Back to Journals » Drug Design, Development and Therapy » Volume 20
Dexamethasone Alone versus Combined with Droperidol for Preventing Postoperative Nausea and Vomiting in Gynecological Day Surgery Under Ciprofol-Alfentanil Anesthesia: A Randomized Double-Blind Controlled Trial
Authors Sun X ![]() , Xiao H
, Xiao H ![]() , Li M, Yin B, Yu S, Ji F
, Li M, Yin B, Yu S, Ji F ![]() , Shan J
, Shan J
Received 19 May 2026
Accepted for publication 1 July 2026
Published 14 July 2026 Volume 2026:20 625824
DOI https://doi.org/10.2147/DDDT.S625824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiaohan Sun,1 Hongyi Xiao,2 Mengge Li,1 Bingzhe Yin,1 Shiyu Yu,1 Fanceng Ji,2,* Jinghua Shan3,*
1School of Anesthesiology, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 2Department of Anesthesiology, Weifang People’s Hospital, Weifang, Shandong, People’s Republic of China; 3Department of Anesthesiology, The Affiliated Hospital of Shandong Second Medical University, Weifang, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanceng Ji, Department of Anesthesiology, Weifang People’s Hospital, Weifang, Shandong, 261041, People’s Republic of China, Email [email protected] Jinghua Shan, Department of Anesthesiology, The Affiliated Hospital of Shandong Second Medical University, Weifang, Shandong, 261031, People’s Republic of China, Email [email protected]
Purpose: To compare the efficacy and safety of dexamethasone alone versus dexamethasone combined with droperidol for the prevention of postoperative nausea and vomiting (PONV) in patients undergoing gynecological day surgery under ciprofol-alfentanil general anesthesia.
Patients and Methods: A total of 268 patients scheduled for gynecological day surgery were randomly assigned to the DD group (dexamethasone–droperidol, n=134) or the DN group (dexamethasone–normal saline, n=134). Before induction of anesthesia, the DD group received 5 mg dexamethasone plus 1 mg droperidol, while the DN group received 5 mg dexamethasone plus normal saline. Anesthesia induction: ciprofol 0.5 mg/kg, alfentanil 20 μg/(kg·h), and mivacurium 0.2 mg/kg. Anesthesia maintenance: ciprofol 1.25 mg/(kg·h), alfentanil 40 μg/(kg·h), with bispectral index (BIS) maintained at 40– 60. The primary outcome was the incidence of PONV within 24 h postoperatively. Secondary outcomes included the incidence of adverse events within 24 h postoperatively, patient satisfaction, hemodynamic changes during anesthesia, BIS changes during anesthesia, and the incidence of intraoperative adverse events.
Results: The incidence of PONV within 24 h postoperatively was significantly lower in the DD group than in the DN group (17.2% vs 31.9%), with a statistically significant difference. No significant differences were found between the two groups in the incidence of postoperative adverse events within 24 h, patient satisfaction, hemodynamic changes during anesthesia, BIS changes during anesthesia, or the incidence of intraoperative adverse events. No specific adverse effects of droperidol were observed in the DD group.
Conclusion: For patients undergoing gynecological day surgery under ciprofol-alfentanil general anesthesia, the combination of dexamethasone and droperidol is significantly more effective than dexamethasone alone in preventing PONV, with no significant difference in safety between the two regimens.
Keywords: glucocorticoids, butyrophenones, ambulatory surgery, emesis
Introduction
Postoperative nausea and vomiting (PONV) is one of the most common complications after general anesthesia, particularly in patients undergoing gynecological day surgery.1 According to a review on PONV prevention and treatment, the incidence of PONV in high-risk patients who do not receive prophylactic antiemetics can be as high as 80%.2 This not only causes patient discomfort but also prolongs the length of stay in the post-anesthesia care unit and the day surgery ward, contradicting the patient-centered, enhanced recovery goal of day surgery.3 In recent years, ciprofol, as a novel intravenous anesthetic, has been gradually applied in ambulatory surgery anesthesia due to its advantages of rapid onset and quick recovery,4 and it is often combined with short-acting opioids such as alfentanil to enhance analgesic efficacy. However, guidelines indicate that both female sex and opioid use are well-established risk factors for PONV.5 Therefore, implementing effective prophylactic strategies is of paramount importance for improving the quality of gynecological day surgery. Dexamethasone, a glucocorticoid, and droperidol, a dopamine receptor antagonist, are both strongly recommended by guidelines for PONV prophylaxis.6 Their mechanisms of action differ: dexamethasone exerts its effects indirectly through anti-inflammatory and multi-target modulation,7 whereas droperidol acts rapidly by directly blocking the vomiting center in the brain.8 Previous studies have demonstrated a synergistic effect of their combination in certain surgeries;9 however, whether this regimen can further reduce the incidence of PONV in gynecological day surgery under ciprofol-alfentanil anesthesia remains to be specifically investigated. For this purpose, A 24-hour postoperative observation window was chosen as the primary endpoint because the majority of PONV episodes occur within the first 24 hours following surgery, and this timeframe is the most commonly used endpoint in the literature, enabling direct comparison with previous studies.6 Furthermore, droperidol has potential side effects such as sedation, QTc prolongation, and extrapyramidal symptoms;10 therefore, its benefit-risk ratio when used in combination in day surgery requires further evaluation.
Materials and Methods
Ethics and Registration
This study was approved by the Medical Ethics Committee of the Weifang People’s Hospital (approval number: KYLL20260214-5). Registered in the Chinese Clinical Trial Registry (www.chictr.org.cn;registration number: ChiCTR2600119674), the study was conducted at Weifang People’s Hospital and all enrolled patients provided signed informed consent.
Patients
In this study, 268 patients scheduled for gynecological day surgery at Weifang People’s Hospital from March 2026 to May 2026 were enrolled. Inclusion criteria: signed informed consent; elective gynecological day surgery; American Society of Anesthesiologists (ASA) grade I–II; BMI 18.5–27.9 kg/m2; age 18–65 years. Exclusion criteria: known or suspected allergy to dexamethasone, droperidol, or any of their components; known long QT syndrome; clinically significant history of arrhythmias; severe electrolyte disturbances; Parkinson’s disease, epilepsy, or history of antipsychotic-induced extrapyramidal symptoms; use of any antiemetics or corticosteroids within 24 hours before surgery; long-term regular use of opioids; chronic medical conditions predisposing to nausea and vomiting, such as gastroesophageal reflux disease or motion sickness; pregnancy or breastfeeding; severe hepatic or renal insufficiency; history of alcohol or drug abuse; presence of mental disorders, cognitive impairment, or communication barriers.
Randomization and Masking
Only the researcher involved in randomization used a random number table to allocate patients in a 1:1 ratio to either the DD group or the DN group, with 134 patients in each group. The randomization results were sealed in sequentially numbered envelopes. Study drugs were prepared by personnel not involved in data collection according to the group assignment in the envelopes. Dexamethasone, droperidol, and normal saline were all clear liquids; therefore, the patients, anesthesiologists, and researchers responsible for postoperative follow-up and data processing were all blinded to the group allocation.
Anesthesia
Preoperatively, all patients fasted for 6 hours and abstained from liquids for 2 hours. After entering the operating room, a peripheral intravenous line was established, and non-invasive blood pressure (NIBP), pulse oximetry (SpO2), electrocardiogram (ECG), and bispectral index (BIS) were monitored. All patients received oxygen at 6 L/min via a face mask. Before induction of anesthesia, flurbiprofen axetil 50 mg was administered. The DD group received 5 mg dexamethasone and 1 mg droperidol, while the DN group received 5 mg dexamethasone and placebo (normal saline). Anesthesia induction regimen: ciprofol 0.5 mg/kg was administered, and sedation was assessed using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale. After the patient fell asleep (MOAA/S ≤1), alfentanil 20 μg/(kg·h) and mivacurium 0.2 mg/kg were given. A laryngeal mask airway was inserted 3 minutes later. If the patient did not fall asleep within 2 minutes, an additional dose of ciprofol 0.25 mg/kg was given. If the patient remained awake after two additional doses, induction was considered a failure, and alternative drugs were used to assist induction. Anesthesia maintenance regimen: ciprofol 1.25 mg/(kg·h), alfentanil 40 μg/(kg·h), with BIS maintained between 40 and 60. Intraoperative mechanical ventilation was used with the following settings: tidal volume 6–8 mL/kg, respiratory rate 10–12 breaths/min, inspiratory-to-expiratory ratio 1:2, and end-tidal CO2 maintained at 35–45 mmHg. If intraoperative body movements interfered with the surgery, a single additional dose of ciprofol 0.25 mg/kg was administered, and repeated if necessary. If more than two additional doses were given within 10 minutes, anesthesia maintenance was considered a failure. When hypotension (MAP < 65 mmHg) occurred, norepinephrine was administered; when bradycardia (HR < 50 beats/min) occurred, atropine was given. At the end of the surgery, anesthetic maintenance drugs were discontinued. After the patient regained consciousness, the laryngeal mask airway was removed and the patient was transferred to the post‑anesthesia care unit (PACU). The patient was transferred to the general ward when the Aldrete score reached ≥ 9. Discharge was allowed after meeting the discharge criteria. Regarding the prevention and management of PONV: Given that short-acting anesthetic agents were used in this cohort, rendering the risk of PONV manageable, preoperative education was primarily based on non-pharmacological instructions (eg, advising patients to avoid vigorous activity, maintain calm breathing, and adopt a relaxed mindset), and no rescue antiemetic regimen was pre-established. Follow-up was conducted within 24 hours after discharge via a questionnaire, which mainly included the presence of postoperative pain, use of analgesics, postoperative nausea and vomiting, and satisfaction with anesthesia.
Patients’ vital signs were recorded at the following time points: after entering the operating room (T0), at the start of anesthesia induction (T1), before laryngeal mask airway insertion (T2), immediately after laryngeal mask airway insertion and fixation (T3), at the start of surgery (T4), 5 minutes after the start of surgery (T5), 10 minutes after the start of surgery (T6), 15 minutes after the start of surgery (T7), at the end of surgery when anesthetic maintenance was discontinued (T8), and 1 minute after laryngeal mask airway removal (T9).
Outcomes
Primary Outcome Measure
The primary endpoint was the incidence of PONV within 24 hours postoperatively.
PONV was defined according to the consensus guidelines as the occurrence of nausea, retching, or vomiting within the specified time period.6 Nausea and vomiting were recorded as a composite endpoint; that is, a patient was considered to have experienced PONV if either nausea or vomiting occurred at any observation time point, rather than recording them as separate endpoints individually.
Secondary Outcome Measure
Incidence of adverse events within 24 hours postoperatively, patient satisfaction, hemodynamic changes during anesthesia, changes in BIS values during anesthesia, incidence of adverse events during anesthesia.
Sample Size and Statistical Analysis
Sample size estimation was performed based on parameters derived from previous literature and preliminary pilot study results. The anticipated event rate in the control group (P1) was set at approximately 30%,11 representing the historical incidence of PONV without prophylactic intervention. The expected event rate in the experimental group (P2) was set at 14.1% according to prior research,12 yielding an absolute risk reduction (ARR) of 15.9%. A two-sided significance level (α) of 0.05 and a statistical power (1-β) of 0.80 were specified. Power analysis was performed using a two-sided Z-test for the difference between two independent proportions (Pearson’s chi-squared test analog) in GPower 3.1 software, yielding a requirement of at least 116 valid samples per group. Assuming a dropout rate of 15%, the adjusted sample size was 134 participants per group, resulting in a total of 268 study subjects. This calculation was fundamentally based on the untreated baseline PONV incidence as the reference, which adheres to the fundamental principles of clinical trial sample size estimation.
The primary analysis was conducted using a modified intention-to-treat (mITT) population, defined as all randomized patients who received at least one dose of the study intervention and had both baseline and at least one post-baseline measurement of the primary outcome. All analyses were performed according to the randomized treatment assignment. Comparison of baseline characteristics (age, ASA physical status, surgical type, and baseline PONV risk score) between excluded and included patients revealed no significant differences (all P > 0.05). The reasons for exclusion were all attributable to objective documentation omissions or non-study-related loss to follow-up, which were unrelated to the interventions or outcome occurrence. We therefore considered the missing data to be missing completely at random (MCAR). To test the robustness of our findings, we further performed sensitivity analyses using best-case and worst-case scenario imputations.
To evaluate the impact of excluding patients after randomization on the stability of our results, we performed extreme-case scenario sensitivity analyses. In the worst-case scenario, all excluded patients in the treatment group were assumed to have experienced the primary outcome (PONV), while all excluded patients in the control group were assumed not to have experienced it; the best-case scenario applied the reverse assumption. The risk ratio (RR) and 95% confidence intervals were recalculated under each scenario.
Statistical analysis was performed using SPSSAU software. The Shapiro–Wilk test was used to assess whether continuous variables followed a normal distribution. Normally distributed continuous variables were expressed as mean ± SD (standard deviation) and analyzed using the independent samples t-test. Non-normally distributed continuous variables were expressed as median (interquartile range) [M (Q1-Q3)] and analyzed using the Mann–Whitney U-test. Categorical variables were expressed as frequency (percentage) and analyzed using the Pearson chi-square test; if the expected frequency was less than 5, Fisher’s exact test was used. The treatment effect for the primary outcome will be presented as RR with its 95% CI. A P-value < 0.05 was considered statistically significant.
Results
Demographic Data and Surgical Characteristics
A total of 268 patients were enrolled in this study. Among them, the DD group included 5 patients with incomplete data and 13 patients lost to follow-up, while the DN group included 4 patients with incomplete data and 14 patients lost to follow-up. Ultimately, 232 patients (86.6%) were included in the mITT analysis: 116 in the DD group and 116 in the DN group. The exclusion rates were comparable between groups (DD: 13/134 [9.7%] vs DN: 14/134 [10.4%] for loss to follow-up; 5/134 [3.7%] vs 4/134 [3.0%] for incomplete data) (Figure 1). The final sample size was consistent with the pre-specified statistical power requirements, and there were no statistically significant differences between the groups in terms of age, height, weight, BMI, ASA, Apfel Score Assessment, type of surgery, or duration of anesthesia (Table 1).
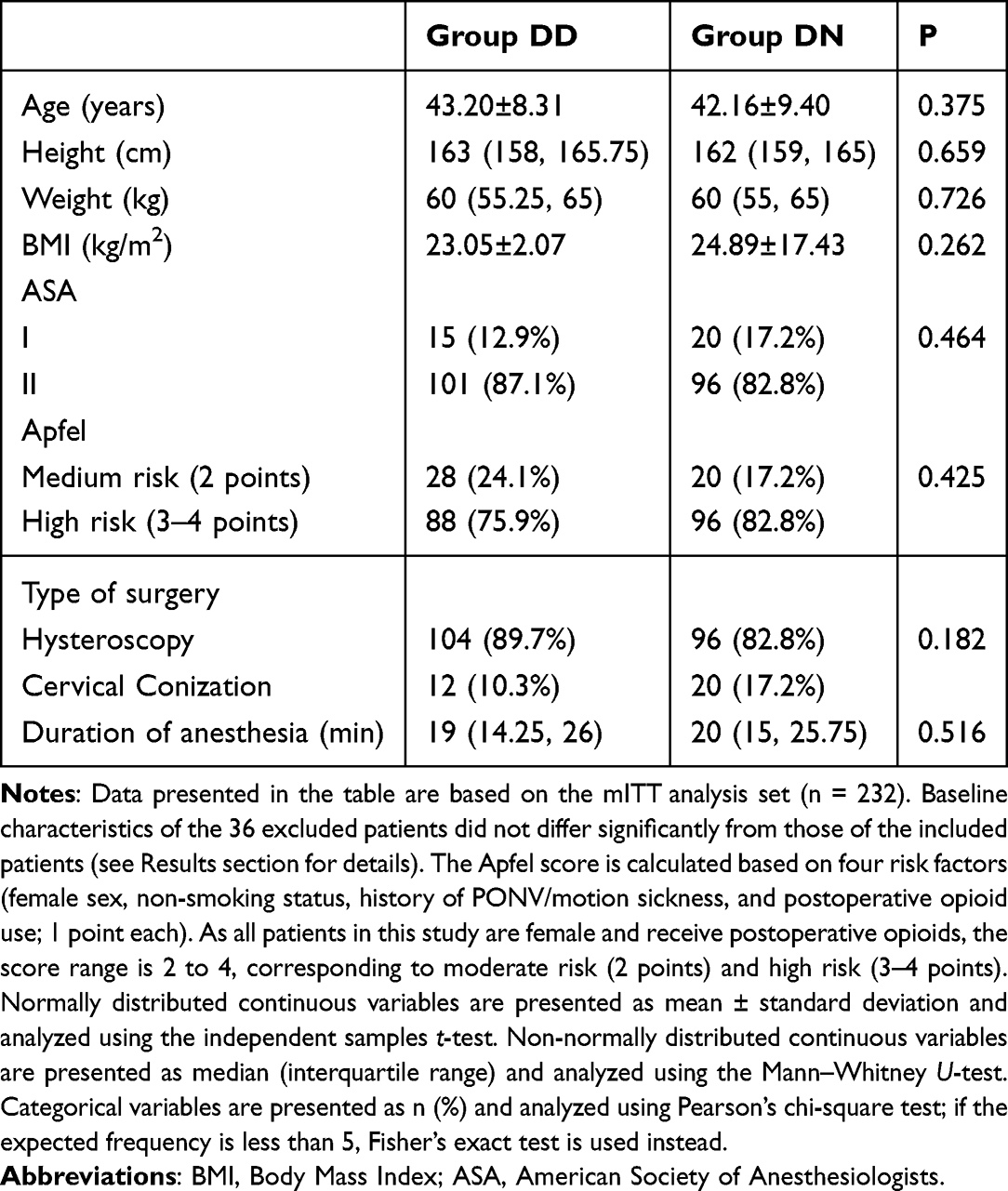 |
Table 1 Comparison of the General Situation of the Two Groups of Patients |
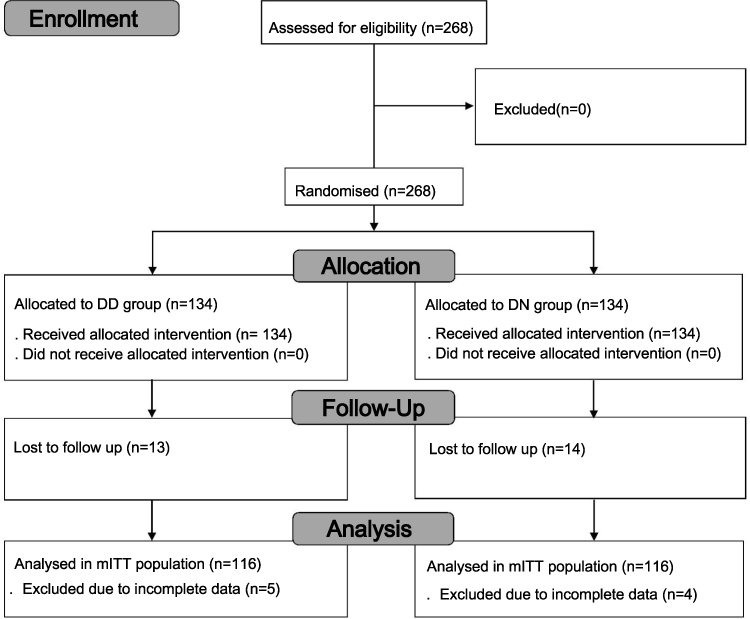 |
Figure 1 CONSORT flow diagram of patient enrollment, randomization, allocation, follow-up and analysis. Of the 268 randomized patients, 27 were lost to follow-up (13 in the treatment group, 14 in the control group) and 9 were excluded due to incomplete key data (5 and 4, respectively), leaving 232 patients (116 per group) in the mITT analysis. Abbreviation: mITT, modified intention-to-treat. |
Primary Outcome
The incidence of the primary outcome event in the experimental group was 17.2% (20/116), compared with 31.9% (37/116) in the control group. Pearson’s chi-square test revealed a statistically significant difference between the two groups (χ2 = 6.722, P = 0.010). The relative risk (RR) was 0.541 (95% CI: 0.335 to 0.873), with an absolute risk reduction (ARR) of 14.7%, corresponding to a number needed to treat (NNT) of 7 (95% CI: 4 to 21). Using the control group as the reference, the odds ratio (OR) was 0.44 (95% CI: 0.23 to 0.82).
Secondary Outcome
Regarding the incidence of adverse events during anesthesia, neither group experienced hiccups or aspiration. There were no statistically significant differences in the incidences of other adverse events between the two groups (Table 2).
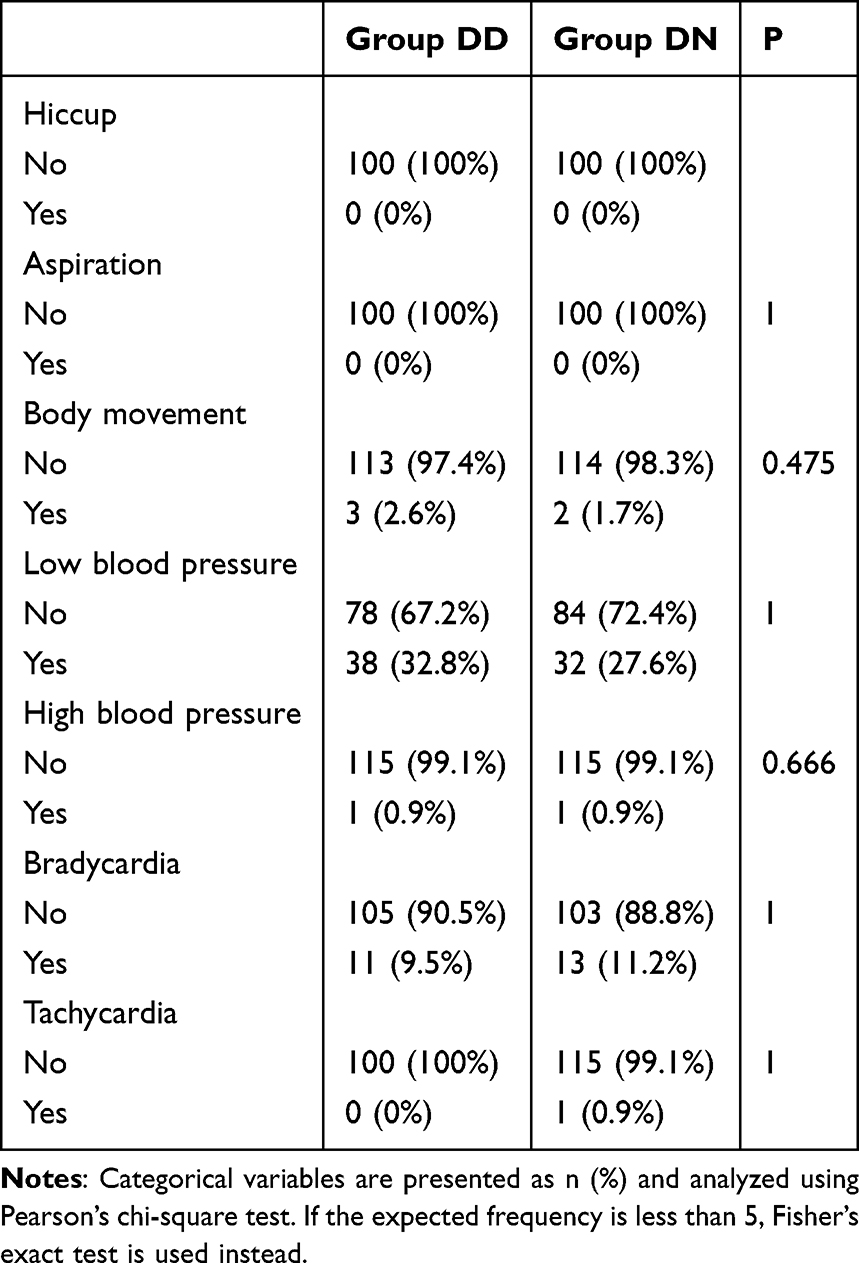 |
Table 2 Incidence of Adverse Reactions During Anesthesia |
Regarding the incidence of other postoperative adverse reactions within 24 hours, there were no statistically significant differences between the two groups. The incidences of mild, moderate, and severe PONV in the DD group were all lower than those in the DN group (Table 3). No specific adverse reactions to droperidol, such as QTc prolongation or extrapyramidal symptoms, were observed in the DD group.
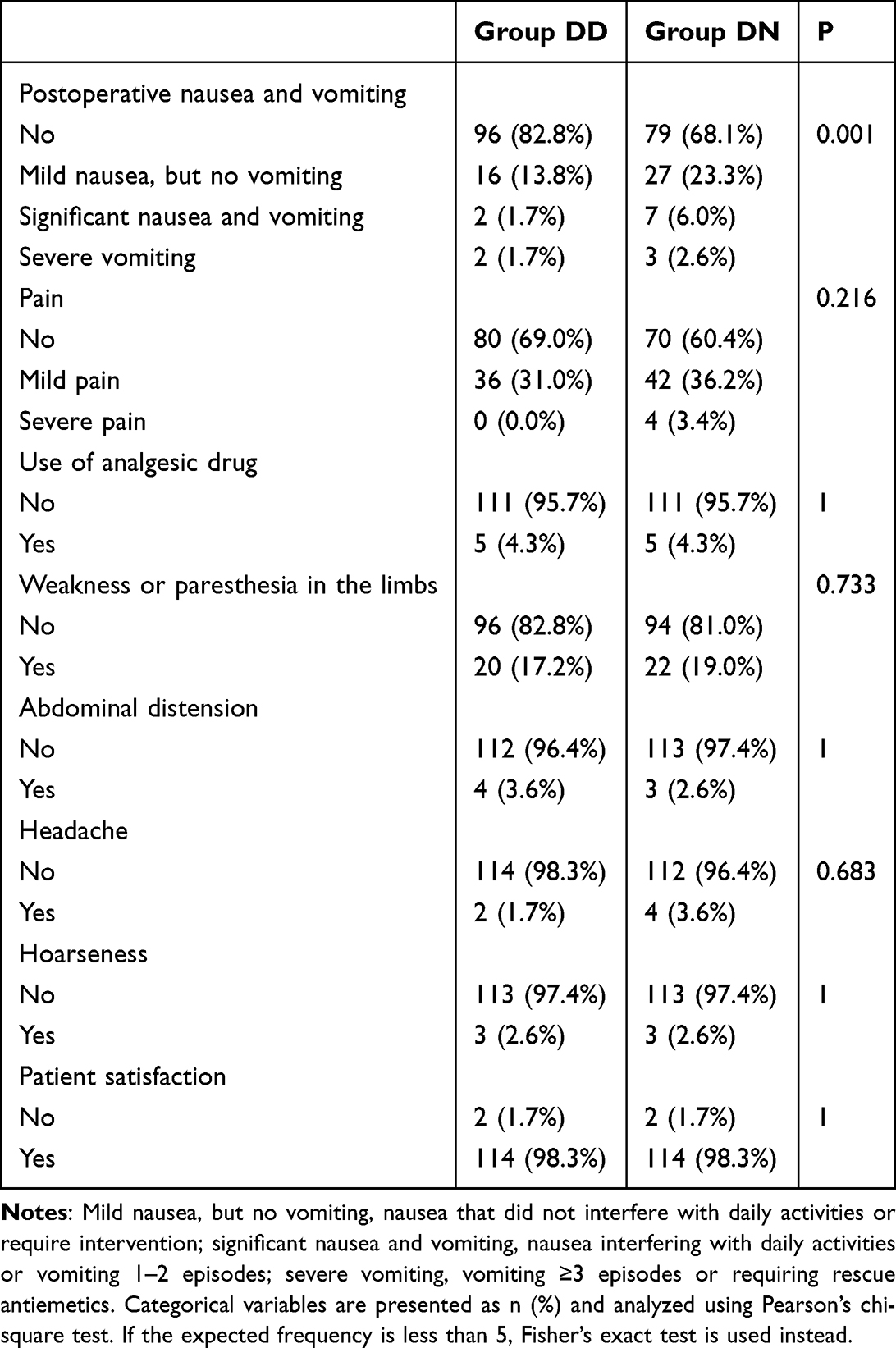 |
Table 3 Incidence of Adverse Reactions Within 24 Hours Post-Surgery and Patient Satisfaction |
In terms of patient satisfaction, there was no statistically significant difference between the two groups (Table 3).
Regarding hemodynamics, there were no statistically significant differences in baseline blood pressure and heart rate between the two groups, and the trends of intraoperative vital signs (such as blood pressure and heart rate) were similar. Heart rate in the DN group was significantly higher than that in the DD group at T2 (P < 0.05). SBP, DBP, and MAP in the DN group were significantly higher than those in the DD group at T3 (P < 0.05), and DBP and MAP in the DN group were significantly higher than those in the DD group at T6 and T9 (P < 0.05) (Figure 2).
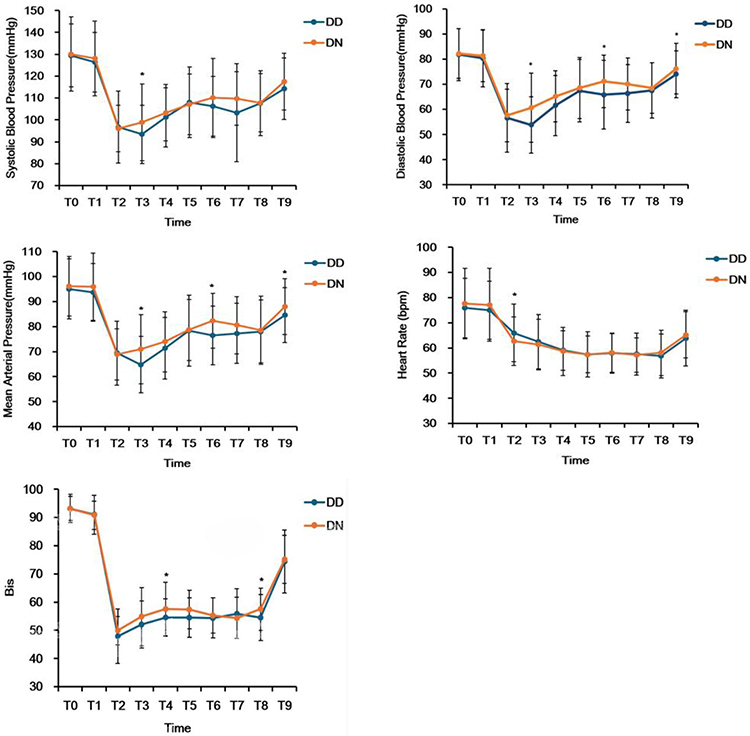 |
Figure 2 Changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), heart rate (HR), and bispectral index (BIS) at perioperative time points. Data are presented as mean ± SD. Asterisks (*) indicate statistically significant differences between groups (P < 0.05). Time points: after entering the operating room (T0), at the start of anesthesia induction (T1), before laryngeal mask airway insertion (T2), immediately after laryngeal mask airway insertion and fixation (T3), at the start of surgery (T4), 5 minutes after the start of surgery (T5), 10 minutes after the start of surgery (T6), 15 minutes after the start of surgery (T7), at the end of surgery when anesthetic maintenance was discontinued (T8), and 1 minute after laryngeal mask airway removal (T9). |
In terms of BIS values, the BIS values in the DN group were significantly higher than those in the DD group at T4 and T8 (P < 0.05) (Figure 2).
Sensitivity Analysis
Extreme-case scenario sensitivity analyses were performed to assess the robustness of the primary findings. In the worst-case scenario, the RR was 1.03 (P = 0.89), indicating that the treatment effect was attenuated to null under this extreme assumption. In the best-case scenario, the RR was 0.36 (P < 0.001), consistent with the direction of the primary analysis. While the worst-case scenario attenuated the effect to non-significance, this extreme assumption is clinically implausible in our study, as all exclusions were due to non-study-related reasons unrelated to PONV occurrence.
Discussion
Ciprofol is a short-acting GABAA receptor agonist. It is a small molecule (R)-configured isomer formed by adding a cyclopropyl group to the chemical structure of propofol.13 The introduction of the cyclopropyl group increases steric hindrance, creating an “R-type chiral structure” that enhances affinity for the GABAA receptor.14 Compared with propofol, the most prominent advantage of ciprofol is its very low incidence of injection pain (approximately 4.9%–16.7%, whereas propofol has an incidence of 28–90%),15 along with fewer adverse events such as respiratory depression16 and more stable hemodynamics.14 In terms of recovery, the anesthesia regimen combining ciprofol with remifentanil significantly shortens the time to spontaneous breathing recovery and eye opening.17
Dexamethasone exerts its antiemetic effect primarily through anti-inflammatory mechanisms. As a glucocorticoid, it inhibits prostaglandin synthesis and prevents PONV via its peripheral and central anti-inflammatory or membrane-stabilizing effects.7 Additionally, dexamethasone suppresses the release of intestinal serotonin (5-HT), reduces 5-HT levels in neural tissues, and inhibits the expression of 5-HT and 3A receptors, thereby blocking the emetic signaling.18 Droperidol, on the other hand, exerts its antiemetic effect by antagonizing dopamine receptors in the central nervous system.19 Studies have shown that droperidol inhibits spontaneous electrical activity of neurons in the ventral midbrain—which express dopamine receptors on their surface—in a dose-dependent manner, suggesting that it achieves its antiemetic effect by blocking dopamine receptors and modulating the activity of relevant neural circuits.20 When the two drugs are used in combination, dexamethasone suppresses peripheral inflammatory pathways while droperidol blocks central dopaminergic pathways, resulting in multiple levels of inhibition of the vomiting reflex and producing a synergistic effect. Clinical studies have confirmed that the prophylactic effect of droperidol combined with dexamethasone is superior to either drug alone, and the combination allows for dose reduction of each single agent to lower the risk of related complications.21
The results of this study showed that there were no significant differences between the two groups in terms of adverse events during anesthesia, vital signs, analgesic effect within 24 hours postoperatively, and adverse events other than PONV. These findings are highly consistent with the meta-analysis by Habib et al, which reported no significant difference in adverse events between antiemetic regimens combining a 5-HT3 receptor antagonist with either droperidol or dexamethasone.22 The RCT by Shi et al demonstrated that ciprofol and propofol showed no significant differences in recovery time, PACU length of stay, or the incidence of other adverse events.23 The meta-analysis by Hung et al confirmed that there were no statistically significant differences between ciprofol and propofol in terms of the risks of complications such as tachycardia, hypertension, and postoperative nausea and vomiting.24 The above studies not only confirm the safety of the combination regimen of droperidol and dexamethasone but also demonstrate the feasibility of using ciprofol in gynecological day surgery.
No increase in extrapyramidal symptoms (eg, akathisia or dystonia) or excessive sedation, and no clinically significant QT-interval prolongation, was observed in the DD group in this study, which may be related to the low dose (1 mg) of droperidol used.25 The study by Habib et al suggested that a low dose (2.5 mg) did not increase the risk of cardiac events.26 We acknowledge that standardized QTc interval measurements using 12-lead ECG were not performed as part of the study protocol. This decision was pragmatic, reflecting real-world clinical practice, where routine 12-lead ECG screening is not universally implemented for low-risk patients undergoing short-duration surgery. Nevertheless, all patients received continuous standard II-lead ECG monitoring throughout the entire intraoperative period and in the PACU. These monitoring records were reviewed in real time by the attending anesthesiologists and were retrospectively scrutinized by the study team for any clinically significant arrhythmic events. However, we fully recognize that this approach is not equivalent to a standardized perioperative QTc assessment. It is worth noting that even in the emergency department setting, where patients often present with more complex comorbidities and polypharmacy, low-dose droperidol (0.625–1.25 mg) has been shown to be generally safe, although attention should still be paid to the risk of dose-dependent QTc prolongation.10 This external evidence further supports the safety of low-dose droperidol in day surgery.
For day surgery, effective prevention of PONV is crucial because it directly affects patient discharge time and satisfaction. Gynecological surgery itself is a high-risk factor for PONV, and day surgery demands rapid recovery.27 Taken together, these findings suggest that for moderate-to-high-risk patients—particularly those who may have an inadequate response to dexamethasone alone—the addition of low-dose droperidol (1 mg) represents a safe and effective prophylactic strategy in the gynecological day-surgery setting.
The innovation of this study lies in its being the first to compare the efficacy of the combination versus the single use of these two classic antiemetics in ciprofol-based anesthesia for gynecological day surgery, thereby providing evidence for the perioperative management of this new anesthetic agent.
This study has several limitations. First, the sample size is relatively small, which may have limited the statistical power to detect significant differences for some secondary outcomes. Second, as a single-center study, patient characteristics, anesthesia practices, and postoperative management may differ across centers; therefore, the generalizability of our findings to other healthcare settings requires further validation. Third, no long-term follow-up was conducted; the observation endpoints of this study were mainly confined to the first 24 hours postoperatively, and delayed PONV occurring after discharge was not assessed. Fourth, although we balanced major confounders (age, weight, anesthesia duration, and surgical type) between groups, we could not control for all potential influencing factors, such as peri-menstrual hormonal fluctuations, which may have influenced PONV incidence. Fifth, 36 patients were excluded after randomization. While we applied a modified intention-to-treat analysis with balanced exclusion rates across groups and considered the missing data to be missing at random, the possibility of attrition bias cannot be completely ruled out. Extreme-case sensitivity analyses showed that the treatment effect was attenuated to null under the worst-case imputation scenario, indicating that our findings are somewhat sensitive to missing-data assumptions. However, given that all exclusions were due to non-study-related reasons independent of PONV outcomes, the worst-case scenario is unlikely in clinical practice; nonetheless, our conclusions warrant confirmation in larger cohorts with lower attrition rates. Sixth, this study did not predefine a pharmacological rescue protocol for PONV. Perioperative management relied solely on preoperative education (eg, advising patients to avoid vigorous activity, maintain calm breathing, and adopt a relaxed mindset) to alleviate nausea symptoms, and no systematic documentation of rescue interventions was performed for patients who actually experienced PONV. Consequently, we were unable to evaluate the efficacy of pharmacological rescue therapies or compare the effectiveness of different rescue regimens. Lastly, our cardiac safety assessment was based on continuous intraoperative II-lead ECG monitoring rather than standardized 12-lead QTc measurements, which precludes the detection of subclinical QTc prolongation. This should be considered when interpreting the negative safety findings regarding droperidol.
Future large-sample, multicenter randomized controlled trials are needed to validate the generalizability of these findings and to further explore the optimal drug dose combinations as well as individualized antiemetic regimens for patient populations at different risk levels for PONV.
Conclusion
For gynecological day surgery patients receiving a general anesthesia regimen of ciprofol combined with alfentanil, the combination of dexamethasone and droperidol for the prevention of postoperative nausea and vomiting was significantly more effective than dexamethasone alone, with no significant difference in safety between the two regimens.
Data Sharing Statement
Individual deidentified participant data will not be shared due to ethical and privacy concerns, as the study involves human participants and the informed consent obtained did not include provisions for data sharing. The data that support the findings of this study are available from the corresponding author, Fanceng Ji (email: [email protected]), upon reasonable request, subject to institutional and ethical approval.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the Medical Ethics Committee of the Weifang People’s Hospital (approval number: KYLL20260214-5) on February 14, 2026. All participants provided written informed consent prior to enrollment.
Acknowledgments
We thank the patients who participated in this study.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Liu J, Han L, Zhang F, et al. Construction and validation of a web-based dynamic predictive model for the risk of postoperative nausea and vomiting in patients undergoing day-case hysteroscopic surgery. Front Med. 2025;12:1582546. doi:10.3389/fmed.2025.1582546
2. Aroke EN, Hicks TL. Pharmacogenetics of Postoperative Nausea and Vomiting. J Perianesth Nurs. 2019;34(6):1088–11. doi:10.1016/j.jopan.2019.03.007
3. Xu Y, Sun H, Liu Q, Liang P. Optimizing efficiency and safety in day surgery: perspectives from China. Anesthesiol Perioper Sci. 2025;3(4):53. doi:10.1007/s44254-025-00132-3
4. Yu Y, Deng J, Yin Y, Yang X, Liao M, Yu R. Ciprofol vs propofol for gastrointestinal endoscopy sedation: a systematic review and meta-analysis. Int J Surg. 2025;111(11):8575–8591. doi:10.1097/js9.0000000000003064
5. Apfel CC, Läärä E, Koivuranta M, et al. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
6. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2020;131(2):411–448. doi:10.1213/ane.0000000000004833
7. Chu CC, Hsing CH, Shieh JP, Chien CC, Ho CM, Wang JJ. The cellular mechanisms of the antiemetic action of dexamethasone and related glucocorticoids against vomiting. Eur J Pharmacol. 2014;722:48–54. doi:10.1016/j.ejphar.2013.10.008
8. Sneyd JR. Droperidol: past, present and future. Anaesthesia. 2009;64(11):1161–1164. doi:10.1111/j.1365-2044.2009.06124.x
9. Weibel S, Rücker G, Eberhart LH, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev. 2020;10(10):Cd012859. doi:10.1002/14651858.CD012859.pub2
10. Alshehri AM, Crowley KE, Lupi KE, Kim CS, DeGrado JR, Marino K. Evaluation of droperidol use in the emergency department: a retrospective analysis of QTc prolongation and adverse events. BMC Emerg Med. 2024;24(1):232. doi:10.1186/s12873-024-01158-9
11. Inam K, Qazi MS, Fatima E, et al. Efficacy and safety of dexamethasone in postoperative recovery following hysterectomy: a systematic review and meta-analysis. BMJ Open. 2025;15(10):e099097. doi:10.1136/bmjopen-2025-099097
12. Zhang S, Dong G, Shi X, Xiao H, Nie P, Ji F. Comparison of ciprofol versus propofol for the general anaesthesia during gynecological day surgery: a prospective, randomized, double-blind, non-inferiority trial. Drug Des Devel Ther. 2025;19:7151–7159. doi:10.2147/dddt.S539028
13. Zhou J, Wang L, Zhong Z, et al. Pharmacological mechanism and clinical application of ciprofol. Front Pharmacol. 2025;16:1572112. doi:10.3389/fphar.2025.1572112
14. Lan L, Liao J, Qin L, et al. The effects of ciprofol on haemodynamics under general anaesthesia during thoracoscopic surgery: a randomised, double-blind, controlled trial. BMC Anesthesiol. 2025;25(1):168. doi:10.1186/s12871-025-03054-6
15. Liu J, Hong A, Zeng J, Liang X. The efficacy of ciprofol versus propofol on anesthesia in patients undergoing endoscopy: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024;24(1):359. doi:10.1186/s12871-024-02721-4
16. Su R, Zhang L, Wang YM, et al. Effects of cipepofol on breathing patterns, respiratory drive, and inspiratory effort in mechanically ventilated patients. Front Med. 2025;12:1539238. doi:10.3389/fmed.2025.1539238
17. Zhang S, Liu Y, Liu Y, Xu T. The recovery of ciprofol, remimazolam and remimazolam-flumazenil for general anesthesia undergoing fundus surgery: a single-center, prospective, randomized, controlled clinical study. Drug Des Devel Ther. 2025;19:3691–3700. doi:10.2147/dddt.S512431
18. Gao PF, Zhao L, Li SY, et al. Prevention of postoperative nausea and vomiting after orthognathic surgery: a scoping review. BMC Anesthesiol. 2024;24(1):121. doi:10.1186/s12871-024-02510-z
19. Lai PC, Huang YT. Evidence-based review and appraisal of the use of droperidol in the emergency department. Tzu Chi Med J. 2018;30(1):1–4. doi:10.4103/tcmj.tcmj_195_17
20. Heyer EJ, Flood P. Droperidol suppresses spontaneous electrical activity in neurons cultured from ventral midbrain. Implications for neuroleptanesthesia. Brain Res. 2000;863(1–2):20–24. doi:10.1016/s0006-8993(00)02066-7
21. Kasagi Y, Hayashida M, Sugasawa Y, et al. Antiemetic effect of naloxone in combination with dexamethasone and droperidol in patients undergoing laparoscopic gynecological surgery. J Anesth. 2013;27(6):879–884. doi:10.1007/s00540-013-1630-8
22. Habib AS, El-Moalem HE, Gan TJ. The efficacy of the 5-HT3 receptor antagonists combined with droperidol for PONV prophylaxis is similar to their combination with dexamethasone. A meta-analysis of randomized controlled trials. Can J Anaesth. 2004;51(4):311–319. doi:10.1007/bf03018234
23. Shi S, Wu J, Wu Y, et al. Effects of ciprofol and propofol general anesthesia on postoperative recovery quality in patients undergoing ureteroscopy: a randomized, controlled, double-blind clinical trial. Drug Des Devel Ther. 2025;19:931–943. doi:10.2147/dddt.S497554
24. Hung KC, Chen JY, Wu SC, et al. A systematic review and meta-analysis comparing the efficacy and safety of ciprofol (HSK3486) versus propofol for anesthetic induction and non-ICU sedation. Front Pharmacol. 2023;14:1225288. doi:10.3389/fphar.2023.1225288
25. Wooltorton E. Droperidol: cardiovascular toxicity and deaths. CMAJ. 2002;166(7):932.
26. Habib AS, Gan TJ. Food and drug administration black box warning on the perioperative use of droperidol: a review of the cases. Anesth Analg. 2003;96(5):1377–1379. doi:10.1213/01.Ane.0000063923.87560.37
27. Luo D, Huang Z, Tang S, et al. Risk analysis of postoperative nausea and vomiting in patients after gynecologic laparoscopic surgery. BMC Anesthesiol. 2024;24(1):345. doi:10.1186/s12871-024-02727-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.