Back to Journals » Drug Design, Development and Therapy » Volume 20
Dexmedetomidine Use and Intraoperative Bradycardia During Radiofrequency Rhizotomy for Trigeminal Neuralgia: A Retrospective Observational Study
Authors Tang CH, Wu SC ![]() , Yu CM, Hong CL, Yang JT, Hsiao PN, Cheng HL
, Yu CM, Hong CL, Yang JT, Hsiao PN, Cheng HL ![]() , Hsu SC, Lai YT, Kao CW
, Hsu SC, Lai YT, Kao CW
Received 29 December 2025
Accepted for publication 28 February 2026
Published 7 March 2026 Volume 2026:20 592347
DOI https://doi.org/10.2147/DDDT.S592347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Chen-Hsi Tang,1 Shao-Chun Wu,2,* Chung-Ming Yu,1 Chian-Lang Hong,1 Jen-Tsung Yang,3 Po-Ni Hsiao,4 Hsiao-Liang Cheng,4 Shih-Che Hsu,5 Yuan-Tao Lai,6 Ching-Wei Kao1,*
1Department of Anesthesiology, Chiayi Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Chiayi, Taiwan; 2Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung City, Taiwan; 3Department of Neurosurgery, Chiayi Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Chiayi, Taiwan; 4Department of Anesthesiology, National Taiwan University Hospital, Taipei City, Taiwan; 5Department of Anesthesiology, Chung Shan Medical University Hospital, Taichung City, Taiwan; 6Department of Anesthesiology, National Cheng Kung University Hospital, Tainan, Taiwan
*These authors contributed equally to this work
Correspondence: Ching-Wei Kao, Department of Anesthesiology, Chiayi Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Chiayi, Taiwan, Tel +886 975056581, Email [email protected] Shao-Chun Wu, Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, 833, Taiwan, Tel +886975056395, Email [email protected]
Purpose: Intraoperative bradycardia is a recognized complication during radiofrequency (RF) rhizotomy for trigeminal neuralgia, primarily related to the trigeminal–cardiac reflex. Dexmedetomidine is commonly used for its sedative and analgesic properties during these procedures; however, its hemodynamic impact has not been well characterized. This study aimed to evaluate the association between dexmedetomidine use and intraoperative bradycardia and to identify relevant clinical risk factors.
Patients and Methods: This retrospective observational study included 517 patients who underwent RF rhizotomy for trigeminal neuralgia under monitored anesthesia care between August 2020 and December 2022. Patients were categorized into dexmedetomidine (Dex) and non-dexmedetomidine (Non-Dex) groups. The primary outcome was intraoperative bradycardia, defined as a heart rate < 60 beats per minute or the need for atropine. Secondary outcomes included atropine use, intraoperative heart rate distribution, and anesthetic drug requirements. Multivariable logistic regression and age-stratified subgroup analyses were performed.
Results: Dexmedetomidine was administered in 331 patients (64.0%). Intraoperative bradycardia occurred more frequently in the Dex group than in the Non-Dex group (59.8% vs 29.0%, p< 0.001), with a higher incidence of atropine administration (18.1% vs 4.8%, p< 0.001). Dexmedetomidine use was independently associated with bradycardia (odds ratio [OR] 5.16; 95% confidence interval [CI] 2.57– 10.39; p< 0.001). Notably, dexmedetomidine significantly reduced intraoperative requirements for midazolam (median 0.038 vs 0.044 mg/kg/h; p< 0.001) and propofol (median 0.73 vs 1.25 mg/kg/h; p< 0.001). Younger age (OR 0.97 per year; 95% CI, 0.96– 0.99; p< 0.001) and longer anesthesia duration (OR 1.04 per minute; 95% CI, 1.02– 1.06; p< 0.001) were additional predictors of bradycardia. Age-stratified analyses revealed a more pronounced reduction in heart rate among younger patients (< 45 years) receiving dexmedetomidine, suggesting an age-dependent modulation of the bradycardic response.
Conclusion: Although dexmedetomidine use was associated with a higher incidence of intraoperative bradycardia, it provided meaningful anesthetic benefits during RF rhizotomy, including significant sedative-sparing effects and reduced exposure to other hypnotic agents. With appropriate monitoring and individualized dosing, particularly in younger patients, dexmedetomidine remains a safe and valuable sedative option for trigeminal neuralgia procedures.
Keywords: radiofrequency rhizotomy, bradycardia, dexmedetomidine, trigeminal neuralgia, trigeminal-cardiac reflex
Introduction
Radiofrequency (RF) rhizotomy, or RF ablation (RFA), is an established treatment for trigeminal neuralgia (TN) with high success rates and significant pain relief for many patients.1–3 However, this procedure appears to be associated with bradycardia in 12.5–25% of cases during the surgical procedure and anesthesia, primarily due to trigeminal-cardiac reflex (TCR), which is characterized by sudden bradycardia due to enhanced parasympathetic activity. In addition, anesthetic agents and techniques may also contribute to intraoperative bradycardia.4,5
Despite these hemodynamic challenges and potential TCR risks, previous literature has not comprehensively explored anesthesia-related factors, including sedative medication selection, that might mitigate or aggravate these complications. Prior studies on bradycardia during RF rhizotomy have largely focused on procedural or neurophysiological triggers, such as foramen ovale puncture and thermal lesioning, with limited attention to the role of sedative choice or dosing strategies in modulating hemodynamic responses. The expression and severity of the TCR may be influenced by anesthetic depth, sedative class, and the degree of autonomic modulation. Furthermore, autonomic responsiveness and vagal tone vary with age, and younger individuals may exhibit heightened parasympathetic reactivity that could amplify bradycardic responses to both the TCR and sympatholytic agents.
Dexmedetomidine (DEX) is a highly selective α2-adrenergic agonist with significant analgesic,6,7 sedative,8 and sympatholytic properties.8 It exerts its analgesic effect through activation of central α2-adrenergic receptors, particularly in the spinal cord and brainstem.9–11 This activation inhibits pain-related neurotransmitter release and enhances descending inhibitory pathways.9,12 Known for its opioid-sparing properties,13,14 dexmedetomidine reduces postoperative opioid requirements and related side effects such as respiratory depression, nausea, and vomiting.15–17 Compared with acetaminophen, it provides greater postoperative analgesia and lowers opioid consumption.18 Furthermore, a systematic review and meta-analysis have demonstrated dexmedetomidine as a viable opioid substitute in opioid-free anesthesia protocols,19 making it an ideal anesthetic option during the RF rhizotomy procedures. Dexmedetomidine is particularly well-suited for the unique biphasic sedation demands of RF rhizotomy. During the sensory stimulation phase, it provides cooperative sedation with preserved airway patency and spontaneous respiration, allowing patients to remain responsive to verbal commands and report paresthesia for accurate needle targeting. During the subsequent ablation phase, when deeper sedation is required, dexmedetomidine produces less respiratory depression than propofol or benzodiazepines at equivalent sedation depths, thereby reducing the risk of airway compromise during the transition to unconsciousness. However, its sympatholytic profile carries a distinctive risk of hemodynamic compromise that differs from the transient hypotension associated with propofol.
Nonetheless, clinicians must remain vigilant regarding potential hemodynamic adverse effects, particularly hypotension and bradycardia,15 which warrants investigation in the specific context of RF rhizotomy procedures for trigeminal neuralgia. Dexmedetomidine, through its central sympatholytic action at the locus coeruleus, reduces sympathetic outflow and may thereby amplify vagally mediated bradycardic responses triggered by trigeminal nerve manipulation. Identifying anesthesia-related risk factors for bradycardia is of particular practical relevance in high-volume neurosurgical pain procedures, where individualized sedative selection and vigilant hemodynamic monitoring may substantially improve patient safety.
Materials and Methods
Study Design
This retrospective observational study was conducted at Chiayi Chang Gung Memorial Hospital, a single center, between August 2020 and December 2022. We reviewed the anesthesia records, and a total of 519 patients who underwent RF rhizotomy were enrolled. Demographic and clinical data were collected from the hospital’s electronic medical and anesthesia recording systems. This study was approved by the Institutional Review Board of the Chang Gung Memorial Hospital, Taiwan (IRB No. 202401798B0). Given the retrospective and observational nature of this study, the requirement for individual informed consent was waived by the IRB. All patient data were de-identified prior to analysis to ensure confidentiality. This study was conducted in accordance with the Declaration of Helsinki.
Surgical Procedure
The surgical protocol comprised three sequential stages. The first stage involved localizing the trigeminal nerve using intraoperative computed tomography (CT) and a navigation system (Brainlab AG, Munich, Germany). Subsequently, the stimulation needle’s position was verified using sensory stimulation (50 Hz, 1 ms, 0–1 V) to elicit paresthesia, with patient feedback ensuring proper targeting. Once needle placement was verified, RF rhizotomy was executed for 2–3 minutes, maintaining a tip temperature of 70°C to 90°C. A single surgeon performed all procedures.
Anesthesia Management
Sedation and analgesia were provided under monitored anesthesia care by a dedicated team of anesthesiologists. During the first stage (CT-guided localization), sedation was initiated with either dexmedetomidine or midazolam at the discretion of the attending anesthesiologist to maintain a Ramsay Sedation Scale (RSS) score of 2. Dexmedetomidine was administered intravenously with a loading dose of 0.5–1.0 μg/kg over 10 minutes, followed by a maintenance infusion of 0.2–1.0 μg/kg/h. Alternatively, midazolam was administered as intermittent boluses of 1–2.5 mg until the target sedation level was reached.
Analgesia was provided using either alfentanil or fentanyl. Alfentanil was administered via a Target-Controlled Infusion (TCI) system using the Scott model, targeting an effect-site concentration (Ce) of 30–80 ng/mL. Fentanyl was administered in 50-µg boluses.
During the second stage (sensory stimulation test), supplementary sedation with midazolam or propofol boluses was titrated to achieve an RSS score of 3, ensuring the patient remained cooperative and responsive to verbal commands. Additional analgesics were administered as needed to maintain adequate pain control. Throughout the procedure, respiratory rate, chest excursion, and oxygen saturation were continuously monitored. Airway patency was maintained via jaw thrust maneuvers when necessary.
In the third stage (RF rhizotomy), prior to the onset of ablation, sedation was deepened to an RSS score of 6 (unresponsive to stimuli) using additional sedative boluses. Atropine was administered if significant bradycardia (< 45 bpm) occurred.
Data Collection and Outcomes
Demographic and intraoperative data—including age, sex, anesthesia duration, heart rate and blood pressure changes, and anesthetic drug usage—were collected from electronic medical and anesthesia records. The values of heart rate were recorded every five minutes automatically by the anesthesia monitoring system or manually by nurses. The patients were divided into two groups, which were the Dexmedetomidine (Dex) group and the Non-Dexmedetomidine (Non-Dex) group depending on the administration of dexmedetomidine or not (Figure 1).
 |
Figure 1 Study Flow Chart. A total of 519 patients were initially screened, and after applying exclusion criteria, 517 patients were included in the final analysis. Patients were stratified into two groups based on dexmedetomidine administration: the Dex group (n = 331) and the Non-Dex group (n = 186). The primary outcome was intraoperative bradycardia, defined as heart rate <60 bpm or the administration of atropine during the procedure. |
The primary outcome of this study was the occurrence of intraoperative bradycardia, defined as a heart rate of < 60 bpm or the administration of atropine during the procedure (Figure 1). This endpoint was selected to evaluate the hemodynamic impact of sedative agents during RF rhizotomy under sedation.
The secondary outcomes included the incidence of atropine administration, intraoperative heart rate distribution, and anesthetic drug requirements (propofol, midazolam, alfentanil, and morphine milligram equivalents). These parameters were analyzed to further characterize the anesthetic and hemodynamic profiles associated with dexmedetomidine use.
Statistical Analyses
Continuous variables were assessed for normality using the Kolmogorov–Smirnov test and expressed as median with interquartile range (IQR). Normally distributed data were analyzed using the independent t-test, while non-normally distributed data were compared using the Mann–Whitney U-test. Categorical variables were presented as counts and percentages and analyzed using the chi-square test or Fisher’s exact test, as appropriate.
The primary outcome, bradycardia, was defined as either a heart rate below 60 bpm or the administration of atropine for hemodynamic support. Univariate logistic regression analyses were initially performed to identify potential predictors of bradycardia. Variables demonstrating statistical significance (p < 0.05) or clinical relevance in the univariate analysis were subsequently entered into a multivariable logistic regression model.
To explore the interaction between age and dexmedetomidine on hemodynamic responses, subgroup analyses were performed by stratifying patients into age groups (< 45 years vs ≥ 45 years). The distribution of intraoperative heart rates across age and treatment subgroups was visualized using violin plots, which display both the probability density and individual data points. Additionally, the relationship between age as a continuous variable and heart rate categories was examined using the Mann–Whitney U-test. All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). All tests were two-tailed, and a p-value < 0.05 was considered statistically significant. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported for logistic regression analyses.
Results
Study Population
A total of 519 patients who underwent RF rhizotomy for trigeminal neuralgia under sedation were initially screened for eligibility (Figure 1). One 89-year-old female patient was excluded due to missing body weight data, and another patient was excluded because of equipment malfunction. After applying these exclusion criteria, 517 patients were included in the final analysis. In this retrospective cohort of 517 patients undergoing trigeminal neuralgia procedures, 64.0% (n = 331) received dexmedetomidine.
Demographic Characteristics and Baseline Data
Demographic analysis (Table 1) showed a significant difference in gender distribution (p = 0.021), with 68.3% females in the non-Dex group versus 58.0% in the Dex group. The median age (66.0 years [59.0–75.3] in non-Dex group vs 65.0 years [56.0–73.0] in Dex group, p = 0.187) and median body weight (60.0 kg [52.0–70.0] vs 61.0 kg [53.0–70.0], p = 0.660) did not differ significantly between groups. The prevalence of hypertension (28.5% vs 28.7%, p = 0.960) and diabetes mellitus (9.1% vs 7.3%, p = 0.446) was comparable between groups. Preoperative VAS pain scores (median 8.0 [7.0–8.0] for both groups, p = 0.864) and postoperative VAS scores (median 0.0 [0.0–2.0] for both groups, p = 0.296) were comparable (Table 2). The presence of abnormal preoperative ECG was similar between groups (12.4% vs 11.8%, p = 0.845). Labetalol use was rare and comparable between groups (1.1% vs 0.6%, p = 0.621).
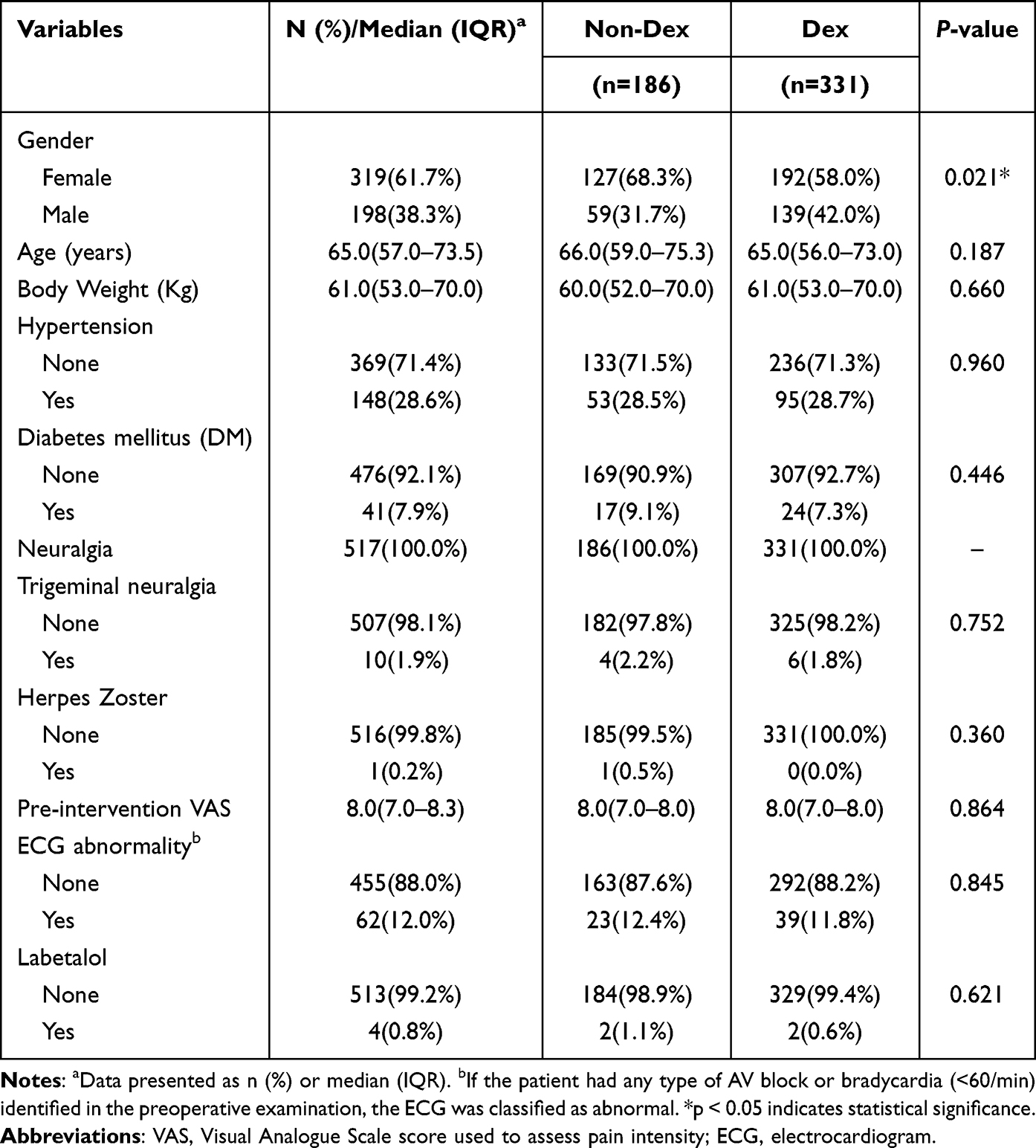 |
Table 1 Demographic Characteristics of the Study Population Comparing Patients Who Received Dexmedetomidine (Dex Group, n = 331) versus Those Who Did Not (Non-Dex Group, n = 186) |
 |
Table 2 Effects of Dexmedetomidine on Intraoperative Hemodynamics and Sedative Requirements |
Hemodynamic Changes and Anesthesia-Related Factors
The values of heart rate were recorded automatically every five minutes by the anesthesia monitoring system. The sudden severe bradycardia would be rescued with atropine immediately, and thus the actual value of these heart rates may not be captured in time by monitors or not be recorded by nurses exactly. These missing data of the exact lowest heart rate were considered when interpreting the relationship between bradycardia and atropine use.
The incidence of intraoperative bradycardia (heart rate < 60 bpm) was significantly higher in the Dex group (59.8%, n = 198) compared to the non-Dex group (29.0%, n = 54; p < 0.001) (Figure 1). Notably, 18.1% of patients in the Dex group required atropine for bradycardia rescue, while only 4.8% did in the non-Dex group (p < 0.001) (Table 2).
Patients receiving dexmedetomidine required significantly lower doses of midazolam (0.038 [0.000–0.058] vs 0.044 [0.030–0.063] mg/kg/h; p < 0.001) and propofol (0.73 [0.32–1.19] vs 1.25 [0.81–1.73] mg/kg/h; p < 0.001). The median morphine milligram equivalent (MME) was not significantly different between groups (0.27 [0.19–0.35] vs 0.25 [0.19–0.35] mg/kg/h, p = 0.363). The median anesthesia duration was significantly longer in the Dex group (44 minutes [36–50] vs 40 minutes [35–47.3], p = 0.011).
Univariate and Multivariable Analysis of Factors Influencing Bradycardia
Table 3 revealed the risk factors associated with intraoperative bradycardia. The increased risk of bradycardia was associated with male gender (OR 1.67; 95% CI, 1.17–2.38; p = 0.005), higher body weight (OR 1.02; 95% CI, 1.01–1.04; p = 0.003), Dexmedetomidine use (OR 3.64; 95% CI, 2.48–5.35; p < 0.001), and longer anesthesia time (OR 1.04; 95% CI, 1.03–1.06; p < 0.001). Conversely, the reduced risk of bradycardia was associated with older age (OR 0.97; 95% CI, 0.96–0.99; p < 0.001), higher propofol dosage (OR 0.55; 95% CI, 0.42–0.71; p < 0.001), and alfentanil use (OR 0.50; 95% CI, 0.35–0.71; p < 0.001).
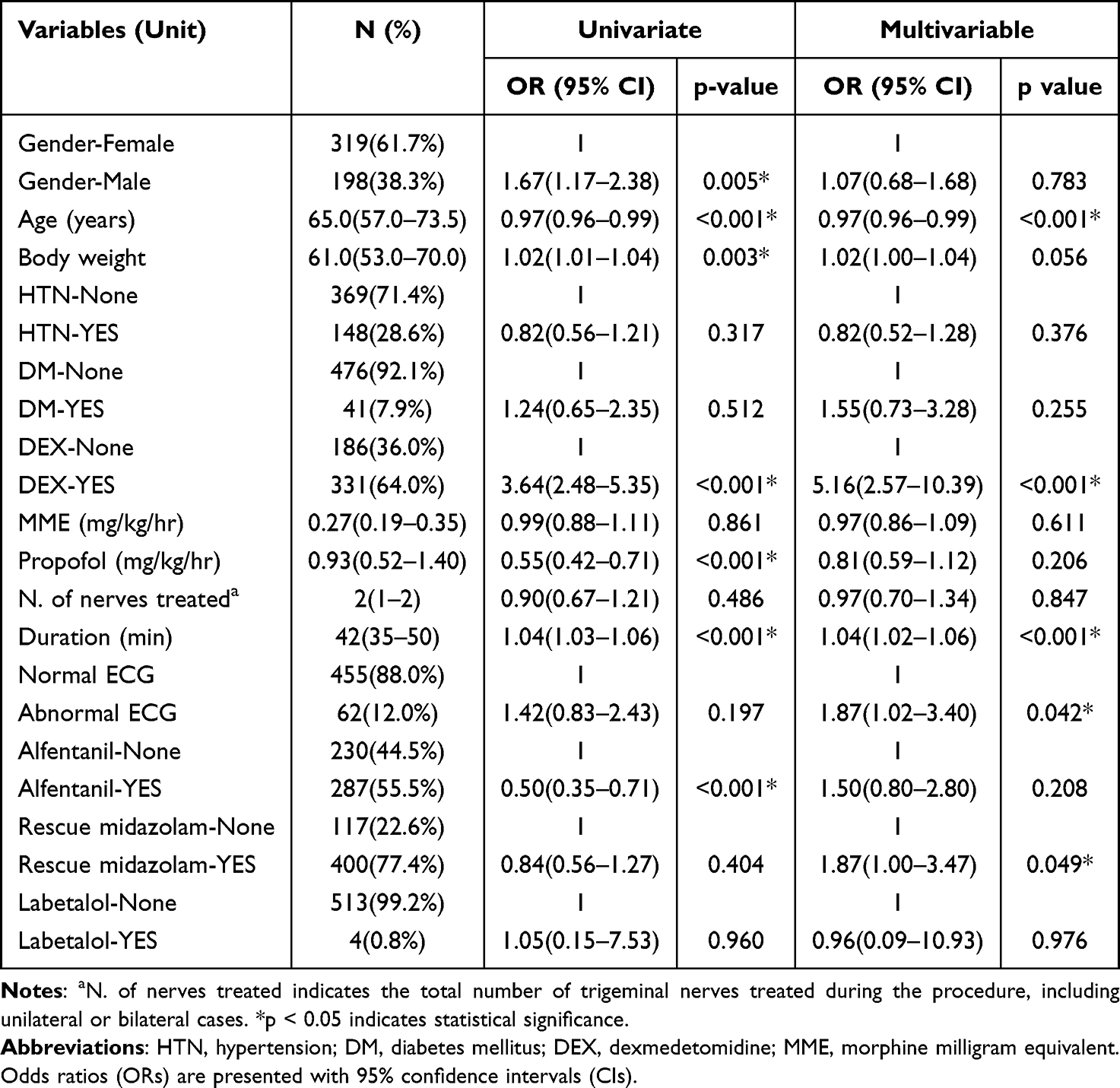 |
Table 3 Univariate and Multivariable Logistic Regression Analyses of Factors Associated with Intraoperative Bradycardia |
Multivariable logistic regression identified dexmedetomidine use as the strongest independent predictor of bradycardia (OR 5.16; 95% CI, 2.57–10.39; p < 0.001). In addition, longer anesthesia duration (OR 1.04; 95% CI, 1.02–1.06; p < 0.001), and younger age were also independently associated with the occurrence of bradycardia. Gender (p = 0.783), body weight (p = 0.056), hypertension (p = 0.376), diabetes (p = 0.255), MME (p = 0.611), propofol dosage (p = 0.206), number of treatments (p = 0.847), alfentanil use (p = 0.208), and labetalol use (p = 0.976) were not independently associated with bradycardia risk.
Association Between Age and Hemodynamic Effects of Dexmedetomidine During RF Rhizotomy
The Mann–Whitney U-test (Table 4) revealed significantly higher mean age in patients with intraoperative heart rate ≥ 60 bpm compared to those < 60 bpm (67.2±12.1 vs 62.3±14.2 years, p < 0.001). Violin plots (Figure 2) were generated to illustrate the distribution of intraoperative heart rate in these two groups, stratified by age (< 45 years and ≥ 45 years). In patients younger than 45 years, the Dex group demonstrated a wider and more inferiorly shifted heart rate distribution compared with the non-Dex group. The density of values in the Dex group extended more prominently into the lower heart rate range, whereas the non-Dex group showed a narrower distribution with a higher central tendency.
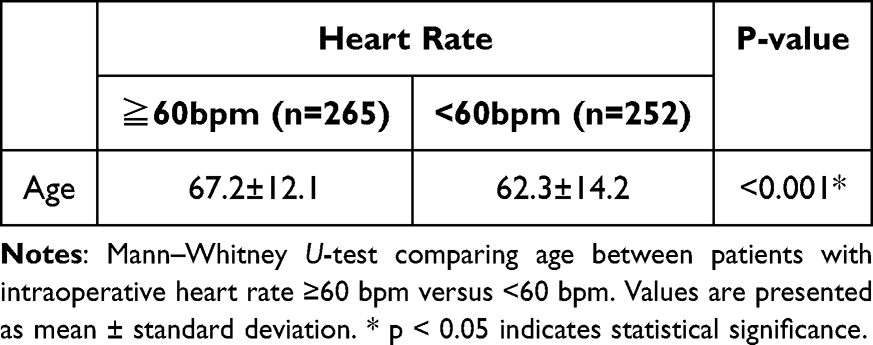 |
Table 4 The Association of Age and Intraoperative Heart Rate |
 |
Figure 2 Violin plot illustrating the distribution of intraoperative heart rates by dexmedetomidine use and age group. The plots display the probability density and individual data points for heart rate distribution. In patients younger than 45 years, the Dex group demonstrated a wider and more inferiorly shifted heart rate distribution compared with the Non-Dex group, with a more pronounced density in the lower heart rate range. In patients aged 45 years and older, both groups exhibited more compact distributions, although the Dex group still showed a lower overall heart rate distribution. |
In patients aged 45 years and older, both groups exhibited more compact distributions relative to the younger cohort. The Dex group still showed a lower overall heart rate distribution compared with the non-Dex group, though the degree of separation between groups was less pronounced than in patients younger than 45 years.
Discussion
Bradycardia resulting from the trigemino-cardiac reflex (TCR) is an important consideration during radiofrequency (RF) rhizotomy. This response is typically triggered by stimulation of the trigeminal nerve or its branches, leading to abrupt hemodynamic changes including bradycardia, hypotension, or even asystole.
In a study of 40 patients, 25% experienced sudden decreases in heart rate: 15% during foramen ovale puncture, 5% during electrical stimulation, and 5% during the heating phase.4 A separate study involving 48 patients reported a 12.5% incidence of bradycardia during foramen ovale puncture, accompanied by concurrent elevations in blood pressure and heart rate.5
In this retrospective cohort study of 517 patients undergoing RF rhizotomy, we investigated the key factors associated with significant bradycardia, particularly under deep sedation. Despite extensive research on the procedural aspects of trigeminal interventions, the impact of anesthesia-related factors—particularly sedative medication selection—has not been comprehensively explored. Our study addresses this knowledge gap by examining how different sedative and analgesic agents influence hemodynamic stability during these procedures.
The use of dexmedetomidine was associated with a significant reduction in the dosage of midazolam or propofol. Patients who received dexmedetomidine required markedly lower doses of midazolam (median 0.038 [0.000–0.058] vs 0.044 [0.030–0.063] mg/kg/h, p < 0.001) to achieve the adequate hypnotic depth, and the dosage of propofol was significantly lower compared to the non-Dex group (0.73 [0.32–1.19] vs 1.25 [0.81–1.73] mg/kg/h; p < 0.001). This hypnotic-sparing effect of dexmedetomidine may be particularly valuable in elderly patients or those with comorbidities who are at higher risk for adverse events related to propofol and midazolam. Dexmedetomidine emerged as a significant factor in our analysis, with administration associated with a fivefold increase in the risk of intraoperative bradycardia. However, this medication also demonstrated substantial clinical benefits.
While our univariate analysis showed alfentanil was associated with reduced bradycardia risk (OR 0.50, 95% CI: 0.35–0.71, p < 0.001), this association was not maintained in the multivariable model (OR 1.50, 95% CI: 0.80–2.80, p = 0.208), suggesting complex interactions between dexmedetomidine, opioids, and hemodynamic regulation.
In the univariate analysis, higher propofol dosage appeared to be associated with a reduced risk of bradycardia (OR 0.55; 95% CI, 0.42–0.71; p < 0.001). However, this association was attenuated and no longer statistically significant in the multivariable model (OR 0.81; 95% CI, 0.59–1.12; p = 0.206). This finding likely reflects a confounding relationship between propofol and dexmedetomidine use rather than a true protective effect. Specifically, patients receiving dexmedetomidine required significantly lower doses of propofol as part of the sedative-sparing interaction. Therefore, the inverse association between propofol dosage and bradycardia observed in the univariate analysis is best interpreted as a surrogate marker for the absence of dexmedetomidine rather than an independent hemodynamic benefit of propofol.
The synergistic mechanism underlying our findings can be understood as a dual-pathway convergence on vagal output. The TCR, mediated via afferent trigeminal signals to the brainstem vagal nucleus, produces parasympathetic-driven bradycardia. Dexmedetomidine, through α2-adrenergic–mediated inhibition of sympathetic outflow from the locus coeruleus, diminishes the compensatory sympathetic response that would normally counterbalance vagal surges. The net effect is an amplified and potentially sustained bradycardic response during trigeminal nerve manipulation. It should be noted that the hemodynamic effects of dexmedetomidine are highly dependent on the administration rate, and the loading dose phase may contribute disproportionately to the observed bradycardic events.
The patient age may act as a modifying factor influencing the cardiac response to dexmedetomidine. While both Dex subgroups showed a substantial reduction in heart rate, the characteristics of the low-end distribution differed in the violin plot. Specifically, the Dex subgroup in the younger cohort (< 45 years) exhibited extreme bradycardia, with the heart rate distribution extending towards 0 bpm and displaying a very high density in the severely bradycardic range. This profound lower tail may imply a more dramatic heart rate reduction or greater inter-individual variability in response to dexmedetomidine among younger patients. In contrast, although the older Dex subgroup (≥ 45 years) also had a low median heart rate (approximately 56 bpm), the violin plot shape in the bradycardic range appeared more centrally concentrated, suggesting that while heart rate reduction occurred, the incidence of the most extreme low heart rates may have been comparatively less variable. These visual distinctions indicate that the severity or the specific pattern of dexmedetomidine-induced bradycardia could be age-dependent.
The results indicated that age may play a role in hemodynamic responses during trigeminal procedures. Younger patients were more prone to developing transient bradycardia during RF rhizotomy, as shown in our results and consistent with previous research.20 Conversely, elderly patients undergoing percutaneous balloon compression (PBC) for trigeminal neuralgia are at a higher risk of severe TCR due to decreased physiological reserve and comorbidities.21 This age-dependent susceptibility highlights the need for individualized anesthetic approaches based on patient demographics and treatment strategies, eg. RFA or PBC.
These findings highlight the importance of careful monitoring and potential prophylactic measures when administering dexmedetomidine, especially in younger patients undergoing procedures with potential for TCR activation. Our study suggests that age-adjusted dosing protocols may be necessary to optimize safety while maintaining the beneficial sedative-sparing effects of dexmedetomidine, particularly in procedures involving the trigeminal nerve where TCR may compound bradycardic effects. Identifying these patient-specific and anesthesia-related factors that contribute to hemodynamic events is essential for optimizing perioperative care and reducing the risk of complications during trigeminal neuralgia procedures.
The sedative-sparing benefits of dexmedetomidine—including significant reductions in propofol and midazolam requirements—must be carefully weighed against the increased risk of clinically significant bradycardia, particularly in younger patients who demonstrate the most pronounced hemodynamic effects. These findings support several practical considerations: dose titration strategies that favor lower loading doses in younger patients, enhanced hemodynamic monitoring with continuous heart rate trending during the TCR-prone phases of the procedure, and ensuring the immediate availability of atropine or glycopyrrolate. However, given the retrospective nature of this study, these recommendations should be regarded as hypothesis-generating rather than prescriptive.
Several limitations of this study merit acknowledgment. The non-randomized assignment of dexmedetomidine, based on the attending anesthesiologist’s discretion, introduces the possibility of confounding by indication. Although multivariable adjustment was performed to mitigate this bias, residual confounding from unmeasured variables cannot be fully excluded. Our composite definition of bradycardia—encompassing both heart rate < 60 bpm and atropine administration—combines an objective physiological measurement with a clinical treatment decision that may vary among individual anesthesiologists. This approach, while clinically pragmatic and inclusive, may introduce some heterogeneity in outcome classification. Additionally, transient severe bradycardic episodes occurring between automated 5-minute recording intervals may not have been captured, potentially leading to underestimation of bradycardia severity. This measurement limitation is inherent to retrospective analysis of routine anesthesia monitoring data. As a single-center study, the internal consistency of anesthetic protocols and surgical technique (performed by a single surgeon) enhances the internal validity of our findings. However, the generalizability of these results to centers with different anesthesia practices, patient populations, or procedural protocols may be limited, and multicenter validation is warranted.
Abbreviations
RF, radiofrequency; RFA, radiofrequency ablation; TN, trigeminal neuralgia; TCR, trigeminal-cardiac reflex; DEX, dexmedetomidine; CT, computed tomography; RSS, Ramsay Sedation Scale; TCI, Target-Controlled Infusion; Ce, effect-site concentration; bpm, beats per minute; CI, confidence interval; ECG, electrocardiogram; HR, heart rate; IQR, interquartile range; OR, odds ratio.
Data Sharing Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Wu H, Zhou J, Chen J, et al. Therapeutic efficacy and safety of radiofrequency ablation for the treatment of trigeminal neuralgia: a systematic review and meta-analysis. J Pain Res. 2019;12:423–11. doi:10.2147/JPR.S176960
2. Mansano AM, Frederico TN, Valentin REB, et al. Percutaneous radiofrequency ablation for trigeminal neuralgia management: a randomized, double-blinded, sham-controlled clinical trial. Pain Med. 2023;24(3):234–243. doi:10.1093/pm/pnac132
3. Gunduz HB, Cevik OM, Asilturk M, et al. Percutaneous radiofrequency thermocoagulation in trigeminal neuralgia: analysis of early and late outcomes of 156 cases and 209 interventions. J Korean Neurosurg Soc. 2021;64(5):827–836. doi:10.3340/jkns.2020.0333
4. Lee JY, Park JH, Hong JH. Analysis of the hemodynamic response during radiofrequency thermocoagulation in trigeminal neuralgia. Pain Physician. 2022;25(7):E1057–E1062.
5. Meng Q, Zhang W, Yang Y, et al. Cardiovascular responses during percutaneous radiofrequency thermocoagulation therapy in primary trigeminal neuralgia. J Neurosurg Anesthesiol. 2008;20(2):131–135. doi:10.1097/ANA.0b013e3181628305
6. Blaudszun G, Lysakowski C, Elia N, et al. Effect of perioperative systemic alpha2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Anesthesiology. 2012;116(6):1312–1322. doi:10.1097/ALN.0b013e31825681cb
7. Ju JY, Kim KM, Lee S. Effect of preoperative administration of systemic alpha-2 agonists on postoperative pain: a systematic review and meta-analysis. Anesth Pain Med. 2020;15(2):157–166. doi:10.17085/apm.2020.15.2.157
8. Yuan D, Liu Z, Kaindl J, et al. Activation of the alpha(2B) adrenoceptor by the sedative sympatholytic dexmedetomidine. Nat Chem Biol. 2020;16(5):507–512. doi:10.1038/s41589-020-0492-2
9. Zhao Y, He J, Yu N, et al. Mechanisms of dexmedetomidine in neuropathic pain. Front Neurosci. 2020;14:330. doi:10.3389/fnins.2020.00330
10. Chabot-Doré AJ, Schuster DJ, Stone LS, et al. Analgesic synergy between opioid and alpha2-adrenoceptors. Br J Pharmacol. 2015;172(2):388–402. doi:10.1111/bph.12695
11. Weerink MAS, Struys MMRF, Hannivoort LN, et al. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
12. Zhang K, Ren Y-Q, Xue Y, et al. Alpha 2-adrenoceptor participates in anti-hyperalgesia by regulating metabolic demand. Front Pharmacol. 2024;15:1359319. doi:10.3389/fphar.2024.1359319
13. Kim M, Huh J, Choi H, et al. Impact of dexmedetomidine-based opioid-sparing anesthesia on opioid use after minimally invasive repair of pectus excavatum: a prospective randomized controlled trial. J Clin Med. 2024;13(23):7264. doi:10.3390/jcm13237264
14. Naik BI, Nemergut EC, Kazemi A, et al. The effect of dexmedetomidine on postoperative opioid consumption and pain after major spine surgery. Anesth Analg. 2016;122(5):1646–1653. doi:10.1213/ANE.0000000000001226
15. Gandhi KA, Panda NB, Vellaichamy A, et al. Intraoperative and postoperative administration of dexmedetomidine reduces anesthetic and postoperative analgesic requirements in patients undergoing cervical spine surgeries. J Neurosurg Anesthesiol. 2017;29(3):258–263. doi:10.1097/ANA.0000000000000301
16. Seppänen SM, Kuuskoski R, Mäkelä KT, et al. Intranasal dexmedetomidine reduces postoperative opioid requirement in patients undergoing total knee arthroplasty under general anesthesia. J Arthroplasty. 2021;36(3):978–985.e1. doi:10.1016/j.arth.2020.09.032
17. Peng K, Liu H-Y, Wu S-R, et al. Effects of combining dexmedetomidine and opioids for postoperative intravenous patient-controlled analgesia: a systematic review and meta-analysis. Clin J Pain. 2015;31(12):1097–1104. doi:10.1097/AJP.0000000000000219
18. Farag E, Yared M. Invited commentary: role of alpha-2 agonists for postoperative pain relief. Proc Bayl Univ Med Cent. 2014;27(1):11. doi:10.1080/08998280.2014.11929036
19. Yu DH, Shen X, Lai L, et al. Application of dexmedetomidine as an opioid substitute in opioid-free anesthesia: a systematic review and meta-analysis. Pain Physician. 2023;26(6):E635–E649. doi:10.36076/ppj.2023.26.E635
20. Wakita R, BaBa Y, Fukayama H, et al. Factors associated with transient bradycardia during local anesthesia administration to the oral cavity under intravenous sedation: a retrospective cohort study. J Dent Sci. 2024;19(2):878–884. doi:10.1016/j.jds.2023.08.017
21. Zhang H, Liu M, Guo W, et al. The effect of trigeminal ganglion block on trigeminocardiac reflex in elderly patients with trigeminal neuralgia undergoing percutaneous balloon compression: a randomized controlled study. Ther Clin Risk Manag. 2022;18:1091–1098. doi:10.2147/TCRM.S373370
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.