Back to Journals » OncoTargets and Therapy » Volume 12
Diagnosis and treatment of synchronous multiple primary lung cancer – a case report
Authors Bao Y, Wu J, Zhang J, Yu Y
Received 9 August 2018
Accepted for publication 21 January 2019
Published 29 May 2019 Volume 2019:12 Pages 4281—4285
DOI https://doi.org/10.2147/OTT.S183319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Yi Bao,1,2 Jiayuan Wu,1 Jun Zhang,3 Yawei Yu4
1The Key Laboratory, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China; 2The Department of Oncology, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China; 3The Department of Thoracic Surgery, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China; 4The Department of Pathology, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China
Abstract: The incidence of synchronous multiple primary lung cancer (SMPLC) has been increased in recent years. Because of a variance in clinical management and outcome, it is important to distinguish SMPLC from a primary tumor with intrapulmonary metastases. Here, we reported a diagnosis and treatment procedure regarding a case of a 58‐year‐old woman who presented with synchronous multiple tumor lesions in separate lungs. Using a next generation sequencing technology, a discordant EGFR gene profile from the separate lungs was revealed for this patient. After standard treatment procedures, the therapeutic effects were evaluated by response evaluation criteria in solid tumors (RECIST). This case shows an essential role in the combination of molecular features, together with pathological analysis, during the management of SMPLC, but challenges still required considering during dealing the cases of SMPLC.
Keywords: lung adenocarcinoma, SMPLC, genetic features, EGFR
Introduction
Lung adenocarcinoma (AC) has become the most dominant subtype of non-small cell lung cancer (NSCLC) in recent years.1 According to the literature, up to 1–8% of lung cancer patients had been reported to be synchronous multiple primary lung cancer (SMPLC) with heterogeneous origins.2 Additionally, meterochronous primary lung cancer has been reported approximately 1% annually.3
Because of a variance in clinical management and outcome, it is essential to distinguish SMPLC from a primary tumor with intrapulmonary metastases. It may be relatively easy to distinguish these two diseases in the presence of discordant histological features in the different tumor tissues; however, in some cases, the identical histology may provide difficulties in discriminating between these two diseases via morphological analyses only. Therefore, exploring genetic features in each individual tumor lesion may provide extra clues for deciphering SMPLC from lung metastases.4,5 In this article, we reported a SMPLC case to emphasize the key role of combining molecular features obtained from each tumor lesion together with pathological analysis in the diagnosis of SMPLC; meanwhile, challenges still need to be solved during diagnosis and treatment of SMPLC.
Case report
A 58-year-old woman was hospitalized after 10 days of fever and cough in June 2015. The patient had a no smoking history. Chest computed tomography (CT) revealed two solid lesions located at the bottom lobes of the right (Figure 1A) and left lungs (Figure 1B). The patient reported no family history of lung cancer. Needle biopsies were performed for both lesions under CT guidance. After histological examination, invasive adenocarcinoma was suggested after observation of acinar cells with abnormal shape and size of nucleus in the bottom lobe of the right lung (Figure 2A, Magnification×200, and Figure 2B, Magnification×400), and in the bottom lobe of the left lung (Figure 2C Magnification×200 and Figure 2D Magnification×400); subsequently the diagnosis was confirmed by immunohistochemistry analysis with biomarker profiles of cytokeratin7 (CK) (+), thyroid transcription factor-1, (TTF-1) (+), CK5/6 (–), P63 (–) from the left lung tumor tissue, and a profile of CK7 (+), TTF-1 (+), CK5/6 (–), and P63 (+) from the right lung tumor tissue.
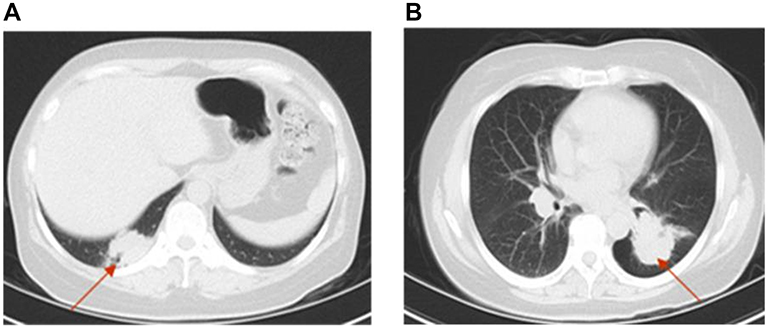 | Figure 1 Chest computed tomography (CT) scans were performed and images were recorded prior to any therapies. (A) The arrow shows a 24.1 mm×32.4 mm size lesion in the bottom lobe of the right lung. (B) The arrow shows a 49.0 mm×32.6 mm size lesion in the bottom lobe of the left lung. |
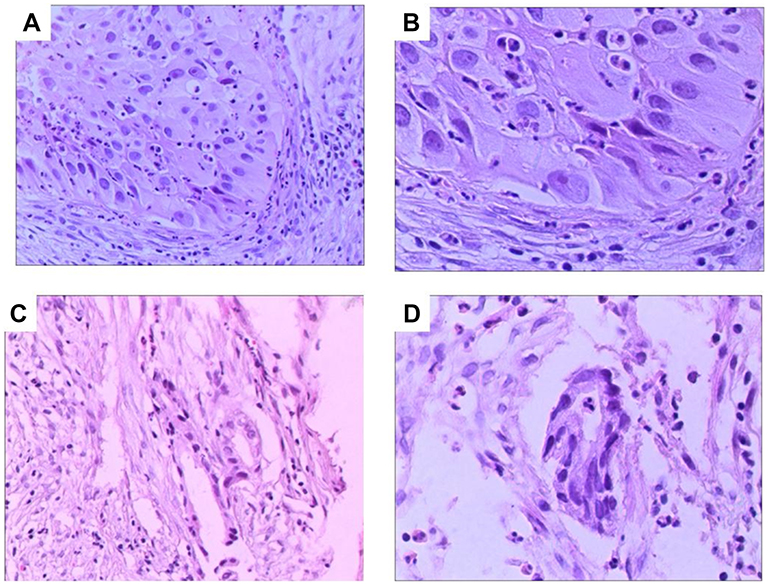 | Figure 2 Histologic features from synchronous multiple tumors. Hematoxylin and Eosin (H and E) staining revealed lung adenocarcinoma at both sides. Tissues were obtained by core needle biopsy from the bottom lobe of the right lung and the subsequent resection specimen demonstrated an Acinar-Predominant AC (A, Magnification×200 and B, Magnification×400). Tissues were obtained by core needle biopsy from the bottom lobe of the left lung and the subsequent resection specimen demonstrated an Acinar-Predominant AC (C, magnification×200 and D, magnification×400). Abbreviation: AC, adenocarcinoma. |
Genetic features of the paraffin-embedded primary tumor tissues from each tumor lesion of the lungs were analyzed by using a next-generation sequencing technology (a TruSight Tumor 15 panel, Illumina platform). The detailed genes information of this panel is shown in Table 1. Small in-frame deletions in exon 19 of the epidermal growth factor receptor (EGFR) gene were detected in the tissue from the right lung, whereas no mutations of exons 18, 19, 20, or 21 of EGFR were revealed in the tumor tissue obtained from the left lung. These data were further confirmed by using Sanger sequencing and the amplification refractory mutation system (ARMS)-PCR technologies. With a combination of the pathological and molecular analyses, the patient was considered as synchronous multiple primary lung AC.
 | Table 1 Gene content on TruSight tumor 15 |
In order to identify the stages of SMPLC and select suitable treatment strategies, a whole body examination was performed and bone metastasis was indicated by a magnetic resonance imaging (MRI) scan. However,the patient refused a further bone biopsy, and, therefore, we were unable to clarify the pathological and genetic characteristics of the metastatic site. Nevertheless, at least one primary site of lung lesion should be stage IV adenocarcinoma on the basis of TNM staging lung cancer.6 Initially, she was treated with four cycles of pemetrexed (500 mg/m2 on day 1, every 3 weeks) and cisplatin (25 mg/m2 on days 1–3, every 3 weeks). The response of the patient with chemotherapy was valued in accordance with the Response Evaluation Criteria in Solid Tumor (RECIST). The chest CT images were obtained after four cycles of chemo treatment, illustrating a dramatic shrinkage of the tumor size from 24.1 mm×32.4 mm to 9 mm×9 mm in the bottom lobe of the right lung (Figure 3A). A slight shrinkage of the tumor lesion from 49.0 mm×32.6 mm to 41 mm×38 mm was detected in the bottom lobe of the left lung (Figure 3B). Unfortunately, newly metastatic lesions in the brain were indicated by a MRI scan after full body examination. The patient was judged as progressive disease (PD), but she refused any alternative chemotherapy protocols and whole brain radiation. She was prescribed icotinib, a tyrosine kinase inhibitor (three times per day at a dose of 125 mg). After 2 months of drug treatment, a chest CT scan was conducted again to evaluate the responding effects of the drugs. The images revealed that the size of the tumor lesion in the right lung was further decreased from 9 mm×9 mm to 5 mm×5 mm (Figure 3C); whereas, the lung-tumor burden in the left lung continuously progressed from 41 mm×38 mm to 55 mm×46 mm (Figure 3D). Additionally, the increased sites of metastatic lesions in the brain suggested a failure of tyrosine kinase inhibitor (TKI) treatment.
 | Figure 3 Chest computed tomography (CT) scans were performed and images were recorded after. (A) The arrow shows a 9.0 mm×9.0 mm lesion in the bottom lobe of the right lung after four cycles of chemotherapy; (B) The arrow shows a 41.0 mm×38.0 mm lesion in the bottom lobe of the left lung after fourcycles of chemotherapy; (C) The arrow showsa 5.0 mm×5.0 mm lesion in the bottom lobe of the right lung after 2months of icotinib; (D) The arrow shows a 55.0 mm×46 mm lesion in the bottom lobe of the left lung after 2months of icotinib. |
Discussion
In clinical practice, it may be a favorable strategy to conduct genetic analysis in each tumor lesion if SMPLC is considered to be present. In this study, we provided a SMPLC case with detailed diagnosis and treatment procedures. This case evidently suggested that the combination of genetic features together with traditional histology should be a standard way for identifying SMPLC compared with using morphology only. However, there are still several issues which need to be addressed for SMPLC from this case.
First, studies are needed to answer how many genes should be included in a well-established genetic panel and what is the most convenient, affordable, and time-saving technology to obtain these genetic features. Based on previous reports, point mutations of EGFR, KRAS, P53, and genetic rearrangement of ALK are relatively higher in lung AC.7 EGFR is the most predominant driver mutation gene in AC patients, particularly in East-Asian populations.8 In our study, compared with other genes including KRAS and P53, EGFR appears to be the most important biomarker for separating SMPLC from primary lung cancer with intrapulmonary metastasis. We used a commercial kit with a 15 genes panel via generating data from an Illumine platform. In our case, EGFR gene mutation was revealed in one tumor site but not in the other site, and, therefore, discordant biological traits should be present in the tumor tissues of this patient. However, obviously, these 15 genes may not be sufficient for screening multiple intrapulmonary neoplasms, and investigation should be conducted among a large scale of patients in order to establish a standard schedule, for instance, there may be coincidental acquisition of the same hotspot mutations in EGFR in clonally different tumors. In addition, although the discordance of a driver gene mutation is present in the two tumor sites, we agree that the heterogeneous characteristics of tumors still need to be considered during diagnosis. Therefore, a 15 genes panel may be insufficient, and further studies are needed to establish a feasible gene panel which is comprehensive for identifying molecular features in each tumor lesion. Moreover, the rearrangement of ALK has been excluded in the panel of this study. Rearrangement of ALK was reported as 6.4% in AC patients in a Western population and 5.4% in an Asia population.8
Second, it may be argued that, without a surgical procedure, it is hard to discriminate the complete pathological features of individual tumor lesion, and, therefore, it cannot use the application of Martini-Melamed criteria.9
Third, we may also raise the question of the value of using circulating tumor-specific DNA (ctDNA) if the presence of multiple neoplasms in the same patient. ctDNA has been proposed to be an important alternative source for genetic analysis due to the convenience of obtaining samples and the development of a more sensitive digital PCR (ddPCR) method to detect gene mutation profiles. Currently, ddPCR has been reported to have a capacity for detecting approximately <0.01% hotspot mutations.10 However, with the presence of multiple tumor lesions, it is hard to discriminate the original derivation in patients with SMPLC using ctDNA to detect gene mutations. Therefore, ctDNA analysis may not be suitable for patients with multiple tumor lesions before the initial target therapy.
Finally, we consider that a platinum-based chemotherapy protocol should be a proper initial therapy for those with discordant EGFR genetic features for the multiple tumor lesions. Pemetrexed has frequently been selected as a first-line drug for patients with lung AC due to its comparable efficacy and well-tolerated toxicities. The patient achieved a partial response in accordance with both sites of primary tumor lesions in the lungs. It is still unclear whether patients who have discordant EGFR mutation features in the multiple tumor lesions would have any beneficial effect from using tyrosine kinase inhibitors after initial chemotherapy failed.
Taken together, in this case, we report the critical need of combining genetic features together with traditional histological analysis in the diagnosis of SMPLC, as well as the problems needed to solve it in the future.
Ethics s tatement
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Jiaxing (Jiaxing, China), and written informed consent was obtained from the studied individual for publication of the case details and images. The manuscript was approved to be published by the Second Affiliated Hospital of Jiaxing (Jiaxing, China).
Acknowledgments
This study was supported by grants from Science and Technology Bureau of Jiaxing (Jiaxing, China; grant no: 2016AY23054); Health Bureau of Zhejiang Province (Hangzhou, China; grant no: 2016KYB292); Natural Science Foundation of Zhejiang Province (Hangzhou, China; grant no: LY16H070007); and Chinese National Science Fund for Young Scholars (Beijing, China; grant no: 81101707).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208
2. Loukeri AA, Kampolis CF, Ntokou A, Tsoukalas G, Syrigos K. Metachronous and synchronous primary lung cancers: diagnostic aspects, surgical treatment, and prognosis. Clin Lung Cancer. 2015;16(1):15–23. doi:10.1016/j.cllc.2014.07.001
3. Johnson BE. Second lung cancers in patients after treatment for an initial lung cancer. J Natl Cancer Inst. 1998;90(18):1335–1345.
4. Warth A, Macher-Goeppinger S, Muley T, et al. Clonality of multifocal nonsmall cell lung cancer: implications for staging and therapy. Eur Respir J. 2012;39(6):1437–1442. doi:10.1183/09031936.00105911
5. Zhang Y, Hu H, Wang R, et al. Synchronous non-small cell lung cancers: diagnostic yield can be improved by histologic and genetic methods. Ann Surg Oncol. 2014;21(13):4369–4374. doi:10.1245/s10434-014-3840-1
6. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
7. Sun Y, Ren Y, Fang Z, et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J Clin Oncol. 2010;28(30):4616–4620. doi:10.1200/JCO.2010.29.6038
8. Dearden S, Stevens J, Wu YL, Blowers D. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap). Ann Oncol. 2013;24(9):2371–2376. doi:10.1093/annonc/mdt205
9. Martini N, Melamed MR. Multiple primary lung cancers. J Thorac Cardiovasc Surg. 1975;70(4):606–612.
10. Diaz LA
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.