Back to Journals » Journal of Asthma and Allergy » Volume 9
Diagnosis of exercise-induced anaphylaxis: current insights
Authors Pravettoni V, Incorvaia C ![]()
Received 20 July 2016
Accepted for publication 25 September 2016
Published 27 October 2016 Volume 2016:9 Pages 191—198
DOI https://doi.org/10.2147/JAA.S109105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Valerio Pravettoni,1 Cristoforo Incorvaia2
1Clinical Allergy and Immunology Unit, Foundation IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy; 2Cardiac/Pulmonary Rehabilitation, ASST Gaetano Pini/CTO, Milan, Italy
Abstract: Exercise-induced anaphylaxis (EIAn) is defined as the occurrence of anaphylactic symptoms (skin, respiratory, gastrointestinal, and cardiovascular symptoms) after physical activity. In about a third of cases, cofactors, such as food intake, temperature (warm or cold), and drugs (especially nonsteroidal anti-inflammatory drugs) can be identified. When the associated cofactor is food ingestion, the correct diagnosis is food-dependent EIAn (FDEIAn). The literature describes numerous reports of FDEIAn after intake of very different foods, from vegetables and nuts to meats and seafood. One of the best-characterized types of FDEIAn is that due to ω5-gliadin of wheat, though cases of FDEIAn after wheat ingestion by sensitization to wheat lipid transfer protien (LTP) are described. Some pathophysiological mechanisms underlying EIAn have been hypothesized, such as increase/alteration in gastrointestinal permeability, alteration of tissue transglutaminase promoting IgE cross-linking, enhanced expression of cytokines, redistribution of blood during physical exercise leading to altered mast-cell degranulation, and also changes in the acid–base balance. Nevertheless, until now, none of these hypotheses has been validated. The diagnosis of EIAn and FDEIAn is achieved by means of a challenge, with physical exercise alone for EIAn, and with the assumption of the suspected food followed by physical exercise for FDEIAn; in cases of doubtful results, a double-blind placebo-controlled combined food–exercise challenge should be performed. The prevention of this particular kind of anaphylaxis is the avoidance of the specific trigger, ie, physical exercise for EIAn, the assumption of the culprit food before exercise for FDEIAn, and in general the avoidance of the recognized cofactors. Patients must be supplied with an epinephrine autoinjector, as epinephrine has been clearly recognized as the first-line intervention for anaphylaxis.
Keywords: anaphylaxis, exercise-induced anaphylaxis, food-dependent exercise-induced anaphylaxis, epinephrine autoinjector
Corrigendum for this paper has been published
Introduction
The term “anaphylaxis” defines an acute, life-threatening, generalized reaction with various clinical presentations that concern the skin, respiratory, gastrointestinal, and cardiovascular systems.1,2 Recent epidemiological surveys have found a prevalence of anaphylaxis of less than 2% in children3 and ranging from 1.6% to 5.1% in adults.4 Anaphylaxis may be caused by a variety of triggers, which may be grouped under two major mechanisms: IgE-mediated and non-IgE-mediated.5
IgE-mediated anaphylaxis
The most common cause of anaphylaxis is exposure to specific allergen to which a subject is sensitized. Allergens related to IgE-mediated mechanism are foods, insect venoms, latex, antibiotics, such as β-lactams, general anesthetics, and biological agents.6
Non-IgE-mediated anaphylaxis
Anaphylactic reactions from nonsteroidal anti-inflammatory drugs (NSAIDs) are mostly non-IgE-mediated, while hypersensitivity reactions to chemotherapeutic drugs, general anesthetics, or biological agents may or may not be IgE-mediated.1,7–10
Mast-cell disorders
Mast-cell disorders may sustain severe reactions in association with exposure to allergens (especially insect venoms and foods), but may also act directly in the frame of mast cell-activation syndromes.11,12
Idiopathic anaphylaxis
The use of the term “idiopathic” refers to anaphylaxis with no identification of causes, but the number of diagnoses of this kind of anaphylaxis is declining, due to the increasing recognition of a mast-cell disorder as the actual cause. The correct diagnosis can be confirmed by measuring tryptase (the mediator exclusively produced by mast cells)13 or detecting mast-cell clonality by bone marrow examination.14 Unfortunately, the measurement of serum tryptase is not often feasible clinically.
Exercised-induced anaphylaxis
The occurrence of anaphylactic symptoms after physical activity defines the type of exercise-induced anaphylaxis (EIAn).15 Here, we review the updated literature on pathophysiological mechanisms and diagnosis of EIAn.
Clinical characteristics of EIAn
Physical exercise may elicit specific forms of asthma or urticaria, but the diagnosis of EIAn relies upon the development after any kind of physical activity of different symptoms that include skin symptoms (itching, flushing, hives, angioedema), respiratory symptoms (wheezing, dyspnea), gastrointestinal symptoms (nausea, vomiting, abdominal pain, diarrhea), and cardiovascular symptoms (hypotension, collapse, loss of consciousness).15 Subjects of any age are involved, with a reported age range of 4–74 years.16 The exercise intensity able to elicit symptoms is variable, even in the same subject.17 EIAn is relatively rare, as suggested by the largest epidemiological study available (including 76,229 adolescents), that detected a prevalence of 0.048%.18 According to data from registries for anaphylaxis in European countries, about 30% of cases of EIAn are associated with cofactors.19 The most important cofactor is food ingestion. The first report dates back to 1979, when the case of a patient who experienced anaphylaxis after eating shellfish and performing strenuous exercise was described.20 Since then, a large series of reports have expanded the number of foods responsible, including several vegetables, cereals, nuts, fish, cow’s milk, beef, pork, chicken/turkey, snails, and mushrooms,20–70 as shown in Table 1. To diagnose food-dependent exercise-induced anaphylaxis (FDEIAn), it is required that physical exercise or food consumption alone do not cause any reaction, while their combination elicits anaphylactic symptoms.15 Early studies reported that a meal with any food (nonspecific FDEIAn) before exercising was able to trigger reactions,71 but today it is clear that such a subtype is much rarer than FDEIAn. It is similarly rare that anaphylaxis is elicited only if two different foods are simultaneously ingested.37,72 Other cofactors needed to cause anaphylaxis from physical exercise have been identified in exposure to warm58 or cold temperature,40 menstrual cycle,28 metal-containing dental amalgams,73 and drug intake, especially NSAIDs. In Table 2, we summarize FDEIAn cofactors reported in the literature. Concerning warm temperature, in its early phase (ie, before respiratory or cardiovascular symptoms appear), EIAn must be differentiated from cholinergic urticaria, which is a form of urticaria associated with elevation of body temperature, possibly triggered by exercise, hot showers, and ingestion of hot or spicy foods.74 The role of NSAIDs was reviewed by Sheffer and Austen in 1984,23 and acetylsalicylic acid is the best-investigated agent.41,47 When one of the aforementioned cofactors reported is present before physical exertion, anaphylaxis symptoms develop mostly within 30 minutes from the onset of physical activity. However, a case of anaphylaxis 5 hours after intake of a wheat-containing meal has been reported.51
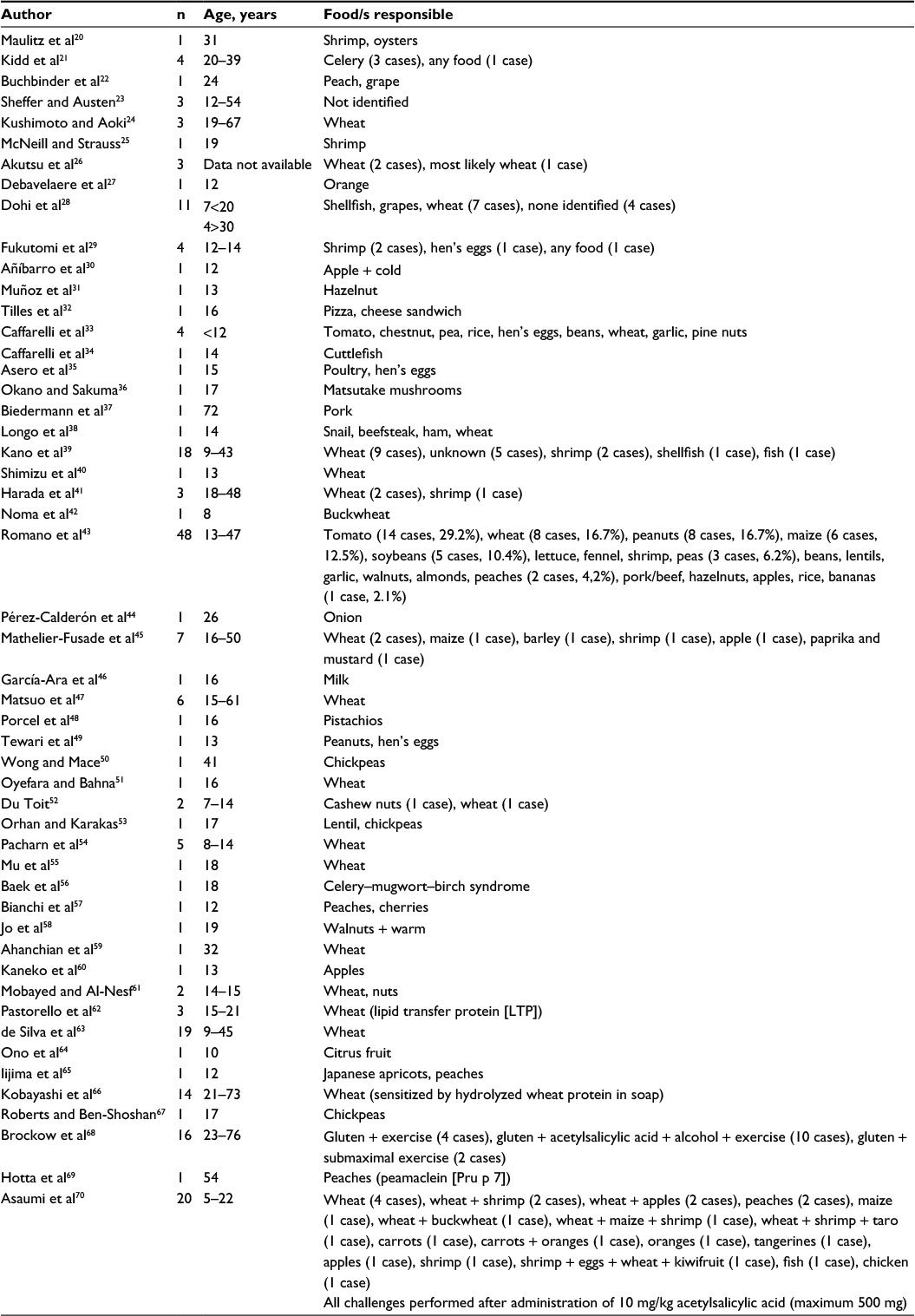 | Table 1 Food-dependent exercise-induced anaphylaxis papers in the literature are reported |
 | Table 2 Cofactors of food-dependent exercise-induced anaphylaxis reported in the literature Abbreviations: NSAIDs, nonsteroidal anti-inflammatory drugs; PPI, proton-pump inhibitor. |
Mechanisms underlying EIAn
As with anaphylaxis in general, the release of mediators by mast cells is considered of critical importance, as suggested by direct observation from skin biopsies75 and detection in serum of histamine76 and tryptase.77 This mechanism is certain in anaphylaxis when mast-cell degranulation is induced by IgE antibodies, but remains unclear in EIAn. In fact, even in FDEIAn, despite the patient being sensitized to specific foods, the food ingestion alone is unable to trigger the reaction, which occurs instead when there is physical exertion after eating the food. Therefore, other pathophysiological mechanisms are likely to be involved. The recent European Academy of Allergy and Clinical Immunology (EAACI) position statement on EIAn reviewed the current hypotheses proposed to explain this kind of anaphylaxis.78 The first hypothesis concerns the increase in gastrointestinal permeability that should be caused by relaxation of the intestinal tight junctions induced by thermal injuries, NSAID intake, prolonged exercise allowing the passage of large molecules triggering EIAn,47 or by impairment of gut permeability resulting in endotoxins entering the circulation, the latter being associated only with very prolonged exercise.79 Another mechanism altering the gut mucosa should concern wheat as a causative food, and particularly its antigen ω5-gliadin, because of alterations in tissue transglutaminase, resulting in peptide aggregation and increased IgE cross-linking;80 augmented production of IL-6 occurring during exercise, which increases the expression of tissue transglutaminase,81 should favor this mechanism.
Other hypotheses have focused on the effect of physical exertion on blood. The redistribution of blood flow from visceral organs to skeletal muscle, skin, and heart caused by even light exercise is well known. Since this also results in transport of allergens from the gut, where mast cells have precise functional and metabolic characteristics, to the skin and skeletal muscle, where there are phenotypically different mast cells, an altered mediator release should occur.82 In addition, the known increase in plasma osmolality caused by prolonged exercise should rise basophil releasability and histamine production.83 Finally, the changes in acid–base balance associated with exercise should lead to a cellular-reduced pH, triggering mast-cell degranulation.84 The authors of the EAACI position statement accurately revised the available literature, concluding that all the proposed mechanisms lacked validity and recommending the development of a global research network on EIAn to gain sufficient power for scientific evaluation.78
Diagnosis of EIAn
The diagnosis of EIAn is not simple. The first component is a history of symptoms suggesting anaphylaxis, with involvement of cutaneous, respiratory, gastrointestinal, and cardiovascular systems within 2 hours, often within 30 minutes, from exposure to a causative agent.1,2 In the case of EIAn, the agent is physical exertion, regardless of its intensity, but quite frequently a cofactor is needed to elicit the reaction. Therefore, clinical history must be very accurate to identify the cofactor, with major importance for foods, followed by NSAIDs and more rarely warm or cold temperature. Concerning foods, a large array of foodstuffs may be responsible, but cereals, peanuts, tree nuts, tomatoes, and seafood are more frequently involved. Allergy testing, including skin tests and in vitro tests, is indicative of sensitization, but its results must be combined with the history to detect the culprit food.
Laboratory testing
In vitro testing offers the advantage of assessing sensitization to single allergen molecules in place of whole-allergen extracts by the technique of component-resolved diagnosis, thus providing better precision.85 For example, in ten patients with suspected FDEIAn from wheat, high levels of IgE against ω5-gliadin were detected in all cases.86 Of interest, in a patient with wheat-dependent EIAn, the responsible allergen was identified as LTP and not ω5-gliadin.62 On the other hand, LTPs were reported to be the most frequent primary allergens in a group of Italian patients with FDEIAn.87 Also, a role for the basophil-activation test, which is based on the expression of CD203c on the basophil surface following incubation with the causative allergen, is emerging in FDEIAn.85
In vivo testing
In diagnosing food allergy, the in vivo test to be considered as a reference standard is challenge with the suspected food.70,88 In patients with suspected EIAn or FDEIAn, the challenge must be performed under strict medical control, with blood pressure and lung-function monitoring and prompt availability of drugs and equipment to manage anaphylaxis. First, an exercise test on fasting should be performed. If positive, the diagnosis of EIAn is achieved; if negative, an exercise test after 1 hour from the assumption of the suspected food should follow.15 Still, the test may give false-negative results.43 The need of concomitant factors, such as cold or warm temperature58,40 or other particular characteristics of the environment where EIAn occurred, may partly account for such outcome.16 Also, in 34 patients with wheat-dependent EIAn, a positive challenge was obtained only by using oral gluten flour (four patients) or gluten plus consumption of acetylsalicylic acid and alcohol as cofactors (ten patients), which were associated with significantly increased plasma gliadin levels.68 Regardless of the food suspected, when the results of the open challenge in patients with FDEIAn are positive but doubtful, a double-blind placebo-controlled combined food–exercise challenge is indicated.89
Treatment and prevention of EIAn
The acute treatment of EIAn does not differ from the treatment of anaphylaxis in general, being based as first-line intervention on epinephrine 1:1,000 (1 mg/mL) at a dose of 0.2–0.5 mg in adults and 0.01 mg/kg in children, by the intramuscular route. The role of corticosteroids and antihistamines, though they are more used than epinephrine, is ancillary.1,2 Also, patients with EIAn must carry with them an epinephrine autoinjector to be used quickly in case of a reaction, following detailed instructions by physicians on how to use it.1,2 Another important factor in anaphylaxis is that the patient must be placed or place themselves in the Trendelenburg position (lying on the back with legs elevated), in order to prevent the “empty-ventricle syndrome” and to favor blood flow to the heart.90
The best prevention is educating the patients in avoiding the triggers, ie, physical exercise when EIAn without a cofactor is concerned or avoiding the various cofactors. If the cofactor is a food, its ingestion before exercise or within 1 hour after exercise in FDEIAn must be abolished.16 Concerning prophylactic drug treatment, there are reports suggesting the utility of chromones, antihistamines, leukotriene antagonists, and corticosteroids, but scientific evidence supporting their recommendation is lacking.15,16 The effectiveness of prevention measures was evaluated in a study on 279 patients with EIAn with an average duration of 10.6 years of anaphylactic reactions (most frequently triggered by such activities as jogging or brisk walking). It was found that the frequency of EIAn attacks had decreased (47% of patients) or stabilized (46% of patients) compared to the onset of the disease; 41% of patients reported they were completely free of attacks in the past year. The frequency of the attacks was reduced by avoiding exercise during extremely hot or cold weather (44%), avoiding eating certain foods before exercise (37%), and restricting exercise during seasonal allergy (36%) or humid weather (33%). The most common pharmacologic agents used to manage symptoms were H1 antihistamines (56%) and/or epinephrine (31%), but 28% of patients did not use any treatment.91
In FDEIAn, desensitizing the patient to the causative food(s) should have a critical role in preventing the reactions, comparable to immunotherapy with Hymenoptera venom in patients with anaphylaxis from insect stings. However, though an increasing number of studies on oral, sublingual, and recently also epicutaneous immunotherapy have been published, immunotherapy for foods is not yet approved in a consensus document, and due to the unavailability of commercial preparations is not included in clinical practice.92
Conclusion
EIAn and FDEIAn are rare disorders that need a careful diagnosis, because they are associated with a risk of life-threatening anaphylactic reactions. The diagnostic workup is quite demanding, and (especially for FDEIAn) requires thorough investigation to identify the culprit food. The two mainstays of management are early treatment of the reaction by epinephrine, especially through patient self-administration using an autoinjector, and prevention of further episodes. The latter needs adequate information and education of patients on how to keep away from the specific triggers.
Disclosure
The authors report no conflicts of interest in this work.
References
Simons FE, Ebisawa M, Sanchez-Borges M, et al. 2015 Update of the evidence base: World Allergy Organization anaphylaxis guidelines. World Allergy Organ J. 2015;8:32. | ||
Muraro A, Roberts G, Worm M, et al. Anaphylaxis: guidelines from the European Academy of Allergy and Clinical Immunology. Allergy. 2014;69:1026–1045. | ||
Gaspar A, Santos N, Piedade S, et al. One-year survey of paediatric anaphylaxis in an allergy department. Eur Ann Allergy Clin Immunol. 2015;47:197–205. | ||
Wood RA, Camargo CA, Lieberman P, et al. Anaphylaxis in America: the prevalence and characteristics of anaphylaxis in the United States. J Allergy Clin Immunol. 2014;133:461–467. | ||
Sicherer SH, Leung DY. Advances in allergic skin diseases, anaphylaxis, and hypersensitivity reactions to foods, drugs, and insect in 2014. J Allergy Clin Immunol. 2015;135:357–367. | ||
Lieberman P, Nicklas RA, Randolph C, et al. Anaphylaxis: a practice parameter update 2015. Ann Allergy Asthma Immunol. 2015;115:341–384. | ||
Stevenson DD. Aspirin and NSAID sensitivity. Immunol Allergy Clin North Am. 2004;24:491–505. | ||
Rossi F, Incorvaia C, Mauro M. [Hypersensitivity reactions to chemotherapeutic antineoplastic agents]. Recenti Prog Med. 2004;95:476–481. Italian. | ||
Mirone C, Preziosi D, Mascheri A, et al. Identification of risk factors of severe hypersensitivity reactions in general anaesthesia. Clin Mol Allergy. 2015;13:11. | ||
Puxeddu I, Caltran E, Rocchi V, Del Corso I, Tavoni A, Migliorini P. Hypersensitivity reactions during treatment with biological agents. Clin Exp Rheumatol. 2016;34:129–132. | ||
Picard M, Giavina-Bianchi P, Mezzano V, Castells M. Expanding spectrum of mast cell activation disorders: monoclonal and idiopathic mast cell activation syndromes. Clin Ther. 2013;35:548–562. | ||
Valent P, Akin C, Arock M, et al. Definitions, criteria and global classification of mast cell disorders with special reference to mast cell activation syndromes: a consensus proposal. Int Arch Allergy Immunol. 2012;157:215–225. | ||
Schwartz LB. Diagnostic value of tryptase in anaphylaxis and mastocytosis. Immunol Allergy Clin North Am. 2006;26(3):451–463. | ||
Gülen T, Hägglung H, Sander B, Dahlén B, Nilsson G. The presence of mast cell clonality in patients with unexplained anaphylaxis. Clin Exp Allergy. 2014;44:1179–1187. | ||
Barg W, Medrala W, Wolanczyk-Medrala A. Exercise-induced anaphylaxis: an update on diagnosis and treatment. Curr Allergy Asthma Rep. 2011:11:45–51. | ||
Dascola CP, Caffarelli C. Exercise-induced anaphylaxis: a clinical view. Ital J Pediatr. 2012;38:43. | ||
Bonini M, Palange P. Anaphylaxis and sport. Curr Opin Allergy Clin Immunol. 2014;14:323–327. | ||
Aihara Y, Takahashi Y, Kotoyori T, et al. Frequency of food-dependent, exercise-induced anaphylaxis in Japanese junior-high-school students. J Allergy Clin Immunol. 2001;108:1035–1039. | ||
Wölbing F, Fischer I, Köberle M, Kaesler S, Biedermann T. About the role and underlying mechanisms of cofactors in anaphylaxis. Allergy. 2013;68:1085–1092. | ||
Maulitz RM, Pratt DS, Schocket AL. Exercise-induced anaphylactic reaction to shellfish. J Allergy Clin Immunol. 1979;63:433–434. | ||
Kidd JM, Cohen SH, Fink JN. Food-dependent exercise-induced anaphylaxis. J Allergy Clin Immunol. 1983;71:407–411. | ||
Buchbinder EM, Bloch KJ, Moss J, Guiney TE. Food dependent exercise-induced anaphylaxis. JAMA. 1983;250:2973–2974. | ||
Sheffer AL, Austen KF. Exercise-induced anaphylaxis. J Allergy Clin Immunol. 1984;73:699–703. | ||
Kushimoto H, Aoki T. Masked type 1 wheat allergy. Arch Dermatol. 1985;121:355–360. | ||
McNeill D, Strauss R. Exercise-induced anaphylaxis related to food intake. Ann Allergy. 1988;61:440–442. | ||
Akutsu I, Motojima S, Ikeda YY, Fukuda T, Ikemori R, Makino S. [Three cases of food-dependent exercise-induced anaphylaxis]. Arerugi. 1989;38:277–284. Japanese. | ||
Debavelaere C, De Blic J, Bodemer C, Teillac D, Paupe J, Scheinmann P. Syndrome d’anaphylaxie induite par l’exervise. Arch Fr Pediatr. 1989;46:281–283. | ||
Dohi M, Suko M, Sugiyama H, et al. Food dependent exercise-induced anaphylaxis: a study on 11 Japanese cases. J Allergy Clin Immunol. 1991;87:34–40. | ||
Fukutomi O, Kondo N, Agata H, Shinoda S, Shinbara M, Orii T. Abnormal responses of the autonomic nervous system in food-dependent exercise-induced anaphylaxis. Ann Allergy. 1992;68:438–445. | ||
Añíbarro B, Domínguez C, Díaz JM, et al. Apple-dependent exercise-induced anaphylaxis. Allergy. 1994;49:481–482. | ||
Muñoz FM, Cazaña JM, Villas F, Contreras JF, Díaz JM, Ojeda JA. Exercise-induced anaphylactic reaction to hazelnut. Allergy. 1994;314–316. | ||
Tilles S, Shocket A, Milgrom H. Exercise-induced anaphylaxis related to specific foods. J Pediatr. 1995;127:587–589. | ||
Caffarelli C, Terzi V, Perrone F, Cavagni G. Food-related, exercise-induced anaphylaxis. Arch Dis Child. 1996;75:141–144. | ||
Caffarelli C, Terzi V, Perrone F. Exercise-induced anaphylaxis related to cuttlefish intake. Eur J Pediatr. 1996;155:1025–1026. | ||
Asero R, Mistrello G, Roncarolo D, Antoniotti P, Falagiani P. Exercise-induced egg anaphylaxis. Allergy. 1997;52:687–689. | ||
Okano M, Sakuma Y. Food-dependent exercise-induced anaphylaxis due to matsutake mushrooms. Br J Dermatol. 1997;136:805. | ||
Biedermann T, Schöpf P, Ruëff F, Przybilla B. [Exertion-induced anaphylaxis after eating pork and beef]. Dtsch Med Wochenschr. 1999;124:456–458. German. | ||
Longo G, Barbi E, Puppin F. Exercise-induced anaphylaxis to snails. Allergy. 2000;55:513–514. | ||
Kano H, Juji F, Shibuya N, et al. [Clinical courses of 18 cases with food-dependent exercise-induced anaphylaxis]. Arerugi. 2000;49:472–478. Japanese. | ||
Shimizu T, Furumoto H, Kinoshita E, et al. Food-dependent exercise-induced anaphylaxis occurring only in winter. Dermatology. 2000;200:279. | ||
Harada S, Horikawa T, Ashida M, et al. Aspirin enhances the induction of type I allergic symptoms when combined with food and exercise in patients with food-dependent exercise-induced anaphylaxis. Br J Dermatol. 2001;145:336–339. | ||
Noma T, Yoshizawa I, Ogawa N, Ito M, Aoki K, Kawano Y. Fatal buckwheat dependent exercise-induced anaphylaxis. Asian Pac J Allergy Immunol. 2001;19:283–286. | ||
Romano A, Di Fonso M, Giuffreda F, et al. Food-dependent exercise-induced anaphylaxis: clinical and laboratory findings in 54 subjects. Int Arch Allergy Immunol. 2001;125:264–272. | ||
Pérez-Calderón R, Gonzalo-Garijo MA, Fernández de Soria R. Exercise-induced anaphylaxis to onion. Allergy. 2000;57:752–753. | ||
Mathelier-Fusade P, Vermeulen C, Leynader F. Responsibility of food in exercise-induced anaphylaxis: 7 cases. Ann Dermatol Venereol. 2002;129:694–697. | ||
García-Ara MC, Sánchez AV, Martinez MT, Díaz Pena JM. Cow’s milk-dependent, exercise-induced anaphylaxis: case report of a patient with previous allergy to cow’s milk. J Allergy Clin Immunol. 2003;111:647–648. | ||
Matsuo H, Morimoto K, Asaki T, et al. Exercise and aspirin increase levels of circulating gliadin peptides in patients with wheat-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2005;35:461–466. | ||
Porcel S, Sanchez AB, Rodriguez E, et al. Food-dependent exercise-induced anaphylaxis to pistachio. J Investig Allergol Clin Immunol. 2006;16:71–73. | ||
Tewari A, Du Toit G, Lack G. The difficulties of diagnosing food-dependent exercise-induced anaphylaxis in childhood: a case study and review. Pediatr Allergy Immunol. 2006;17:157–160. | ||
Wong CG, Mace SR. Food-dependent exercise-induced anaphylaxis: a case related to chickpea ingestion and review. Allergy Asthma Clin Immunol. 2007;3:134–137. | ||
Oyefara BI, Bahna SL. Delayed food-dependent exercise-induced anaphylaxis. Allergy Asthma Proc. 2007;28:64–66. | ||
Du Toit G. Food-dependent exercised-induced anaphylaxis in childhood. Pediatr Allergy Immunol. 2007;18:455–463. | ||
Orhan F, Karakas T. Food-dependent exercise-induced anaphylaxis to lentil and anaphylaxis to chickpea in a 17-year-old boy. J Investig Allergol Clin Immunol. 2008;18:465–468. | ||
Pacharn P, Jiraponggsananuruk O, Daengsywan T, Vichyanond P, Visitsunthorn N. Wheat-dependent, exercise-induced anaphylaxis in Thai children: a report of 5 cases. Asian Pac J Allergy Immunol. 2009;27:115–120. | ||
Mu XL, Yu J, Gao ZC. [Food-dependent exercise-induced anaphylaxis: case report and review of literature]. Zhonghua Jie He He Hu Xi Za Zhi 2009;32:923–925. Chinese. | ||
Baek CH, Bae YJ, Cho YS, Moon HB, Kim TB. Food-dependent exercise-induced anaphylaxis in the celery-mugwort-birch-spice syndrome. Allergy. 2010;65:792–793. | ||
Bianchi A, Businco AR, Bondanini F, Mistrello G, Carlucci A, Tripodi S. Rosaceae-associated exercise-induced anaphylaxis with positive SPT and negative IgE reactivity to Pru p 3. Eur Ann Allergy Clin Immunol. 2011;43:122–124. | ||
Jo EJ, Yang MS, Kim YJ, et al. Food-dependent exercise-induced anaphylaxis occurred only in a warm but not in a cold environment. Asia Pac Allergy. 2012;2:161–164. | ||
Ahanchian H, Farid R, Ansari E, et al. Food-dependent exercise-induced anaphylaxis due to wheat in a young woman. Iran J Allergy Asthma Immunol. 2013;12:93–95. | ||
Kaneko M, Yagi H, Koyama H, et al. [A case of apple allergy with initial symptoms like food-dependent exercise-induced anaphylaxis]. Arerugi. 2013;62:698–703. Japanese. | ||
Mobayed HM, Al-Nesf MA. Two cases of food-dependent exercise-induced anaphylaxis with different culprit foods. Ann Thorac Med. 2014;9:42–44. | ||
Pastorello EA, Farioli L, Stafylaraki C, et al. Wheat-dependent exercise-induced anaphylaxis caused by a lipid transfer protein and not by ω-5 gliadin. Ann Allergy Asthma Immunol. 2014;112:386–387.e1. | ||
de Silva NR, Dasanayake WM, Karunatilleke C, Malavige GN. Food dependant exercise induced anaphylaxis a retrospective study from 2 allergy clinics in Colombo, Sri Lanka. Allergy Asthma Clin Immunol. 2015;25;11:22. | ||
Ono R, Motomura C, Takamatsu N, et al. [A case of food-dependent exercise-induced anaphylaxis caused by ingestion of orange]. Arerugi. 2015;64:149–155. Japanese. | ||
Iijima S, Ito M, Makabe K, Murakami Y, Yokooji T, Matsuo H. Case of food-dependent exercise-induced anaphylaxis due to Japanese apricot and peach: detection of causative antigens. J Dermatol. 2015;42:916–917. | ||
Kobayashi T, Ito T, Kawakami H, et al. Eighteen cases of wheat allergy and wheat-dependent exercise-induced urticarial/anaphylaxis sensitized to hydrolyzed wheat protein in soap. Int J Dermatol. 2015;54:302–305. | ||
Roberts H, Ben-Shoshan M. Food-dependent exercise-induced anaphylaxis to chickpea in a 17-year-old female: a case report. J Med Case Rep. 2015;9:186. | ||
Brockow K, Kneissl D, Valentini L, et al. Using a gluten oral food challenge protocol to improve diagnosis of wheat-dependent exercise-induced anaphylaxis. J Allergy Clin Immunol. 2015;135:977–984. | ||
Hotta A, Inomata N, Tanegasima T, Oda K, Inoue Y, Aihara M. Case of food-dependent exercise-induced anaphylaxis due to peach with Pru p 7 sensitization. J Dermatol. 2016;43:222–223. | ||
Asaumi T, Yanagida N, Sato S, et al. Provocation tests for the diagnosis of food-dependent exercise-induced anaphylaxis. Pediatr Allergy Immunol. 2016;27:44–49. | ||
Novey HS, Fairshter RD, Salness K, Simon RA, Curd JG. Post-prandial exercise-induced anaphylaxis. J Allergy Clin Immunol. 1983;71:498–504. | ||
Aihara K, Kotoyori T, Takahashi Y, Osuna H, Ohnuma S, Ikezawa Z. The necessity for dual food intake to provoke food-dependent exercise-induced anaphylaxis (FEIAn): a case report of FEIAn with simultaneous intake of wheat and umeboshi. J Allergy Clin Immunol. 2001;107:1100–1105. | ||
Katsunuma T, Ikura Y, Nagakura T, et al. Exercise-induced anaphylaxis: improvement after removal of amalgam in dental caries. Ann Allergy. 1990;64;472–475. | ||
Montgomery SL. Cholinergic urticaria and exercise-induced anaphylaxis. Curr Sports Med Rep. 2015;14:61–63. | ||
Sheffer AL, Tong AK, Murphy GK, et al. Exercise-induced anaphylaxis: a serious form of physical allergy associated with mast cell degranulation. J Allergy Clin Immunol. 1985;75:479–484. | ||
Volcheck G, Li JT. Exercise-induced urticaria and anaphylaxis. Mayo Clin Proc. 1997;72:140–147. | ||
Schwartz HJ. Elevated serum tryptase in exercise-induced anaphylaxis. J Allergy Clin Immunol. 1995;95:917–919. | ||
Ansley L, Bonini M, Delgado L, et al. Pathophysiological mechanisms of exercise-induced anaphylaxis: an EAACI position statement. Allergy. 2015;70:1212–1221. | ||
Jeukendrup AE, Veet-Jop K, Sturk A, et al. Relationship between gastro-intestinal complaints and endotoxaemia, cytokine release and the acute-phase reaction during and after a long-distance triathlon in highly trained men. Clin Sci (Lond). 2000;98:47–55. | ||
Nurminskaya MV, Belkin AM. Cellular functions of tissue transglutaminase. Int Rev Cell Mol Biol. 2012;294:1–97. | ||
Pedersen BK, Steensberg A, Schjerling P. Exercise and interleukin-6. Curr Opin Hematol. 2001;8:137–141. | ||
Heavey DJ, Ernst PB, Stevens RL, Befus AD, Bienenstock J, Austen KF. Generation of leukotriene C4, leukotriene B4, and prostaglandin D2 by immunologically activated rat intestinal mucosa mast cells. J Immunol. 1988;140:1953–1957. | ||
Barg W, Wolanczyk-Medrala A, Obojski A, Wytrychowski K, Panaszek B, Medrala W. Food-dependent exercise-induced anaphylaxis: possible impact of increased basophil histamine releasability in hyperosmolar conditions. J Investig Allergol Clin Immunol. 2008;18:312–315. | ||
Wasserman K, Cox TA, Sietsema KE. Ventilatory regulation of arterial H(+) (pH) during exercise. Respir Physiol Neurobiol. 2014;190:142–148. | ||
Morita E, Chinuki Y, Takahashi H. Recent advances of in vitro tests for the diagnosis of food-dependent exercise-induced anaphylaxis. J Dermatol Sci. 2013;71:155–159. | ||
Brans R, Sauer I, Czaja K, Pfutzner W, Merk HF. Microarray-based detection of specific IgE against recombinant ω-5-gliadin in suspected wheat-dependent exercise-induced anaphylaxis. Eur J Dermatol. 2012;22:358–362. | ||
Romano A, Scala E, Rumi G, et al. Lipid transfer proteins: the most frequent sensitizer in Italian subjects with food-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2012;42:1643–1653. | ||
Macchia D, Melioli G, Pravettoni V, et al. Guidelines for the use and interpretation of diagnostic methods in adult food allergy. Clin Mol Allergy. 2015;13:27. | ||
Fiocchi A, Mirri GP, Santini I, et al. Exercise-induced anaphylaxis after food contaminants ingestion in double-blinded, placebo-controlled, food-exercise challenge. J Allergy Clin Immunol. 1997;100:424–425. | ||
Pumphrey RS. Fatal posture in anaphylactic shock. J Allergy Clin Immunol. 2003;112:451–452. | ||
Shadick NA, Liang MH, Partridge AJ, et al. The natural history of exercise-induced anaphylaxis: survey results from a 10-year follow-up study. J Allergy Clin Immunol. 1999;104:123–127. | ||
Wood RA. Food allergen immunotherapy: current status and prospects for the future. J Allergy Clin Immunol. 2016;137:973–982. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.