Back to Journals » Clinical Interventions in Aging » Volume 20
Diagnostic Value of Two-Dimensional Speckle Tracking Echocardiography in Assessing Cardiac Function in Elderly Patients with Hypertensive Heart Disease
Authors Guo JN, Zhou QY, Peng XX, Li X, Yang RX
Received 4 July 2025
Accepted for publication 13 November 2025
Published 3 December 2025 Volume 2025:20 Pages 2377—2387
DOI https://doi.org/10.2147/CIA.S551673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Jian-Nan Guo,1 Qiu-Yan Zhou,2 Xiao-Xing Peng,3 Xin Li,1 Rui-Xue Yang1
1Department of Electro-Diagnosis, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun City, Jilin Province, 130021, People’s Republic of China; 2Department of Lung Disease, Tumor and Blood Center, Lung Oncology, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun City, Jilin Province, 130021, People’s Republic of China; 3Department of Medical Imaging, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun City, Jilin Province, 130021, People’s Republic of China
Correspondence: Jian-Nan Guo, Department of Electro-diagnosis, Affiliated Hospital of Changchun University of Chinese Medicine, No. 1475 Gongnong Road, Chaoyang District, Changchun City, Jilin Province, 130021, People’s Republic of China, Email [email protected]
Background: Hypertensive heart disease (HHD) in older adults is characterized by structural remodeling and subtle functional impairment that may escape conventional echocardiography. This study aimed to determine the diagnostic value of two-dimensional speckle tracking echocardiography (2D-STE)–derived left atrial strain rates for functional assessment in elderly patients with HHD.
Methods: In this retrospective, single-center cohort, 236 patients aged ≥ 65 years were enrolled (January 2023–January 2025): 118 with echocardiographic HHD and 118 age-matched hypertensive controls without structural abnormalities. Transthoracic echocardiography with 2D-STE quantified mean peak left atrial strain rates in late diastole (mSRa), early diastole (mSRe), and systole (mSRs). Elderly HHD patients were stratified by New York Heart Association (NYHA) class. Group comparisons used t-tests, and receiver operating characteristic (ROC) curves with area under the curve (AUC) evaluated discrimination.
Results: Compared with controls, the HHD group had larger left ventricular end-diastolic diameter (LVEDD 60.29 ± 5.26 vs 48.17 ± 5.46 mm; P< 0.001), lower left ventricular ejection fraction (LVEF 51.10 ± 7.25% vs 61.21 ± 4.96%; P< 0.001), and impaired atrial mechanics (mSRa − 2.20 ± 0.27 vs − 2.75 ± 0.30 s−1; P< 0.001; mSRe − 2.29 ± 0.33 vs − 1.90 ± 0.38 s−1; P< 0.001; mSRs 1.34 ± 0.30 vs 2.15 ± 0.31 s−1; P< 0.001). Within HHD, NYHA III–IV showed worse strain than NYHA I–II (eg, mSRa − 1.90 ± 0.26 vs − 2.48 ± 0.23 s−1; P< 0.001). ROC analysis demonstrated excellent discrimination of functional severity: AUC 0.916 for mSRa (cut-off − 2.367 s−1; sensitivity 96.8%; specificity 76.7%), AUC 0.876 for mSRe (− 2.302 s−1; 91.6%; 65.0%), and AUC 0.881 for mSRs (1.361 s−1; 92.5%; 68.7%) (all P< 0.001).
Conclusion: In elderly HHD, 2D-STE–derived atrial strain rates (mSRa, mSRe, mSRs) are significantly impaired, correlate with NYHA class, and provide high diagnostic accuracy for differentiating mild versus severe functional limitation. These indices may serve as sensitive, non-invasive markers to support early detection and clinical stratification in this population. Prospective studies are needed to establish prognostic utility.
Keywords: two-dimensional speckle tracking echocardiography, hypertensive heart disease, atrial strain, mSRa, mSRe, mSRs, elderly patients, ROC analysis
Introduction
Hypertensive heart disease (HHD) encompasses a continuum of structural and functional cardiac alterations secondary to chronic arterial hypertension, including left ventricular hypertrophy (LVH), diastolic dysfunction, left atrial enlargement, and eventually systolic heart failure and arrhythmias.1,2 As hypertension disproportionately affects the elderly and remains a leading contributor to cardiovascular morbidity and mortality worldwide, the burden of HHD is particularly significant in older populations. Age-related myocardial fibrosis, vascular stiffness, and impaired diastolic reserve further exacerbate hypertensive cardiac remodeling in the elderly, making early detection of functional impairment both challenging and essential.3–5
Conventional echocardiographic parameters, including left ventricular ejection fraction (LVEF), left ventricular mass index (LVMI), and left atrial diameter, are routinely used to assess cardiac structure and function. However, these indices often remain within normal ranges in early-stage HHD, especially in elderly patients with preserved systolic function, thereby limiting their sensitivity for identifying subclinical myocardial dysfunction.6,7 Two-dimensional speckle tracking echocardiography (2D-STE) offers a non-invasive, angle-independent technique to evaluate myocardial deformation.8 While global longitudinal strain (GLS) has been widely validated as an early marker of left ventricular dysfunction, recent studies underscore the added diagnostic value of atrial strain parameters in hypertensive populations.9,10 In particular, left atrial strain has shown promise in detecting impaired diastolic function and increased filling pressures before overt symptoms develop. Recent studies have shown that left atrial strain, particularly during systole and diastole, is closely associated with elevated left ventricular filling pressure and adverse outcomes in hypertensive patients, even when conventional parameters remain within normal ranges.11,12 For instance, reduced atrial strain has been linked to symptom burden, impaired functional class, and increased hospitalization risk in patients with preserved LVEF.13 Accordingly, 2D-STE provides a valuable tool for early detection of myocardial impairment in hypertensive patients, supporting timely risk stratification and guiding the implementation of intensified antihypertensive and cardioprotective therapies.14–16
However, despite the growing body of evidence linking left atrial strain to hypertension-related cardiac dysfunction, few studies have specifically examined its diagnostic performance in elderly patients with confirmed HHD.17,18 Most prior investigations have focused on early hypertension, preserved LVEF, or general hypertensive populations without stratified analysis by functional class. Moreover, the relationship between atrial strain parameters and New York Heart Association (NYHA) functional classification remains underexplored in this population.19 To address this gap, the present study aimed to evaluate the diagnostic value of 2D-STE–derived left atrial strain rates in elderly patients with HHD. We sought to determine the association between strain indices and NYHA functional status, and to quantify their ability to discriminate functional severity using ROC analysis. This may support the use of atrial strain as a sensitive, non-invasive tool for early risk stratification and clinical decision-making in older adults with hypertensive heart disease.
Methods
Study Design
This retrospective observational study included patients diagnosed with hypertension who received treatment at our institution between January 2023 and January 2025. All clinical and echocardiographic data were retrieved from the institutional electronic medical record system and echocardiography database. For each potentially eligible case, demographic characteristics (age, sex, body mass index), blood pressure records, laboratory results, and echocardiographic measurements were extracted. A total of 236 patients were ultimately enrolled in the study. Among them, 118 elderly patients with confirmed hypertensive heart disease comprised the HHD group, while 118 age- and sex-matched patients with essential hypertension but without echocardiographic features of HHD served as the hypertension control group. Informed consent was obtained from all subjects. The study protocol was reviewed and approved by the hospital’s ethics committee. All procedures complied with relevant regulations and the ethical principles outlined in the Declaration of Helsinki. Participant data were anonymized before analysis to ensure confidentiality and protect privacy.
Eligibility and Exclusion Criteria
Eligibility Criteria
(1) Age ≥ 65 years.
(2) Echocardiographic evidence of HHD, defined as the presence of at least one of the following (in the absence of other structural cardiac abnormalities), according to the 2016 American Society of Echocardiography (ASE) and American College of Cardiology (ACC) guidelines:
a. LVH: LV mass index ≥115 g/m2 for men or ≥95 g/m2 for women.
b. Left atrial enlargement: Left atrial volume index (LAVI) ≥34 mL/m2.
c. Diastolic dysfunction: E/e′ ratio ≥14, supported by additional parameters such as reduced e′ velocity or a pseudonormal filling pattern.
(3) Sinus rhythm at the time of echocardiography.
(4) Adequate image quality for 2D speckle-tracking echocardiography (2D-STE) analysis.
Exclusion Criteria
- Significant valvular heart disease (moderate or severe).
- Non-hypertensive cardiomyopathies (eg, dilated, hypertrophic, or restrictive forms).
- Ischemic heart disease or cardiomyopathy, defined by a history of myocardial infarction, prior coronary revascularization, ≥50% coronary stenosis on angiography or CT, or regional wall motion abnormalities suggestive of ischemia.
- Persistent arrhythmias (eg, atrial fibrillation), which would compromise strain measurements.
- Advanced renal dysfunction: eGFR <30 mL/min/1.73 m2 or dialysis dependency.
- Incomplete clinical or echocardiographic data precluding comprehensive analysis.
Echocardiographic Equipment and Image Acquisition Protocol
All echocardiographic examinations were performed using commercially available color Doppler ultrasound systems, including the Philips iE33 (Philips Medical Systems, Andover, MA, USA) and the GE Vivid E95 (GE Healthcare, Chicago, IL, USA). The imaging probes included an M5Sc transducer with a frequency range of 1.7–3.3 MHz and an S5-1 phased-array transducer with a frequency range of 1–5 MHz. 2D-STE analyses were conducted using the QLAB 9.0 software platform (Philips Medical Systems) and the integrated automated quantification system of the GE Vivid E95.
All subjects underwent transthoracic echocardiography while in the left lateral decubitus position, with simultaneous electrocardiogram gating. Standard parasternal and apical views were acquired. The left ventricular end-diastolic diameter (LVEDD) was measured using the S5-1 probe in the parasternal long-axis view. LVEF was calculated using the biplane Simpson’s method. Patients were instructed to maintain steady breathing, and breath-holding was employed when necessary to optimize image clarity. Following conventional echocardiographic assessment, 2D-STE was performed using the QLAB-TMQA analysis module. Regions of interest (ROI) were manually traced along the endocardial borders of the left atrium in the apical two-chamber, three-chamber, and four-chamber views. The ROI width was adjusted to match the myocardial wall thickness. Automated frame-by-frame tracking of myocardial motion within each ROI was conducted by the software.
For strain analysis, the left atrium was segmented into five anatomical walls—anterior, posterior, septal, lateral, and inferior. Each wall was divided into three segments: basal, mid, and apical, yielding a total of 15 segments. From each mid-wall segment, longitudinal left atrial strain rate parameters were extracted, including:
- SRa: peak strain rate during late diastole (atrial contraction),
- SRe: peak strain rate during early diastole (ventricular relaxation),
- SRs: peak strain rate during left ventricular systole.
Each strain rate parameter was measured three times per segment, and the average was calculated and reported as mean strain rate in late diastole (mSRa), early diastole (mSRe), and systole (mSRs), respectively (all in s−1).
Assessment and Classification of Cardiac Functional Status
Cardiac functional status in all elderly patients with hypertensive heart disease was evaluated based on the classification system proposed by the NYHA. The NYHA functional classification is a widely accepted clinical tool used to assess the severity of heart failure symptoms and the degree of physical activity limitation. It consists of the following four grades:
- Class I: No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnea.
- Class II: Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, or dyspnea.
- Class III: Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes fatigue, palpitation, or dyspnea.
- Class IV: Unable to carry out any physical activity without discomfort. Symptoms of heart failure may be present even at rest. Any physical activity increases discomfort.
Data Collection
Clinical and echocardiographic data were retrospectively obtained from the institutional electronic medical record and echocardiography reporting systems between January 2023 and January 2025. Demographic variables (age, sex, and body mass index), hemodynamic parameters [systolic blood pressure (SBP), diastolic blood pressure (DBP), and resting heart rate (HR)], and laboratory findings [fasting plasma glucose (FPG), total cholesterol (TC), and low-density lipoprotein cholesterol (LDL-C)] were extracted from standardized medical records. Comorbid conditions, including diabetes mellitus and smoking history, were identified through clinical documentation.
Echocardiographic measurements were collected from finalized structured reports generated by board-certified echocardiographers at the time of examination. These reports were routinely validated through the department’s internal quality assurance process to ensure measurement reliability. For this study, data entry and extraction were independently cross-checked by two investigators to minimize transcription errors. Only cases with complete clinical and echocardiographic datasets were included in the final analysis.
Statistical Analysis
All statistical analyses were conducted using SPSS software, version 28.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Data with a normal distribution were expressed as mean ± standard deviation and compared between groups using the independent samples t-test. Non-normally distributed data were expressed as median and interquartile range (IQR), and the Mann–Whitney U-test was applied for group comparisons. Categorical variables were reported as frequencies and percentages, and differences between groups were analyzed using the chi-square (χ2) test. Receiver operating characteristic (ROC) curves were plotted to assess the diagnostic performance of echocardiographic parameters, and the area under the curve (AUC) was calculated. A two-tailed P value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Study Cohort
Baseline demographic, anthropometric, hemodynamic, metabolic, and comorbidity profiles were comparable between the HHD group (n = 118) and the Hypertension (HTN) group (n = 118). There was no significant difference in gender distribution (50.8% vs 55.1% male, P = 0.514) or mean age (73.6 ± 5.8 years vs 72.6 ± 5.7 years, P = 0.178). Body mass index was similarly distributed (20.9 ± 1.1 kg/m2 vs 21.1 ± 1.2 kg/m2, P = 0.295). Resting blood pressures and heart rates did not differ appreciably between groups (SBP: 155.2 ± 6.9 mmHg vs 153.3 ± 9.0 mmHg, P = 0.079; DBP: 110.8 ± 7.0 mmHg vs 109.0 ± 7.4 mmHg, P = 0.055; HR: 74.8 ± 6.0 bpm vs 75.6 ± 5.9 bpm, P = 0.319). Fasting plasma glucose and lipid parameters were also similar (all P > 0.1). Prevalence of diabetes (21.2% vs 20.3%, P = 0.873) and smoking history (28.8% vs 23.7%, P = 0.375) did not differ. These findings confirm that the two groups were well matched at baseline (Table 1).
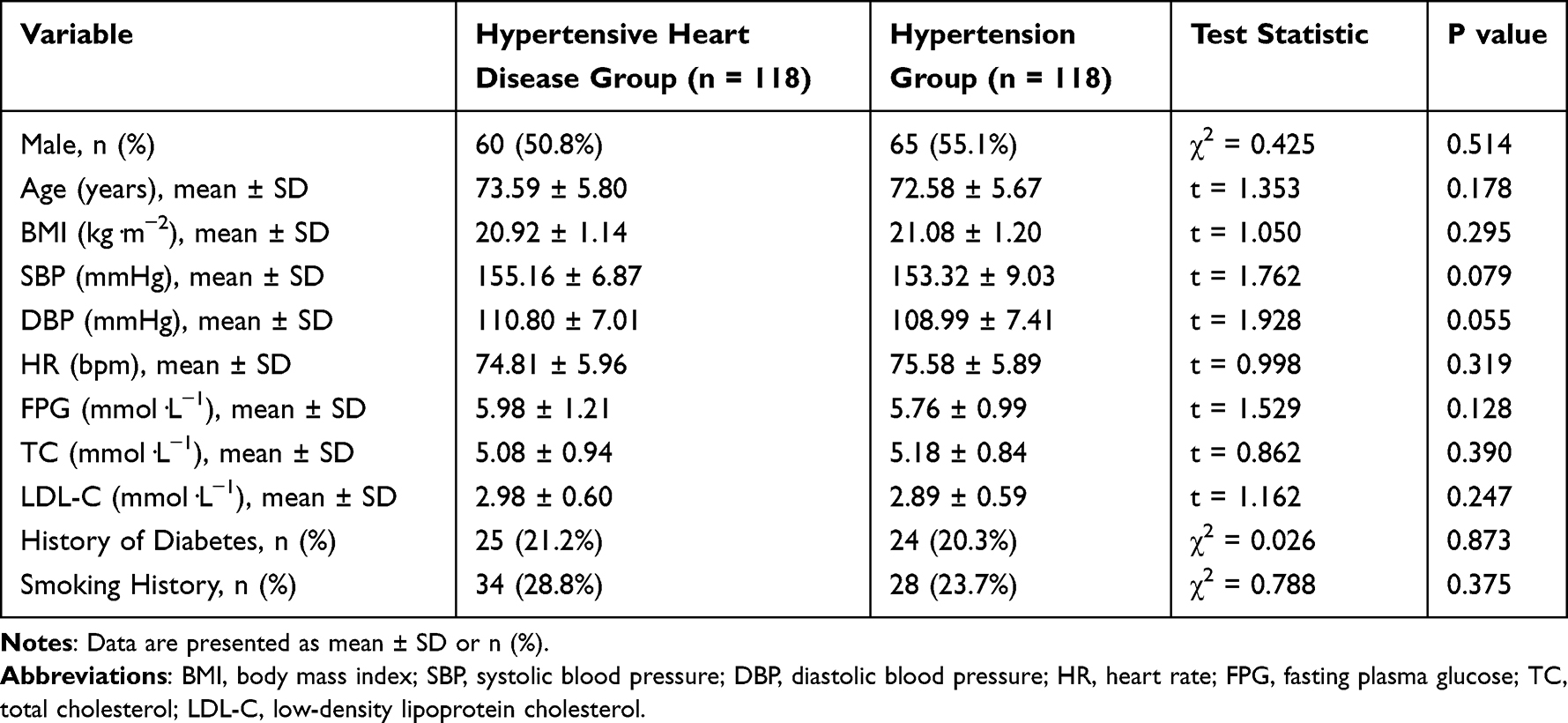 |
Table 1 Baseline Demographic and Clinical Variables in the Hypertensive Heart Disease (HHD) and Hypertension (HTN) Groups |
Comparison of Left Ventricular Dimensions, Ejection Fraction, and Atrial Strain Parameters Between Hypertensive Heart Disease and Hypertension Groups
As shown in Table 2, patients with hypertensive heart disease demonstrated significant differences in both conventional echocardiographic measurements and 2D-STE–derived atrial strain rates compared with those having hypertension alone. Specifically, the HHD group exhibited a markedly larger LVEDD (60.29 ± 5.26 mm vs 48.17 ± 5.46 mm; t = 17.373, P < 0.001) and a lower LVEF (51.10 ± 7.25% vs 61.21 ± 4.96%; t = 14.982, P < 0.001). Regarding atrial mechanics, mSRa was significantly attenuated in the HHD cohort (–2.20 ± 0.27 s−1 vs –2.75 ± 0.30 s−1; t = 14.801, P < 0.001), and mSRe was similarly reduced (–2.29 ± 0.33 s−1 vs –1.90 ± 0.38 s−1; t = 8.418, P < 0.001). Furthermore, the HHD group showed a significantly reduced systolic atrial strain rate (mSRs: 1.34 ± 0.30 s−1 vs 2.15 ± 0.31 s−1; t = 20.402, P < 0.001), indicating both adverse cardiac remodeling on conventional echocardiography and pronounced atrial deformation impairment detected by 2D-STE in elderly patients with hypertensive heart disease.
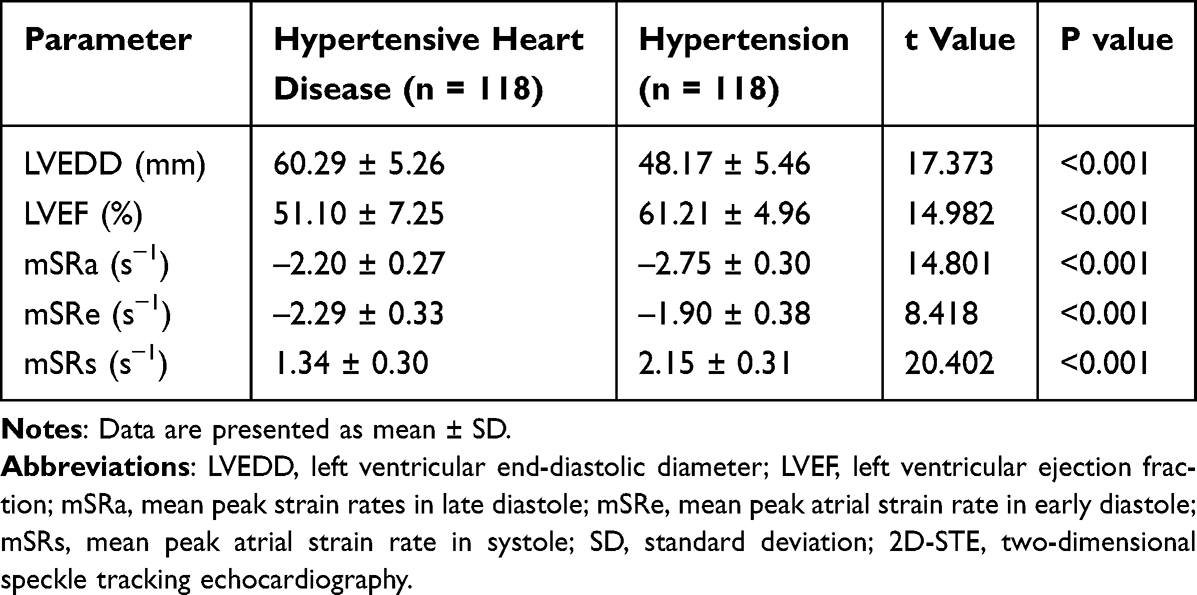 |
Table 2 Comparison of Standard Echocardiographic and Two-Dimensional Speckle Tracking Echocardiography (2D-STE) Parameters Between HHD and HTN Groups ( |

Comparison of Atrial Strain Rates by NYHA Functional Classification in Elderly HHD Patients
Among the 118 elderly patients diagnosed with HHD, NYHA functional classification was as follows: Class I (n = 12, 10.2%), Class II (n = 31, 26.3%), Class III (n = 45, 38.1%), and Class IV (n = 30, 25.4%). The corresponding atrial strain rate parameters measured by 2D-STE were compared between patients with NYHA Class I–II (n = 43, 36.4%) and those with NYHA Class III–IV (n = 75, 63.6%), as presented in Table 3. The mSRa was significantly more positive (less negative) in the NYHA III–IV group compared to the NYHA I–II group (–1.90 ± 0.26 s−1 vs –2.48 ± 0.23 s−1; t = 12.151, P < 0.001). Similarly, the mSRe was significantly more negative in the NYHA III–IV group (–2.60 ± 0.21 s−1 vs –2.11 ± 0.20 s−1; t = 12.431, P < 0.001), and the mSRs was lower in the NYHA III–IV group (1.30 ± 0.28 s−1 vs 1.53 ± 0.30 s−1; t = 4.184, P < 0.001).
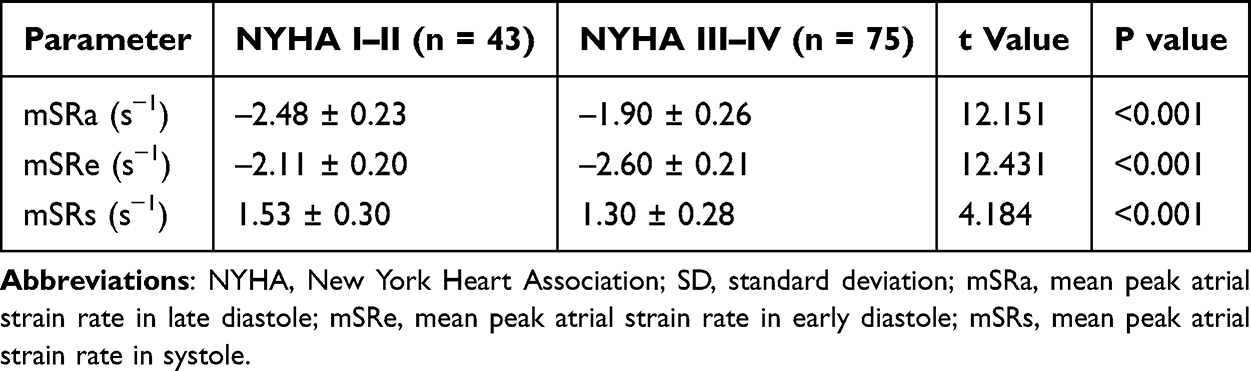 |
Table 3 Comparison of Two-Dimensional Speckle Tracking Echocardiography (2D-STE) Parameters in Elderly HHD Patients by New York Heart Association (NYHA) Functional Class |
ROC Analysis of Atrial Strain Parameters for Functional Assessment
In order to determine the utility of atrial strain metrics in distinguishing degrees of cardiac dysfunction among elderly HHD patients, ROC analysis was performed. As shown in Table 4, all three 2D-STE–derived parameters demonstrated excellent discriminative ability (all P < 0.001). Specifically, mSRa yielded the highest area under the curve (AUC = 0.916; 95% CI, 0.805–0.987) with an optimal cut-off of –2.367 s−1, achieving a sensitivity of 96.8% and specificity of 76.7%, corresponding to a Youden index of 0.735. mSRe also performed robustly (AUC = 0.876; 95% CI, 0.788–0.952) at a threshold of –2.302 s−1, yielding 91.6% sensitivity and 65.0% specificity (Youden index = 0.566). mSRs showed similarly high diagnostic accuracy (AUC = 0.881; 95% CI, 0.791–0.961), with a cut-off of 1.361 s−1, sensitivity of 92.5%, specificity of 68.7%, and Youden index of 0.612 (Figure 1).
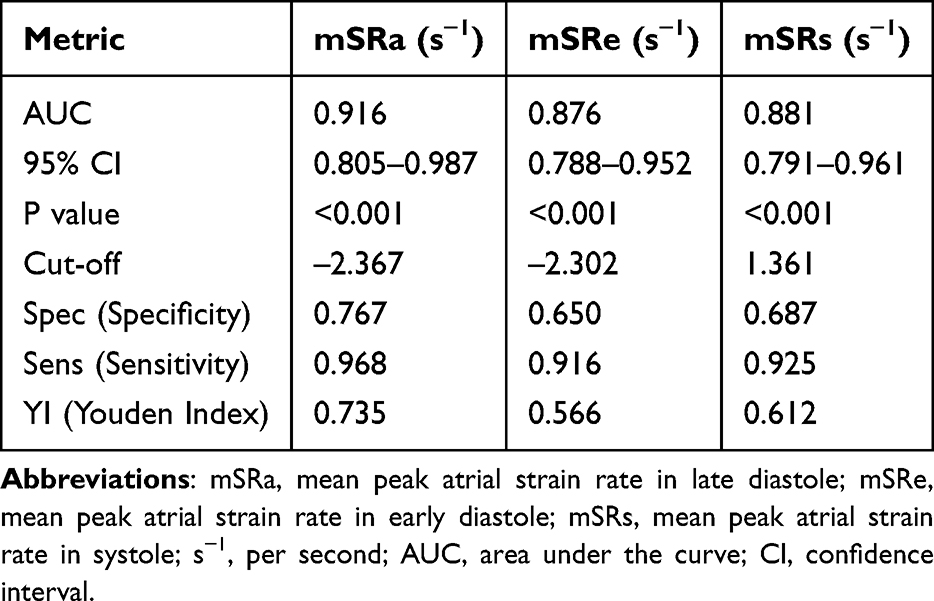 |
Table 4 Diagnostic Value of Mean Peak Atrial Strain Rate in Late Diastole (mSRa), Early Diastole (mSRe), and Systole (mSRs) for Assessing Cardiac Function in Elderly HHD Patients |
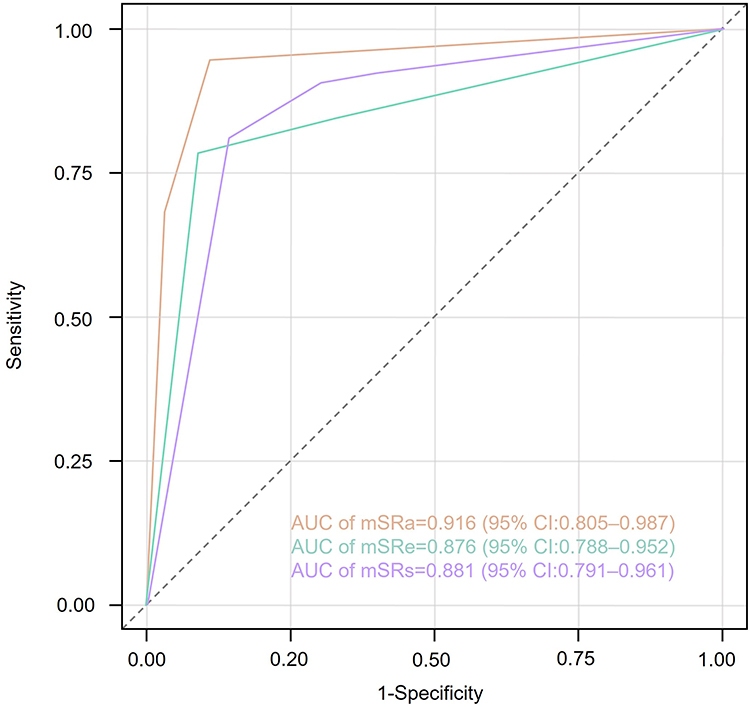 |
Figure 1 Receiver operating characteristic (ROC) curves of two-dimensional speckle tracking echocardiography (2D-STE)–derived strain rate parameters: mSRa (mean peak atrial strain rate in late diastole, s−1), mSRe (mean peak atrial strain rate in early diastole, s−1), and mSRs (mean peak atrial strain rate in systole, s−1) for evaluating left atrial function in elderly patients with hypertensive heart disease (HHD). |
Discussion
This study evaluated the clinical utility of 2D-STE derived atrial strain parameters in elderly patients with HHD. Our findings demonstrate that the strain rate metrics, specifically mSRa, mSRe, and mSRs, were significantly impaired in patients with HHD compared to hypertensive controls without structural cardiac involvement. These alterations reflect atrial dysfunction across reservoir, conduit, and booster pump phases, suggesting that 2D-STE can sensitively detect atrial remodeling in the context of hypertensive myocardial damage. Furthermore, the strain parameters correlated closely with clinical functional status as defined by the NYHA classification20,21 Among patients with HHD, those classified as NYHA III–IV exhibited significantly reduced mSRa, mSRe, and mSRs values compared to those in NYHA I–II, indicating progressive impairment of atrial mechanics with increasing symptom burden. These results underscore the incremental value of atrial strain analysis for functional assessment and stratification in elderly individuals with HHD, beyond conventional echocardiographic measurements such as LVEDD and LVEF.22–24
The current results align with and extend the findings of recent studies evaluating the role of 2D-STE in hypertensive heart disease. In a prospective study of 90 hypertensive patients by Hennawy et al,25 left atrial longitudinal strain parameters were shown to decline progressively with increasing degrees of diastolic dysfunction, even in the setting of preserved LVEF, highlighting the sensitivity of atrial strain to subclinical myocardial changes. Similarly, Longobardo et al26 reported that reduced mSRa was independently associated with impaired exercise tolerance and elevated NT-proBNP in elderly hypertensive individuals with left ventricular hypertrophy. While prior work has primarily focused on LV strain or global longitudinal strain (GLS), our study adds to the growing recognition of atrial strain as a clinically meaningful metric in hypertensive remodeling.27,28 The utility of atrial strain has also been validated in other high-risk elderly cohorts. For example, Oki et al29 demonstrated that reduced LA strain parameters predicted heart failure hospitalization in elderly hypertensive patients with preserved EF. Moreover, our ROC analysis yielded AUC values exceeding 0.87 for all three atrial strain markers, with mSRa showing the highest discriminative power (AUC = 0.916), sensitivity (96.8%), and Youden index (0.735). These diagnostic indices are comparable to or superior to those reported in prior investigations. In a cross-sectional analysis by Monte et al,30 mSRa yielded an AUC of 0.89 for identifying early-stage heart failure with preserved ejection fraction (HFpEF) in elderly hypertensives. Our study corroborates these findings and extends their applicability specifically to the HHD population.
Taken together, our results confirm that 2D-STE–derived atrial strain is a robust, reproducible, and clinically relevant tool for functional assessment in elderly patients with hypertensive heart disease. It not only complements traditional echocardiographic measurements but also provides additional value in risk stratification. From a clinical standpoint, these findings highlight the potential of 2D-STE atrial strain analysis as a noninvasive method to detect early cardiac dysfunction and monitor disease progression in elderly patients with HHD. Given the limitations of conventional parameters such as LVEF in identifying subclinical myocardial impairment, especially in the elderly, the incorporation of mSRa, mSRe, and mSRs into routine echocardiographic evaluation could enhance early detection and guide therapeutic decision-making, particularly in those with borderline symptoms or preserved EF. These indices may also be useful in evaluating treatment response and improving clinical decision-making in this high-risk population.
Recent developments in echocardiographic image analysis, such as Zhang et al’s31 bidirectional reciprocal cycle framework for text-guided segmentation, demonstrate the potential of AI to enhance image interpretation efficiency. Additionally, Sandhu et al32 highlights how focused echocardiographic protocols impact overall utilization. While our study emphasizes diagnostic performance of atrial strain metrics in hypertensive heart disease, these advances in image-guided automation and streamlined imaging approaches may facilitate broader clinical translation and integration of strain-based assessments. Maseliene et al33 demonstrated that LA strain and compliance are impaired in hypertensive disorders of pregnancy despite preserved EF, highlighting atrial mechanics as early indicators of cardiovascular dysfunction. Similarly, our findings in elderly HHD patients confirm that atrial strain parameters detect subclinical impairment before overt systolic dysfunction, but our study extends this concept to a chronic hypertension population with structural heart changes and stratifies by NYHA class, enabling severity discrimination. Seçkin et al34 found reduced LA strain in non-dipper hypertension and its association with end-organ damage, underscoring its diagnostic and prognostic relevance in systemic hypertension. Consistent with this, we observed marked LA strain reduction in HHD, but we further quantified diagnostic accuracy via ROC analysis and provided functional classification correlation, enhancing clinical applicability. Van’t Hof et al35 linked cumulative SBP from midlife to late life with reduced LA strain even in normal LA size, suggesting hypertension-induced atrial remodeling precedes LV dysfunction. Our results align, demonstrating that LA strain is impaired in advanced HHD, but we extend the evidence by focusing on an elderly, clinically stratified cohort with echocardiographic HHD diagnosis, showing superior discriminatory performance of strain parameters for functional severity. These studies collectively reinforce the utility of atrial strain beyond GLS in hypertensive cohorts; our work builds on this by integrating structural, functional, and diagnostic performance metrics in a well-characterized elderly HHD population.
The present study possesses several strengths. First, it is among the few to focus specifically on an elderly population with hypertensive heart disease, a group often underrepresented in echocardiographic validation studies. Second, the study applied a well-matched comparison group of hypertensive patients without structural cardiac changes, enhancing the interpretability of observed differences. Third, multiple atrial strain parameters were evaluated in parallel with NYHA classification, and their diagnostic performance was rigorously assessed via ROC analysis, providing robust evidence for clinical application. This study has several limitations. First, its retrospective, single-center, cross-sectional design introduces inherent biases, including potential selection bias and residual confounding, as patient inclusion relied on available medical records and echocardiographic data. These factors limit both the generalizability of the results and the ability to establish causal relationships. Second, although 2D-STE is a highly sensitive technique, its accuracy depends on image quality and operator expertise, which may introduce measurement variability in routine practice. Third, we did not include biochemical markers such as NT-proBNP or correlate atrial strain parameters with advanced imaging modalities like cardiac MRI, which could have provided additional validation of myocardial fibrosis or diastolic dysfunction. Fourth, we acknowledge the inherent subjectivity of NYHA functional classification, which may introduce inter-observer variability in symptom assessment. Future studies should consider integrating objective functional measures such as the 6-minute walk test (6MWT) or cardiopulmonary exercise testing (CPET) to complement NYHA grading and improve diagnostic precision. Finally, the absence of longitudinal follow-up precluded evaluation of the prognostic value of atrial strain parameters for adverse outcomes such as heart failure hospitalization, arrhythmia, or mortality. Future prospective, multicenter studies incorporating multimodal imaging and biomarker assessment are warranted to confirm these findings, establish temporal relationships, and determine the prognostic utility of atrial strain in hypertensive heart disease.
Conclusions
In elderly patients with hypertensive heart disease, 2D speckle tracking echocardiography–derived atrial strain parameters (mSRa, mSRe, and mSRs) might be significantly impaired and could correlate with functional status. These indices could demonstrate excellent diagnostic performance for differentiating mild from severe functional impairment and might serve as valuable non-invasive markers for early detection and clinical stratification. Although these findings indicate potential clinical relevance, this study was cross-sectional in design; thus, the prognostic utility of these parameters should be validated in future prospective follow-up studies.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Affiliated Hospital of Changchun University of Chinese Medicine. All procedures involving human participants complied with institutional and/or national ethical standards and the Declaration of Helsinki.
Acknowledgments
We thank every staff member and patient who participated in this study.
Consent for Publication
Informed consent was obtained from all subjects.
Funding
The work was not funded by any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Tanaka H. Efficacy of echocardiography for differential diagnosis of left ventricular hypertrophy: special focus on speckle-tracking longitudinal strain. J Echocardiogr. 2021;19(2):71–79. doi:10.1007/s12574-020-00508-3
2. Tadic M, Sala C, Carugo S, Mancia G, Grassi G, Cuspidi C. Myocardial strain in hypertension: a meta-analysis of two-dimensional speckle tracking echocardiographic studies. J Hypertens. 2021;39(10):2103–2112. doi:10.1097/hjh.0000000000002898
3. Hiebert JB, Vacek J, Shah Z, Rahman F, Pierce JD. Use of speckle tracking to assess heart failure with preserved ejection fraction. J Cardiol. 2019;74(5):397–402. doi:10.1016/j.jjcc.2019.06.004
4. Liu Q, Hu Y, Chen W, et al. Evaluation of right ventricular longitudinal strain in pediatric patients with pulmonary hypertension by two-dimensional speckle-tracking echocardiography. Front Pediatr. 2023;11:1189373. doi:10.3389/fped.2023.1189373
5. Özer S, Aydın E, Şahin M. Evaluation of the relationship between speckle tracking echocardiography and arrhythmia markers Tp-e interval and Tp-e/QTc in patients with arterial hypertension. Eur Rev Med Pharmacol Sci. 2023;27(11):5167–5174. doi:10.26355/eurrev_202306_32634
6. Hosseinsabet A, Yarmohamadi S, Narimani S, Amini-Farshidmehr N. Right ventricular function in coronary slow flow: a two-dimensional speckle-tracking echocardiographic study. Turk Kardiyol Dern Ars. 2016;44(6):466–473. doi:10.5543/tkda.2016.72699
7. Kinoshita M, Tanabe Y, Yoshida K, et al. Left ventricular longitudinal strain is a major determinant of CT-derived three-dimensional maximum principal strain: comparison with two-dimensional speckle tracking echocardiography. Heart Vessels. 2022;37(1):31–39. doi:10.1007/s00380-021-01901-3
8. Smiseth OA, Rider O, Cvijic M, Valkovič L, Remme EW, Voigt JU. Myocardial Strain Imaging: theory, Current Practice, and the Future. JACC Cardiovasc Imaging. 2025;18(3):340–381. doi:10.1016/j.jcmg.2024.07.011
9. Mihos CG, Liu JE, Anderson KM, et al. Speckle-tracking strain echocardiography for the assessment of left ventricular structure and function: a scientific statement from the American heart association. Circulation. 2025;152(10):e96–e109. doi:10.1161/cir.0000000000001354
10. Alizadehasl A, Mokhayeri M, Sohani Z, Zamanian MY, Shahbazi P, Borzouei S. A comprehensive review of two-dimensional speckle-tracking echocardiography in assessing right and left ventricular function in diabetic patients. Clin Cardiol. 2025;48(5):e70153. doi:10.1002/clc.70153
11. Iannaccone G, Graziani F, Del Buono MG, et al. Left atrial strain analysis improves left ventricular filling pressures non-invasive estimation in the acute phase of Takotsubo syndrome. Eur Heart J Cardiovasc Imaging. 2023;24(6):699–707. doi:10.1093/ehjci/jead045
12. Rösner A, Kornev M, Caglayan HA, et al. Atrial strain and strain rate in a general population: do these measures improve the assessment of elevated NT-proBNP levels? Cardiol Res Pract. 2024;2024(1):1546629. doi:10.1155/2024/1546629
13. Sharifov OF, Denney TS Jr, Girard AA, Gupta H, Lloyd SG. Coronary artery disease is associated with impaired atrial function regardless of left ventricular filling pressure. Int J Cardiol. 2023;387:131102. doi:10.1016/j.ijcard.2023.05.052
14. Tanaka S, Segawa T, Noda T, et al. Assessment of visit-to-visit variability in systolic blood pressure over 5 years and phasic left atrial function by two-dimensional speckle-tracking echocardiography. Heart Vessels. 2021;36(6):827–835. doi:10.1007/s00380-020-01751-5
15. Radwan H, Hussein E. Value of global longitudinal strain by two dimensional speckle tracking echocardiography in predicting coronary artery disease severity. Egypt Heart J. 2017;69(2):95–101. doi:10.1016/j.ehj.2016.08.001
16. Demircan T, Kizilca Ö, Yilmaz N, Zihni C, Kir M, Ünal N. Evaluation of left ventricular functions by speckle-tracking echocardiography in coarctation patients. Echocardiography. 2021;38(3):410–416. doi:10.1111/echo.14993
17. Nemtsova V, Burkard T, Vischer AS. Hypertensive heart disease: a narrative review series—part 2: macrostructural and functional abnormalities. J Clin Med. 2023;12(17):5723. doi:10.3390/jcm12175723
18. Larsen BS, Biering-Sørensen T, Olsen FJ. Exploring the link between left atrial strain and exercise-induced pulmonary hypertension. Echocardiography. 2025;42(5):e70187. doi:10.1111/echo.70187
19. Gotsman I, Zwas D, Lotan C, Keren A. Heart failure and preserved left ventricular function: long term clinical outcome. PLoS One. 2012;7(7):e41022. doi:10.1371/journal.pone.0041022
20. Ma H, Wu H, Sun X, Wang Q, Zheng Y. The evaluation of right ventricular synchrony by two-dimensional speckle tracking echocardiography in connective tissue disease-associated pulmonary arterial hypertension. Echocardiography. 2025;42(1):e70060. doi:10.1111/echo.70060
21. Helmy KM, Biomy R, Salama MK, Haseeb WA. Left atrial function assessment by speckle tracking echocardiography in low-risk atrial fibrillation patients. J Pak Med Assoc. 2023;73(Suppl 4):S142–s145. doi:10.47391/jpma.Egy-s4-29
22. Kalaycıoğlu E, Çetin M, Kırış T, Özyıldız AG. Paradoxical association between lipoprotein cholesterol levels and left atrial function in hypertensive diabetic patients: a speckle tracking study. J Clin Ultrasound. 2021;49(7):667–673. doi:10.1002/jcu.23032
23. Sayed A, Razik NA, Galal AW, et al. Effect of dipping and nondipping pattern of blood pressure on subclinical left ventricular dysfunction assessed by two-dimensional speckle tracking in hypertensive patients. Blood Press Monit. 2022;27(1):43–49. doi:10.1097/mbp.0000000000000564
24. Zhang L, Zhang P, Qi H, et al. Right ventricular function in pulmonary hypertension due to left heart disease by two-dimensional speckle tracking and real time three-dimensional echocardiography. Acta Cardiol. 2016;71(4):473–482. doi:10.2143/ac.71.4.3159702
25. Hennawy B, El Kilany W, Galal H, Mamdouh A. Role of speckle tracking echocardiography in detecting early left atrial dysfunction in hypertensive patients. Egypt Heart J. 2018;70(3):217–223. doi:10.1016/j.ehj.2018.05.004
26. Longobardo L, Suma V, Jain R, et al. Role of two-dimensional speckle-tracking echocardiography strain in the assessment of right ventricular systolic function and comparison with conventional parameters. J Am Soc Echocardiogr. 2017;30(10):937–946.e6. doi:10.1016/j.echo.2017.06.016
27. Mu Y, Qin C, Wang C, Huojiaabudula G. Two-dimensional ultrasound speckle tracking imaging in evaluation of early changes in left ventricular diastolic function in patients with essential hypertension. Echocardiography. 2010;27(2):146–154. doi:10.1111/j.1540-8175.2009.00984.x
28. Ping L, Huang Y, Sun G, et al. Early detection of left atrial dysfunction in young hypertensive patients with a normal left atrial size: a comprehensive analysis using four-dimensional auto left atrial quantification echocardiography. BMC Cardiovasc Disord. 2025;25(1):363. doi:10.1186/s12872-025-04825-2
29. Oki T, Miyoshi H, Oishi Y, Mizuguchi Y, Ara N, Iuchi A. The impact of hypertension as a road to heart failure with preserved ejection fraction: diagnostic value of two-dimensional speckle tracking echocardiography for the early impairment of left atrial-left ventricular-arterial coupling. Curr Hypertens Rev. 2014;10(4):177–188. doi:10.2174/1573402111666150206123245
30. Monte IP, Di Benedetto C, Atanasio FA, Losi V, Licciardi S, Tamburino C. Morpho-functional cardiovascular adaptation in hypertensive patients: two-dimensional speckle tracking echocardiographic study. Minerva Cardioangiol. 2018;66(4):368–375. doi:10.23736/s0026-4725.17.04496-6
31. Zhang Z, Zhang H, Zeng T, Yang G, Shi Z, Gao Z. Bridging multi-level gaps: bidirectional reciprocal cycle framework for text-guided label-efficient segmentation in echocardiography. Med Image Anal. 2025;102:103536. doi:10.1016/j.media.2025.103536
32. Sandhu AT, Parizo J, Moradi-Ragheb N, Heidenreich PA. Association between offering limited left ventricular ejection fraction echocardiograms and overall use of echocardiography. JAMA Intern Med. 2018;178(9):1270–1272. doi:10.1001/jamainternmed.2018.3317
33. Maseliene T, Laurinaviciene A, Dzenkeviciute V. Early cardiovascular changes in hypertensive pregnancies: insights from left atrial strain and compliance. BMC Pregnancy Childbirth. 2025;25(1):737. doi:10.1186/s12884-025-07857-w
34. Seçkin Ö, Ünlü S, Yalçın MR. The hidden role of left atrial strain: insights into end-organ damage in dipper and nondipper hypertension. J Hum Hypertens. 2025;39(6):425–431. doi:10.1038/s41371-025-01017-5
35. Van’t Hof JR, Parikh R, Moser ED, et al. Association of cumulative systolic blood pressure with left atrial function in the setting of normal left atrial size: the atherosclerosis risk in communities (ARIC) study. J Am Soc Echocardiogr. 2024;37(9):884–893. doi:10.1016/j.echo.2024.04.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.