Back to Journals » International Medical Case Reports Journal » Volume 19
Diagnostic Challenges in Spondylodiscitis After Endoscopic Retrograde Cholangiopancreatography Mimicking Malignancy and Radiculopathy
Authors Dadakci YC ![]() , Asoglu I
, Asoglu I ![]()
Received 21 March 2026
Accepted for publication 5 June 2026
Published 12 June 2026 Volume 2026:19 610678
DOI https://doi.org/10.2147/IMCRJ.S610678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Yagmur Can Dadakci, Ibrahim Asoglu
Department of Algology, Sanliurfa Training and Research Hospital, Sanliurfa, Turkey
Correspondence: Yagmur Can Dadakci, Department of Algology, Sanliurfa Training and Research Hospital, Sanliurfa, Turkey, Email [email protected]
Abstract: Endoscopic retrograde cholangiopancreatography (ERCP) is a common procedure for biliary tract diseases, but it can rarely be followed by severe infectious complications such as spondylodiscitis. We present a 57-year-old woman who developed severe low back and leg pain after ERCP performed on 10 December 2025 for biliary sludge. An outside-hospital evaluation on 17 December 2025 documented fever, right upper quadrant pain, pneumobilia, and a catheter/stent-like structure within the bile duct with minimal surrounding fluid, raising concern for biliary infection. Initial laboratory results later showed markedly elevated C-reactive protein (75 mg/L), procalcitonin (0.6 ng/mL), vitamin B12 (> 2000 pg/mL), and mildly increased tumor markers (CA 19– 9 59.8 U/mL; CA 15– 3 42 U/mL), initially raising concern for occult malignancy. Early sacroiliac magnetic resonance imaging demonstrated extensive inflammatory edema and was initially interpreted as reactive inflammation. Because pain persisted and inflammatory markers remained elevated despite initial treatment, dedicated lumbar magnetic resonance imaging was obtained after pain management reassessment on 18 February 2026; this confirmed aggressive L5-S1 spondylodiscitis with epidural abscess and psoas involvement. The patient improved after 6 weeks of intravenous antibiotic therapy. This case highlights how severe inflammation may produce biochemical red flags that mimic malignancy and underscores the value of multidisciplinary evaluation. Persistent post-procedural pain warrants diagnostic vigilance and timely dedicated spinal imaging even when early imaging is non-specific and microbiological confirmation is unavailable.
Keywords: endoscopic retrograde cholangiopancreatography, magnetic resonance imaging, pain management, radiculopathy, spondylodiscitis, tumor markers, vitamin B12
Introduction
Spondylodiscitis is a serious infection of the intervertebral disc and adjacent vertebrae that requires prompt recognition to prevent neurological deficits. Although most cases arise from hematogenous spread, iatrogenic causes after abdominal, vascular, and spinal procedures have also been described. ERCP is generally safe; however, transient bacteremia may occur and, rarely, may be followed by metastatic infection. Post-ERCP spondylodiscitis appears to be rare, with only isolated case reports in the literature.1
Diagnostic delay may occur when clinicians become anchored to the earliest available explanation, a cognitive bias commonly described as diagnostic anchoring. In inflammatory biliary conditions, biochemical abnormalities such as increased CA 19–9, CA 15–3, and marked vitamin B12 elevation may strengthen that anchoring by mimicking malignancy.2,3 In addition, patients with persistent lumbosacral pain after abdominal procedures may first present to pain clinics because the symptoms resemble common radiculopathy. In such settings, pain specialists may be among the first clinicians to suspect an occult spinal infection and redirect the workup toward dedicated spinal imaging.
We report a case of radiologically diagnosed L5-S1 spondylodiscitis identified after pain management reassessment in a patient with persistent pain following ERCP. The educational value of the case lies in the diagnostic delay, the misleading biochemical profile, and the importance of multidisciplinary re-evaluation when symptoms and inflammatory markers fail to improve as expected.
Case Presentation
A 57-year-old woman with diabetes mellitus and coronary artery disease underwent ERCP on 10 December 2025 for biliary sludge. The formal ERCP procedure report was not available in the accessible records; however, a subsequent outside-hospital computed tomography report described a catheter/stent-like structure within the common bile duct, suggesting biliary instrumentation and likely stent placement.
On 17 December 2025, the patient presented to another hospital with right upper quadrant pain and fever. According to the available hospital note, computed tomography showed prior cholecystectomy, a catheter-related appearance within the common bile duct and biliary tree, minimal fluid around the common bile duct stent with suspicion for abscess, and air within the biliary tract. These findings were clinically interpreted in the context of biliary infection/sepsis, and the patient received empirical antibiotic therapy. Exact agent and dose details from the outside treatment were not available in the records reviewed for this report.
Despite this treatment, severe low back pain radiating to the right leg persisted. The patient was first evaluated in the pain management clinic on 18 February 2026. She reported intractable pain with a visual analog scale score of 9/10. Electromyography demonstrated L5-S1 sensorimotor neuropathy. Laboratory evaluation during the clinical course showed persistent inflammation and misleading biochemical abnormalities, including CRP 75 mg/L at initial presentation, procalcitonin 0.6 ng/mL, vitamin B12 >2000 pg/mL without prior supplementation, CA 19–9 59.8 U/mL, CA 15–3 42 U/mL, and leukocytosis (Table 1). Because these findings coexisted with persistent pain after ERCP, the initial differential diagnosis included occult malignancy as well as biliary sepsis.
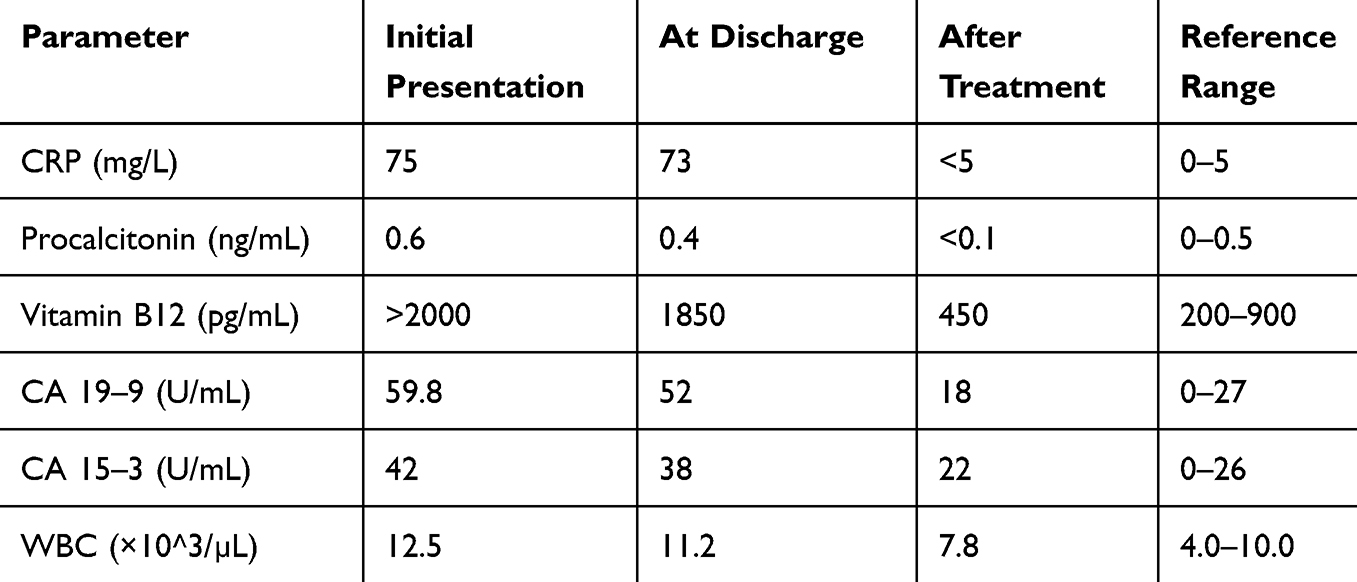 |
Table 1 Laboratory Findings During the Clinical Course |
An initial sacroiliac magnetic resonance imaging study demonstrated extensive inflammatory edema in the right paravertebral soft tissues and gluteal muscles (Figures 1 and 2) but did not establish definite disc-space infection. Ongoing severe radicular pain, continued elevation of inflammatory markers at discharge, and insufficient clinical improvement prompted the pain management team to request repeat laboratory testing and dedicated lumbar magnetic resonance imaging. The lumbar study revealed aggressive L5-S1 spondylodiscitis with disc-space abnormality, adjacent endplate destruction/erosive change, epidural abscess causing foraminal compression, and associated psoas involvement (Figure 3).
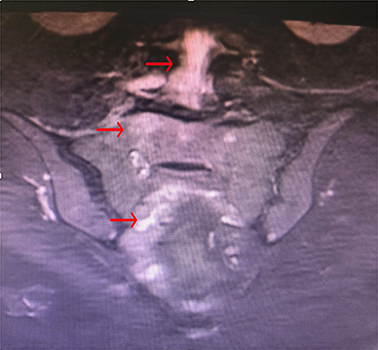 |
Figure 1 Coronal sacroiliac MRI demonstrating extensive inflammatory involvement. Coronal T2-weighted sacroiliac MRI showing extensive inflammatory changes. Red arrows indicate paravertebral soft tissue inflammation (upper arrow), sacral region involvement (middle arrow), and associated gluteal muscle inflammatory edema (lower arrow). |
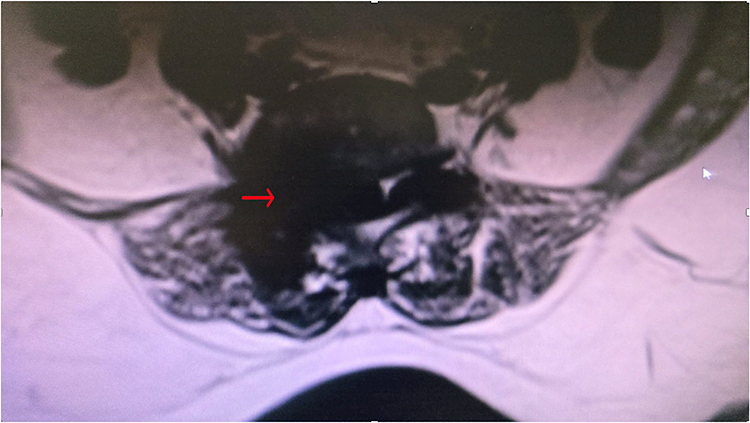 |
Figure 2 Axial MRI demonstrating epidural and paravertebral involvement. Axial T2-weighted sacroiliac MRI demonstrating epidural and adjacent paravertebral soft tissue involvement. The red arrow indicates the region of inflammatory extension. |
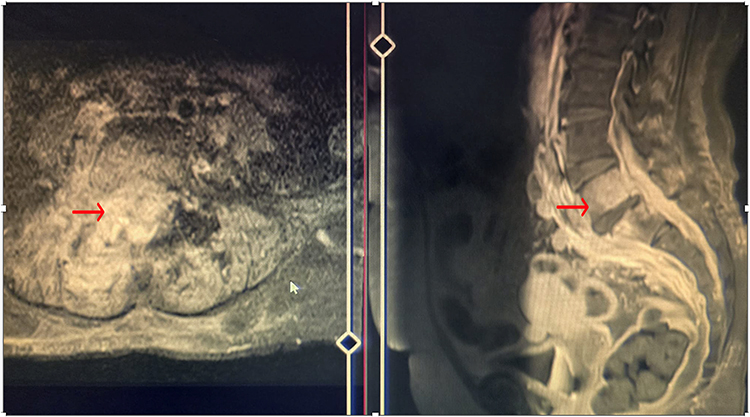 |
Figure 3 Multiplanar MRI findings of L5-S1 spondylodiscitis. Combined axial (left) and sagittal (right) T2-weighted lumbar MRI views demonstrate infection at the L5-S1 level. In the axial image, the red arrow indicates epidural/paravertebral inflammatory involvement. In the sagittal image, the red arrow highlights L5-S1 disc-space infection with adjacent vertebral body marrow edema. The sagittal image was cropped to remove timestamps for patient confidentiality. |
The patient was rehospitalized and treated with 6 weeks of intravenous antibiotics. Blood cultures were not obtained, and spinal biopsy was not performed; therefore, microbiological confirmation was not available. Management was guided by the clinical course and radiological findings. After treatment, inflammatory markers normalized and the patient’s pain resolved completely.
Discussion
This case illustrates several clinically important points. First, severe inflammatory states may create a biochemical picture that mimics malignancy. CA 19–9 can rise during acute cholangitis and other biliary inflammatory conditions, while vitamin B12 may become markedly elevated because the liver is its principal storage site and hepatobiliary inflammation may increase its release into the circulation.2,3 These abnormalities should therefore be interpreted cautiously in the acute inflammatory setting and should not be viewed in isolation as evidence of neoplasia.
Second, the case demonstrates diagnostic anchoring and the consequences of non-specific early imaging. The initial sacroiliac MRI showed substantial inflammatory change but did not answer the key clinical question. Because the patient’s pain pattern remained radicular and inflammatory markers remained elevated, pain management reassessment redirected the workup toward dedicated lumbar imaging, which revealed the true pathology. This sequence is educational because persistent pain after an invasive biliary procedure is easily attributed to musculoskeletal or reactive causes unless the overall timeline is reconsidered.
Third, the association with ERCP should be interpreted cautiously but remains clinically meaningful. We have intentionally framed this as spondylodiscitis occurring after ERCP in the context of biliary infection rather than as microbiologically proven procedure-caused infection. The available chronology supports a plausible pathway of transient bacteremia and hematogenous seeding: ERCP on 10 December 2025, documented febrile biliary illness with suspicious computed tomography findings on 17 December 2025, and subsequent persistent spinal pain culminating in radiological diagnosis. Similar post-biliary-infection spinal complications have been reported, although they are rare.1,4
The principal limitations are the absence of blood cultures, lack of spinal biopsy, incomplete outside-hospital treatment documentation, and unavailable formal ERCP report. These limitations reduce etiological certainty and should be acknowledged explicitly. Nevertheless, the clinico-radiological picture, the evolution of symptoms, and complete response to prolonged intravenous therapy support the working diagnosis of pyogenic spondylodiscitis.4,5 In everyday practice, not every patient is diagnosed under ideal microbiological conditions; this case therefore remains relevant as a report of diagnostic delay, multidisciplinary recognition, and practical clinical decision-making.
Conclusion
Spondylodiscitis should be considered in patients with persistent back pain, radiculopathy, and systemic inflammation after ERCP or biliary infection. Marked vitamin B12 elevation and mildly increased tumor markers may be reactive rather than neoplastic in this setting. When symptoms persist despite initial treatment and early imaging is non-specific, dedicated spinal magnetic resonance imaging and multidisciplinary reassessment are essential to reduce diagnostic delay and prevent complications.
Generative AI Statement
We used ChatGPT-4.1 Mini (Abacus.AI ChatLLM Teams) for language editing and formatting only. The authors take full responsibility for the accuracy and completeness of the manuscript.
Data Sharing Statement
All relevant data are included within the article.
Ethics and Declarations
Ethics Statement: Institutional Review Board approval was not required for this retrospective case report according to the policies of Sanliurfa Training and Research Hospital. The report was prepared in accordance with the principles of the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding was received for this work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Katsinelos P, Fasoulas K, Terzoudis S, Chatzimavroudis G, Zavos C, Kountouras J. Spondylodiscitis complicating cholangitis caused by stent occlusion. Gastrointest Endosc. 2011;73(6):1326–5.PMID:21628020. doi:10.1016/j.gie.2011.01.007
2. Albert MB, Steinberg WM, Henry JP. Elevated serum levels of tumor marker CA19-9 in acute cholangitis. Dig Dis Sci. 1988;33(10):1223–1225. doi:10.1007/BF01536670
3. Sugihara T, Koda M, Okamoto T, et al. Falsely elevated serum vitamin B12 levels were associated with the severity and prognosis of chronic viral liver disease. Yonago Acta Med. 2017;60(1):31–39. PMCID: PMC5355842.
4. Skaf GS, Domloj NT, Fehlings MG, et al. Pyogenic spondylodiscitis: an overview. J Infect Public Health. 2010;3(1):5–16. doi:10.1016/j.jiph.2010.01.001
5. Rutges JPHJ, Kempen DHR, van Dijk M, Oner FC. Spondylodiscitis: diagnosis and treatment options: a systematic review. Eur Spine J. 2016;25(4):983–999. doi:10.1007/s00586-015-4318-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.