Back to Journals » International Journal of Women's Health » Volume 18
Development and Validation of an Early-Pregnancy Prediction Model for Indicated Preterm Birth Using Three-Dimensional Placental Ultrasound and Maternal Clinical Characteristics
Authors Chen B, Chen H, Chen S, Chen Q, Wu S
Received 24 July 2025
Accepted for publication 9 January 2026
Published 14 January 2026 Volume 2026:18 555983
DOI https://doi.org/10.2147/IJWH.S555983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Birong Chen,* Huie Chen,* Shunji Chen, Qiong Chen, Shufen Wu
Department of Ultrasound, Zhangzhou Affiliated Hospital of Fujian Medical University, Zhangzhou, 363000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shufen Wu, Department of Ultrasound, Zhangzhou Affiliated Hospital of Fujian Medical University, No. 59 Shengli West Road, Xiangcheng District, Zhangzhou, Fujian Province, 363000, People’s Republic of China, Tel +8613338333911, Email [email protected]
Objective: To identify factors associated with indicated preterm birth (IPB) based on early pregnancy placental three-dimensional power Doppler ultrasound (3D-PDU) indices and maternal clinical characteristics, and to develop and validate a predictive model for IPB.
Methods: A total of 458 singleton pregnancies from 2022 were retrospectively analyzed. Early pregnancy placental 3D-PDU indices—vascularization index (VI), flow index (FI), vascularization-flow index (VFI)—along with maternal clinical characteristics, were collected. Subjects were randomly divided into a training set and a test set (7:3 ratio), and further categorized into the IPB group or the full-term group based on pregnancy outcomes. Logistic regression analysis and Akaike Information Criterion (AIC) were used to identify predictors and construct an IPB prediction model. Model performance was evaluated using discrimination, calibration, and clinical utility metrics.
Results: Multifactorial logistic regression identified a history of recurrent pregnancy loss, preterm birth history, and hypertensive disorders of pregnancy as independent risk factors for IPB, while early-pregnancy placental VFI was an independent protective factor. Based on the filter results, a nomogram model was plotted, which showed good discrimination (AUC: 0.900 [training set] and 0.882 [test set]). Hosmer-Lemeshow tests indicated good calibration (P = 0.449 for training set, P = 0.585 for test set), and decision curve analysis confirmed clinical utility.
Conclusion: The 3D-PDU indices, particularly VFI, may serve as valuable indicators of early placental perfusion. The nomogram developed in this study showed good predictive performance by integrating the early pregnancy placental 3D-PDU index (VFI) with maternal clinical characteristics, providing a potential tool for early identification of high-risk IPB pregnancies. Nonetheless, larger multicenter, prospective studies are needed to validate its applicability, and standardized protocols for 3D-PDU use should be established to ensure consistency.
Keywords: three-dimensional energy Doppler ultrasound, indicated preterm birth, placenta, early pregnancy period, predictive model
Introduction
Preterm birth, defined as delivery between 22 and 37 weeks of gestation,1,2 occurs in approximately 9.9% of pregnancies worldwide, with no evidence of a declining trend.3,4 It remains a leading cause of perinatal mortality and long-term neurodevelopmental disabilities.5,6 Preterm births are categorized into spontaneous preterm birth and indicated preterm birth (IPB), with the latter now accounting for nearly half of all cases and showing a rising incidence.7 Compared to spontaneous preterm birth, IPB is associated with lower birth weights and higher risks of neonatal infection, admission to intensive care, and adverse perinatal outcomes.8 Furthermore, IPB significantly contributes to the rising cesarean section rate and increases the risk of related complications, including intraoperative tissue injury and long-term consequences such as cesarean scar pregnancy.9 Therefore, the prevention and management of IPB have become critical areas of focus in contemporary maternal and fetal medicine research.
IPB typically represents a clinical outcome of severe maternal–fetal complications such as severe preeclampsia, fetal growth restriction (FGR), and intrauterine distress.8 Preeclampsia, as a key contributing factor, is closely associated with impaired spiral artery remodeling in early pregnancy, leading to inadequate placental perfusion.10 Studies have reported distinct risk factors for spontaneous and IPB: the former is mainly associated with infection, stress, and cervical insufficiency, whereas the latter primarily involves placental vascular abnormalities.8,11 Thus, IPB can be considered a manifestation of uteroplacental hypoperfusion syndrome, with its pathophysiological mechanisms traceable to early pregnancy spiral artery (SA) remodeling disorders and trophoblastic invasion defects.12,13 Anticoagulant therapy in early pregnancy can improve placental microcirculation by reducing hypercoagulability and inhibiting the formation of microthrombi, thereby increasing placental blood perfusion, promoting maternal-fetal substance exchange, and reducing the risk of IPB.14,15 Therefore, evaluating placental blood perfusion in early pregnancy is particularly important for guiding early intervention and improving pregnancy outcomes.
Three-dimensional power Doppler ultrasound (3D-PDU) combines 3D imaging with energy Doppler blood flow analysis, enabling quantitative assessment of tissue vascularization and perfusion.16 It quantifies tissue perfusion through three key metrics: vascularization index (VI), which measures vascular volume as a percentage of total tissue volume to assess vascular density; the flow index (FI), reflecting average blood flow intensity in the region and correlating with red blood cell count and velocity; and the vascularization-flow Index (VFI), the product of VI and FI, providing a comprehensive evaluation of tissue perfusion.17 Currently, the standard method for assessing placental perfusion is uterine artery Doppler ultrasound, which evaluates maternal uterine artery inflow resistance and hemodynamics using the pulsatility index (PI), resistance index (RI), and early diastolic notch index.18 In contrast, 3D-PDU can directly and angle-independently assess perfusion within the placental villous space, with a greater focus on microvascular evaluation of fetal-side placental function and showing potential advantages for early identification of placental dysfunction.19 3D-PDU measurements of the placenta during early pregnancy can assess placental perfusion and provide valuable predictive insights for adverse pregnancy outcomes.18–21 Given the strong association between IPB and maternal health status, we aimed to develop a logistic regression model that integrates early-pregnancy placental 3D-PDU indices (VI, FI, VFI) with maternal clinical characteristics. Such a model could serve as a potential reference tool for identifying high-risk pregnancies and guiding early anticoagulation interventions, ultimately aiming to improve maternal and fetal outcomes.
Materials and Methods
Clinical Data
We retrospectively collected data from singleton pregnancies with regular prenatal examinations and placental 3D-PDU in early pregnancy at our hospital between January 2022 and December 2022. The study protocol was approved by the Ethics Committee of Zhangzhou Hospital, Fujian, China (Approval No. 2025LWB150). The requirement for written informed consent was waived by the ethics committee due to retrospective study design and use of anonymized patient data. The study protocol adhered to the principles enshrined in the Declaration of Helsinki and relevant ethical guidelines.
Participants were included in the study if they met all of the following conditions: 1) Singleton pregnancy; 2) gestational age between 11 and 13+6 weeks; 3) Crown-rump length (CRL) measured by ultrasound between 45 and 84 mm; 4) no fetal structural abnormalities detected on early pregnancy screening; 5) nuchal translucency (NT) < 2.5 mm; 6) complete clinical data available. The exclusion criteria were as follows: 1) fetal genetic abnormalities or structural malformations detected during pregnancy; 2) spontaneous preterm birth due to cervical insufficiency, premature rupture of membranes, congenital genital tract malformations, etc.; 3) incomplete clinical data.
Preterm birth includes two types: IPB and spontaneous preterm birth. IPB refers to preterm delivery resulting from active medical intervention due to severe maternal or fetal complications, whereas spontaneous preterm birth occurs without a clear medical indication and is often associated with spontaneous uterine contractions, cervical insufficiency, preterm premature rupture of membranes, infection, or multiple pregnancy. To comprehensively assess preterm birth risk, this study analyzed delivery cases occurring between 22 and 37 weeks of gestation.1,2 Full-term delivery refers to births occurring between 37 and 41+6 weeks of gestation. Based on the inclusion criteria, 517 cases were initially identified. After excluding 59 cases, 458 pregnant women were included in the final analysis. A detailed case selection and grouping process is illustrated in the flowchart (Figure 1).
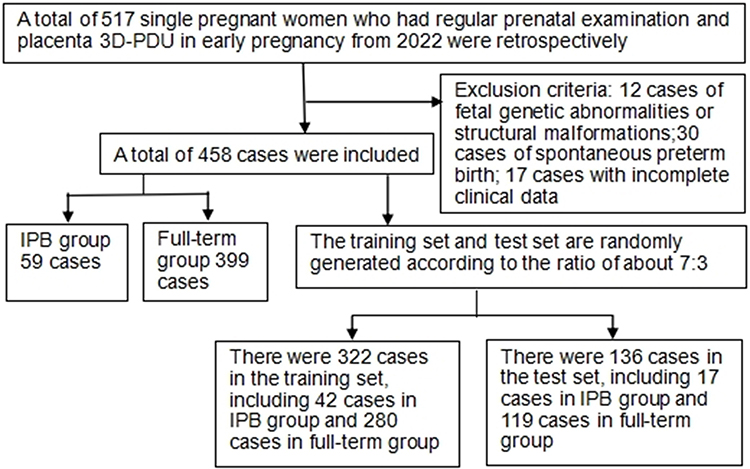 |
Figure 1 Flow chart of case selection and grouping. |
Instruments and Methods
Ultrasound examinations were performed using the GE Voluson E8 ultrasound diagnostic system, equipped with two convex array probes: the 4C-D (3.5–5.0 MHz) and the RAB4-8D (4.0–8.5 MHz). The system is integrated with 3D-PDU imaging capabilities. All scans were conducted by two obstetricians, each with over ten years of experience in prenatal diagnosis. Image acquisition strictly adhered to the following unified operating standards to ensure consistency.
The examination was conducted in a supine position. Following completion of fetal NT screening and structural assessment using the 4C-D convex array probe, the placental localization was identified, and the RAB4-8D 3D volume probe was activated. The placental structure and umbilical cord attachment site were assessed to ensure that the maximal placental outline was captured within the region of interest. To minimize motion artifacts, subjects were instructed to hold their breath or minimize breathing movements during data acquisition. The 3D power Doppler mode was then initiated, and placental scanning was performed for no more than 15 seconds to obtain 3D volume data. Offline analysis was carried out using Virtual Organ Computer-aided Analysis software. The region of interest was manually traced at six rotational steps, each at 30° intervals, to reconstruct a 3D image of the placental morphology. The software then automatically calculated the three 3D-PDU indices—VI, FI, and VFI—using the Doppler blood flow histogram (Figure 2).
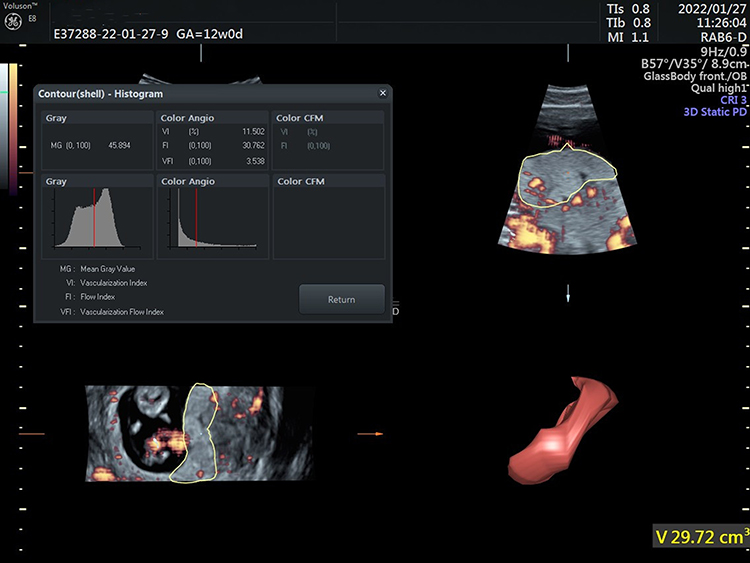 |
Figure 2 Quantitative assessment of placental perfusion using 3D-PDU. Measurement of the vascularization index (VI), flow index (FI), and vascularization-flow index (VFI) based on Doppler blood flow histogram analysis. |
Observation Indicators
The following maternal characteristics were collected: maternal age, clinical gestational age, body mass index (BMI), use of assisted reproductive technology, history of recurrent pregnancy loss, history of preterm birth, hypertensive disorders of pregnancy (HDP), FGR, gestational diabetes, and placental location. In addition, 3D-PDU indices of the placenta (VI, FI, and VFI) were recorded in early pregnancy.
Statistical Methods
Statistical analysis was conducted using the R (version 4.0.4) software. Normally distributed continuous variables were presented as mean ± standard deviation, and categorical variables were presented as frequency (percentage). Inter-group comparisons were performed using the t-test, Mann–Whitney U-test, and χ2-test. A significance level of α = 0.05 was used for all tests. Univariate and multivariate logistic regression analyses were conducted using the rms package to identify independent risk factors, with results expressed as odds ratios (OR) and 95% confidence intervals (CI). A logistic regression model was then constructed based on the identified predictors and selected using the Akaike Information Criterion (AIC) for optimal model fit. Receiver operating characteristic (ROC) curves were plotted for both training and test datasets, with the area under the curve (AUC) used to assess discriminative ability. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test and the Bootstrap method (1000 iterations). The clinical applicability of the model was evaluated using Decision Curve Analysis (DCA).
Results
Comparison of Baseline Clinical Characteristics and Placental 3D-PDU Indices
A total of 458 eligible pregnant women were enrolled and classified into two groups based on IPB and full-term diagnostic criteria: the IPB group (n = 59) and the full-term group (n = 399). No significant between-group differences were observed regarding maternal age, gestational age, BMI, use of assisted reproductive technologies, gestational diabetes mellitus, or placental position (P>0.05). The IPB group had higher rates of recurrent pregnancy loss, preterm birth history, HDP, and FGR, along with lower placental 3D-PDU indices (VI, FI, VFI) compared with the full-term group (P<0.05 for all) (Table 1).
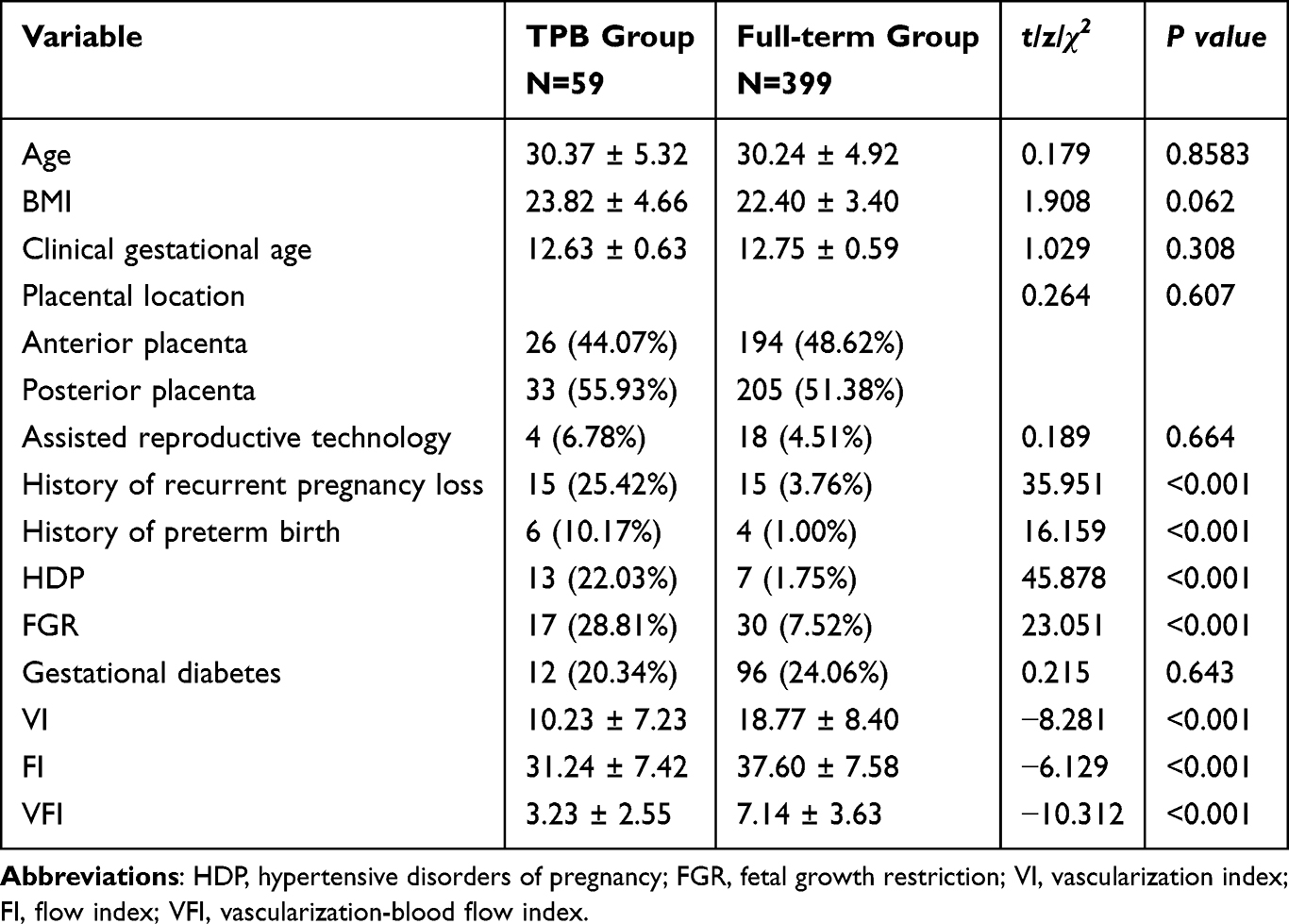 |
Table 1 Comparison of Baseline Clinical Characteristics and Early Pregnancy 3D-PDU Placental Indices in the Two Groups |
Comparison of Clinical Characteristics and Placental 3D-PDU Indices Between the Training and Test Sets
Except for a statistically significant difference in the proportion of gestational diabetes mellitus (P<0.05), there were no significant differences between the training and test sets in terms of the incidence of IPB, other maternal clinical characteristics, or early pregnancy 3D-PDU placental indices (P>0.05) (Table 2). These findings suggest that the training and test sets were comparable and suitable for model development and validation.
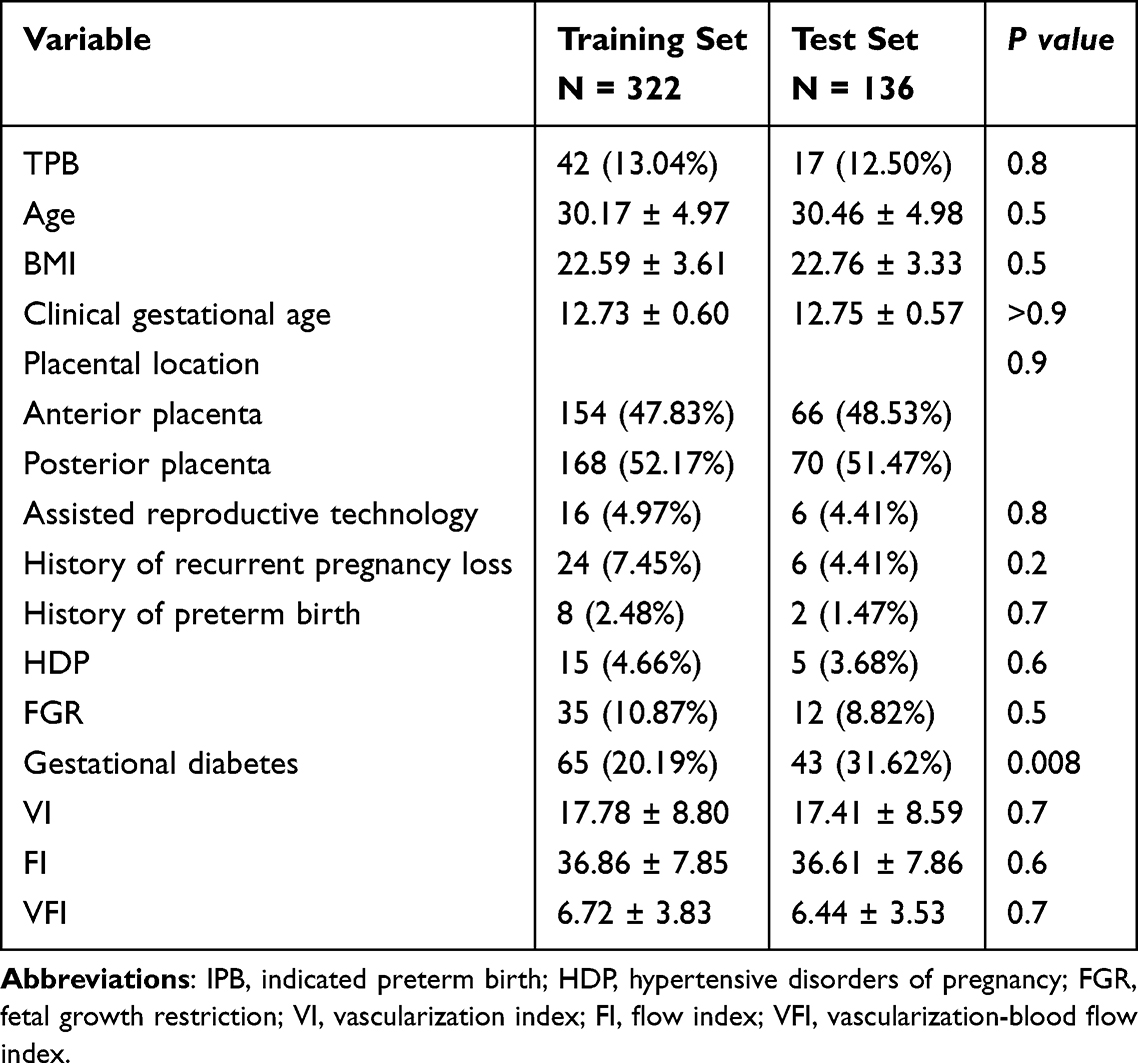 |
Table 2 Comparison of Clinical Characteristics and Early Pregnancy 3D-PDU Placental Indices Between Training and Test Sets |
Univariate and Multivariate Logistic Regression Analysis and Nomogram Model in the Training Set
Univariate logistic regression analysis identified seven variables significantly associated with TPB (history of recurrent pregnancy loss, history of preterm birth, HDP, FGR, and early pregnancy placental 3D-PDU indices [VI, FI, VFI], all P<0.05). Multivariate logistic regression further identified four independent predictors of TPB. A history of recurrent pregnancy loss (OR = 7.33), history of preterm birth (OR = 26.33), and HDP (OR=4.36) were identified as independent risk factors, while VFI in early pregnancy was an independent protective factor (OR = 0.55) (Table 3).
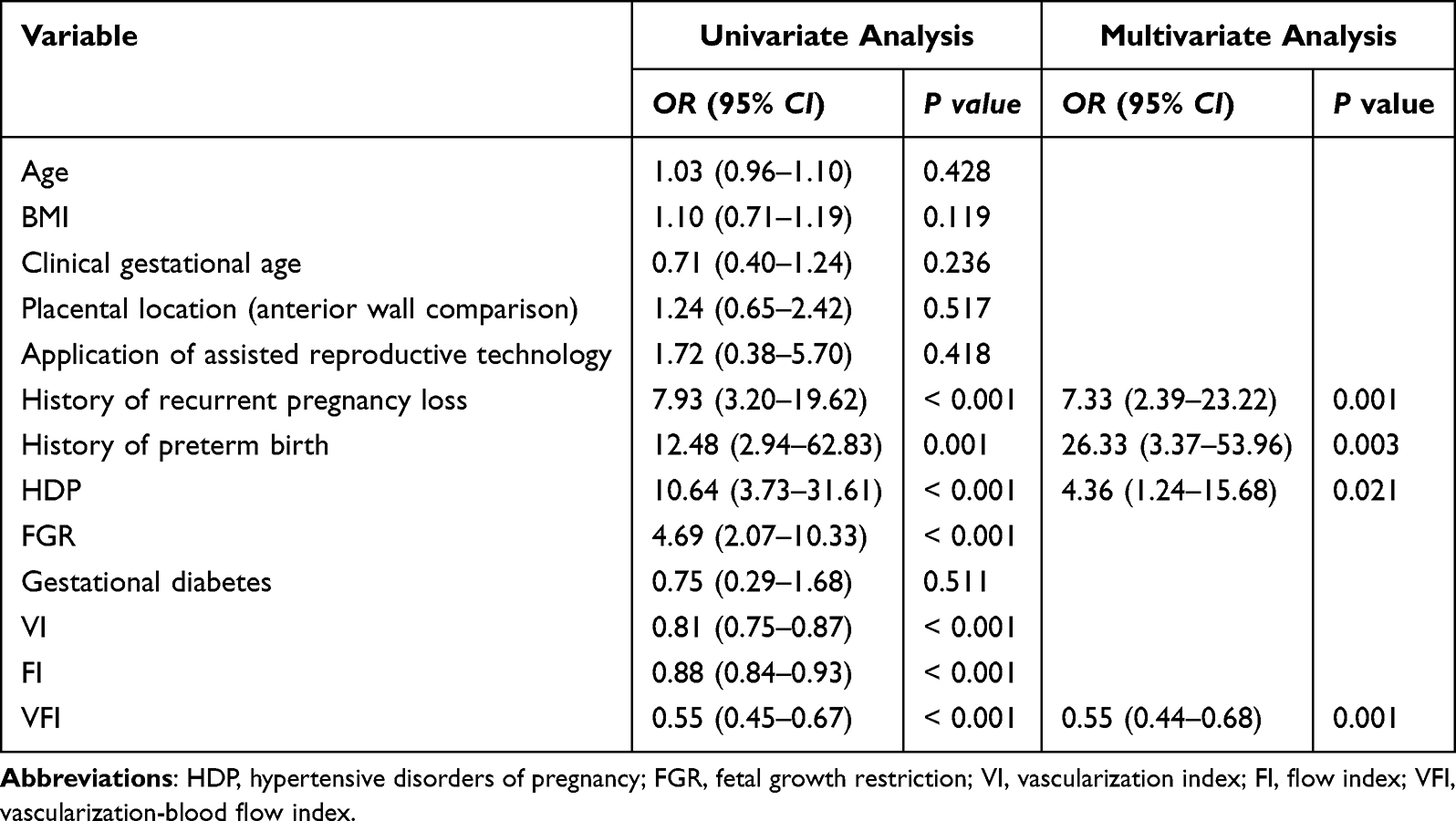 |
Table 3 Univariate and Multivariate Logistic Regression Analysis in the Training Set |
A logistic regression model was constructed based on the AIC, yielding the lowest AIC value of 162.665. The final model is defined by the following equation:
Y = 0.430+1.992×X1 + 3.271×X2 + 1.473×X3 − 0.590×X4, where X1 represents the history of recurrent pregnancy loss (0 = none, 1 = yes), X2 represents the history of preterm birth (0 = none, 1 = yes), X3 represents the HDP (0 = none, 1 = yes), X4 represents the VFI value from early pregnancy placental 3D-PDU, and Y represents the predicted risk score for IPB. A corresponding nomogram (Figure 3) was developed to visualize the model. The chart assigns weighted scores to each predictive factor based on a standardized scale. The total score is then mapped to a probability axis, allowing for quantitative estimation of an individual’s IPB risk.
 |
Figure 3 Nomogram of the IPB prediction model. |
An application example of the nomogram model (Figure 4) involves a 34-year-old pregnant woman with a history of recurrent pregnancy loss but no prior preterm birth. She was diagnosed with HDP and had a VFI value of 0.72. Her scores were as follows: 14 for recurrent pregnancy loss, 11 for HDP, and 96 for VFI, yielding a total score of 121 points, which corresponded to a predicted probability >0.9. Subsequent follow-up confirmed this case as IPB.
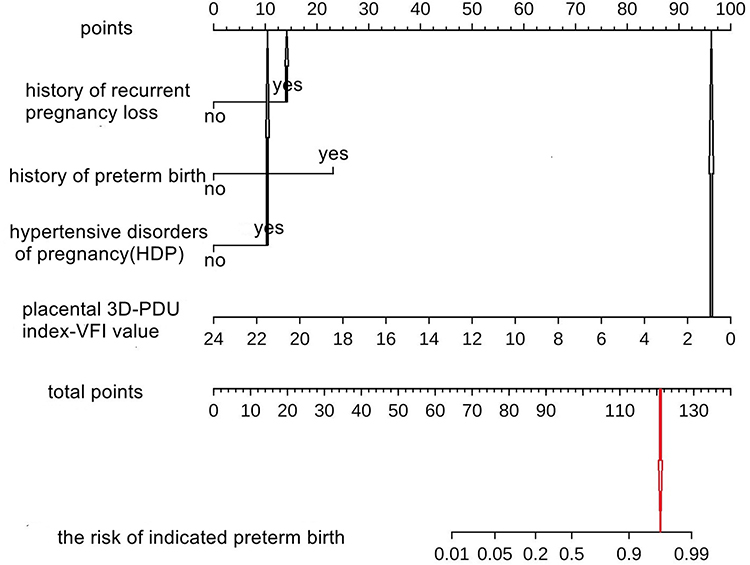 |
Figure 4 Application example of the nomogram model. |
Internal Model Verification
The ROC curve analysis (Figure 5) demonstrated the strong discriminatory power of the model. In the training set, the optimal diagnostic cut-off was −1.441, corresponding to a maximum Youden’s index of approximately 0.848. The AUC value was 0.900 (95% CI: 0.840–0.959), yielding a sensitivity of 87.1%, a specificity of 85.7%, a positive predictive value (PPV) of 45.49%, and a negative predictive value (NPV) of 97.98%. In the test set, the model also showed good performance with an AUC of 0.882 (95% CI: 0.784–0.986), yielding a sensitivity of 70.6%, a specificity of 98.3%, a PPV of 85.58%, and a NPV of 95.91%. The calibration curve drawn by the Bootstrap method (B=1000 times) and H-L goodness-of-fit test (Figure 6) (P=0.449 for the training set and P=0.585 for the test set, P>0.05) demonstrated the reliability of the prediction accuracy. Decision curve analysis (Figure 7) indicated that the model’s risk threshold in both the training and test sets ranged from approximately 0.04 to 1.0, both exceeding the two reference lines representing strategies of treating no or all patients, respectively. These results support the clinical applicability of the prediction model.
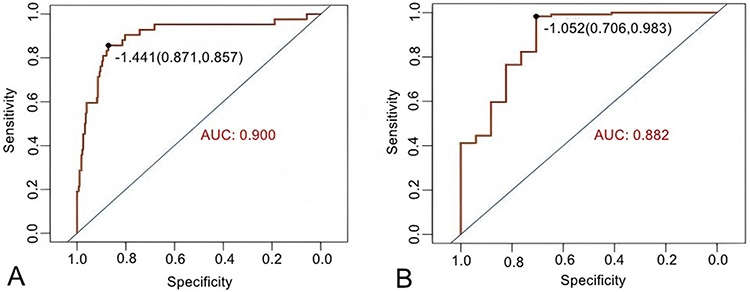 |
Figure 5 ROC curves of the IPB prediction model in the training set (A) and test set (B). |
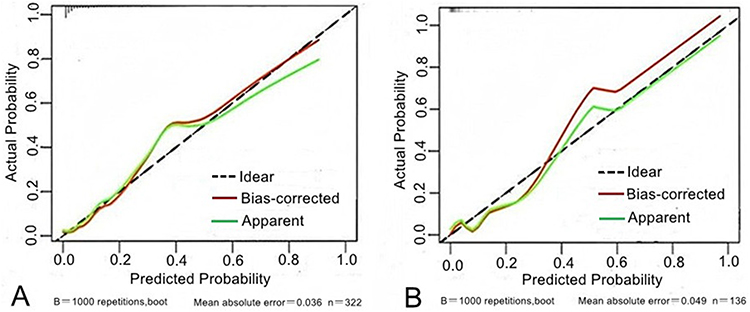 |
Figure 6 Calibration curves of the IPB model in the training set (A) and the test set (B). |
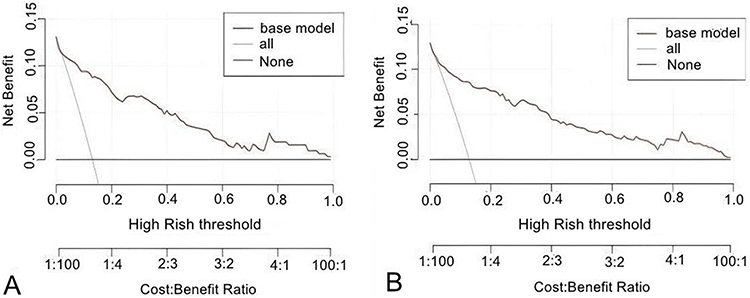 |
Figure 7 IPB model decision curves for training set (A) and test set (B). |
Discussion
This study aimed to address the need for early identification of high-risk pregnancies associated with adverse outcomes of IPB by combining quantitative placental perfusion assessment with maternal high-risk clinical factors. Our findings indicate that incorporating the first-trimester placental 3D-PDU index (particularly VFI as an independent protective factor) along with maternal history-based risk factors into a nomogram model provides a preliminary potential predictive tool. The model demonstrated high discriminative ability and clinical utility, highlighting the value of 3D-PDU in enhancing early risk assessment to improve pregnancy management.
The placenta is essential for sustaining pregnancy and fetal development, serving as the primary organ for maternal–fetal exchange, endocrine regulation, and immune modulation. The first trimester is a critical period for placental development, during which uterine spiral artery (SA) remodeling is the key process. The SA, originating from the uterine artery and extending into the functional endometrium, provides the main channel for maternal–fetal blood perfusion. Normal physiological remodeling involves degradation of the vascular muscular layer and luminal dilation, transforming blood flow from high resistance and low flow to low resistance and high flow, thereby enhancing placental perfusion and supporting efficient maternal–fetal circulation.22 Impaired SA remodeling leads to placental ischemia and related complications such as preeclampsia and FGR,23,24 significantly increasing the risk of IPB. Therefore, research on the placental blood supply is crucial for predicting IPB.
This study demonstrated that early pregnancy placental 3D-PDU indices (VI, FI, VFI) were significantly lower in the IPB group than in the full-term group (VI: 10.23 ± 7.23 vs 18.77 ± 8.40; FI: 31.24 ± 7.42 vs 37.60 ± 7.58; VFI: 3.23 ± 2.55 vs 7.14 ± 3.63; P<0.001). Multivariate logistic regression analysis identified VFI as an independent protective factor against IPB (OR = 0.55, 95% CI: 0.46–0.68, P = 0.001). Previous studies25 identified VFI in early pregnancy as an independent protective factor for FGR (OR = 0.563), and Ying et al26,27 found that VI, FI, and VFI were reduced in HDP, with VFI showing a high sensitivity. In addition, Qin et al28 reported that increased placental perfusion in early pregnancy, assessed by VFI, demonstrated good predictive value for macrosomia (AUC = 0.826).These findings align with our results, supporting the utility of 3D-PDU for assessing placental perfusion in early pregnancy. VFI, in particular, provides a comprehensive measure of placental perfusion status. This is likely because VFI simultaneously captures both the presence (density) of blood vessels and their functional activity (blood flow signals). Prior research25 also indicated that VFI had greater predictive value for FGR than the uterine artery PI in the first trimester (AUC = 0.741 vs 0.692). Abdallah et al29 demonstrated higher first-trimester sensitivity of VFI than uterine artery PI for preeclampsia prediction. Therefore, VFI may offer advantages over conventional 2D Doppler ultrasound PI in evaluating placental perfusion. A low VFI value may reflect abnormal development of the placental villous vascular network, potentially impairing the maternofetal nutrient and gas exchange process. Thus, 3D-PDU technology enables the detection of early signs of placental dysfunction by quantifying the hemodynamic characteristics of the placental chorionic network.
This study identified a history of recurrent pregnancy loss and preterm birth as risk factors for IPB, consistent with the “placental dysfunction persistence hypothesis” proposed by Bhattacharya et al30,31. Recurrent pregnancy loss can impair the endometrial vascular network, resulting in shallow placental implantation and defective spiral artery remodeling. These pathophysiological changes contribute to a vicious cycle of maternal-fetal interface injury, placental hypoperfusion, and elevated IPB risk.32 Notably, this study found that the risk of IPB in patients with HDP was 4.36 times higher. This association may be attributed to the bidirectional exacerbation between systemic vascular endothelial dysfunction and placental ischemia–hypoxia.33,34 Although FGR did not emerge as an independent predictor in the multivariate analysis, its shared pathological basis of placental hypoperfusion with IPB35 suggests that both conditions may represent distinct clinical manifestations of a common underlying placental pathology.
Recent years have seen progress in preterm birth risk prediction systems based on medical history and pregnancy complications. Liu et al36 developed a model integrating prenatal examination results, preterm birth history, and HDP, demonstrating stable discriminative performance (AUC > 0.7) and confirming the broad applicability of clinical phenotype parameters. Zimeng et al37 analyzed mid-trimester singleton pregnancies and found strong correlations between cervical morphological changes (eg, shortened cervical length and persistent internal os dilation) and spontaneous preterm birth risk. Their model achieved AUC values of 0.850 in the training set and 0.881 in the validation set, highlighting the importance of dynamic cervical function monitoring. However, most existing studies focus on the prediction of preterm birth and spontaneous preterm birth,38 with few addressing intervention-induced preterm birth (IPB). This present study integrates placental hemodynamics with high-risk maternal characteristics to construct an IPB nomogram model, demonstrating excellent discrimination (training set AUC 0.900 [95% CI: 0.840–0.959]; test set AUC 0.882 [95% CI: 0.784–0.986]), good calibration (H–L test P>0.05), and strong clinical applicability based on decision curve analysis. Notably, this model captures early compensatory changes in placental blood flow at 11–13 weeks, enabling early identification of high-risk cases before irreversible damage and providing a time window for intervention. Moreover, the quantitative 3D-PDU index offers a potential tool for assessing placental perfusion.
The clinical translational value of this model lies in its ability to simplify complex hemodynamic and clinical data into a practical, user-friendly risk assessment tool. By estimating IPB risk based on individualized profiles, the model may facilitate early interventions such as low-dose aspirin or heparin therapy, enhanced prenatal monitoring, and nutritional support for high-risk pregnancies, thereby improving pregnancy outcomes. An international multicenter study14 has demonstrated that anticoagulation intervention during early pregnancy can reduce the risk of IPB by 1.5 percentage points. Building on this evidence, the high-risk population screening framework proposed in our model may offer a valuable tool for identifying candidates who would benefit most from such interventions. However, the applicability of this model needs to be validated in large-scale prospective studies.
The low PPV of 45.5% in the training set is mainly attributed to the combination of its limited specificity (85.7%) and low prevalence (13.0%) in this dataset, which increases false positives—a characteristic consistent with the calculation of predictive values. Conversely, the test set demonstrated high specificity (98.3%) and higher PPV (85.6%), confirming the model’s good generalization ability and making the results more clinically valuable.
This study preliminarily validated the predictive value of combining 3D-PDU indices with clinical characteristics for IPB but has several limitations: First, its single-center retrospective design (n = 458) and data sparsity prevented the inclusion of certain variables (eg, BMI, smoking, diabetes, placenta previa), which may have introduced confounding bias. Second, the model underwent only internal validation and lacks independent external validation, making it susceptible to selection bias. Third, reliance on a specific device (GE Voluson E8) limits cross-platform applicability, underscoring the need for a standardized acquisition protocol to enhance generalizability. Fourth, the relatively short study period (data from 2022 only) limits assessment of long-term trends. Despite these limitations, this study provides a potential reference for IPB risk identification and clinical intervention by quantifying placental perfusion in early pregnancy and integrating maternal clinical characteristics.
Conclusion
This study developed an IPB prediction model integrating the early placental 3D-PDU index (VFI) and maternal clinical characteristics (recurrent pregnancy loss, preterm birth history, and HDP). The 3D-PDU indices, particularly VFI, may serve as potential reference tools for quantifying early placental perfusion. The model demonstrated good predictive performance in internal validation, offering a potential approach for early identification and management of high-risk IPB pregnancies to reduce adverse outcomes. Nonetheless, larger multicenter, prospective studies are needed to validate its applicability, and standardized protocols for 3D-PDU use should be established to ensure consistency.
Acknowledgment
We thank Medjaden Inc. for the scientific editing of this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Applying Artificial Neural Network to Develop a First-Trimester Multidimensional Data Model for Predicting Preeclampsia in High-Risk Pregnant Women (2021J011414).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Sibiude J. Quels outils de prédiction de l’accouchement prématuré en cas de menace d’accouchement prématuré? Gynecol Obstet Fertil Senol. 2025. doi:10.1016/j.gofs.2025.10.001
2. Leneuve-Dorilas M, Favre A, Louis A, Bernard S, Carles G, Nacher M. Risk factors for very preterm births in French Guiana: the burden of induced preterm birth. AJP Rep. 2019;9(1):e44–12. doi:10.1055/s-0039-1678716
3. Chawanpaiboon S, Vogel JP, Moller AB, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(1):e37–e46. doi:10.1016/S2214-109X(18)30451-0
4. Ohuma EO, Moller AB, Bradley E, et al. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. Lancet. 2023;402(10409):1261–1271. doi:10.1016/S0140-6736(23)00878-4
5. Perin J, Mulick A, Yeung D, et al. Global, regional, and national causes of under-5 mortality in 2000-19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Health. 2021;6(2):106–115. doi:10.1016/S2352-4642(21)00311-4
6. Zhou L, Liu X, He G, Chen M, Zeng S, Sun C. Alteration of fractional anisotropy in preterm-born individuals: a systematic review and meta-analysis. J Obstet Gynaecol. 2024;44(1):2371956. doi:10.1080/01443615.2024.2371956
7. Mensah NA, Fassett MJ, Shi JM, et al. Examining recent trends in spontaneous and iatrogenic preterm birth across race and ethnicity in a large managed care population. Am J Obstet Gynecol. 2022;228(6):
8. Jiang Y, Zhou F, Zhang H, et al. Risk factors and birth outcomes of preterm birth subtypes: a case-control study of singleton natural pregnancy. Gynecol Obstet Clin Med. 2024;4(3):e000027. doi:10.1136/gocm-2024-000027
9. Shutak M, Makarchuk O, Perkhulyn O, et al. Risk factors for formation of uterine scar defect after cesarean section: parameters of reproductive health disorders. RHW. 2025;4:52–59. doi:10.30841/2708-8731.4.2025.335424
10. Brouwers L, de Gier S, Vogelvang TE, et al. Prevalence of placental bed spiral artery pathology in preeclampsia and fetal growth restriction: a prospective cohort study. Placenta. 2024;156:1–9. doi:10.1016/j.placenta.2024.08.010
11. Pickett KE, Abrams B, Selvin S. Defining preterm delivery--the epidemiology of clinical presentation. Paediatr Perinat Epidemiol. 2000;14(4):305–308. doi:10.1046/j.1365-3016.2000.00293.x
12. James JL, Boss AL, Sun C, Allerkamp HH, Clark AR. From stem cells to spiral arteries: a journey through early placental development. Placenta. 2021;125:68–77. doi:10.1016/j.placenta.2021.11.004
13. Vornic I, Buciu V, Furau CG, et al. The interplay of molecular factors and morphology in human placental development and implantation. Biomedicines. 2024;12(12):2908. doi:10.3390/biomedicines12122908
14. Hoffman MK, Goudar SS, Kodkany BS, et al. Low-dose aspirin for the prevention of preterm delivery in nulliparous women with a singleton pregnancy (ASPIRIN): a randomised, double-blind, placebo-controlled trial. LANCET. 2020;395(10220):285–293. doi:10.1016/S0140-6736(19)32973-3
15. Cruz-Lemini M, Vázquez JC, Ullmo J, Llurba E. Low-molecular-weight heparin for prevention of preeclampsia and other placenta-mediated complications: a systematic review and meta-analysis. Am J Obstet Gynecol. 2021;226(2s):S1126–S1144.e17. doi:10.1016/j.ajog.2020.11.006
16. Schiffer V, Pellaers D, Hoenen J, van Kuijk SMJ, Spaanderman MEA, Al-Nasiry S. Feasibility of three dimensional power Doppler ultrasonography methods to assess placental perfusion. Eur J Obstet Gynecol Reprod Biol. 2020;254:321–328. doi:10.1016/j.ejogrb.2020.08.006
17. Yamasato K, Zalud I. Three dimensional power Doppler of the placenta and its clinical applications. J Perinat Med. 2017;45(6):693–700. doi:10.1515/jpm-2016-0366
18. Hegab A, Taher A, Elzayyat A. Comparison between placental 3D power Doppler and uterine artery pulsatility index in early prediction of pre-eclampsia ijhs. Int J Health Sciences. 2022;6(S1):1627–1645. doi:10.53730/ijhs.v6ns1.4918
19. Wang Y, Zheng M, Bao M, et al. Assessment of uteroplacental perfusion with 3D power Doppler for the early prediction of pre-eclampsia: a systematic review and meta-analysis. Quant Imaging Med Surg. 2025;15(10):9765–9777. doi:10.21037/qims-2025-158
20. Wang Y, Liang L, Liu Y, Li P, Ren J. The application value of three-dimensional power doppler ultrasound in fetal growth restriction. Evid Based Complement Alternat Med. 2022;2022:4087406. doi:10.1155/2022/4087406
21. Park IY, Wie JH, Park JH, Kwon JY. Combination of three-dimensional placental vascular indices and volume and uterine artery pulsatility index at 10-13 weeks of gestation could improve the prediction of adverse pregnancy outcomes. J Obstet Gynaecol Res. 2021;47(6):2051–2058. doi:10.1111/jog.14781
22. Szukiewicz D, Trojanowski S, Wróbel E, et al. Mechanosensing of shear stress and uterine spiral artery remodeling by invasive trophoblasts in early pregnancy. Int J Mol Sci. 2025;26(19). doi:10.3390/ijms26199565
23. Liu S, Chen W, Chen J, et al. m6A deficiency impairs uterine spiral artery remodeling to induce preeclampsia-like symptoms via FGF2. Sci China Life Sci. 2025. doi:10.1007/s11427-024-2846-4
24. Zhang Y, Shao Y. Current knowledge of fetal growth restriction in relation to thrombosis at the maternal‐fetal interface–placenta and umbilical cord: a literature review. Reprod Female Child Health. 2025;4(1). doi:10.1002/rfc2.70013
25. Chen SJ, Lv GR, Chen BQ, et al. The application value of 2D and 3D ultrasound in early pregnancy for predicting fetal growth restriction. J Chin Foreign Medical Research. 2023;21(18):72–76. (in Chinese). doi:10.14033/j.cnki.cfmr.2023.18.019
26. Liu Y, Gao X, Shi D, et al. Changes of placental three-dimensional power Doppler ultrasonography in third trimester among hypertensive disorders complicating pregnancy. J Biomol Biomed. 2023;23(5):894–901. doi:10.17305/bb.2023.9085
27. Tian F, Dou LF, Tang LW, et al. Predictive value of placental real-time shear wave elastography combin.ed with 3-dimensional power Doppler index for preeclampsia. Med. 2024;103(10):e37372. doi:10.1097/MD.0000000000037372
28. Qin M, Zhu T, Wang W, Tang L, Wang Y, Chen L. Application value of two-dimensional ultrasound combined with three-dimensional power doppler in the prediction of macrosomia in early pregnancy. J Clin Ultrasound. 2024;53(3):452–458. doi:10.1002/jcu.23885
29. Abdallah A, Khairy M, Tawfik M, et al. Role of first-trimester three-dimensional (3D) power Doppler of placental blood flow and 3D placental volume in early prediction of pre-eclampsia. Int J Gynaecol Obstet. 2021;154(3):466–473. doi:10.1002/ijgo.13572
30. Bhattacharya S, McCall SJ, Woolner AMF. Recurrent pregnancy loss and subsequent preterm birth: association or causation? Fertil Steril. 2022;117(4):820–821. doi:10.1016/j.fertnstert.2022.01.038
31. Patel K, Pirie D, Heazell AEP, Morgan B, Woolner A. Subsequent pregnancy outcomes after second trimester miscarriage or termination for medical/fetal reason: a systematic review and meta-analysis of observational studies. Acta Obstet Gynecol Scand. 2024;103(3):413–422. doi:10.1111/aogs.14731
32. Wu CQ, Nichols K, Carwana M, Cormier N, Maratta C. Preterm birth after recurrent pregnancy loss: a systematic review and meta-analysis. Fertil Steril. 2022;117(4):811–819. doi:10.1016/j.fertnstert.2022.01.004
33. Staff AC, Fjeldstad HE, Fosheim IK, et al. Failure of physiological transformation and spiral artery atherosis: their roles in preeclampsia. Am J Obstet Gynecol. 2022;226(2s):S895–s906. doi:10.1016/j.ajog.2020.09.026
34. Guida JPS, Dias TZ, Lajos GJ, et al. Hypertensive disorders during pregnancy as a major cause of preterm birth and adverse perinatal outcomes: findings from a Brazilian National Survey. Einstein. 2024;22:eAO0514. doi:10.31744/einstein_journal/2024AO0514
35. Pinheiro B, Sarmento-Gonçalves I, Ramalho C. Association between placental pathology and early-onset fetal growth restriction: a systematic review. Fetal Pediatr Pathol. 2024;44(1):40–52. doi:10.1080/15513815.2024.2437642
36. Liu Y, Liu J, Shen H. Machine learning model-based preterm birth prediction and clinical nomogram: a big retrospective cohort study. Int J Gynaecol Obstet. 2024;169(1):332–340. doi:10.1002/ijgo.16036
37. Li ZM, Hu JY, Zhang NW, Liu H, Liu W, Wei L. Establishment and validation of a predictive model for spontaneous preterm birth in singleton pregnant women. BMC Pregnancy Childbirth. 2024;24(1):595. doi:10.1186/s12884-024-06772-w
38. Liang S, Chen Y, Jia T, et al. Development of a spontaneous preterm birth predictive model using a panel of serum protein biomarkers for early pregnant women: a nested case-control study. Int J Gynaecol Obstet. 2024;168(2):701–708. doi:10.1002/ijgo.15876
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.