Back to Journals » Open Access Emergency Medicine » Volume 10
Differences in implementation strategies of the European Resuscitation Council Guidelines 2015 in Danish hospitals – a nationwide study
Authors Stærk M ![]() , Lauridsen KG, Mygind-Klausen T, Løfgren B
, Lauridsen KG, Mygind-Klausen T, Løfgren B ![]()
Received 16 April 2018
Accepted for publication 21 June 2018
Published 2 October 2018 Volume 2018:10 Pages 123—128
DOI https://doi.org/10.2147/OAEM.S171250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Mathilde Stærk,1–3 Kasper G Lauridsen,1–3 Troels Mygind-Klausen,1–3 Bo Løfgren2–5
1Clinical Research Unit, Randers Regional Hospital, Randers, Denmark; 2Research Center for Emergency Medicine, Aarhus University Hospital, Aarhus, Denmark; 3Department of Internal Medicine, Randers Regional Hospital, Randers, Denmark; 4Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 5Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark
Introduction: Guideline implementation is essential to improve survival following cardiac arrest. This study aimed to investigate awareness, expected time frame, and strategy for implementation of the European Resuscitation Council (ERC) Guidelines 2015 in Danish hospitals.
Methods: All public, somatic hospitals with a cardiac arrest team in Denmark were included. A questionnaire was sent to hospital resuscitation committees one week after guideline publication. The questionnaire included questions on awareness of ERC Guidelines 2015 and time frame and strategy for implementation.
Results: In total, 41 hospitals replied (response rate: 87%) between October 22 and December 22, 2015. Overall, 37% hospital resuscitation committees (n=15) were unaware of the guideline content. Most hospitals (80%, n=33) expected completion of guideline implementation within 6 months and 93% hospitals (n=38) expected the staff to act according to the ERC Guidelines 2015 within 6 months. In contrast, 78% hospitals (n=32) expected it would take between 6 months to 3 years for all staff to have completed a resuscitation course based on ERC Guidelines 2015. Overall, 29% hospitals (n=12) planned to have a strategy for implementation later than a month after guideline publication and 10% (n=4) hospitals did not plan to make a strategy.
Conclusion: There are major differences in guideline implementation strategies among Danish hospitals. Many hospital resuscitation committees were unaware of guideline content. Most hospitals expected hospital staff to follow ERC Guidelines 2015 within six months after the publication even though they did not offer information or skill training to all staff members within that time frame.
Keywords: resuscitation, guidelines, implementation
Introduction
Implementation of resuscitation guidelines is emphasized as a key factor to improve survival after cardiac arrest.1 Adherence to guidelines is associated with improved survival following in-hospital cardiac arrest.2 Moreover, implementing resuscitation guidelines is known to increase survival after out-of-hospital cardiac arrest.3,4
Several barriers for guideline implementation exist, eg, scheduling training, upgrading equipment, and decision-making processes.5,6 Studies report that implementation of guidelines in emergency medical services lasts up to 1.5 years.7,8 Likewise, there were limited implementation of resuscitation guidelines in hospital protocols more than two years after guideline publication.9 The International Liaison Committee on Resuscitation (ILCOR) states that guideline implementation cannot be effective without a discussion of how to implement the guidelines.10 However, it is unknown how hospitals plan to implement resuscitation guidelines.
This study aims to investigate awareness, expected time frame, and strategy for implementation of the European Resuscitation Council (ERC) Guidelines 2015 in Danish hospitals.
Methods
Study design
This nationwide cross-sectional study included all public somatic hospitals in Denmark with a cardiac arrest team. Hospitals serving outpatients only were excluded. All Danish hospitals are under administration of five Danish regions. Each Danish Region was contacted for a verified list of hospitals. Hospital administrations were contacted to obtain information on 1) whether the hospital had a cardiac arrest team, and 2) contact information on the hospital resuscitation committee. A structured questionnaire was emailed to the hospital resuscitation committee.
Questionnaire
The questionnaire inquired information on 1) awareness of ERC Guidelines 2015, 2) strategy and time frame to implement the guidelines, 3) attitude toward guideline implementation, and 4) implementation of the ERC Guidelines 2010. Awareness and methods for implementation were dichotomously assessed (yes/no). Time frame was assessed using predefined time intervals and attitude toward the guideline implementation was assessed using five-point Likert scale.
Data collection
The questionnaire was emailed on October 22, 2015, one week after the ERC Guidelines 2015 publication. If hospitals did not respond, a reminder email was sent after one, two, and eight weeks. Further, hospitals were contacted by telephone after four, six, nine, and eleven weeks as a reminder to complete the questionnaire. Respondents were offered a gift certificate of DKK 100 (€ 13.5) for completing the questionnaire.
Guideline release in Denmark
The ERC released their 2015 guidelines on October 15, 2015. Simultaneously, the Danish Resuscitation Council endorsed the guidelines and released action cards/pocket folders in Danish based on the new guidelines. Within weeks of guideline publication, two open meetings were held to inform about the content of the new guidelines. During the following months, a short summary of important guideline changes was released in Danish.
Ethics
In conformity with the Danish National Committee on Biomedical Research Ethics, no ethical review committee approval was required.
Data analysis
Categorical data are presented as number (percentage). Data were analyzed using statistical software package R version 3.2.1 (R Core Team, Vienna, Austria). No statistical tests were conducted.
Results
In total, 47 hospitals were eligible for inclusion; four hospitals (9%) denied participating and two hospitals (4%) did not answer the questionnaire. Accordingly, 41 hospitals (87%) answered the questionnaire (complete n=38, incomplete n=3). Respondents were chairman of the hospital resuscitation committee (n=31, 76%), a member of the resuscitation committee (n=5, 12%), or stated other function (n=5, 12%). All respondents were key figures in guideline implementation at the hospital. Questionnaires were answered between October 22 and December 22, 2015.
All hospital resuscitation committees were aware of the ERC Guidelines 2015 publication but 15 hospital resuscitation committees (37%) were not aware of the overall content of the guidelines. Overall, 31 hospitals (76%) did not inform hospital staff about upcoming guideline publication, eight hospitals (20%) did not intent to inform hospital staff about guideline publication at all, and two hospitals (5%) did not plan to inform hospital staff about the content of the ERC Guidelines 2015. In total, seven hospitals (17%) would inform hospital staff about the content within one month, and 32 hospitals (78%) would inform hospital staff later than one month after publication.
Overall, 33 hospitals (80%) expected to complete implementation of the ERC Guidelines 2015 within 6 months compared with seven hospitals (18%) completing implementation of ERC Guidelines 2010 within 6 months (Figure 1). Twenty hospitals (49%) had allocated staff hours to implement the guidelines. No hospitals had allocated financial resources. The majority of hospitals expected hospital staff to act according to the ERC Guidelines 2015 within 6 months (Figure 2). In contrast, most hospitals expected hospital staff to have completed a resuscitation course based on ERC Guidelines 2015 between 6 months to 3 years after guideline publication (Figure 2). Overall, three hospitals (7%) found the new guidelines to contain clinically important changes. Furthermore, three hospitals (7%) disagreed that it was important to implement the ERC Guidelines 2015.
 | Figure 1 Expected time of completion of the ERC Guidelines 2015 implementation (black) and completion of the ERC Guidelines 2010 implementation (gray). Notes: Time started at publication of guidelines. aAnswers only provided for implementation of ERC Guidelines 2015. Abbreviation: ERC, European Resuscitation Council. |
 | Figure 2 Time after publication for clinical hospital staff expected to act according to the ERC Guidelines 2015 (black) compared with time after publication for all clinical hospital staff to have completed resuscitation courses based on the ERC Guidelines 2015 (gray). Abbreviation: ERC, European Resuscitation Council. |
Hospitals used various methods for implementation of ERC 2015 and 2010 guidelines (Table 1). Further, five hospitals (13%) planned to use skill stations, workshops, or would arrange a “café” as part of their implementation of the ERC Guidelines 2015. Overall, 22 hospitals (54%) planned to have a strategy prior to or within one month of guideline publication, 12 hospitals (29%) expected to have a strategy later than a month after publication, and four hospitals (10%) did not plan to make a strategy for implementing the guidelines.
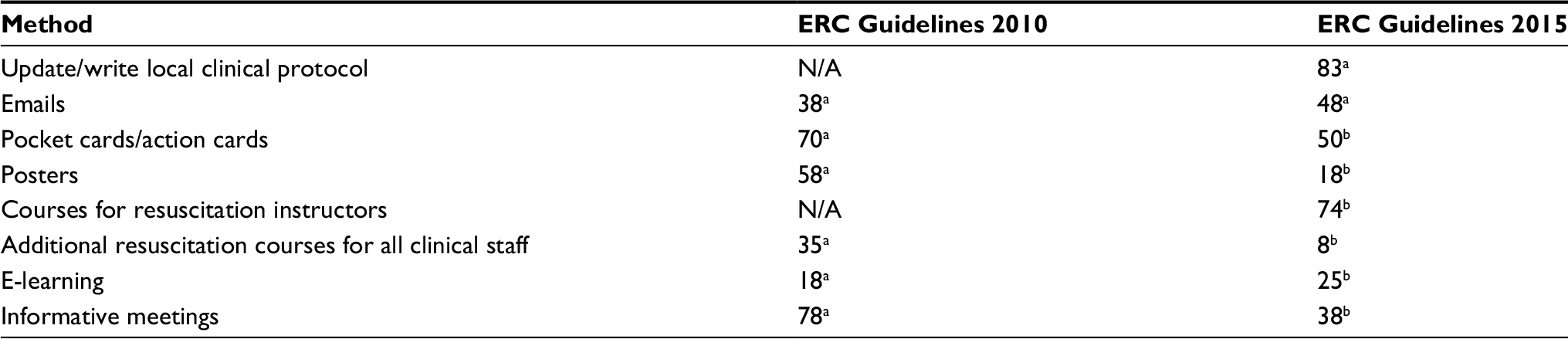 | Table 1 Methods used for the 2010 and 2015 ERC guideline implementation Notes: Data presented as percentages of hospitals. aData missing for one hospital. bData missing for three hospitals. Two hospitals did not know which methods were used for 2010 guideline implementation. Abbreviations: ERC, European Resuscitation Council; N/A, not available. |
Discussion
This nationwide study found that more than a third of resuscitation committees were not aware of the content in the new guidelines. The majority of hospitals expected swift guideline implementation but did not inform or train hospital staff in the guideline changes. Implementation strategies and methods varied among Danish hospitals.
Despite hospitals being aware of the publication of the ERC Guidelines 2015, more than a third of hospitals did not know the guideline content when answering the questionnaire. Studies suggest that local opinion leaders are important when implementing guidelines.11,12 Therefore, it may be crucial that resuscitation committees know the guideline content and stress the importance of guidelines adherence to hospital staff. Delayed awareness of new guidelines and lack of informative meetings for all clinical staff may be critical for implementation. Studies found increased survival following out-of-hospital cardiac arrest after implementation of guidelines,3,4 and it is implied that the increase in survival following guideline publication is due to awareness and education.13 Information about new guidelines shortly after publication to increase awareness may therefore be essential to improve survival following cardiac arrest. In our study, most hospitals expected to complete guideline implementation within six months but only half of hospitals allocated resources to implementation. Staff hours were the only resource allocated. Lack of resources is a known barrier when implementing guidelines.6 The Resuscitation Council (UK) recommends one full-time-equivalent resuscitation officer per 750 clinical hospital staff members in order to fulfill the responsibilities related to resuscitation.14
Importantly, hospital staff was not expected to have completed resuscitation training before up to three years after guideline publication. This is in major contrast to the statement that hospital staff should follow guidelines within six months. Education is known to be an important part of implementation.5,7 Thus, offering additional resuscitation training or skill stations may be important to facilitate faster implementation. Hospitals stated that the implementation of ERC Guidelines 2010 was completed for the majority of hospitals between 1 and 2 years after publication. This is in accordance with previous findings showing limited implementation and knowledge of the ERC Guidelines 2005 and 2010.9,15 The discrepancy between expected completion of ERC Guidelines 2015 implementation and prior findings may be due to the relatively few clinical changes in the ERC Guidelines 2015 compared with previous guidelines. However, the vast majority of hospitals still believe it is important to implement the new guidelines. Based on these findings, the hospitals’ expectation of the 2015 guideline implementation being completed within 6 months may be considered an optimistic vision.
Hospitals mainly planned to use passive methods to disseminate the 2015 guidelines (eg, printed material and meetings). However, studies show that active methods are more effective than passive methods when implementing guidelines.12,16–19 Where passive methods are merely a one-way directed method, eg, didactic lectures and printed educational material, active approaches can be two-way and include an interactive participation by the hospital staff. Examples of active implementation methods that have been shown to be effective are interactive workshops, educational outreach, and audit and feedback.11,12,17–21 A few Danish hospitals did plan to use active methods in the form of, eg, skill stations and workshops, but it is unknown if this has resulted in faster implementation of the guidelines compared with the hospitals not using active methods. Multifaceted strategies have also been implied to have a larger effect than single intervention strategies.12,17–19,21 Multifaceted strategies can consist of both passive and active methods, eg, educational material and feedback. A correlation between the number of combined methods in a multifaceted strategy and the effectiveness has although not been found.20
The methods used for implementing the ERC Guidelines 2010 varied from the methods planned for the implementation in 2015. One notable difference is the use of extra resuscitation courses for all clinical hospital staff, which decreased from 35% in 2010 to only 8% in 2015. Resuscitation courses are an active method to implement guidelines and could facilitate implementation. However, extra resuscitation courses for all clinical hospital staff demand resources to conduct, which had not been allocated at many hospitals. Besides being a resource demanding method, resuscitation courses may have been omitted because hospitals did not consider the ERC Guidelines 2015 to contain important clinical changes and therefore not being significant enough to justify spending many resources on implementing.
Even though, active approaches can be expensive to conduct, whereas most passive approaches are affordable and easier to use,12,17,20 using active methods may ease and shorten time of implementation. This can hopefully lead to optimized patient care that can compensate for a more expensive implementation at a later point.
Besides mainly using passive methods for implementing the ERC Guidelines 2015, Danish hospitals also delayed their implementation strategies. About half of the hospitals did not have a strategy for guideline implementation within one month after guideline publication and 10% did not find a strategy necessary. Studies suggest that one of the first elements in implementation should be an implementation strategy.11,16 The lack hereof by Danish hospitals may jeopardize guideline implementation.
To ensure an effective implementation of future resuscitation guidelines, all hospitals should plan a strategy for implementing the guidelines and allocate resources. In order to keep the implementation period to a minimum, it is important that hospitals become aware of the content of guidelines at an early stage and that hospitals use active approaches to implement the guidelines, eg, the use of workshops and skill stations, as well as considering which methods hospital staff prefers. In order to improve survival, it is essential to increase awareness of new guidelines by informing, educating, and reminding hospital staff about the new guidelines.
Recently, ILCOR has changed the five year evidence review to a continuous evaluation process and correspondingly continuous publication of guidelines.22 The changing face of resuscitation guidelines additionally challenges implementation. Hence, implementation science in resuscitation becomes more relevant than ever.
Limitations
This study used online questionnaires. Therefore, we cannot infer on actual implementation or change in behavior. A part of the questionnaire considered the implementation of ERC Guidelines 2010. This may have led to recall bias.
Conclusion
There are major differences in guideline implementation strategies among Danish hospitals. Many hospital resuscitation committees were unaware of guideline content. Most hospitals expected hospital staff to follow ERC Guidelines 2015 within six months after the publication even though they did not offer information or skill training to all staff members within that time frame.
Acknowledgment
We thank all hospitals participating in the study. Gift certificates were paid by the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
Søreide E, Morrison L, Hillman K, et al. The formula for survival in resuscitation. Resuscitation. 2013;84(11):1487–1493. | ||
Anderson ML, Nichol G, Dai D, et al. Association between hospital process composite performance and patient outcomes after in-hospital cardiac arrest care. J Am Med Assoc Cardiol. 2016;1(1):37. | ||
Aufderheide TP, Yannopoulos D, Lick CJ, et al. Implementing the 2005 American Heart Association Guidelines improves outcomes after out-of-hospital cardiac arrest. Heart Rhythm. 2010;7(10):1357–1362. | ||
Steinmetz J, Barnung S, Nielsen SL, Risom M, Rasmussen LS. Improved survival after an out-of-hospital cardiac arrest using new guidelines. Acta Anaesthesiol Scand. 2008;52(7):908–913. | ||
Bigham BL, Aufderheide TP, Davis DP, et al. Knowledge translation in emergency medical services: a qualitative survey of barriers to guideline implementation. Resuscitation. 2010;81(7):836–840. | ||
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. J Am Med Assoc. 1999;282(15):1458–1465. | ||
Berdowski J, Schmohl A, Tijssen JG, Koster RW. Time needed for a regional emergency medical system to implement resuscitation Guidelines 2005--The Netherlands experience. Resuscitation. 2009;80(12):1336–1341. | ||
Bigham BL, Koprowicz K, Aufderheide TP, et al. Delayed prehospital implementation of the 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiac care. Prehosp Emerg Care. 2010;14(3):355–360. | ||
Schmidt AS, Lauridsen KG, Adelborg K, Løfgren B. Hospital implementation of resuscitation guidelines and review of CPR training programmes: a nationwide study. Eur J Emerg Med. 2016;23(3):232–234. | ||
Finn JC, Bhanji F, Lockey A, et al. Part 8: Education, implementation, and teams: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2015;95:e203–e224. | ||
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–1230. | ||
Grimshaw JM, Eccles MP, Walker AE, Thomas RE. Changing physicians’ behavior: what works and thoughts on getting more things to work. J Contin Educ Health Prof. 2002;22(4):237–243. | ||
Ageron FX, Debaty G. Survival is surfing on the guidelines wave. Resuscitation. 2016;98:e2–e3. | ||
Resuscitation Council (UK). Quality standards for cardiopulmonary resuscitation practice and training. London: Resuscitation Council (UK); 2013. Available from: https://www.resus.org.uk/quality-standards/acute-care-quality-standards-for-cpr/. Accessed March 21, 2015. | ||
Nielsen AM, Isbye DL, Lippert FK. Have the 2005 guidelines for resuscitation been implemented? Ugeskr Laeger. 2008;170(47):3843– 3847. | ||
Unverzagt S, Oemler M, Braun K, Klement A. Strategies for guideline implementation in primary care focusing on patients with cardiovascular disease: a systematic review. Fam Pract. 2014;31(3):247–266. | ||
Prior M, Guerin M, Grimmer-Somers K. The effectiveness of clinical guideline implementation strategies--a synthesis of systematic review findings. J Eval Clin Pract. 2008;14(5):888–897. | ||
Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thomson MA. Closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings. The Cochrane Effective Practice and Organization of Care Review Group. BMJ. 1998;317(7156):465–468. | ||
Brusamento S, Legido-Quigley H, Panteli D, et al. Assessing the effectiveness of strategies to implement clinical guidelines for the management of chronic diseases at primary care level in EU Member States: a systematic review. Health Policy. 2012;107(2–3):168–183. | ||
Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE. Knowledge translation of research findings. Implement Sci. 2012;7:50. | ||
Chan WV, Pearson TA, Bennett GC, et al. ACC/AHA Special Report: Clinical Practice Guideline Implementation Strategies: A Summary of Systematic Reviews by the NHLBI Implementation Science Work Group: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135(9):e122–e137. | ||
Morley PT. Towards a more continuous evidence evaluation: a collaborative approach to review the resuscitation science. Resuscitation. 2017;118:A1–A2. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.