Back to Journals » International Medical Case Reports Journal » Volume 19
Diagnostic Challenge at the Knee: A Large (15 Cm) Rapidly Growing Calcified Mass with Features of Desmoplastic Fibroblastoma
Received 5 December 2025
Accepted for publication 8 March 2026
Published 11 March 2026 Volume 2026:19 586776
DOI https://doi.org/10.2147/IMCRJ.S586776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Duaa Knaj,1 Ghanem Ahmad2
1Department of Oncology, Tishreen University, Latakia, Syrian Arab Republic; 2Department of Vascular Surgery, Tishreen University, Latakia, Syrian Arab Republic
Correspondence: Duaa Knaj, Department of Oncology, Tishreen University, Latakia, Syrian Arab Republic, Email [email protected]
Background: Desmoplastic fibroblastoma is a rare, benign fibrous tumor typically characterized by slow growth and absence of calcification. However, atypical presentations can pose significant diagnostic challenges. Here, we present a case of a large prepatellar mass with unusual features that complicated the preoperative and differential diagnosis.
Case Presentation: A 45-year-old male presented in June 2023 with a progressively enlarging mass in the left extremity over one year prior to presentation, following direct trauma to the area. While desmoplastic fibroblastomas are typically slow- growing, the rapid enlargement of this mass raised suspicion for more aggressive entities such as sarcomas. Clinical examination revealed a large (13 × 15 cm), firm, well-defined, and non-pulsatile mass in the prepatellar region. Plain radiography revealed calcifications within the soft tissue mass-a feature rarely associated with desmoplastic fibroblastoma and more commonly seen in other lesions like synovial sarcomas or calcifying aponeurotic fibromas. The mass was surgically excised and appeared well -circumscribed and non-infiltrative to the surrounding tissues. Histopathological examination revealed dense fibrocollagenous tissue with perivascular lymphocytic infiltration, a finding that overlaps with other fibrous tumors and necessitated clinicopathological correlation to confirm the diagnosis.
Conclusion: This case highlights the diagnostic dilemma posed by large fibrous lesions when clinicoradiological and histopathological features overlap. It underscores the critical importance of integrating all available clinical, imaging, and histological data; particularly when confirmatory immunohistochemistry is unavailable. Furthermore, it expands the known spectrum of desmoplastic fibroblastoma to include presentations with rapid growth and calcification, serving as a reminder for clinicians to consider this rare entity even in the presence of atypical features.
Keywords: desmoplastic fibroblastoma, desmoid, tumor, benign, case report
Introduction
Masses in the anterior knee joint region present with a broad differential diagnosis. While most cases are due to common inflammatory or traumatic conditions, a large, rapidly growing mass poses diagnostic and management challenges. We report an exceptional case of a likely benign fibrous tumor in this location, which defies the typical expectations regarding its size, growth rate, and radiographic appearance.
Case Presentation
We report the case of a 45-year-old male Syrian- patient who visited our hospital in June 2023 with a large mass in the left lower extremity. On clinical examination, the patient had a good general status. He had a large mass on the anterior aspect of the knee measuring approximately 15×13 cm (Figure 1). On palpation, the mass was firm, tense, minimally tender, non-pulsatile, and relatively mobile with clear boundaries, showing no clinical evidence of deep infiltration into the muscles or joint structures. The overlying skin was intact with no local warmth or erythema. The patient reported that he had no significant past medical history, no previous surgeries, and no chronic diseases, but had a history of smoking for ten years ago. The mass first appeared as a small nodule following direct trauma to his knee approximately one year prior to presentation, with steady growth noted over the subsequent months, causing an important limitation of joint movement and mild pain in motion. At presentation, laboratory tests revealed WBC 10,200/mm3, RBC 6.39×106/mm3, Hgb 14.3 g/dl, Plt count 294×103/mL, ESR 22 mm, CRP 3.9 mg/L, Urea 35 mg/dl, Creatinine 0.9 mg/dl.
 |
Figure 1 Clinical photograph of the left knee (anterior view) in a 45-year-old male, demonstrating a large prepatellar mass. The overlying skin is intact with no evidence of erythema, discharge, or skin changes. |
Plain radiographs (X-ray) of the knee in the anteroposterior and lateral positions revealed a large soft tissue mass anterior to the patella. Notably, the texture was heterogeneous, with some calcifications while maintaining relatively well-defined margins. No attachment or destruction of the adjacent bone was observed (Figure 2). US confirmed the solid and partially heterogeneous nature of the mass. Magnetic resonance imaging (MRI) was suggested for surgical planning but was not available to perform.
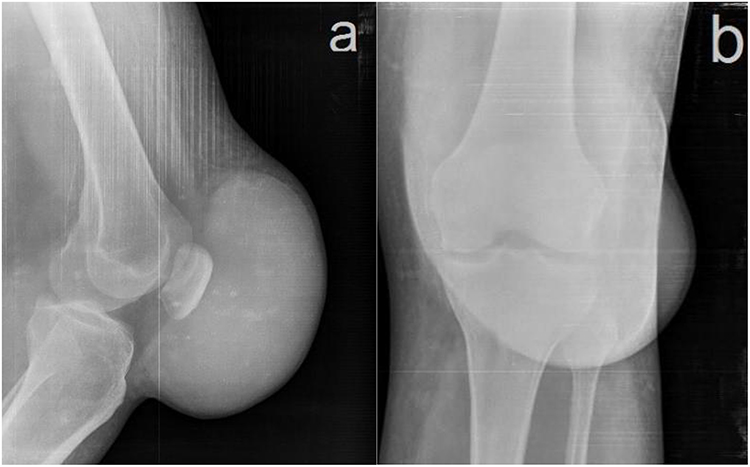 |
Figure 2 Plain radiography of the left knee. (a) Lateral view and (b) Anteroposterior view showing a well-defined mass in the prepatellar region. The mass contains calcifications, with increased soft tissue density. No cortical erosion, or bone involvement is observed. The join space is preserved. |
This mass was isolated without any other lesions in the body according to clinical and radiological examinations, which suggested the absence of malignancy. Color Doppler evaluation was normal, and the mass was non-pulsatile, as previously mentioned. Given the increasing size and mechanical symptoms, surgical excision was performed with the intent to completely excise the mass. Intraoperative, the mass was found to be well-encapsulated by a fibrous capsule with well-define anatomical boundaries. It was dissected with ease from the subcutaneous tissue superficially and deeply from the fascia and muscle, showing no evidence of locally aggressive infiltration characteristic of desmoid tumors. A complete en bloc intracapsular excision was performed (Figure 3). Microscopic examination of the specimen revealed the presence of a benign fibrous tissue. Histological examination revealed bundles of bland, mature spindle-shaped fibroblasts embedded in an abundant stroma of dense collagen. Small, scattered blood vessels were present, accompanied by mild perivascular lymphocytic infiltration. No infiltration of the skeletal muscle at the periphery of the lesion was observed, and there was no evidence of giant cells or osteoid formation. Immunohistochemical staining for definitive markers (such as β-catenin and FOSL1) could not be performed because of technical constraints at our center, which limited our ability to reach a definitive molecular histopathological diagnosis (Figure 4). Therefore, diagnosis primarily relies on distinctive clinicopathological and histomorphological features.
 |
Figure 3 Gross specimen photograph following complete surgical excision. The mass measures 15×13 cm, appears well circumscribed with clear borders, and exhibits a heterogeneous texture. |
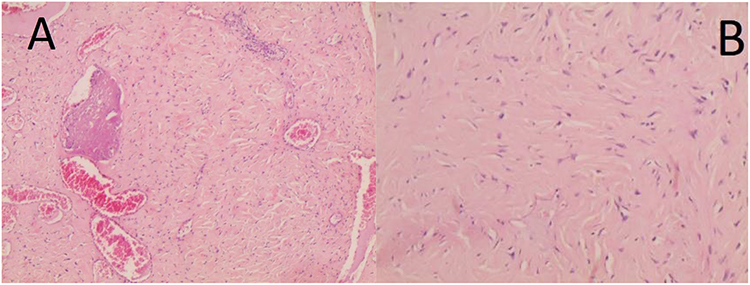 |
Figure 4 Histopathological examination (hematoxylin and eosin stain). (A) Low-power magnification (×40) showing dense fibrocollagenous stroma with scattered blood vessels and perivascular lymphatic infiltration (top right). (B) Higher-power magnification (×100) demonstrating bland spindle cells embedded in abundant dense collagenous matrix, with no cellular atypia or mitotic activity. |
The patient’s postoperative recovery was uneventful. The patient was followed for 2 years post- operatively with no clinical or radiological evidence of local recurrence, and knee function was excellent as of July 2025. Diagnostic uncertainty was explained to the patient, who was advised to undergo periodic clinical surveillance.
Discussion
Desmoplastic fibroblastoma (DF), also known as collagenous fibroma, is a rare benign soft-tissue tumor first described in 1995 by Evans.1 It has a peak incidence in the fifth to seventh decades of life, with a male predominance; however, few cases have been encountered in children.2,3 While its classic histopathological features are well- described in the literature, there remains a diagnostic gap regarding its atypical presentations- particularly when associated with rapid enlargement, calcification, or preceding trauma.
This case is novel in several aspects: it documents, for the first time, the coexistence of rapid growth, radiographic calcifications, and a history of preceding trauma in a single desmoplastic fibroblastoma- features that have not been previously reported together in the literature. This case report presents a large prepatellar mass with features that do not perfectly align with any single common benign fibrous lesion. The primary diagnostic considerations, based on the clinicoradiological and histopathological triad, lie between markedly atypical desmoplastic fibroblastoma (DF) and highly unusual, non-infiltrative desmoid-type fibromatosis.
While the histological findings were compatible with both entities, dense collagen with bland spindle cells, rapid growth over 12 months, and radiographic calcifications were highly atypical in DF. This divergence from the classic presentation underscores a key clinical point: benign fibroblastic tumors can exhibit a spectrum of behaviors. The absence of infiltration into the quadriceps muscle strongly argues against a classic desmoid tumor, which is known for its infiltrative growth, poor margins, and high local recurrence rate (despite a history of trauma). The presence of calcifications, although unusual, may represent dystrophic calcification within a long-standing, large, benign mass. DF is classically described as a slow-growing lesion, and calcification is not a usual features.4 These calcifications may represent dystrophic changes within a long-standing large benign mass, a phenomenon rarely documented. The perception of rapid growth could be related to a latent period following trauma before clinical presentation, or may indicate a more biologically active variant.
Given the atypical features of this case- large size, rapid growth, and calcification- a broad differential diagnosis was considered. Desmoid fibromatosis can occur around the knee and associate with trauma, but its infiltrative margins contrast with the well- circumscribed appearance of our case. Synovial sarcoma was considered due to its prediction for the knee and calcifications, but was excluded by the bland cytology and non-aggressive gross findings. Calcifying aponeurotic fibroma and soft tissue chondroma typically involve hands and feet in younger patients, making them unlikely. Myositis ossificans and tumoral calcinosis were ruled out by imaging pattern and absence of metabolic abnormalities, respectively.
Recent literature on desmoplastic fibroblastoma provided valuable insights into its clinicopathological and imaging characteristic. Shinohara et al reported a case of DF of the knee with characteristic MRI findings and FOSL1 positivity.5 Cuinet et al described DF of the ankle and highlighted the importance of distinguishing this benign entity from malignant tumors,6 and Nakayama et al discussed the diagnostic utility of FOSL1 rearrangements.4 Compared to these reports, our case is unusual in size, rapid growth over 12 months and calcification, has not been documented in recent series.
Ultimately, this case highlights that, in resource-limited settings, a carefully weighed clinicoradiological and histopathological correlation becomes the cornerstone of diagnosis, and expands the known phenotypic variety of prepatellar masses. The main limitation of this study was the unavailability of MRI, confirmatory IHC staining (specifically for FOSL1) and molecular markers. This demonstrates that the accurate synthesis of all available data (history of trauma, exact anatomic location, radiographic details of calcification, gross surgical findings of circumscription, and classic dense collagenous histology) can effectively guide management when advanced diagnostics are inaccessible. Future research directions: Larger case series or registry- based studies are needed to better characterize the frequency and clinical significance of atypical features such as rapid growth and calcification in desmoplastic fibroblastoma.
Conclusion
This case study highlighted several critical issues, and key learning points include (1) Desmoplastic fibroblastoma should be considered in the differential diagnosis of rapidly growing calcified soft tissue masses, despite its indolent presentation. (2) The absence of confirmatory immunohistochemistry does not preclude a working diagnosis when clinical, radiological, and histological findings are carefully integrated.(3) A history of preceding trauma may be present in rare cases but should not be over-interpreted as a causal factor. Long-term follow-up is essential to monitor for recurrence and validate the benign clinical course predicted by the initial findings.
Abbreviations
WBC, white blood cells; Hgb, hemoglobin; RBC, red blood cell; Plt, platelet count; ESR, erythrocyte sedimentation rate; CRP, C - reactive protein; US, ultra-sound; CT, computed tomography; MRI, magnetic resonance imaging; IHC, immunohistochemistry; FOSL1, original simian-like antigen 1.
Ethical Approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. The institutional approval for the study of the case was not required to publish the case details.
Disclosure
The authors declare no conflicts of interest regarding the publication of this article.
References
1. Evans HL.Desmoplastic fibroblastoma. A report of seven cases. Am J Surg Pathol. 1995;19(9):1077–6.
2. Magro G, Venti C. Childhood desmoplastic fibroblastoma (collagenous fibroma) with a 12-year follow-up. Pediatr Dev Pathol. 1999;2(1):62–64. doi:10.1007/s100249900091
3. Nishio J, Iwasaki H, Nishijima T, Kikuchi M. Collagenous fibroma (desmoplastic fibroblastoma) of the finger in a child. Pathol Int. 2002;52(4):322–325. doi:10.1046/j.1440-1827.2002.01351.x
4. Nakayama S, Junnishio J, AOKI, k NABESHIMA, AOKI M, YAMAMOTO T. An Update on Clinicopathological, Imaging and Genetic Features of Desmoplastic Fibroblastoma (Collagenous Fibroma). In Vivo. 2021;35(1):69–73. doi:10.21873/invivo.12233
5. Shinohara Y, Chijiiwa Y, Nishio J. Desmoplastic fibroblastoma (collagenous fibroma) of the knee: a case report and literature review. Cancer Diagnosis Prognosis. 2024;4(6):825–827. doi:10.21873/cdp.10403
6. Cuinet T, Couraudon A, Lefevre M, Fernandez A, Galois L. Desmoplastic fibroblastoma of the ankle: a case report of a rare localization and a literature review. J Orthopaedic Case Reports. 2024;14(6):96–100. doi:10.13107/jocr.2024.v14.i06.4516
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Isolated Asymptomatic Fetal Intracardiac Mass: A Case of Rhabdomyoma

Eticha TG, Ararso R, Sultan S, Terefe K, Berhe SW, Tsega T, Abebe Y, Baye C
International Medical Case Reports Journal 2023, 16:97-102
Published Date: 28 February 2023