Back to Journals » Clinical Interventions in Aging » Volume 21
Diabetes, Osteosarcopenia, and Immobilization: A Novel Nomogram for Predicting Kümmell’s Disease After Osteoporotic Vertebral Fractures
Authors Chen F, Du X, Yang N, Ma K, Wang S, Luo M, Wang W
Received 30 January 2026
Accepted for publication 5 May 2026
Published 15 May 2026 Volume 2026:21 597128
DOI https://doi.org/10.2147/CIA.S597128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Feifan Chen,1,* Xueming Du,2,* Ningning Yang,1,* Ke Ma,1 Songsong Wang,1 Ming Luo,3 Wengang Wang4
1Department of Emergency Medicine, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2Department of Gynaecology and Obstetrics, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 3Department of Spine Surgery and Musculoskeletal Tumor, Zhongnan Hospital of Wuhan University, Wuhan, People’s Republic of China; 4Department of Orthopedics, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ming Luo, Email [email protected] Wengang Wang, Email [email protected]
Background: Kümmell’s disease is a severe post-traumatic vertebral osteonecrosis characterized by delayed collapse and kyphosis following osteoporotic vertebral compression fractures (OVCFs). The transition from acute fracture to nonunion remains poorly understood. Using a single-center retrospective cohort, we aimed to develop and validate a nomogram to predict Kümmell’s disease in patients with acute OVCFs undergoing conservative management.
Methods: We included 626 patients (aged ≥ 50 years) with acute or subacute OVCFs treated conservatively between January 2021 and October 2024, randomly partitioned into a training cohort (n=470) and a validation cohort (n=156). Demographic characteristics, metabolic profiles, medication history, and radiological parameters including MRI-based paraspinal muscle metrics were analyzed. LASSO regression-based feature selection identified candidate predictors from high-dimensional variables, followed by multivariate logistic regression to construct a nomogram.
Results: Kümmell’s disease developed in 12.6% of the training cohort and 10.9% of the validation cohort. Six independent predictors were identified. Diabetes mellitus (OR 40.61, 95% CI 7.80– 211.34), prolonged bed rest > 2 weeks (OR 9.69, 95% CI 3.92– 23.93), and higher initial vertebral compression rate were risk factors. Anti-osteoporosis treatment (OR 0.02), higher lumbar bone mineral density, and greater relative cross-sectional area of the multifidus muscle were protective. The nomogram achieved an area under the curve of 0.938 (95% CI 0.906– 0.970) in the training cohort and 0.882 (95% CI 0.784– 0.980) in the validation cohort.
Conclusion: This nomogram integrates metabolic, biomechanical, and pharmacological factors to predict Kümmell’s disease. Prolonged bed rest was associated with increased nonunion risk, while anti-osteoporosis pharmacotherapy and multifidus muscle integrity were protective. This tool may support precision risk stratification, guiding a shift from passive observation to active intervention for high-risk patients.
Keywords: Kümmell’s disease, osteoporotic vertebral compression fracture, nomogram, osteosarcopenia
Introduction
Osteoporotic vertebral compression fractures (OVCFs) represent a rapidly growing public health crisis in aging populations globally. Although they are the most prevalent fragility fractures, their clinical impact is frequently underestimated until significant complications arise.1 While conservative management, comprising analgesia, bracing, and varying degrees of immobilization, remains the standard first-line treatment for stable fractures, a substantial and distinct subset of patients fails to heal. These patients progress to Kümmell’s disease, a severe form of post-traumatic vertebral osteonecrosis characterized by the delayed development of an intravertebral vacuum cleft, progressive vertebral collapse, and debilitating kyphosis.2 This condition typically manifests insidiously weeks to months after an initially low-energy injury, often leading to severe neurological deficits and necessitating high-risk reconstructive spinal surgery.3–5 The clinical and economic burden is immense, yet the transition from an acute and seemingly benign fracture to this catastrophic nonunion remains poorly elucidated in current orthopedic practice.6
The pathogenesis of Kümmell’s disease is widely believed to be multifactorial, involving a complex interaction between ischemic necrosis and biomechanical instability, yet accurate risk stratification remains elusive.7 Although advanced age and low bone mineral density (BMD) are established risk factors for the initial fracture, they fail to specifically predict which fractures will progress to nonunion.8 Emerging evidence points to a broader constellation of risk factors, including metabolic comorbidities like diabetes mellitus, which may impair bone microvascularity, and the functional status of paraspinal musculature, often referred to as osteosarcopenia.9,10 However, prior studies have largely analyzed these variables in isolation or through univariate associations, and they have failed to capture the synergistic effects of systemic metabolic health, local mechanical stability, and functional muscle integrity. Recent studies have attempted to identify predictive factors for Kümmell’s disease. Farrokhi et al reported incidence and risk factors following vertebroplasty but did not construct a predictive model,6 and Huang et al identified several associated factors through conventional regression without integrating them into a clinically applicable tool.8 No validated, multivariate prediction model currently exists for this condition. Consequently, clinicians are forced to rely on reactive management strategies, often identifying the disease only after irreversible deformity has been established.
In this study, we aimed to bridge this knowledge gap by developing and validating a comprehensive and multivariate clinical prediction nomogram for Kümmell’s disease in patients with acute OVCFs. By systematically integrating a wide array of potential predictors, such as detailed metabolic profiles, medication history including glucocorticoids and anti-osteoporosis agents, fracture morphology, and quantitative paraspinal muscle metrics, we sought to mathematically model the risk of nonunion. Our primary objective is to move beyond traditional passive observation and provide clinicians with a robust and quantitative instrument. This tool aims to estimate individual risk precisely at the time of diagnosis, thereby guiding more aggressive monitoring or early intervention to alter the natural history of this devastating complication.
Materials and Methods
Study Design and Participants
We conducted a retrospective cohort study at our institution to develop a prediction model for Kümmell’s disease. Ethical clearance for this study was granted by the Ethics Committees of the First Affiliated Hospital of Zhengzhou University (No. 2023001K). The research was performed in compliance with the guidelines of the Declaration of Helsinki. Given the retrospective nature of the study and the anonymization of patient data, the requirement for informed consent was waived.
We screened patients admitted to our institution between January 2021 and October 2024. The inclusion criteria were as follows: (1) patients aged 50 years or older; (2) a confirmed diagnosis of acute or subacute OVCFs based on clinical presentation (eg, back pain) and magnetic resonance imaging demonstrating bone marrow edema; (3) patients who opted for conservative treatment strategies; (4) availability of complete clinical and radiological data, including BMD of the lumbar spine and paraspinal muscle assessments; and (5) a minimum clinical follow-up period of 12 months to ascertain the development of Kümmell’s disease.
Patients were excluded if they met any of the following criteria: (1) vertebral fractures resulting from high-energy trauma or pathological fractures secondary to malignancy; (2) presence of confounding spinal pathologies, such as severe spinal stenosis, spinal infection, or ankylosing spondylitis; (3) history of prior surgical interventions at the index vertebral level (eg, vertebroplasty, kyphoplasty, or pedicle screw fixation) before the diagnosis of Kümmell’s disease; (4) incomplete baseline data or loss to follow-up; or (5) contraindications preventing necessary imaging examinations.
Data Collection and Radiological Assessment
Data extraction was performed by two independent investigators using the hospital’s electronic medical record system. Any discrepancies were resolved through consultation with a senior investigator.
Demographic and Clinical Variables
Baseline characteristics included age, gender, smoking status, and history of comorbidities. Specifically, we recorded diabetes status, history of systemic glucocorticoid use, and adherence to anti-osteoporosis treatment. Clinical outcomes included the duration of bed rest (dichotomized as >2 weeks for analysis) and pain intensity, assessed using the Visual Analogue Scale (VAS) at admission and at 1-month follow-up.
Radiological Parameters
Radiological data were obtained from the Picture Archiving and Communication System. The specific fracture segment was recorded, with fractures located between T11 and L2 defined as thoracolumbar fractures. BMD of the lumbar spine was measured using dual-energy X-ray absorptiometry. Vertebral body compression rate (%) was calculated on lateral radiographs using the formula: compression rate = [1−(anterior vertebral height/posterior vertebral height)] ×100%.
Paraspinal Muscle Measurement
To assess sarcopenia and muscle quality, the cross-sectional areas (CSA) of the psoas major, erector spinae, and multifidus muscles were measured on axial T2-weighted magnetic resonance images at the level of the L3 pedicle. To adjust for inter-patient variability in body size, the relative cross-sectional area (rCSA) was calculated using the following formula: rCSA=CSA muscle/CSA L3 vertebral body. All radiological measurements were performed by two experienced orthopedic surgeons blinded to the clinical outcomes, with the average values used for analysis to ensure reliability.
Outcome Definition
The primary outcome of interest was the development of Kümmell’s disease. This was defined based on established radiographic criteria observed during the follow-up period (Figure 1A–C), specifically: (1) the presence of an intravertebral vacuum cleft sign on plain radiographs or CT scans; or (2) distinct dynamic instability of the fractured vertebral body observed on hyperextension and flexion lateral radiographs.
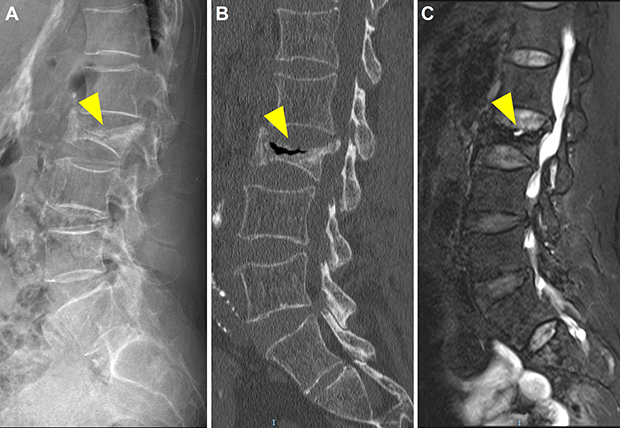 |
Figure 1 Representative images of Kümmell’s disease. (A) Lateral X-ray taken 9 months after minor trauma shows collapse of the L2 vertebral body with angular kyphosis. (B) Sagittal CT image confirms L2 vertebral body collapse and signs of osteonecrosis with an intravertebral vacuum cleft. (C) T2-weighted MRI shows post-traumatic avascular necrosis. The yellow arrowhead indicates the intravertebral vacuum cleft, a hallmark sign of Kümmell’s disease. |
Construction of Training and Validation Cohorts
To ensure the robustness and generalizability of the predictive model, the study population was randomly partitioned into a training cohort and a validation cohort at a ratio of 7:3. The randomization process was performed using computer-generated random numbers (R software) to avoid selection bias. The training cohort was utilized to identify independent predictive factors and construct the nomogram, while the validation cohort was strictly reserved to evaluate the model’s external performance and prevent overfitting. Baseline characteristics were compared between the two cohorts to ensure balanced distribution.
Statistical Analysis
Continuous variables were examined for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation and compared using the Student’s t-test. Non-normally distributed data were presented as median and compared using the Mann–Whitney U-test. Categorical variables were expressed as frequencies (%) and analyzed using the Chi-square test or Fisher’s exact test, as appropriate. In the training cohort, the Least Absolute Shrinkage and Selection Operator (LASSO) logistic regression algorithm was employed to minimize collinearity and select the most significant predictive features with non-zero coefficients. Multivariable logistic regression analysis was then conducted to identify independent risk factors for Kümmell’s disease, which were subsequently incorporated into a nomogram prediction model. The performance of the nomogram was evaluated in both cohorts using the receiver operating characteristic curve, with the area under the curve (AUC) quantifying discrimination ability. Calibration plots were generated to assess the agreement between predicted probabilities and observed outcomes (bootstrapping with 1000 resamples). Furthermore, Decision Curve Analysis was performed to evaluate the clinical utility and net benefit of the model across a range of threshold probabilities. No formal a priori sample size calculation was performed given the exploratory nature of this study; however, the training cohort included 59 events for 6 predictors, yielding an events per variable ratio of approximately 10, which meets the commonly recommended minimum threshold for stable logistic regression estimates. All statistical analyses were performed using R software (version 4.2.2). A two-sided P-value of <0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
A total of 626 patients with OVCFs were included in the final analysis. The cohort was divided into a training set (n = 470) and an internal validation set (n = 156). The incidence of Kümmell’s disease was 12.6% (59/470) in the training cohort and 10.9% (17/156) in the validation cohort. Baseline demographic and clinical characteristics were generally well-balanced between the two cohorts (Table 1). No significant differences were observed in age, sex distribution, comorbidities (diabetes, glucocorticoid use), or BMD, indicating that the datasets were comparable (p > 0.05). The only exception was smoking history, which was more prevalent in the validation cohort (22.4% vs 15.1%, p = 0.034).
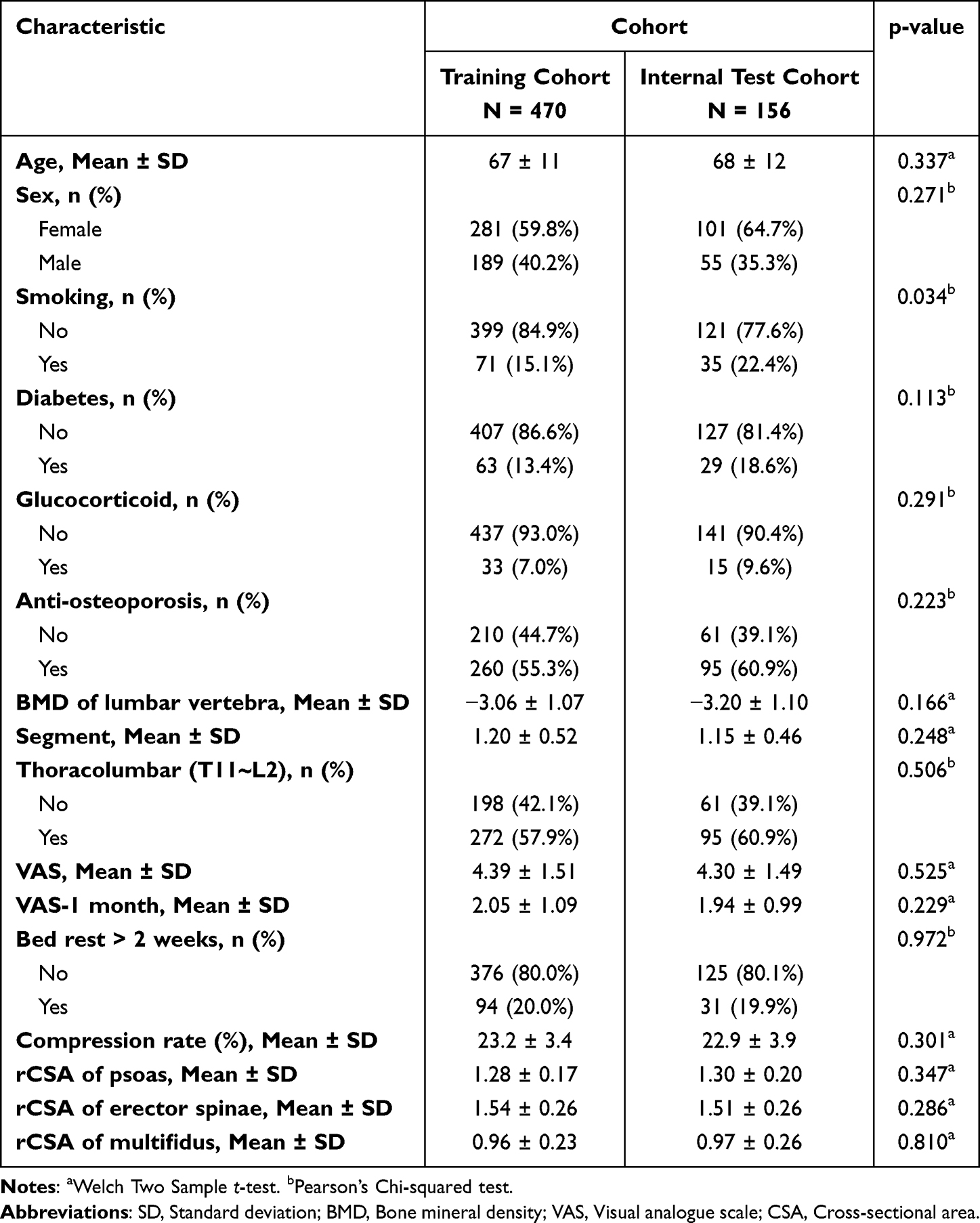 |
Table 1 Patient Demographics and Baseline Characteristics |
Variable Selection via LASSO Regression
To avoid overfitting and address multicollinearity, the LASSO regression was applied to the initial candidate variables in the training cohort. Based on the optimal lambda value (λ = 0.012), dimensionality reduction was performed, narrowing down the potential predictors from the original comprehensive list to nine candidate variables with non-zero coefficients (Figure 2A and B). These factors included diabetes, glucocorticoid use, anti-osteoporosis treatment, lumbar BMD, VAS score at 1 month, duration of bed rest, vertebral compression rate, and paraspinal muscle metrics (rCSA of erector spinae and multifidus). Receiver operating characteristic curve analysis for individual predictors of Kummell’s disease demonstrated variable discriminatory performance, with area under the curve values ranging from 0.525 to 0.846 (Figure 2C).
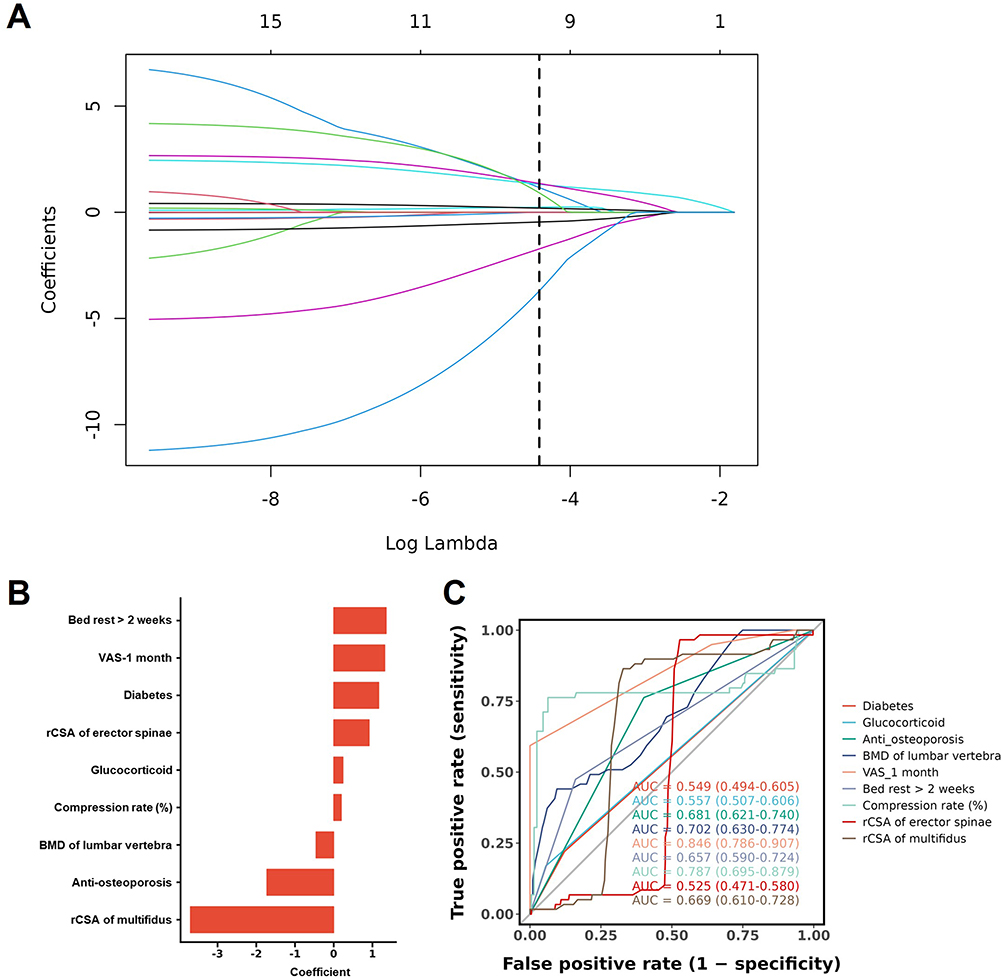 |
Figure 2 Variable screening using the LASSO regression. (A) LASSO coefficient profiles of the candidate variables. Each colored line represents a candidate predictor; the x-axis shows the log(λ) value and the y-axis shows the coefficient magnitude. As the regularization penalty increases (left to right), less informative variables are shrunk to zero. (B) Selection of the optimal tuning parameter (λ) via ten-fold cross-validation. The left dashed vertical line indicates the λ with minimum deviance (λmin = 0.012), which retained nine variables with non-zero coefficients. (C) Receiver operating characteristic curves for individual predictors evaluated by univariate logistic regression, with AUC values ranging from 0.525 to 0.846. |
Identification of Independent Predictors
Multivariable logistic regression analysis was performed on the candidate variables to identify independent risk factors for Kümmell’s disease. The final model identified six independent predictors (Table 2). Significant risk factors associated with disease progression included a history of diabetes (adjusted odds ratio [OR] 40.61, 95% CI 7.80–211.34; p < 0.001), prolonged bed rest >2 weeks (adjusted OR 9.69, 95% CI 3.92–23.93; p < 0.001), and a higher initial vertebral compression rate (adjusted OR 1.42 per percentage increase, 95% CI 1.23–1.63; p < 0.001). Conversely, protective factors included receiving anti-osteoporosis treatment (adjusted OR 0.02, 95% CI 0.00–0.09; p < 0.001), higher lumbar BMD (adjusted OR 0.41, 95% CI 0.28–0.62; p < 0.001), and a greater rCSA of the multifidus muscle (p < 0.001).
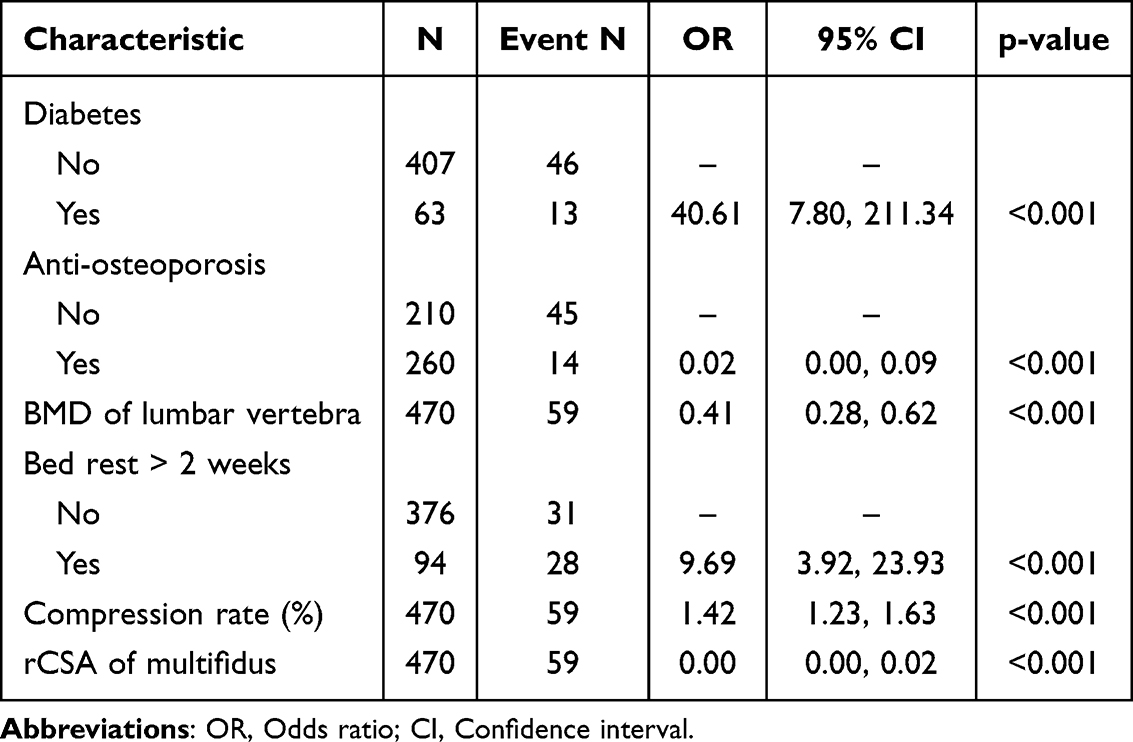 |
Table 2 Results of Multivariate Logistic Regression for Training Cohort |
Development and Validation of the Prediction Model
A diagnostic nomogram was constructed based on the six independent predictors (Figure 3A). The model demonstrated excellent discrimination performance. In the training cohort, the AUC was 0.938 (95% CI 0.906–0.970). This high predictive accuracy was maintained in the independent validation cohort, with an AUC of 0.882 (95% CI 0.784–0.980), suggesting robust generalizability (Figure 3B). Calibration plots for both cohorts showed good agreement between the nomogram-predicted probabilities and the actual observed outcomes, with the curves fitting close to the ideal diagonal line (Figure 3C and D).
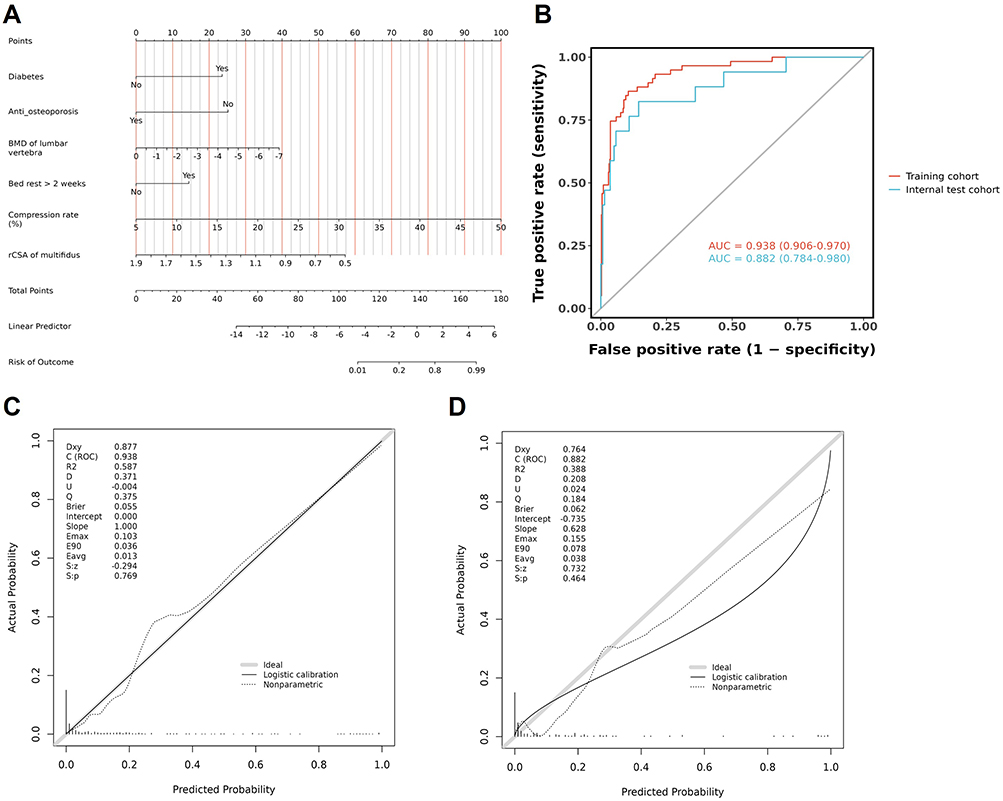 |
Figure 3 Development and validation of the prediction model. (A) Nomogram for predicting the probability of Kümmell’s disease after osteoporotic vertebral compression fractures. (B) Receiver operating characteristic curves for the training and validation cohorts. (C) Calibration plot of the nomogram in the training cohort. (D) Calibration plot of the nomogram in the validation cohort. |
Clinical Utility
Decision Curve Analysis was performed to evaluate the clinical utility of the nomogram. The decision curve analysis showed that using this nomogram to predict Kümmell’s disease provided a greater net benefit than treating either all or no patients across a wide range of threshold probabilities (Figure 4A and B). This indicates that the model is clinically useful for decision-making without increasing the rate of false positives unnecessarily.
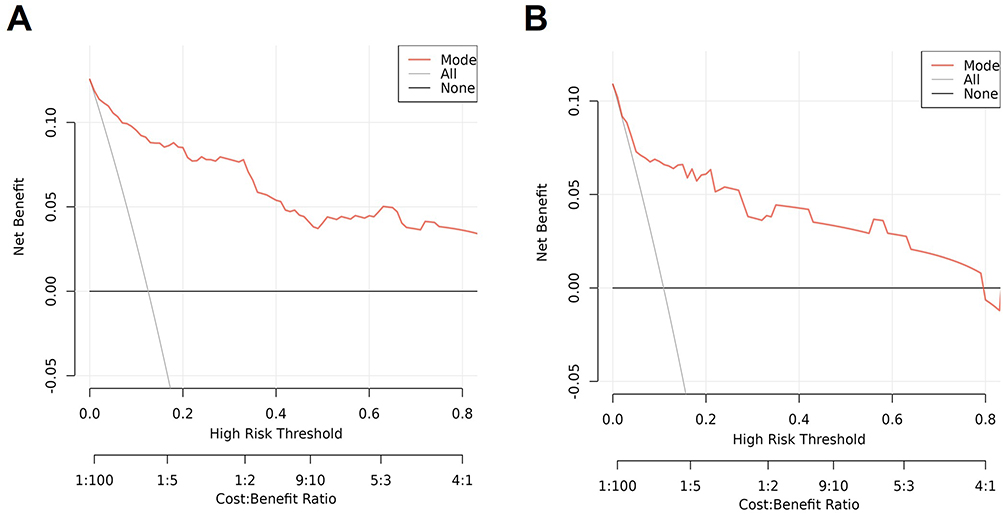 |
Figure 4 Assessment of clinical utility of the nomogram. (A) Decision curve analysis of the nomogram in the training cohort. (B) Decision curve analysis of the nomogram in the validation cohort. The x-axis represents the threshold probability, defined as the minimum predicted risk at which a clinician would consider intervention. The y-axis represents the net benefit, which accounts for the trade-off between true positives and false positives. The red line represents the nomogram; the gray line represents the strategy of treating all patients, and the horizontal black line represents treating none. The nomogram provides a greater net benefit than both default strategies across a wide range of threshold probabilities. |
Discussion
This study successfully established and validated a novel clinical nomogram to predict the risk of Kümmell’s disease, demonstrating exceptional discriminatory performance with an AUC of 0.938 in the training cohort and 0.882 in the independent validation cohort. By employing LASSO and multivariate logistic regression, we distilled a complex clinical profile into six independent predictors: diabetes mellitus, prolonged bed rest, higher initial vertebral compression rate, lower lumbar BMD, reduced relative cross-sectional area of the multifidus muscle, and the absence of anti-osteoporosis treatment. These findings provide a multi-dimensional view of fracture nonunion, suggesting that it is not merely a consequence of bone fragility but the result of a pathological convergence of metabolic compromise, mechanical instability, and inadequate biological repair. This model significantly outperforms reliance on any single risk factor and offers a precision medicine tool that can be immediately integrated into clinical workflows.
The most striking finding of our analysis is the profound impact of systemic metabolic and bone health on the healing process. Diabetes mellitus was identified as a strong risk factor with an adjusted odds ratio of 40.61 (95% CI 7.80–211.34). The wide confidence interval reflects the relatively small number of diabetic patients with events (13 of 63) and should be interpreted with caution, as the point estimate may overstate the true effect size. Residual confounding from unmeasured variables such as glycemic control (HbA1c), diabetes duration, and diabetic microvascular complications cannot be excluded. Nonetheless, the direction and statistical strength of this association are consistent with the established pathophysiology of diabetic bone disease, in which hyperglycemia, oxidative stress, and the accumulation of advanced glycation end-products deteriorate collagen quality and impair osteoblast function, rendering the bone microenvironment incapable of bridging the fracture gap.11–13 Conversely, the use of anti-osteoporosis medication provided near-complete protection with an adjusted odds ratio of 0.02. This finding strongly validates the mechanistic theory that stabilizing bone turnover, whether through anti-resorptives like bisphosphonates and denosumab or through anabolic agents, is essential to prevent the resorption of the fracture callus.14,15 It highlights that treating the underlying osteoporosis is as critical as managing the fracture itself, yet a significant deficiency in appropriate pharmaceutical management persists in clinical practice.
From a biomechanical perspective, our results illuminate the critical role of dynamic spinal stability. We found that atrophy of the multifidus muscle, which serves as a key stabilizer of the lumbar spine, was a significant predictor of progression to Kümmell’s disease. This supports the concept of osteosarcopenia, in which the loss of deep muscular support transfers excessive load onto the already compromised vertebral body, accelerating collapse and preventing union.16,17 Furthermore, our data challenges the dogma of strict bed rest. We found that bed rest exceeding two weeks significantly increased the risk of nonunion. Rather than protecting the spine, prolonged immobilization appears to fuel a deleterious cycle of disuse osteoporosis and rapid paraspinal muscle atrophy, further destabilizing the fracture site. Additionally, a higher initial compression rate indicates severe disruption of the trabecular architecture and vascular supply, creating a mechanical defect that is too large for spontaneous healing.18
The clinical implications of this nomogram are transformative for the management of acute OVCFs. Currently, many patients are managed with a standard protocol of bracing and pain control, but our model suggests this approach is inadequate for high-risk groups. For a patient identified by the nomogram as high-risk, such as a diabetic patient with sarcopenia and a severe compression fracture, the standard of care should shift from passive observation to active intervention. This includes the immediate initiation of anti-osteoporosis pharmacotherapy, strict glycemic control, and targeted rehabilitation to preserve muscle tone rather than prolonged bed rest. Furthermore, early surgical stabilization techniques such as percutaneous vertebral augmentation might be indicated for these patients before the development of a vacuum cleft or neurological deficit, effectively serving as a prophylactic measure against collapse.19
Despite its strengths, this study has limitations that merit consideration. First, the retrospective single-center design introduces potential selection bias. Patients who were lost to follow-up or transferred to other institutions were excluded, which may have led to an underrepresentation of more severe or less compliant cases. Treatment decisions, including the initiation of anti-osteoporosis therapy and the duration of bed rest, were not standardized but reflected individual physician judgment, introducing indication bias that cannot be fully adjusted for in a retrospective analysis. Second, internal validation was performed using a random cohort split rather than k-fold cross-validation or bootstrapped internal validation, which may provide more stable performance estimates. External validation using independent multicenter datasets is needed to confirm the generalizability of the model across different ethnic groups and healthcare settings. Third, MRI-based paraspinal muscle measurements are subject to inter-observer variability. Although our measurements were performed by trained radiologists, we did not report inter-rater or intra-rater reliability coefficients, and this measurement may not be routinely available in resource-limited settings. Future studies should assess measurement reproducibility and explore more accessible surrogates such as CT-based muscle indices or functional assessments. Finally, translating this nomogram into clinical practice requires consideration of practical and ethical challenges. Implementing risk-stratified early intervention, particularly recommending early surgical stabilization for high-risk patients, necessitates shared decision-making with patients and validation through prospective interventional trials before it can be adopted as a standard of care. Nevertheless, this study represents a significant step forward as it provides a validated and evidence-based framework to identify fractures susceptible to nonunion and prevent the transition to Kümmell’s disease, ultimately improving long-term functional outcomes for this fragile patient population.
Conclusion
This study addresses the lack of precision tools for predicting vertebral osteonecrosis by establishing and validating a novel, multidimensional clinical nomogram for Kümmell’s disease. The model achieved high predictive accuracy by synthesizing systemic metabolic health, local biomechanics, and treatment history. A notable finding is the association between prolonged bed rest and increased risk of Kümmell’s disease, suggesting that immobilization may contribute to a cycle of disuse osteoporosis and paraspinal muscle atrophy rather than serving as a protective measure. Furthermore, the study quantifies the profound protective effect of anti-osteoporosis medication and the severe risk posed by diabetes. This evidence-based framework empowers clinicians to identify high-risk patients at diagnosis, advocating for a paradigm shift towards early mobilization, aggressive metabolic management, and pharmacotherapy to prevent irreversible spinal deformity. Prospective, multicenter validation across diverse populations and healthcare settings is warranted to confirm the generalizability of this nomogram before its widespread clinical adoption.
Abbreviations
OVCF, Osteoporotic vertebral compression fracture; BMD, Bone mineral density; VAS, Visual Analogue Scale; CSA, Cross-sectional areas; LASSO, Least Absolute Shrinkage and Selection Operator; AUC, Area under the curve.
Data Sharing Statement
The data supporting this study are available from the corresponding author (Wengang Wang) for a reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committees of the First Affiliated Hospital of Zhengzhou University. The data were obtained from the medical records, as a retrospective study and data analysis were performed anonymously, this study was exempt from the informed consent from patients. All procedures were in compliance with the Helsinki Declaration (https://www.wma.net/policies-post/wma-declaration-of-helsinki/).
Funding
Key Scientific and Technological Project of the Science and Technology Department of Henan Province (No. 242102310075).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ao J, Xu Z, Gao Z, et al. What factors contribute to the poor prognosis of conservative treatment for Osteoporotic Vertebral Compression Fracture (OVCF): a systematic review. Clin Interv Aging. 2025;20:2717–11. doi:10.2147/cia.S556710
2. Kim YC, Kim YH, Ha KY. Pathomechanism of intravertebral clefts in osteoporotic compression fractures of the spine. Spine J. 2014;14(4):659–666. doi:10.1016/j.spinee.2013.06.106
3. Sun YL, Dun W, Gu T, Shi HG, Cui W, Deng XG. Short-segment fixation with bone cement augmentation for unstable Kümmell disease: a minimum 2-year follow-up study. Clin Spine Surg. 2025. doi:10.1097/bsd.0000000000001956
4. Huang Y, Chang Z, Wang S, He B. Short-segment bone cement-augmented pedicle screw fixation combined with bone grafting for management of Kummell disease with segmental instability. Med Sci Monitor. 2025;31:e949901. doi:10.12659/msm.949901
5. Dong C, Wei H, Zhu Y, Zhou J, Ma H. Application of titanium alloy 3D-printed artificial vertebral body for stage III Kümmell’s disease complicated by neurological deficits. Clin Interv Aging. 2020;15:2265–2276. doi:10.2147/cia.S283809
6. Farrokhi MR, Mousavi SR, Hosseini SA, Rafieossadat R, Masjoodi S, Hosseini K. Kümmell’s disease in benign vertebral compression fractures: incidence, risk factors, and outcomes following percutaneous vertebroplasty. Clin Neurol Neurosurg. 2026;261:109262. doi:10.1016/j.clineuro.2025.109262
7. Xu Y, Huang S, Li Z, et al. Single-cell RNA landscape of osteoimmune microenvironment in osteoporotic vertebral compression fracture and Kümmell’s disease. Front Cell Development Biol. 2023;11:1276098. doi:10.3389/fcell.2023.1276098
8. Huang Y, Yue D, Gu Y, et al. Predictive factors associated with the onset of Kummell’s disease. Eur Spine J. 2025;34(11):4966–4976. doi:10.1007/s00586-025-08833-w
9. Schwartz AV. Diabetes, bone and glucose-lowering agents: clinical outcomes. Diabetologia. 2017;60(7):1170–1179. doi:10.1007/s00125-017-4283-6
10. Hirschfeld HP, Kinsella R, Duque G. Osteosarcopenia: where bone, muscle, and fat collide. Osteoporos Int. 2017;28(10):2781–2790. doi:10.1007/s00198-017-4151-8
11. Hofbauer LC, Busse B, Eastell R, et al. Bone fragility in diabetes: novel concepts and clinical implications. Lancet Diabetes Endocrinol. 2022;10(3):207–220. doi:10.1016/s2213-8587(21)00347-8
12. Saito M, Marumo K. Collagen cross-links as a determinant of bone quality: a possible explanation for bone fragility in aging, osteoporosis, and diabetes mellitus. Osteoporos Int. 2010;21(2):195–214. doi:10.1007/s00198-009-1066-z
13. Napoli N, Chandran M, Pierroz DD, Abrahamsen B, Schwartz AV, Ferrari SL. Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinol. 2017;13(4):208–219. doi:10.1038/nrendo.2016.153
14. Bone HG, Bolognese MA, Yuen CK, et al. Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. J Clin Endocrinol Metab. 2011;96(4):972–980. doi:10.1210/jc.2010-1502
15. Langdahl BL, Lorentzon M, Borgen TT, et al. Treatment patterns of romosozumab in postmenopausal women with severe osteoporosis in Denmark: findings from the ROmosozumab in Scandinavia real-world Evidence Study (ROSES). Osteoporos Int. 2025. doi:10.1007/s00198-025-07756-y
16. Jiang JL, Yu R, Zhang Y, et al. Developing and validating a combined model with CT-based paraspinal muscle radiomics and clinical features to predict residual low back pain after percutaneous kyphoplasty. Eur Spine J. 2025. doi:10.1007/s00586-025-09627-w
17. Gao X, Du J, Hao D, He B, Yan L. Risk factors for residual back pain following percutaneous vertebral augmentation: the importance of paraspinal muscle fatty degeneration. Int Orthop. 2023;47(7):1797–1804. doi:10.1007/s00264-023-05809-7
18. Chen T, Chu G, Qu Y, et al. Risk factor analysis of refracture in the same cemented vertebra after percutaneous kyphoplasty for Kümmell’s disease. J Neurosurg Spine. 2024;40(2):255–264. doi:10.3171/2023.8.Spine23498
19. Jiang J, Lei C, Guo Z, et al. Comparison of the percutaneous kyphoplasty “Trinity” anchoring technique versus conventional percutaneous kyphoplasty for Kummell disease: a retrospective observational study. World Neurosurg. 2025;205:124747. doi:10.1016/j.wneu.2025.124747
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.