Back to Journals » International Journal of Nanomedicine » Volume 21
Developments & Potential of Nanotechnology for the Detection and Treatment of Pancreatic Cancer
Received 7 November 2025
Accepted for publication 30 January 2026
Published 5 February 2026 Volume 2026:21 559038
DOI https://doi.org/10.2147/IJN.S559038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Eng San Thian
Danielle O’Meara, Clare Hoskins
Department of Pure and Applied Chemistry, University of Strathclyde, Glasgow, UK
Correspondence: Clare Hoskins, Department of Pure and Applied Chemistry, University of Strathclyde, Glasgow, UK, Email [email protected]
Abstract: Pancreatic cancer is projected to become the second leading cause of cancer death by 2030 with a dismal 5-year survival rate compared to other cancers (12%). Due to the absence of clear early symptoms, diagnosis is often delayed resulting in many patients presenting with advanced disease and limited treatment options. Surgery remains the only potential curative option. However, only about 20% of cases are detected early enough for surgery. Consequently, most patients rely on chemotherapy, immunotherapy and radiotherapy. Among these, chemotherapy offers the best chance of tumor shrinkage, it comes with many problems such as harsh side effects which kill healthy cells and cancer cells, leaving the patient sometimes too ill to continue treatment. With immuno- and radiotherapy, it offers limited success in the treatment of pancreatic cancer despite its success in treating other forms of cancer. Nanotechnology offers promising opportunities for more effective diagnosis and less aggressive treatment. Fortunately, there has been some success for pancreatic cancer with two nano formulations currently approved by the Food and Drug Agency (Onivyde and Abraxane) offering greater survival rates and reduced side effects compared to traditional chemotherapy. Unfortunately, progress in nanotechnology-based diagnostics for pancreatic cancer remains limited. However, numerous different types of nanoparticles are under investigation in preclinical and clinical studies showing positive results. This review gives an overview of the potential of nanotechnology within this area looking at harnessing its potential in more effective diagnosis strategies and for more efficient therapy.
Keywords: pancreatic cancer, drug delivery, cancer nanomedicine, diagnostics, theranostics, nanotechnology
Introduction
Pancreatic cancer (PC) is a highly fatal disease with 511,000 new cases and 467,000 deaths globally, in 2022 alone, ranking it as the 6th leading cause of cancer death and the 12th most prevalent cancer.1 PC has the worst 5-year survival rate compared to other common cancers, with only 12% of patients surviving, and as such in the UK, the cancer has been officially designated as a cancer of unmet need. Unfortunately, giving the rising numbers of cases annually, the mortality to incidence ratio is expected to increase, with PC projected to become the second leading cause of cancer death by 2030 in the United States.1–3
Pancreatic ductal adenocarcinoma (PDAC) is the most common form of exocrine PC and accounts for ~90% of all pancreatic malignancies.4 With ~60–70% of PDAC occurring at the head of the pancreas, 15% residing within the body and the remainder in the tail (15%). Conventional treatment for PC includes surgery, chemo- and radiotherapy, with surgery being the most favourable option.5 However, due to a multitude of challenges such as the asymptomatic early stages, lack of known biomarkers resulting in lack of early detection/screening methods, PC is typically diagnosed at much later stages than the other cancers, with ~70–80% of cases being diagnosed at the locally advanced (LA) or metastatic stage.6–8 As a result, surgical resection is only feasible in fewer than 20% of patients, underscoring the urgent need for improved therapeutic and early diagnostic approaches.5
Nanotechnology sits at the forefront of innovation in the 21st century with applications spanning a vast array of sectors including electronics, food, cosmetics and most promisingly in medicinal detection and therapeutics.9 Nanomaterials possess many unique properties that make them highly versatile such as optical properties, enhanced permeation, ease of synthesis and purification. Their high surface area to volume ratios allows them to be easily tailored and surface engineered for their intended application. In the pharmaceutical industry various nanocarriers, such as solid lipid nanoparticles (SLNs), liposomes, polymeric micelles and polymeric drug conjugate (PDU) have shown to improve stability, control drug release and offer targeted drug delivery. Additionally, nanotechnology has been shown to increase solubility and bioavailability, a vital advantage due to the increase in highly hydrophobic drugs arriving on the market. Nanocarriers can be functionalized with ligands, proteins or antibodies to target specific cells/tissues. Alternatively, nanocarriers can be engineered to respond to external (light) or internal stimuli (pH, enzymes), leaving a wide range of opportunities for as therapeutics. Aside from drug delivery, the inorganic nanoparticles have been developed as diagnostic agents, usually as tracer molecules used as an aid in illuminating tumor tissue, with some of these combining this powerful diagnostic tool with triggered drug delivery, acting as theranostic molecules.
This review focuses on the current climate of PC research up to late 2025, highlighting recent success in preclinical and clinical therapeutic and diagnosis studies, addressing the challenges associated and the critical need to address the knowledge gap, analysing the advances which nanotechnology has made to date, and its future potential in the diagnosis and treatment of PC.
Challenges in Pancreatic Cancer
PC remains one of the most lethal malignancies, with limited progress over the last few decades. The common treatment options for PC are summarized in Figure 1A with the associated challenges in treating pancreatic cancer in Figure 1B.
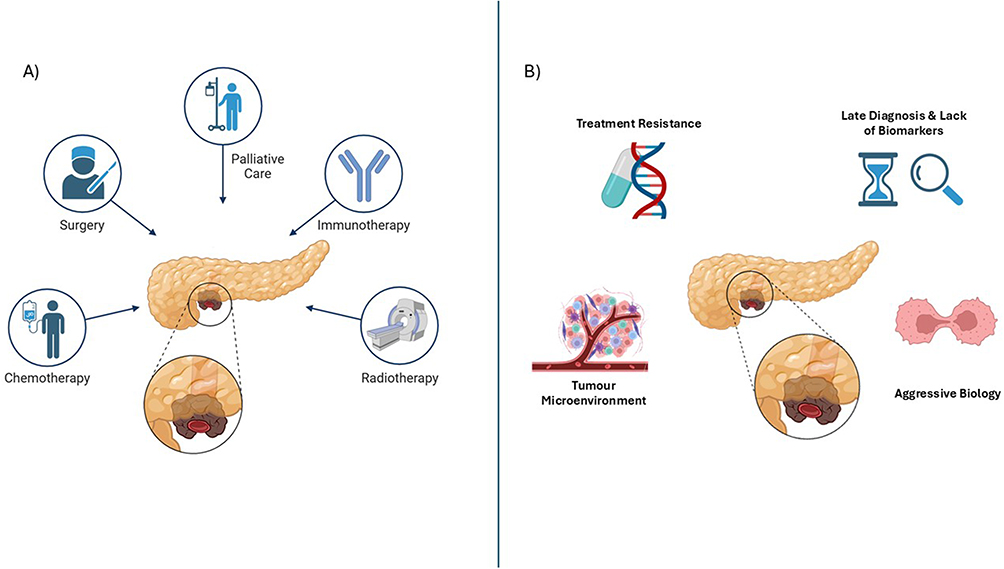 |
Figure 1 (A) Summary of common treatment options for pancreatic cancer (B) Summary of the major challenges in treating pancreatic cancer created with BioRender.com. |
Late Diagnosis and Lack of Biomarkers
There are many factors which are challenging for the diagnosis and treatment of PC, including the lack of known, reliable biomarkers at the early stages of cancer, meaning it is incredibly hard to detect, and no large-scale screening technique is used, which often results in the tumor being undetected until it is too late.10 PC forms extremely solid (cartilage like) tumors, surrounded by a dense stroma, this hostile rapidly growing body has been designed by the microenvironment (TME) to hinder penetration – including therapeutics.11 Often large drug doses are required to exert any effect on the tumor size or rate of proliferation, however, given such low quantities of chemotherapy penetrate the tumor, resistance often rapidly develops.
Unlike in other cancers, such as breast cancer (BRCA gene), biomarkers have been identified in body fluids which are used to definitively diagnose a disease at an early, curable stage.12 PC only has one biomarker currently approved by the Food and Drug Agency (FDA), cancer antigen 19–9 (CA19-9).4 However, it is only used to monitor treatment response and to detect recurrence – as it is not accurate in diagnosing the disease in the general population due to its low predictive value. Carcinoembryonic agent (CEA) is another traditional biomarker, which has been investigated for use in early-stage diagnostics, as it is present in PC, however, CEA have proven to be less effective than CA19-9.5 However, when the two biomarkers are used in combination, diagnostic accuracy increased. A newer potential biomarker, cell migration-inducing hyaluronan binding protein (CEMIP) has been observed in multiple cancers, including PC, and when combined with CA19-9, is better at identifying PC than CA19-9 alone.
Cost-effective screening remains challenging due to its low incidence rate, typically asymptotic early stages and lack of definitive biomarkers.10,12 Diagnosis currently relies on imaging modalities, such as, computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET) and endoscopic ultrasound (EUS). However, none of these techniques are perfect and come with their own issues.
Tumor Microenvironment (TME)
The TME severely hinders delivery of therapeutics to their intended site of need. Desmoplasia, a key feature in many cancers, is especially prominent in PC.13,14 It is a buildup of dense fibrous tissue around the tumor, caused by rapid proliferation of fibroblasts. They secrete large amounts of extracellular matrix (ECM), which are proteins which form a thick and rigid structure around the tumor. The continued overproduction of ECM increases the pressure within the TME, resulting in the blood vessels being restricted, forming a hypoxic environment and blocking the delivery of chemotherapies/immunotherapies into the tumor. Additionally, certain ECM components, such as, hyaluronan and tenascin-C interact with the toll-like receptors (TLRs) on immune cells, confusing the immune system resulting in chronic, non-productive inflammation, which further fuels tumor growth. Within the TME, the tumor will continue growing undetected due to the secretion of immunosuppressive cytokines. All these components, help PC tumors form an impenetrable wall, making therapeutic interventions very difficult and ineffective.
Resistance to Therapeutic/Chemo Side Effects
Chemotherapy can be administered as a neoadjuvant therapy (before surgery), to shrink the tumor, increasing access to the tumor site, reducing surgical complications particularly with the surrounding vasculature and increases chances of complete resection.15–17 Otherwise, they are administered as adjuvant therapies (after surgery) to kill residual cancer cells and reduce recurrence risk. However, in PC, the prognosis for those patients receiving adjuvant care remains poor and ultimately surgery with neoadjuvant care is the best option. In many PC cases, the tumor is too advanced to allow for surgical intervention, in these cases radiation therapy or chemotherapy are used as the first-line treatments to shrink or reduce the rate of tumor growth.
Gemcitabine (GEM) demonstrated its effectiveness as a first-line chemotherapy for PC in 1997, overtaking 5-fluorouacil (5-FU) as the most frequently used drug.18 Before this discovery, 5-FU had exceptionally low survival rates with 5.51 months and a 2% one-year survival probability. GEM offered an increase in this survival rate to 5.56 months and 18%, respectively. Although this does not seem substantial, any increase in survival chances in PC is a major breakthrough. However, GEM was not effective in all patients, huge interpatient variability was observed and ultimately, many patients who responded well to GEM treatment, ultimately developed resistance at later stages of their recovery journey.19 In recent years, new evidence has emerged that poor penetration and resistance may not be the only mechanism behind the poor GEM performance, with Geller et al reporting in 2017 that intertumoral bacterial in PC tumors had been shown to be degrading GEM before it could even enter the cells and carry out its activity.20 As a result, GEM is now administered in combination with other chemotherapies clinically to enhance its performance.
Other chemotherapies used in PC include paclitaxel, irinotecan or capecitabine (cap) (oral 5-FU drug).21 Platinum drugs have been incorporated such as cisplatin or oxaliplatin. Additionally, these drugs can be used in combinations, such as FOLFIRINOX (folinic acid/leucovirin (LV), 5-FU, irinotecan and oxaliplatin), GemCap, nab paclitaxel/Abraxane + GEM or OFF (LV, 5-FU and oxaliplatin).22
Unfortunately, although chemotherapy is arguably the second-best treatment action, it is accompanied by a host of negative side effects. Henry et al conducted a cross-sectional national survey in the United States to analyse side effects affected by chemo and/or radiotherapy.23 Notably, the most common side effects reported were fatigue, pain, nausea and/or vomiting, anxiety and insomnia. With patients also showing moderate-to-high levels of depression and an average time of 4.5 hours spent on visits to professionals to treat side effects. In the study, 43% of patients were still employed and of those patients, 78% were still working and the remainder on medical leave. Patients were reported to miss an average of 26 days of work due to receiving treatment and a further 18 days for side effects experienced. Another well-known and most common side effect is hair loss which can negatively affect the patient’s mental health. Others include low platelet and white blood cell counts, changes in appetite, diarrhea, skin rashes and “chemo brain” – affecting concentration levels and focus. Unfortunately, due to the late-stage diagnosis, some patients are simply too ill to take chemotherapy due to these unforgiving off target effects, and PC ultimately is their death sentence.
Chemoresistance remains a major barrier in the effective treatment of PC, contributed by multiple factors, such as the TME, dense stroma and genetic mutations, limiting effective drug delivery.24 As a result, common chemotherapy drugs such as GEM and FOLFIRINOX achieve subpar results, further highlighting the importance of finding more reliant and effective therapeutic drugs.
While essential, chemotherapy is extremely harsh and non-discriminatory, high doses are required to combat PC, leading to significant side effects. It is critical to discover alternative treatment to increase efficacy, reduce hospital visits and minimise harsh side effects.
Immunotherapy Limitations
Given the remarkable success of several FDA approved immunotherapies in other malignancies, such as non-small cell lung cancer (NSCLC), non-Hodgkin’s lymphoma and tumors with high microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR), there was great hope that similar immunotherapies could hold promise in PC treatment.25–29 Unfortunately, its impact in PC has been disappointing despite early optimism. Immunotherapy utilizes the body’s own natural immune system to eliminate cancer cells.30 Immune checkpoint inhibitors (ICI) are a type of immunotherapy which work by blocking the T cells which the cancer cells use to evade detection.25 By blocking these cells, they remain active and attack cancer cells. Despite success in other cancers, they have shown poor performance with PC, even when combined with chemotherapy.25,31 Perhaps, like the chemotherapies, this is due to the dense stroma hindering their entrance into the TME to exert their effect. Although this lack of promise, one ICI, pembrolizumab has been recommended as a second line therapy for patients with dMMR or MSI-H, including certain PC types; however, not all patients are eligible. It is speculated that due to the TME actively suppressing immune responses through cells like myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs), tumor cells possess poor antigenicity and even when presented, they remain “invisible” and can evade the immune system. This landscape makes ICI largely ineffective in PC treatment compared to other cancers.
Radiotherapy Limitations
Radiotherapy uses high doses of radiation (X-rays, gamma rays, or particle beams) to irreversibly damage cancerous tissue or cells, resulting in tumor shrinkage. Radiotherapy may be used after and occasionally before surgery to eliminate the cancer.32 Stereotactic body radiotherapy (SBRT) delivers higher focussed doses of radiation directly to the tumor in only a few treatment fractions. Since the tumor core exists in a higher hypoxic environment than the tumor periphery or boundary, it experiences a greater extent of radio resistance. In SBRT a hotspot in this radioresistant area allows for a high-dose distribution, resulting in dose escalation. This phenomenon has proved beneficial to PC patients, as it is rapid and generally better tolerated than conventional radiotherapy.33
Primarily in PC, radiotherapy it is used as an intervention which can slow tumor growth, but it is not curative as it is not effective enough to eliminate the tumor completely. Therefore, it is common practice for it to be used in combination with chemotherapy34 or immunotherapy.35 As radiotherapy is a focussed therapy, it targets only the localized disease; therefore, it is not helpful in cases of metastasis. In PC specifically, it is also problematic given the location of the organ, which hinders the dose that can be safely delivered without risk of adverse off target radiation damage.
Cancer Nanotechnology
With cancer as the leading cause of death globally, with approximately 10 million deaths in 2020 alone, an effective treatment/early diagnosis is vital to decrease the ever-growing mortality and incidence rates.36 Nanotechnology offers opportunities in this area due to its versatility, functionality and ability to precision target sites of need. Targeted delivery is believed to occur in two ways, either through passive or active mechanisms.37 Passive targeting utilizes the TME through the enhanced permeability and retention (EPR) effect, where the leaky vasculature and the impaired lymphatic drainage of tumors allow for the accumulation of nanoparticles. However, the EPR effect remains controversial, as it is often significantly overestimated in animal models compared to human models.37 Whilst debate rages on about whether the EPR effect exists in a helpful manner for many cancers, consensus is that for PC, the harsh TME does not allow for EPR to occur. Therefore, a different targeting mechanism is employed. Active targeting involves modifying the surface of the nanoparticle with ligands/antibodies which specifically bind to biomarkers on certain cells or tissues.38,39 Due to the size of nanoparticles (10–100 nm), they can move in the body without triggering strong immune responses.40 There is a wealth of studies using various types of nanoparticles in a range of cancers, summarised in Figure 2.
 |
Figure 2 Types of nanoparticles (NP) used in cancer, created with BioRender.com. |
Liposomes were among the first clinically successful nanoparticles in oncology with poly(ethylene glycol) functionalised (PEGylated) liposomal doxorubicin (Doxil) approved by the FDA in 1995 for the treatment of ovarian cancer, AIDS related Kapisi’s sarcoma.41 Doxil altered doxorubicin pharmacokinetics and reduced cardiotoxicity compared to the free drug. Following this success, several other liposome-based products were approved the management of various cancers: Depocyt, Myocet, Mepact and Marqibo. More recently, lipid nanoparticles gained significant interest due to rapid and scalable production, high precision and favourable safety profile.42 There are multiple mRNA vaccines in animal and human trials for several types of cancers.43,44
Metallic nanoparticles (MNPs) offer unique properties such as optical, magnetic, electrical characteristics which increase their capabilities to be used for diagnosis.43–45 With studies highlighting improved imaging and the ability to detect prostate cancer biomarkers in blood and urine with high sensitivity and specificity.46,47 Currently, only one MNP-based formulation is approved for glioblastoma or prostate cancer, NanoTherm.
Clinical Success of Cancer Nanotechnology for PC
The FDA approved two nanotechnologies for use in PC, both licensed for drug delivery. These are Abraxane and Onyvide. Abraxane/nab-paclitaxel is an albumin-bound drug formulation, where paclitaxel, the well-known microtubule stabilizing chemotherapy, is bound to human serum albumin. In the case of paclitaxel, its aqueous solubility severely hinders its clinical use, despite its promising potency.48 The drug itself is highly toxic and often cannot be tolerated as the off-target effects are too extensive. However, the Abraxane formulation allows the active to travel systemically for longer, enhancing accumulation within the pancreas, reducing off target effects. Effectively, allowing patients, which would not be able to tolerate paclitaxel, to undertake this regime. Abraxane gained significant traction in the MPACT trial which demonstrated that providing it in combination with GEM, significantly improved response, overall survival and progression free (OS and PF respectively) survival rates compared to GEM alone (8.5 vs 6.7 OS months with survival rates of 35% vs 22% at year one and 9% vs 4% at year two) in patients with metastatic PDAC.49 A follow up report investigated the long term survival of patients receiving Abraxane and GEM in a combination therapy regimen, further demonstrating that Abraxane and GEM delivered sustained survival rates over GEM alone (median OS: 8.7 vs 6.6 months) with a small positive >3% year survival in only the combination arm.50 However, neurotoxicity and myelosuppression were higher in the combination than GEM alone, though these were observed to be manageable.
Onivyde, is a liposomal formulation of irinotecan (nal-IRI) approved to PC. Irinotecan is a topoisomerase inhibitor, which disturbs the cancer cell ability to replicate DNA, leading to cell death. The drug molecules are encapsulated within the liposome macromolecular structure, which protects it on its journey to the PC, prolongs drug circulation times, enhances ability to accumulate and in effect increases drug exposure, increasing therapeutic effectiveness. Onivyde is mainly used in combination with other drugs, with the NAPOLI-1 Phase III trial highlighting the importance of the liposomal formulation.51 The trial consisted of 417 patients with metastatic PC previously treated with GEM-based therapy, who were randomly grouped and administered Onyvide with or without 5-FU/LV or 5-FU & LV. Results demonstrated that OS of Onivyde in combination with 5-FU and LV was 6.1 months vs 4.1 months with 5-FU and LV alone. No difference was observed in Oniyvde alone with 5-FU and LV (4.9 vs 4.2 months). Additionally, it was noted that Oniyvde alone presented more side effects than 5-FU and LV. This study led to the approval of Onivyde in combination with 5-FU/LV for metastatic PC patients whose disease has progressed after GEM-based therapy. More recently, the FDA approved another combination chemotherapy treatment for metastatic PC using Onivyde along with 5-FU, LV and oxaliplatin (NALIRIFOX).52 The NAPOLI 3 trial consisted of 770 patients with metastatic PC, who were randomly assigned NALIRIFOX on days 1 and 25 or Abraxane and GEM on days 1, 8 and 15 of a 28-day cycle. NALIRIFOX median OS was significantly greater than standard chemotherapy (11.1 vs 9.2 months) with PF at 7.4 vs 5.6 months.
While some success has been made in improving treatment for PDAC patients with two FDA nano formulations approved for use, there is still demanded to strive for better. Prescribing Onivyde on its own was determined not to be effective as a single agent and resulted in more adverse events. Its strength is demonstrated when it is used as a combination therapy with a slight improvement in OS.51,52 The liposomal formulation alters irinotecan’s pharmacokinetics, extending circulation time and shown to accumulate in tumour cells through the EPR effect.53 Similarly, this is observed with Abraxane with the nanoparticle formulation disrupting the tumor stroma, improving penetration of both paclitaxel and GEM.48
There is no diagnostic technique or nanotechnology which has been approved specifically for PC. The existing contrast agents are predominantly nanotechnology based where inorganic nanoparticles such as Dotarem, Clariscan and Primovist which are all Gadolinium-based or Feridex which is iron oxide based are used combined with magnetic resonance imaging. Other imaging modalities under investigation with the use of nanoparticle tracers, such as CT scanning, will be discussed later.
Nanotechnologies Undergoing Clinical Trial for PC
Beyond metastatic settings, Abraxane is used in ongoing studies investigating its effectiveness in neoadjuvant, adjuvant and combination strategies to further improve outcomes in PC, some examples are shown in Table 1 below with other clinical trials involving other common chemotherapy drugs.
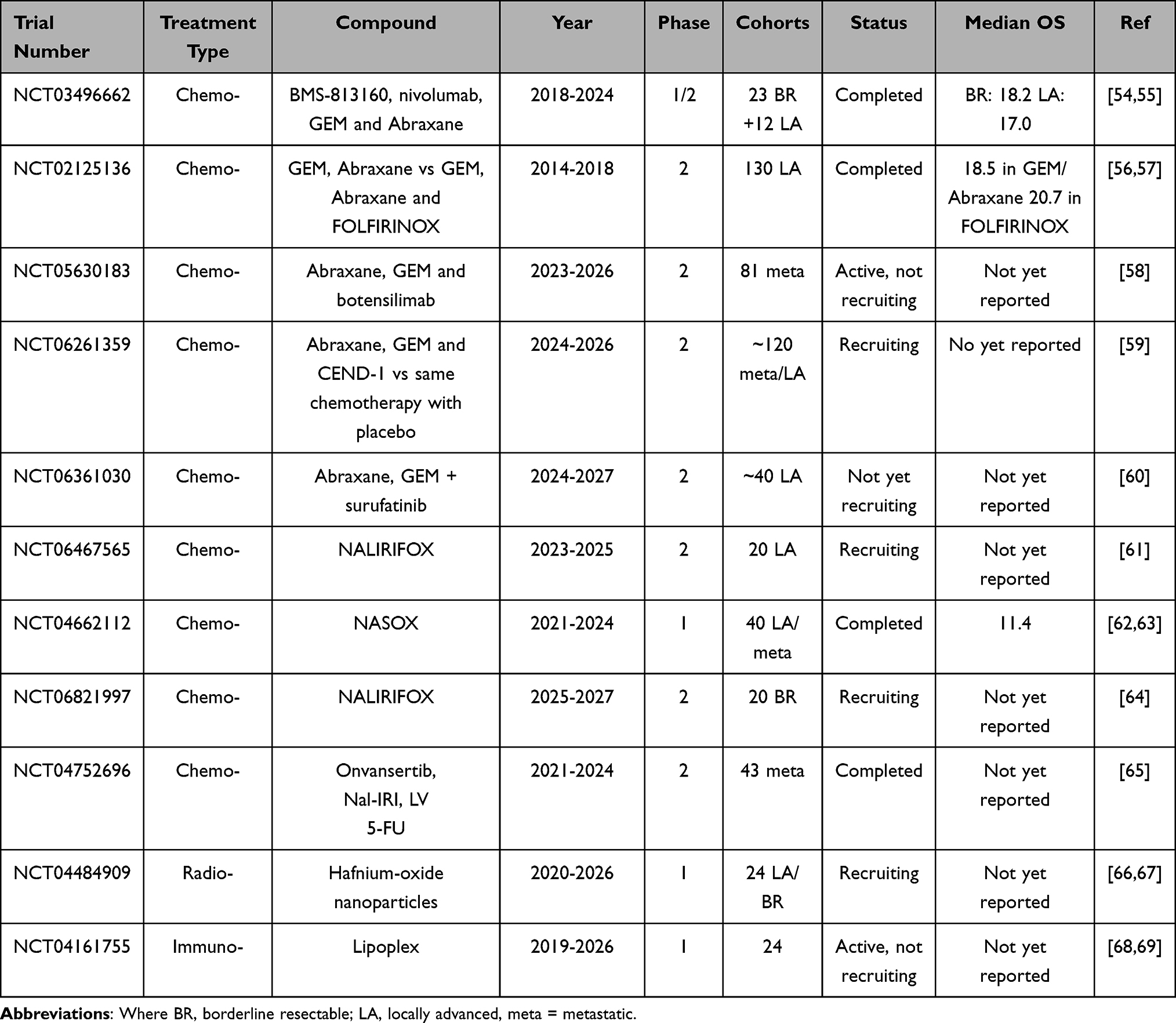 |
Table 1 Clinical Trials Involving Nanoparticles for the Treatment of PC |
NCT03496662 evaluated the safety and efficacy of combining the CCR2/5 inhibitor immunotherapy, BMS-813160 with nivolumab, GEM and Abraxane in patients with borderline resectable (BR) and locally advanced (LA) PDAC.54,55 The regimen consisted of four 28-day cycles of patients receiving chemo or combination treatment. Generally, treatment was well tolerated with only one instance of each Grade 3 diarrhea and QTc prolongation, which increases the risk of developing dangerous arrhythmias. The objective response rate (ORR) was 42% in BR and 20% in LA with 0% in chemotherapy control group. Importantly, meaningful surgical conversion rates were observed at 83% of BR and 20% of LA after treatment. Additionally, survival outcomes with median progression and overall survival for BR and LA was 11.9 and 18.2 months and 14.7 and 17.0 months, respectively.
The NEOLAP (NCT02125136) study was a multicentre randomized phased 2 trial evaluating conversion rate to resectability in LA PDAC with intensified neoadjuvant chemotherapy.56,57 Initially, all patients received two rounds of Abraxane and GEM as neoadjuvant chemotherapy and were restaged. Patients without disease progression were randomised into a 1:1 trial and received either two further rounds of Abraxane and GEM or four rounds of FOLFIRINOX. All patients without progression underwent exploratory laparotomy, while those with resectable tumors underwent curative surgery followed by three rounds of adjuvant chemotherapy. Among 130 patients, resection rates were comparable with Abraxane/GEM at 36% and 44% with FOLFIRINOX and median OS rates similar at 18.5 vs 20.7 months, respectively. It is important to note that FOLFIRINOX produced significant nodal downstaging, suggesting deeper pathological response. Both regimens had manageable toxicity with grade 3 adverse effects in ~55% of patients and no treatment-related induction deaths.
NCT04662112 is a completed multicentre study, which evaluated the safety and efficacy of NASOX regimen (Onivyde, S-1 and oxaliplatin) in advanced PC.62,63 Recommended dose consisted of receiving Onivyde and oxaliplatin on day 1 and S-1 twice daily on days 1–7, repeating every 14 days. Overall, the regimen has a manageable safety profile with most common Grade 3–4 adverse events being neutropenia (31.7%), enterocolitis (9.8%), anorexia (7.3%) and diarrhea (2.4%). The objective response rate (ORR) was 58.5% (with one complete and 23 partial responses). Additionally, two patients underwent surgery with complete resection and after a median follow up of 17.5 months, the median progression-free survival was 6.5 months and OS at 11.4 months. Therefore, showing potential to replace current chemotherapy treatments.
NCT04752696 assessed the efficacy of immunotherapy onvansertib in combination with Onivyde, LV, 5-FU for second line treatment of metastatic PC. Treatment schedule included oral delivery of onvansertib on days 1–10 per 14-day cycle, co administered with Onivyde, LV and 5-FU. Current available results show 19% ORR, a median PFS of 5 months. However, these results are early and full data on OS and safety have yet to be published, but trial shows promising results as when compared to conventional treatment in similar patients, ORR is ~7.7% and 3.1 months PFS.
NCT05630183 is an ongoing multicentre trial due for completion in 2025 with currently 81 patients receiving intravenous care for metastatic PC. The study aims to assess if the addition of immunotherapy botensilimab to Abraxane and GEM combinations will improve the efficacy. While NCT06261359 is trial that is currently recruiting and aims to assess the safety and efficacy of CEND-1 in combination with standard chemotherapy for patients with locally advanced unresectable or metastatic PC. CEND-1 is a cyclic peptide, which will form a nanoparticle, it targets αV integrins and neuropilin-1 and enhances tumor delivery of co-administered anticancer drugs and has been hailed as a frontrunner as a new therapeutic targeting strategy in PC. NCT06361030 is an active, not yet recruiting trial looking the evaluate the safety and efficacy of surufatinib combined with standard chemotherapy in patients with locally advanced PC due to complete in 2027.
Rojas et al evaluated autogene cevumeran, an individualized mRNA neoantigen vaccine delivered in lipoplex nanoparticles, given sequentially with atezolizumab and mFOLFIRINOX.68,69 Primary findings show vaccine was well-tolerated and induced de novo high-magnitude neoantigen-specific T cell responses in 8 of 16 patients, including expansion of functional CD8+ T cells detectable in blood. Patients who showed these responses, also had longer recurrence-free survival compared with non-responders.
NCT03589339 reports for the first time an LA PDAC patient receiving a functionalized hafnium oxide crystalline nanoparticle, NBTXR3.66,67 The patient received EUS-guided intratumoral injection of NBTXR3 followed by intensity-modulated radiation therapy. NBTXR3 was well retained within the tumor, confirmed by daily imaging and no acute adverse events or treatment-related toxicities observed. All these studies are ongoing, but the hope is that all or most progress onto clinical success.
As observed, most clinical trials for the treatment of PC are chemotherapy or immunotherapy based. However, one radiotherapy trial is currently recruiting for LA or BR PC patients. Using NBTXR3 (hafnium-oxide nanoparticle, a radio enhancer) which will be injected into the tumor to enhance the effect of radiation therapy.
Therapeutic Nanotechnology in Pancreatic Cancer
The need for novel treatments may open new therapeutic avenues for patients with PC, some examples of other novel treatments are shown below in Table 2 which are in preclinical stages.
 |
Table 2 Preclinical Studies Involving Nanoparticles for the Treatment of PC |
Prabhuraj et al designed a mesoporous silica nanoparticle loaded with curcumin and coated with PEG and targeting ligand, transferrin.71 Results showed cellular uptake was 7-fold higher than curcumin alone in pancreatic cells and 3-fold higher cytotoxicity in MIA PaCa-2. The in vivo studies showed significant tumor growth inhibition and reduced metastasis in a pancreatic cancer xenograft model. Additionally, it was observed that the nanoparticles sensitized the cancer cells to GEM, boosting GEM’s ability to kill cancer cells.
Responsive nanoparticles are an emerging class of smart materials engineered to change their behavior in relation to a specific internal or external stimuli.78 These nanoparticles are designed to have built-in “triggers”, some examples include changes in pH, temperature, light, magnetic fields, enzymes, redox conditions or mechanical stress. This change causes a change in structure, surface chemistry or release of encapsulated cargo. A few approaches have been explored in recent years with examples summarized in Table 3 and Figure 3 summarizing the external and internal stimulus.
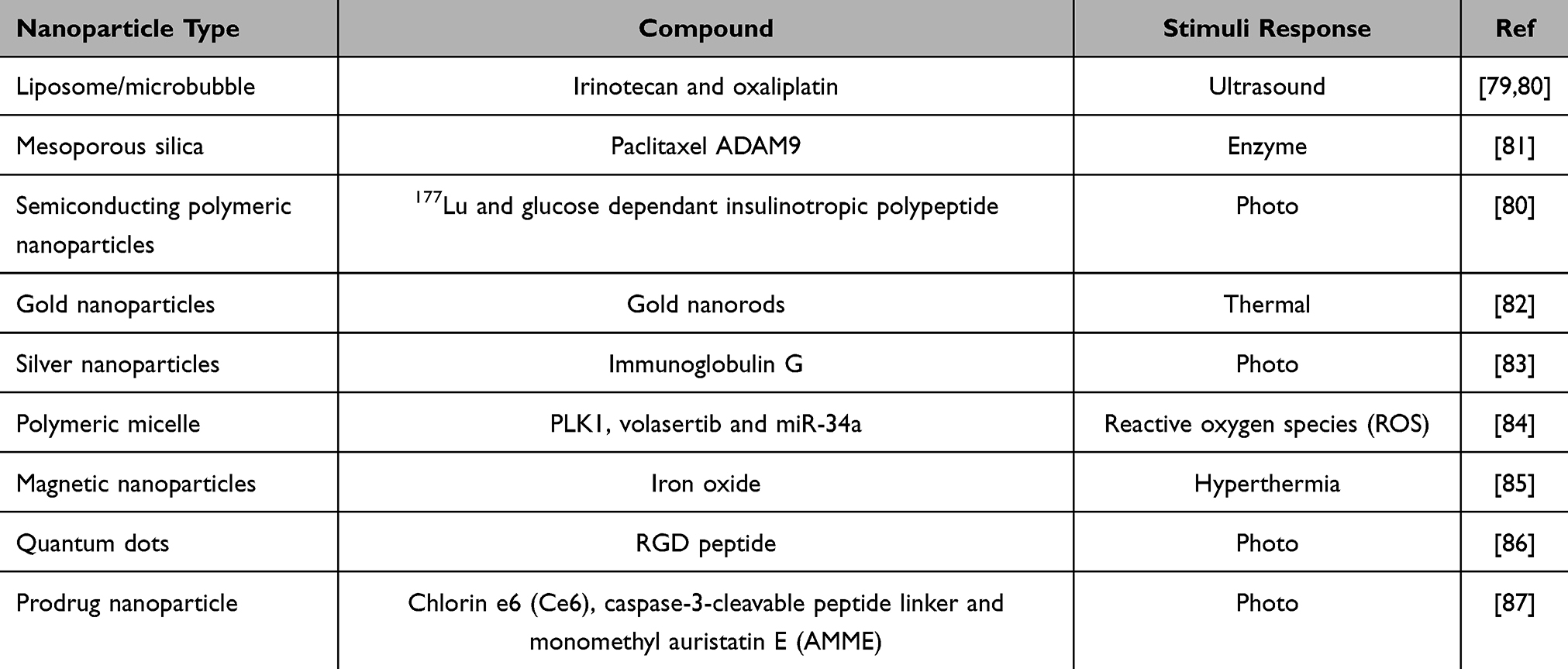 |
Table 3 Stimuli Responsive Nanoparticles in Preclinical Studies for the Treatment of Pancreatic Cancer |
 |
Figure 3 External and internal stimuli nanoparticles used in pancreatic cancer, created with BioRender.com. |
Nedelcu et al investigated using silver nanoparticles functionalized with immunoglobulin G (IgG) for phototherapy.83 Under 808 nm laser exposure, the functionalized nanoparticle converted laser irradiation to localised heat, producing significant dose-dependent cytotoxicity in PANC-1 cells with silver nanoparticles or laser exposure alone showing minimal effect. Treatment induced Golgi apparatus disruption, leading to the activation of caspase 3 apoptosis, confirming cell death. Xin et al developed reactive oxygen species (ROS) responsive polymeric micelle to co-deliver PLK1 inhibitor, volasertib and tumor suppressor microRNA, miR-34a.84 Results demonstrated synergistic cytotoxic effects with reduced IC50 by 2–4.5-fold compared to volasertib alone. Additionally, the combination treatment induced greater G2/M cell-cycle arrest, increased apoptosis (~55% in one assay), reduced colony formation. In an orthotopic pancreatic tumor model (NSG mice), it was observed that the micelles accumulated in tumors, resulting in significantly reduced tumor volume with negligible systemic toxicity in major organs.
Diaz-Riascos et al developed iron oxide magnetic nanoparticles for localised magnetic hyperthermia.85 The formulation, termed NTT agent generated heat under an alternating magnetic field designed to be injected along with GEM + Abraxane. In PDAC cell lines and xenograft models, the combined treatment produced synergistic cytotoxicity, significantly reduced tumor growth inhibition and enhanced intratumoral drug penetration.
Recent advances in nanomedicines have explored stimulus-responsive prodrug formulations to improve therapeutic precision. Cho et al developed a light-activated MMAE prodrug nanoparticle for photo-chemotherapy treatment.87 MMAE is conjugated to the photosensitizer Ce6 via a caspase-3-cleavable linker. Upon light irradiation, Ce6 produces ROS that induced apoptosis and elevates caspases-3 levels which cleave the linker to release active MMAE within tumor tissue. This produced enhanced cytotoxicity in vitro compared with monotherapies while remaining inactive without light exposure. In orthotopic PDAC models, treatment with the prodrug nanoparticle and irradiation resulted in substantial tumor growth suppression with improved survival (Figure 4). Additionally, reduced systemic toxicity relative to free MMAE was observed.87
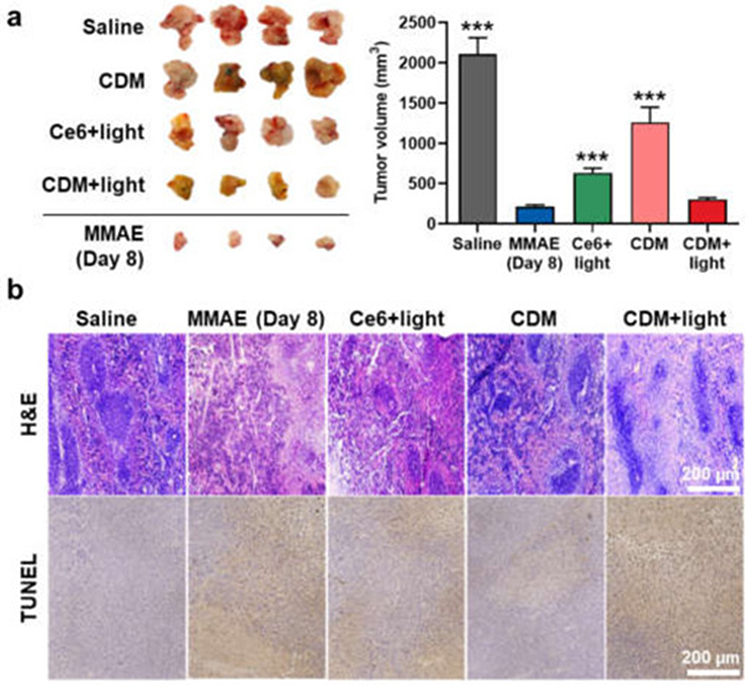 |
Figure 4 In vivo therapeutic efficacy of CDM in orthotopic pancreatic cancer models. (a) Optical images and volume of cancer tissues from orthotopic pancreatic cancer models after treatment with saline, MMAE, Ce6, or CDM. The tumors of Ce6- or CDM-treated mice were locally irradiated with visible light with power of 160 mW for 10 min. The 3 asterisks in Figure indicate the comparison to the CDM+light group. (b) Pancreatic cancer tissues stained with H&E or TUNEL.87 |
Nanoparticles as Radiation Enhancers in PC
Nanoparticle-enhanced radiotherapy (NERT) uses biocompatible nanoparticles functionalized for tumor targeting. In NERT, the nanoparticles act as radiosensitizers or radiation enhancers, thereby, increasing the local radiation dose experienced within the tumor tissue, whilst reducing the overall dose requirement, which minimizes the off-target effects. Park et al reported the fabrication of a docetaxel-contained polymeric nanoparticle (DTX-PNP) to act as a radiosensitizer for PC.88 The novel DTX-PNP was tested in vitro and in vivo in AsPC-1 or BxPC-3 cell lines or xenografts. The combined DTX-PNP administration and radiation therapy DTX-PNP in combination with IR possessed a high level of cytotoxicity in the cell lines. In vivo radiotherapeutic efficacy of the DTX-PNP nanoplatform was compared to the standard chemoradiation agent Gemzar. The data showed that in both PC xenograft models, the DTX-PNP combined with radiotherapy showed a significant enhancement in tumor retardation compared with the radiotherapy alone, an improvement when compared with the Gemzar and IR. This combined approach for chemoradiation plus radiosensitization holds promise for further therapeutics in PC. Other organic nanoparticles coupled with drugs which act as radiosensitizer such as albumin encapsulating paclitaxel have shown to possess enhanced therapeutic outcomes in PC when used in combination.89
Colloidal gold (nanoparticles, nanospheres, rods etc) is well known to act as radiation enhancers. The high atomic number of gold leads to a greater absorption of X-rays and gamma rays compared to the biological tissue. The focused radiation absorption by the gold nanoparticle enhances the local damage within the tumor microenvironment. Aliru et al created gold nanospheres (AuNSs) which were surface decorated with a nuclear localization sequence (NLS) peptide to promote accumulation within the nucleus in PC cells.90 In vitro radiosensitization studies were carried out in Panc-1cells, and in vivo models. The study showed that internalization within the nucleus of the targeted particles was significantly higher than for the non-targeted particles. Clonogenic cell survival indicated a statistical significance (p<0.05) in radiosensitization enhancement factors, calculated at the 10% survival fraction between the treatment groups using different types of radiation. In vivo studies showed increased tumor retardation with the AuNSs and radiation, compared with the radiation alone. Besides gold, other metallic nanoparticles such as gadolinium and hafnium oxide exert a comparative effect.91,92
Nanotechnology as Diagnostics for PC
There have been promising results in this arena, ranging from improving biomarker detection, contrast enhancement, to the detection of circulating cancer cells (CTCs) and enabling multiplexed detection.
Conventional biomarkers such as CA-19 are useful but they lack the sensitivity and specificity for utilization in screening. Nanoparticles can provide signal amplification and physiochemical properties (magnetic, plasmonic, fluorescent and catalytic) which can be exploited to enhance current diagnostic tools or create more suitable methods. A recent breakthrough is the development of a protease-activated magnetic nano-sensor (PAC-MANN).93 Designed to measure protease activity by monitoring the cleavage of peptides on nano-sensors. Each nano-sensor is functionalized with short peptide probes labeled with a fluorescent molecule and any change in fluorescence by protease-mediated cleavage is measured by a detector. PAC-MANN successfully identified PC at all stages with 98% specificity and 73% sensitivity in a blind trial, distinguishing 100% of non-cancer patients. When combined with CA19-9, stage one detection PC identified with 85% sensitivity and 96% specificity, a significant increase in sensitivity to CA 19–9 alone (62%).
When nanoparticles interact with a biological environment, a protein corona is formed.94 This alters the nanoparticles’ properties and influences how the body interacts with them. In a small pilot study, plasma from PC and non-cancerous patients were mixed with liposomes and analyzed by particle size and surface charge measurement. Results demonstrated that particle size and surface charge were different from the two groups, suggesting different proteins were interacting with the nanoparticle. However, no proteomics-based mass spectrometry was conducted and therefore could not pinpoint what the proteins were. Other sources have studied different nanoparticles, observing similar effects. A recent study incubated 106 samples (PC and control) with the nanosheets and then combined with CA19-9.95 There was a significant improvement in distinguishing PC samples from non-cancerous with up to 92% accuracy and boosted PC classification by 50% relative to using CA19-9 alone. In another study, using graphene oxide consisting of 50 samples (PC and control) incubated with plasma. Additionally, a double-blind trial was performed on an independent set (10 cancer and 10 control) with sensitivity ~92% and in the independent trial, strong discrimination was replicated.96
Gold nanopartices (AuNP) possess unique optical properties due to their nano-size, whereby they experience a strong surface plasmon resonance when irradiated with light at resonant wavelengths. They can be fabricated to form particles of various architectures (sphere, shell, rod, star) and sizes, each with unique and exploitable optical properties. Gold nanoparticles can be used as contrast agents for MRI and CT scans. Here, the AuNPs accumulate at the tumor site, and illuminate the scan in this accumulation region, helping clinicians diagnose the presence of cancer. Sobol et al attached a 5B1 targeting antibody, onto the surface of AuNPs, before radiolabeling the particles with88 Zr.97 The particles were administered to a CA19.9-positive BxPC-3 orthotopic tumor model in mice. The mice had been pre-treated with clodronate liposomes for PET imaging and biodistribution studies. Their study showed that the functionalised particles increased targeted delivery to CA19.9-positive pancreatic tumors. The combination of clodronate liposomes and a functionalised AuNPs allowed for PET/CT imaging of the orthotopic xenografts, giving better resolution and tumor information.
Using another powerful imaging tool, work has been carried out investigating the use of gold nanoparticles coated PEG and functionalised with F19 monoclonal antibodies, which have been shown to be effective as labelling agents in human PC tissues using darkfield microscopy.98 The nanoparticles were incubated with tumor stroma sections of resected human pancreatic adenocarcinoma before imaging with a darkfield microscope. The study showed that these particles could be used as a novel labeling method could provide future biopsy diagnosis of PC.
AuNPs are also utilised as signal enhancers in surface-enhanced Raman spectroscopy (SERs). Here the light used for the spectroscopic technique can be scattered more effectively from the surface of particulates with a rough surface and optical properties such as gold nanoparticles. These are often exploited in lateral flow or immunoassays. A study has shown the promise of this combination in an immunoassay for PC.99 Here gold colloids were surface decorated with a Raman reporter and an anti-MUC4 monoclonal antibody (8G7). The SERS platform was used for detecting cancer biomarkers in a sandwich format, using the same antibody for capture and detection and the analyte was cell lysate from MUC4-expressing PC cells. The study demonstrated that the assay could distinguish between PC cells and non-PC cells, and that it demonstrated superior performance to other existing assays, being able to detect and quantify levels of MUC4 in individual serum samples. It is hoped that this may lead to advances in screening of identified patients at risk. Other nanoparticle platforms being investigated for PC detection include iron oxide based magnetic nanoparticles, and quantum dots.100–103
More recently, Zhang et al reported a plectin-1-targeted multimodal nanoparticle imaging probe for detecting PDAC in orthotopic mice.104 A superparamagnetic iron oxide-based probe, labeled with a targeting peptide and near-infrared dye, IRDye800CW, enabled fluorescence molecular imaging, magnetic particle imaging and MRI. Compared to non-targeted controls, it showed higher tumor accumulation and clearer tumor delineation, demonstrating its potential use in improving specificity and precision of PDAC diagnostic imaging. Similarly, by the same group, developed a fibronectin-targeting dual-modality contrast agent for MRI and near-infrared fluorescence imaging of PDAC.105 In mouse models, the agent provided enhanced tumor contrast at half the clinical gadolinium dose with imaging signals correlating with chemotherapy-induced TME changes, enabling for non-invasive diagnosis and treatment monitoring.
Theranostic Nanotechnology in Pancreatic Cancer
Theranostics are platforms consisting of a diagnostic modality as well as a therapeutic one. They allow for rapid treatment after diagnosis, which can cut down the current lag time that can be so detrimental to PC patients’ survival chances. Although, currently, there are no clinical trials for these technologies, it is believed that these are the next-generation gold standard for cancer.
The Hoskins lab focuses on the development of iron oxide core-gold shell hybrid nanoparticles and their use as theranostic entities for pancreatic cancer.106–110 Here, iron oxide acts as an MRI contrast agent whilst the gold shell confers biocompatibility and serves as an anchor point for other molecules such as drugs or other biomolecules. Barnett et al demonstrated the MRI contrast ability of these systems, and their acceptability to pancreatic cancer cell lines.111,112 Malekigorji et al immobilized a novel cytotoxic agent based on a bisnaphthalimido spermine molecule, which due to the charges in its polyamine backbone, was capable of electrotstatically attaching onto the particle surface.108 Oluwasanmi et al used a different method for drug conjugation onto the hybrid nanoparticle surface, instead conjugating a maleamide-GEM prodrug onto the gold surface via a thiofuran anchor, forming a Diel-Alder cycloadduct.107 The optical properties of gold allow for it to absorb/scatter light within the biological NIR window with no detriment to tissue. This was exploited by irradiating the nanoparticles with 1064 nm, 10 ns pulsed laser light for 20 seconds, resulting in rapid heat generation, which was exploited as a thermal trigger for drug release. In the Malekigroji study, this temperature resulted in the threshold temperature required to break the electrostatic bonds being exceeded leading to drug release. In PC BxPC-3 xenograft models, this led to significant reduction in tumor volume after intratumoral injection once per week for four weeks.108 Similarly, in the Olumawamni study, the heat generation was sufficient to initiate the retro Diels-Alder reaction, where the anchor furan and maleamide became uncoupled, liberating the prodrug. In the xenograft study, this resulted in a 56% tumor size reduction compared to GEM alone.107 Work is currently underway in this group, to confer active targeting properties and move these studies further towards the clinic.
Qiu et al developed a theranostic nanoparticle-based platform of gold nanocages (AuNCs) modified with hyaluronic acid (HA) and conjugated with an anti-Glypican-1 antibody (anti-GPC1), anti-cancer agent oridonin, contrast agent gadolinium (Gd), and a fluorescent dye Cy7 dye.113 Their platform showed excellent MRI contrast ability as well as fluorescence. The modified AuNCs enhanced apoptosis in PC cells in vitro, whilst showing negligible haemolytic activity. In vivo trials on PC xenograft mice showed that the modified AuNCs were capable of multimodal imaging combined with targeted therapy.
Other theranostics under consideration include the combination of MRI guidance with photodynamic therapy. Khan et al coated gadolinium nanoparticles with gold nanoparticles, stabilised by a lactose-modified chitosan polymer.114 These particles were tested in vitro on MiaPaCa-2 PC cell lines. The particles were stable under physiological conditions, and non-toxic until activated. Once irradiated at 808 nm, the photothermal effect resulted in significant loss in cell viability, indicating their effectiveness as an ablation source. The MRI data showed that the particles were effective as contrast agents in vitro and in vivo. The authors concluded that these particles are suitable for diagnosis and therapy in one single platform.
Barui et al constructed a gadolinium-doped zinc oxide nanoparticle platform which possessed MRI imaging capabilities.115 Onto the surface of these nanocrystals, they adsorbed GEM. Surrounding the drug loaded nanoparticle was a biomimetic layer composed of extracellular vesicles to confer biocompatibility and finally a synthetic targeting peptide was anchored onto the surface (CKAAKN). This drug loaded platform was testing in vitro in both BxPC3 and AsPC-1 PC cells. Up to 90% of the targeted construct was internalized by the cells, showing the effectiveness of the synthetic peptide, the unloaded nanoparticle construct was not toxic to the cells, neither was the GEM treatment alone (30 µg/mL); however, once loaded onto the platform, the cytotoxic effect became evident in both cell lines. The authors concluded that the GEM-loaded nano construct enhanced the drug efficacy, without changing its mechanism of action, by simply trafficking it more effectively into cells.
Harnessing in vivo fluorescent tracking combined with therapeutics, Tao et al fabricated a sequence-activated construct consisting of a diblock pH sensitive copolymer nano carrier, a NIR Förster resonance energy transfer (FRET) donor (AIEgen TCM-DN) with a PDAC targeting peptide (U11) and a FRET acceptor (cyanine).116 This nanotheranostic: TCM-U11&Cy@P possessed dual-channel near-infrared fluorescence outputs which allowed for in vivo tracking. The programmable targeting ability was able to break through the PDAC stroma, entering the tumor, after which in vivo behaviors were monitored via activatable dual-channel near-infrared (NIR) fluorescence, showing enhanced tumor permeability. Once inside the tumor where the microenvironment is more acidic, the block copolymer released their internalized TCM-U11 nanoparticles where they were activated and photodynamic therapy was used to ablate tumors. The 3D tissue culture in Panc-1 tumor spheroids and xenografts in vivo demonstrated that the novel thernaostic platform was successful in tumor targeting and phototoxicity, whilst real-time monitoring was achievable by exploiting the FRET-based dual-channel activatable fluorescence.
Although all these technologies are in pre-clinical stages, more interest is being attracted to this arena, with publications showing promise over a host of theranostic nanoplatforms, where imaging and therapeutic modalities are combined, most recently in the systems demonstrated by Appidi et al and Fukumitsu et al.117,118
Conclusions and Future Prospective
PC remains one of the most formidable challenges in oncology, owing to its complex biology, late diagnosis and limited responsiveness to conventional therapies. Despite significant advances in nanotechnology and the clinical approval of more than 50 nanomedicines across various disease areas, only two have been approved for PC. This highlights evidence of critically low investment in a disease area often described as an unmet cancer need. Compared with other cancers that receive higher levels of funding and commercial interest.
The studies discussed in this review demonstrate that meaningful progress has been achieved through innovative nano-based strategies, including prodrug nanoparticles, combination therapy, radiation enhancers, responsive nanoparticles and using nanoparticles as an enhancement tool for diagnostics. Unfortunately, the pace of advancement has been slow. However, the growing number of preclinical and clinical evidence continues to prove the potential in nanomedicine to address key challenges such as poor drug solubility, poor drug penetration, therapeutic resistance and systemic toxicity.
Looking ahead, continued interdisciplinary collaboration between academic and industry will be critical if any change is to be done. Increased investment and earlier intervention from regulatory agencies may accelerate this process. While significant challenges remain, the ever-expanding knowledge base offers optimism that nanomedicine has more to give for more effective diagnostic and therapeutic options for patients with PC cancer and their families.
Acknowledgment
Figures created using BioRender n.d. Available online: https://app.biorender.com/illustrations/65ff040d4603630b1370a481 (accessed January 2026).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We would like to thank the EPSRC CEDAR Centre for Doctoral Training (EP/Y035593/1) for funding this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–19. doi:10.3322/caac.21834
2. Bizuayehu HM, Ahmed KY, Kibret GD, et al. Global disparities of cancer and its projected burden in 2050. JAMA Network Open. 2024;7(11):e2443198. doi:10.1001/jamanetworkopen.2024.43198
3. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. doi:10.1158/0008-5472.CAN-14-0155
4. McGuigan A, Kelly P, Turkington RC, Jones C, Coleman HG, McCain RS. Pancreatic cancer: a review of clinical diagnosis, epidemiology, treatment and outcomes. World J Gastroenterol. 2018;24(43):4846–4861. doi:10.3748/wjg.v24.i43.4846
5. Kunovsky L, Tesarikova P, Kala Z, et al. The use of biomarkers in early diagnostics of pancreatic cancer. Can J Gastroenterol Hepatol. 2018;2018:1–10. doi:10.1155/2018/5389820
6. Pancreatic cancer statistics - pancreatic cancer UK. Available from: https://www.pancreaticcancer.org.uk/what-we-do/media-centre/pancreatic-cancer-statistics/.
7. Stoop TF, Rompen IF, Ali M, et al. Resectability stages of pancreatic cancer: nationwide reference. BJS. 2025;112(7). doi:10.1093/bjs/znaf120
8. Hayat U, Croce PS, Saadeh A, et al. Current and emerging treatment options for pancreatic cancer: a comprehensive review. J Clin Med. 2025;14(4):1129. doi:10.3390/jcm14041129
9. Mehta M, Bui TA, Yang X, Aksoy Y, Goldys EM, Deng W. Lipid-based nanoparticles for drug/gene delivery: an overview of the production techniques and difficulties encountered in their industrial development. ACS Materials Au. 2023;3(6):600–619. doi:10.1021/acsmaterialsau.3c00032
10. Zhang L, Sanagapalli S, Stoita A. Challenges in diagnosis of pancreatic cancer. World J Gastroenterol. 2018;24(19):2047–2060. doi:10.3748/wjg.v24.i19.2047
11. Dunn M, Dymock L, Hoskins C. Solid lipid nanoparticles in pancreatic cancer treatment. BJC Reports. 2025;3(1):21. doi:10.1038/s44276-025-00130-9
12. Sattar Z, Ali S, Hussain I, Sattar F, Hussain S, Ahmad S. Diagnosis of pancreatic cancer. Theranostic Approach Pancreat Canc. 2019;51–68.
13. Chakkera M, Foote JB, Farran B, Nagaraju GP. Breaking the stromal barrier in pancreatic cancer: advances and challenges. BBA. 2024;1879(1):189065. doi:10.1016/j.bbcan.2023.189065
14. Valkenburg KC, de Groot AE, Pienta KJ. Targeting the tumour stroma to improve cancer therapy. Nat Rev Clin Oncol. 2018;15(6):366–381. doi:10.1038/s41571-018-0007-1
15. Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet. 2020;395(10242):2008–2020. doi:10.1016/S0140-6736(20)30974-0
16. Kolbeinsson HM, Chandana S, Wright GP, Chung M. Pancreatic cancer: a review of current treatment and novel therapies. J Invest Surg. 2023;36(1). doi:10.1080/08941939.2022.2129884
17. Brunner M, Wu Z, Krautz C, Pilarsky C, Grützmann R, Weber GF. Current clinical strategies of pancreatic cancer treatment and open molecular questions. Int J Mol Sci. 2019;20(18):4543. doi:10.3390/ijms20184543
18. Burris HA, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15(6):2403–2413. doi:10.1200/JCO.1997.15.6.2403
19. Koltai T, Reshkin SJ, Carvalho TMA, et al. Resistance to gemcitabine in pancreatic ductal adenocarcinoma: a physiopathologic and pharmacologic review. Cancers. 2022;14(10):2486. doi:10.3390/cancers14102486
20. Geller LT, Barzily-Rokni M, Danino T, et al. Potential role of intratumor bacteria in mediating tumor resistance to the chemotherapeutic drug gemcitabine. Science. 2017;357(6356):1156–1160. doi:10.1126/science.aah5043
21. Chemotherapy for pancreatic cancer | American cancer society. Available from: https://www.cancer.org/cancer/types/pancreatic-cancer/treating/chemotherapy.html.
22. Drugs approved for pancreatic cancer - NCI. Available from: https://www.cancer.gov/about-cancer/treatment/drugs/pancreatic.
23. Henry DH, Viswanathan HN, Elkin EP, Traina S, Wade S, Cella D. Symptoms and treatment burden associated with cancer treatment: results from a cross-sectional national survey in the U.S. Support Care Cancer. 2008;16(7):791–801. doi:10.1007/s00520-007-0380-2
24. Amrutkar M, Gladhaug IP. Pancreatic cancer chemoresistance to gemcitabine. Cancers. 2017;9(11):157. doi:10.3390/cancers9110157
25. Farhangnia P, Khorramdelazad H, Nickho H, Delbandi AA. Current and future immunotherapeutic approaches in pancreatic cancer treatment. J Hematol Oncol. 2024;17(1):40. doi:10.1186/s13045-024-01561-6
26. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non–small-cell lung cancer with PD-L1 tumor proportion Score ≥ 50%. J Clin Oncol. 2021;39(21):2339–2349. doi:10.1200/JCO.21.00174
27. Macioch T, Krzakowski M, Gołębiewska K, Dobek M, Warchałowska N, Niewada M. Pembrolizumab monotherapy survival benefits in metastatic non-small-cell lung cancer: a systematic review of real-world data. Discover Oncology. 2024;15(1):303. doi:10.1007/s12672-024-01153-3
28. Knight A, Karapetyan L, Kirkwood JM. Immunotherapy in melanoma: recent advances and future directions. Cancers. 2023;15(4):1106. doi:10.3390/cancers15041106
29. Vassilakopoulos TP, Chatzidimitriou C, Asimakopoulos JV, et al. Immunotherapy in hodgkin lymphoma: present status and future strategies. Cancers. 2019;11(8):1071. doi:10.3390/cancers11081071
30. Yoon JH, Jung YJ, Moon SH. Immunotherapy for pancreatic cancer. World J Clin Cases. 2021;9(13):2969–2982. doi:10.12998/wjcc.v9.i13.2969
31. Ye X, Yu Y, Zheng X, Ma H. Clinical immunotherapy in pancreatic cancer. Cancer Immunol Immunother. 2024;73(4):64. doi:10.1007/s00262-024-03632-6
32. Ejlsmark MW, Schytte T, Bernchou U, et al. Radiotherapy for locally advanced pancreatic adenocarcinoma-a critical review of randomised trials. Curr Oncol. 2023;30(7):6820–6837. doi:10.3390/curroncol30070499
33. Burkoň P, Trna J, Slávik M, et al. Stereotactic Body Radiotherapy (SBRT) of pancreatic cancer-a critical review and practical consideration. Biomedicines. 2022;10(10):2480. doi:10.3390/biomedicines10102480
34. Falco M, Masojć B, Sulikowski T. Radiotherapy in pancreatic cancer: to whom, when, and how? Cancers. 2023;15(13):3382. doi:10.3390/cancers15133382
35. Wang J, Gai J, Zhang T, et al. Neoadjuvant radioimmunotherapy in pancreatic cancer enhances effector T cell infiltration and shortens their distances to tumor cells. Sci Adv. 2024;10(6):1827. doi:10.1126/sciadv.adk1827
36. Cancer. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
37. Wu J. The Enhanced Permeability and Retention (EPR) effect: the significance of the concept and methods to enhance its application. J Pers Med. 2021;11(8):771. doi:10.3390/jpm11080771
38. Hong L, Li W, Li Y, Yin S. Nanoparticle-based drug delivery systems targeting cancer cell surfaces. RSC Adv. 2023;13(31):21365–21382. doi:10.1039/D3RA02969G
39. Chang D, Gao Y, Wang L, et al. Polydopamine-based surface modification of mesoporous silica nanoparticles as pH-sensitive drug delivery vehicles for cancer therapy. J Colloid Interface Sci. 2016;463:279–287. doi:10.1016/j.jcis.2015.11.001
40. Joudeh N, Linke D, Zhang T. Nanoparticle classification, physicochemical properties, characterization, and applications: a comprehensive review for biologists. J Nanobiotechnology. 2022;20(1):1–29. doi:10.1186/s12951-021-01184-w
41. Bulbake U, Doppalapudi S, Kommineni N, Khan W. Liposomal formulations in clinical use: an updated review. Pharmaceutics. 2017;9(2):12. doi:10.3390/pharmaceutics9020012
42. Wu Y, Yu S, de Lázaro I. Advances in lipid nanoparticle mRNA therapeutics beyond COVID-19 vaccines. Nanoscale. 2024;16(14):6820–6836. doi:10.1039/D4NR00019F
43. Weber JS, Carlino MS, Khattak A, et al. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, Phase 2b study. Lancet. 2024;403(10427):632–644. doi:10.1016/S0140-6736(23)02268-7
44. Kon E, Ad-El N, Hazan-Halevy I, Stotsky-Oterin L, Peer D. Targeting cancer with mRNA–lipid nanoparticles: key considerations and future prospects. Nat Rev Clin Oncol. 2023;20(11):739–754. doi:10.1038/s41571-023-00811-9
45. Păduraru DN, Ion D, Niculescu AG, et al. Recent developments in metallic nanomaterials for cancer therapy, diagnosing and imaging applications. Pharmaceutics. 2022;14(2):435. doi:10.3390/pharmaceutics14020435
46. Roshani M, Rezaian-Isfahni A, Lotfalizadeh MH, Khassafi N, Abadi MHJN, Nejati M. Metal nanoparticles as a potential technique for the diagnosis and treatment of gastrointestinal cancer: a comprehensive review. Cancer Cell Int. 2023;23(1). doi:10.1186/s12935-023-03115-1
47. Saadh MJ, Khidr WA, Alfarttoosi KH, et al. Metal nanoparticles as a promising therapeutic approach for prostate cancer diagnosis and therapy: a comprehensive review. Med Oncol. 2025;42(4). doi:10.1007/s12032-025-02633-4
48. Hassanin I, Elzoghby A. Albumin-based nanoparticles: a promising strategy to overcome cancer drug resistance. Cancer Drug Resist. 2020;3(4):930. doi:10.20517/cdr.2020.68
49. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
50. Goldstein D, El-Maraghi RH, Hammel P, et al. Nab-paclitaxel plus gemcitabine for metastatic pancreatic cancer: long-term survival from a phase III trial. J Natl Cancer Inst. 2015;107(2):dju413–dju413. doi:10.1093/jnci/dju413
51. Wang-Gillam A, Hubner RA, Siveke JT, et al. NAPOLI-1 Phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: final overall survival analysis and characteristics of long-term survivors. Eur J Cancer. 2019;108:78–87. doi:10.1016/j.ejca.2018.12.007
52. Wainberg ZA, Melisi D, Macarulla T, et al. NAPOLI-3: a randomized, open-label phase 3 study of liposomal irinotecan + 5-fluorouracil/leucovorin + oxaliplatin (NALIRIFOX) versus nab-paclitaxel + gemcitabine in treatment-naïve patients with metastatic pancreatic ductal adenocarcinoma (mPDAC). J clin oncol. 2023;41(4_suppl):LBA661–LBA661. doi:10.1200/JCO.2023.41.4_suppl.LBA661
53. Milano G, Innocenti F, Minami H. Liposomal irinotecan (Onivyde): exemplifying the benefits of nanotherapeutic drugs. Cancer Sci. 2022;113(7):2224. doi:10.1111/cas.15377
54. Researcher view | BMS-813160 with nivolumab and gemcitabine and nab-paclitaxel in borderline resectable and locally advanced Pancreatic Ductal Adenocarcinoma (PDAC) | Clinicaltrials.gov. Available from: https://clinicaltrials.gov/study/NCT03496662?cond=PDAC%20-%20Pancreatic%20Ductal%20Adenocarcinoma%20&term=Pancreatic%20Cancer&intr=Nab-Paclitaxel&rank=9&tab=table.
55. Grierson PM, Wolf C, Suresh R, et al. Neoadjuvant BMS-813160, nivolumab, gemcitabine, and nab-paclitaxel for patients with pancreatic cancer. Clin Cancer Res. 2025;31(17):3644–3651. doi:10.1158/1078-0432.CCR-24-1821
56. Study details | trial to investigate intensified neoadjuvant chemotherapy in locally advanced pancreatic cancer | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT02125136.
57. Kunzmann V, Siveke JT, Algül H, et al. Nab-paclitaxel plus gemcitabine versus nab-paclitaxel plus gemcitabine followed by FOLFIRINOX induction chemotherapy in locally advanced pancreatic cancer (NEOLAP-AIO-PAK-0113): a multicentre, randomised, phase 2 trial. Lancet Gastroenterol Hepatol. 2021;6(2):128–138. doi:10.1016/S2468-1253(20)30330-7
58. Study details | a study of botensilimab in participants with metastatic pancreatic cancer | clinicaltrials.gov. Available from: https://clinicaltrials.gov/study/NCT05630183?cond=PDAC%20-%20Pancreatic%20Ductal%20Adenocarcinoma&term=Pancreatic%20Cancer&intr=Nab-Paclitaxel&page=4&rank=33.
59. Study details | a study of CEND-1 with chemotherapy as first-line therapy in patients with pancreatic ductal adenocarcinoma | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT06261359?cond=PDAC%20-%20Pancreatic%20Ductal%20Adenocarcinoma&term=Pancreatic%20Cancer&intr=Nab-Paclitaxel&rank=6.
60. Study details | surufatinib combined with gemcitabine plus nab-paclitaxel in locally advanced pancreatic cancer | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT06361030?cond=PDAC%20-%20Pancreatic%20Ductal%20Adenocarcinoma&term=Pancreatic%20Cancer&intr=Nab-Paclitaxel&page=2&rank=18.
61. Study details | NCT06467565 | NALIRIFOX as induction therapy in LAPC | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT06467565.
62. Study Details | NCT04662112 | liposomal irinotecan, S-1, and oxaliplatin in advanced pancreatic adenocarcinoma | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04662112?cond=PDAC%20-%20Pancreatic%20Ductal%20Adenocarcinoma&term=Pancreatic%20Cancer&intr=Nanoliposomal%20Irinotecan&page=2&rank=11.
63. Jeong H, Kim BJ, Lee CK, et al. Liposomal irinotecan, oxaliplatin, and S-1 as first-line therapy for patients with locally advanced or metastatic pancreatic adenocarcinoma (NASOX): a multicenter phase I/IIa study. Eur J Cancer. 2024;208.
64. Study details | NCT06821997 | NALIRIFOX before surgery for the treatment of borderline resectable pancreatic ductal adenocarcinoma, nectar trial | clinicalTrials.gov. Available from: https://www.clinicaltrials.gov/study/NCT06821997?term=AREA%5BInterventionSearch%5D(SUCROSOFATE)%20AND%20AREA%5BStudyType%5D(INTERVENTIONAL)&rank=5.
65. Study details | NCT04752696 | onvansertib in combination with nanoliposomal irinotecan, leucovorin, and fluorouracil for second-line treatment of participants with metastatic pancreatic ductal adenocarcinoma | clinicalTrials.gov. Available from: https://www.clinicaltrials.gov/study/NCT04752696?term=AREA%5BBasicSearch%5D(AREA%5BSponsorSearch%5D(COVERAGE%5BFullMatch%5DEXPANSION%5BNone%5D(%22Cardiff%20Oncology%22)))&rank=3.
66. Study details | NCT04484909 | NBTXR3 activated by radiation therapy for the treatment of locally advanced or borderline-resectable pancreatic Cancer | clinicalTrials.gov. Available from: https://www.clinicaltrials.gov/study/NCT04484909?term=HAFNIUM&rank=3.
67. Bagley AF, Ludmir EB, Maitra A, et al. NBTXR3, a first-in-class radioenhancer for pancreatic ductal adenocarcinoma: report of first patient experience. Clin Transl Radiat Oncol. 2022;33:66–69. doi:10.1016/j.ctro.2021.12.012
68. Rojas LA, Sethna Z, Soares KC, et al. Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer. Nature. 2023;618(7963):144–150. doi:10.1038/s41586-023-06063-y
69. Study details | NCT04161755 | study of Personalized Tumor Vaccines (PCVs) and a PD-L1 blocker in patients with pancreatic cancer that can be treated with surgery | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT04161755.
70. Zhu Q, Yu C, Chen Y, et al. Dual mRNA nanoparticles strategy for enhanced pancreatic cancer treatment and β-elemene combination therapy. Proc Natl Acad Sci. 2025;122(11):e2418306122. doi:10.1073/pnas.2418306122
71. Prabhuraj RS, Mal A, Valvi SK, Srivastava R, De A, Bandyopadhyaya R. Noninvasive preclinical evaluation of targeted nanoparticles for the delivery of curcumin in treating pancreatic cancer. ACS Appl Bio Mater. 2020;3(7):4643–4654. doi:10.1021/acsabm.0c00515
72. Huang S, Huang X, Yan H. Peptide dendrimers as potentiators of conventional chemotherapy in the treatment of pancreatic cancer in a mouse model. Eur J Pharm Biopharm. 2022;170:121–132. doi:10.1016/j.ejpb.2021.11.005
73. Chibaya L, DeMarco KD, Lusi CF, et al. Nanoparticle delivery of innate immune agonists combined with senescence-inducing agents promotes T cell control of pancreatic cancer. Sci Transl Med. 2024;16(762). doi:10.1126/scitranslmed.adj9366
74. Delkhah AMD, Karimi E, Farivar S. Herniarin-loaded solid lipid nanoparticles: promising molecular mechanism and therapeutic potential against pancreatic cancer line. Mol Biol Rep. 2023;50(8):6469–6479. doi:10.1007/s11033-023-08560-9
75. Liu X, Jiang J, Chang CH, et al. Development of facile and versatile platinum drug delivering silicasome nanocarriers for efficient pancreatic cancer chemo-immunotherapy. Small. 2021;17(14).
76. Quiñonero F, Parra-Torrejón B, Ramírez-Rodríguez GB, et al. Combining olaparib and ascorbic acid on nanoparticles to enhance the drug toxic effects in pancreatic cancer. Int J Nanomed. 2023;18:5075–5093. doi:10.2147/IJN.S415631
77. Alhussan A, Jackson N, Chow N, et al. In vitro and in vivo synergetic radiotherapy with gold nanoparticles and docetaxel for pancreatic cancer. Pharmaceutics. 2024;16(6):713. doi:10.3390/pharmaceutics16060713
78. Ochioni AC, Vieira IRS, Conte-Junior CA. Advances in stimuli-responsive nanoparticles for cancer therapy: mechanisms, functional materials, and emerging technologies. J Drug Deliv Sci Technol. 2025;114:107519. doi:10.1016/j.jddst.2025.107519
79. Gao J, Nesbitt H, Logan K, et al. An ultrasound responsive microbubble-liposome conjugate for targeted irinotecan-oxaliplatin treatment of pancreatic cancer. Eur J Pharm Biopharm. 2020;157:233–240. doi:10.1016/j.ejpb.2020.10.012
80. Shi X, Li Q, Zhang C, et al. Semiconducting polymer nano-radiopharmaceutical for combined radio-photothermal therapy of pancreatic tumor. J Nanobiotechnology. 2021;19(1):1–12. doi:10.1186/s12951-021-01083-0
81. Slapak EJ, El Mandili M, Brink MST, Kros A, Bijlsma MF, Spek CA. Preclinical assessment of ADAM9-Responsive mesoporous silica nanoparticles for the treatment of pancreatic cancer. Int J Mol Sci. 2023;24(13):10704. doi:10.3390/ijms241310704
82. Bianchi L, Baroni S, Paroni G, et al. Thermal effects and biological response of breast and pancreatic cancer cells undergoing gold nanorod-assisted photothermal therapy. J Photochem Photobiol B. 2024;259:112993. doi:10.1016/j.jphotobiol.2024.112993
83. Nedelcu A, Mocan T, Sabau LI, et al. In vitro photothermal therapy of pancreatic cancer mediated by immunoglobulin G-functionalized silver nanoparticles. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-63142-4
84. Xin X, Lin F, Wang Q, Yin L, Mahato RI. ROS-Responsive polymeric micelles for triggered simultaneous delivery of PLK1 inhibitor/miR-34a and effective synergistic therapy in pancreatic cancer. ACS Appl Mater Interfaces. 2019;11(16):14647. doi:10.1021/acsami.9b02756
85. Díaz-Riascos ZV, Llaguno-Munive M, Lafuente-Gómez N, et al. Preclinical development of magnetic nanoparticles for hyperthermia treatment of pancreatic cancer. ACS Appl Mater Interfaces. 2025;17(2):2924–2939. doi:10.1021/acsami.4c16129
86. Li MM, Zhang Y, Sun F, et al. Photodynamic therapy using RGD-Functionalized quantum dots elicit a potent immune response in a syngeneic mouse model of pancreatic cancer. Int J Nanomed. 2024;19:9487–9502. doi:10.2147/IJN.S479123
87. Cho IK, Shim MK, Um W, Kim JH, Kim K. Light-Activated monomethyl auristatin e prodrug nanoparticles for combinational photo-chemotherapy of pancreatic cancer. Molecules. 2022;27(8):2529. doi:10.3390/molecules27082529
88. Park J, Park SS, Lee KJ, et al. Docetaxel-polymeric nanoparticle enhances radiotherapeutic efficacy in human pancreatic cancer. Transl Cancer Res. 2018;7(1):60–67. doi:10.21037/tcr.2018.01.09
89. Wiedenmann N, Valdecanas D, Hunter N, et al. 130-nm Albumin–Bound paclitaxel enhances tumor radiocurability and therapeutic gain. Clin Cancer Res. 2007;13(6):1868–1874. doi:10.1158/1078-0432.CCR-06-2534
90. Aliru ML, Aziz K, Bodd M, et al. Targeted gold nanoparticles enhance radiation effects in pancreatic tumor models. Int J Radiat Oncol Biol Phys. 2017;99(2):E574–E575. doi:10.1016/j.ijrobp.2017.06.1983
91. Detappe A, Kunjachan S, Rottmann J, et al. AGuIX nanoparticles as a promising platform for image-guided radiation therapy. Cancer Nanotechnol. 2015;6(1):4. doi:10.1186/s12645-015-0012-3
92. Zhang P, Marill J, Darmon A, Anesary NM, Lu B, Paris S. NBTXR3 Radiotherapy-activated functionalized hafnium oxide nanoparticles show efficient antitumor effects across a large panel of human cancer models. Int J Nanomed. 2021;16:2761. doi:10.2147/IJN.S301182
93. Montoya Mira JL, Quentel A, Patel RK, et al. Early detection of pancreatic cancer by a high-throughput protease-activated nanosensor assay. Sci Transl Med. 2025;17(785). doi:10.1126/scitranslmed.adq3110
94. Caputo D, Pozzi D, Farolfi T, Passa R, Coppola R, Caracciolo G. Nanotechnology and pancreatic cancer management: state of the art and further perspectives. World J Gastrointest Oncol. 2021;13(4):231. doi:10.4251/wjgo.v13.i4.231
95. Digiacomo L, Caputo D, Cammarata R, et al. Nanoparticle-protein Corona enhances accuracy of Ca-19.9-based pancreatic cancer classification. Nanoscale. 2025;17(12):7066–7075. doi:10.1039/D4NR02435D
96. Papi M, Palmieri V, Digiacomo L, et al. Converting the personalized biomolecular Corona of graphene oxide nanoflakes into a high-throughput diagnostic test for early cancer detection. Nanoscale. 2019;11(32):15339–15346. doi:10.1039/C9NR01413F
97. Sobol NB, Korsen JA, Younes A, Edwards KJ, Lewis JS. ImmunoPET imaging of pancreatic tumors with 89Zr-Labeled gold nanoparticle-antibody conjugates. Mol Imaging Biol. 2021;23(1):84–94. doi:10.1007/s11307-020-01535-3
98. Eck W, Craig G, Sigdel A, et al. PEGylated gold nanoparticles conjugated to monoclonal F19 antibodies as targeted labeling agents for human pancreatic carcinoma tissue. ACS Nano. 2008;2(11):2263–2272. doi:10.1021/nn800429d
99. Krasnoslobodtsev AV, Torres MP, Kaur S, et al. Nano-immunoassay with improved performance for detection of cancer biomarkers. Nanomedicine. 2015;11(1):167–173. doi:10.1016/j.nano.2014.08.012
100. Kalubowilage M, Covarrubias-Zambrano O, Malalasekera AP, et al. Early detection of pancreatic cancers in liquid biopsies by ultrasensitive fluorescence nanobiosensors. Nanomedicine. 2018;14(6):1823–1832. doi:10.1016/j.nano.2018.04.020
101. Luo Y, Li Y, Li J, Fu C, Yu X, Wu L. Hyaluronic acid-mediated multifunctional iron oxide-based MRI nanoprobes for dynamic monitoring of pancreatic cancer. RSC Adv. 2019;9(19):10486–10493. doi:10.1039/C9RA00730J
102. Oliveira D, Oliveira P, Xu A, et al. Optical immunosensor panel using quantum dot-antibody conjugates for highly sensitive detection of carbohydrate antigen 19–9 (CA19-9). Anal Chim Acta. 2025;1333:343399. doi:10.1016/j.aca.2024.343399
103. Yong KT. Biophotonics and biotechnology in pancreatic cancer: cyclic RGD-Peptide-conjugated type II quantum dots for in vivo imaging. Pancreatology. 2010;10(5):553–564. doi:10.1159/000283577
104. Zhang W, Liang X, Zhu L, et al. Optical magnetic multimodality imaging of plectin-1-targeted imaging agent for the precise detection of orthotopic pancreatic ductal adenocarcinoma in mice. EBioMedicine. 2022;80.
105. Zhang W, Liang X, Zhang X, et al. Magnetic-optical dual-modality imaging monitoring chemotherapy efficacy of pancreatic ductal adenocarcinoma with a low-dose fibronectin-targeting Gd-based contrast agent. Eur J Nucl Med Mol Imaging. 2024;51(7):1841–1855. doi:10.1007/s00259-024-06617-w
106. Oluwasanmi A, Lindsay S, Curtis A, Perrie Y, Hoskins C. Chain length impact on the retro diels-alder mediated release of gemcitabine from hybrid nanoparticles towards pancreatic cancer therapy. Int J Pharm. 2023;644:123304. doi:10.1016/j.ijpharm.2023.123304
107. Oluwasanmi A, Al-Shakarchi W, Manzur A, et al. Diels alder-mediated release of gemcitabine from hybrid nanoparticles for enhanced pancreatic cancer therapy. J Control Release. 2017;266:355–364. doi:10.1016/j.jconrel.2017.09.027
108. Malekigorji M, Alfahad M, Kong Thoo Lin P, Jones S, Curtis A, Hoskins C. Thermally triggered theranostics for pancreatic cancer therapy. Nanoscale. 2017;9(34):12735–12745. doi:10.1039/C7NR02751F
109. Oluwasanmi A, Malekigorji M, Jones S, Curtis A, Hoskins C. Potential of hybrid iron oxide-gold nanoparticles as thermal triggers for pancreatic cancer therapy. RSC Advances. 2016;6:95044.
110. Curtis A, Malekigorji M, Holman J, Skidmore M, Hoskins C. Heat dissipation of hybrid iron oxide-gold nanoparticles in an agar phantom. J Nanomed Nanotechnol. 2015;6(6):335. doi:10.4172/2157-7439.1000335
111. Barnett CM, Gueorguieva M, Lees MR, McGarvey DJ, Darton RJ, Hoskins C. Effect of the hybrid composition on the physicochemical properties and morphology of iron oxide–gold nanoparticles. J Nanopart Res. 2012;14(10):1–12. doi:10.1007/s11051-012-1170-4
112. Barnett CM, Gueorguieva M, Lees MR, McGarvey DJ, Hoskins C. Physical stability, biocompatibility and potential use of hybrid iron oxide-gold nanoparticles as drug carriers. J Nanopart Res. 2013;15(6):1–14. doi:10.1007/s11051-013-1706-2
113. Qiu W, Chen R, Chen X, et al. Oridonin-loaded and GPC1-targeted gold nanoparticles for multimodal imaging and therapy in pancreatic cancer. Int J Nanomed. 2018;13:6809–6827. doi:10.2147/IJN.S177993
114. Khan M, Liu H, Sacco P, et al. DOTAREM (DOTA)-Gold-Nanoparticles: design, spectroscopic evaluation to build hybrid contrast agents to applications in nanomedecine. Int J Nanomed. 2022;17:4105–4118. doi:10.2147/IJN.S368458
115. Barui S, Percivalle NM, Conte M, et al. Development of doped ZnO-based biomimicking and tumor-targeted nanotheranostics to improve pancreatic cancer treatment. Cancer Nanotechnol. 2022;13(1):1–24. doi:10.1186/s12645-022-00140-z
116. Tao Y, Yan C, Li D, et al. Sequence-activated fluorescent nanotheranostics for real-time profiling pancreatic cancer. JACS Au. 2022;2(1):246–257. doi:10.1021/jacsau.1c00553
117. Fukumitsu N, Matsumoto Y, Chen L, et al. Development of Layer-by-Layer magnetic nanoparticles for application to radiotherapy of pancreatic cancer. Molecules. 2025;30(6):1382. doi:10.3390/molecules30061382
118. Appidi T, China D, Ștefan GR, et al. Engineered multifunctional nanoparticles for enhanced radiation therapy: three-in-one approach for cancer treatment. Mol Cancer. 2025;24(1):68. doi:10.1186/s12943-025-02266-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.