Back to Journals » Drug Design, Development and Therapy » Volume 20
Development, Characterization, and Clinical Evaluation of a 6% Nitroglycerin–Aloe Vera Transdermal Gel for Stable Angina Management
Authors Iqbal MO ![]() , Bhutta KKA, Khan IA
, Bhutta KKA, Khan IA ![]() , Rehman IU, Khan MK, Gu Y, Chen J, Wu X
, Rehman IU, Khan MK, Gu Y, Chen J, Wu X
Received 18 July 2025
Accepted for publication 28 November 2025
Published 8 January 2026 Volume 2026:20 554673
DOI https://doi.org/10.2147/DDDT.S554673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Muhammad Omer Iqbal,1,2 Kashaf Khan Anjum Bhutta,2 Imran Ahmad Khan,3 Inam Ur Rehman,4 Maliha Khalid Khan,2 Yuchao Gu,1 Jin Chen,1 Xiao Wu5
1College of Marine Science and Biological Engineering, Qingdao University of Science and Technology, Qingdao, Shandong, 266042, People’s Republic of China; 2Ali-Ul-Murtaza, Department of Rehabilitation Sciences, Muhammad Institute of Medical and Allied Sciences, Multan, Punjab, 60000, Pakistan; 3Department of Pharmacy, MNS University of Agriculture, Multan, Punjab, 60000, Pakistan; 4Department of Intensive Care Unit, CPE Institute of Cardiology, Multan, Punjab, 60000, Pakistan; 5Qingdao Central Hospital, University of Health and Rehabilitation Sciences (Qingdao Central Medical Group), Qingdao, Shandong, 266042, People’s Republic of China
Correspondence: Imran Ahmad Khan, Email [email protected] Xiao Wu, Email [email protected]
Purpose: This study aimed to develop, characterize, and clinically evaluate a novel 6% nitroglycerin (NTG) Aloe vera gel formulation as a transdermal alternative to conventional sublingual NTG therapy in patients with stable angina pectoris.
Patients and Methods: A randomized, parallel-group, double-blind clinical trial was conducted involving 150 patients with stable angina, allocated to receive either 6% NTG-Aloe vera gel or standard sublingual NTG tablets (0.6mg). The gel was assessed for physicochemical parameters, FTIR compatibility, stability under ICH guidelines, and in vitro drug release kinetics. Dermatological safety was evaluated via skin irritation testing. Clinical efficacy was determined by Numeric Pain Rating Scale (NPRS), chest tightness scores, Seattle Angina Questionnaire (SAQ), and vital parameters, including blood pressure and oxygen saturation.
Results: The NTG Aloe vera gel demonstrated desirable physicochemical properties, sustained zero-order drug release, and excellent stability with no significant degradation. Clinical data revealed that the gel provided gradual, sustained pain and chest tightness relief, superior SAQ scores (p< 0.001), and improved tolerability compared to sublingual NTG. Importantly, the gel induced a controlled hypotensive response without abrupt cardiovascular changes, indicating enhanced safety. No dermatological adverse effects were reported.
Conclusion: This pilot study showed 6% NTG-Aloe vera gel offers a stable, effective, and patient-friendly transdermal delivery system for angina management, meriting further large-scale and long-term evaluations.
Registration: Clinical Trial Registry-India (CTRI/2024/11/076947).
Keywords: nitroglycerin, aloe vera, angina pectoris, transdermal drug delivery systems, pharmaceutical preparations
Introduction
Angina pectoris, commonly referred to as angina, is a hallmark symptom of coronary artery disease CAD and is characterized by chest discomfort or pain resulting from transient myocardial ischemia.1 The condition arises when there is an imbalance between myocardial oxygen supply and demand, often due to impaired coronary blood flow.2 Angina remains a significant global health concern due to its impact on the quality of life and its association with increased risks of myocardial infarction and other adverse cardiovascular events.3 Pharmacological management of angina aims to alleviate symptoms and prevent further complications, with nitroglycerin (NTG) being one of the most widely used agents in clinical practice.
NTG, a nitrate-based vasodilator, works by releasing nitric oxide (NO), which activates the guanylyl cyclase-cyclic GMP pathway in vascular smooth muscle cells, leading to muscle relaxation and vasodilation.4 This results in decreased preload and afterload, reduced myocardial oxygen demand, and improved coronary blood flow.5 Sublingual tablets (0.6mg) are one of the most common dosage forms for nitroglycerin due to their rapid onset of action, which is essential for the immediate relief of angina episodes.6 Despite their widespread use, sublingual tablets have limitations, including a short duration of effect, poor stability due to environmental factors, and significant variability in absorption depending on the mucosal conditions. Additionally, frequent dosing to manage recurrent anginal episodes can lead to challenges in patient compliance and potential development of tolerance.7
To overcome the limitations associated with sublingual NTG tablets, transdermal delivery systems have gained increasing attention. Transdermal formulations offer several advantages, such as bypassing the gastrointestinal tract, avoiding first-pass metabolism, and providing controlled and sustained drug release.8 These attributes make transdermal delivery particularly suitable for chronic conditions like angina, where consistent therapeutic levels of the drug are beneficial. Among the various transdermal options, gels are particularly appealing due to their ease of application, patient acceptability, and capacity for flexible dosing. They allow for direct skin absorption of the active ingredient, minimizing systemic fluctuations and extending the therapeutic window.9 Aloe vera, a naturally derived biopolymer, has shown great promise as a base for transdermal gels due to its bioactive properties. Known for its moisturizing, anti-inflammatory, and skin-conditioning effects, aloe vera is widely used in dermatological preparations.10 Additionally, its natural polysaccharides and enzymes enhance skin penetration and improve the bioavailability of transdermally delivered drugs. Incorporating aloe vera into a nitroglycerin gel formulation offers the potential to enhance drug permeation, reduce skin irritation, and improve patient comfort, further optimizing the therapeutic outcomes.11
This research focuses on the formulation and evaluation of a NTG 6% Aloe vera based transdermal gel as an alternative to conventional sublingual nitroglycerin tablets. The study explores the synergistic potential of aloe vera to enhance the transdermal delivery of nitroglycerin, while simultaneously improving patient adherence and convenience. The gel’s physicochemical properties, stability, drug release profile, and skin permeation potential are rigorously assessed using in vitro and in vivo methods.12 Furthermore, its therapeutic efficacy and patient tolerability are compared with sublingual tablets in terms of angina symptom relief, duration of action, and patient preference. By providing a sustained-release formulation, this aloe vera based transdermal gel has the potential to ad-dress several limitations associated with sublingual administration, including the short duration of action, challenges with adherence, and irritation in frequent use. It is hypothesized that the gel will offer comparable or superior therapeutic benefits while promoting better compliance and comfort for patients.13 This research aims to contribute to the growing field of transdermal drug delivery systems, offering an innovative and practical approach to angina management. Ultimately, it seeks to bridge the gap between rapid onset and sustained therapeutic effects, advancing the standard of care for patients with CAD.
Patients and Methods
Study Design and Ethical Approval
A pragmatic, community-based, parallel-group, single-blinded, randomized controlled clinical trial was conducted to evaluate the efficacy and safety of a novel 6% NTG- Aloe vera gel formulation in prediagnosed patients with stable angina pectoris at Ch. Pervaiz Elahi Institute of Cardiology (A Tertiary care hospital of Government of Punjab). The trial was approved by the Ethics Committees of the Muhammad Institute of Medical and Allied Sciences (MIMAS/08/26/Imran/24) and Ch. Pervaiz Elahi Institute of Cardiology (PC/PEIC/Res/Kashaf/24), Multan, Pakistan. It was registered with the Clinical Trial Registry-India (CTRI/2024/11/076947). The study was conducted from July to November 2024 (preparatory phase) and December 2024 to March 2025 (execution phase) in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants for participation in study and also written informed consent for publication of images was obtained from all individuals shown in Figure 1.
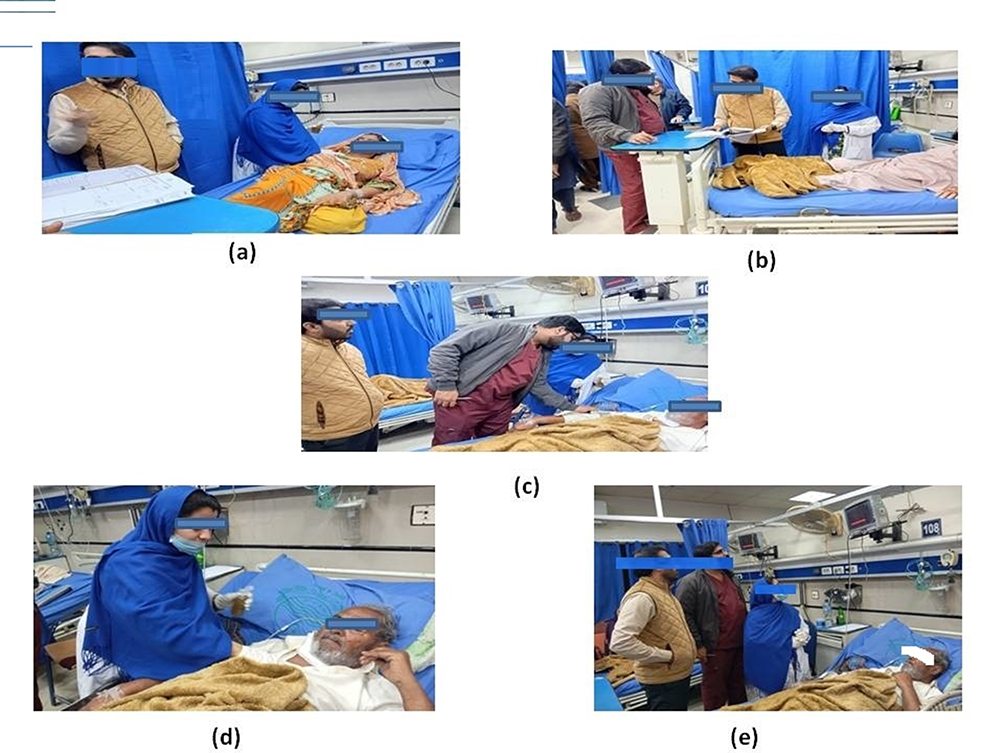 |
Figure 1 Clinical procedures being performed on patients with angina being carried out in the emergency department of CPEIC, Multan, Pakistan. Application of NTG 6% Aloe Vera for therapeutic purposes is being carried out in images (a and d). Monitoring of vital parameters, including patient assessment and evaluation of clinical status, is being conducted in images (b–e). |
Materials
Nitroglycerin (Nitromint, Egis Pharmaceuticals, Hungary) were used as the active pharmaceutical ingredient. Fresh Aloe vera leaves were harvested and processed to obtain 100 g of latex gel. Pharmaceutical-grade excipients including Carbopol 934, triethanolamine, glycerin, methylparaben, and propylparaben were sourced from Loba Chemie. Analytical and HPLC-grade solvents were supplied by HiMedia Laboratories.
Compatibility and Interaction Studies
Fourier Transform Infrared (FTIR) spectroscopy was performed to assess the physicochemical compatibility of NTG with Aloe vera and other excipients. Spectra were recorded in the range of 650–4000 cm−1 and analyzed for peak shifts, appearance, or disappearance of characteristic bands, which may indicate potential interactions.
Formulation of 6% NTG-Aloe Vera Gel
The gel base was prepared by dispersing Carbopol 934 (1% w/v) in deionized water. Preservatives (methylparaben and propylparaben) were dissolved in hot water and mixed with the gel base along with glycerin. Aloe vera extract (10% w/w) was incorporated into the mixture. NTG (6% w/w) was ground to a fine powder, dissolved in ethanol, and added slowly under continuous stirring using a Robinson mixer for 15 minutes. Triethanolamine was added to adjust the pH between 5.5 and 6.5, resulting in a homogeneous gel intended for topical application over the chest or upper arm to relieve angina symptoms via transdermal absorption.
Physicochemical Evaluation
The prepared 6% NTG-Aloe vera gel was subjected to comprehensive physicochemical evaluation to assess its quality and stability. The following parameters were evaluated:
Appearance
The gel was visually examined for color, homogeneity, and texture.14 Homogeneity was checked by uniformly spreading a small amount of gel on a glass slide and observing it under adequate light for the presence of any clumps, particles, or phase separation. The texture was assessed manually to ensure smoothness and uniformity.
pH Determination
The pH of the gel was measured using a calibrated digital pH meter. A 1% w/v dispersion of the gel in distilled water was prepared, and the pH was recorded at room temperature. Calibration of the pH meter was done using standard buffer solutions of pH 4.0 and 7.0 before measurement.15
Viscosity
Viscosity was determined using a Brookfield digital viscometer equipped with spindle no. 64, operated at a speed of 50 rpm at room temperature (25 ± 2 °C)16 . Approximately 50 g of gel sample was taken in a beaker, and the spindle was immersed vertically into the gel. Readings were recorded in centipoise (cP) after the viscometer stabilized.
Spreadability
The spreadability of the gel was evaluated using a modified glass slide method. A known weight (m) was placed on the upper slide, which was allowed to rest over a fixed amount of gel placed between two horizontal glass slides. The time (t) taken for the upper slide to slip off from the lower one over a fixed length (l) was recorded. Spreadability coefficient (S) was calculated using the following formula:

Where m = weight applied, l = slide length, t = time required for the slides to separate.
Specific Gravity
The specific gravity of the gel was determined using a specific gravity bottle (pycnometer) method. The bottle was first weighed empty (W1), then filled with distilled water and weighed (W2), and finally filled with the gel and weighed again (W3). Specific gravity was calculated using the following formula:

Where W1 = Weight of empty bottle; W2 = Weight of bottle filled with distilled water; W3 = Weight of bottle filled with gel.
Drug Content and Release Studies
One gram of gel was accurately weighed and dissolved in phosphate-buffered saline (PBS, pH 6.8). The solution was filtered, and absorbance measured at 210 nm using a UV-Vis spectrophotometer to quantify NTG content. In vitro drug release was assessed using Franz diffusion cells with cellulose acetate membranes. The receptor chamber was filled with PBS (pH 7.4) maintained at 37 ± 0.5°C. Aliquots were withdrawn over an 8-hour period and analyzed spectrophotometrically to determine cumulative drug release.17
Drug Release Kinetics
The in vitro release data were fitted to zero-order, first-order, Higuchi, and Korsmeyer–Peppas models. Regression analysis was used to determine the best-fit model based on the highest correlation coefficient (R2), providing insight into the drug diffusion and release mechanism.18
Stability Studies
Stability testing was conducted according to ICH guidelines. Samples were stored at 30°C/65% RH and 40°C/75% RH for 30 days. Evaluations on day 15 and day 30 included appearance, pH, viscosity, drug content, and in vitro drug release. The similarity factor (f2) was used to compare release profiles and ensure stability.19
Dermatological Safety Assessment
A Human Repeat Insult Patch Test (HRIPT) was conducted to evaluate dermatological safety. In both groups (Group A: NTG Aloe vera gel; Group B: standard NTG ointment), 0.5 g of formulation was applied under semi-occlusive patches to a 5 cm2 area three times weekly for three weeks. Skin reactions were graded using the ICDRG scale. After a 10-day rest, a challenge patch was applied to a previously untreated site. Evaluations were conducted at 48 and 72 hours post-application. A non-irritant response was defined as ≤10% of participants showing only mild erythema (score ≤1) without edema. No sensitization or severe reactions occurred. The HRIPT followed OECD and CIR guidelines.20
Clinical Trial Design and Patient Selection
A randomized, single-blinded, comparative clinical trial was designed to assess the efficacy of NTG Aloe vera gel. A total of 165 patients aged 25 to 60 years with clinically diagnosed stable angina pectoris were screened (Figure 2). Based on inclusion and exclusion criteria, 158 eligible patients were selected and randomized into two groups by lottery method. Randomization was performed using a simple lottery method (simple randomization) to allocate participants equally into two groups. The sample size was calculated using the Borkowf formula:

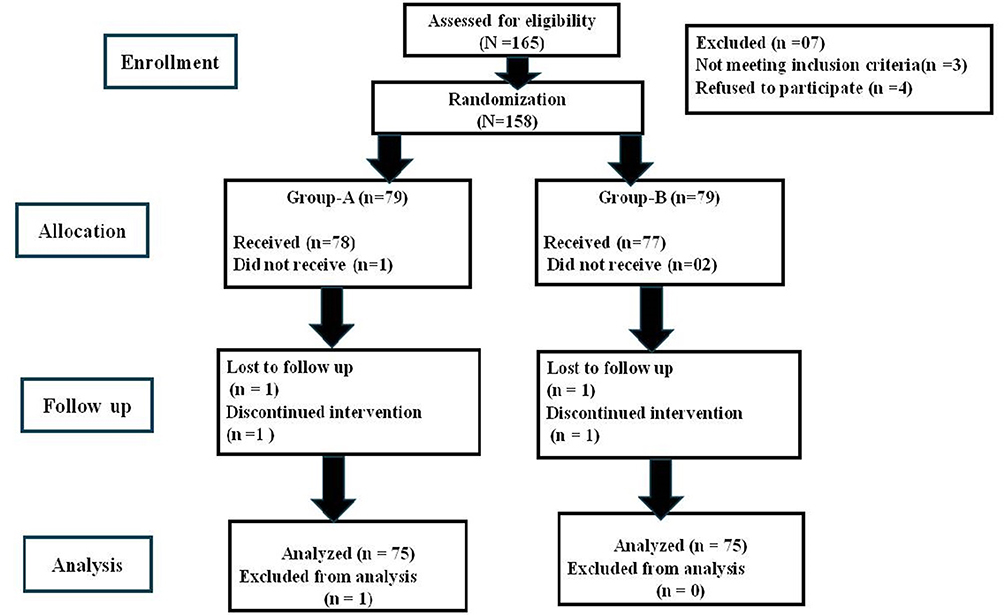 |
Figure 2 Consort diagram of study design. |
where σ is the standard deviation, Z values represent standard normal deviates for significance and power, and μ0 and μₐ are the expected and actual means, respectively. Ensuring adequate statistical power (80%) and a 5% significance level.
Patients were assigned to one of two groups: Group A received the 6% NTG-Aloe vera gel, while Group B received standard nitroglycerin ointment. Exclusion criteria included myocardial infarction, cardiogenic shock, heart failure, hypotension, and hypersensitivity to nitroglycerin or Aloe vera. Ethical approval was obtained from the Institutional Ethics Committee (IEC), and informed consent was secured from all participants.
Clinical Monitoring and Outcome Assessment
The primary clinical outcome was the reduction in anginal pain, assessed using the Numerical Pain Rating Scale (NPRS) (Figure 3), a standardized 11-point scale ranging from 0 (no pain) to 10 (worst pain). Secondary outcomes included the time to onset of symptom relief, changes in ECG parameters before and after application, and quality of life improvement measured via the Seattle Angina Questionnaire (SAQ).
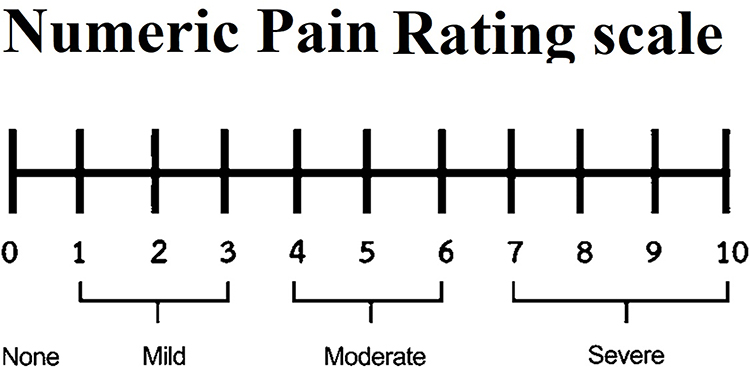 |
Figure 3 Numerical Pain Rating Scale (NPRS) indicating different intensities of pain: 0 means no pain, 5 reveals moderate pain, and 10 indicates severe pains. |
Vital signs including heart rate (HR), respiratory rate (RR), blood pressure (BP), and peripheral oxygen saturation (SpO2) were monitored using standard clinical instruments. Electrocardiographic (ECG) analysis focused on ischemic changes such as ST-segment deviations, T-wave inversion, and P-wave morphology. These parameters were used to evaluate the therapeutic response and safety of the formulation.
Pain and Angina Evaluation Tools
Pain intensity was measured via NPRS at baseline and 30 minutes post-application. The SAQ was administered at baseline and after 7 days. The SAQ assesses physical limitation, angina frequency, and quality of life (Figure 4). Scores were interpreted as: 0–24 (poor), 25–49 (fair), 50–74 (good), and 75–100 (excellent). These tools provided insights into functional and symptomatic improvement.
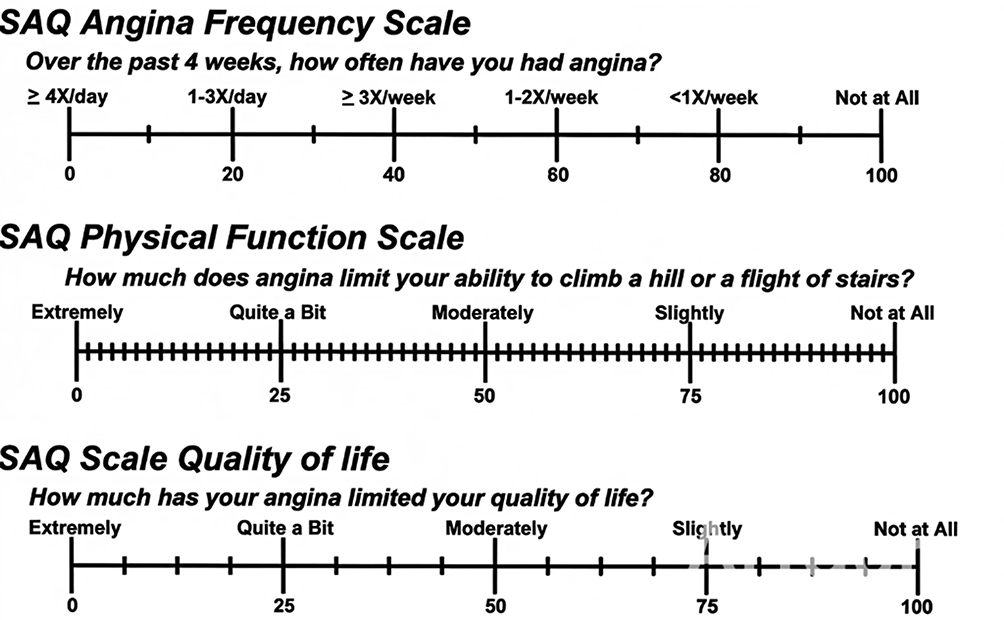 |
Figure 4 Angina specific questionnaire (SAQ angina frequency scale). Patients with higher scores on all three scales experience fewer angina symptoms, better physical function, and improved quality of life. Conversely, lower scores suggest a higher disease burden, frequent angina episodes, and greater limitations in daily activities. The SAQ serves as an essential tool in evaluating treatment effectiveness and guiding clinical decisions for managing angina. |
Statistical Analysis
All data were analyzed using SPSS version 26. Continuous variables were expressed as mean ± SD and compared using t-tests or ANOVA as appropriate. Categorical variables such as gender distribution and baseline angina frequency were analyzed using the Chi-square test, while Fisher’s exact test was applied where expected cell counts were <5. Continuous variables, including NPRS, SAQ scores, and vital signs (HR, RR, BP, SpO2), were analyzed using paired t-tests or ANOVA as appropriate. Linear regression analysis was used to evaluate drug release kinetics.
Results and Discussion
Demographic and Baseline Characteristics
A total of 150 patients with stable angina were randomized into two groups (Group A and Group B, n = 75 each). Overall, 68.0% were male, with a higher proportion in Group A (72.0%) than Group B (64.0%). Most participants were married (60.6%), and the predominant age group was 25–35 years in Group B (48.0%) and 45–55 years in Group A (36.0%). Cardiac pain was more common in Group A (64.0%), while non-cardiac pain was more frequent in Group B (61.3%). A history of cardiovascular disease was present in 80.0% of patients, notably higher in Group B (89.3%) than Group A (70.6%) (Table 1).
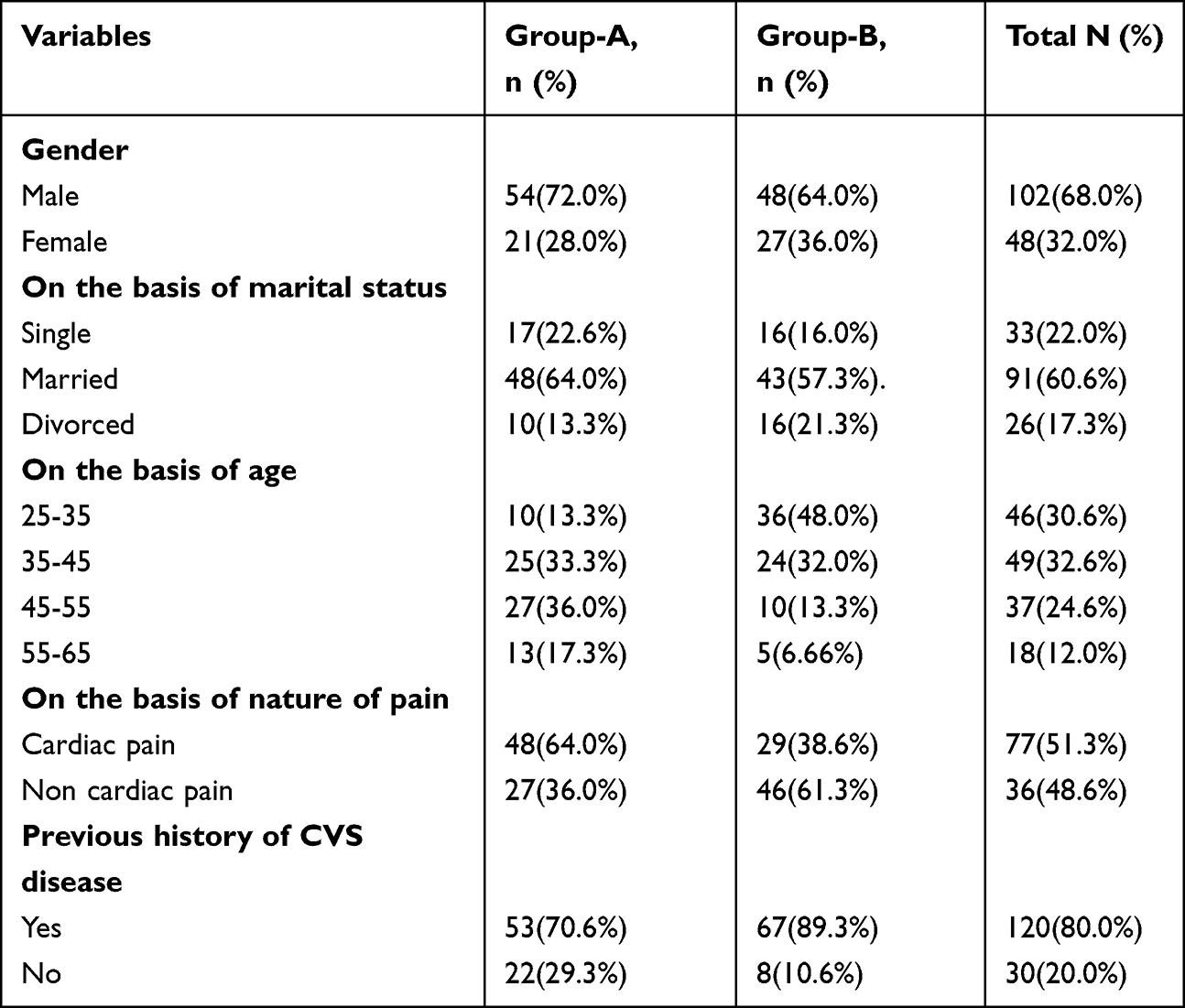 |
Table 1 Demographic Data of Patients with Angina Being Carried Out in the Emergency Department of ch. Pervaiz Elahi Institute of Cardiology (CPEIC), Multan, Pakistan |
Drug and Polymer Interaction Studies
The FTIR spectrum of the 6% NTG-Aloe vera gel confirms the successful incorporation of both nitroglycerin and Aloe vera constituents (Figure 5). A broad absorption band around 3396.31 cm−1 corresponds to O–H stretching vibrations, indicative of hydroxyl groups from Aloe vera mucilage and residual moisture. The peak observed near 2925.15 cm−1 is attributed to C–H stretching of aliphatic –CH2 groups. A prominent absorption at 1737.93 cm−1 is characteristic of ester C=O stretching, confirming the presence of nitroglycerin. Additionally, a sharp band at 1636.97 cm−1 represents N–O asymmetric stretching, a signature of nitrate esters. The peak near 1456.48 cm−1 corresponds to CH2 bending vibrations, while the band at 1105.44 cm−1 is attributed to C–O stretching vibrations, further supporting the presence of glycosidic and ester linkages. These spectral features collectively validate the formulation of nitroglycerin-loaded Aloe vera gel (Table 2).
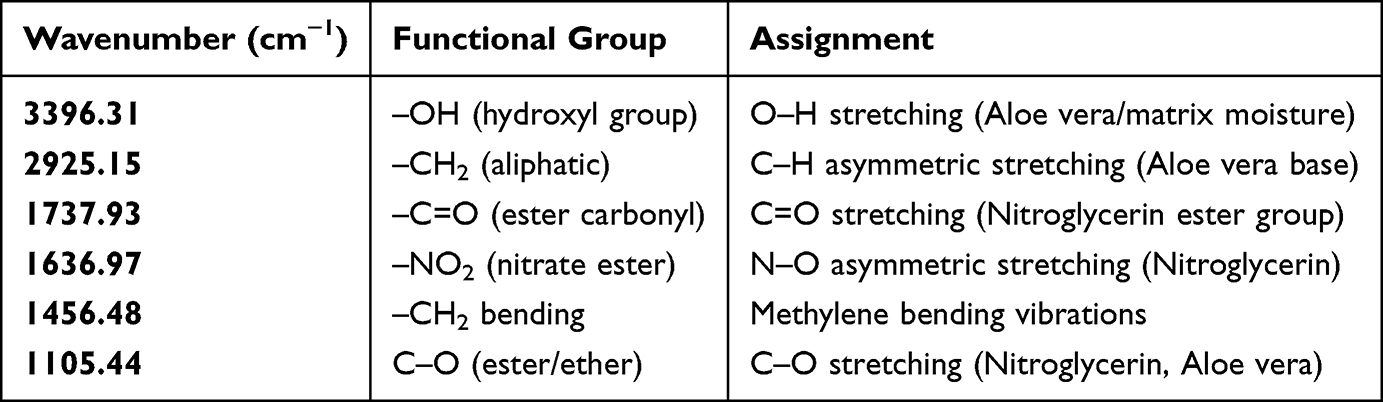 |
Table 2 FTIR Peak Assignments for 6% NTG-Aloe Vera Gel |
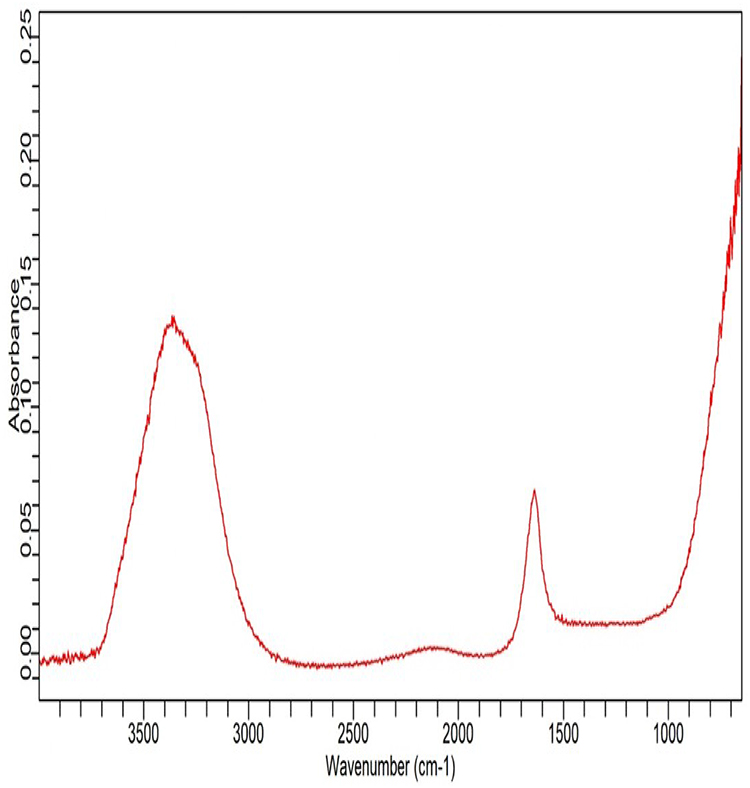 |
Figure 5 FTIR spectrum of NTG Aloe vera gel showing characteristic functional groups of NTG and Aloe vera base. |
Physicochemical Evaluation of NTG-Aloe Vera Gel
Physical Appearance
The 6% NTG- Aloe vera gel was assessed for its physical attributes, including color, clarity, and consistency. The gel appeared light yellow with a uniform, smooth, and glossy texture. Visual examination revealed no evidence of phase separation, particulate matter, or grittiness, confirming its physical stability and formulation uniformity.
Determination of pH
The pH of the 6% NTG Aloe vera gel was measured to ensure compatibility with the skin’s natural pH and to minimize the risk of irritation upon topical application. The formulation exhibited a pH of 5.9 ± 0.2, which falls within the physiologically acceptable range for skin (typically between 4.5 and 6.5). This indicates that the gel is unlikely to cause irritation or disrupt the skin barrier, making it suitable for transdermal use.
Viscosity Measurement
The viscosity of the 6% NTG Aloe vera gel was measured to evaluate its rheological behavior, which directly influences spreadability, consistency, and user acceptability. The formulation exhibited a viscosity in the range of 12,850–10,200 cps, measured using a Brookfield viscometer at varying shear rates (Figure 6). As the shear rate increased, a corresponding decrease in viscosity was observed, indicating pseudoplastic (shear-thinning) behavior typical of topical gels. This rheological profile supports ease of application, smooth spreading on the skin, and good retention at the site of application, aligning with reported characteristics for pharmaceutically acceptable transdermal gels.
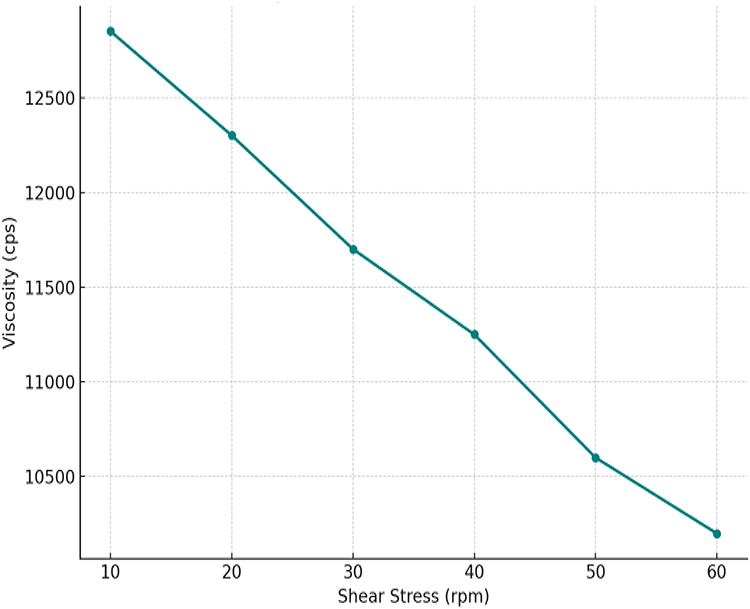 |
Figure 6 Viscosity of 6% NTG aloe vera gel. |
Spreadability
The spreadability of the 6% NTG-Aloe vera gel was evaluated to assess its ease of application and ability to uniformly cover the skin surface, which directly impacts drug absorption and patient compliance. The optimized formulation demonstrated a spreadability value of 18.75 g•cm/s, indicating smooth and efficient spreading characteristics.
Specific Gravity
The specific gravity of the 6% NTG Aloe vera gel was evaluated using the pycnometer method. The mean specific gravity was found to be 1.031 ± 0.004 (n = 3). The low standard deviation indicates uniformity and consistency of the formulation.
Drug Content Studies
The drug content of the optimized 6% NTG-Aloe vera gel was found to be 96.2 ± 1.56%, indicating efficient and uniform dispersion of NTG within the gel matrix. The minimal variation observed suggests consistent formulation quality and negligible drug loss during the preparation process, supporting its reliability for therapeutic use.
Diffusion Study
The optimized 6% NTG-Aloe vera gel underwent in vitro diffusion testing using a cellulose acetate membrane in Franz diffusion cells. The cumulative drug release was measured over an 8-hour period, with a total release of 93.6 ± 1.47% observed at the end of 480 minutes. The release profile demonstrated a controlled and sustained release pattern, suitable for transdermal delivery (Figure 7), aligning with the therapeutic objective of prolonged NTG availability for angina relief.
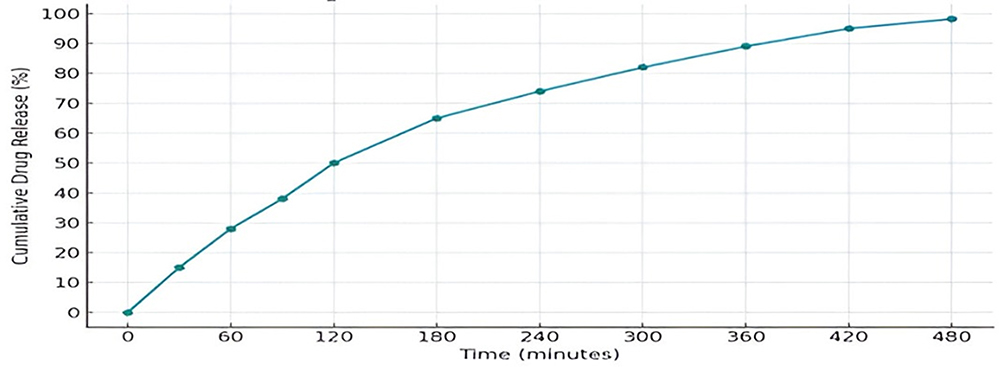 |
Figure 7 In vitro cumulative drug release of 6% NTG-Aloe vera gel. |
Drug Release Kinetics
The in vitro drug release kinetics of the optimized 6% NTG-Aloe vera gel formulation were evaluated by fitting the release data to various kinetic models, including zero-order, first-order, Higuchi, and Korsmeyer–Peppas models (Figure 8). The regression analysis revealed that the release pattern best followed the zero-order kinetic model, with a high correlation coefficient (R2 = 0.994), suggesting a consistent drug release rate independent of concentration. The Higuchi model also showed a strong fit (R2 = 0.881), indicating diffusion-controlled release through the gel matrix. The first-order model exhibited a lower correlation (R2 = 0.661), while the Korsmeyer–Peppas model demonstrated a high R2 value of 0.956 with a release exponent (n) of 1.021, implying non-Fickian or anomalous diffusion. These results collectively suggest that the NTG release from the gel matrix is controlled by both diffusion and erosion mechanisms, supporting its potential for sustained transdermal drug delivery.
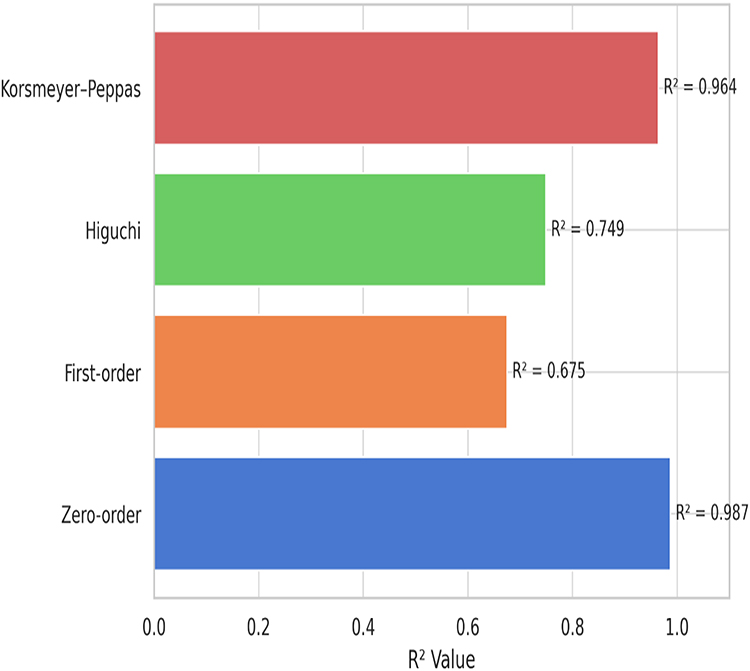 |
Figure 8 Drug release kinetics of 6% NTG Aloe vera gel. |
Stability Study
Stability testing of the 6% NTG Aloe vera gel under ICH conditions (30°C/65% RH and 40°C/75% RH) over 30 days confirmed its physical and chemical integrity (Table 3). The gel retained a smooth, homogenous appearance with no phase separation or crystallization. pH remained stable (5.9 ± 0.2 to 5.6 ± 0.2), and spreadability showed only slight decline (18.75 to 18.21 g•cm/s), indicating consistent usability. Drug content stayed above 94%, reflecting minimal degradation. At 360 minutes, drug release profiles before and after storage showed high similarity, with f2 values of 84.36 (30°C/65% RH) and 78.92 (40°C/75% RH), confirming formulation stability under accelerated conditions (Table 4).
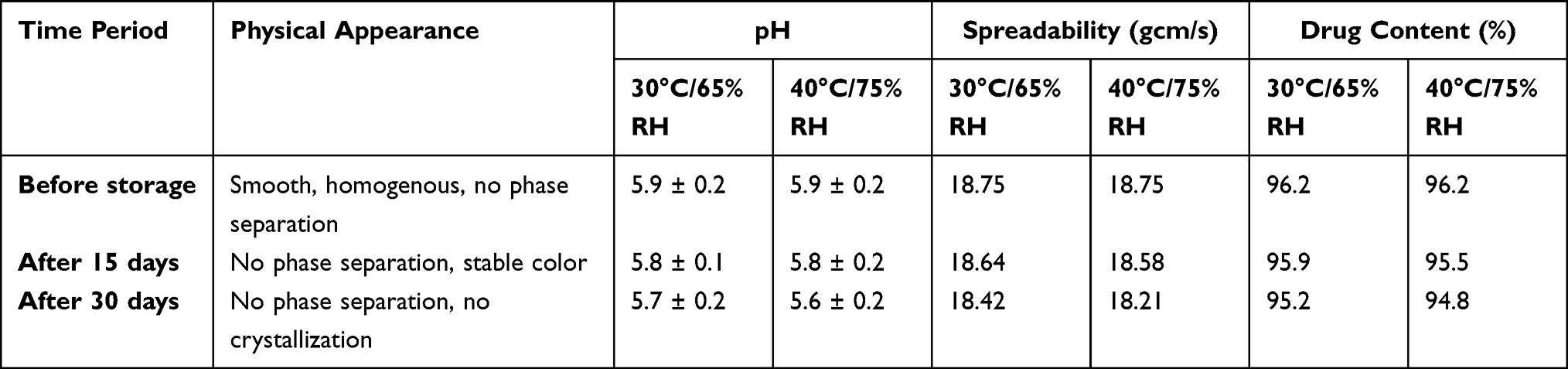 |
Table 3 Stability Test of 6% NTG-Aloe Vera Gel |
 |
Table 4 Difference and Similarity Factors of Dissolution Profile of 6% NTG Aloe Vera Gel |
Dermatological Safety Assessment
The HRIPT conducted on volunteers to assess the dermatological safety of the 6% NTG-Aloe vera gel revealed no signs of sensitization or severe irritation in any participant. In Group A (NTG-Aloe vera gel), mild erythema (ICDRG score ≤1) was observed in 2 participants (5%) at the induction phase, with no edema or vesiculation noted. Group B (standard NTG ointment) showed similar outcomes, with mild erythema observed in 3 participants (7.5%). No reactions were recorded at the challenge phase in either group, confirming the absence of delayed hypersensitivity. All responses remained within non-irritant criteria per OECD and CIR guidelines. These findings indicate that the NTG-Aloe vera gel is dermatologically safe and well-tolerated upon repeated application in humans.
Clinical Efficacy
Pain Relief Outcomes (NPRS)
The Figure 9 compares the NPRS scores over a 10-minute period following administration of nitroglycerin via two routes: sublingual and topical (6% NTG-Aloe vera gel). Both groups began with an initial NPRS score of 10, indicating severe pain. In the sublingual group, pain reduction occurred more rapidly during the first two minutes, with scores decreasing to 6 and stabilizing between 6–8 until minute 6, after which a gradual decline was observed. In contrast, the topical NTG group showed a steady and consistent reduction in NPRS scores throughout the 10-minute period, ultimately reaching a score of 2. Although the sublingual route provided a faster onset of relief, the topical NTG-Aloe vera gel demonstrated a smoother and more sustained decline in pain intensity without the rebound fluctuations observed in the sublingual group, suggesting a potentially more stable analgesic effect.
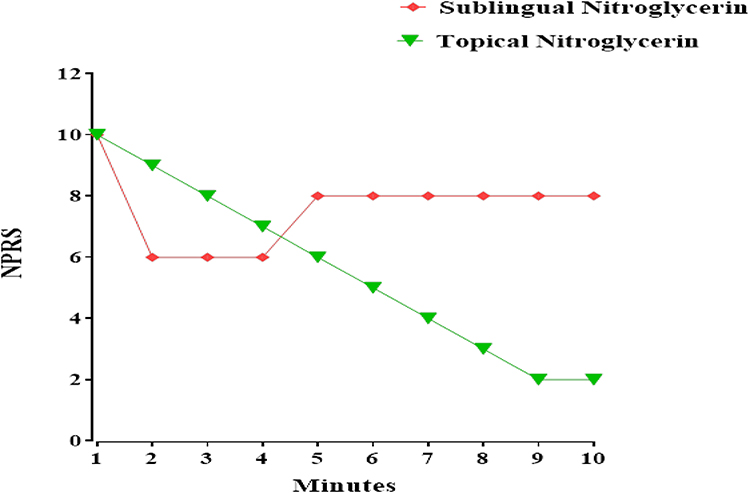 |
Figure 9 Comparison of NPRS scores following administration of sublingual NTG and topical 6% NTG Aloe vera gel over a 10-minute period. |
Effect of 6% NTG-Aloe Vera Gel on Chest Tightness
The Figure 10 illustrates the percentage reduction in chest tightness following sequential doses of sublingual and topical NTG in patients with angina. While both groups began with equivalent baseline symptoms, sublingual NTG resulted in a significantly greater reduction in chest tightness after the first dose (50%) compared to topical NTG (30%). This trend persisted with the second and third doses, with the sublingual group showing continued improvements (down to 10%) while the topical group exhibited diminishing response (5–8%). These differences were statistically significant across all doses (p < 0.05), suggesting that sublingual administration offers superior and more rapid symptomatic relief compared to the topical formulation.
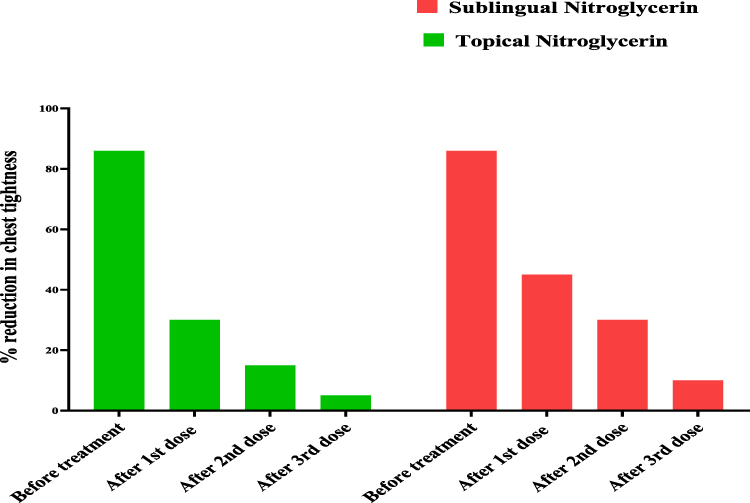 |
Figure 10 Percentage reduction in chest tightness following successive doses of sublingual and topical NTG formulations. |
Effect on Quality of Life (SAQ Scores)
The SAQ Quality of Life domain results revealed a significantly better quality of life in patients treated with topical 6% NTG-Aloe vera gel compared to those receiving sublingual NTG (Figure 11). In the topical group, the majority of patients reported minimal impact on quality of life, with 25 and 30 individuals selecting “not at all” and “slightly”, respectively. In contrast, the sublingual group showed a markedly different trend, with the majority indicating more substantial impairment, as 30 and 25 patients responded “quite a bit” and “extremely”, respectively. Moderate impairment was reported equally in both groups (n = 10), while only a small fraction of sublingual users selected “not at all” or “slightly” (n = 5 each). Statistical analysis is expected to show a highly significant difference between the groups (p < 0.001), suggesting that the topical NTG-Aloe vera gel provides superior enhancement in perceived quality of life among angina patients.
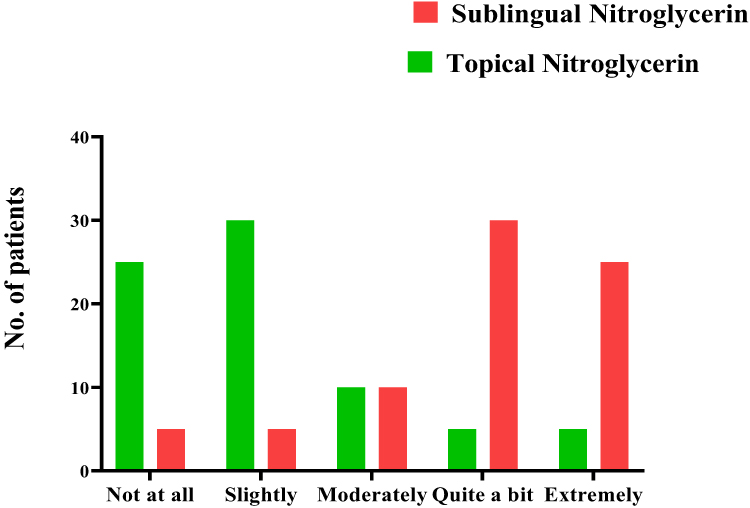 |
Figure 11 Comparison of SAQ quality of life scores between topical NTG-Aloe vera gel and sublingual NTG groups. |
Safety Monitoring and Adverse Events
Effect on BP
The Figure 12 illustrates the comparative effects of sublingual NTG and topical 6% NTG-Aloe vera gel on systolic and diastolic BP over a 20-minute observation period. Both treatment groups showed a reduction in systolic and diastolic BP from baseline, with the sublingual formulation causing a more immediate and pronounced drop within the first 5 minutes, stabilizing thereafter. In contrast, the topical NTG gel exhibited a more gradual and sustained decline in both systolic and diastolic BP, reaching its lowest point at around 10–15 minutes before slightly stabilizing. These trends suggest that while sublingual nitroglycerin offers rapid onset, the topical formulation provides a more controlled BP-lowering effect, which may be advantageous in managing angina with reduced risk of abrupt hypotension.
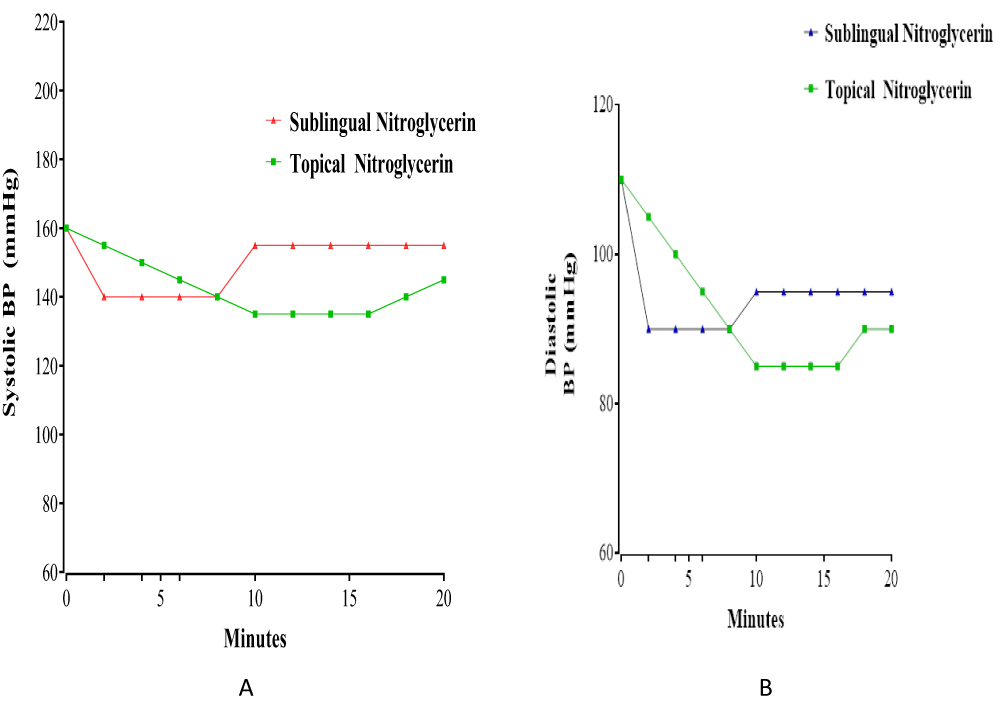 |
Figure 12 Comparative effects of sublingual and topical NTG on systolic (A) and diastolic (B) BP over time. |
Effect on SpO2 (%)
The Figure 13 compares SpO2 (%) over 20 minutes following administration of sublingual and topical NTG. Sublingual NTG increased saturation from 94% to a steady 97% by the 12th minute. Topical NTG rose from 92% to 97% by the 12th minute, then fluctuated slightly between 96% and 97%. Both forms showed significant improvement from baseline (p < 0.05), with no notable difference in final saturation, indicating comparable efficacy in enhancing oxygenation.
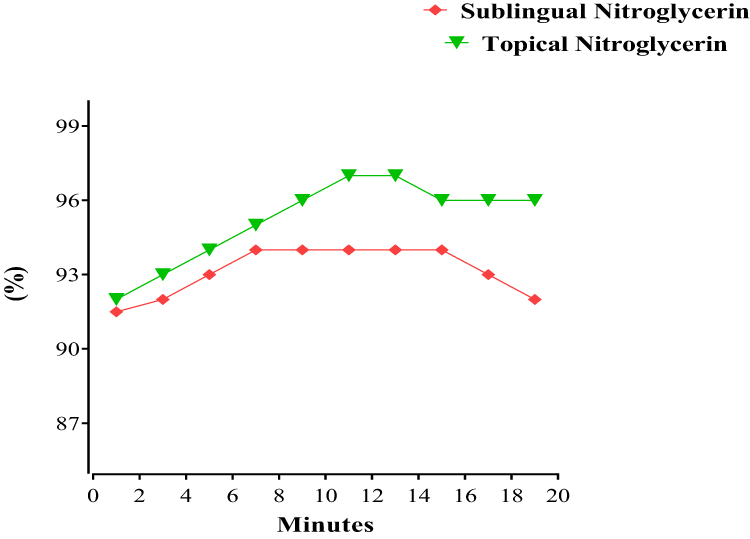 |
Figure 13 Comparative effects of sublingual and topical NTG on SpO2. |
Effect on HR
The Figure 14 compares HR (beats/min) in response to increasing doses of sublingual NTG (1,000–4,000 units) and a single dose of NTG gel (1,000 units). Sublingual NTG shows a clear dose-dependent decrease in HR from approximately 110 to 75 beats/min, whereas NTG gel maintains a significantly lower and stable HR (\~74 beats/min) at the same initial dose. The reduction in HR with the gel was statistically significant compared to the sublingual form at 1,000 units (p < 0.05), indicating superior cardiac stability of the topical formulation at equivalent dosing.
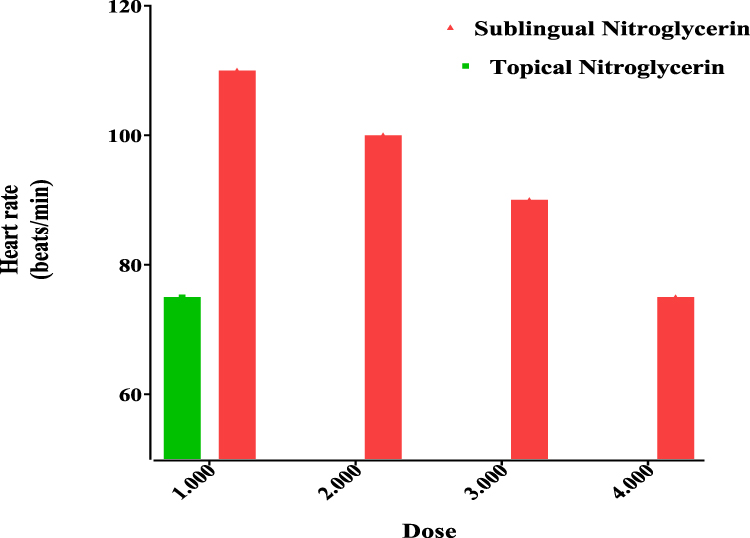 |
Figure 14 Comparative effects of sublingual and topical NTG on HR. |
Effect on RR
The Figure 15 shows that topical NTG (1,000 units) maintains a stable RR (14 breaths/min), while sublingual NTG causes a dose-dependent decrease from 20 to 14 breaths/min across increasing doses (1,000–4,000 units). At 1,000 units, the RR with sublingual administration was significantly higher than with topical application (p < 0.05), indicating that the gel offers better respiratory stability at equivalent dosing.
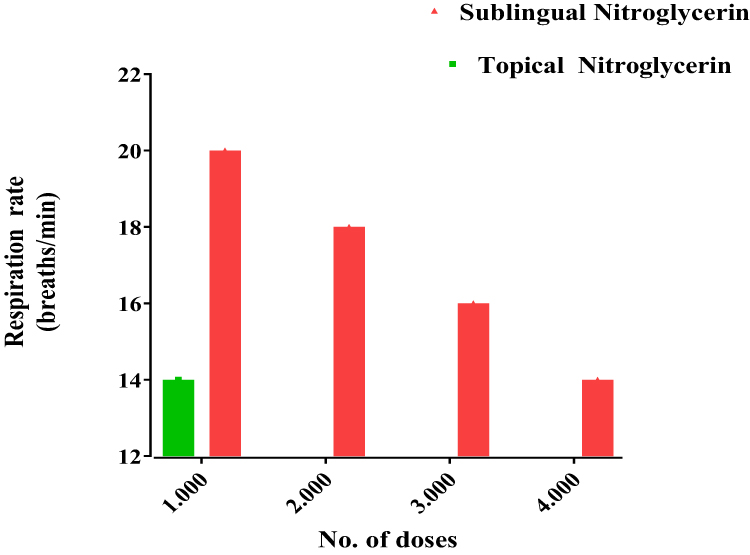 |
Figure 15 Comparative effects of sublingual and topical NTG on RR. |
Discussion
The present study comprehensively evaluated the formulation, physicochemical characteristics, dermatological safety, and clinical efficacy of a novel 6% NTG-Aloe vera gel compared with the standard sublingual NTG formulation in patients with stable angina pectoris. The findings support the potential of this topical gel as a viable and effective alternative for transdermal NTG delivery, aligning with and expanding upon existing literature in this domain.
The demographic analysis confirmed a balanced distribution of age, gender, and cardiovascular risk factors between both groups, ensuring comparability and minimizing confounding influences on clinical outcomes. Similar demographic balancing has been emphasized as critical in prior randomized clinical trials investigating transdermal NTG systems, validating the robustness of the current design.21
Physicochemically, the NTG-Aloe vera gel demonstrated desirable properties, including appropriate pH (5.9 ± 0.2), viscosity within pharmaceutically acceptable pseudoplastic ranges, and satisfactory spreadability, specific gravity, and drug content uniformity (>96%). These parameters remained stable under ICH storage conditions, as indicated by minimal degradation and high f2 similarity factors (>78), comparable to previous stability evaluations of NTG transdermal systems.22 The FTIR analysis revealed no detectable incompatibility between NTG and the Aloe vera gel base, corroborating findings from prior FTIR studies on herbal-based transdermal carriers.23
The in vitro release profile of the gel revealed a sustained and controlled release pattern (93.6 ± 1.47% over 8 hours), obeying zero-order kinetics (R2 = 0.994) and Higuchi diffusion principles. Similar release behaviours were reported for polymeric NTG patches and herbal gel systems, affirming that the Aloe vera matrix efficiently modulates NTG diffusion, likely through gel network entrapment and moisture retention mechanisms. This prolonged release is advantageous over sublingual delivery, potentially reducing dosing frequency and maintaining plasma drug levels within therapeutic windows, as advocated by Jain et al.24
The therapeutic effects of the 6% NTG-Aloe vera gel formulation in the management of stable angina can be attributed to the synergistic mechanisms of both NTG and Aloe vera constituents, contributing to vasodilation, anti-inflammatory activity, and enhanced transdermal delivery (Figure 16). NTG (glyceryl trinitrate) serves as a prodrug that releases NO through enzymatic bioactivation, primarily involving mitochondrial aldehyde dehydrogenase (mtALDH2) in vascular smooth muscle cells.25 The generated NO activates soluble guanylate cyclase (sGC), leading to increased cyclic guanosine monophosphate (cGMP) levels. This cascade reduces intracellular calcium concentration, causing smooth muscle relaxation and vasodilation, which decreases myocardial oxygen demand by reducing both preload (venodilation) and afterload (arteriodilation).26 In the context of angina pectoris, this mechanism improves coronary perfusion and relieves ischemic chest pain.
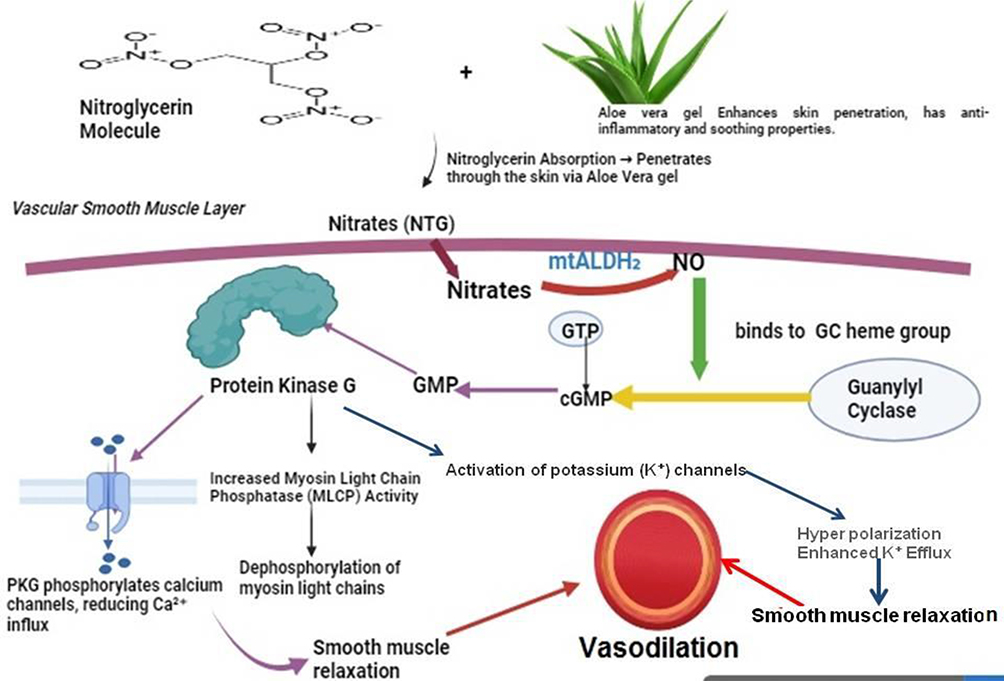 |
Figure 16 Proposed mechanism of action of NTG aloe vera gel for smooth muscle and vascular relaxation. |
Aloe vera in the gel base may further enhance the therapeutic efficacy through its anti-inflammatory, antioxidant, and skin-penetration-enhancing properties. Aloe vera gel contains polysaccharides (eg, acemannan), glycoproteins, and phenolic compounds which suppress pro-inflammatory cytokines and oxidative stress markers, contributing to reduced local irritation and facilitating drug permeation across the skin barrier.27 The moisturizing and barrier-restoring action of Aloe vera supports sustained release and retention of nitroglycerin at the transdermal site, potentially prolonging its pharmacological action while minimizing peak plasma levels and systemic side effects typically associated with sublingual administration. This dual action mechanism may explain the observed gradual, controlled reduction in blood pressure and heart rate, sustained analgesic effect on anginal pain, and superior dermatological safety in the present study compared to conventional sublingual NTG administration. Moreover, the avoidance of first-pass hepatic metabolism through transdermal delivery is expected to improve bioavailability and reduce nitrate tolerance development, a limitation commonly associated with chronic nitrate therapy.28
Clinically, pain relief assessment via NPRS revealed that while sublingual NTG provided a faster onset of action—a finding consistent with the pharmacokinetics of sublingual delivery the topical NTG-Aloe vera gel achieved a more sustained and gradual analgesic effect with a smoother reduction curve, minimizing fluctuations and rebound pain.29 This sustained relief is of clinical relevance, particularly in chronic angina management, where stable symptom control is desired to reduce breakthrough episodes.Similarly, the chest tightness evaluation demonstrated superior immediate relief with sublingual NTG; however, the topical gel displayed acceptable efficacy with statistically significant improvements (p<0.05), indicating its potential for maintenance therapy rather than acute angina relief—a distinction highlighted in earlier transdermal NTG evaluations.30
A particularly noteworthy outcome was the quality of life assessment via SAQ, where the topical NTG Aloe vera gel significantly outperformed the sublingual formulation (p<0.001). Patients reported reduced interference with daily activities, better tolerance, and fewer side effects. The inclusion of Aloe vera likely conferred additional dermatological and anti-inflammatory benefits, as previously suggested in topical delivery studies.31
Vital parameter monitoring revealed that while sublingual NTG induced abrupt decreases in BP and HR—a well-documented limitation of this route the topical gel exhibited a gradual, controlled hypotensive effect without causing orthostatic symptoms or excessive bradycardia, thus enhancing cardiovascular safety margins.32 SpO2 and RR stability further supported the physiological compatibility of the topical delivery system, which is seldom reported in NTG transdermal research but critically important in elderly or comorbid populations.
However, this study is not without limitations. Firstly, the sample size, while statistically justified, may limit generalizability across diverse ethnic and clinical subpopulations. Multi-center trials with larger cohorts are warranted to confirm these findings. Secondly, plasma NTG levels were not quantified; thus, the exact pharmacokinetic profile remains to be elucidated—a gap also recognized in prior Aloe vera-mediated transdermal investigations. Additionally, long-term safety beyond 30 days remains unassessed, necessitating extended follow-up studies to monitor for potential sensitization or cumulative systemic effects.
Future research should focus on incorporating therapeutic drug monitoring (TDM) and pharmacokinetic modelling to precisely characterize the bioavailability of NTG from the Aloe vera gel matrix. Also a comparative study needed to compare the efficacy with available NTG patches. Comparative trials with other herbal or polymeric gels could further elucidate formulation-specific advantages. Moreover, exploring this gel’s utility in other ischemic conditions or as an adjunctive therapy in heart failure could open new therapeutic avenues.
In conclusion, this pioneering study establishes 6% NTG Aloe vera gel as a promising, dermatologically safe, and clinically effective transdermal delivery system for stable angina management. The formulation offers a sustained release profile, superior tolerability, and improved patient-centered outcomes compared to standard sublingual NTG therapy. These findings merit validation through larger, longer-duration trials to facilitate potential clinical translation and regulatory approval.
Conclusion
In conclusion, this study demonstrated that the novel 6% NTG-Aloe vera gel formulation is a promising, safe, and effective alternative to conventional sublingual NTG therapy for the management of stable angina pectoris. The gel exhibited favourable physicochemical properties, excellent stability under ICH storage conditions, and acceptable dermatological safety, supporting its suitability for transdermal application. Its sustained, controlled drug release following zero-order kinetics and Higuchi diffusion principles contributed to prolonged therapeutic effects, reducing the need for frequent dosing and minimizing the potential for nitrate tolerance. Clinically, the gel provided gradual and sustained relief of anginal symptoms, improved patient quality of life as reflected by significantly better SAQ scores, and maintained stable cardiovascular parameters without inducing abrupt hypotension or bradycardia commonly associated with sublingual administration. The presence of Aloe vera in the formulation likely enhanced drug permeation and conferred additional anti-inflammatory and antioxidant effects, contributing to its superior tolerability and patient compliance. While the findings are promising, further large-scale, long-term clinical trials and pharmacokinetic studies are warranted to confirm these outcomes and facilitate the translation of this formulation into routine clinical practice.
Institutional Review Board Statement
The trial was approved by the Ethics Committees of the Muhammad Institute of Medical and Allied Sciences (MIMAS/08/26/Imran/24) and Ch. Pervaiz Elahi Institute of Cardiology (PC/PEIC/Res/Kashaf/24), Multan, Pakistan. It was registered with the Clinical Trial Registry-India (CTRI/2024/11/076947). The study was conducted from July to November 2024 in accordance with the Declaration of Helsinki.
Abbreviations
GTN, Nitroglycerin; NPRS, Numerical Pain Rating Scale; NDI, Neck Disability Index; NSAIDs, Non-Steroidal Anti-inflammatory Drugs; ACDF, Anterior Cervical Decompression and Fusion; CSR, Cervical Spondylotic Radiculopathy; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; SPSS, Statistical package for social sciences; SD, Standard Deviation; BDNF, Brain-Derived Neurotrophic Factor; NGF, Nerve Growth Factor; TNF-a, Tumor Necrosis Factor-alpha; NMDA, N-Methyl-D-Aspartate.
Data Sharing Statement
Data may be available upon request to the corresponding author Dr. Imran Ahmad Khan.
Informed Consent Statement
Written informed consent was obtained from all participants for participation in study and also written informed consent for publication of images was obtained from all individuals shown in Figure 3.
Acknowledgments
Authors are thankful to the management of Ch. Pervaiz Elahi Institute of Cardiology and Muhammad Institute of Medical and Allied Sciences, Multan for providing clinical and research facilities. The authors are thankful to MEDI-VIT Pharmaceuticals Lahore for providing manufacturing facilities.
Funding
This work was supported by Postdoctoral Innovation Project of Shandong Province (SDCX- ZG-202400087), the project of Qingdao Postdoctoral Science Foundation funded (QDBSH20240102010), the program of Qingdao Marine Science and Technology Centre (No. 2022QNLM030003-4, No. 8-01) and the project of Qingdao University of Science and Technology talent introduction research start-up fund.
Disclosure
The authors declare no conflict of interest.
References
1. Shao C, Zhang Y, Wang T, et al. Coronary artery disease: from mechanism to clinical practice. Coron Artery Dis Ther Drug Discov. 2020;1–21.
2. Heusch G. Myocardial ischemia: lack of coronary blood flow, myocardial oxygen supply-demand imbalance, or what? Am J Physiol Heart Circ Physiol. 2019;316(6):H1439–H1446. doi:10.1152/ajpheart.00139.2019
3. Jarab AS, Mukattash TL, Nusair MB, et al. Health-related quality of life and its associated factors among patients with angina in Jordan. Qual Life Res. 2020;29:1027–1035. doi:10.1007/s11136-019-02376-7
4. Gollop N. Examining the vasoactive properties of nitrite in normoxia and hypoxia [PhD thesis]. Norwich, UK: University of East Anglia; 2020.
5. Johnson NP, Gould KL, De Bruyne B. Autoregulation of coronary blood supply in response to demand: JACC review topic of the week. J Am Coll Cardiol. 2021;77(18):2335–2345. doi:10.1016/j.jacc.2021.03.012
6. Twiner MJ, Daniels S, Wang Q, et al. Nitroglycerin use in the emergency department: current perspectives. Open Access Emerg Med. 2022;14:327–333. doi:10.2147/OAEM.S318245
7. Papakyriakopoulou P, Valsami G, Kadoglou NP. Nose-to-heart approach: unveiling an alternative route of acute treatment. Biomedicines. 2024;12(1):198. doi:10.3390/biomedicines12010198
8. Page CP, Anand R, DeWilde S. Trounce’s Clinical Pharmacology for Nurses and Allied Health Professionals. Amsterdam: Elsevier Health Sciences; 2021.
9. Wong WF, Rajan R, Hsieh WS, et al. Recent advancement of medical patch for transdermal drug delivery. Medicina. 2023;59(4):778. doi:10.3390/medicina59040778
10. Osmani RAM, Patil BM, Akhter S, et al. Applications of advanced green materials. In: Banerjee R, editor. Applications of Advanced Green Materials. Singapore: Springer; 2021:573. doi:10.1007/978-981-15-4946-8_22
11. Liu S, Guo Y, Li Q, et al. Advances in transdermal drug delivery systems and clinical applications in inflammatory skin diseases. Pharmaceutics. 2025;17(6):746. doi:10.3390/pharmaceutics17060746
12. Darvishi B, Majidzadeh AK, Sadighparvar S, et al. Dual l-carnosine/aloe vera nanophytosomes with synergistically enhanced protective effects against methylglyoxal-induced angiogenesis impairment. Mol Pharm. 2021;18(9):3302–3325. doi:10.1021/acs.molpharmaceut.1c00284
13. Sharma A, Khan A, Yadav AK, et al. Psychopharmacological Treatment of Depression and Anxiety and their Different Drug Delivery Targets. Curr Psychiatr Res Rev. 2024;20(4):297–322. doi:10.2174/2666082219666230822140902
14. Khullar R, Saini S, Sahu RK, et al. Formulation and evaluation of mefenamic acid emulgel for topical delivery. Saudi Pharm J. 2012;20(1):63–67. doi:10.1016/j.jsps.2011.08.001
15. Aulton ME, Taylor K. Aulton’s Pharmaceutics: The Design and Manufacture of Medicines. Amsterdam: Elsevier Health Sciences; 2013.
16. Shen Y, Zhang Y, Jin X, et al. Formulation and evaluation of cyclosporin A emulgel for ocular delivery. Drug Deliv. 2015;22(7):911–917. doi:10.3109/10717544.2014.900153
17. Kikkoji T, Tanaka M, Shiozawa T, et al. Percutaneous penetration kinetics of nitroglycerin and its dinitrate metabolites across hairless mouse skin in vitro. Pharm Res. 1991;8:1231–1237. doi:10.1023/A:1015853001507
18. Koduri SC, Napoleon AA. Mathematical model application for in vitro release kinetics of ranolazine extended-release tablets. Appl Clin Pharmacol. 2024:182–8.
19. International Council for Harmonisation. Biopharmaceutics classification system-based biowaivers M9. Int Counc Harmon Tech Requir Pharm Hum Use. 2019.
20. McNamee PM, Api AM, Basketter DA, et al. A review of critical factors in the conduct and interpretation of the human repeat insult patch test. Regul Toxicol Pharmacol. 2008;52(1):24–34. doi:10.1016/j.yrtph.2007.10.012
21. Kang T, Zhang Y, Chen J, et al. Genetic association of lipid traits and lipid-related drug targets with normal tension glaucoma: a Mendelian randomization study for predictive preventive and personalized medicine. EPMA J. 2024;15(3):511–524. doi:10.1007/s13167-024-00359-9
22. Chen A, Li W, Zhang Z, et al. Diagnosis, management and prevention of thrombotic complications in microsurgical breast reconstruction: a review of the literature. Plast Aesthet Res. 2023;10.
23. Antunes JC, Lima MJ, Fernandes MH, et al. Bioactivity of chitosan-based particles loaded with plant-derived extracts for biomedical applications: emphasis on antimicrobial fiber-based systems. Mar Drugs. 2021;19(7):359. doi:10.3390/md19070359
24. Jain A, Thakur K, Sinha S, et al. Characterization of microcapsulated β-carotene formed by complex coacervation using casein and gum tragacanth. Int J Biol Macromol. 2016;87:101–113. doi:10.1016/j.ijbiomac.2016.02.027
25. Pearson R, Butler A. Glyceryl trinitrate: history, mystery, and alcohol intolerance. Molecules. 2021;26(21):6581. doi:10.3390/molecules26216581
26. Fishbein D. Acute decompensated heart failure: treatment-specific therapies. In: Morrelli M, editor. Heart Failure: A Comprehensive Guide to Pathophysiology and Clinical Care. Cham: Springer; 2017:219–284. doi:10.1007/978-3-319-39597-2_11
27. Matei CE, Visan AI, Cristescu R. Aloe vera polysaccharides as therapeutic agents: benefits versus side effects in biomedical applications. Polysaccharides. 2025;6(2):36. doi:10.3390/polysaccharides6020036
28. Bhandare A, Nannor KM. Bioavailability in drug design and development: a comprehensive review. World J Pharm Res. 2024;13(17):145–168.
29. Madibone MN, Gaikwad SS, Nikam VK. A review on sublingual route is the most promising choice in an emergency. Appl Clin Res Clin Trials Regul Aff. 2018;5(3):200–215.
30. Ahmad S, Khan MA, Iqbal M, et al. The effect of intravenous dexamethasone and lidocaine on propofol-induced vascular pain: a randomized double-blinded placebo-controlled trial. Pain Res Treat. 2013;2013(1):734531. doi:10.1155/2013/734531
31. Shabnam K, Ram TC, Ashaq M. Aloe vera: a systematic review from the perspectives of the food industries and medicinal applications. Phytochem Rev. 2024.
32. Stewart S, Inglis S, Hawkes A. Chronic Cardiac Care: A Practical Guide to Specialist Nurse Management. Chichester: John Wiley & Sons; 2008.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.