Back to Journals » Research and Reports in Tropical Medicine » Volume 13
Diagnosis and Clinical Management of Chagas Disease: An Increasing Challenge in Non-Endemic Areas
Authors Suárez C ![]() , Nolder D, García-Mingo A, Moore DAJ
, Nolder D, García-Mingo A, Moore DAJ ![]() , Chiodini PL
, Chiodini PL
Received 17 September 2021
Accepted for publication 16 June 2022
Published 22 July 2022 Volume 2022:13 Pages 25—40
DOI https://doi.org/10.2147/RRTM.S278135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Mario Rodríguez-Pérez
Cristina Suárez,1,2 Debbie Nolder,1,3 Ana García-Mingo,1,4 David AJ Moore,1,5,6 Peter L Chiodini1,5,7
1UK Chagas Hub, London, UK; 2Department of Infection, Barts Health NHS Trust, London, UK; 3Diagnostic Parasitology Laboratory, London School of Hygiene & Tropical Medicine, London, UK; 4Microbiology Department, Whittington Health NHS Trust, London, UK; 5Hospital for Tropical Diseases, University College London Hospitals NHS Trust;, London, UK; 6Department of Clinical Research, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, UK; 7London School of Hygiene and Tropical Medicine, London, UK
Correspondence: Cristina Suárez, Barts Health NHS Trust, Royal London Hospital, Department of Infection, Pharmacy & Pathology Building – 3rd floor, 80 Newark Street, London, E1 2ES, UK, Tel +44 20 3246 0302, Email [email protected]
Abstract: Chagas disease (CD) is caused by the parasite Trypanosoma cruzi, and it is endemic in Central, South America, Mexico and the South of the United States. It is an important cause of early mortality and morbidity, and it is associated with poverty and stigma. A third of the cases evolve into chronic cardiomyopathy and gastrointestinal disease. The infection is transmitted vertically and by blood/organ donation and can reactivate with immunosuppression. Case identification requires awareness and screening programmes targeting the population at risk (women in reproductive age, donors, immunocompromised patients). Treatment with benznidazole or nifurtimox is most effective in the acute phase and prevents progression to chronic phase when given to children. Treating women antenatally reduces but does not eliminate vertical transmission. Treatment is poorly tolerated, contraindicated during pregnancy, and has little effect modifying the disease in the chronic phase. Screening is easily performed with serology. Migration has brought the disease outside of the endemic countries, where the transmission continues vertically and via blood and tissue/organ donations. There are more than 32 million migrants from Latin America living in non-endemic countries. However, the infection is massively underdiagnosed in this setting due to the lack of awareness by patients, health authorities and professionals. Blood and tissue donation screening policies have significantly reduced transmission in endemic countries but are not universally established in the non-endemic setting. Antenatal screening is not commonly done. Other challenges include difficulties accessing and retaining patients in the healthcare system and lack of specific funding for the interventions. Any strategy must be accompanied by education and awareness campaigns directed to patients, professionals and policy makers. The involvement of patients and their communities is central and key for success and must be sought early and actively. This review proposes strategies to address challenges faced by non-endemic countries.
Keywords: Trypanosoma cruzi, antenatal, transplant, migrant, screening, prevention
Introduction
Chagas disease (CD) or American trypanosomiasis is a neglected parasitic disease associated with significant mortality and morbidity that includes long-term disability, social stigma and a mental health toll. Perceived as a disease of the very poor, this infection, once limited to rural areas of Latin America (LA), has now spread via migration to non-endemic areas and countries, where transmission is maintained via non-vectorial routes. The lack of individual and institutional awareness, particularly in non-endemic countries, contributes to the perpetuation of the cycle by failing to identify individuals with the disease or at risk of acquisition, and treatment and prevention opportunities. This review aims, with a specific focus on non-endemic countries, to 1) summarise the current knowledge in epidemiology, diagnostics, treatment and prevention strategies in CD; 2) propose strategies to implement screening and treatment programmes; and 3) identify common challenges.
Methods
Non-systematic literature review of relevant papers, textbooks and grey literature (policy documents, available local and national guidelines, social media and websites of patient and public organisations working with CD). The authors also describe their own experience treating patients with CD and implementing a screening and treatment programme in London, as members of the UK Chagas Hub.1
Epidemiology
Cause, Pathogenesis and Mechanisms of Transmission
CD is caused by the hemoflagellate protozoan Trypanosoma cruzi which is transmitted in endemic areas by species of night-active, blood-sucking triatomine insects (Triatoma, Panstrongylus, and Rhodnius) that live in roofs and wall cracks of houses and peridomestic structures. The flagellate or infective forms of the parasite (trypomastigote) are carried in the host´s blood and acquired by the vector insect during a blood meal; the parasite then develops in the insect´s midgut into epimastigote and later into the metacyclic trypomastigote forms that are excreted with the faeces. These are introduced to the host via breaks in the skin (following or not a bite) or mucosal membranes and invade host cells where they divide intracellularly to form nests of non-flagellated amastigote forms. These may remain quiescent inside the cells but may also revert to trypomastigote and be released to the bloodstream, from where they can either infect other cells or be acquired by the insect vector, closing the cycle.2 T. cruzi infects a broad range of domestic and wild mammals that maintain the domestic and sylvatic lifecycles.3,4 Trypanosoma cruzi responsible for CD can be grouped into seven discrete typing units (DTUs), genetic lineages, TcI to TcVI5 and Tcbat6 . TcI–TcVI parasites, traditionally associated with CD, have diverse ecological niches in endemic areas and associations between parasite lineage and clinical presentation are not clearly defined.7 Tcbat, a lineage recently found in a human case in Ecuador,8 is very closely related to the TcI clade; however, its clinical significance is unknown.
Transmission involves the acquisition of infective forms of the parasite from either the insect vector directly (vectorial) or from blood or tissues (non-vectorial). Vector-borne transmission occurs in endemic areas via contamination with insect faeces of bites of areas of exposed broken skin or mucosal surfaces, typically by rubbing the skin or the eye after an unnoticed night bite or defecation on or close to the conjunctiva. Oral transmission is also possible via contamination of food or drinks by the vector faeces, and it may cause outbreaks.9 Non-vectorial routes of transmission include maternal-fetal, via blood transfusions, solid organ or bone marrow transplant.
Maternal–fetal (congenital) transmission refers to the transmission during pregnancy and delivery, and occurs mainly via the transplacental route after the first trimester and perinatally via contact with infected blood from the mother.10 Vertical transmission is a broader theoretical concept that also includes post-natal transmission and refers to the transgenerational perpetuation of the infection through undiagnosed, chronically infected asymptomatic women of child-bearing age who can transmit the infection with each pregnancy. Transmission is similar for babies delivered vaginally and via cesarean section, suggesting that the majority of transmission occurs before labor. A chronically infected woman can potentially transmit the parasite with each pregnancy. Treatment of women before or between pregnancies reduces – but does not eliminate - the risk of transmission.
Maternal parasitaemia is the key determinant for congenital transmission and seems to occur when the maternal parasitaemia reaches a critical threshold of 10 parasites/mL.10 The risk of congenital infection can be very high in those situations associated with high parasite load, for example, acute infection (54%), reactivated chronic infection during pregnancy or in patients with non-controlled HIV co-infection (up to 100% in the latter).10 Mothers in endemic areas are continuously exposed to re-infection and display higher parasitaemia levels. High parasitaemias are associated with invasion of the placenta by T. cruzi, causing disfunction by severe inflammation and necrosis. The level of parasitaemia is also inversely related to the production of pro-inflammatory cytokines, mainly IFN-ɣ, and T-cell response, both reduced in transmitting mothers. Chronically infected, non-transmitting mothers have strong inflammatory response, shown as high levels of IFN-ɣ and low parasitaemia, resulting in placentitis that is able to prevent infection, as opposed to transmitting mothers (low IFN-ɣ, high parasitaemia). This partially explains why, despite the relative immunosuppression that occurs naturally during pregnancy, most chronically infected mothers (95% of them) will have no or low degree parasitaemia and are less likely to transmit the parasite to their foetuses.
The rate of congenital T. cruzi infection (redefined to account for multiple births as congenitally infected infants divided by the number of infants born to infected mothers)10,11 occurs on average in 5% of pregnancies in endemic countries,10 but varies substantially depending on factors mentioned in the paragraph above and the specific geographical area. This route of transmission is responsible for nearly 9000 cases of infection in endemic countries each year.10 It also perpetuates transmission and accounts for the vast majority of new infections in non-endemic countries or areas where the vector has been eliminated. Although the congenital transmission rate is on average lower in non-endemic countries (2.7%),11 it may be increased depending on the characteristics of the specific migrant population. For example, congenital rates for at-risk migrant women have been reported to be 4% in Bergamo (Italy)12 and 13.8% in Murcia (Spain),13 both areas with a high proportion of migrants from Bolivia, one of the countries in LA with the highest prevalence of CD. Chronically infected mothers treated before the pregnancy with benznidazole have been reported not to transmit the parasite.13–15 However, transmission from mothers previously treated is possible if reinfection occurs from repeated exposure or if treatment fails. Post-natal transmission of T. cruzi in a viable form able to produce infection via breastfeeding is considered very unlikely.10
The transmission rate associated with blood transfusion of one infected unit is 10 to 25%.16 The seroprevalence in blood donors in non-endemic countries is determined by the particularities of the migrant population and the success of the blood screening programmes, ranging from 0.004% (1:27,500) of unselected blood donations in the United States16 to 0.6% (1:160 of at-risk donors from LA) in Catalonia (Spain),17 and is above 10% for the very high-risk group of donors from Bolivia.17,18 In the UK, where a universal screening programme exists, the seroprevalence is approximately 0.01% (1:10,000) of at-risk donors.19
In non-endemic areas, transmission via the congenital, blood transfusion, solid organ and bone marrow transplant routes has been well documented.20 However, many of those transmissions reported were diagnosed in immunocompromised patients who developed symptoms. Most of the infections in immunocompetent patients are likely to be asymptomatic and to go unnoticed given the lack of awareness and of robust screening programmes.
Prevalence
Distribution in Endemic Countries
The infection by T. cruzi is endemic where the vector exists, in the Americas, from the South of the USA (human cases have been reported in Texas and Louisiana) to the North of Chile and Argentina.3 Globally, there are 75 million people at risk of CD.21 Only in LA, there are 60 million at risk, 6 million cases and it results in 12,000 to 20,000 deaths per year.2,22 The prevalence is not homogeneous and depends on the specific region and population characteristics. Based on estimates done in 2010, Argentina and Brazil had the highest absolute numbers of people infected. In hyperendemic areas, such as the Bolivian Chaco, the force of infection is about 4% new infections per year, and nearly 100% of the population older than 30 years are seropositive.23 It is not straightforward to extrapolate the individual risk of infection directly from the country of origin, and all LA countries should be considered at-risk of infection by T. cruzi. WHO estimates of country –specific prevalence and incidence data have been published.20,24
Prevalence in Non-Endemic Countries
Human migration has brought the disease outside the endemic areas by chronically infected, asymptomatic adults, who can transmit the disease via non-vectorial routes. In 2017, 32 out of 38 million of international migrants from the LA and Caribbean region were living outside of their area of birth, mostly in North America (26 million) and Europe (5 million),25,26 mainly in Spain. Estimates suggest a significant number of cases of chronic infection by T. cruzi in the United States (more than 300,000),27 Europe (80,000 to 120,000)28,29 and the Western Pacific region (4000 in Japan30 and 2000 in Australia and New Zealand).31 An estimated 186,000 LA people were living in the UK by 2010, of which 113,500 lived in London.32 Even presuming a conservative median point prevalence estimate of 4%,33 the disease is massively underdiagnosed in non-endemic countries, up to in 96% of the cases in a European-wide study using data from 2009.28 Only a handful of cases had been diagnosed in Japan between 1994 and 2014.30 A specialist, London-based clinic treated only 60 cases in a 23-year-long series.34
Estimating the true prevalence of CD in non-endemic areas is challenging for many reasons: (1) in many countries, “Latin American” is not recognised as a separate ethnic group, making it difficult, if not impossible, to have an accurate register of people at risk of infection, (2) the high mobility of the LA migratory population, (3) at-risk migrants may not be registered with the health care systems due to issues/fears around legal/immigration status, (4) social stigma, cultural beliefs and practices around health care (eg, preference for private health care) may prevent patients from seeking help, (5) lack of awareness by patients but also by governments, health systems and professionals.
The infection rates in non-endemic countries depend not only on the country of origin but also on the particular socioeconomic, housing circumstances and exposures before migrating. The actual prevalence of infection in the migrant population in the country of destination may be higher than that of the endemic country.35 For example, migrants from rural areas, from highly endemic countries/regions (eg, El Chaco region in Bolivia, El Salvador, and Guatemala) have higher prevalence rates than their country average. The absolute number of infected people is expected to be high in those areas/countries attracting high numbers of migrants from countries with the highest absolute number of infected people (Argentina, Brazil and Mexico).36 The relative frequency of each form of non-vectorial transmission form also depends on the characteristics of the migrating population. For instance, the predominant migration of women from Bolivia and other LA countries has an impact in estimating the relevance of congenital transmission in the countries of destination.
Clinical Features and Clinical Diagnosis
Understanding the life cycle of T. cruzi and the pathogenesis of the disease, initially described in 1908,37–39 has allowed clinicians to differentiate the two stages of the disease: the acute and the chronic phase.
Acute Phase
Most cases in the acute phase are asymptomatic or pauci-symptomatic, and it is only 10% of cases that develop more specific symptoms in a clinical syndrome that tends to unfold within weeks. At this stage, the invasive trypomastigotes form can be detected in peripheral blood (peaking parasitaemia at 30 days following infection).
The signs and symptoms of the vector-transmitted acute form appear after an incubation period of 7–30 days. The incubation period can be dramatically shorter in orally transmitted infections, caused by direct ingestion of viable parasites in food and beverages (contaminated with triatomine faeces)40 or extend to months when the transmission takes place by organ or blood transfusion. The most severe presentations of acute CD are seen in cases related to the oral route (higher parasitic load).
Occasionally, a specific oedematous skin lesion (namely chagoma) can be observed at the portal of entry, in areas of thin skin, where the triatomine insect has taken a blood meal. In 1934, Romaña (and Mazza) described their homonymous pathognomonic sign of unilateral non-pitting palpebral oedema with conjunctivitis and generalized face oedema. Oedema, secondary to the blockage of lymphatic vessels, is the primary lesion, where the replicating form of the parasite, the amastigote, multiplies and progresses to invade the reticuloendothelial system. Regional lymphadenopathy becomes apparent followed by liver and splenic enlargement that can be palpable on physical examination. Non-specific and general symptoms of the acute phase include tachycardia, anorexia, malaise, vomiting, myalgia, and headache.
The parasitic preference/tropism for mesenchymal cells targets the adipose (lypochagomas), reticuloendothelial, myocardial and neuroglial tissues. The tissue inflammatory response is a key feature of this phase. An acute and severe myocarditis (myocyte invasion and necrosis) can occur, and meningoencephalitis can be life-threatening, especially in the immunocompromised host.
Chronic Phase
Untreated, the acute phase is followed in 70% of cases by an indeterminate phase (chronic asymptomatic infection) that can be lifelong, whilst 30% evolve – within 10 to 30 years – into a chronic symptomatic form affecting the heart (20–30% of infections), the gastrointestinal tract (15–20%) and, more rarely, the peripheral nervous system (sensory polyneuropathy, less than 5%).41 Cardiac myocardiopathy is the most common manifestation of the chronic symptomatic form of the disease. A combination of factors, including the parasitic load, parasite lineage, and the host immune response to the initial stages of the disease and subsequent tissue damage play a role in the pathogenesis of the chronic form. Although not consistent,42 some of the parasite lineages have been associated with specific clinical manifestations of the disease (for example, TcI with cardiomyopathy in regions north to the Amazon; TcII, IV, VI with megaoesophagus and megacolon in Central Brazil and the Southern Cone region).43,44
Chronic Indeterminate Form
The indeterminate form is the commonest presentation of CD. It is characterized by an unremarkable physical examination, normal electrocardiogram (ECG) tracing and gastrointestinal studies in asymptomatic but serologically positive individuals. However, there is potential for disease progression and reactivation in cases of immunosuppression (immunosuppressive therapy, HIV-infected individuals and transplant recipients) hence the recommendation for clinical and laboratory follow-up.
Chronic Symptomatic Forms
Cardiac Manifestations of CD
A good cardiovascular history is an essential part of assessing a patient with suspected or confirmed CD. Cardiac involvement is the most common form of the disease, it is present in up to 45% of chronically infected patients, and includes thromboembolism, conduction abnormalities, arrhythmias, and heart failure due to dilated cardiomyopathy.
Some patients develop a characteristic apical left ventricle aneurysm that predisposes to thromboembolic events and stroke.
Atrial and ventricular arrhythmias classically involving the sinus node are well described in CD. They often present in combination with other cardiac manifestations following fibrotic changes in the cardiac conduction system. The most common findings found in the 12-lead electrocardiogram are left anterior fascicular block, right bundle branch block and ST-T wave changes. Patients may describe palpitations, dizziness or syncope. Sudden death accounts for the highest cause of overall mortality in CD (55–66%) and it is mainly secondary to ventricular tachyarrhythmia.45
Chagas cardiomyopathy affects 20–40% of patients with chronic CD. The pathophysiology that underlies CD is thought to comprise a combination of factors including direct parasitic damage, immune mediated inflammation and neural denervation of the myocardial fibers. Destroyed fibers are substituted by fibrosis with progression to hypertrophic myopathy. Dilatation occurs when the extent of fibrosis no longer allows for efficient compensatory hypertrophy.46,47 Overall systolic dysfunction is a poor prognostic indicator and reflects end-stage Chagasic cardiomyopathy.
Ischaemic brain changes are commonly seen in these patients as a consequence of hypoxaemia, acute changes in brain blood supply secondary to cardiac arrhythmias and thromboembolism.
The most common initial cardiac manifestations found are left and right bundle branch blocks and left wall segmental motion abnormalities.2 Echocardiogram and 12 lead-ECG are routinely used in the initial assessment and follow-up of these patients, bearing in mind that ECG abnormalities increase with age due to other pathologies.48,49 More recently, the use of cardiac-MRI has been found to be very useful to identify and characterize myocardial fibrosis, but it is expensive and its use is not widespread. A chest X-ray may detect cardiomegaly and also dilated oesophagus and exclude other potential causes for the symptoms.
Gastrointestinal Manifestations of Chronic Chagas Disease
Mega-visceral syndromes are caused by denervation of the enteric nervous system that appear years after the acute infection and include:
1) Megacolon: the commonest form, mainly affecting the sigmoid colon and rectum, causes symptoms from constipation to severe dysmotility, faecal impaction and bowel ischemia,
2) Megaoesophagus: esophageal dysmotility such as achalasia is classic features of CD. Patients may refer odynophagia, dysphagia, reflux, and secondary cough and regurgitation,
3) Chagasic enteropathy is the least common presentation of megaviscera (megaduodenum, megajejunum) and is mostly invariably linked to megaesophagus or megacolon. Dyspeptic syndrome, altered absorption and bacterial overgrowth may occur.50
About 10% of asymptomatic patients with chronic CD have radiological gastrointestinal abnormalities. Some groups recommend contrast-based radiological studies (barium enema, oesophagogram) even for asymptomatic patients,51 while others only advise so if symptoms are present (authors´ practice at the Hospital for Tropical Diseases in London). Other studies such as manometry and endoscopy are used to classify and address cases that present with gastrointestinal symptoms. Even in geographical areas with high prevalence of gastrointestinal forms of the disease, cardiac myocardiopathy is more common, so the relevant investigations to investigate cardiac disease must always be performed simultaneously.
Congenital Infection
T. cruzi infection/transmission is defined by detection in babies of (1) T. cruzi parasites at birth or (2) specific antibodies that are not of maternal origin from month eight onwards. The term congenital Chagas disease is usually reserved for symptomatic/clinical infections.
T. cruzi cannot infect the foetus before 12 weeks of gestation and so is not linked to developmental malformations. The prevalences of miscarriages, stillbirth and prematurity are similar or slightly increased in pregnancies of women chronically infected by T. cruzi, but may be under-reported. Premature rupture of membranes is frequent and characteristic. Most T. cruzi infections in live births are asymptomatic (in some series, up to 100%). Symptoms of the disease may present until several weeks following birth and include non-specific features (fever, splenomegaly, oedema, anasarca, skin lesions, purpura, jaundice, anaemia, thrombocytopenia) that overlap with other congenital infectious syndromes. Some characteristic, but less common symptoms, seen more often in the context of high maternal parasitaemia are meningoencephalitis/neurological disorders and myocarditis.10 The mortality of congenital infection can be very high in severe cases or in impoverished areas of endemic countries but it probably strongly depends on the socio-economic structure of the country and the quality of the antenatal and postnatal care. As an example, the mortality dropped from 13% to 2% in a specific area in Bolivia between 1992 and 2001, coinciding with a parallel decrease in poverty52. In non-endemic countries, neonatal death has been anecdotally documented,53 but it may be under-diagnosed.
If left untreated, a third of cases of congenital T. cruzi infection will enter the chronic phase of infection within the first year of life. Of those, a third will develop a symptomatic form of the disease and will be at risk of a premature death and severe disability. Anti-parasitic treatment (benznidazole or nifurtimox) is indicated as soon as congenital infection by T. cruzi has been diagnosed. The treatment is well tolerated in children and achieves cure (negativization of serology and parasitaemia, if initially detected) in over 90% of cases treated within the first year of life.10,54 Cure rates decline rapidly with further delays in treatment (as low as 20% when started at one year of age or older in a recent study conducted in Spain).55 Antiparasitic treatment is contraindicated during pregnancy, but diagnosed mothers should be treated after delivery to minimise transmission in future pregnancies. It is important to note that, even when treated in the chronic phase, vertical transmission can still occur during pregnancy.
Laboratory Diagnosis of Chagas Disease in the Non-Endemic Setting
Diagnostic Algorithms
In the non-endemic setting, most referrals for laboratory diagnosis of CD are for adult migrants from LA who will likely be in the indeterminate or chronic stage of infection. However, acute cases may arise in neonates born to seropositive mothers (congenital transmission), seropositive individuals who require immunosuppressive therapy (reactivation), immunocompromised recipients of organs from seropositive donors (transplantation transmission) and laboratory workers (accidental transmission) or returning travellers (vectorial or oral transmission).
The laboratory diagnosis of T. cruzi infection in non-endemic areas is usually performed in reference laboratories. Diagnostic algorithms for acute and indeterminate/chronic disease may differ between centres, but use combinations of microscopy, PCR and serology.
Laboratory Diagnosis of Acute Chagas Disease
At the peak of acute infection, characteristic flagellated extracellular trypomastigote forms of the parasite will be present in peripheral blood. On entering the indeterminate/chronic phase of the infection, however, parasitaemia becomes extremely low and intermittent, as trypomastigotes invade nucleated cells in tissues.
Samples required for diagnosing suspected acute cases are as follows: unfixed thick and methanol-fixed thin blood films made fresh from whole blood (minimum of 2 each) and 8–10mL (adults) or 1–2mL (babies) of EDTA blood. For neonates, both cord blood and venous blood should be submitted where possible. EDTA blood should be fresh and must not be frozen before sending. Blood films should be made from blood within 6 hours of taking.
Both microscopy and PCR are performed: diagnosis can be made by direct demonstration of the parasite by light microscopy of thick blood films or buffy coats or by detection of T. cruzi DNA by PCR. Serology is not helpful in the acute stage (see below).
In non-endemic settings, referrals for laboratory diagnosis of acute CD are made for:
Diagnosing Congenital Infection in Babies Born to Seropositive Mothers
Blood films and PCR should be performed on neonatal cord and venous blood. Venous blood is preferred, as false positives may occur with cord blood samples.
If the PCR is positive at birth but the blood films are negative, another PCR is performed 4 weeks later to confirm the diagnosis.
If the initial PCR result is negative, PCR testing should be repeated at one month. If still negative, it should be repeated again at three months, or at any time if the baby becomes unwell.
Serology is not indicated at less than 9 months of age because results will be confounded by transplacentally transferred maternal IgG. If previous microscopy and PCR results were negative, serology should be used to exclude infection in babies at 9 months of age.55
Basile et al described a useful algorithm for congenital Chagas disease screening,55 and reviewed recommendations for the management of congenital infection have also been published recently.54
Monitoring for Reactivation in Immunocompromised Chagas Seropositive Individuals
Serology is not indicated in this context because results will be confounded by existing antibodies. The recommendations are to monitor for clinical signs of reactivation and to perform microscopy and PCR on peripheral blood, unfixed tissue, and cerebrospinal fluid (CSF) as clinically indicated.
Monitoring for Reactivation in Chagas Seropositive Transplant Recipients
Serial serology is not indicated here.
Serial quantitative PCR on peripheral blood should be performed following the transplant weekly in months one and two, every two weeks in months three and four, once a month in months five and six, and then based on the clinical picture.10
Diagnosing Acute Infection in Travellers Returning from Endemic Regions with Suggestive Signs and Symptoms
Blood films and PCR should be performed on venous blood. Baseline serology is required, with repeat samples at 6 to 8 weeks and at 6 months to check for late seroconversion, unless another explanation for the acute illness has been found.
Laboratory Diagnosis in Indeterminate/Chronic Chagas Disease
Serology is used for primary diagnosis in the indeterminate or chronic stage. In immunocompetent individuals, parasitaemia will likely be extremely low and intermittent, so microscopy is not sufficiently sensitive. Parasitaemia may be detectable using molecular methods targeting highly multi-copy targets; however, positivity may be intermittent in an individual patient.
In untreated seropositive individuals, PCR should also be requested to detect and establish the level of parasitemia, particularly relevant in pregnant women, for whom detectable DNA carries an increased risk of mother-to-child transmission,10,57,58 and for individuals undergoing immunosuppressive treatments, for whom DNA levels assessed through PCR can be used to monitor response to treatment. The levels of parasitaemia can vary in the chronic stage in individual patients and that parasitaemia cannot always be used for monitoring purposes.
Samples required for the diagnosis of CD in the indeterminate or chronic stage are serum and a large volume (8–10mL) of EDTA blood. EDTA blood should be fresh and must not be frozen before sending.
Laboratory Diagnostic Methods
Microscopy
To diagnose acute CD, thin blood films stained with Giemsa at pH 7.2 and thick blood films stained with rapid Field or Giemsa stain are examined at x500–1000 magnification under oil immersion. Diagnosis is confirmed if characteristic T. cruzi trypomastigotes are seen on blood films. Diagnostic features include a prominent nucleus and a large kinetoplast; the undulating flagellum can be seen in thin films.
Parasites may not be detectable by microscopy in the early and late stages of the acute phase due to low starting parasitaemia (early infection) or because trypomastigotes disappear from the blood following the development of an immune response (late acute and chronic stages).
Other microscopy-based approaches involve examination of stained fixed films from the buffy coat layer for trypomastigotes or to look for live, motile parasites in a direct wet preparation or using standard (microhematocrit) or fluorescent (QBC) capillary technologies.54
Serology
Where chronic T. cruzi infection is suspected, PAHO recommends using two serological tests with antigens that detect different antibodies against T. cruzi, for example ELISA or indirect fluorescent antibody test, with the addition of a third test if there are conflicting results.59 For population studies, the use of an ELISA or immunochromatographic test is recommended.
PCR
Molecular PCR-based methods targeting highly multi-copy kinetoplast (kDNA) and nuclear genome (nuclear satellite DNA) sequences have been developed.60,61 For review, see Schijman et al and others.62,63 These methods are able to detect very low numbers of parasites in the peripheral blood of acute and congenital infections and also in some indeterminate/chronic stage CD patients. Diagnosis is confirmed if T. cruzi DNA is detected by PCR. However, as PCR sensitivities are in the range of one parasite per 10mL of blood, negative PCR tests do not exclude T. cruzi infection.
Additionally, the sensitivity of molecular methods for the diagnosis of T. cruzi is complicated by the existence of genetic subtypes (lineages, TcI – TcVI), which differ in the copy number of PCR targets and DNA sequence resulting in up to a 10-fold difference in assay sensitivity, thus making quantitation difficult.64
LAMP
A loop-mediated isothermal amplification (LAMP) assay has been developed for the detection of T. cruzi DNA65 and has recently been evaluated on a range of materials from congenital and other acute cases, reporting an overall 93% sensitivity and 100% specificity.66 The assay is not sufficiently sensitive for use in chronic CD, where much lower parasitaemias are found, but may be applicable to laboratories in hospitals with maternity clinics serving large numbers of migrants from LA.
Rapid Diagnostic Tests
These tests, based on the immunochromatographic detection of antibodies or antigens, can be done on a small blood sample obtained via fingerprick, do not need cold chain and have a quick turnaround (within 1 hour). Their performance is generally very good in endemic areas where the pre-test probability is high (pooled sensitivity of 97% and specificity of 99%),67,68 but varies between geographical areas. Positive results need to be confirmed with two positive conventional tests.69 Initially developed to facilitate testing in endemic areas, they have been successfully used in non-endemic countries, as a point-of-care test in screening events designed to attract people at risk (Elkheir, poster communication in ECCMID 2022).
Management of Chagas Disease
Overview
The care of individuals with CD entails consideration of anti-parasitic drug therapy and management of end-organ disease and starts with staging of the condition as determinate or indeterminate. There is an evolving sentiment towards the expansion of the patient groups which may be offered anti-parasitic therapy driven by accumulating supportive parasitological data (rather than strong clinical data) and the near-future promise of better-tolerated, shorter courses of therapy.
Detection and Management of End-Organ Disease
As outlined above, notwithstanding case reports of involvement of other organ systems, the principal clinical consequences of T. cruzi infection in the otherwise immunocompetent host are cardiac and gastrointestinal diseases. In the absence of clinical, radiological or ECG manifestations of end-organ damage, the disease is classified as indeterminate. An unanswered question in the newly diagnosed, asymptomatic individual is how far the investigation should go to warrant designation as indeterminate. A 12-lead resting ECG and a chest radiograph are mandatory (for detection of conduction defects and dilated cardiomyopathy), and in our practice, all patients undergo echocardiography. Investigation of the gastrointestinal tract and 24-hour Holter ECG monitoring is generally reserved for patients reporting symptoms.
Follow-Up for Indeterminate Disease
Once a designation of indeterminate CD is made (asymptomatic with normal chest radiograph, ECG and echocardiogram), individuals enter a programme of annual clinical, ECG and T. cruzi PCR review, the goals of which are to identify early development of determinate disease, to optimise management and to detect the appearance of circulating T. cruzi DNA, which would be an indication for anti-parasitic (re)treatment.
Follow-Up for Determinate Disease
If cardiac conduction defects, dysrhythmias, structural myocardial abnormalities (including aneurysm) or thromboembolism are detected – whether symptomatic or not – cardiological review and management are advised. In general, management of each follows the same approach as other conditions leading to dilated cardiomyopathy and electrophysiological perturbance, though Chagas cardiomyopathy tends to be progressive.70
Overt gastrointestinal involvement is less frequent than cardiac disease, with which it often co-exists, though investigation with imaging, manometry and endoscopy is driven by symptoms so subclinical involvement may be under-recognised. The most common manifestations of megaoesophagus and megacolon contribute to morbidity but rarely confer significant mortality risk. Optimal management has not been clearly established. Megaoesophagus is not reversible, so the aim is to reduce lower oesophageal sphincter (cardiac) pressure for which nitrates and nifedipine may be useful if tolerated, whilst, as for achalasia from other aetiologies, success in ameliorating symptoms is reported following endoscopic balloon dilatation or (laparoscopic) Heller myotomy.51 Colonic disease is also not reversible, so symptom management entails behavioural approaches to regulate bowel habit and use of laxatives and enemas as required. If complicated by volvulus or nutritional compromise, surgical options include resection of sigmoid colon with or without preservation of the rectum.
Anti-Parasitic Therapy
Two agents with activity against T. cruzi are available: benznidazole and nifurtimox. There is limited evidence to suggest that for efficacy or tolerability, there is much to choose between them, though benznidazole is currently easier to access. Both nifurtimox and benznidazole have significant and frequent side effects (nifurtimox causes nausea, vomiting and neurological disorders; benznidazole, hypersensitivity reactions with rash and fevers) that often lead to discontinuation of the treatment.2
A standing controversy relates to the capacity for effective anti-parasitic therapy to influence the natural history of established T. cruzi infection. Benznidazole has been clearly demonstrated in the randomised controlled “BENEFIT” trial to clear PCR-detectable T. cruzi DNA from the circulation of treated adults with determinate cardiac disease,71 albeit a little less effectively than in earlier studies of subjects with indeterminate disease. Disappointingly, however, in this trial population, which included a significant proportion of patients with established advanced cardiac disease, this parasitological response did not translate into measurable clinical impact upon cardiac disease progression or mortality, in contrast to previous observational data.
Patient groups in whom effectiveness and clinically important outcomes have been established and for whom anti-parasitic treatment is now recommended are as follows: (1) infants and children with congenital infection, (2) girls and non-pregnant women of child-bearing age (to prevent vertical transmission), and (3) individuals with acute T. cruzi infection.59 Despite the low certainty of evidence, anti-parasitic treatment is also now recommended for (4) patients with indeterminate disease and may be of particular benefit to those at highest risk of reactivation disease (transplantation, HIV, and immunosuppressive therapy).
Conversely, the lack of a demonstrable impact upon established disease despite parasitological clearance has led to PAHO not recommending treatment for patients with determinate disease, though with the caveat that there may be instances in which patients and their physicians may choose to do so.
Though conventionally anti-parasitic treatment has required 60–90 days of therapy, there is strong evidence in support of non-inferior, sustained parasitological responses to shorter regimens.72 Since most adverse reactions occur beyond two weeks, the 14-day course of benznidazole holds particular appeal. The lower cost and higher completion rate of such a regimen may further swing the weight of opinion behind treating for those with determinate disease who are T cruzi DNA PCR-positive, even without conclusive demonstration of clinical benefit.
Approaches to Case Detection and Prevention
Rationale
Early diagnosis is difficult outside screening programs in both endemic and non-endemic areas as it is mostly an asymptomatic infection that goes unnoticed. As pointed out previously in this review, treatment of infection by T. cruzi is highly successful in cases of congenital transmission that are diagnosed early, and very difficult once it becomes chronic. Therefore, identifying the risk factors and the main opportunities for transmission in order to prevent infection in the first place is extremely important. Outside of endemic areas, congenital infection is, by large, the main determinant of ongoing transmission and must be addressed. Screening programmes or rejection of blood/tissue from donors at risk are pretty well established, but the diagnosis of reactivation in immunocompromised patients is still anecdotal. Blood screening by serology is simple and inexpensive.
The population at risk of CD to target in any prevention strategy needs to be defined in a way that is pragmatic and integrates seamlessly with any existing policies. This is of particular importance in non-endemic countries, where screening for CD may be seen as a not cost-effective, low-priority intervention by policymakers. For instance, early detection of congenital transmission may be more easily done by performing serology on all pregnant women attending the antenatal clinic that were born in LA or to mothers born in LA, than by doing a detailed risk-assessment to identify high-risk exposures.
Common barriers encountered in non-endemic countries have been very well described recently28 and include difficulties to identify the at-risk population as those born in LA may not be registered as a separate ethnic group, lack of awareness of the disease by health providers, logistic problems to access those migrants that are undocumented or that do not use the public health system, and difficulties with follow-up of cases given patients mobility (migration to other country or city). Case identification and prevention strategies for the main target groups are described, with a specific focus on the non-endemic setting. For the purposes of case detection strategies in non-endemic countries in this section, the at-risk population is defined here as those born in LA or to mothers born in LA. Vector control strategies are not reviewed, as they are not relevant outside of endemic areas.
The success of any strategy aimed to improve case detection and prevention eventually depends on the appropriate integration in existing healthcare systems, the acceptance by the population being targeted and the appropriate response of relevant policy makers. This is why strategies must be seen as part of wider programs. The implementation of new strategies to improve case detection and the evaluation of their success must happen in real-world conditions, in order to take into account and identify– rather than control for – variables that may have an influence on their success. In this sense, implementation research can provide a very useful framework. Methods typically used in implementation research are more likely to be appropriate when designing or evaluating the outcome of interventions in CD and may include pragmatic, effectiveness trials, quality improvement studies and qualitative and mixed methods.73
It is not possible to emphasize enough how important the context is. The population at risk, their communities and their circumstances must be seen as central and essential elements of any intervention or change in policy, and should be involved in all the stages. For example, starting from scratch a new community-based screening campaign is virtually impossible without collaborating and liaising with LA cultural organisations, charities or community groups that can enormously help with reaching the intended population in a culturally appropriate manner. Table 1 outlines the most important steps to take into account when implementing Chagas disease control programs in non-endemic countries.
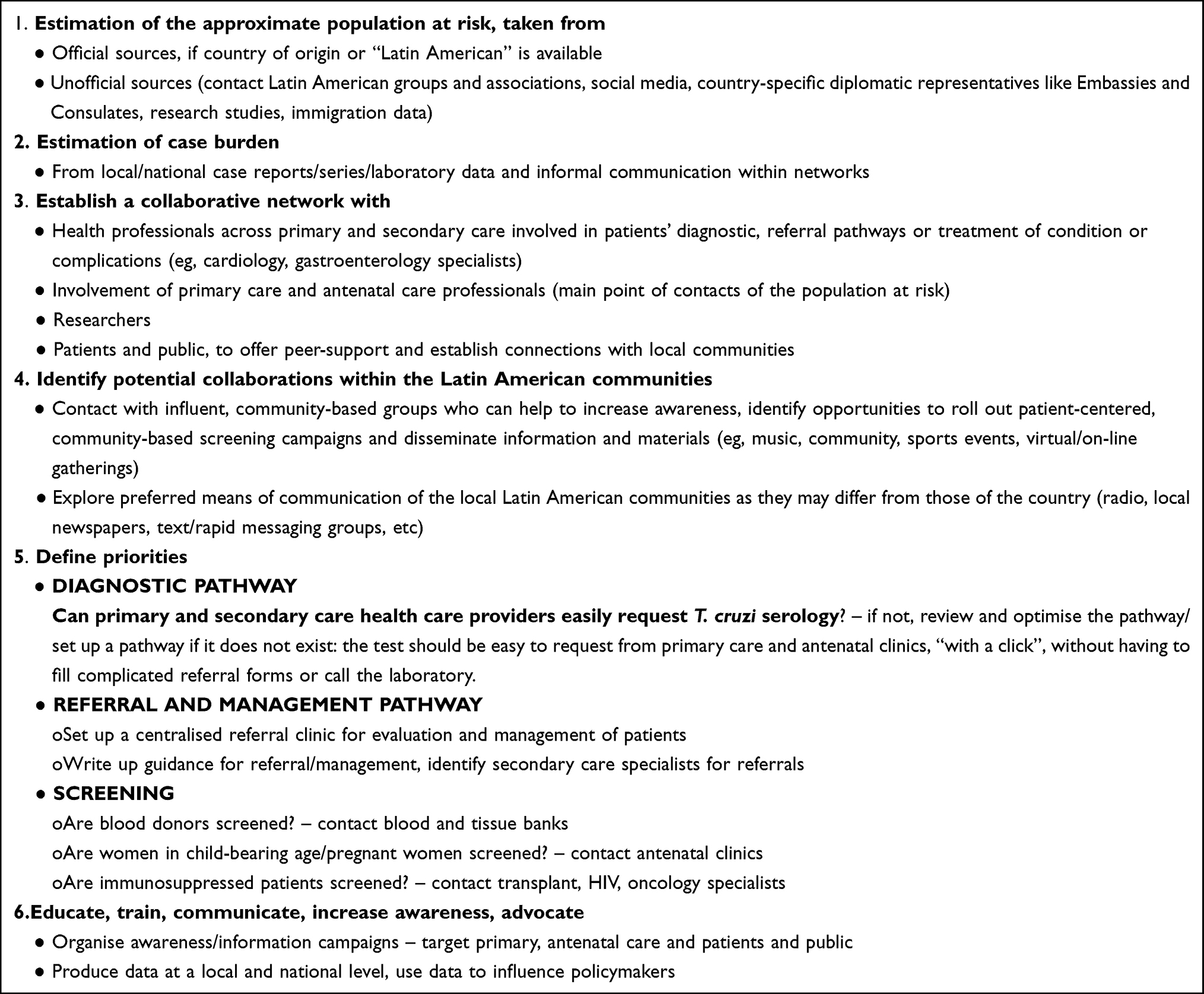 |
Table 1 Strategy for Non-Endemic Countries |
Antenatal/Congenital Transmission
Ideally, at-risk women of childbearing age or young girls should be screened with serology before pregnancy and treated if positive, to prevent maternal–fetal transmission (treatment is contraindicated during pregnancy).
The most commonly used approach is the screening with serology of at-risk pregnant women, aiming to diagnose infection in the newborn and, if present, offer treatment, which is highly successful in young children. This should be followed by (1) treatment of the seropositive mothers following delivery, (2) screening of other children from previous pregnancies, and (3) screening of the mother’s siblings.
Antenatal screening is a clear recommendation from the PAHO and the WHO, also in non-endemic countries.14,28 Pre-conception antiparasitic therapy is a highly effective intervention to minimise the risk of vertical transmission. However, screening programmes exist only at local (hospital) and regional level in some countries (Italy, Spain, Switzerland, UK) but are absent in many others (Canada and the US, Japan, Australia and New Zealand). To our knowledge, there are no established screening programmes at a national level in any non-endemic country.
The implementation of antenatal screening programs requires the engagement from professionals (by training sessions directed to midwives, obstetricians, general practitioners) and mothers (eg, talks directed to mothers, in the relevant native Language, run in antenatal clinics or baby-mum groups), optimisation of the screening test request processes (electronic prescribing, implementation of country of birth-based algorithms to screen new patients). It may be necessary to do seroprevalence studies or estimate the population at risk and to do cost-effective analysis before deciding which areas to target for antenatal testing, particularly if screening of T. cruzi is not part of the current policy. High-level conversations with stakeholders (Public Health agencies, relevant professional Colleges – Obstetricians, Midwives) may also be necessary to influence policy.
Immunocompromised Patients
Detecting cases of infection by T. cruzi in this setting requires a high level of clinical suspicion, awareness of the variety of clinical presentations and prospective laboratory monitoring, as there is little guidance out of endemic countries. Guidance from different solid organ transplant societies in non-endemic countries recommends regular monitoring following transplant.74–76 Patients with HIV at risk of CD should have screening serology, as recommended by guidelines in endemic countries.77 The first and the most difficult step to implement these recommendations in non-endemic countries is to increase awareness amongst the relevant professionals (by training/educative sessions, case reports, etc). Country of birth-based criteria can easily be incorporated in fever and pre-transplant screening algorithms. The typical scenarios to consider are as follows:
1) Transplant-related infection following the transplant of an organ from an infected donor, described in 19% of kidney78 and 29% of liver recipients.74 These patients may present with severe, disseminated acute infection including fulminant myocarditis, and the incubation period can be very prolonged, from 23 to 420 days;75 treatment is effective if done promptly.
2) Reactivation of T. cruzi infection in chronically infected patients following immunosuppression for transplant, seen typically in 20–60% or heart transplant recipients,75 and also reported with other transplants although less commonly. The range of presentation is broad, from only parasitological evidence of reactivation (positive PCR in peripheral blood) without symptoms to disseminated infection with skin lesions, myocarditis or, less commonly, central nervous system (CNS) symptoms. It may mimic rejection, and it is typically not curable, even despite anti-parasitic treatment.
3) Reactivation in HIV-coinfected individuals is associated with declining CD4 count and has been described in 21 to 35% of co-infected individuals in endemic areas.49,79 It presents characteristically with CNS infection, mimicking other opportunistic infections like toxoplasmosis, and it may also cause skin symptoms and myocarditis.
4) Reactivation in patients with rheumatologic conditions has been described (6 out of 58 patients in a prospective cohort study in Argentina)80 and associated with prednisolone doses higher than 20 mg/day.
Travellers
Identifying cases in travellers requires education of health care providers and patients to identify potential exposures during the travel and clinical suspicion, being also mindful that oral transmission is possible during travel to endemic areas.
Blood, Tissue and Organ Donors/Donations
The American Association of Blood Banks states that T. cruzi parasites persist and remain in whole blood at 4°C for at least 18 days. They survive in red cell components at 4°C for days to weeks; for up to 5 days in platelets under normal storage conditions; and for 24 hours or less in frozen plasma components.81
The risk of acquiring T. cruzi infection after transfusion of an infected unit is estimated to be 10 to 25%.16
Serological screening of blood donations is practised extensively in endemic Latin American countries. The health policies to control CD, including blood screening, in European countries have been recently reviewed.76
The UK National Health Service Blood and Transplant introduced a blood donor screening programme in 1998, the first non-endemic country to do so.19
Tissue and organ donors are also risk-assessed, and the UK Advisory Committee on Microbiological Safety of Blood, Tissues, Organs and Cells (SaBTO) recommends discretionary T. cruzi antibody screening of donors with identified risk factors for American trypanosomiasis. Those with a history of CD are permanently deferred from donation.
The current UK blood donor selection guidelines for T. cruzi are as follows.
Obligatory exclusion criteria. Must not donate if:
- Born in South America or Central America (including Southern Mexico),
- Mother was born in South America or Central America (including Southern Mexico),
- Has had a transfusion in South America or Central America (including Southern Mexico),
- Has lived and/or worked in rural subsistence farming communities in these countries for a continuous period of four weeks or more.
Discretionary: If at least four months following the date of last exposure (or if transfused prior to 1980) and a validated test for T. cruzi antibody is negative, donation can be accepted.
For blood bank screening, PAHO59 recommends the use of highly sensitive ELISA kits or chemiluminescent microparticle immunoassay (CMIA) tests.
Public Health Campaigns, Global and Local Collaborations and Awareness Initiatives
Public health, no-shame, information and awareness campaigns, involving patients and the public, are essential in both endemic and non-endemic areas, in order to (1) normalise the diagnosis and remove the stigma, (2) encourage screening of the asymptomatic population at risk, and (3) educate the public and the professionals about the disease, prevention and treatment options.
The Pan American Health Organisation (PAHO)82 and World Health Organisation (WHO)83,84 published in 2009 and 2010 their strategy and roadmaps for control and elimination of CD. The legislation and practices to prevent transmission in Europe were first described in the 2009 WHO report and reviewed recently.85,86 However, as described elsewhere in this review, they have not been fully implemented.
In non-endemic countries, official public health initiatives are virtually non-existent, and awareness and screening campaigns are organised by organisations rather, often at regional/local level. A number of not-for-profit, patient-centered organisations exist in many endemic and some non-endemic countries that offer information and peer support. Many of these are also part of Findechagas, an international federation that offers resources and links between the different country-level organisations.87 The Global Chagas Coalition is a multi-disciplinary collaborative group of institutions, funders, researchers, patients and health practitioners that focuses on advocacy, raising awareness of policymakers and mobilisation of resources.88 Coinciding with the 110th anniversary since the discovery of CD, the WHO approved the creation of the World Chagas Disease Day in 2019 with the aim of increasing its visibility.
Acknowledgments
Peter L Chiodini is supported by the National Institute for Health Research and the University College London Hospitals Biomedical Research Centre, UK.
Disclosure
The authors report no conflicts of interest in this work.
References
1. The UK Chagas hub; 2013. Available from: http://www.thehtd.org/chagasuk.aspx.
2. Pérez-Molina JA, Molina I. Chagas disease. Lancet. 2018;391:82–94.
3. Browne AJ, Guerra CA, Alves RV, et al. The contemporary distribution of Trypanosoma cruzi infection in humans, alternative hosts and vectors. Sci Data. 2017;4:170071. doi:10.1038/sdata.2017.71
4. Lidani KCF, Andrade FA, Bavia L, et al. Chagas disease: from discovery to a worldwide health problem. Front Public Heal. 2019;49(6):1–13.
5. Zingales B, Andrade SG, Briones MRS, et al. A new consensus for Trypanosoma cruzi intraspecific nomenclature: second revision meeting recommends TcI to TcVI. Mem Inst Oswaldo Cruz. 2009;104(7):1051–1054. doi:10.1590/S0074-02762009000700021
6. Lima L, Espinosa-álvarez O, Ortiz PA, et al. Genetic diversity of Trypanosoma cruzi in bats, and multilocus phylogenetic and phylogeographical analyses supporting Tcbat as an independent DTU (discrete typing unit). Acta Trop. 2015;151(1):166–177. doi:10.1016/j.actatropica.2015.07.015
7. Nielebock MAP, Moreira OC, Das Chagas Xavier SC, et al. Association between Trypanosoma cruzi DTU TcII and chronic Chagas disease clinical presentation and outcome in an urban cohort in Brazil. PLoS One. 2020;15(12December):1–15. doi:10.1371/journal.pone.0243008
8. Ramírez JD, Hernández C, Montilla M, et al. First report of human Trypanosoma cruzi infection attributed to TcBat genotype. Zoonoses Public Health. 2014;61(7):477–479. doi:10.1111/zph.12094
9. de Noya BA, Díaz-Bello Z, Colmenares C, et al. Update on oral Chagas disease outbreaks in Venezuela: epidemiological, clinical and diagnostic approaches. Mem Inst Oswaldo Cruz. 2015;110(3):377–386. doi:10.1590/0074-02760140285
10. Carlier Y, Truyens C. Maternal-fetal transmission of Trypanosoma cruzi. In: Telleria J, Tibayrenc M, editors. American Trypanosomiasis Chagas Disease: One Hundred Years of Research.
11. Howard EJ, Xiong X, Carlier Y, Sosa-Estani S, Buekens P. Frequency of the congenital transmission of Trypanosoma cruzi: a systematic review and meta-analysis. Br J Obstet Gynaecol. 2014;121(1):22–23. doi:10.1111/1471-0528.12396
12. Rodari P, Angheben A, Gennati G, et al. Congenital Chagas disease in a non-endemic area: results from a control programme in Bergamo province, Northern Italy. Travel Med Infect Dis. 2018;25:31–34. doi:10.1016/j.tmaid.2018.04.011
13. Murcia L, Carrilero B, Munoz-Davila MJ, Thomas MC, López MC, Segovia M. Risk factors and primary prevention of congenital Chagas disease in a nonendemic country. Clin Infect Dis. 2013;56(4):496–502. doi:10.1093/cid/cis910
14. Carlier Y, Torrico F, Sosa-Estani S, et al. Congenital Chagas disease: recommendations for diagnosis, treatment and control of newborns, siblings and pregnant women. PLoS Negl Trop Dis. 2011;5(10):4–6. doi:10.1371/journal.pntd.0001250
15. Moscatelli G, Moroni S, García-Bournissen F, et al. Prevention of congenital Chagas through treatment of girls and women of childbearing age. Mem Inst Oswaldo Cruz. 2015;110(4):507–509. doi:10.1590/0074-02760140347
16. Bern C, Kjos S, Yabsley MJ, Montgomery SP. Trypanosoma cruzi and Chagas’ disease in the United States. Clin Microbiol Rev. 2011;24(4):655–681. doi:10.1128/CMR.00005-11
17. Piron M, Vergés M, Muñoz J, et al. Seroprevalence of Trypanosoma cruzi infection in at-risk blood donors in Catalonia (Spain). Transfusion. 2008;48(9):1862–1868. doi:10.1111/j.1537-2995.2008.01789.x
18. El Ghouzzi MH, Boiret E, Wind F, et al. Testing blood donors for Chagas disease in the Paris area, France: first results after 18 months of screening. Transfusion. 2010;50(3):575–583. doi:10.1111/j.1537-2995.2009.02476.x
19. Kitchen AD, Hewitt PE, Chiodini PL. The early implementation of Trypanosoma cruzi antibody screening of donors and donations within England: preempting a problem. Transfusion. 2012;52(9):1931–1939. doi:10.1111/j.1537-2995.2012.03599.x
20. Gascon J, Bern C, Pinazo MJ. Chagas disease in Spain, the United States and other non-endemic countries. Acta Trop. 2010;115(1–2):22–27. doi:10.1016/j.actatropica.2009.07.019
21. World Health Organization. World Chagas Disease Day 2021 - WHO campaigns. Available from: https://www.who.int/campaigns/world-chagas-disease-day/2021.
22. PAHO. Chagas disease. Available from: https://www.paho.org/en/topics/chagas-disease.
23. Samuels AM, Clark EH, Galdos-Cardenas G, et al. Epidemiology of and impact of insecticide spraying on Chagas disease in communities in the Bolivian Chaco. PLoS Negl Trop Dis. 2013;7(8):e2358. doi:10.1371/journal.pntd.0002358
24. World Health Organization. Expert committee on the control of Chagas disease: second report. WHO Tech Rep Ser. 2002;905:1–99.
25. United Nations Department of Economic and Social Affairs. 2015 international migration report; 2015.
26. IOM. World migration report 2020; 2020.
27. Bern C, Montgomery SP. An estimate of the burden of Chagas disease in the United States. Clin Infect Dis. 2009;49(5):52–54. doi:10.1086/605091
28. Basile L, Jansà JM, Carlier Y, et al. Chagas disease in European countries: the challenge of a surveillance system. Eurosurveillance. 2011;16(37):3. doi:10.2807/ese.16.37.19968-en
29. World Health Organization. Control y prevención de la enfermedad de Chagas en Europa - Informe de una consulta informal de la OMS [Prevention and Control of Chagas Disease in Europe - report of a WHO informal survey]; 2009.
30. Imai K, Maeda T, Sayama Y, et al. Chronic Chagas disease with advanced cardiac complications in Japan: case report and literature review. Parasitol Int. 2015;64(5):240–242. doi:10.1016/j.parint.2015.02.005
31. Jackson Y, Pinto A, Pett S. Chagas disease in Australia and New Zealand: risks and needs for public health interventions. Trop Med Int Heal. 2014;19(2):212–218. doi:10.1111/tmi.12235
32. McIlwaine C, Cock JC, Brian L. No longer invisible: the Latin American community in London. Queen Mary, Univ London; 2011:142.
33. Monge-Maillo B, López-Vélez R. Challenges in the management of Chagas disease in Latin-American migrants in Europe. Clin Microbiol Infect. 2017;23(5):290–295. doi:10.1016/j.cmi.2017.04.013
34. Sanz MG, De Sario V, Mingo AG, et al. Chagas disease in the United Kingdom: a review of cases at the hospital for Tropical Diseases London 1995–2018. The current state of detection of Chagas disease in the UK. Travel Med Infect Dis. 2020;36:101760. doi:10.1016/j.tmaid.2020.101760
35. Conners EE, Vinetz JM, Weeks JR, Brouwer KC. A global systematic review of Chagas disease prevalence among migrants. Acta Trop. 2016;156(Mc0507):68–78. doi:10.1016/j.actatropica.2016.01.002
36. World Health Organization. Chagas disease in Latin America: an epidemiological update based on 2010 estimates = Maladie de Chagas en Amérique latine: le point épidémiologique basé sur les estimations de 2010. Wkly Epidemiol Rec. 2015;90(06):33–44.
37. Coura JR. The discovery of Chagas disease (1908–1909): great successes and certain misunderstandings and challenges. Rev Soc Bras Med Trop. 2013;46(4):389–390. doi:10.1590/0037-8682-0143-2013
38. Chagas C. Nova tripanozomiaze humana: estudos sobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n. gen., n. sp., ajente etiolojico de nova entidade morbida do homem [Studies about the morphology and life cycle of Schizotrypanum cruzi n. gen., n. sp., causative agent of a new human disease]. Mem Inst Oswaldo Cruz. 1909;1(2):159–218. doi:10.1590/S0074-02761909000200008
39. Segovia J. Estudio sobre tripanosomiasis por el Dr. Juan C. Segovia. [Study about trypanosomiasis by Dr Juan C. Segovia] Rev La Univ. 1916;X(1 (Enero–Marzo)):65–70.
40. Franco-Paredes C, Villamil-Gómez WE, Schultz J, et al. A deadly feast: elucidating the burden of orally acquired acute Chagas disease in Latin America – public health and travel medicine importance. Travel Med Infect Dis. 2020;36:101565. doi:10.1016/j.tmaid.2020.101565
41. Sica RE, Gonzalez Cappa SM, Sanz OP, Mirkin G. Peripheral nervous system involvement in human and experimental chronic American trypanosomiasis. Bull Soc Pathol Exot. 1995;88:156–163.
42. Del Puerto R, Nishizawa JE, Kikuchi M, et al. Lineage analysis of circulating Trypanosoma cruzi parasites and their association with clinical forms of Chagas disease in Bolivia. PLoS Negl Trop Dis. 2010;4(5):1–6. doi:10.1371/journal.pntd.0000687
43. Bhattacharyya T, Falconar AK, Luquetti AO, et al. Development of peptide-based lineage-specific serology for chronic Chagas disease: geographical and clinical distribution of epitope recognition. PLoS Negl Trop Dis. 2014;8(5):e2892. doi:10.1371/journal.pntd.0002892
44. Miles MA, Feliciangeli MD, Rojas De Arias A. Clinical review of molecular epidemiology in guiding control strategies. Br Med J. 2003;326(fig1):1444–1448. doi:10.1136/bmj.326.7404.1444
45. Rassi A, Rassi SG, Rassi A. Sudden death in Chagas’ disease. Arq Bras Cardiol. 2001;76:75–96. doi:10.1590/s0066-782x2001000100008
46. Mady C, Pereira-Barretto AC, Ianni BM, Lopes EA, Pileggi F. Right ventricular endomyocardial biopsy in undetermined form of Chagas’ Disease. Angiology. 1984;35(12):755–759. doi:10.1177/000331978403501201
47. Rassi A, Marin-Neto JA, Rassi A. Chronic Chagas cardiomyopathy: a review of the main pathogenic mechanisms and the efficacy of aetiological treatment following the BENznidazole evaluation for interrupting trypanosomiasis (BENEFIT) trial. Mem Inst Oswaldo Cruz. 2017;112(3):224–235. doi:10.1590/0074-02760160334
48. Brito BODF, Ribeiro ALP. Electrocardiogram in Chagas disease. Rev Soc Bras Med Trop. 2018;51(5):570–577. doi:10.1590/0037-8682-0184-2018
49. Sartori AMC, Ibrahim KY, Nunes Westphalen EV, et al. Manifestations of Chagas disease (American trypanosomiasis) in patients with HIV/AID S. Ann Trop Med Parasitol. 2007;101(1):31–50. doi:10.1179/136485907X154629
50. Meneghelli UG. Chagasic enteropathy. Rev Soc Bras Med Trop. 2004;37(3):252–260. doi:10.1590/S0037-86822004000300012
51. Pinazo MJ, Cañas EG, Elizalde JI, et al. Diagnosis, management and treatment of chronic Chagas’ gastrointestinal disease in areas where Trypanosoma cruzi infection is not endemic. Gastroenterol Hepatol. 2010;33(3):191–200. doi:10.1016/j.gastrohep.2009.07.009
52. Carlier Y, Truyens C, Suarez E, et al. Maternal Trypanosoma cruzi infection, pregnancy outcome, morbidity, and mortality of congenitally infected and non-infected newborns in Bolivia. Am J Trop Med Hyg. 2004;70(2):201–209. doi:10.4269/ajtmh.2004.70.201
53. Flores-Chávez M, Faez Y, Olalla JM, et al. Fatal congenital Chagas’ disease in a non-endemic area: a case report. Cases J. 2008;1(1):302. doi:10.1186/1757-1626-1-302
54. Carlier Y, Altcheh J, Angheben A, et al. Congenital Chagas disease: updated recommendations for prevention, diagnosis, treatment, and follow-up of newborns and siblings, girls, women of childbearing age, and pregnant women. PLoS Negl Trop Dis. 2019;13(10):1–9. doi:10.1371/journal.pntd.0007694
55. Basile L, Ciruela P, Requena-Méndez A, et al. Epidemiology of congenital Chagas disease 6 years after implementation of a public health surveillance system, Catalonia, 2010 to 2015. Eurosurveillance. 2019;24(26):1–16. doi:10.2807/1560-7917.ES.2019.24.26.19-00011
56. Bern C, Messenger LA, Whitman JD, Maguire JH. Chagas disease in the United States: a public health approach. Clin Microbiol Rev. 2019;33(1). doi:10.1128/CMR.00023-19
57. Bua J, Volta BJ, Velazquez EB, Ruiz AM, de Rissio AM, Cardoni RL. Vertical transmission of Trypanosoma cruzi infection: quantification of parasite burden in mothers and their children by parasite DNA amplification. Trans R Soc Trop Med Hyg. 2012;106(10):623–628. doi:10.1016/j.trstmh.2012.03.015
58. Carlier Y, Truyens C. Congenital Chagas disease as an ecological model of interactions between Trypanosoma cruzi parasites, pregnant women, placenta and fetuses. Acta Trop. 2015;151(1):103–115. doi:10.1016/j.actatropica.2015.07.016
59. Pan American Health Organization. Guidelines for the diagnosis and treatment of Chagas disease; 2019.
60. Schijman AG, Altcheh J, Burgos JM, et al. Aetiological treatment of congenital Chagas’ disease diagnosed and monitored by the polymerase chain reaction. J Antimicrob Chemother. 2003;52(3):441–449. doi:10.1093/jac/dkg338
61. Piron M, Fisa R, Casamitjana N, et al. Development of a real-time PCR assay for Trypanosoma cruzi detection in blood samples. Acta Trop. 2007;103(3):195–200. doi:10.1016/j.actatropica.2007.05.019
62. Schijman AG. Molecular diagnosis of Trypanosoma cruzi. Acta Trop. 2018;184(July2017):59–66. doi:10.1016/j.actatropica.2018.02.019
63. Alonso-Padilla J, Gallego M, Schijman A, Gascon J. Molecular diagnostics for Chagas disease: up to date and novel methodologies. Expert Rev Mol Diagn. 2017;17(7):699–710. doi:10.1080/14737159.2017.1338566
64. Duffy T, Bisio M, Altcheh J, et al. Accurate real-time PCR strategy for monitoring bloodstream parasitic loads in Chagas disease patients. PLoS Negl Trop Dis. 2009;3(4):e419. doi:10.1371/journal.pntd.0000419
65. Besuschio SA, Llano Murcia M, Benatar AF, et al. Analytical sensitivity and specificity of a loop-mediated isothermal amplification (LAMP) kit prototype for detection of Trypanosoma cruzi DNA in human blood samples. PLoS Negl Trop Dis. 2017;11(7):1–18. doi:10.1371/journal.pntd.0005779
66. Besuschio SA, Picado A, Muñoz-Calderón A, et al. Trypanosoma cruzi loop-mediated isothermal amplification (Trypanosoma cruzi loopamp) kit for detection of congenital, acute and Chagas disease reactivation. PLoS Negl Trop Dis. 2020;14(8):1–17. doi:10.1371/journal.pntd.0008402
67. Angheben A, Boix L, Buonfrate D, et al. Chagas disease and transfusion medicine: a perspective from non-endemic countries. Blood Transfus. 2015;13(4):540–550. doi:10.2450/2015.0040-15
68. Angheben A, Buonfrate D, Cruciani M, et al. Rapid immunochromatographic tests for the diagnosis of chronic Chagas disease in at-risk populations: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2019;13(5):1–15. doi:10.1371/journal.pntd.0007271
69. Pinazo MJ, Gascon J, Alonso-Padilla J. How effective are rapid diagnostic tests for Chagas disease? Expert Rev Anti Infect Ther. 2021;19(12):1489–1494. doi:10.1080/14787210.2021.1873130
70. Nunes MCP, Beaton A, Acquatella H, et al. Chagas cardiomyopathy: an update of current clinical knowledge and management: a scientific statement from the American Heart Association. Circulation. 2018;138:e169–e209. doi:10.1161/CIR.0000000000000599
71. Morillo CA, Marin-Neto JA, Avezum A, et al. Randomized trial of benznidazole for chronic Chagas’ cardiomyopathy. N Engl J Med. 2015;373(14):1295–1306. doi:10.1056/NEJMoa1507574
72. Torrico F, Gascón J, Barreira F, et al. New regimens of benznidazole monotherapy and in combination with fosravuconazole for treatment of Chagas disease (BENDITA): a phase 2, double-blind, randomised trial. Lancet Infect Dis. 2021;21(8):1129–1140. doi:10.1016/S1473-3099(20)30844-6
73. Peters DH, Adam T, Alonge O, Agyepong IA, Tran N. Republished research: implementation research: what it is and how to do it. Br J Sports Med. 2014;48(8):731–736. doi:10.1136/bmj.f6753
74. Chin-Hong PV, Schwartz BS, Bern C, et al. Screening and treatment of Chagas disease in organ transplant recipients in the United States: recommendations from the Chagas in transplant working group. Am J Transplant. 2011;11(4):672–680. doi:10.1111/j.1600-6143.2011.03444.x
75. Bern C. Chagas disease in the immunosuppressed host. Curr Opin Infect Dis. 2012;25(4):450–457. doi:10.1097/QCO.0b013e328354f179
76. Requena-Méndez A, Albajar-Viñas P, Angheben A, Chiodini P, Gascón J, Muñoz J. Health policies to control Chagas disease transmission in European countries. PLoS Negl Trop Dis. 2014;8(10):e3245. doi:10.1371/journal.pntd.0003245
77. Infectologia SA. Recomendaciones de diagnóstico y seguimiento de la infección por HIV (Sociedad Argentina de Infectología); 2019.
78. Riarte A, Luna C, Sabatiello R, et al. Chagas´disease in patients with kidney transplants: 7 years of experience, 1989–1996. Clin Infect Dis. 1999;29:561–567. doi:10.1086/598634
79. Almeida EA, Lima JN, Lages-Silva E, et al. Chagas’ disease and HIV co-infection in patients without effective antiretroviral therapy: prevalence, clinical presentation and natural history. Trans R Soc Trop Med Hyg. 2010;104(7):447–452. doi:10.1016/j.trstmh.2010.02.004
80. Ringer A, Ruffino JP, Leiva R, et al. Chagas disease reactivation in rheumatologic patients: association with immunosuppressive therapy and humoral response. Clin Rheumatol. 2021;40(7):2955–2963. doi:10.1007/s10067-021-05581-2
81. American Association of Blood Banks. Regulations about Chagas disease; 2021. Available from: https://www.aabb.org/regulatory-and-advocacy/regulatory-affairs/infectious-diseases/chagas-disease.
82. PAHO. Chagas disease. Available from: https://www.paho.org/en/topics/chagas-disease.
83. World Health Organization. Chagas disease: control and elimination. Sixty-Third World Heal Assem. 2010;4:56.
84. World Health Organization. Chagas disease. Available from: https://www.who.int/health-topics/chagas-disease.
85. World Health Organization. Control and prevention of Chagas Disease in Europe. Report of a WHO Informal Consultation (Jointly Organized by WHO Headquarters and the WHO Regional Office for Europe) Geneva, Switzerland, 17–18 December 2009; 2009.
86. Ortí-Lucas RM, Parada-Barba MC, De La Rubia-Ortí JE, Carrillo-Ruiz A, Beso-Delgado M, Boone ALD. Impact of Chagas disease in Bolivian immigrants living in Europe and the risk of stigmatization. J Parasitol Res. 2014;2014:1–7. doi:10.1155/2014/514794
87. Findechagas. Findechagas home page. Available from: https://findechagas.org/home-en/.
88. Coalicion C. Coalición Chagas. Available from: http://www.coalicionchagas.org/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.