Back to Journals » Drug Design, Development and Therapy » Volume 20
Development and Validation of an HPLC-MS/MS Method for Pharmacokinetic Evaluation of Tofacitinib/Simvastatin Compound Ointment in Rats
Authors Wang S, Zhang C, Li J, Li G ![]() , Qi Y
, Qi Y ![]()
Received 22 September 2025
Accepted for publication 12 February 2026
Published 3 March 2026 Volume 2026:20 562181
DOI https://doi.org/10.2147/DDDT.S562181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Shengnan Wang,1 Chenxiao Zhang,2 Jiaxin Li,1 Guofei Li,2 Yingjie Qi1
1Department of Pharmacy, Cancer Hospital of China Medical University, Liaoning Cancer Hospital & Institute, Shenyang, Liaoning, People’s Republic of China; 2Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Yingjie Qi, Department of Pharmacy, Cancer Hospital of China Medical University, Liaoning Cancer Hospital & Institute, Number 44 Xiaoheyan Road, Dadong District, Shenyang, Liaoning, 110042, People’s Republic of China, Email [email protected]
Propose: Oxidative stress and immune dysfunction are closely associated with the onset and progression of vitiligo. Therefore, simultaneously regulating these two key pathological processes to achieve synergistic therapy is a practically feasible strategy. Based on this rationale, we previously developed a topical ointment co-loaded with antioxidant simvastatin and immunosuppressant tofacitinib, and evaluated its therapeutic potential for vitiligo. However, the lack of a bioanalytical method for simultaneous in vivo quantification of the two drugs has hindered further pharmacodynamic and pharmacokinetic studies of the formulation. The present study aimed to establish and validate an HPLC-MS/MS method for simultaneous determination of their in vivo concentrations, to support pharmacokinetic investigations of the ointment in rats.
Methods: : Chromatographic separation was performed on a ZORBAX Eclipse C18 column (50.0 × 3.5 mm, 1.7 μm) using a gradient elution program. The mobile phase comprised phase A (20 mM ammonium acetate aqueous solution) and phase B (acetonitrile), with a constant flow rate of 0.4 mL/min. The method was fully validated in strict accordance with the bioanalytical method validation guidelines specified in the Chinese Pharmacopoeia, including evaluations of specificity, calibration curve and linear range, lower limit of quantification, carryover effect, precision, recovery, matrix effect, stability, and dilution integrity.
Results: The results demonstrated that the method met all validation criteria and was suitable for pharmacokinetic studies. Pharmacokinetic data showed that, compared with oral gavage, the 24 h bioavailability of tofacitinib and simvastatin after topical administration was only 7.1% and 5.2%, respectively. This low systemic exposure indicated that the ointment formulation could effectively reduce the potential toxicity caused by excessive drug absorption into the circulation.
Keywords: HPLC-MS/MS, methodology validation, simvastatin/tofacitinib ointment, vitiligo, pharmacokinetics
Introduction
Vitiligo is characterized by progressive loss of epidermal melanocytes, leading to well-demarcated hypopigmented macules/patches.1,2 The visible cutaneous manifestations impose significant psychological distress on patients and their families, markedly impairing quality of life.3 Consequently, developing effective strategies to halt disease progression or achieve sustained remission remains an urgent unmet medical need. The pathogenesis of vitiligo remains incompletely elucidated, with current research primarily focusing on genetic predisposition, environmental triggers, oxidative stress, dysregulated immune responses and neural hypothesis.4,5 In the above pathogenesis, oxidative stress and immune imbalance are recognized as key factors.6–8 Therefore, although the exact relationship between oxidative stress and immune imbalance is not clear, it has become a research hotspot in the field of vitiligo.
The Nuclear factor erythroid 2-related factor 2/antioxidant response element (Nrf2/ARE) signaling pathway plays an important role in protecting melanocytes from oxidative stress damage.9,10 Many antioxidants targeting the NRF2/ARE pathway have been discovered, such as simvastatin, aspirin, berberine, etc.11,12 Among them, simvastatin has shown promising application prospects. Research has found that simvastatin can increase the activity of melanocytes, reduce H2O2 mediated cell apoptosis, and protect melanocytes from oxidative stress damage.13,14 At present, research on simvastatin for the treatment of vitiligo has been primarily focused on the animal level. However, clinical trials have also confirmed that systemic and symmetrical repigmentation was observed in some patients treated with simvastatin (40 mg/d) combined with oral alendronate sodium. It is widely believed that high doses of simvastatin have a more significant therapeutic effect on vitiligo, but excessive doses can easily lead to serious adverse reactions such as rhabdomyolysis and liver damage.15 The janus kinase-ignal transducer and activator of transcription (JAK-STAT) signaling pathway is a critical signal transduction cascade for the occurrence and development of immune-mediated inflammatory diseases.16,17 While the IFN-γ-JAK-STAT signaling pathway is the most important pathway in the pathogenesis of vitiligo, especially mediating the recruitment of cytotoxic CD8+ T lymphocytes.18,19 JAK inhibitors exert their inhibitory effect on the selective assault of CD8⁺ T cells against melanocytes through the suppression of the IFN-γ-JAK-STAT pathway. At present, non selective inhibitors such as tofacitinib, rutinib, and baritinib, as well as selective inhibitors upatinib and abuxitinib, have been widely used in clinical practice.20–22 Our preliminary research found that ointment loaded with simvastatin and tofacitinib can effectively inhibit the progression of vitiligo, and the two have a significant synergistic effect.
For topical ointment formulations, it is essential to ensure effective drug penetration across the stratum corneum while minimizing systemic absorption into circulation. On the one hand, the therapeutic effect can be improved by increasing the drug concentration in the diseased tissue; On the other hand, potential drug toxicity can be reduced by decreasing the proportion of drugs entering the bloodstream, thereby increasing patient tolerance. Therefore, the aim of this paper was to develop a bioanalytical method for simultaneous quantification of simvastatin and tofacitinib in plasma and apply it to pharmacokinetic studies of the simvastatin/tofacitinib ointment. Generally, various analytical techniques including high-performance liquid chromatography (HPLC), high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS), immunoassays, and ultraviolet spectrophotometry, can be employed for determining drug concentrations in biological matrices.23,24 Currently, immunoassays and ultraviolet spectrophotometry are rarely used for in vivo drug concentration analysis. Meanwhile, HPLC method is also greatly restricted in its application due to its inability to simultaneously determine multiple drugs and their metabolites. While HPLC-MS/MS method has emerged as the most widely adopted method due to its superior attributes, such as high sensitivity, high specificity, high throughput, and capability for simultaneous quantification of multiple drugs and their metabolites.25,26 Firstly, HPLC-MS/MS technology exhibits extremely high specificity, enabling the simultaneous determination of multiple drugs and their metabolites with minimal interference from matrices and metabolites. This saves substantial human and material resources in practical applications, greatly improving work efficiency—for instance, in therapeutic drug monitoring (TDM). Secondly, HPLC-MS/MS technology boasts high sensitivity, with the lower limit of quantification (LLOQ) for most drugs reaching the picogram (pg) level or even lower. This holds significant clinical value for measuring drug concentrations at target sites, such as cerebrospinal fluid (CSF), pus, and synovial fluid, and is particularly suitable for investigating the correlation between dosage, plasma drug concentration, target site concentration, and therapeutic efficacy. Thirdly, HPLC-MS/MS technology features high throughput, making it especially applicable for large-sample-size testing. Additionally, HPLC-MS/MS technology can effectively compensate for the shortcomings of immunoassays, ultraviolet spectrophotometry, and HPLC method. Consequently, HPLC-MS/MS method is considered as the gold standard for analyzing small-molecule drugs in vivo. Hence, an HPLC-MS/MS method was established in this study to simultaneously determine the plasma concentrations of simvastatin and tofacitinib in vivo, with a full set of method validation performed to evaluate parameters such as specificity, linear rang and standard curve, residual effects, recovery rate, precision, stability, matrix effects, and dilution reliability based on the Chinese pharmacopoeia guidelines for validation of quantitative analytical methods for biological samples. Moreover, the method was applied to investigate the pharmacokinetics of the simvastatin/tofacitinib ointment. Rat pharmacokinetic data revealed that the 24 h bioavailability of tofacitinib and simvastatin after topical administration was only 7.1% and 5.2%, respectively, compared to oral gavage. This indicates effective drug retention in localized lesional skin tissues, where elevated drug concentrations not only enhance therapeutic efficacy but also minimize systemic adverse effects associated with significant drug absorption into circulation. In conclusion, the developed method complies with the requirements of bioanalytical method validation guidelines and can accurately determine the concentrations of simvastatin and tofacitinib in rats. Of course, this study also had certain limitations. For instance, it did not systematically investigate the relationship between the administered dosage and the drug concentration in the plasma, nor did it examine the differences in drug disposition between vitiligo model mice and normal mice; additionally, isotopic internal standards were not selected for the experiment. To some extent, these factors had compromised the integrity of the experiment.
Methods
Experimental Reagents
Tofacitinib (purity 99.7%) and diazepam (purity 99.9%) were purchased from Selleck & bimake (Texas, USA). Simvastatin (purity 99.5%) and lovastatin (purity 99.6%) were purchased from the National Institutes for Food and Drug Control (Beijing, China). Reagents used in this study were as follows: HPLC-grade water, methanol and acetonitrile (Fisher Scientific, Fair Lawn, NJ, USA); formic acid and ammonium acetate (Sigma-Aldrich, St. Louis, USA); and methyl tert-butyl ether (Concord Technology Co., Ltd, Tianjin, China). The chemical structures of four compounds, namely tofacitinib, simvastatin, diazepam and lovastatin, are illustrated in Figure 1.
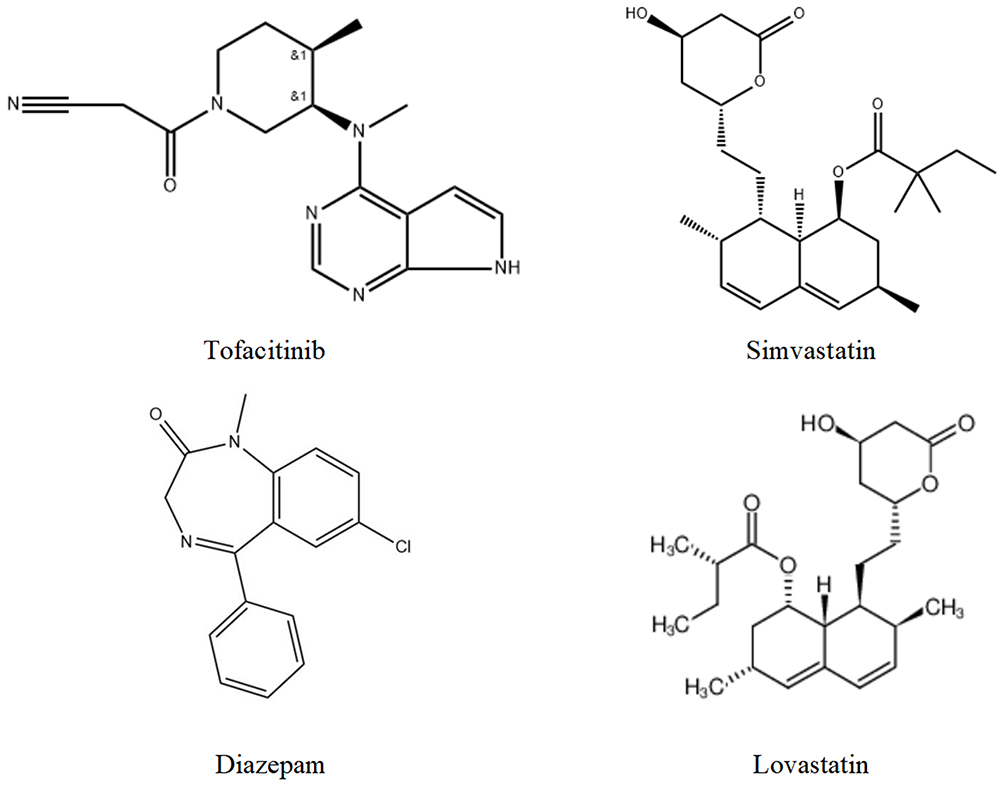 |
Figure 1 The structure diagram of tofacitinib, simvastatin, diazepam and lovastatin. |
Equipment and Conditions
The Jasper™ HPLC system, composed of SCIEX Dx Sampler, SCIEX Dx Pump (x2), SCIEX Dx Controller, SCIEX Dx Oven, and SCIEX Dx Degasser, was used for the separation of the analytes and internal standards (IS). Tofacitinib, simvastatin, diazepam and lovastatin were separated via a ZORBAX Eclipse C18 column (50.0 × 3.5 mm, 1.7 μm) under 35 °C. Two mobile phase components were employed: eluent A was aqueous 20 mmol ammonium acetate solution, and eluent B was pure acetonitrile. The elution method was gradient elution, and the conditions were shown in Table 1. The injection volume was 2.0 μL.
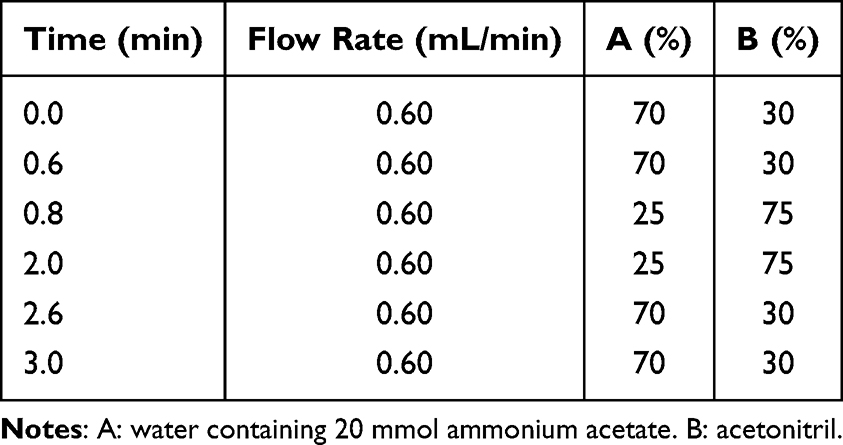 |
Table 1 Gradient Condition of HPLC |
Mass spectrometric analysis of the four analytes (tofacitinib, simvastatin, diazepam, lovastatin) was performed on an AB SCIEX Triple Quad™ 4500MD instrument fitted with an electrospray ionization (ESI) detector. The ionization mode of tofacitinib, simvastatin, diazepam and lovastatin was positive. The MRM transition of tofacitinib, simvastatin, diazepam and lovastatin was m/z 313.2/149.2, 436.4/199.1, m/z 285.1/193.0 and 405.2/199.1 respectively. The main MS parameters were displayed in Table 2. Other optimized mass spectrometry parameters were set as follows: source temperature (TEM) at 450 °C, entrance potential (EP) at 30, curtain gas (CUR) at 50, turbo gas 2 (GS2) at 45, and turbo gas 1 (GS1) at 45. Data acquisition was performed using Analyst software (Version 1.6.2).
 |
Table 2 MS Parameters of Tofacitinib, Simvastatin, Diazepam and Lovastatin |
Stock Solutions, Quality Control Specimens and Calibration Reference Standards
The reference standards of tofacitinib, simvastatin, diazepam and lovastatin were individually dissolved in methanol to yield stock solutions with a final concentration of 100.0 μg/mL. Then, the calibration curve was prepared by diluting tofacitinib and simvastatin stock solution with methanol to obtain a series of tofacitinib and simvastatin mixed standard solutions with concentrations of 2.0, 8.0, 20.0, 80.0, 200.0, 800.0, 2000.0 ng/mL (tofacitinib) and 10.0, 40.0, 100.0, 400.0, 1000.0, 4000.0, 10,000.0 ng/mL (simvastatin). 100 ng/mL diazepam and lovastatin mixed solutions were obtained by diluting the diazepam and lovastatin stock solution respectively. The LLOQ was 2.0 ng/mL for tofacitinib, 10.0 ng/mL for simvastatin.
The stability of the HPLC-MS/MS method and the reliability of the extraction method were evaluated using QC samples, which consisted of high-concentration, medium-concentration, low-concentration QC samples and the lower limit of quantification (LLOQ). For quality control purposes, concentrations of 1600.0 ng/mL, 100.0 ng/mL, 5.0 ng/mL, and 2.0 ng/mL were assigned to tofacitinib QC samples, while simvastatin QC samples were prepared at concentrations of 8000.0 ng/mL, 500.0 ng/mL, 20.0 ng/mL, and 10.0 ng/mL. Diazepam and lovastatin was used as IS for tofacitinib and simvastatin respectively, and the concentration was 100 ng/mL.
Plasma and Skin Sample Processing Method
After completion of blood collection for the pharmacokinetic experiment, the rats were euthanized. First, the residual ointment on the back was wiped off with dry cotton. Next, the skin was swabbed with cotton soaked in normal saline, followed by repeated wiping with dry cotton for 5 times. The skin at the administration site was excised and weighed. The minced skin samples were mixed with 2 mL of methanol, subjected to high-speed shear homogenization for 4 min, and then centrifuged at 15000 r/min for 10 min to obtain the skin homogenate.
Aliquots of 100.0 μL plasma or skin homogenate were transferred to 7.0 mL screw-capped EP tube, 20.0 μL of internal standard solution, 150.0 μL acetonitrile, and 100.0 μL mobile phase (20.0 mM ammonium acetate solution) were added sequentially. The mixture was vortex-mixed for 5 mins. Subsequently, 3 mL methyl tert-butyl ether was added for liquid-liquid extraction, followed by 8 mins of vortexing and centrifugation at 4000 rpm for 5 mins. After this, the supernatant was carefully transferred to 10 mL conical-bottom EP tube. The extract was evaporated to dryness under a gentle nitrogen stream at 40°C. The residue was reconstituted in 200.0 μL acetonitrile with 5 min vortex-mixing, then centrifuged at 15,000 rpm for 5 mins to remove particulate matter. Ultimately, aliquots of the supernatant were injected into the HPLC-MS/MS instrument to perform quantitative analysis.
Method Validation
Validation of the established HPLC-MS/MS method was performed following the bioanalytical method validation criteria outlined in the Chinese Pharmacopoeia.27
Specificity
A pooled blank plasma sample (100.0 μL), prepared by combining plasma from six rats, was processed following the “Plasma samples processing method” protocol. A 2.0 μL aliquot was injected to establish the baseline chromatographic profile. A certain concentration of simvastatin, tofacitinib and mixed internal standard solution were added to blank plasma, following the procedure “Plasma samples processing method”, and 2.0 μL aliquot was injected to obtain the chromatogram. Plasma samples collected post-dosing were processed as the “Plasma samples processing method” protocol. And then 2.0 μL of the final extract was injected for HPLC-MS/MS quantification.
Linearity, LLOQ and Carryover
Linear ranges were established at 2.0–2000.0 ng/mL for tofacitinib and 10.0–10,000.0 ng/mL for simvastatin. Validation requirements specified that recalculated calibration standard concentrations must be within ±15% of the labeled values, while the LLOQ was permitted a wider deviation of ±20%. For this assay, the LLOQ was designated as the minimum concentration point of the standard curve. Carryover effects, which posed a notable threat to determination accuracy, were thus subject to comprehensive evaluation and mitigation. Here, the carryover effect was evaluated by injecting a blank plasma sample after injecting the sample with the highest concentration of the standard curve. It was required that and the carryover should be less than ± 20% of LLOQ and should not exceed 5% of ISs.
Accuracy and Precision
The degree of closeness between an analyte’s detected concentration and its nominal concentration is defined as accuracy, while the degree of reproducibility of concentration values obtained from repeated determinations of the analyte is referred to as precision. Precision and accuracy were expressed as relative standard deviation (RSD%) and relative error (RE%) respectively. In this article, Accuracy and precision were investigated by determining six repeated measurements of the plasma samples at HQC, MQC, LQC, and LLOQ on three consecutive days. Acceptance criteria stipulated that RSD and RE values must not exceed ±15%, with a more lenient threshold of ±20% established for the LLOQ.
Extraction Recovery and Matrix Effect
Extraction recovery and matrix effect of tofacitinib and simvastatin were assessed at the concentration of LLOQ and three QCs respectively. Recovery was evaluated by comparing the peak area of the extracted plasma sample to that of blank plasma spiked with a tofacitinib and simvastatin postextraction. Matrix effect of endogenous components present in plasma was assessed by comparing peak areas of tofacitinib or simvastatin existed in extracted blank plasma with the peak areas of tofacitinib or simvastatin diluted in water.
Stability
To comprehensively characterize the stability profile of tofacitinib and simvastatin in rat plasma, QC samples were subjected to four stability tests: short-term storage at room temperature for 12 h, long-term storage at −20 °C for 30 d, three freeze-thaw cycles between −20.0 °C and room temperature, and autosampler storage at 4 °C for 24 h. All stability results were required to yield an RE below 15%.
Dilution Integrity
Two complementary experiments were conducted to assess dilution integrity: plasma samples with concentrations higher than the ULOQ were diluted with blank plasma to the corresponding HQC level, using 5-fold and 30-fold dilution factors that could cover 100% of the study samples. For all dilution tests, the relative error between the measured concentration and the theoretical concentration was required to be less than 15.0%.
Application
The Preparation of Simvastatin/Tofacitinib Ointment
The formulation and preparation process of the ointment were as follows: 70.5% yellow petrolatum, 5% liquid paraffin, 15% phospholipids and 2.5% cholesterol were mixed thoroughly and then heated to 85 °C for melting. After the molten matrix was gradually cooled down to 45 °C, 5% simvastatin and 2% tofacitinib were added. The mixture was stirred for 3 hours and subsequently cooled to room temperature to obtain the final preparation.
Animal Experimental Protocol
Male Sprague-Dawley rats (body weight ≈200 g) were randomly allocated into four groups (n=6 per group) following a 12 h fasting period with free access to water prior to experimentation. Group 1: Simvastatin suspension was administered to rats by gavage at a dose of 20 mg/kg. Group 2: Tofacitinib suspension was administered to rats by gavage at a dose of 10 mg/kg. Group 3: Co-administered both suspensions by gavage (simvastatin 20 mg/kg + tofacitinib 10 mg/kg) orally. Group 4: Pretreated with depilatory cream on dorsal skin (5×5 cm2) 24 h prior to application of 0.02g simvastatin/tofacitinib ointment (equivalent to the gavage dose) and fixed with breathable surgical tape. Both simvastatin and tofacitinib suspensions were prepared in 0.5% (w/v) sodium methylcellulose aqueous vehicle at final concentrations of 4 mg/mL and 2 mg/mL, respectively. Following drug administration, 0.3 mL blood samples were collected via the orbital venous plexus at 0.25, 0.5, 0.75, 1, 2, 3, 4, 6, 8, 12, and 24 h, respectively. Each sample was immediately transferred to pre-chilled, heparinized 1.5 mL polypropylene microcentrifuge tubes. The blood samples were centrifuged at 4000 rpm for 5 mins and processed according to the validated “Plasma and Skin Sample Processing Method”. Meanwhile, skin samples were collected from the rats upon completion of the experiment and processed for subsequent analysis in accordance with the validated “Plasma and Skin Sample Processing Method”. Prior to the initiation of the experiments, ethical clearance was granted by the Ethics Committee of China Medical University (Ethics Approval No. 2023PS763K). The committee strictly complies with the national standard Guidelines for the Ethical Review of Experimental Animal Welfare (GB/T 35892–2018), jointly promulgated by the General Administration of Quality Supervision, Inspection and Quarantine of the People’s Republic of China and the Standardization Administration of China, as well as the Guidelines for the Care and Use of Laboratory Animals formulated by the International Association for the Study of Pain. We euthanized the rats using isoflurane after the experiment. The specific steps were to place the rats in an anesthesia machine and continuously increase the concentration of isoflurane until the rats’ breathing and heartbeat stopped.
Processing and Assessment of Pharmacokinetic Parameters
Upon finishing the pharmacokinetic study in rats and detecting the plasma concentrations of each group at various time points, the resultant data were subjected to processing and statistical analysis with the aid of DAS 3.0 software (Drug and Statistics Software).
Results and Discussion
Method Optimization
In this study, we first systematically optimized the chromatographic conditions based on retention time, peak shape of the chromatographic peaks and matrix effect. It was demonstrated that the use of a ZORBAX Eclipse C18 column (50.0 mm × 3.5 mm, 1.7 μm), combined with a mobile phase composed of acetonitrile and 20 mmol ammonium acetate aqueous solution and a column temperature maintained at 35 °C, yielded sharp, symmetrical chromatographic peaks. While gradient elution method can provide appropriate retention time for tofacitinib, simvastatin, diazepam and lovastatin, and the conditions were demonstrated in Table 1. The retention times of tofacitinib, simvastatin, diazepam and lovastatin were 1.87 min, 1.96 min, 2.16 and 1.82 min respectively.
Next, we systematically optimized the mass spectrometry conditions such as the declustering voltage, ionization mode, curtain gas, collision energy, and ion source temperature, etc. to obtain highly stable and sensitive analyte signals. Optimization experiments revealed that the signals corresponding to tofacitinib, simvastatin, diazepam and lovastatin exhibited greater intensity and stability in positive ion ionization mode compared with negative ion ionization mode. The mass spectrometry parameters and the final ion pairs were demonstrated in Table 2, and the chromatograms of tofacitinib, simvastatin, diazepam and lovastatin were shown in Figure 2. The same mass spectrometry parameters were as follows: CUR:45, TEM:450 °C, GS1:45, GS2:50, CAD: Medium, IS:5000, EP:25, CXP:18.
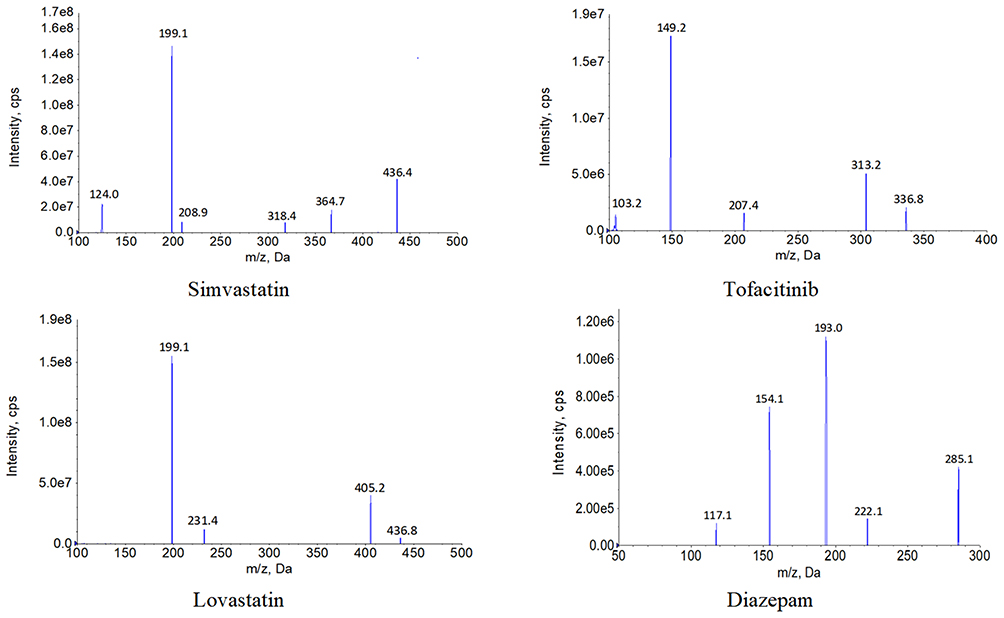 |
Figure 2 The diagrams of daughter scan of tofacitinib, simvastatin, diazepam and lovastatin. |
In addition to chromatographic and mass spectrometry conditions, the extraction method of the analytes was also crucial, as it was closely related to the matrix effect, extraction recovery, LLOQ and other indicators of the HPLC-MS/MS method. Three commonly utilized approaches for plasma sample processing have been identified to date: solid-phase extraction, protein precipitation, and liquid-liquid extraction. The three extraction methods each had their own advantages and disadvantages. For example, the precipitation protein method was relatively simple, but the purity of the samples was low, which can easily contaminate the ion source of the mass spectrometer and produce matrix effects; Solid phase extraction can obtain relatively pure samples, but it had higher requirements for equipment and consumables than the other two methods; Liquid-liquid extraction can also obtain pure samples, but the commonly used extraction solvents were organic solvents, which can easily pollute the environment and pose certain risks. Therefore, we should choose an appropriate extraction method based on the properties of the analytes. In this paper, we found that using acetonitrile to precipitate proteins in plasma samples, followed by liquid-liquid extraction with methyl tert butyl ether, resulted in higher recovery rates and lower matrix effects, which can meet the experimental requirements.
Method Validation
Specificity
The specificity validation results confirmed that endogenous components in the plasma exerted no interference on the quantitative determination of tofacitinib, simvastatin, diazepam and lovastatin. It indicated that the matrix in the plasma could be largely removed thoroughly by precipitate proteins and liquid-liquid extraction process. The typical chromatograms of tofacitinib, simvastatin, diazepam, lovastatin and blank plasma were demonstrated in Figure 3.
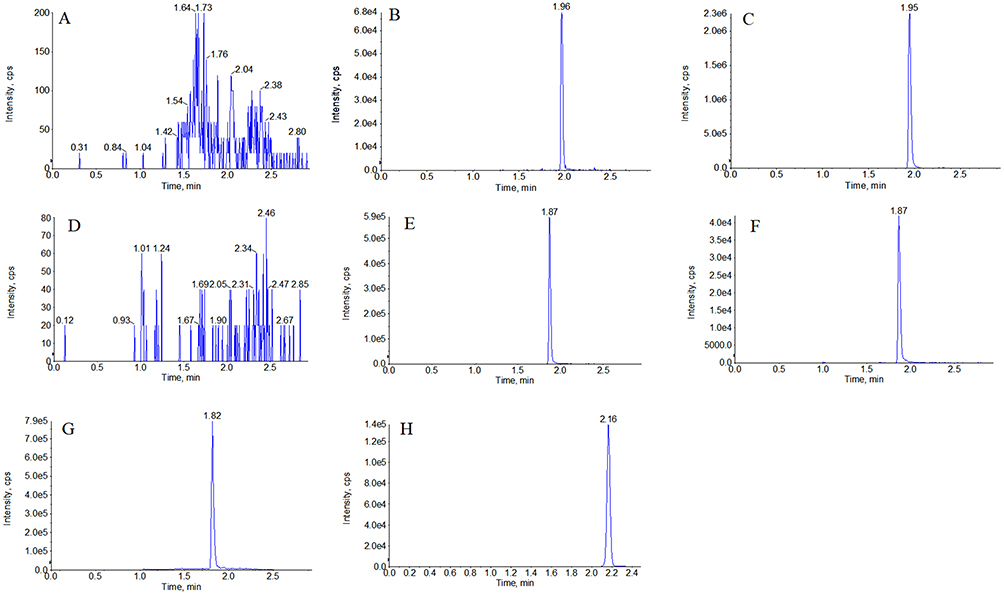 |
Figure 3 Typical chromatogram of tofacitinib, simvastatin, diazepam and lovastatin ((A), Blank plasma-simvastatin; (B), Simulated plasma-simvastatin; (C), Rat plasma-simvastatin; (D), Blank plasma-tofacitinib; (E), Simulated plasma-tofacitinib; (F), Rat plasma-tofacitinib; (G), Simulated plasma-lovastatin; (H), Simulated plasma-diazepam). |
Linearity and LLOQ
The linear range of tofacitinib and simvastatin was set to be 2.0~2000.0 ng/mL and 10.0~10,000.0 ng/mL, and the typical equation of the calibration curve was as follows: y=0.7963x+0.8628 (r=0.9993, tofacitinib) and y=0.9805x+07219 (r=0.9991, simvastatin). The LLOQ of tofacitinib and simvastatin was 2.0 ng/mL and 10.0 ng/mL respectively.
Precision and Accuracy
The results of the accuracy and precision of the established HPLC-MS/MS method were displayed in Table 3. It can be seen that the accuracy, intra-day precision, and inter-day precision of tofacitinib and simvastatin were all less than 12.5%, which met the requirements. In other words, the method had satisfactory precision and accuracy and can be used for the determination of tofacitinib and simvastatin.
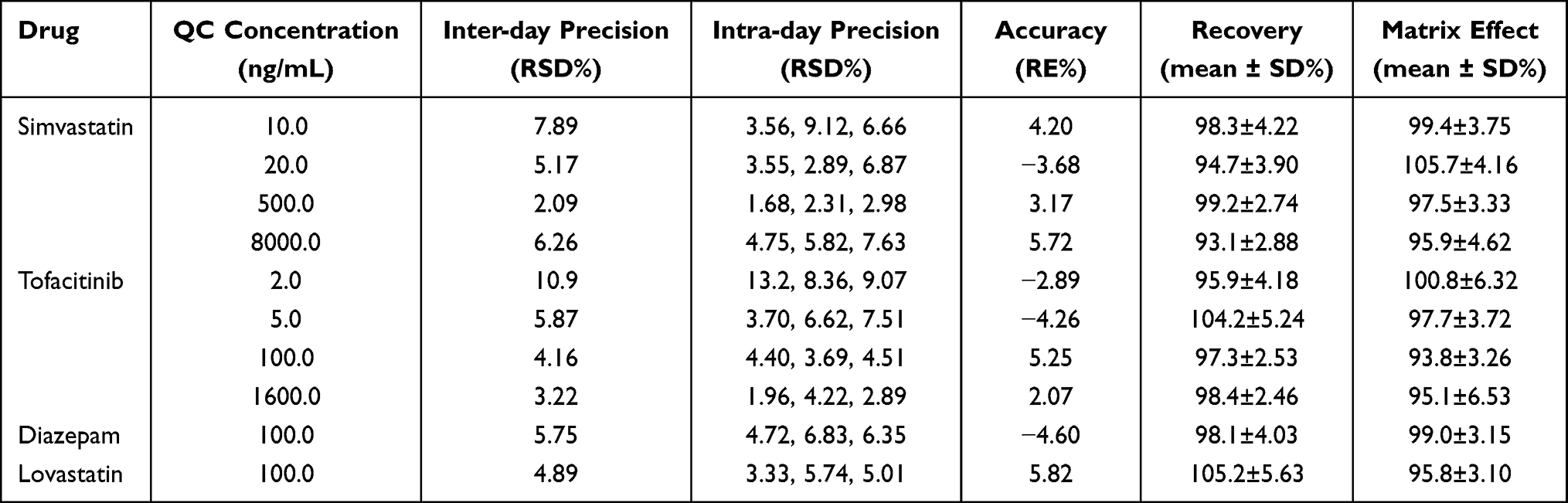 |
Table 3 Methodology Verification Results of Precision, Accuracy, Recovery and Matrix Effect |
Recovery and Matrix Effect
Data on the recovery rate and matrix effect are presented in Table 3. Our experiments confirmed that the extraction recoveries of tofacitinib, simvastatin, diazepam and lovastatin ranged from 96.1% to 106.3%, 94.9% to 112.5%, 95.8% to 108.9% and 93.2% to 103.6%, respectively. Matrix effect values for the four target analytes (tofacitinib, simvastatin, diazepam, lovastatin) were measured as 97.8–108.4%, 91.0–110.7%, 94.5–102.2% and 95.8–107.0%, respectively, and these results were in compliance with the methodological validation requirements. These findings fully confirmed the successful optimization of chromatographic, mass spectrometric and sample extraction procedures, and verified that matrix components (eg, phospholipids and proteins) in rat plasma exerted no interference on the ionization efficiency or accurate quantitative determination of tofacitinib, simvastatin, diazepam and lovastatin.
Stability
As illustrated in Table 4, the freeze-thaw stability, autosampler stability, and long-term stability of the plasma samples all satisfied the predefined validation criteria, indicating that tofacitinib, simvastatin, diazepam and lovastatin possessed favorable stability profiles under the tested conditions.
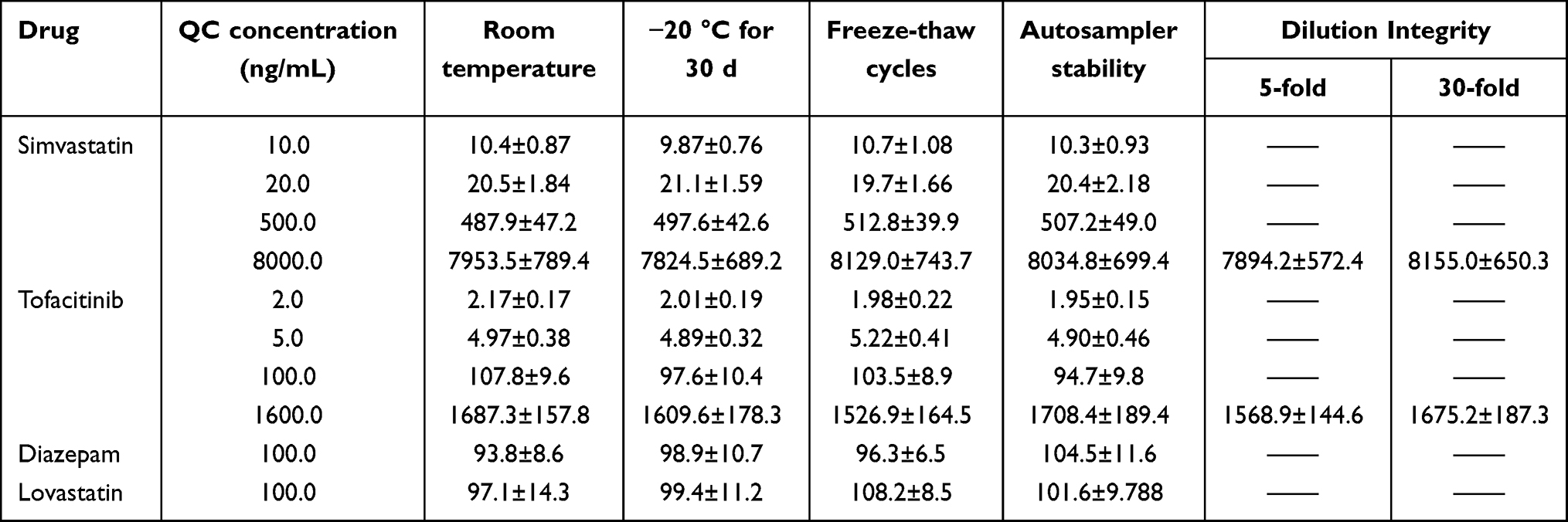 |
Table 4 Stability of Tofacitinib, Simvastatin, Diazepam and Lovastatin Under Various Storage Conditions (Mean ± SD, n=4) |
Dilution Integrity
The outcomes of the dilution integrity test are presented in Table 4. These findings demonstrated that the RE values for all dilution experiments did not exceed 11.2%, confirming that the quantification of plasma samples was not compromised by the dilution process.
Application
The validated HPLC-MS/MS method was employed for the quantitative determination of tofacitinib, simvastatin, diazepam and lovastatin in plasma samples, with the corresponding pharmacokinetic parameters and drug concentration-time curves presented in Tables 5 and 6, Figures 4 and 5, respectively.
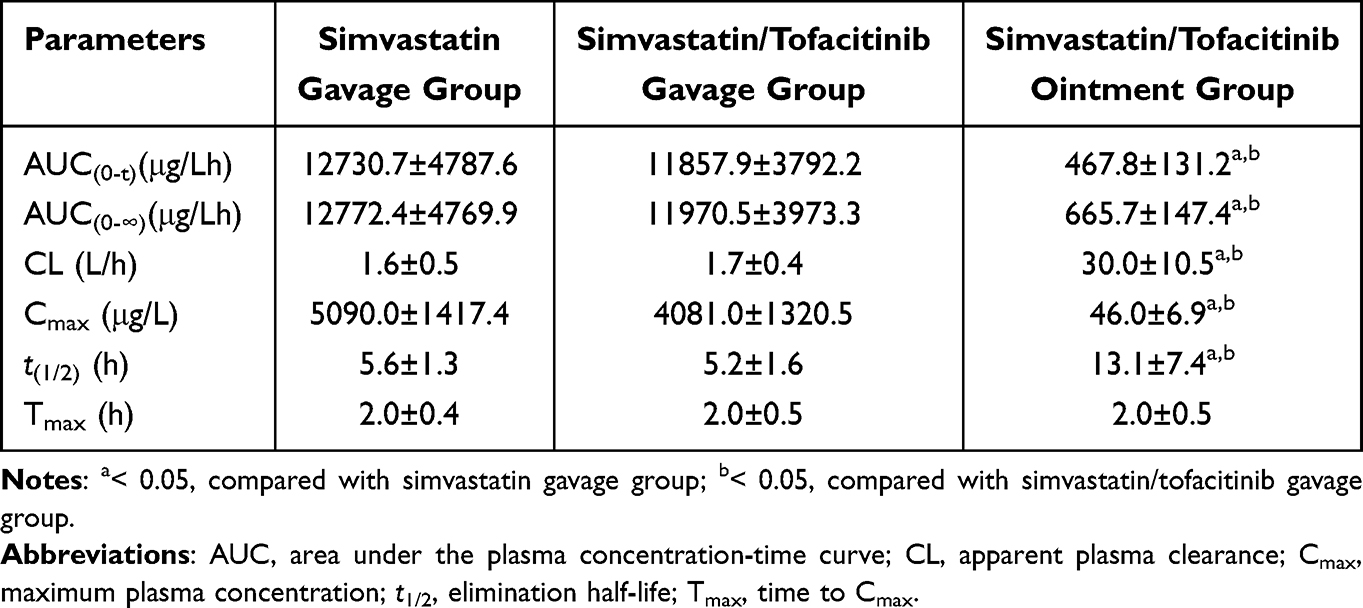 |
Table 5 Pharmacokinetic Parameters of Simvastatin in Different Experimental Groups (Means ± SD, n = 6) |
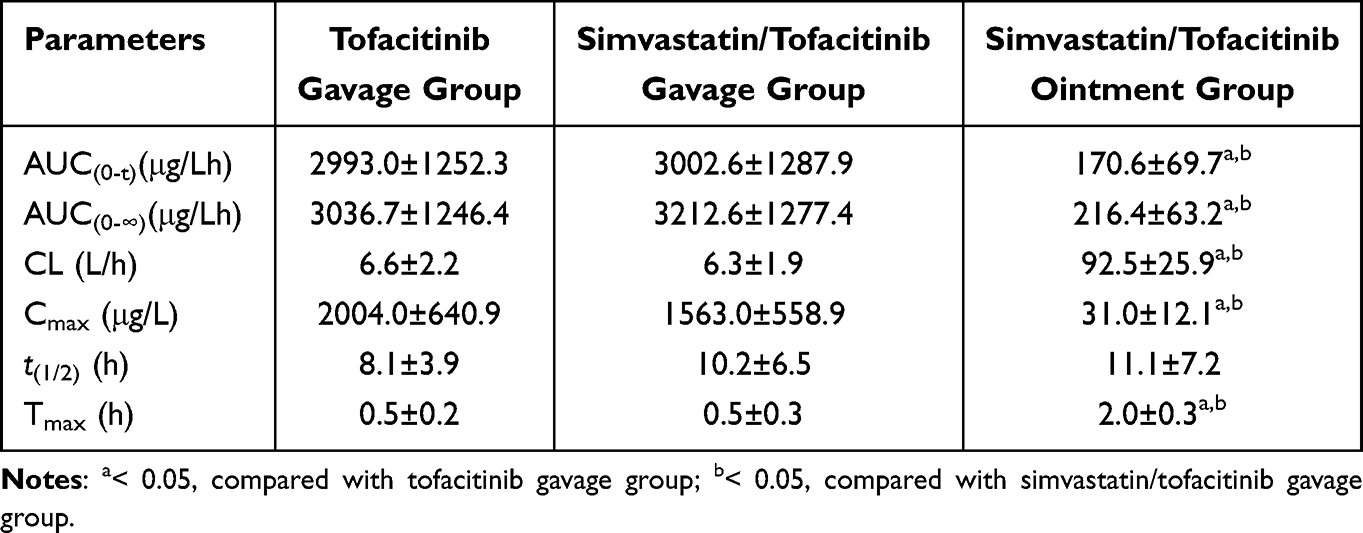 |
Table 6 Pharmacokinetic Parameters of Tofacitinib in Different Experimental Groups (Means ± SD, n = 6) |
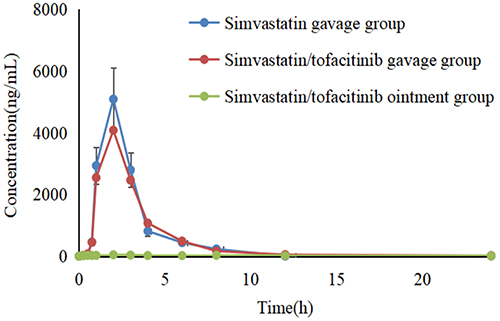 |
Figure 4 The drug concentration-time curve of tofacitinib under different administration regimens. |
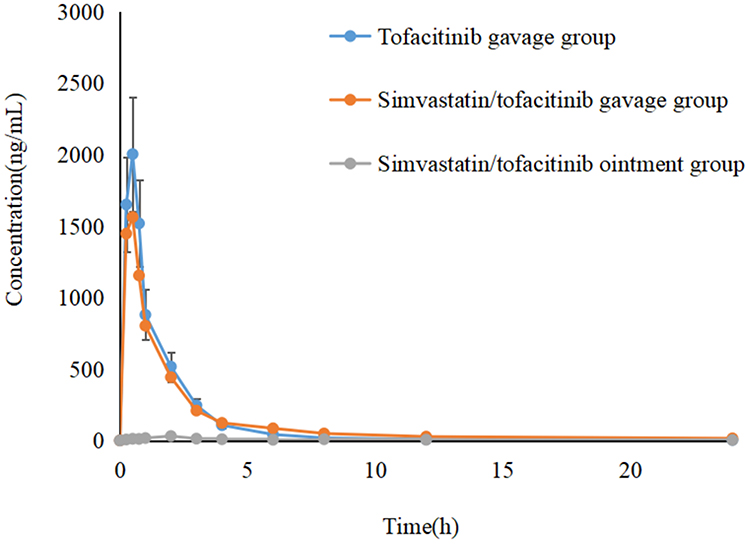 |
Figure 5 The drug concentration-time curve of simvastatin under different administration regimens. |
The results of the rat pharmacokinetic study demonstrated the following: (1) The combined administration of tofacitinib and simvastatin did not induce significant drug-drug interactions. Except for minor differences in Cmₐₓ, no notable variations were observed in other pharmacokinetic parameters. This avoids the uncertainty regarding drug efficacy and toxicity arising from pharmacokinetic drug-drug interactions, thereby ensuring the achievement of synergistic effects between the two agents from a pharmacodynamic perspective; (2) The bioavailability of tofacitinib/simvastatin ointment via transdermal administration was significantly reduced. Specifically, the 24 h bioavailability of tofacitinib and simvastatin delivered through the skin was only 7.1% and 5.2% of that achieved by oral gavage, respectively. If the drugs can accumulate locally in the lesional skin tissues, the relatively high local drug concentration will not only enhance therapeutic efficacy but also mitigate the adverse reactions caused by extensive systemic drug exposure. (3) Despite the low bioavailability of tofacitinib/simvastatin ointment via transdermal delivery, the formulation exhibited distinct drug release characteristics. Overall, the plasma drug concentrations of tofacitinib/simvastatin remained relatively stable within 1–2 hours post-administration; thereafter, the concentrations increased markedly at approximately 2 hours post-administration, followed by a decline and stabilization during the subsequent 2–4 h, and another significant elevation occurring between 6–8 h post-administration. In other words, the plasma concentration-time profiles of tofacitinib/simvastatin ointment after transdermal application in rats exhibited a double-peak or even multi-peak pattern, which may be attributed to the composition of the ointment. The ointment formulation in this study contained matrix-forming materials, and its drug release behavior was analogous to that of matrix-type sustained/controlled-release preparations. The drug release process is associated with the skin microenvironment, matrix erosion, and the displacement between upper and lower matrix layers. In conclusion, the limited percutaneous absorption of tofacitinib/simvastatin ointment into the systemic circulation can effectively circumvent the potential toxicity caused by excessive systemic drug exposure. However, the low bioavailability of tofacitinib/simvastatin ointment is not indicative of favorable therapeutic efficacy. Only when the skin tissue acts as a drug reservoir and maintains a relatively high local drug concentration can the therapeutic effects be guaranteed. Therefore, it is imperative to determine the drug concentrations in the skin tissues.
The determination results of drug concentrations in skin samples for pharmacokinetic studies were shon in Table 7. The results indicated that the accumulative amounts of simvastatin and tofacitinib in the skin following oral gavage were far lower than those achieved via transdermal administration, with a difference of 34-fold and 28-fold, respectively. This finding demonstrates that the simvastatin-tofacitinib ointment enables drug accumulation in the stratum corneum and sustained, gradual delivery to the deeper skin tissues. This not only enhances the bioavailability and therapeutic efficacy of the drugs at the cutaneous site but also reduces the adverse reactions associated with systemic drug exposure, thereby improving medication safety. In addition, these results also provide indirect evidence for the rationality of the ointment’s low systemic bioavailability in rats.
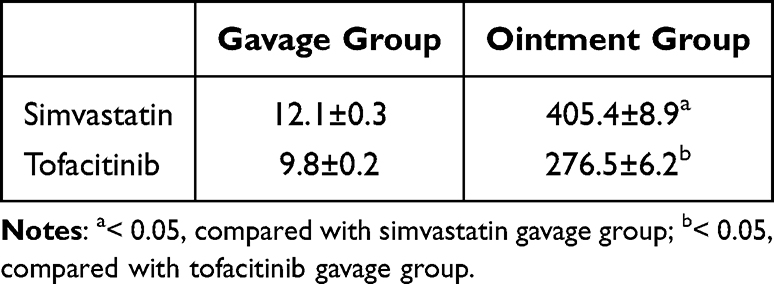 |
Table 7 The Concentration of Simvastatin and Tofacitinib in the Skin (μg/g) at 24 h After Gavage and Transdermal Administration |
In summary, the established HPLC-MS/MS method can accurately determine the plasma concentrations of tofacitinib and simvastatin, and confirm that tofacitinib/simvastatin ointment was qualified as a topical preparation, which may help to further study the efficacy and mechanism of tofacitinib/simvastatin ointments.
Conclusion
In this study, an HPLC-MS/MS method capable of simultaneously determining the concentrations of tofacitinib, simvastatin, diazepam, and lovastatin in rat plasma was established and validated. This method was successfully applied to the pharmacokinetic study of tofacitinib/simvastatin ointment in SD rats. The pharmacokinetic results showed that the combined use of simvastatin and tofacitinib did not cause significant drug-drug interactions. Meanwhile, the bioavailability of tofacitinib/simvastatin ointment via transdermal administration was significantly lower than that via oral administration, which helps enhance the accumulation of the drug in vitiligo tissues and improve the therapeutic effect. In addition, there were significant differences in all other pharmacokinetic parameters except for t1/2 (for tofacitinib) and Tmax (for simvastatin), indicating that the ointment can alter the in vivo behavior of the drugs. In summary, the findings of this study provide a guarantee for further exploring the dose-response relationship and adverse reactions of tofacitinib/simvastatin ointment.
Disclosure
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this manuscript.
References
1. Frisoli M, Essien K, Harris J. Vitiligo: mechanisms of pathogenesis and treatment. Annu Rev Immunol. 2020;38:621–13. doi:10.1146/annurev-immunol-100919-023531
2. Speeckaert R, Caelenberg E, Belpaire A, et al. Vitiligo: from pathogenesis to treatment. J Clin Med. 2024;13(17):5225. doi:10.3390/jcm13175225
3. Ting Y, Ng T. Prevalence of depression and anxiety among adults with vitiligo in a Malaysian tertiary hospital. Med J Malaysia. 2023;78:696–704.
4. Yamaguchi HL, Yamaguchi YJ, Peeva E. Pathogenesis of alopecia areata and vitiligo: commonalities and differences. Int J Mol Sci. 2024;25:4409. doi:10.3390/ijms25084409
5. Seidel P, Böhm M. Vitiligo-update on pathogenesis, diagnostics and therapy. Dermatologie. 2025;76:168–178. doi:10.1007/s00105-024-05467-9
6. Białczyk A, Wełniak A, Kamińska B, et al. Oxidative stress and potential antioxidant therapies in vitiligo: a narrative review. Mol Diagn Ther. 2023;27(6):723–739. doi:10.1007/s40291-023-00672-z
7. Chang WL, Ko CH. The role of oxidative stress in vitiligo: an update on its pathogenesis and therapeutic implications. Cells. 2023;12(6):936. doi:10.3390/cells12060936
8. Post NF, Ginski G, Peters R, et al. Trained immunity in the pathogenesis of vitiligo. Pigm Cell Melanoma Res. 2023;36(5):348–354. doi:10.1111/pcmr.13101
9. Qiu L, Song ZQ, Setaluri V. Oxidative stress and vitiligo: the Nrf2-ARE signaling connection. J Invest Dermatol. 2014;134(8):2074–2076. doi:10.1038/jid.2014.241
10. Lin XR, Meng XM, Song ZQ, et al. Nuclear factor erythroid 2-related factor 2 (Nrf2) as a potential therapeutic target for vitiligo. Arch Biochem Biophys. 2020;696:108670. doi:10.1016/j.abb.2020.108670
11. Jian Z, Tang L, Yi X, et al. Aspirin induces Nrf2-mediated transcriptional activation of haem oxygenase-1 in protection of human melanocytes from H2 O2 -induced oxidative stress. J Cell Mol Med. 2016;20:1307–1318. doi:10.1111/jcmm.12812
12. Elhalmoushy P, Elsheikh M, Matar N, et al. Novel berberine-loaded hyalurosomes as a promising nanodermatological treatment for vitiligo: biochemical, biological and gene expression studies. Int J Pharm. 2022;615(615):121523. doi:10.1016/j.ijpharm.2022.121523
13. Hasan R, Agarwal K, Podder I, et al. Simvastatin in vitiligo: an update with recent review of the literature. Int J Dermatol. 2021;60(10):e390–e396. doi:10.1111/ijd.15330
14. Shaker ESE, Allam SH, Mabrouk MM, et al. Simvastatin and non-segmental vitiligo: a new potential treatment option? Dermatol Ther. 2022;35(12):e15969. doi:10.1111/dth.15969
15. Zhang S, Serag I, Olama S, et al. Safety and efficacy of Simvastatin in the treatment of vitiligo: a systematic review and meta-analysis of randomized controlled trials. Arch Dermatol Res. 2025;317(1):726. doi:10.1007/s00403-025-04234-7
16. Xue C, Yao Q, Gu X, et al. Evolving cognition of the JAK-STAT signaling pathway: autoimmune disorders and cancer. Signal Transduct Target Ther. 2023;8:204.
17. Benucci M, Bernardini P, Coccia C, et al. JAK inhibitors and autoimmune rheumatic diseases. Autoimmun Rev. 2023;22:103276. doi:10.1016/j.autrev.2023.103276
18. Qi F, Liu F, Gao L. Janus kinase inhibitors in the treatment of vitiligo: a review. Front Immunol. 2021;12:790125. doi:10.3389/fimmu.2021.790125
19. Inoue S, Suzuki T, Sano S, et al. JAK inhibitors for the treatment of vitiligo. J Dermatol Sci. 2024;113(3):86–92. doi:10.1016/j.jdermsci.2023.12.008
20. Craiglow BG, King BA. Tofacitinib citrate for the treatment of vitiligo: a pathogenesis-directed therapy. JAMA Dermatol. 2015;151:1110–1112. doi:10.1001/jamadermatol.2015.1520
21. Mobasher P, Guerra R, Li SJ, et al. Open-label pilot study of tofacitinib 2% for the treatment of refractory vitiligo. Br J Dermatol. 2020;182(4):1047–1049. doi:10.1111/bjd.18606
22. Olamiju B, Craiglow BG. Tofacitinib cream plus narrowband ultraviolet B phototherapy for segmental vitiligo in a child. Pediatr Dermatol. 2020;37:754–755. doi:10.1111/pde.14159
23. Tron C, Kloosterboer S, Nagel B, et al. Dried blood spots combined with ultra-high-performance liquid chromatography mass spectrometry for the quantification of the antipsychotics risperidone, aripiprazole, pipamperone, and their major metabolites. Ther Drug Monit. 2017;39(4):429–440. doi:10.1097/FTD.0000000000000411
24. Patteet L, Cappelle D, Maudens K, et al. Advances in detection of antipsychotics in biological matrices. Clin Chim Acta. 2015;441:11–22. doi:10.1016/j.cca.2014.12.008
25. Nahar L, Onder A, Sarker S. A review on the recent advances in HPLC, UHPLC and UPLC analyses of naturally occurring cannabinoids (2010–2019). Phytochem Anal. 2020;31:413–457. doi:10.1002/pca.2906
26. Mei Y, Luo S, Ye L, et al. Validated UPLC-MS/MS method for quantification of fruquintinib in rat plasma and its application to pharmacokinetic study. Drug Des Devel Ther. 2019;13:2865–2871. doi:10.2147/DDDT.S199362
27. National Pharmacopoeia Commission. The Pharmacopoeia of the People’s Republic of China. Beijing China: China Medical Science and Technology Press; 2020.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of an HPLC-MS/MS Method for Determining I-BET151 in Rat Plasma and Its application to Pharmacokinetic Studies
Wang S
Drug Design, Development and Therapy 2025, 19:8679-8689
Published Date: 25 September 2025