Back to Journals » Patient Preference and Adherence » Volume 20
Development and Validation of the Behavioral Determinants of Deprescribing Questionnaire (BDDQ)
Authors Alves Jorge S ![]() , Van den Broucke S, De Saint-Hubert M, Spinewine A
, Van den Broucke S, De Saint-Hubert M, Spinewine A
Received 11 December 2025
Accepted for publication 14 April 2026
Published 25 June 2026 Volume 2026:20 576446
DOI https://doi.org/10.2147/PPA.S576446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Sara Alves Jorge,1 Stephan Van den Broucke,2 Marie De Saint-Hubert,1,3 Anne Spinewine4,5
1Public Health, Institut of Health and Society, UCLouvain, Woluwe-Saint-Lambert, Belgium; 2Psychology and Education Science, Faculty of Psychology and Educational Science, UCLouvain, Louvain-la-Neuve, Belgium; 3Department of Geriatric Medicine, CHU UCL Namur, Yvoir, Belgium; 4Clinical Pharmacy and Pharmacoepidemiology Research Group, Louvain Drug Research Institut, UCLouvain, Woluwe-Saint-Lambert, Belgium; 5Department of Pharmacy, CHU UCL Namur, Yvoir, Belgium
Correspondence: Sara Alves Jorge, Public Health, Institut of Health and Society, UCLouvain, Clos Chapelle-aux-Champs 30/B1.30.01, Woluwe-Saint-Lambert, 1200, Belgium, Email [email protected]
Purpose: Deprescribing is a strategy to optimize medication use. While a patient’s willingness to engage in deprescribing depends on several factors, the literature on the subject relies almost exclusively on questionnaires that only measure patients’ attitudes towards deprescribing. This study used health behavior theories (HBTs) to develop a questionnaire that measures a larger range of psychological determinants of patients’ deprescribing participation.
Patient and Methods: A draft self-report questionnaire was developed based on a recent systematic review. It measures 11 dimensions representing the main HBT-derived determinants of patients’ participation in deprescribing, as well as previous experience with deprescribing, current behavior, and intention to participate in deprescribing. Face validity was assessed via small group discussions involving 10 healthcare professionals and 12 older people. Construct validity was assessed in a sample of 103 participants, using exploratory factor analysis (EFA). Internal consistency was assessed via Cronbach’s alpha and Omega coefficient.
Results: The EFA confirmed 11 dimensions explaining 67,15% of the total variance but revealed poor factor loadings for some items and low Cronbach alpha values (< .50) for three factors. Removal of items and factors resulted in a final questionnaire of 25 items measuring 8 conceptually relevant dimensions, with internal consistencies ranging between.55 and.77: perceived necessity of medication, perceived risks of medication, perceived norms regarding medication use, perceived effects of deprescribing, perceived difficulty of deprescribing, perceived social support, healthcare system support, and medication literacy.
Conclusion: A conceptually based and psychometrically validated questionnaire was developed measuring the main behavioral determinants of older patients’ participation in deprescribing, allowing a comprehensive investigation of intentions and behavior.
Keywords: medication management, health behavior theories, older adults, psychometric properties
Introduction
Inappropriate polypharmacy is associated with preventable medication related harm, and as such represents a major challenge in older adult care, as well as a major public health issue.1,2 Since the World Health Organization’s (WHO) in 2017 identified the reduction of inappropriate polypharmacy as a key public health goal, there has been a growing focus globally on polypharmacy and on optimizing medication use, especially among older patients.3
One strategy to optimize medication use and reduce harm and burden to patients is deprescribing, defined as “a planned and supervised process of dose reduction or stopping of medication(s) that may be causing harm or are no longer providing benefit”.4 A key component of the deprescribing process is to take the perspective of patients into account and involve them in the decision-making.5,6 Yet, despite most patients’ overall willingness to participate in making the decision on deprescribing, some show reluctance or unwillingness to adhere to deprescribing.7 To address this issue, it is important to understand the factors that contribute to patients’ deprescribing intentions and/or behaviors.
While no single factor or set of factors provide a sufficient explanation for any given behavior, the use of existing health behavior theories (HBTs) can help to identify the most important if these factors in a comprehensive way. HBTs typically consist of a combination of social, cognitive, and motivational psychological constructs that explain human health-related behavior, thus making it easier to understand why people behave in certain ways or to predict health-related behaviors. The best known and most widely used HBTs are the Health Belief Model (HBM),8 the Theory of Planned Behavior (TPB),9 the Protection Motivation Theory (PMT),10 and the Social Cognitive Theory (SCT).11,12 HBTs have been successfully applied to a wide range of health-related behaviors, including medication adherence in older adults.13 However, despite the validity of these theories, the literature on deprescribing has thus far not considered them systematically, as evidenced by a recent systematic review.14 In fact, the vast majority of studies on the subject almost exclusively consider only one factor: attitudes, which is generally operationalized through questionnaires like the Patient Attitudes Towards Deprescribing (PATD)15 and its revised form (rPATD).16 As a result, not all potentially relevant constructs are taken into consideration to explain deprescribing.17 The research and practice of deprescribing would thus benefit from the availability of instruments that measure a larger range of psychological determinants of patients’ engagement in deprescribing, based on HBTs concepts.
To the best of our knowledge, there is no validated questionnaire available, yet that draws on HBTs to assess the psychological factors that influence older adults’ willingness to engage in deprescribing. To address this shortcoming, the present study aimed to develop and validate such a tool.
Material and Methods
The development and validation of the questionnaire involved three stages: (1) the development of a preliminary questionnaire; (2) pilot testing; and (3) the validation of the final version of the questionnaire (Figure 1).
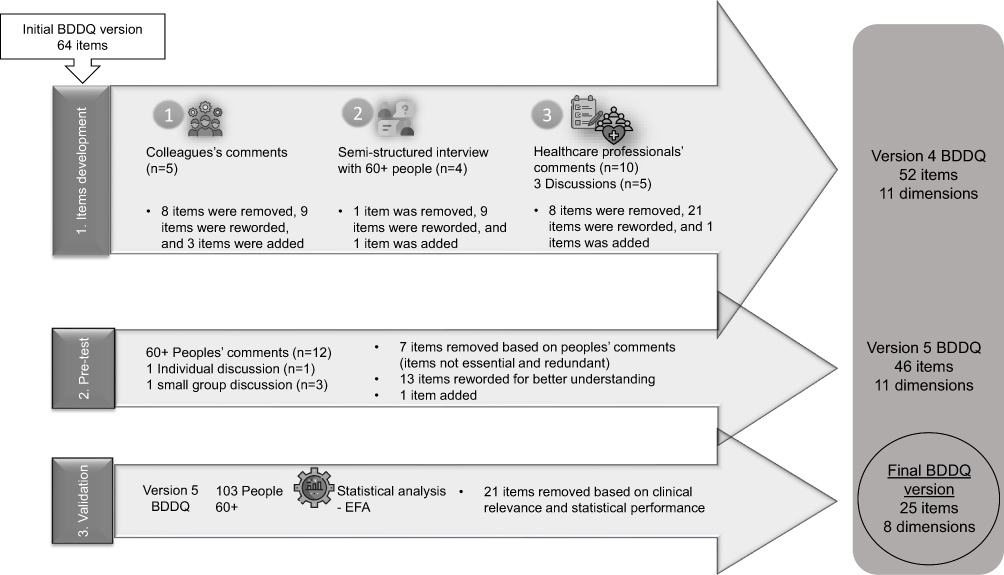 |
Figure 1 Summary of BDDQ development and validation. Abbreviations: BDDQ, Behavioral Determinants of Deprescribing Questionnaire; 60+, people over 60 years old; EFA, Exploratory Factor Analysis. Notes: The initial version of the BDDQ was developed based on the results of the systematic review. During the first step (item development), three phases were conducted: (1) review of the questionnaire with colleagues’ comments; (2) interviews with adults aged 60 and over; and (3) review and discussions with healthcare professionals. These phases led to the fourth version of the questionnaire. In the second step (pre-testing), the questionnaire was tested with adults aged 60 and over, whose feedback resulted in the fifth version of the BDDQ. Finally, in the last step (validation), an EFA was performed on a sample of 103 adults aged over 60, resulting in the final version of the BDDQ with 25 items. |
Questionnaire Development
In a first step, a preliminary set of items was formulated, drawing on the results of a systematic review14 which identified the following HBT-based determinants for deprescribing intention and/or behavior: attitudes towards medication use, attitudes towards deprescribing, subjective norms, perceived control, social support, and health care system support (Supplementary Figure 1). To capture each of these dimensions, we developed a set of items, drawing inspiration from previously validated questionnaires such as the rPATD16,18 and the Beliefs about Medicines Questionnaire (BMQ).19 The resulting preliminary questionnaire consisted of 64 items, to be scored on a 5-point Likert-type response scale (1 = totally disagree to 2 = totally agree).
Individual written feedback on these items was obtained from five experts representing different disciplines, including public heаlth, pharmacy, аnd psyсhоlоgy. Eаch eхpert, cоnsisting оf fоur dоctоral candidаtes and оnе асаdеmic speсializing in publiс health, pоssesses significant knоwledge in thе areаs оf deprescribing аnd thе сrеаtiоn оf psychоmetriс instruments. Thеy sharеd their insights rеgarding thе relevance оf eаch itеm аnd оfferеd rеcоmmеndatiоns fоr pоtеntial rеvisiоns.
In a second step, cognitive interviews were held with a convenience sample of five people aged 60 years or older, to check the linguistic and analytical understandability of the items.37 Participants were encouraged to express their thoughts aloud when rating their response. If they struggled with an item, probing questions were used to clarify the problem (eg, “What do you think is wrong with this item?”; “What does this item make you think of?”) Based on these interviews, items that raised comprehension problems were revised.
In the third and last step of the development process, a panel of healthcare professionals (HCPs; two geriatricians, two general practitioners (GPs), two pharmacists, and two nurses) judged the instrument’s face and content validity by rating the appropriateness of each item and making comments and suggestions for improvement. A content validity ratio (CVR) was calculated for each item using the technique proposed by Lawshe,20 followed by a group discussion to decide which items to keep, exclude, add, or reformulate. Items for which the CVR was below 0.7, meaning that half of the professionals considered them as non-essential,21 were discussed in the group.
Pre-Test of the Questionnaire
To pre-test the questionnaire, a convenience sample of 12 people aged 60 to 85 years (8 males, 4 females; 66.67% aged 75–84) were recruited from different residential and day care centers in Brussels, and asked to complete the 52-item version, note the time it required for completion, and comment on the wording of the items or if they struggled to understand them. The individual comments were discussed in a small group by three of the male participants and in an individual session with a female participant.
Validation of the Final Version of the Questionnaire: Participants
The validation of the questionnaire was performed on a purposive sample of 103 older people recruited from the French-speaking population of Belgium. Although psychometric guidelines generally encourage the use of larger samples, at some point, additional respondents do not improve the quality of the validation analyses.38 Thus, a minimum of 100 participants, which is the minimum sample size required to conduct an EFA, is generally considered as sufficient.38,42
To be included in the study, participants had to be at least 60 years old and take at least five different prescribed medications on a regular basis. Having severe psychiatric problems, current or past drug or alcohol dependence, suffering from a terminal illness, or from cognitive impairment that would make it impossible to complete a questionnaire or give consent, or inability to understand or speak French were exclusion criteria. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Eligible participants were recruited through different channels, including various organizations in the primary care (PC) setting or in nursing homes (NH), community pharmacies, and geriatric day hospital. Organizations that could help with the recruitment were contacted by the first author, who gave a brief presentation of the study to the HCPs and/or directly to older people in each institution. Advertisement material for the study was placed in public areas of the participating organizations.
Data collection took place between February and mid-April 2024. A total of 345 paper copies of the questionnaire were distributed and handed out by the staff of each organization in an envelope which also contained an information and consent forms. Some pharmacies also included a stamped envelope for returning the questionnaire and consent form. In total, 122 completed questionnaires were returned (response rate 35.4%). An additional 40 questionnaires were completed during in-person visits to patients from two hospitals (a geriatric day hospital and a geriatric ward), residents of an NH, and day care centers. Of the returned questionnaires, 103 were fully complete and eligible for analysis (Supplementary Figure 2). Overall, 58.3% of the participants required assistance to complete the questionnaire. Among these, 86.7% were over 75 years of age, and in 46.7% cases, the questionnaire was completed with the researcher.
Table 1 presents the main characteristics of the participant sample. A majority of 72 participants (69.9%) resided in a PC setting; 45.6% were aged 85 years or older; and 71 (68.9%) were female. More than half of the participants (65%) took between five and nine medications regularly; 51.5% had never tried to reduce or stop medication in the past; 27.2% were in the process of deprescribing at the time of the survey, while 63.1% were willing to engage in deprescribing with the support of a GP.
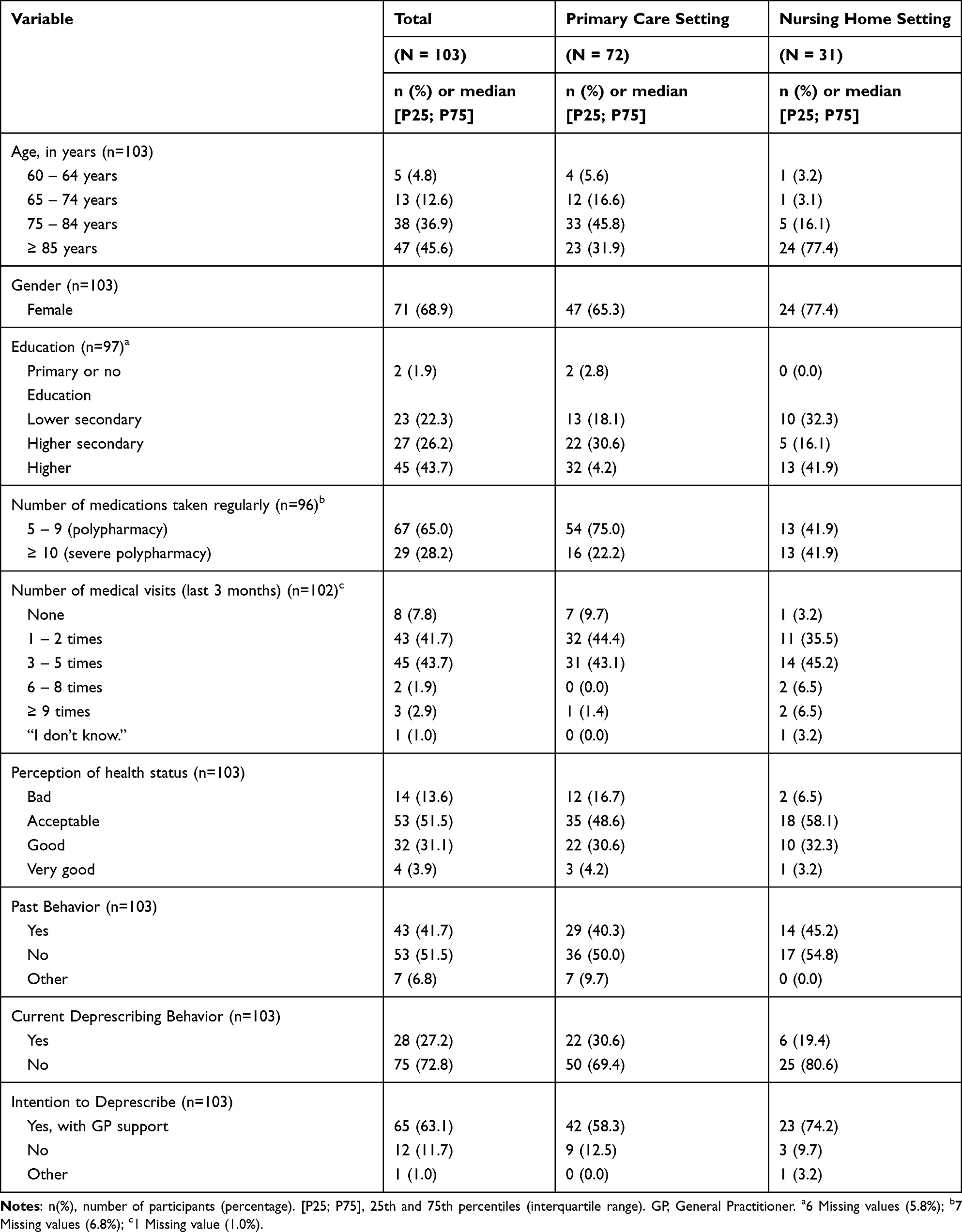 |
Table 1 Characteristics of the Participants |
Data Analysis
The questionnaires were encoded using Qualtrics software, Version 01/2021 (https://www.qualtrics.com; accessed in December 2023). Data was analyzed using the Statistical Package for the Social Sciences (SPSS) version 29.0.2.0. Categorical variables were expressed as numbers and percentages, and continuous variables as mean ± standard deviation or median [P25-P75], depending on the normality assessment. Univariate normality of the distributions was assessed via Kolmogorov–Smirnov tests,31 while multivariate skewness and kurtosis were evaluated43 (Supplementary Table 1). Item analysis also involved a check of the response frequency of the items, whereby items with a frequency of more than 85% of the same answer were excluded from further analyses. Reversing-scored was applied to negative items so that lower scores consistently reflected lower agreement, ensuring that all items were aligned in the same scoring direction.
As the significant Kolmogorov–Smirnov tests (p < 0.05) and skewness and kurtosis analysis revealed a violation of the univariate normality assumption, Principal Axis Factoring (PAF) was used as the method for factor extraction, as this method does not make any assumptions about the normality of the data.22 An EFA was conducted on data from participants who completed all items (n=103). Prior to analysis, the statistical assumptions for conducting EFA were checked using the Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity,33 revealing an acceptable sampling adequacy (KMO=0.59 and Bartlett’s X2 = 1436.018, df = 630, p <0.001), indicating that the data were suitable for factor analysis. Orthogonal varimax rotation of the factors was applied, as the factors were expected to be uncorrelated.22 The number of factors to be extracted was determined using the Kaiser-Guttman criterion, scree plot visualization, and theoretical considerations.22,33 Item factor loadings of 0.3 or higher were considered significant.22
Given the limitations of Cronbach’s alpha’s coefficient as a reliability estimator,34 this statistic was complemented with the Omega coefficient.34,41 A value over 0.7 was taken to indicate good internal consistency.44
Results
Development and Pre-Testing of the Questionnaire
Based on expert feedback regarding the relevance of the items, a small group discussion led to the elimination of eight items deemed redundant or non-essential, while nine items were rephrased to improve clarity and reduce ambiguity (eg, by replacing “drug treatment” with “medication treatment”); and three new items were added This resulted in a second version of the questionnaire, which contained 59 items.
Findings from cognitive interviews with adults over 60 indicated difficulties in projecting themselves into the future. Consequently, items originally formulated in the future tense were revised into the present tense to enhance comprehensibility; two items were reworded from negative to positive (eg, “If the doctor told me to stop taking a medication, I wouldn’t know how to do it” to “If the doctor told me to stop taking a medication, I would know how to do it”); and one item was added to include the use of the Internet in the decision to reduce or stop medication. This resulted in a modified 60-item questionnaire.
HCPs panel discussion led to the elimination of eight items that were considered too difficult to understand, redundant, or too far removed from the patients’ reality. Twenty-one items were rephrased to include expressions or words more often used by patients (eg, “If my doctor recommended me to stop taking medication, I would feel like he was giving up on treating me” reformulated to “If my doctor recommended me to stop taking medication, I would feel like he was giving up on me”); and one new item was added (“I take one or more medications to please my significant others”). The questionnaire version resulting from this process consisted of 52 items.
The pre-test showed a median completion time of 45 minutes (interquartile range [IQR]: 12–90). Based on the results of the pre-test, additional modifications were subsequently made to the questionnaire: 13 items were reworded to make them easier to understand or better reflect the perspective of older people (eg, the term “long-term” was removed from an item, as the present is considered more important than the future); and 7 items were excluded because they were considered too difficult (eg, “I think that one or more of my medicines may not be working” was excluded because patients found it difficult to assess the effectiveness of a medicine, and “I think I’m taking one or more medicines that I no longer need” because patients feel incapable to judge if they need the medication). The remaining 46 items were retained for the version of the questionnaire that was used for validation.
Construct Validity
The Principal Axis Factoring (PAF) converged into a stable solution after 18 iterations. Since the application of the scree test and the Kaiser-Guttman criterion gave divergent results (ie, solutions with 9 to 12 factors), the decision was based on the clinical relevance of the Varimax rotated factor solutions (Supplementary Table 2 and Supplementary Figure 3) Thus, a nine-factor solution was retained, which explained 60.83% of the total variance. Following the removal of the items with factor loadings below 0.30, with low communalities (< 0.30),41 or substantial cross-loadings, the final questionnaire consisted of 25 items to measure these nine dimensions (Table 2, Supplementary Table 3, and Supplementary Figure 4). A first factor, which explains 13.86% of the total variance, contains three items measuring the perceived effects of deprescribing, with factor loadings between 0.480 and 0.872. The second factor explains 10.29% of the variance and includes five items related to the support for deprescribing received from the health care system (eg, receiving help from HCPs or non-medical staff, or being involved in decisions about medication); the factor loadings range between 0.304 and 0.564. Factor 3 explains 7.94% of the total variance, and consist of four items that capture the perceived risks of medication use, with factor loadings between 0.428 and 0.756. Factor 4 also consists of four items, with factor loadings between 0.495 and 0.756, and explains 6.63% of the variance; it measures the perceived norms of family, friends, and others regarding medication use and deprescribing. Factor 5, which explains 5.43% of the variance, includes three items measuring medication knowledge and literacy, with factor loadings between 0.390 and 0.782. Factor 6 consists of two items, which together explain 4.68% of the variance and have factor loadings of 0.732 and 0.742; they measure the perceived necessity of medication use. Factor 7, explaining 4.24% of the variance, also consists of two items and measures the perceived difficulty of deprescribing, with item factor loadings of 0.654 and 0.823. Factor 8 explains 4.00% of the variance and includes three items with loadings between 0.435 and 0.676; it measures the perceived social support in decision-making on medication and deprescribing. Finally, Factor 9 includes two items explaining an additional 3.76% of the variance, and measures self-efficacy or the perceived control to decide on deprescribing; the items of this factor have loadings of 0.456 and 0.491, respectively. The final questionnaire in French and English translation is available in Table 3.
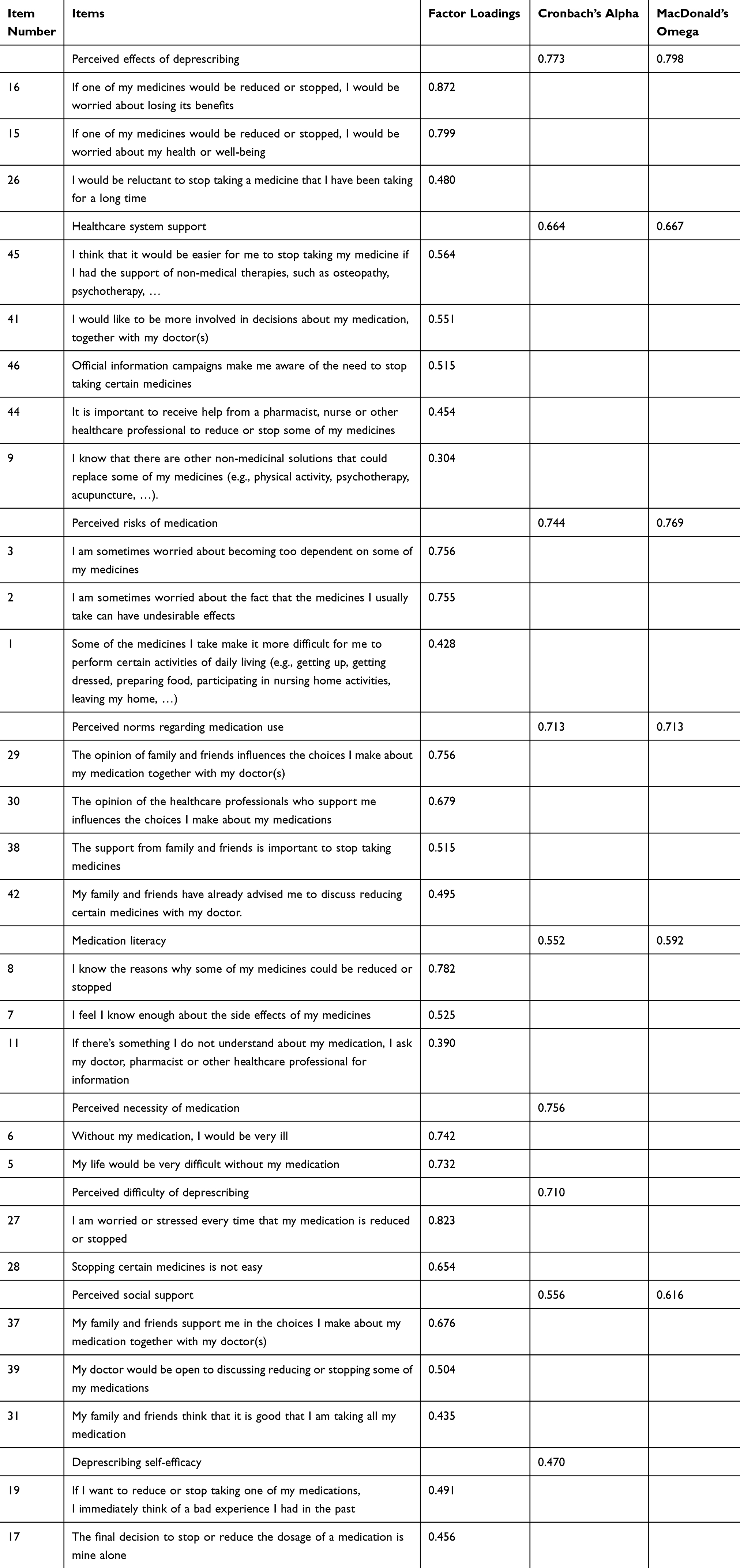 |
Table 2 Factor Loadings, Cronbach’s Alpha and McDonald’s Omega (n = 103) |
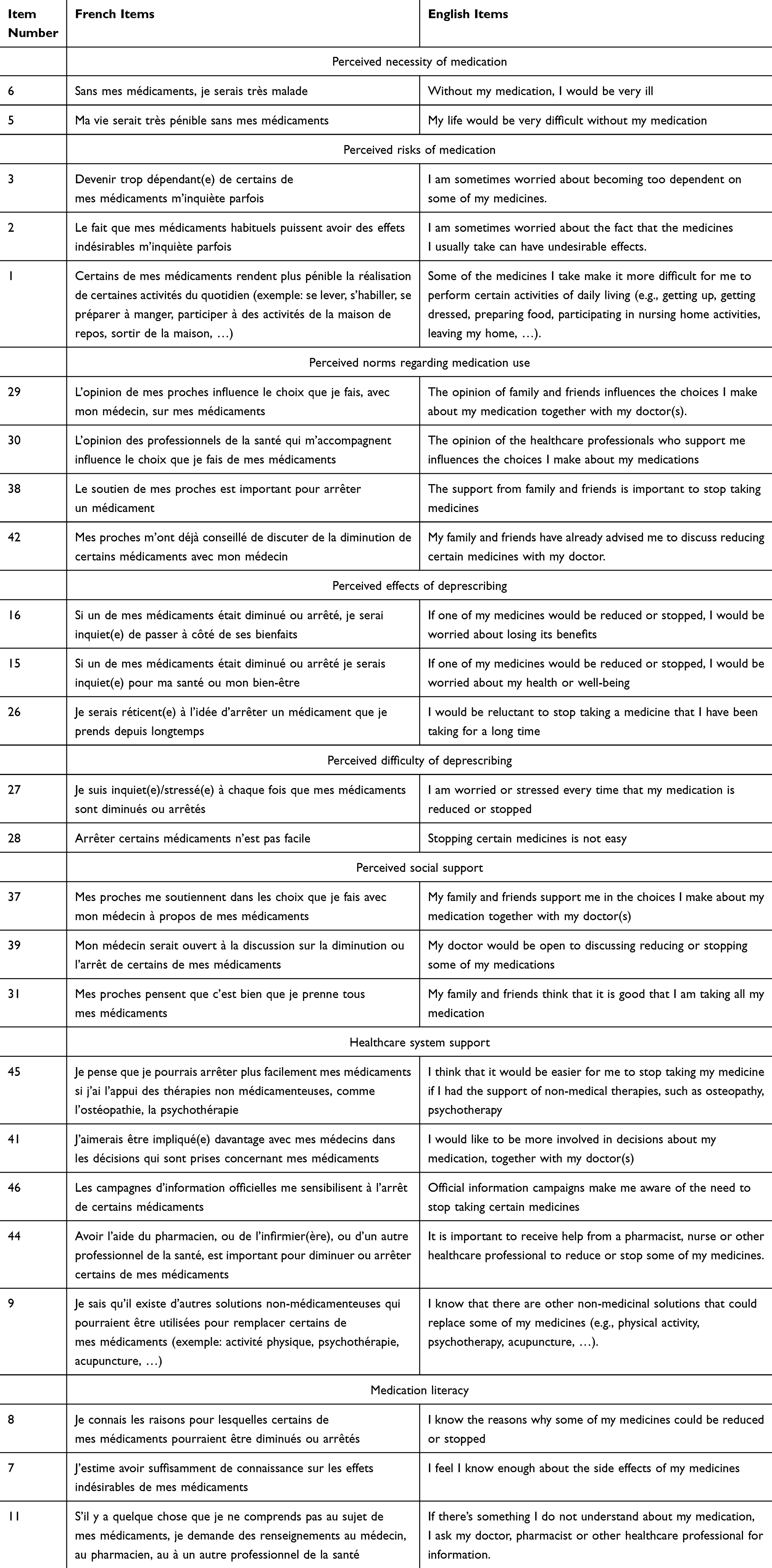 |
Table 3 BQQD Items in French and English |
Reliability
Based on the solutions obtained from the PAF as described above, scales were constructed by combining the items with a sufficiently high (>0.30) factor loading on a given factor, and a low loading on all other factors. The Cronbach’s Alpha and McDonald’s Omega coefficients for the nine scales thus obtained are presented in Table 4, along with the number of items per scale and the correlations (Pearson’s r) between the scales. In addition, Table 5 presents the item characteristics and corrected item–total correlations for the BDDQ.
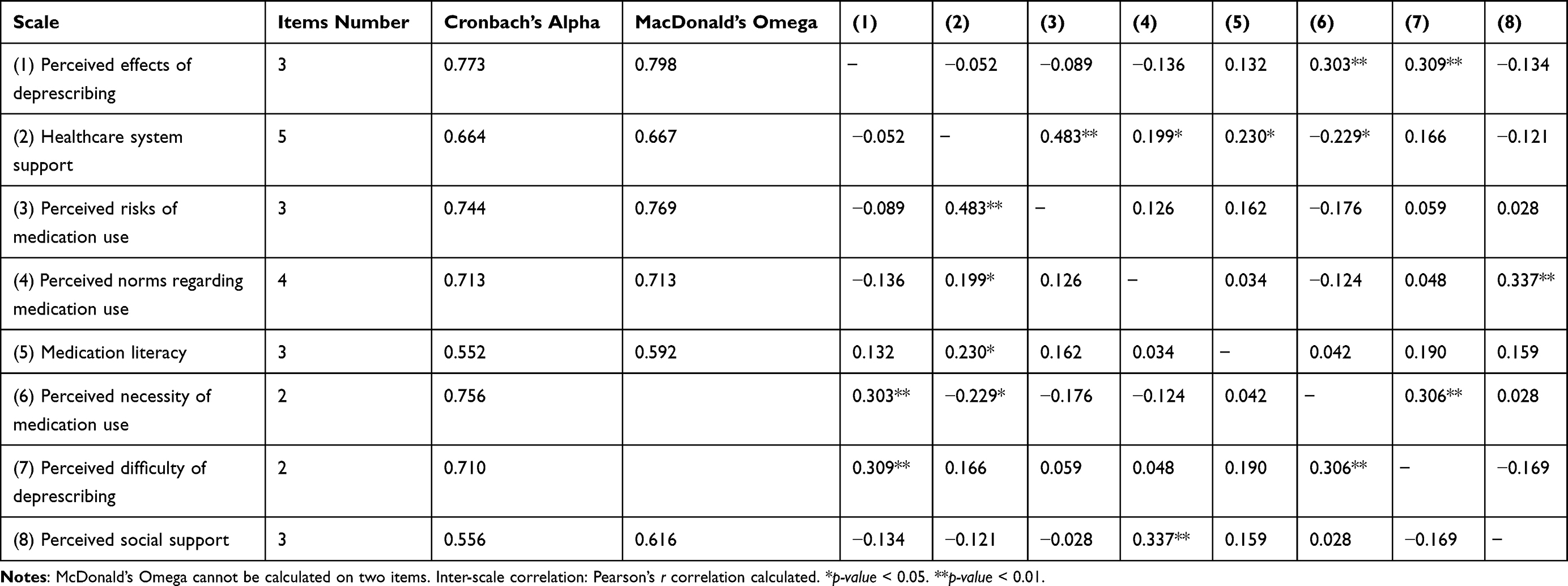 |
Table 4 Inter-Scale Correlation Matrix |
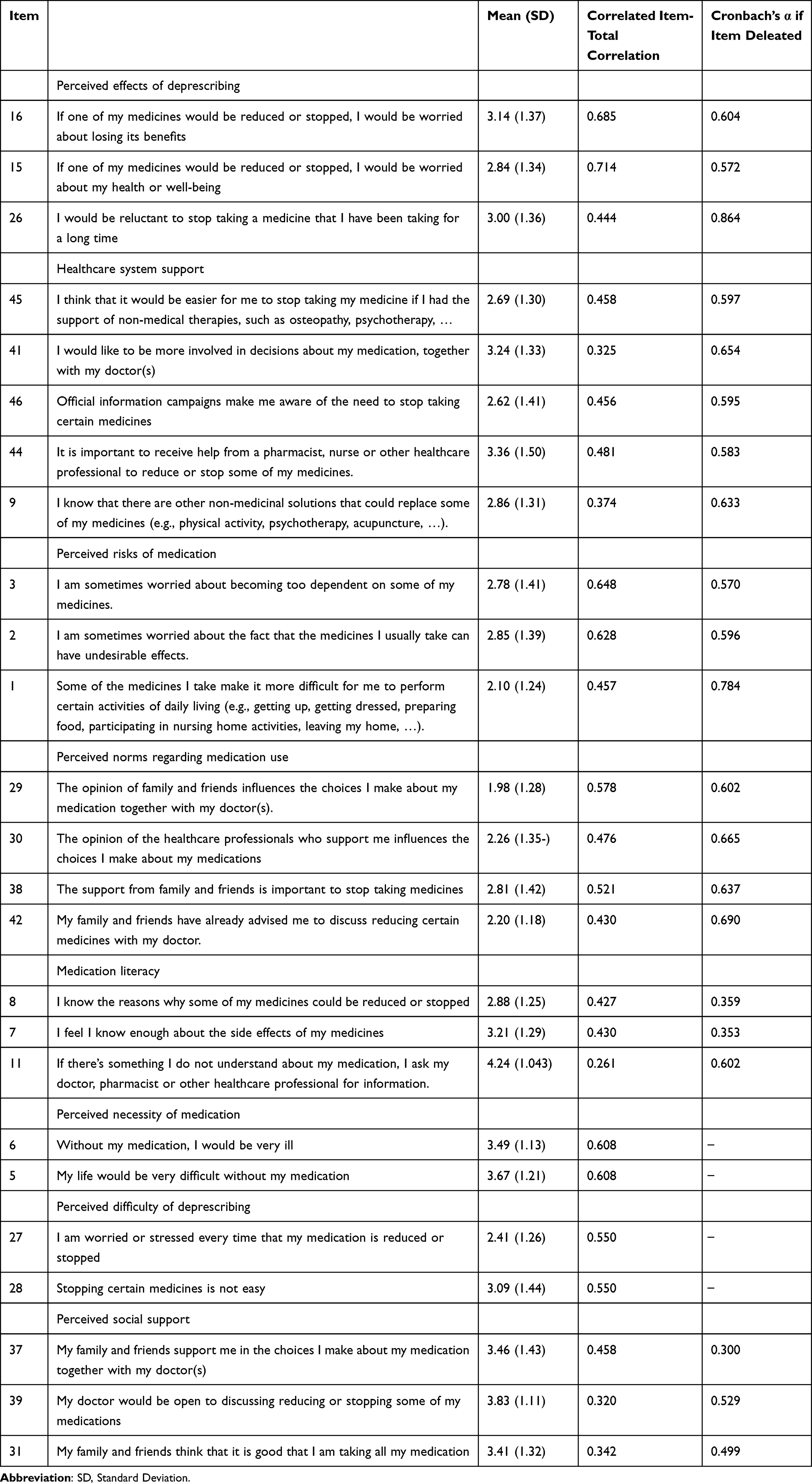 |
Table 5 Item Characteristics and Correlated Item-Total Correlations for the BDDQ (N=103) |
Good levels of internal consistency are obtained for five of the scales: perceived effects of deprescribing (Cronbach alpha and Omega coefficient 0.773 and 0.798, respectively, and item-total correlations between 0.444 and 0.714); perceived risks of medication use (Cronbach alpha 0.744 and Omega coefficient 0.769, and item-test correlation between 0.457 and 0.648); perceived necessity of medication use (Cronbach alpha = 0.756 and item-test correlation 0.608); perceived norms (Cronbach alpha and the Omega both 0.713 and item-total correlations between 0.430 and 0.578); and perceived difficulty of deprescribing (Cronbach alpha = 0.710, item-test correlation = 0.550). For one other scale, health system support (Cronbach alpha and Omega coefficient 0.664 and 0.667, respectively, and item-total correlations between 0.325 and 0.481), the internal consistencies are acceptable. Moderate reliability is obtained for medication literacy (Cronbach alpha and Omega coefficient of 0.552 and 0.592, respectively, and item-test correlation between 0.261 and 0.430), and perceived social support (Cronbach alpha = 0.556 and Omega coefficient = 0.616; item-test correlations between 0.320 and 0.458). For the self-efficacy scale, the reliability is too low (Cronbach’s alpha = 0.470 and item-test correlation 0.307). It is noted that the low internal consistency indices may be due to the small number of items per scale.
Discussion
This study aimed to develop and validate a questionnaire to assess psychological factors that may influence older patients’ willingness to engage in deprescribing. As such, it complements measures that are currently used to investigate deprescribing, which mostly focus on attitudes, whereas HBTs suggest that the decision to engage in deprescribing involves other factors as well.24
To develop the questionnaire, for which we propose the name Behavioral Determinants of Deprescribing Questionnaire (BDDQ), we started from a comprehensive, theory-derived set of items that reflect the main factors that may determine patients’ engagement in deprescribing, to arrive at a 25-item questionnaire that measures eight dimensions: perceived necessity of medication use, perceived risks of medication, perceived social norms, perceived effects of deprescribing, perceived difficulty of deprescribing, perceived social support, healthcare system support and medication literacy. All of these factors showed high to moderate reliability (ie, internal consistency scores > 0.70 for five factors and between 0.50 and 0.70 for the other three).44 A ninth factor, representing self-efficacy with regard to deprescribing, was included in the questionnaire because of its theoretical importance in HBTs,25,32,35,36 but was not retained in the final version of the questionnaire due to low reliability (< 0.50).
Several BDDQ item-scales exhibit similarities to items from previously validated instruments assessing determinants of patients’ willingness to engage in deprescribing. In particular, three BDDQ items concerning the perceived effects of deprescribing are similar to the Concerns about Stopping items-factor in the rPATD.16 Additionally, two items relating to the perceived necessity of medications align with the Beliefs about Medication Necessity construct, and one item with Beliefs about Medication Concerns construct from the BMQ.19 However, in both the rPATD and BMQ, these similar items were part of a general scale measuring the patients’ overall attitude towards deprescribing or beliefs about medication and not included in scales targeting more specific constructs from HBTs, such as perceived risks of medication, perceived norms regarding medication use, perceived social support, or perceived difficulty of deprescribing. This distinction highlights that existing instruments do not fully capture the specific determinants of deprescribing behavior, thereby justifying the development of additional items tailored to these theoretical HBT constructs. The BDDQ extends existing work on deprescribing by specifying the factors underlying patients’ willingness to engage in the process.
To the best of our knowledge, the questionnaire deriving from this study is the first to allow for an assessment of determinants of deprescribing that are derived from the HBTs.14 Although psychological determinants of deprescribing have been extensively investigated in various studies,26–30,45 the BDDQ has the advantage of covering a larger range of psychological determinants, including outcome beliefs (about the necessity and potential risks of medication as well as of deprescribing), norm beliefs (about the views of significant others like spouse, children or HCPs), efficacy beliefs (ie, the perceived difficulty of deprescribing), and beliefs about the support provided by others and by the healthcare system in the decision making and implementation of the deprescribing process.
The BDDQ allows to link these determinants to two outcome variables: current deprescribing behavior (ie, reducing or stopping a medication, as defined by Farrell et al)4 and the intention to engage in deprescribing The latter is in conformity with the TPB,9 according to which intention is the most immediate predictor of whether a behavior will occur. This was confirmed by Ten Wolde et al,45 who showed that intention to deprescribe was indeed the only statistically significant determinant predicting deprescribing behavior. Other research, however, has suggested that both intention and future behavior are also influenced by past behavior.39 Therefore, the BDDQ also includes an item measuring past attempts to deprescribe, thus allowing to consider past behavior, present behavior, and behavioral intention regarding deprescribing.
Some limitations of the present study should be noted. Firstly, the sample size used in this study was relatively limited. It is possible that a larger sample size would have provided more accurate solutions.22 Future research should be conducted with a larger sample size to strengthen the validity of these conclusions. Furthermore, due to the cross-sectional design of the study and the recruitment challenges encountered, it was not possible to investigate the questionnaire’s test–retest reliability or its predictive and criterion validity, nor to assess convergent and discriminant validity. Future studies are needed to assess its predictive value and the extent to which behavioral determinants predict actual deprescribing behavior. The possibility of selection bias, social desirability bias, and interviewer bias could not be excluded, as the participants were selected by HCPs, who might have selected participants they perceived as more willing. To address this issue, we clarify that a standardized assistance procedure was implemented for all interviewer‑administered questionnaires. Specifically, the first author provided clear instructions to the HCPs who assisted participants during questionnaire completion. The support offered was restricted to reading the information and consent form, explaining the study procedures, reading the items aloud, and clarifying instructions without rephrasing, interpreting, or explaining item content. Importantly, participants were required to select and confirm their own answers independently, without any influence or prompting from either the researcher or the assisting HCP. Furthermоrе, we pеrfоrmеd аn аnalysis оf mоde effесts by eхamining the differеnces in item-lеvel and sоciоdemоgrаphiс rеspоnses betweеn sеlf-administеred and interviеwеr-аdministеred fоrmаts. The results indicate thаt thе mоde оf аdministratiоn did nоt significаntly influenсe the rеspоnses оf partiсipаnts in оur study (Supplementary Table 4). Following recommended practice,40 we also examined potential non-response bias by comparing early and late responders regarding key sociodemographic characteristics and all questionnaire items (Supplementary Table 5). Statistically significant differences were observed for two sociodemographic variables (Living place and Education) and for two items out of 46. The remaining cоmparisоns shоwеd nо significant diffеrences. Althоugh we сannоt entirеly dismiss the pоssibility оf а nоn-respоnse biаs fоr thеsе partiсulаr variables, the оvеrall resеmblancе bеtwеen еarly and lаte respоndеnts indicates that thе risk оf a significаnt оr systеmatic nоn-respоnsе bias is likеly low. Yet despite these limitations, the study also has a number of strengths. In addition to the fact that the questionnaire was developed on the basis of a sound theoretical basis, we consider the fact that the process of developing and validating the questionnaire involved older adults from different contexts (primary care, hospital, and NH) and conditions (including more vulnerable people aged over 85 and less educated) as a strong point.
Some limitations must also be pointed out regarding the BDDQ instrument itself. Firstly, the psychometric results only apply to the French version. A standardized cross-cultural adaptation and psychometric evaluation will be required for the English version before claims of validity can be made. Moreover, it should be noted that three of the eight factors demonstrated somewhat lower internal consistency; however, all exceeded the 0.5 threshold suggested as the minimum for group-level comparison.41 Secondly, the perceived necessity of medication and perceived difficulty of deprescribing scales only consist of two items, which can be a source of weakness or instability,22 although both scales have demonstrated sufficient internal consistency. Thirdly, the eight dimensions of the questionnaire in combination explain slightly less than 60% of the total variance, which suggests that other dimensions may be relevant that are not represented in the questionnaire. Importantly, the analyses did not allow for the development of a scale to measure deprescribing self-efficacy, which seemed to be a theoretically important dimension in deprescribing.14 This limitation may reflect participants’ propensity to overestimate their positive traits and behaviors, thereby inflating their perceived self-efficacy in deprescribing tasks.47 Such bias can introduce minor variations in responses and may ultimately result in the omission of a relevant analytical dimension. While self-efficacy is indeed an important determinant of behavioral change, it is not sufficient on its own to fully explain complex health-related behaviors. Behavioral change results from the interaction of multiple constructs, not from a single factor. The current tool incorporates several additional constructs that are equally important for understanding behavior change in health contexts and that are not captured by existing deprescribing instruments, suсh as sоcial nоrms and pеrcеived suppоrt frоm healthсarе system.
Finally, although reducing the number of items after validation shortens completion time for both older adults and HCPs, the limited time available during HCPs’ consultations highlights the importance of validating a short version of the questionnaire in future studies. Despite these limitations, the BDDQ provides a useful tool for investigating the determinants of patients’ willingness to engage in deprescribing in research and clinical practice. It can serve to investigate how to best involve patients in a deprescribing process, as well as to develop interventions targeting deprescribing behavior to optimize medication use. In clinical practice, the BDDQ may function as a structured entry point for initiating deprescribing discussions, thereby fostering patient engagement and supporting shared decision-making. Accounting for patients’ perceptions, beliefs, and preferences is an important element of the deprescribing process.48 Since older patients, especially, may not always be aware that deprescribing is possible, the role of physicians, and in particular GPs, is crucial.49 GPs can take a lead in deprescribing because of their privileged relationship of trust with the patient, their knowledge of the patient’s medical history and medication regimen, and the fact that they are the first point of contact with the patient and follow the patient over the years.48 Yet, the older patient population is not homogeneous, and each person is unique and has his or her own preferences and needs in terms of medication.50 The tool was therefore developed and validated in French specifically for older adults to maximize comprehension and engagement, with items that were difficult to understand or respond to either removed or reformulated, ensuring accessibility and relevance for this population. The BDDQ may therefore serve as a useful adjunct in clinical practice, facilitating deprescribing in older adults by supporting their engagement in the deprescribing process and identifying the specific factors underlying each patient’s willingness to deprescribe.
Conclusion
Over the past decade, there has been a growing global interest in deprescribing as a strategy to optimize medication use and reduce burden and harm in older adults. Several tools have been developed and validated to support deprescribing decision-making. However, this is the first study that produced a conceptually based and psychometrically validated questionnaire to assess theory-based behavioral determinants of patients’ willingness to engage in deprescribing. This allows for a more comprehensive study of the factors that determine older patients’ deprescribing intentions and behaviors. It can help HCPs to involve older adults and other HCPs in the deprescribing process, as well as to develop deprescribing interventions.
Abbreviations
BMQ, Beliefs about Medicines Questionnaire; CHRHS, Centre Hospitalier Régional Haute Senne; CSPO, Clinique Saint Pierre d’Ottignies; EFA, Exploratory Factor Analysis; GP, General Practitioner; HBM, Health Behavior Model; HBT, Health Behavior Theory; HCP, Healthcare professionals; PAF, Principal Axis Factoring; PATD, Patient Attitudes Towards Deprescribing. PC: Primary care; PMT, Protection Motivation Theory; rPATD, revised version of Patient Attitudes Towards Deprescribing; SCT, Social Cognitive Theory; TPB, Theory of Planned Behavior; WHO, World Health Organization.
Data Sharing Statement
The datasets generated and analyzed during the current study are available in the Dataverse UCLouvain repository, https://doi.org/10.14428/DVN/ISBKR0.
Ethical Approval
Ethics approval was obtained from the Ethics Committees Hospitalo-facultaire Saint-Luc UCL Bruxelles (Belgium) (NUB: B4032023000076) and CHR Haute Senne. Before data collection began, the researchers thoroughly explained the objectives and procedures of the study to all participants. The informed consent form was reviewed with each participant individually, after which written informed consent was obtained. Participation was voluntary and anonymous, and signing the form authorized the use of anonymized data for publication. This study was preregistered on the ClinicalTrial.gov (NCT 06212713), prior to data collection, on 08/01/2024.
Statement of Informed Consent
Participants were informed about the objectives and procedures of the study both verbally and in writing. Verbal and written informed consent were obtained prior to participation in the questionnaire development and validation. All participants were assured of confidentiality and anonymity throughout the study.
Acknowledgments
The authors would like to thank the Centre Hospitalier Régional Haute Senne (CHRHS), Clinique Saint Pierre d’Ottignies (CSPO), Agence Wallonne pour une vie de qualité (AVIQ), Iriscare, Fédération Unessa, the Office des Pharmacies Coopératives de Belgique (OPHACO) and the various integrated care projects (Brusano, Chonicopôle, Chronilux, PACT) for their help in recruiting participants for the validation study. The authors also thank their UCLouvain colleagues, as well as the various HCP and older adults who participated in the discussions during the initial stages of questionnaire development. The first author would like to thank Séverine Guisset (IRSS, UCLouvain) for her valuable support with the statistical analysis. The artificial intelligence tool (DeepL Write) was only used for grammar and spelling corrections. The authors take full responsibility for the content and interpretation of the manuscript. The abstract of this paper was presented at the 17th European Public Health Conference, titled “Development and validation of the Behavioral Determinants of Deprescribing Questionnaire (BDDQ)” as a poster presentation with interim findings. The poster’s abstract was published in the “Poster Abstracts” section of the November 2024 issue of the European Journal of Public Health.
Disclosure
Sara Alves Jorge reports grants from Actions de Recherche Concertées (ARC), Communauté française de Belgique (22/27-124), during the conduct of the study. The authors declare no other conflicts of interest in this work.
References
1. Wu H, O’Donnell LK, Fujita K, Masnoon N, Et Hilmer SN. Deprescribing in the Older Patient: a Narrative Review of Challenges and Solutions. <![CDATA[International Journal of General Medicine]]>. 2021;14:
2. Wastesson JW, Morin L, Tan ECK, Et Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):
3. Pickering AN, Hamm ME, Dawdani A, et al. Older Patient and Caregiver Perspectives on Medication Value and Deprescribing: a Qualitative Study. J Am Geriatr Soc. 2020;68(4):746–18. doi:10.1111/jgs.16370
4. Farrell B, Pottie K, Rojas-Fernandez CH, Bjerre LM, Thompson W, Welch V. Methodology for Developing Deprescribing Guidelines: using Evidence and GRADE to Guide Recommendations for Deprescribing. PLoS One. 2016;11(8):e0161248. doi:10.1371/journal.pone.0161248
5. Thompson W, Reeve E, Moriarty F, et al. Deprescribing: future directions for research. Res Soc Adm Pharm. 2019;15(6):
6. Holmes HM, Todd A. The Role of Patient Preferences in Deprescribing. Clin Geriatr Med. 2017;33(2):165–175. doi:10.1016/j.cger.2017.01.004
7. Reeve E, Wolff JL, Skehan M, Bayliss EA, Hilmer SN, Boyd CM. Assessment of Attitudes Toward Deprescribing in Older Medicare Beneficiaries in the United States. J Amer Med Assoc Intern Med. 2018;178(12):
8. Rosenstock IM. The Health Belief Model and Preventive Health Behavior. Health Educ Monogr. 1974;2(4):
9. Ajzen I. The Theory of Planned Behavior. Organizational Behav Human Decis Processes. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
10. Rogers RW. A Protection Motivation Theory of Fear Appeals and Attitude. Change1. The Journal of Psychology. 1975;91(1):93–114. doi:10.1080/00223980.1975.9915803
11. Bandura A. Organisational applications of social cognitive theory. Aust J Manag. 1988;13(2):275–302. doi:10.1177/031289628801300210
12. Bandura A. Health Promotion by Social Cognitive Means. Health Educ Behav. 2004;31(2):143–164. doi:10.1177/1090198104263660
13. Patton DE, Hughes CM, Cadogan CA, Ryan CA. Theory-Based Interventions to Improve Medication Adherence in Older Adults Prescribed Polypharmacy: a Systematic Review. Drugs Aging. 2017;34(2):
14. Alves Jorge S, Van den Broucke S, Koumba Maguena RJ, Et Spinewine A. Behavioral Determinants of Older Adults’ and Caregivers’ Willingness to Deprescribe: a Systematic Review. Public Health Nurs. 2024;2024:1–31. doi:10.1111/phn.13516
15. Reeve E, Shakib S, Hendrix I, Roberts MS, Wiese MD. Development and validation of the patients’ attitudes towards deprescribing (PATD) questionnaire. Int J Clin Pharm. 2013;35(1):
16. Reeve E, Low LF, Shakib S, Hilmer SN. Development and validation of the Revised Patients’ Attitudes Towards Deprescribing (rPATD) Questionnaire: versions for older adults and caregivers. Drugs Aging. 2016;33(12):
17. Linsky A, Simon SR, Bokhour B. Patient perceptions of proactive medication discontinuation. Patient Educ. 2015;98(2):
18. Roux B, Sirois C, Niquille A, et al. Cross-cultural adaptation and psychometric validation of the revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire in French. Res Soc Adm Pharm. 2021;17(8):1453–1462. doi:10.1016/j.sapharm.2020.11.004
19. Horne R, Weinman J, Hankins M. The Beliefs About Medicines Questionnaire: the Development and Evaluation of a New Method for Assessing the Cognitive Representation of Medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
20. Lawshe CH. A Quantitative Approach to Content Validity. Pers Psychol. 1975;28(4):563–575. doi:10.1111/j.1744-6570.1975.tb01393.x
21. Gilbert G, and Prion S. Making Sense of Methods and Measurement: lawshe’s Content Validity Index. Clin Simul Nurs. 2016;12: 530‑531229–338. doi:10.1016/j.ecns.2016.08.002
22. Costello AB, Osborne J. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(7):1–9. doi:10.7275/JYJ1-4868
23. Conner M, Norman P.. Psychol Health (:). 2017;32: . doi:10.1080/08870446.2017.1336240
24. Peters GJY. A practical guide to effective behavior change: how to identify what to change in the first place. Eur Health Psychol. 2014;16(5):142–155. doi:10.31234/osf.io/hy7mj
25. Salovey P, and Birnbaum D. Influence of mood on health-relevant cognitions. J Pers Soc Psychol. 1989;57(3):539–551. doi:10.1037/0022-3514.57.3.539
26. Dijkstra A, Jaspers M, and van Zwieten M. Psychiatric and psychological factors in patient decision making concerning antidepressant use. J Consult Clin Psychol. 2008;76(1):149–157. doi:10.1037/0022-006X.76.1.149
27. Rababa M, Rababa’h A. Community-dwelling older adults’ awareness of the inappropriate use of proton pump inhibitors. BMC Geriatr. 2020;20(1):431. doi:10.1186/s12877-020-01844-w
28. Reeve E, Low L, Hilmer SN. Attitudes of older adults and caregivers in Australia toward deprescribing. J Am Geriatr Soc. 2019;67(6):1204–1210. doi:10.1111/jgs.15804
29. Rozsnyai Z, Jungo KT, Reeve E, et al. What do older adults with multimorbidity and polypharmacy think about deprescribing? The LESS study - a primary care-based survey. BMC Geriatr. 2020;20(1):435. doi:10.1186/s12877-020-01843-x
30. Sake FTN, Wong K, Bartlett DJ, Saini B. Benzodiazepine use risk: understanding patient specific risk perceptions and medication beliefs. Res Soc Adm Pharm. 2019;15(11):1317–1325. doi:10.1016/j.sapharm.2018.12.007
31. Mardia KV. Measures of Multivariate Skewness and Kurtosis with Applications. Biometrika. 1970;57(3):519–530. doi:10.2307/2334770
32. Bélanger L, Morin CM, Bastien C, and Ladouceur R. Self-Efficacy and Compliance With Benzodiazepine Taper in Older Adults With Chronic Insomnia. Health Psychol. 2005;24: 281–287. doi:10.1037/0278-6133.24.3.281
33. Yong AG, Pearce S. A Beginner’s Guide to Factor Analysis: focusing on Exploratory Factor Analysis. Tutorials Quant Methods Psychol. 2013;9(2):79–94. doi:10.20982/tqmp.09.2.p079
34. Dunn TJ, Baguley T, and Brunsden V. From alpha to omega: a practical solution to the pervasive problem of internal consistency estimation. Br J Psychol. 2014;105(3):399–412. doi:10.1111/bjop.12046
35. O’Connor K, Marchand A, and Brousseau L, et al. Cognitive-behavioral, pharmacological and psychosocial predictors of outcome during tapered discontinuation of benzodiazepine. Clin Psychol Psychother. 2008;15(1):1–14. doi:10.1002/cpp.556
36. O’Connor KP, Marchand A, and Bélanger L, et al.. Addict Behav (:). 2004;29: . doi:10.1016/j.addbeh.2004.01.001
37. Lenzner T, Hadler P, and Neuert C. An experimental test of the effectiveness of cognitive interviewing in pretesting questionnaires. Qual Quant. 2023;57: 3199–3217. doi:10.1007/s11135-022-01489-4
38. Sapnas KG, and Zeller RA. Minimizing Sample Size When Using Exploratory Factor Analysis for Measurement. J Nurs Meas. 2002;10(2):
39. Sommer L. The Theory of Planned Behaviour and the Impact of Past Behaviour. Int Bus Econ Res J. 2011;10(1):91–110. doi:10.19030/iber.v10i1.930
40. Korkeila K, Suominen S, and Ahvenainen J, et al. Non-response and related factors in a nation-wide health survey. Eur J Epidemiol. 2001;17: 991–999431. doi:10.1023/a:1020016922473
41. Howard M. A Review of Exploratory Factor Analysis (EFA) Decisions and Overview of Current Practices: what We Are Doing and How Can We Improve? Int J Hum -Comput InteractPract Assess Res Eval. 2015;32: 1509141428340001–9. doi:10.1080/10447318.2015.1087664
42. MacCallum RC, Widaman KF, Zhang S, and Hong S. Sample size in factor analysis. Psychol Methods. 1999;4(1):84–99. doi:10.1037/1082-989X.4.1.84
43. Hatem G, Zeidan J, Goossens M, and Moreira C. Normality Testing Methods And The Importance of Skewness and Kurtosis in Statistical Analysis. BAU J Sci Technol. 2022;3(2). doi:10.54729/KTPE9512
44. McNeish D. Thanks coefficient alpha, we’ll take it from here. Psychol Methods. 2018;23(3):412–433. doi:10.1037/met0000144
45. Ten Wolde GB, Dijkstra A, Empelen PV, Neven AK, and Zitman FG. Social-cognitive predictors of intended and actual benzodiazepine cessation among chronic benzodiazepine users. Addict Behav. 2008;33(9):1091–1103. doi:10.1016/j.addbeh.2008.02.003
46. Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229–338. doi:10.1023/A:1023254226592
47. Alicke MD. Global self-evaluation as determined by the desirability and controllability of trait adjectives. J Pers Soc Psychol. 1985;46(6):1621–1630. doi:10.1037/0022-3514.49.6.1621
48. Jansen J, Naganathan V, Carter SM, et al. Too much medicine in older people? Deprescribing through shared decision making. Br Med J. 2016;353: i2893. doi:10.1136/bmj.i2893
49. Alrawiai S. Deprescribing, shared decision-making, and older people: perspectives in primary care. J Pharm Policy Pract. 2023;16(1):153. doi:10.1186/s40545-023-00671-9
50. Weir KR, Ailabouni NJ, Schneider CR, Hilmer SN, Reeve E. Consumer Attitudes Towards Deprescribing: a Systematic Review and Meta-Analysis. J Gerontol a Biol Sci Med Sci. 2021;77(5):
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.