DM, et al. Are there differences in short-term pelvic floor muscle function after cesarean section or vaginal delivery in primiparous women? A systematic review with meta-analysis. 2019. (1433-3023 (Electronic)).
15. Hagovska M, Dudic R, Dudicova V, Svihra J, Urdzik P. Prevalence of diastasis m. rectus abdominis and pelvic floor muscle dysfunction in postpartum women. Bratislava Med J. 2023;125(01):12–16. (0006-9248 (Print)). doi:10.4149/BLL_2024_003
16. Braekken IH, Majida M, Ellström Engh M, Holme IM, Bø K. Pelvic floor function is independently associated with pelvic organ prolapse. BJOG. 2009;116(13):1706–1714. (1471-0528 (Electronic)). doi:10.1111/j.1471-0528.2009.02379.x
17. Persu C, Chapple CR, Cauni V, Gutue S, Geavlete P. Pelvic organ prolapse quantification system (POP-Q) - a new era in pelvic prolapse staging. Journal of Medicine and Life. 2011;4(1):75–81. (1844-122X (Print)).
18. Petronilla OC, Uruchi EA, Francis EC, Linda UC. Assessment of diastasis recti abdominis: clinimetric properties of four measuring instruments. Int J Health Sci. 2023;17(6):6–14. (1658-3639 (Print)).
19. Lemos NL, Auge AP, Lunardelli JL, Carramão S, Faria ALA, Aoki T. Validation of the Pelvic Organ Prolapse Quantification Index (POP-Q-I): a novel interpretation of the POP-Q system for optimization of POP research. Int Urogynecol J. 2008;19(7):995–997. doi:10.1007/s00192-007-0556-9
20. Rai A, Sharma N, Jain SK, Lalwani A, Sharma S. Accuracy and reliability of different approaches for the assessment of pelvic floor muscle strength: a systematic review. J Pharmacy Bioallied Sci. 2023;15(Suppl 2):S856–S861. (0976-4879 (Print)). doi:10.4103/jpbs.jpbs_241_23
21. Romero-Cullerés G, Jané-Feixas C, Vilaseca-Grané A, Arnau A, Montesinos J, Abenoza-Guardiola M. Inter-rater reliability of the digital palpation of pelvic floor muscle by the modified Oxford Grading Scale in continent and incontinent women. Fiabilidad inter evaluador de la palpación digital de los músculos del suelo pélvico utilizando la escala modificada de Oxford graduada en mujeres continentes e incontinentes. (0004-0614 (Print)).
22. Brækken IA-O, Stuge B, Tveter AT, Bø K. Reliability, validity and responsiveness of pelvic floor muscle surface electromyography and manometry. Int Urogynecol J. 2021;32(12):3267–3274. (1433-3023 (Electronic)). doi:10.1007/s00192-021-04881-0
23. Michalik DA-O, Herman UA-O, Stangel-Wojcikiewicz KA-O. Quantitative tools to assess pelvic floor muscle function - systematic review. Ginekologia Polska. 2024;95(9):718–728. (2543-6767 (Electronic)). doi:10.5603/gpl.90873
24. DeLancey JO, Kearney R, Chou Q, Speights S, Binno S. The appearance of levator ani muscle abnormalities in magnetic resonance images after vaginal delivery. 2003. (0029-7844 (Print)).
25. Peschers UM, Schaer GN, DeLancey JO, Schuessler B. Levator ani function before and after childbirth. (0306-5456 (Print)).
26. Grinbaum MA-O, Bianchi-Ferraro A, Rodrigues CA, Sartori MGF, Bella Z. Impact of parity and delivery mode on pelvic floor function in young women: a 3D ultrasound evaluation. Int Urogynecol J. 2023;34(8):1849–1858. (1433-3023 (Electronic)). doi:10.1007/s00192-022-05440-x
27. Bø KA-O, Næss K, Stær-Jensen J, Siafarikas F, Ellström Engh M, Hilde G. Recovery of pelvic floor muscle strength and endurance 6 and 12 months postpartum in primiparous women-a prospective cohort study. Int Urogynecol J. 2022;33(12):3455–3464. (1433-3023 (Electronic)). doi:10.1007/s00192-022-05334-y
28. Elenskaia K, Thakar R, Sultan AH, Scheer I, Beggs A. The effect of pregnancy and childbirth on pelvic floor muscle function. Int Urogynecol J. 2011;22(11):1421–1427. (1433-3023 (Electronic)). doi:10.1007/s00192-011-1501-5
29. Bø K, Kvarstein B, Hagen RR, Larsen S. Pelvic floor muscle exercise for the treatment of female stress urinary incontinence: II. Validity of vaginal pressure measurements of pelvic floor muscle strength and the necessity of supplementary methods for control of correct contraction. Neurourol Urodynamics. 1990;9(5):479–487. doi:10.1002/nau.1930090504
30. Zachovajeviene B, Siupsinskas L, Zachovajevas P, Venclovas Z, Milonas D. Effect of diaphragm and abdominal muscle training on pelvic floor strength and endurance: results of a prospective randomized trial. Scientific Reports. 2019;9(1). (2045-2322 (Electronic)). doi:10.1038/s41598-019-55724-4
31. Talasz H, Kremser C, Kofler M, Kalchschmid E, Lechleitner M, Rudisch A. Phase-locked parallel movement of diaphragm and pelvic floor during breathing and coughing-a dynamic MRI investigation in healthy females. Int Urogynecol J. 2011;22(1):61–68. (1433-3023 (Electronic)). doi:10.1007/s00192-010-1240-z
32. Neumann P, Gill V. Pelvic floor and abdominal muscle interaction: EMG activity and intra-abdominal pressure. 2001.
33. Talasz H, Kofler M, Kalchschmid E, Pretterklieber M, Lechleitner M. Breathing with the pelvic floor? Correlation of pelvic floor muscle function and expiratory flows in healthy young nulliparous women. Int Urogynecol J. 2010;21(4):475–481. (1433-3023 (Electronic)). doi:10.1007/s00192-009-1060-1
34. Zhang S, Fu F, Li W, Ding TA-O, Gu Y, Xie ZA-OX. Analysis of multisite surface electromyography characteristics of pelvic floor muscles in postpartum patients with diastasis recti abdominis. J Obstetrics Gynaecol Res. 2023;49(12):2938–2945. (1447-0756 (Electronic)). doi:10.1111/jog.15787
35. Bodner-Adler BA-O, Kimberger O, Laml T, et al. Prevalence and risk factors for pelvic floor disorders during early and late pregnancy in a cohort of Austrian women. Archiv Gynecol Obstetrics. 2019;300(5):1325–1330. (1432-0711 (Electronic)). doi:10.1007/s00404-019-05311-9
36. Handa VL, Blomquist JL, Knoepp LR, Hoskey KA, McDermott KC, Muñoz A. Pelvic floor disorders 5–10 years after vaginal or cesarean childbirth. Obstetrics Gynecol. 2011;118(4):777–784. doi:10.1097/AOG.0b013e3182267f2f
37. Tucker J, Grzeskowiak L, Murphy EM, Wilson A, Clifton VL. Do women of reproductive age presenting with pelvic floor dysfunction have undisclosed anal incontinence: a retrospective cohort study. Women Birth. 2017;30(1):18–22. (1878-1799 (Electronic)). doi:10.1016/j.wombi.2016.05.009
38. Söderberg MW, Byström B, Kalamajski S, Malmström A, Ekman-Ordeberg G. Gene expressions of small leucine-rich repeat proteoglycans and fibulin-5 are decreased in pelvic organ prolapse. Mol Human Reproduction. 2009;15(4):251–257. (1460-2407 (Electronic)). doi:10.1093/molehr/gap011
39. Glick I, Kadish EA-O, Rottenstreich MA-O. Management of pregnancy in women of advanced maternal age: improving outcomes for mother and baby. Int J Women’s Health. 2021;Volume 13:751–759. (1179-1411 (Print)). doi:10.2147/IJWH.S283216
40. Cattani LA-O, Neefs L, Verbakel JY, Bosteels J, Deprest JA-OX. Obstetric risk factors for anorectal dysfunction after delivery: a systematic review and meta-analysis. Int Urogynecol J. 2021;32(9):2325–2336. (1433-3023 (Electronic)). doi:10.1007/s00192-021-04723-z
41. Koc O, Duran B, Ozdemırcı S, Bakar Y, Ozengin N. Is cesarean section a real panacea to prevent pelvic organ disorders? Int Urogynecol J. 2011;22(9):1135–1141. (1433-3023 (Electronic)). doi:10.1007/s00192-011-1457-5
42. Bortolini MA, Drutz Hp Fau - Lovatsis D, Lovatsis D, Fau - Alarab M, Alarab M. Vaginal delivery and pelvic floor dysfunction: current evidence and implications for future research. Int Urogynecol J. 2010;21(8):1025–1030. (1433-3023 (Electronic)). doi:10.1007/s00192-010-1146-9
43. Memon H, Handa VL. Pelvic floor disorders following vaginal or cesarean delivery. Curr Opinion Obstetrics Gynecol. 2012;24(5):349–354. (1473-656X (Electronic)). doi:10.1097/GCO.0b013e328357628b
44. Dietz HP, Lanzarone V. Levator trauma after vaginal delivery. Obstetrics Gynecol. 2005;106(4):707–712. (0029-7844 (Print)). doi:10.1097/01.AOG.0000178779.62181.01
45. Blomquist JL, Muñoz A, Carroll M, Handa VL. Association of delivery mode with pelvic floor disorders after childbirth. JAMA. 2018;320(23):2438. (1538-3598 (Electronic)). doi:10.1001/jama.2018.18315
46. Bo K, Frawley HC, Haylen BT, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Neurourol Urodynamics. 2017;36(2):221–244. doi:10.1002/nau.23107
47. Frawley HA-O, Shelly B, Morin MA-O, et al. An international continence society (ICS) report on the terminology for pelvic floor muscle assessment. Neurourol Urodynamics. 2021;40(5):1217–1260. (1520-6777 (Electronic)). doi:10.1002/nau.24658
48. Maurice Nahabedian M, David C, Brooks M. Rectus abdominis diastasis. Available from: http://update.0000.tsg211.com/contents/rectus-abdominis-diastasis?search=Rectus%20abdominis%20diastasis&source=search_result&selectedTitle=1~17&usage_type=default&display_rank=1.
49. Rortveit G, Daltveit AK, Hannestad YS, Hunskaar S. Urinary incontinence after vaginal delivery or cesarean section. (1533-4406 (Electronic)).
50. Handa VL, Blomquist J, McDermott KC, Friedman S, Muñoz A. Pelvic floor disorders after vaginal birth: effect of episiotomy, perineal laceration, and operative birth. (1873-233X (Electronic)).
51. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J. 2007;18(3):321–328. doi:10.1007/s00192-006-0143-5
52. Kepenekci I, Keskinkilic B, Akinsu F, et al. Prevalence of pelvic floor disorders in the female population and the impact of age, mode of delivery, and parity. Dis Colon Rectum. 2011;54(1):85–94. (1530-0358 (Electronic)). doi:10.1007/DCR.0b013e3181fd2356
53. Tuominen RA-O, Jahkola TA-OX, Saisto TA-O, Arokoski JA-O, Vironen JA-O. The prevalence and consequences of abdominal rectus muscle diastasis among Finnish women: an epidemiological cohort study. Hernia. 2022;26(2):599–608. (1248-9204 (Electronic)). doi:10.1007/s10029-021-02484-8
54. Qu E, Wu J, Zhang M, et al. The ultrasound diagnostic criteria for diastasis recti and its correlation with pelvic floor dysfunction in early postpartum women. Quantitative Imag Med Surg. 2021;11(2):706–713. (2223-4292 (Print)). doi:10.21037/qims-20-596
55. Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clinical Anatomy. 2009;22(6):706–711. (1098-2353 (Electronic)). doi:10.1002/ca.20836
56. Liaw LJ, Hsu MJ, Liao C-F, Liu M-F, Hsu AT. The relationships between inter-recti distance measured by ultrasound imaging and abdominal muscle function in postpartum women: a 6-month follow-up study. J Orthopaedic Sports Phys Ther. 2011;41(6):435–443. (1938-1344 (Electronic)). doi:10.2519/jospt.2011.3507
57. Guzmán Rojas R, Quintero C, Shek KL, Dietz HP, Dietz HP. Does childbirth play a role in the etiology of rectocele? Int Urogynecol J. 2015;26(5):737–741. (1433-3023 (Electronic)). doi:10.1007/s00192-014-2560-1
58. Dietz HA-O, Gómez M, Atan IK, Ferreira CSW. Association between vaginal parity and rectocele. Int Urogynecol J. 2018;29(10):1479–1483. (1433-3023 (Electronic)). doi:10.1007/s00192-017-3552-8
59. Lipschuetz M, Cohen SM, Israel A, et al. Sonographic large fetal head circumference and risk of cesarean delivery. Am J Obstetrics Gynecol. 2018;218(3):
60. Parente MP, Jorge RM, Mascarenhas T, Fernandes AA, Martins JA. Deformation of the pelvic floor muscles during a vaginal delivery. Int Urogynecol J. 2007;19(1):65–71. doi:10.1007/s00192-007-0388-7
61. Martins JA, Pato MP, Pires EB, Jorge RMN, Parente M, Mascarenhas T. Finite element studies of the deformation of the pelvic floor. (0077-8923 (Print)).
62. Lien KC, Mooney B, DeLancey JO, Ashton-Miller JA, Ashton-Miller JA. Levator ani muscle stretch induced by simulated vaginal birth. Obstetrics Gynecol. 2004;103(1):31–40. (0029-7844 (Print)). doi:10.1097/01.AOG.0000109207.22354.65
63. Yagi T, Kodama M, Bun M, et al. Magnetic resonance imaging evaluation of pelvic floor structure during pregnancy. European J Obstetrics Gynecol Reproductive Biol. 2021;264:289–293. (1872-7654 (Electronic)). doi:10.1016/j.ejogrb.2021.07.045
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Patient-Reported Outcomes in Chinese Women with Postpartum Diastasis Recti Abdominis: An Observational Study
Zhu Y, Jiang L, Ye T, Liu Y, Sun L, Xiao L, Chen J, Wang T, Ren Y, Xu H, Zhao H, Mao X, Shen T
International Journal of Women's Health 2024, 16:179-192
Published Date: 31 January 2024