Back to Journals » Patient Preference and Adherence » Volume 20
Development and Validation of a Multidimensional Scale to Assess Cancer Health Education Outcomes in Patients
Received 19 December 2025
Accepted for publication 24 March 2026
Published 15 April 2026 Volume 2026:20 590382
DOI https://doi.org/10.2147/PPA.S590382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ping Yong,1 Tianyun Wang2
1College of International Education, Sichuan International Studies University, Chongqing, People’s Republic of China; 2Department of Oncology, The Third Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Tianyun Wang, Email [email protected]
Background: Effective cancer health education enhances patients’ understanding, emotional regulation, and treatment compliance. However, validated instruments specific to educational outcomes remain limited. These items reflect the proximal effects of education and are not meant to represent generic mental health states.
Objective: To develop and validate a multidimensional scale to assess the effects of cancer health education, including a clear distinction of the outcomes as proximal educational results.
Methods: Following ethical approval, a cross-sectional study was conducted among 236 adult cancer patients recruited at the Third Affiliated Hospital of Chongqing Medical University, Chongqing, China, from 06 January 2025 to 21 March 2025. Item generation was informed by the Health Belief Model, patient interviews, and expert review. The 13-item scale was administered via self-report questionnaire. Internal consistency was evaluated using Cronbach’s alpha, and construct validity was assessed through exploratory factor analysis (EFA).
Results: EFA revealed a three-factor structure—Health Knowledge Comprehension, Emotional-Attitudinal Support, and Health Behavior Implementation—that explained 60.07% of the total variance. This suggests the multidimensional nature of cancer health education outcomes. The scale demonstrated excellent internal consistency (α =0.902), with all subscale alphas exceeding 0.80. Factor loadings ranged from 0.72 to 0.89, indicating strong item-factor relationships.
Conclusion: The Cancer Health Education Scale is a multidimensional instrument with preliminary psychometric support for evaluating educational outcomes in cancer care. Further validation in diverse populations is required. The scale may provide a useful foundation for tailoring patient education programs and supporting future cross-cultural validation studies.
Keywords: health education, neoplasms, questionnaires, patient reported outcome measures, psychometrics
Introduction
Cancer remains one of the leading causes of mortality worldwide and imposes a substantial psychological burden on patients throughout diagnosis and treatment. In addition to its physiological effects, cancer is frequently accompanied by anxiety, depression, and post-traumatic stress symptoms, with prevalence rates significantly higher than those observed in the general population,1 These psychological difficulties can reduce patients’ quality of life, hinder adherence to treatment regimens, and undermine motivation for recovery.2 Prolonged physical discomfort, uncertainty regarding prognosis, and the demanding nature of chemotherapy and radiotherapy further compound emotional distress.3
To address these challenges, increasing attention has been directed toward patient education and self-management interventions.4,5 Hospitals and community health institutions have implemented programs that provide guidance on risk behavior management, medication adherence, symptom monitoring, and emotional coping strategies. Evidence indicates that such interventions can improve self-efficacy, strengthen decision-making autonomy, and enhance overall quality of life.6 Recent work has also framed patient education as a component of broader “patient matters” initiatives that emphasize patient-centered care, safety, and satisfaction within sustainable healthcare systems.7 Despite these advances, there remains a lack of validated instruments capable of comprehensively assessing the cognitive, emotional, and behavioral outcomes of cancer health education, particularly within culturally specific contexts.5,8
A central goal of cancer health education is to equip patients with accurate illness-related knowledge, support emotional adjustment, and promote health-related behaviors that enhance treatment adherence and self-care. In the context of cancer education, improved knowledge and understanding may also enhance patients’ psychological readiness, confidence, and coping ability. Therefore, certain items in this scale capture proximal outcomes of health education, as patients’ emotional and psychological readiness significantly influences their ability to engage with and apply the knowledge gained. These outcomes, though related to mental health, are considered part of the educational process and represent short-term educational effects rather than general psychological well-being. In this sense, they capture the impact of cancer health education on patients’ coping strategies and their readiness to manage their condition. Empirical evidence shows that psychological interventions, such as cognitive behavioral strategies, help reduce emotional distress among cancer patients.9 Additionally, digital health interventions delivered through mobile applications and online platforms have demonstrated benefits for symptom management and psychological well-being.10,11
Although the value of cancer health education has been increasingly recognized, existing assessment tools tend to focus narrowly on knowledge acquisition and often fail to capture emotional responses, behavior change, and psychological adaptation in an integrated manner. This limitation restricts the ability of clinicians and researchers to evaluate how effectively patients internalize and apply educational content in real-world settings.6,12 Therefore, there is a clear need for a cancer-specific, theoretically grounded, and psychometrically sound instrument that can measure the multidimensional outcomes of health education programs.
The present study addresses this gap by developing and validating the Cancer Health Education Scale for adult patients in China. The instrument was constructed through patient interviews, expert review, and empirical testing, and includes dimensions related to health knowledge comprehension, emotional and attitudinal adjustment, and health behavior implementation. The scale aims to support the systematic evaluation of educational outcomes, guide the refinement of intervention strategies, and ultimately contribute to improved psychological well-being and patient-centered cancer care.
Theoretical Background
The development of the Cancer Health Education Scale was guided by a comprehensive theoretical framework that integrates health behavior change models and psychological adjustment theories. Specifically, the scale draws from the Health Belief Model (HBM), Self-Efficacy Theory, the Theory of Planned Behavior (TPB), and Emotion Regulation Theory. Collectively, these models illustrate how educational interventions can shape patients’ cognition, emotional functioning, and health-related behaviors. Based on this framework, three core dimensions were identified: Health Knowledge Comprehension, Emotional–Attitudinal Support, and Health Behavior Implementation.
Health Belief Model
The HBM proposes that individuals’ engagement in health-related behaviors is influenced by their perceived susceptibility and severity of illness, perceived benefits of action, and perceived barriers.13 In cancer education contexts, providing information about cancer etiology, treatment mechanisms, and side-effect management can increase patients’ perceived control and readiness to act. This theoretical foundation informed the development of the Health Knowledge Comprehension dimension, which evaluates how education improves patients’ understanding of their illness and treatment.
Self-Efficacy Theory and Theory of Planned Behavior
Self-efficacy theory emphasizes that individuals’ beliefs in their ability to perform specific behaviors critically influence perseverance, emotional adjustment, and behavioral execution.14 In oncology settings, enhanced self-efficacy has been associated with better symptom management, psychological resilience, and adherence to treatment recommendations.10 Complementing this, the TPB posits that behavioral intentions are shaped by attitudes toward the behavior, perceived social norms, and perceived behavioral control.15,16
Integrating these perspectives, cancer health education should not only increase patients’ awareness of healthy practices but also strengthen motivational and volitional factors that facilitate action. Accordingly, the Health Behavior Implementation dimension was designed to measure patients’ readiness and capacity to follow treatment plans, adopt healthier routines, and engage in self-management behaviors following educational interventions.
Emotion Regulation Theory
Cancer diagnosis and treatment often precipitate substantial emotional distress, including anxiety, fear, and uncertainty. Emotion Regulation Theory posits that individuals cope by monitoring, interpreting, and modifying emotional experiences.17,18 Recent evidence further suggests that improved affect regulation can facilitate sustained engagement in health-promoting behaviors following educational programs.19 Cancer health education can therefore serve as an external resource that helps patients cognitively reframe their experiences, develop adaptive coping strategies, and strengthen emotional resilience. Based on this theoretical foundation, the Emotional–Attitudinal Support dimension was developed to assess the emotional and psychological benefits derived from education.
Existing Instruments and Conceptual Origins
Existing health education outcome instruments generally fall into two broad categories. The first includes measures emphasizing self-efficacy and behavior change, such as the Chronic Disease Self-Efficacy Scale (CDSE) and the Communication and Attitudinal Self-Efficacy Scale for Cancer (CASE-Cancer). While the CDSE assesses patients’ confidence in managing chronic illnesses,12,20 it does not capture cancer-specific knowledge or emotional adjustment. CASE-Cancer focuses primarily on communication-related self-efficacy within healthcare interactions,21 making it useful for clinical consultations but less suitable for evaluating broader educational effectiveness.
The second category comprises multidimensional tools such as the Health Education Impact Questionnaire (heiQ), which evaluates emotional regulation, skill acquisition, constructive attitudes, and social support.6 Although heiQ has been validated among cancer patients,22 it does not address illness-specific cognitive needs or the unique emotional and behavioral challenges of oncology populations.
To address these limitations, this study incorporated qualitative insights from cancer patients to identify key cognitive, emotional, and behavioral outcomes of education. By integrating patient experiences with theoretical constructs, the final instrument provides a contextually grounded and conceptually robust measure reflecting health knowledge, emotional support, and behavioral execution within cancer care.
Methods
This study employed a cross-sectional quantitative design to assess cancer patients’ responses to health education and to evaluate the reliability and preliminary validity of a newly developed measurement scale. The research procedure consisted of five stages: (1) patient interviews and item generation, (2) expert review and content validation, (3) patient pretesting and item refinement, (4) formal questionnaire administration, and (5) exploratory factor analysis (EFA).
The study protocol was approved by the Ethics Committee of the Third Affiliated Hospital of Chongqing Medical University. Written informed consent was obtained from all participants before data collection. All procedures adhered to the ethical principles outlined in the Declaration of Helsinki.
Participants
Participants were adult cancer patients receiving treatment in the oncology department of the Third Affiliated Hospital of Chongqing Medical University, Chongqing, China. Recruitment and questionnaire administration were conducted between 06 January 2025 and 21 March 2025. Inclusion criteria were: (1) clinically confirmed cancer diagnosis; (2) age ≥18 years; (3) ability to read and understand Chinese; (4) willingness to participate and provide informed consent. Exclusion criteria were: (1) severe cognitive impairment; (2) acute medical crisis requiring immediate intervention; (3) inability to complete the questionnaire independently or with minimal assistance.
The study involved multiple participant groups across different development stages. During the item development stage, ten patients who had previously attended cancer health education sessions were purposively recruited to participate in semi-structured interviews. These interviews explored patients’ cognitive, emotional, and behavioral reactions to educational content and informed the initial pool of scale items.
For expert review, six specialists in health education, oncology, and psychology independently assessed the relevance, clarity, and conceptual alignment of the drafted items. During the pretesting phase, an additional group of 20 patients completed a preliminary version of the scale and provided feedback regarding item clarity, wording precision, and contextual appropriateness. Their suggestions guided subsequent refinement of item phrasing and structure.
For the formal survey, 278 questionnaires were distributed through convenience sampling at the same hospital. After excluding 42 incomplete or invalid responses, 236 valid questionnaires were retained, yielding an effective response rate of 84.9%. All participants had a clinically confirmed cancer diagnosis and were undergoing treatment at different stages. Detailed demographic and clinical characteristics are reported in the Results section.
Data Analysis
Data analysis was conducted using SPSS 26.0 and AMOS 24.0. Descriptive statistics were first computed to examine missing data patterns, item distributions, and sample characteristics. Prior to analysis, missing values were evaluated and found to account for 15.1% of the dataset. As the proportion of missing data did not exceed commonly recommended thresholds and preliminary inspection indicated that the missing values were randomly distributed across variables, listwise deletion was applied. Although approximately 15% missing data is not negligible, this approach is considered acceptable in psychometric research when missingness does not appear to be systematic.23,24 Therefore, listwise deletion was used to maintain consistency in the exploratory factor analysis.
Internal consistency was evaluated using Cronbach’s alpha coefficients and corrected item–total correlations. Before performing exploratory factor analysis (EFA), distributional assumptions were assessed. Univariate skewness and kurtosis values were first examined for each item, and multivariate normality was tested using Mardia’s multivariate skewness and kurtosis statistics in AMOS. The results indicated acceptable levels of normality for factor analysis.
EFA was conducted using principal axis factoring (PAF) with Promax rotation to identify the underlying factor structure. Sampling adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) statistic, and the factorability of the correlation matrix was evaluated with Bartlett’s test of sphericity. Factors with eigenvalues greater than 1 and item loadings of at least 0.40 were retained.
Instrument Development
Item Generation
The initial pool of items was generated using a theory-driven and patient-informed approach. First, key constructs were derived from the Health Belief Model, Self-Efficacy Theory, Theory of Planned Behavior, and Emotion Regulation Theory. Second, qualitative data from patient interviews were analyzed using thematic analysis to identify frequently reported needs and experiences related to health knowledge, emotional adjustment, and behavioral change in the context of cancer education. Third, item wording and structure were further informed by established instruments, including the Health Education Impact Questionnaire (heiQ) and the Communication and Attitudinal Self-Efficacy Scale for Cancer (CASE-Cancer).
A total of 18 preliminary items were generated based on theoretical frameworks and patient interviews. During the first stage of expert consultation, three items were removed due to conceptual redundancy and insufficient alignment with the underlying construct. The remaining 15 items were retained as the initial version of the questionnaire. The dimensional classification, sub-constructs, and theoretical foundations of these 15 items are presented in Table 1.
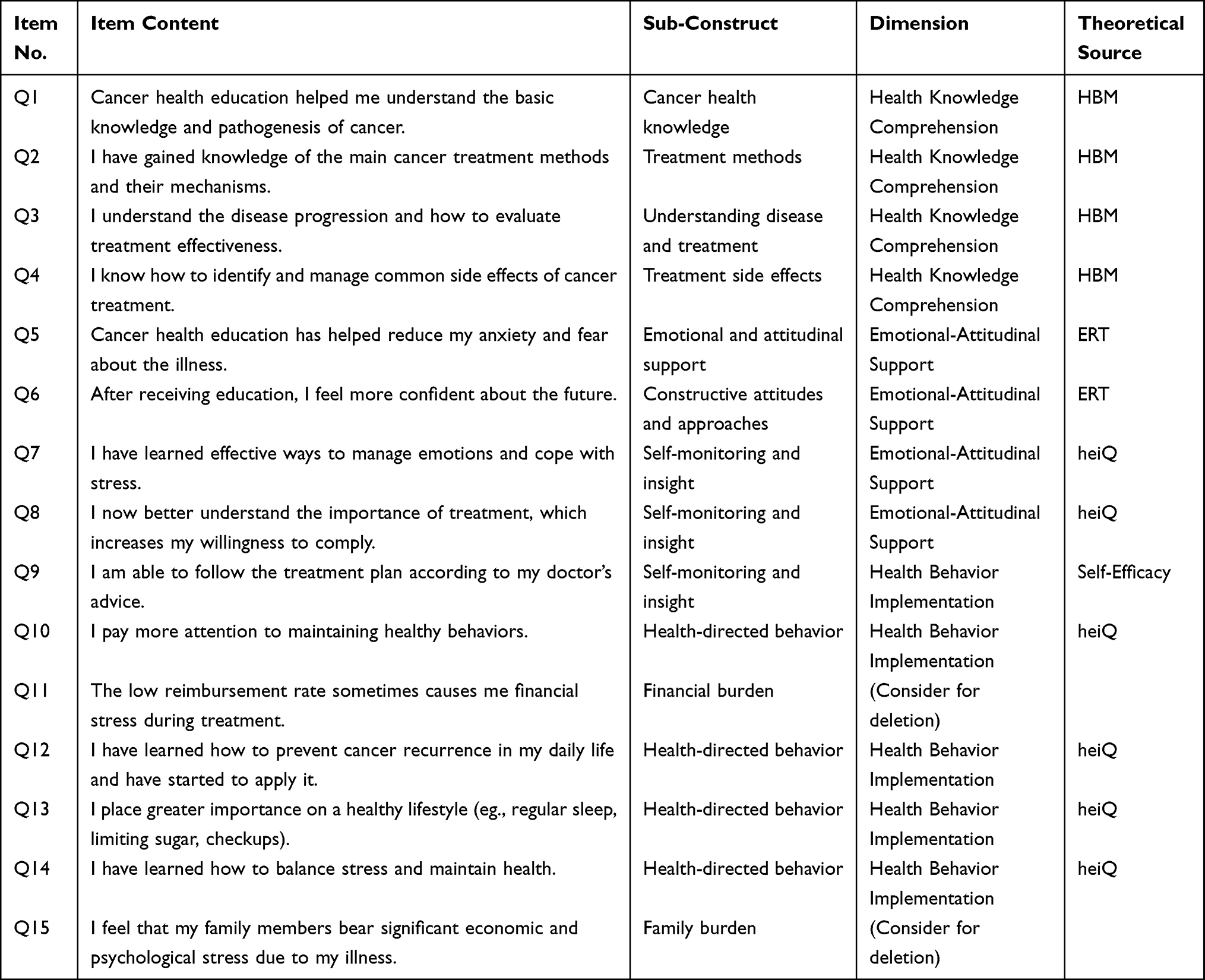 |
Table 1 Presents the Dimensional Classification, Sub-Constructs, and Theoretical Sources for Each Item |
Expert Review and Content Validity Evaluation
Two rounds of content validity assessment were conducted by six experts specializing in health education, psychology, and oncology. Following the preliminary qualitative screening that retained 15 items, experts independently evaluated the relevance and clarity of each item using a 4-point Likert scale (1 = not relevant, 4 = highly relevant). Item-level and scale-level Content Validity Indexes (I-CVI and S-CVI/Ave) were calculated according to established procedures.
In the first round of quantitative evaluation, the average I-CVI across the 15 retained items was 0.944, and the S-CVI/Ave reached 0.969, both exceeding the recommended threshold of 0.90 for satisfactory content validity.25 Two items (Q11 and Q15), which addressed financial stress and family burden, obtained I-CVI values below 0.78 and were therefore removed. Minor wording refinements were made based on expert feedback to enhance clarity and contextual appropriateness. After this process, a final 13-item scale was retained for subsequent psychometric evaluation in Table 2.
 |
Table 2 Item-Level and Scale-Level Content Validity Indices |
Patient Pretesting and Item Refinement
Following expert review, a pilot test was conducted with 20 cancer patients to evaluate item clarity, comprehensibility, and overall acceptability. Most items were well understood by participants, although a few were perceived as abstract or insufficiently specific.
Based on patient feedback, several items were revised to improve linguistic precision and contextual relevance. For instance, the item “I pay more attention to maintaining healthy behaviors” was revised to “Cancer health education has encouraged me to start paying attention to and actively improving my health behaviors (e.g., maintaining a healthy diet, exercising regularly)”. Similarly, “I have learned how to balance stress and maintain health” was modified to “I have learned how to manage stress and improve physical and mental health through specific actions (eg., physical activity, relaxation techniques).” These revisions enhanced the clarity, concreteness, and practical applicability of the items, thereby improving the overall usability of the scale for the target patient population.
Results
Sample Characteristics
A total of 278 questionnaires were distributed through convenience sampling at the Third Affiliated Hospital of Chongqing Medical University, Chongqing, China, between 06 January 2025 and 21 March 2025. After excluding 42 incomplete or invalid responses, 236 valid questionnaires were retained, yielding an effective response rate of 84.9%.
Table 3 presents the demographic and clinical characteristics of the participants. The sample was predominantly female (79.2%) and middle-aged to older adults (age range: 44–88 years). Educational attainment was relatively high, with over 90% having completed middle school or above. Cancer stages were distributed across all four stages, with Stage I and Stage III being most common. The majority of participants (88.1%) had previous exposure to cancer health education, with most reporting moderate frequency (4–6 times).
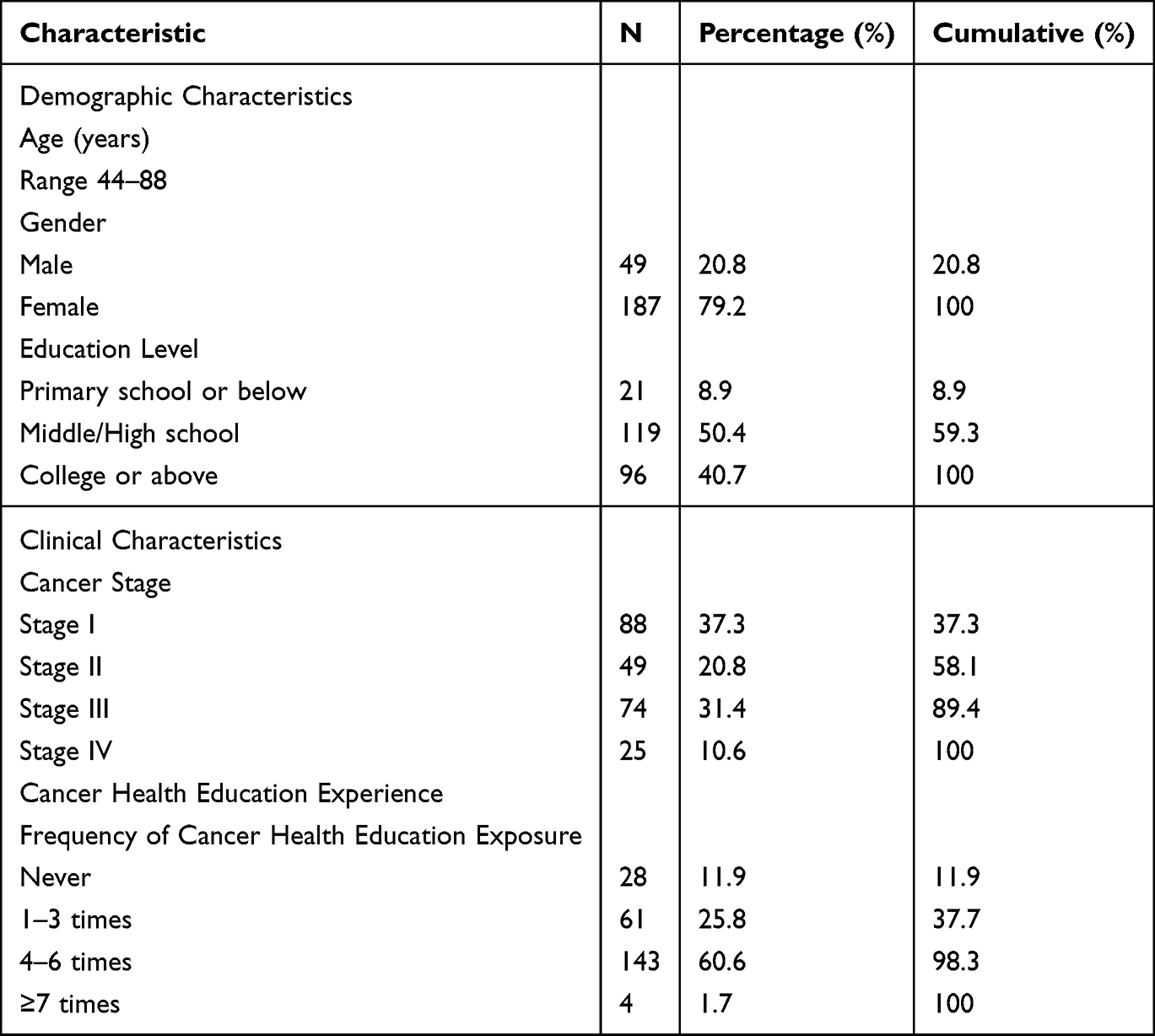 |
Table 3 Demographic and Clinical Characteristics of the Sample (N = 236) |
Descriptive Statistics
A total of 236 valid responses were included in the final analysis. The overall missing data rate was 15.1%, and listwise deletion was applied. Tests of univariate normality showed that item skewness ranged from –1.891 to 0.185 and kurtosis ranged from –0.786 to 5.663. While several items showed elevated kurtosis values, all skewness values fell within the commonly referenced ±2 guideline for approximate normality. The dataset was therefore considered appropriate for subsequent reliability testing and exploratory factor analysis. Mardia’s multivariate kurtosis was –1.848 (CR = –0.719), indicating no violation of multivariate normality. Descriptive statistics for all scale items are presented in Table 4.
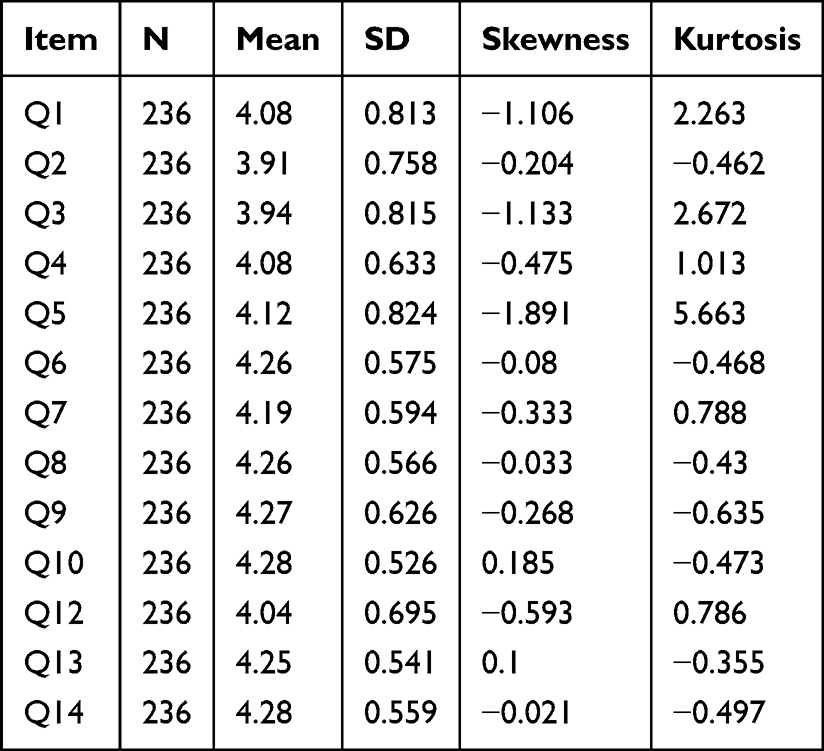 |
Table 4 Descriptive Statistics of Items |
Reliability Analysis
The scale demonstrated excellent internal consistency, with a total Cronbach’s alpha of 0.902. Subscale reliabilities ranged from 0.827 to 0.893. All corrected item–total correlations exceeded 0.40, indicating that each item contributed meaningfully to its respective dimension. Detailed reliability indices, including Cronbach’s alpha coefficients and corrected item–total correlations, are reported in Table 5.
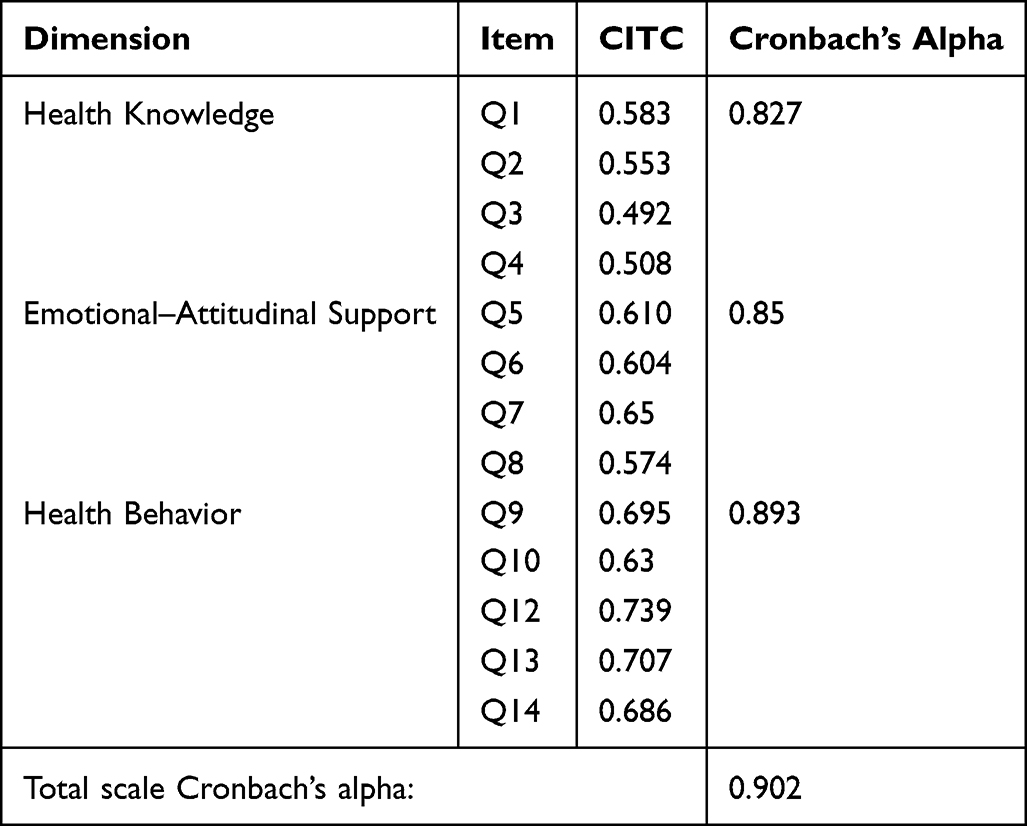 |
Table 5 Cronbach’s Alpha and Corrected Item–Total Correlations for the Cancer Health Education Scale |
Validity Analysis
Content validity was established during the scale development phase through two rounds of expert review. Item-level content validity indices (I-CVI), scale-level indices (S-CVI/UA and S-CVI/Ave), and modified Kappa coefficients (K*) were calculated to assess expert agreement. As the procedures and results were detailed in the Methods section, they are not repeated here.
Exploratory Factor Analysis (EFA)
To examine the underlying structure of the newly developed Cancer Health Education Scale, EFA was conducted on the final 13 items. Principal axis factoring (PAF) was used as the extraction method, followed by Promax rotation to account for potential correlations among factors.
KMO and Bartlett’s Test
Sampling adequacy was confirmed with a Kaiser–Meyer–Olkin (KMO) value of 0.901, indicating an excellent level of inter-item correlation. Bartlett’s test of sphericity was significant (χ2 = 1599.391, df = 78, p < 0.001), supporting the factorability of the correlation matrix. The results of the KMO measure and Bartlett’s test are summarized in Table 6.
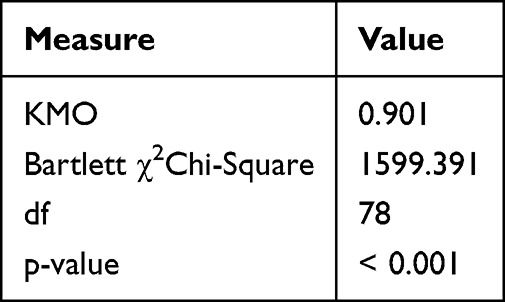 |
Table 6 KMO and Bartlett’s Test |
Total Variance Explained
Three factors were extracted based on eigenvalues greater than 1, accounting for a cumulative variance of 60.072%. Factor 1 explained 43.360% of the variance, Factor 2 explained 9.181%, and Factor 3 explained 7.531%. The eigenvalues and cumulative variance explained by each factor are presented in Table 7.
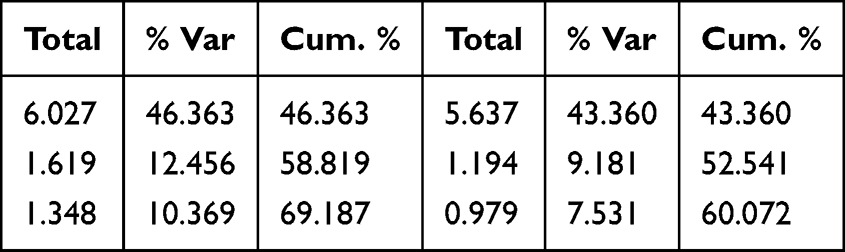 |
Table 7 Total Variance Explained |
Structure Matrix
The structure matrix displays the factor loadings of each item on the extracted components. Most items loaded strongly (≥0.40) on their designated factors, indicating good convergent validity and supporting the theoretical dimensional structure. The factor loadings for all items across the three factors are displayed in Table 8.
 |
Table 8 Structure Matrix |
Discussion
Analysis of Factor Structure Validity
This study developed the Cancer Health Education Scale based on the Health Belief Model (HBM), Self-Efficacy Theory, and Emotion Regulation Theory. Exploratory factor analysis (EFA) identified a three-factor structure—Health Knowledge Comprehension, Emotional-Attitudinal Support, and Health Behavior Implementation—which together accounted for 60.1% of the total variance. This proportion exceeds the commonly referenced 50% guideline in social science research and aligns with recommendations for newly developed patient-reported outcome measures.26 However, given the exploratory nature of EFA, these findings should be interpreted as preliminary rather than definitive evidence of structural validity.
As shown in the structure matrix, the factor loadings for all retained items exceeded 0.70 on their primary factors, suggesting adequate item–factor alignment and limited cross-loadings. This pattern is consistent with psychometric studies of other cancer-specific instruments, such as empowerment, quality-of-life, and health-belief scales, which commonly report item loadings above 0.40–0.60 when theoretical constructs are clearly defined and items are well aligned with patient experience.27 Nevertheless, EFA is primarily intended for initial construct identification rather than confirmatory model testing.
Moreover, the sample size (n = 236, 13 items) meets commonly cited empirical guidelines for exploratory factor analysis, which recommend at least 5–10 participants per item and a minimum of 200 cases to obtain stable factor solutions.28 The scale also demonstrated strong internal consistency (Cronbach’s α = 0.902), with subscale alphas exceeding 0.80. Taken together, these psychometric indicators provide initial support for the structural coherence of the Cancer Health Education Scale. However, further validation using confirmatory factor analysis (CFA) in independent samples is required to verify the stability, replicability, and generalizability of the proposed three-factor model.
Theoretical Alignment and Comparison with Existing Instruments
Theoretical Foundation
Each of the three extracted factors appears to align conceptually with established theoretical frameworks. The Health Knowledge Comprehension dimension appears to reflect key elements of the HBM, particularly perceived benefits and perceived control over illness management, which have been found to predict cancer-related screening and treatment behaviors in recent work on culturally adapted HBM questionnaires and knowledge-attitude-practice (KAP) scales among Chinese patients.29 The Emotional-Attitudinal Support factor may correspond to central processes in Emotion Regulation Theory, such as emotional recognition, cognitive reappraisal, and adaptive coping, which have been shown to mediate the effects of psychoeducational interventions on distress and quality of life in oncology populations.30 The Health Behavior Implementation dimension draws upon constructs from Self-Efficacy Theory and the Theory of Planned Behavior (TPB), consistent with studies demonstrating that perceived behavioral control and self-efficacy are key mechanisms through which cancer education improves adherence, symptom management, and self-care.31
Positioning Among Existing Instruments
Compared to existing tools, the Cancer Health Education Scale may contribute to addressing a gap in outcome measurement. The Health Education Impact Questionnaire (heiQ), while validated in cancer populations and demonstrating good reliability, was originally designed as a generic chronic disease measure focusing on empowerment-related constructs such as health service navigation and skill acquisition.32 However, heiQ was not originally designed to specifically assess disease-specific knowledge or emotional adaptation to cancer diagnosis and treatment, limiting its sensitivity for evaluating oncology-specific education programs.
Similarly, instruments such as the Chronic Disease Self-Efficacy Scale and the Communication and Attitudinal Self-Efficacy Scale for Cancer (CASE-Cancer) focus primarily on self-efficacy in symptom management or healthcare communication, respectively, capturing certain aspects of educational impact rather than a comprehensive multidimensional profile.33 Recent psychometric work on cancer-specific quality-of-life scales—such as the QLICP series and the Cancer Dependent Quality of Life (CancerDQoL) questionnaire—has emphasized the importance of integrating multiple domains (physical, psychological, social, and informational) to assess intervention outcomes comprehensively.34 By explicitly incorporating health knowledge, emotional-attitudinal support, and behavioral implementation into a concise 13-item structure, the present scale may help bridge the gap between generic empowerment tools and more narrowly focused self-efficacy measures, potentially providing a cancer-specific, multidimensional assessment framework. However, further validation is required to confirm its comparative advantages.
Clinical Implications and Quality Improvement Applications
Beyond theoretical alignment, The Cancer Health Education Scale may provide useful insights into clinical applications across three key contexts in oncology care settings, though further validation is needed to confirm its effectiveness.
Baseline Assessment and Needs Identification
As a baseline assessment tool, the scale may be administered at treatment initiation to begin identifying patients’ educational needs across cognitive, emotional, and behavioral domains. However, further studies are needed to confirm its utility in clinical practice. Oncology nurses and patient educators can use the three-dimensional profile to detect specific deficits. For instance, patients scoring low on Health Knowledge Comprehension (Factor 1) may lack understanding of treatment protocols, disease progression, or side-effect management strategies, indicating the need for structured information delivery through multimedia resources, one-on-one counseling, or written educational materials. Conversely, patients with reduced scores on Emotional-Attitudinal Support (Factor 2) may experience heightened anxiety, fear of recurrence, or inadequate psychological preparation for treatment challenges, suggesting the need for psychosocial interventions such as cognitive-behavioral therapy, peer support groups, or mindfulness-based stress reduction programs.
This multidimensional assessment provides an initial step toward moving beyond generic, one-size-fits-all educational approaches and towards more targeted intervention planning. Further research is required to confirm the effectiveness of this approach in practice. Recent systematic reviews have called for more robust and context-sensitive outcome measures to evaluate oncology patient education and self-management interventions, particularly in resource-constrained settings.35 The Cancer Health Education Scale responds directly to this need by providing a brief, psychometrically sound instrument that can be administered alongside education programs to monitor proximal outcomes in real time.
Personalized Education Program Design
The scale may assist in designing personalized education programs by enabling healthcare teams to tailor interventions to individual patient profiles. However, further testing is required to validate its practical application in diverse clinical settings. By analyzing dimension-specific scores, clinicians can match educational strategies to patients’ unique needs and readiness levels. For example, patients demonstrating adequate knowledge (high Factor 1 scores) but poor behavioral implementation (low Factor 3 scores) may benefit from practical skill-building sessions, behavioral coaching, or peer mentorship programs rather than additional didactic instruction. These patients may understand what they should do but lack the confidence, resources, or social support to translate knowledge into action. Interventions such as goal-setting workshops, self-monitoring tools, or family-inclusive education sessions may be particularly effective for this subgroup.
Conversely, patients with strong emotional resilience (high Factor 2 scores) but knowledge gaps (low Factor 1 scores) may respond optimally to structured information delivery through evidence-based educational materials, interactive digital platforms, or nurse-led teaching sessions. This precision approach aligns with contemporary patient-centered care models and maximizes the efficiency of limited educational resources. Studies of continuous care models, nurse-led education, and self-help workbooks suggest that when educational content is customized to patients’ readiness, self-efficacy, and psychosocial context, the impact on self-management and treatment adherence is significantly greater.36
Furthermore, the modular structure of the scale supports targeted refinement of educational content. Low scores on specific dimensions can guide program developers to strengthen particular components—for example, enhancing emotional support resources if Factor 2 scores are consistently low across patient cohorts, or incorporating more practical behavior-change techniques if Factor 3 scores lag behind other dimensions. This evidence-based approach to program improvement aligns with findings from meta-analyses showing that multi-component psychoeducational interventions—those combining information, skills training, and emotional support—are more likely to reduce fatigue, distress, and symptom burden while improving quality of life.35
Outcome Evaluation and Quality Improvement
As an outcome evaluation instrument, the scale may enable systematic monitoring of health education program effectiveness through pre-post comparisons. However, these findings should be considered preliminary, and further validation is needed to assess the scale’s long-term impact across different patient populations. This supports evidence-based quality improvement initiatives by providing objective data on which aspects of education are most effective and which require enhancement. Healthcare institutions can use aggregated data to identify systemic educational gaps, allocate resources strategically, and benchmark performance against established standards or peer institutions.
For example, if pre-post analyses reveal significant improvements in Health Knowledge Comprehension but minimal changes in Emotional-Attitudinal Support, program coordinators can prioritize the integration of psychosocial components such as support groups, counseling services, or stress management workshops. Similarly, if behavioral implementation scores remain low despite improvements in knowledge and emotional adjustment, this may signal the need for more intensive follow-up, environmental modifications to reduce barriers to behavior change, or family-inclusive interventions to strengthen social support networks.
Longitudinal tracking of patient cohorts can also reveal temporal patterns in educational needs across different treatment phases. For instance, newly diagnosed patients may prioritize knowledge acquisition (Factor 1), while those undergoing active treatment may require greater emotional support (Factor 2), and survivors transitioning to long-term follow-up may focus on sustaining health behaviors (Factor 3). Understanding these phase-specific patterns can inform the development of stage-appropriate educational protocols that align with patients’ evolving needs throughout the cancer care continuum.
By providing a standardized, theory-grounded measurement framework, the Cancer Health Education Scale has the potential to enhance care quality through improved patient engagement, treatment adherence, and health outcomes, while simultaneously supporting institutional efforts to optimize educational service delivery in resource-constrained oncology settings. This aligns with broader healthcare quality improvement frameworks that emphasize patient-centered outcomes, evidence-based practice, and continuous performance monitoring.
Limitations and Future Research Directions
This study has several limitations that should be acknowledged. First, participants were recruited from a single tertiary hospital in Chongqing, China, using convenience sampling. This approach may limit the generalizability of the findings to other geographic regions, healthcare settings, or patient populations.25 Therefore, the results should be interpreted with caution, and future studies should aim to replicate these findings in more diverse settings to test their broader applicability.
Second, the sample was predominantly female (79.2%) and middle-aged to older adults (age range: 44–88 years), which may limit the applicability of the scale to male cancer patients and younger adults. This age distribution reflects the demographic characteristics of the hospital’s catchment area, which is located in an older urban district where the majority of residents are middle-aged and elderly. Consequently, younger cancer patients (aged 18–43 years) were underrepresented in this sample. However, it is important to recognize that younger patients may have distinct health education needs related to fertility preservation, career planning, and digital health literacy.37,38 Additionally, research has shown that younger cancer patients exhibit different patterns of information-seeking behavior and emotional responses to diagnosis compared to older adults.39 These age-related differences in health education needs and coping strategies suggest that the three-factor structure identified in this study may not fully capture the experiences of younger cancer populations. Therefore, future studies should aim to recruit more balanced samples across gender and age groups, particularly including younger adults from diverse geographic settings and healthcare facilities. Measurement invariance testing should also be conducted to assess whether the scale’s factor structure remains stable across different demographic subgroups.40
Third, the majority of participants (88.1%) had previous exposure to cancer health education, with most reporting moderate frequency (4–6 times). This high baseline exposure may have influenced their responses to the scale items, potentially inflating scores on certain dimensions. Future studies could aim to recruit patients with varying levels of prior exposure to cancer education to explore whether baseline knowledge impacts the results.
Fourth, due to sample size and design constraints, only exploratory factor analysis (EFA) was conducted. While EFA is appropriate for initial scale development, it is important to recognize that confirmatory factor analysis (CFA) is necessary to establish the stability and replicability of the identified factor structure. Future work should employ independent samples to perform CFA and examine measurement invariance across subgroups.41
Finally, all data were collected through self-report at a single time point, which may introduce social desirability bias and common-method variance.42 To mitigate these limitations, future studies could adopt longitudinal designs and incorporate objective indicators of patient outcomes.
Beyond addressing these methodological limitations, future research should establish additional psychometric properties, including criterion-related validity and cross-cultural validation. Given the age-related differences in health education needs, future validation studies should specifically examine the scale’s performance across different age cohorts.
Conclusion
This study developed and provided preliminary validation evidence for the Cancer Health Education Scale designed for adult cancer patients. Grounded in the Health Belief Model, Self-Efficacy Theory, and Emotion Regulation Theory, the scale was systematically constructed through literature review, patient interviews, expert evaluation, pilot testing, and a hospital-based survey.
Exploratory factor analysis suggested a three-factor structure—Health Knowledge Comprehension, Emotional-Attitudinal Support, and Health Behavior Implementation—with acceptable internal consistency and initial structural support. These findings provide preliminary evidence that the scale may capture cognitive, emotional, and behavioral dimensions of cancer-related health education outcomes. However, as only exploratory analyses were conducted, further confirmatory validation is required to establish the stability and generalizability of the factor structure.
The instrument may offer a concise and theory-informed framework for assessing educational outcomes in oncology settings. Its multidimensional structure has the potential to support needs assessment, intervention tailoring, and outcome monitoring. Nevertheless, its broader clinical applicability should be interpreted cautiously until further validation studies are completed.
Future research should conduct multicenter studies, perform confirmatory factor analysis (CFA), and examine measurement invariance across demographic subgroups to strengthen the psychometric evidence base. Cross-cultural validation and longitudinal research are also necessary to determine predictive validity and long-term utility. Such continued investigation will clarify the scale’s role in supporting evidence-informed and patient-centered cancer education practices.
Data Sharing Statement
All relevant data generated or analyzed during this study are included in the manuscript.
Ethics Statement
Ethical approval for this study was obtained from the Ethics Committee of the Third Affiliated Hospital of Chongqing Medical University (Approval No: 202557). Written informed consent was obtained from all participants.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that no competing interests exist.
References
1. Hinz A, Krauss O, Hauss JP, et al. Anxiety and depression in cancer patients compared with the general population. Eur J Cancer Care. 2009;19(4):522–14. doi:10.1111/j.1365-2354.2009.01088.x
2. Mehnert A, Brähle E, Faller H, Härter M, Keller M. Four-Week prevalence of mental disorders in patients with cancer across major tumor entities. J Clin Oncol. 2014;32(31):3540–3546. doi:10.1200/JCO.2014.56.0086
3. Krebber AMH, Buffart LM, Kleijn G, et al. Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments. Psychooncology. 2014;23(2):121–130. doi:10.1002/pon.3409
4. Bodenheimer T. Patient Self-management of chronic disease in primary care. JAMA. 2002;288(19):2469. doi:10.1001/jama.288.19.2469
5. Newman S, Steed L, Mulligan K. Self-management interventions for chronic illness. Lancet. 2004;364(9444):1523–1537. doi:10.1016/S0140-6736(04)17277-2
6. Osborne RH, Elsworth GR, Whitfield K. The Health Education Impact Questionnaire (heiQ): an outcomes and evaluation measure for patient education and self-management interventions for people with chronic conditions. Patient Educ Couns. 2007;66(2):192–201. doi:10.1016/j.pec.2006.12.002
7. Moldovan F, Moldovan L. Assessment of patient matters in healthcare facilities. Healthcare. 2024;12(3):3. doi:10.3390/healthcare12030325
8. Brady TJ. Measures of self-efficacy, helplessness, mastery, and control: the Arthritis Helplessness Index (AHI)/Rheumatology Attitudes Index (RAI), Arthritis Self-Efficacy Scale (ASES), Children’s Arthritis Self-Efficacy Scale (CASE), Generalized Self-Efficacy Scale (GSES), Mastery Scale, Multi-Dimensional Health Locus of Control Scale (MHLC), Parent’s Arthritis Self-Efficacy Scale (PASE), Rheumatoid Arthritis Self-Efficacy Scale (RASE), and Self-Efficacy Scale (SES). 2003. doi:10.1002/art.11413
9. Faller H, Schuler M, Richard M, Heckl U, Weis J, Küffner R. Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: systematic review and meta-analysis. J Clin Oncol. 2013;31(6):782–793. doi:10.1200/JCO.2011.40.8922
10. Kim SH, Sung JH, Yoo SH, et al. Effects of digital self-management symptom interventions on symptom outcomes in adult cancer patients: a systematic review and meta-analysis. Eur J Oncol Nurs. 2023;66:102404. doi:10.1016/j.ejon.2023.102404
11. Qin M, Chen B, Sun S, Liu X. Effect of mobile phone app–based interventions on quality of life and psychological symptoms among adult cancer survivors: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res. 2022;24(12):e39799.
12. Beatty L, Kemp E, Butow P, et al. A systematic review of psychotherapeutic interventions for women with metastatic breast cancer: context matters. Psychooncology. 2018;27(1):34–42. doi:10.1002/pon.4445
13. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
14. Bandura A. Self-efficacy: the exercise of control. 1997.
15. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991.
16. Ajzen I. The theory of planned behavior: frequently asked questions. Hum Behav Emerg Technol. 2020;2(4):314–324. doi:10.1002/hbe2.195
17. Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2(3):271–299. doi:10.1037/1089-2680.2.3.271
18. Gross JJ. Emotion regulation: current status and future prospects. Psychol Inq. 2015;26(1):1–26. doi:10.1080/1047840X.2014.940781
19. Yang MZ, Conner M, Sheeran P. The role of affect regulation in health behavior change. Health Psychol. 2025;44(9):876–885. doi:10.1037/hea0001507
20. Lorig K, Stewart A, Ritter P, González V, Laurent D, Lynch J. Outcome Measures for Health Education and Other Health Care Interventions. Sage Publications; 1996.
21. Wolf MS, Chang CH, Davis T, Makoul G. Development and validation of the communication and attitudinal self-efficacy scale for cancer (CASE-cancer). Patient Educ Couns. 2005;57(3):333–341. doi:10.1016/j.pec.2004.09.005
22. Maunsell E, Lauzier S, Brunet J, et al. Health-related empowerment in cancer: validity of scales from the Health Education Impact Questionnaire (heiQ). Health Qual Life Outcomes. 2014;12(1):1–13. doi:10.1186/s12955-014-0126-5
23. Bennett DA. How can I deal with missing data in my study? Aust N Z J Public Health. 2001;25(5):464–469. doi:10.1111/j.1467-842X.2001.tb00294.x
24. Schafer JL, Graham JW. Missing data: our view of the state of the art. Psychol Methods. 2002;7(2):147–177. doi:10.1037/1082-989X.7.2.147
25. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
26. Morgado FFR, Meireles JFF, Neves CM, Amaral ACS, Ferreira MEC. Scale development: ten main limitations and recommendations to improve future research practices. Psicol Reflex Crít. 2017;30:3. doi:10.1186/s41155-016-0057-1
27. Maunsell E, Lauzier S, Brunet J, Pelletier S, Osborne RH, Campbell HS. Health-related empowerment in cancer: validity of scales from the health education impact questionnaire. Cancer. 2014;120(20):3228–3236. doi:10.1002/cncr.28847
28. MacCallum RC, Widaman KF, Zhang S, Hong S. Sample size in factor analysis. Psychol Methods. 1999;4(1):84–99. doi:10.1037/1082-989X.4.1.84
29. Liao Y, Hairon SM, Yaacob NM, Ismail TAT, Luo L. Psychometric validation of a culturally adapted health belief model scale for breast cancer screening in Chinese women. PLoS One. 2025;20(9):e0331279. doi:10.1371/journal.pone.0331279
30. Howell D, Harth T, Brown J, Bennett C, Boyko S. Self-management education interventions for patients with cancer: a systematic review. Support Care Cancer. 2017;25(4):1323–1355. doi:10.1007/s00520-016-3500-z
31. Shahraki M, Bameri F, Mashmooli S, Taheri M. The effect of continuous care model on cancer patients’ self-efficacy: a randomized controlled trial. J Nurs Adv Clin Sci. 2024;1(4):182–186. doi:10.32598/JNACS.2408.1050
32. Davidson J, Taylor MD, Gilbride CJ, et al. Psychometric evaluation of the cancer dependent quality of life (CancerDQoL) questionnaire: an individualised measure of the impact of cancer and its treatment on quality of life. Psychooncology. 2024;33(10):e70002. doi:10.1002/pon.70002
33. Momayyezi M, Fallahzadeh H, Momayyezi M. Construction and validation the lifestyle questionnaire related to cancer. Iran J Cancer Prev. 2015;8(5):0–6. doi:10.17795/ijcp-3965
34. Li F, Jiali Z, Wan C, et al. Development and validation of the breast cancer scale QLICP-BR V2.0 based on classical test theory and generalizability theory. Front Oncol. 2022;12(915103). doi:10.3389/fonc.2022.915103
35. Christiansen K, Buswell L, Fadelu T. A systematic review of patient education strategies for oncology patients in low- and middle-income countries. Oncologist. 2023;28(1):2–11. doi:10.1093/oncolo/oyac206
36. Reif K, de Vries U, Petermann F, Görres S. A patient education program is effective in reducing cancer-related fatigue: a multi-centre randomised two-group waiting-list controlled intervention trial. Eur J Oncol Nurs: Off J Eur Oncol Nurs Soc. 2013;17(2):204–213. doi:10.1016/j.ejon.2012.07.002
37. Keegan THM, Lichtensztajn DY, Kato I, et al. Unmet adolescent and young adult cancer survivors information and service needs: a population-based cancer registry study. J Cancer Surviv. 2012;6(3):239–250. doi:10.1007/s11764-012-0219-9
38. Smith AW, Bellizzi KM, Keegan THM, et al. Health-related quality of life of adolescent and young adult patients with cancer in the United States: the adolescent and young adult health outcomes and patient experience study. J Clin Oncol. 2013;31(17):2136–2145. doi:10.1200/JCO.2012.47.3173
39. Rabin C, Simpson N, Morrow K, Pinto B. Behavioral and psychosocial program needs of young adult cancer survivors. Qual Health Res. 2011;21(6):796–806. doi:10.1177/1049732310380060
40. Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. 2016;41:71–90. doi:10.1016/j.dr.2016.06.004
41. Brown TA. Confirmatory Factor Analysis for Applied Research (2nd Ed.). Guilford Press.; 2015.
42. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.