Back to Journals » Patient Preference and Adherence » Volume 11
Development and utilization of the Medicines Use Review patient satisfaction questionnaire
Authors Hindi A ![]() , Parkhurst C, Rashidi Y
, Parkhurst C, Rashidi Y ![]() , Ho SY, Patel N
, Ho SY, Patel N ![]() , Donyai P
, Donyai P ![]()
Received 21 July 2017
Accepted for publication 14 September 2017
Published 20 October 2017 Volume 2017:11 Pages 1797—1806
DOI https://doi.org/10.2147/PPA.S146991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ali Hindi,1 Caroline Parkhurst,1,2 Yasamin Rashidi,1 Shun Yan Ho,1 Nilesh Patel,1 Parastou Donyai1
1Department of Pharmacy, University of Reading, Berkshire, UK; 2Professional Services Department, Day Lewis Pharmacy Group, Croydon, London, UK
Abstract: The Medicines Use Review is a community pharmacy service funded in the United Kingdom to improve patients’ adherence to medication and reduce medicines waste. The objective was to develop, pilot, and utilize a new Medicines Use Review patient satisfaction questionnaire. A questionnaire for patient self-completion was developed using a published framework of patient satisfaction with the Medicines Use Review service. The questions were validated using the content validity index and the questionnaire piloted through three pharmacies (February–April 2016). The revised questionnaire contained 12 questions with responses on a 5-point Likert scale, and a comments box. The questionnaire was distributed to patients following a Medicines Use Review consultation via community pharmacies (June–October 2016). Exploratory factor analysis and Cronbach’s α were performed to investigate the relationships between the items and to examine structural validity. The survey results were examined for patients’ reported satisfaction with Medicines Use Reviews, while the handwritten comments were thematically analyzed and mapped against the questionnaire items. An estimated 2,151 questionnaires were handed out, and a total of 505 responses were received indicating a 24% response rate. Exploratory factor analysis revealed two factors with a cumulative variance of 68.8%, and Cronbach’s α showed high internal consistency for each factor (α=0.90 and α=0.89, respectively). The survey results demonstrated that patients could show a high degree of overall satisfaction with the service, even if initially reluctant to take part in a Medicines Use Review. The results support the Medicines Use Review patient satisfaction questionnaire as a suitable tool for measuring patient satisfaction with the Medicines Use Review service. A wider study is needed to confirm the findings about this community pharmacy-based adherence service.
Keywords: community pharmacy, Medicines Use Review, patient satisfaction, questionnaire, adherence
Plain language summary
We wanted to see if patients are happy with a drug store service. The service focuses on checking people’s medicines with them. The service is also about checking that people are taking their medicines. We produced a list of questions for people to answer. We made certain that the list of questions was as best as possible. We gave the list of questions to over 2,000 people. Just over 500 people sent us their answers. People were happy with the service even if they did not want to take part at first. Our results mean we have a list of questions for other people to use in the future.
Introduction
The medical management and prevention of many conditions rely on the prescribing and use of medicines. Yet, for a variety of reasons, patients commonly fail to adhere to medication instructions.1,2 The issue of medication nonadherence is particularly problematic with chronic conditions where adherence is estimated to be around 50%.3 Medication nonadherence potentially reduces clinical benefit and quality of life in patients, in turn increasing the burden of ill health, medicines waste, hospitalization, emergency admissions, and death.4 As a potential solution, medication adherence reviews are offered as a pharmacy service across a number of European countries, including the United Kingdom.5
In the UK, the Medicines Use Review (MUR) service consists of a yearly one-to-one patient–pharmacist consultation; introduced in 2005, the aim of the service is to address concerns and questions about all of a patient’s medication to improve their adherence.6 Yet, patients’ satisfaction with the service has not been formally measured. Internationally, the World Health Organization has emphasized the importance of the patient’s perspective in the evaluation of health services.7 Patient satisfaction is broadly conceptualized as the extent to which a patient is content with a health service encounter. As well as being a significant indicator of the perceived quality of care and success of health care services in general,8,9 past research has demonstrated patient satisfaction to be a key determinant of adherence to medical advice.10 Logically, if patients are satisfied with a service such as the MUR, this has the potential to improve their adherence, and measuring patient satisfaction, for example using a questionnaire, could then become a valid mechanism for auditing service quality.7,11 But existing pharmacy patient satisfaction questionnaires offer limited scope as detailed in the following paragraphs.
The hallmark of a good questionnaire is one that fully captures all of the constructs relating to the concept it is measuring.12 An in-depth review conducted by Panvelkar et al13 evaluated five instruments for measuring patient satisfaction with community pharmacy services per se, none of which was developed by collaborating with patients to obtain their perspectives on the topic. Moreover, only two of the instruments14,15 focused on patient satisfaction with services that might resemble the MUR, and while one requires further testing14 the other was developed in the Spanish language.15 A different, more recently published study can also be criticized for not being based on patients’ own perspectives of the pharmacy service in question.16 Examining the broader concept of pharmaceutical care services provided for outpatients, a more recent review of patient satisfaction questionnaires unearthed 12 studies, but highlighted that only one study had developed an instrument to be directly applied in the evaluation of community pharmacy services.17 The authors recommended that consistent with Donabedian’s framework,18 future research should be directed toward the development and validation of structure, process, and outcome indicators for evaluating the quality of pharmaceutical care services. The constructs identified by patients as being important to their experience and satisfaction with the MUR have in fact been previously mapped against Donabedian’s structure–process–outcome framework.19 Based on the MUR patient satisfaction framework,19 the current paper aimed to assess patient satisfaction with the MUR service by developing, piloting, and utilizing a new MUR patient satisfaction questionnaire (MUR-PSQ), which was completed and is described here.
Materials and methods
Compliance with ethical standards
This study was approved by the University of Reading’s Research Ethics Committee through the School Exemptions process reference number 13/16 on 25/02/2016.
Instrument development and content validation
The MUR-PSQ version 1 (v1) was designed to have items that were relevant to patient satisfaction with the MUR service19 and be simple and easy to understand, with clear instructions, and a reasonable completion time (<10 minutes). Therefore there were no negatively worded items or reverse scoring of any item. The MUR-PSQ-v1 included 12 positively worded questions (items) each with a 5-point Likert response scale (1= strongly disagree to 5= strongly agree). A comments box was also added to check that the questionnaire captured all of the relevant concepts being expressed by people experiencing the service.
Ascertaining the content validity index (CVI) was deemed appropriate for establishing the content validity (CV) of the questionnaire. This is because CVI measures the extent of agreement between experts about each questionnaire item (hereon referred to as the item CVI; I-CVI), and this helps improve each question where needed.20 A panel of 12 pharmacists involved in patient care (eg, community or hospital pharmacy posts) was recruited for the CV exercise. Specifically, a set of three questions for validating each item of the MUR-PSQ-v1 (Table 1) was devised by adapting an established cognitive theory model for determining CV.21 Each pharmacist panel member was asked to read each of the items on the MUR-PSQ-v1 in turn and answer three distinct CV questions on a 4-point Likert response scale from (1= strongly disagree to 4= strongly agree). The three distinct CV questions were “Q1. This question is easy to understand,” “Q2. The responses available are appropriate for the question asked” and “Q3. This question is relevant to measuring patient satisfaction with an MUR service.”
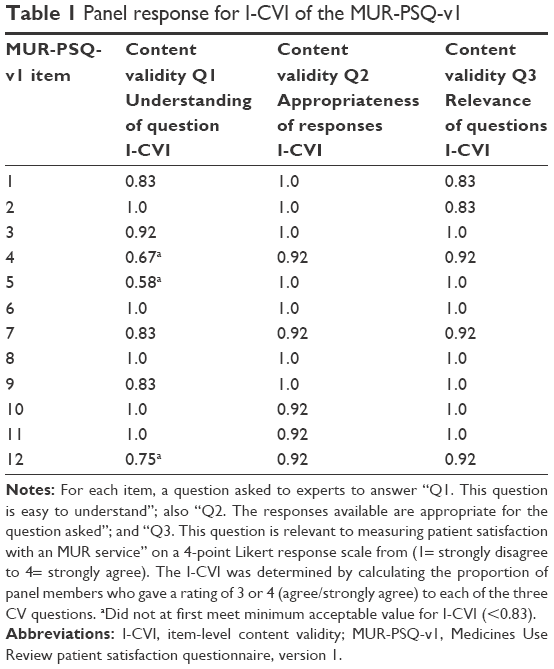 | Table 1 Panel response for I-CVI of the MUR-PSQ-v1 |
The I-CVI was determined by calculating the proportion of panel members who gave a rating of 3 or 4 (agree or strongly agree) to each of three CV questions relating to each questionnaire item. An I-CVI of ≥0.83 (10 ratings of 3 or 4 from 12 ratings) was judged as the minimum acceptable value for the combined rating for responses to each CV question. This minimum acceptable value was based on Lynn’s criteria,22 and any item not receiving the minimum acceptable value for any of the three CV questions was subjected to revision and re-evaluation.
The response options were judged to be appropriate for all 12 items of the questionnaire (CV Q2 I-CVI ≥0.83), and all 12 items were judged to be relevant (CV Q3 I-CVI ≥0.83) for measuring patient satisfaction with MURs (Table 1). The panel recommended rephrasing three items (items 4, 5, and 12) for greater clarity (CV Q1). The wording of these was amended to produce a second version of the MUR-PSQ version 2. A further review by the panel deemed all three revised items to be acceptable (I-CVI ≥0.83).
In addition to the this, the appropriateness and understandability of the MUR-PSQ-v1 in the target population was examined with the help of three community pharmacists in the East of England, who handed out the MUR-PSQ-v1 (and accompanying information letters and return envelopes) to 60 patients following an MUR consultation during February–April 2016. Patients in turn posted their self-completed questionnaire to the University for the authors’ attention. The returned questionnaires (n=30) were completed in full, and no comments regarding the questionnaire layout or wording were reported.
Instrument testing
The revised questionnaire (MUR-PSQ-v2) was distributed to 250 community pharmacies belonging to one pharmacy chain in England (covering the South East, Central, and West of England, but with branches also in the North of England) between June and October 2016. Each pharmacy involved in the study received 20 patient questionnaire packs for distribution. The questionnaire packs contained the MUR-PSQ-v2, an accompanying information letter, two copies of a written informed consent form, and a return envelope (addressed to the University for the authors’ attention). Each pharmacy also received a letter inviting the pharmacist to take part by handing out one questionnaire pack to each patient following an MUR consultation. It was not possible to accurately determine the number of patient packs handed out, but an attempt was made to estimate this through a retrospective telephone survey completed with the 250 pharmacies. This involved one of the coauthors (CP) telephoning each pharmacy branch to ask about the number of questionnaire packs given out/remaining from the batch of 20 packs sent to them. Patients in turn posted their self-completed questionnaire and one copy of the signed written informed consent form to the authors, thus allowing an estimation of the response rate to be made by dividing the number of responses returned to the researchers by the total number of patient packs which pharmacists declared to have handed out.
On receipt, the questionnaire responses were analyzed using the Statistical Software for Social Sciences version 21 (IBM Corp., Armonk, NY, USA). Exploratory factor analysis was carried out to identify, understand, and interpret the relationships between the items on the MUR-PSQ-v2, explicitly in order to determine independent latent constructs known as “factors.” As part of the analysis, the correlation between the variables was examined by creating a correlation matrix.
The Kaiser–Meyer–Olkin (KMO) value was used to evaluate sample adequacy for factor analysis, where a KMO of 0.5 is considered to be minimum, 0.5–0.7 mediocre, 0.7–0.8 good, 0.8–0.9 great, and >0.9 superb.23 Bartlett’s test of sphericity was also completed to ensure that the study assumptions were satisfied for factor analysis by looking for a statistically significant value of less than 0.05.23
A number of procedures exist to determine the optimal number of factors to retain in exploratory factor analysis. In this study, based on Kaiser’s criteria,23 factors with eigenvalues greater than 1 were selected. Also, the scree plot method,23 a subjective test requiring researchers’ judgment, was used to confirm factor findings. Construct validity was confirmed if the factors accounted for a minimum of 50% of the variance.24 Items on the questionnaire were grouped into factors based on the factor loadings, and an item was considered significant if its loading was ≥0.40.25 To retain an item, the factor loading of the item was higher than 0.30. Cronbach’s α was used to measure the instrument’s internal reliability by evaluating the consistency of responses between the items contained within any identified factors on the MUR-PSQ-v2.26
The MUR-PSQ-v2 survey responses were also examined for patient-reported satisfaction with MURs. In addition, the handwritten comments received were analyzed by theoretical thematic analysis,27 meaning data were examined, coded, and themed for ideas that related to the research question, ie, patients’ satisfaction with MURs. The themes generated were juxtaposed against items on the MUR-PSQ-V2 to check if the questionnaire captured all of these concepts.
Results
All 250 branches of a community pharmacy chain (covering mainly the South East, Central, and West of England, but with branches also in the North of England) were invited to take part by handing out one questionnaire pack to each patient following an MUR consultation. A telephone survey completed between November and December 2016 estimated that 2,151 questionnaires had been given out to patients. A total of 505 questionnaires were returned by patients to the authors, resulting in an estimated response rate of 24%.
Exploratory factor analysis & reliability testing
The intercorrelation between all the items was 0.2–0.825, which provided an indication that all the individual items were interrelated yet not redundant or highly correlated (Table S1).23 A high KMO value of 0.94 confirmed that the sample was acceptable for factor analysis.23 Additionally, Bartlett’s test of sphericity (4,229.155, df=66, p=0.000) confirmed that the assumptions for factor analysis were satisfied in this study. Based on the Kaisers criteria, in which factors with eigenvalue >1 are retained (Table S2), factor analysis presented two factors, with a cumulative variance of 68.8%. The presence of two factors was also confirmed with the scree plot.
None of the items loaded significantly onto both factors, thereby indicating the uniqueness of each individual item and its specificity to a certain factor (Table 2). The first factor had 7 items and was labeled as “experiencing the service”, while the other 5 items loaded onto factor 2 which was labeled as “judging the service.” Furthermore, reliability analysis using Cronbach’s α revealed that all items on factor 1 (α=0.90) and factor 2 (α=0.89) had excellent internal consistency.
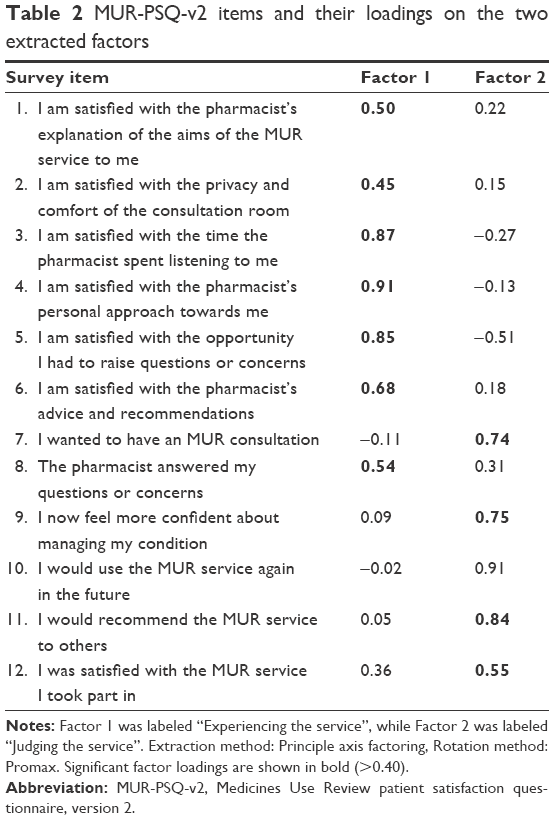 | Table 2 MUR-PSQ-v2 items and their loadings on the two extracted factors |
Patient satisfaction with the MUR
A total of 489 people (97%) agreed or strongly agreed that they were satisfied with the MUR service they had received (Table S3, specifically responses to item 12). Agreement was highest in relation to satisfaction with the time spent by the pharmacist listening (98%) and the pharmacist’s personal approach toward the patient (98%). There was also high satisfaction with explanations of the aims of the service (96%), the comfort and privacy of the consultation room (96%), the opportunity to raise questions or concerns (97%) and have these answered (95%), and generally the pharmacists’ advice and recommendations (96%). Eight out of ten patients agreed they felt more confident about their condition following the MUR. Interestingly, only 328 people (65%) had wanted to have an MUR at the outset. Despite this, nine out of ten people would use the service again, and the same number would recommend it to others.
The handwritten comments on the returned questionnaires were grouped into four main themes, which are shown below with illustrative quotes. The themes identified could all be mapped against the items on the MUR-PSQ-v2 (Table 3).
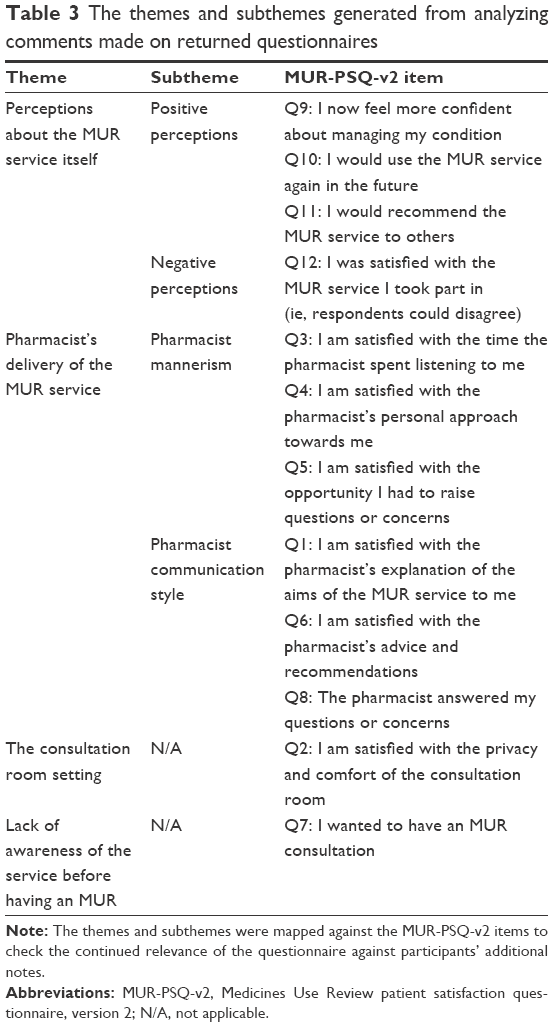 | Table 3 The themes and subthemes generated from analyzing comments made on returned questionnaires |
Theme 1: Perceptions about the MUR service itself
Positive perceptions
This subtheme relates to positive perceptions about the MUR, such as it being a helpful, reassuring, informative, and personalized patient–pharmacist discussion. For example:
Found it very helpful to have this MUR with my local pharmacist if anything more helpful than my GP. (Patient no 217)
Didn’t realize just how beneficial this service could be to me – felt more comfortable, reassured, realized more could be done for me as when necessary – very good. (Patient no 218)
Negative perceptions
This subtheme relates to negative perceptions about the MUR, mainly about the purpose of the MUR being unclear. For example:
Think this is a waste of time and money. If I need further advice I would ask my doctor and consultant has already explained the medications. (Patient no 299)
Theme 2: Pharmacist’s delivery of the MUR service
Pharmacist mannerism
This subtheme relates to pharmacists being professional, approachable, helpful, friendly, or caring. For example:
The pharmacist was very friendly and made me feel very well calm and comfortable. (Patient no 364)
The pharmacist was very helpful young man, and did not try to rush me through it. (Patient no 211)
Pharmacist communication style
This subtheme relates to pharmacists as people who offered advice, answered relevant questions, and delivered adequate as well as new explanations about medications. For example:
My pharmacist advised me on questions I had and also taught me some things I did not know. (Patient no 93)
I am grateful to be given the chance and time to ask questions about the medications I take and their interaction with each other. The pharmacist also suggested the best times to take individual drugs. (Patient no 310)
Theme 3: The consultation room setting
This theme relates to the privacy and size of the consultation room. For example:
The only issue I had was once in consulting room anybody on other side of the room could hear! (Patient no 155)
Consultation room was very small referred to as cupboard, but ok. (Patient no 240)
Theme 4: Lack of awareness of the service before having an MUR
This theme relates to people being unaware of the MUR service prior to their consultation. For example:
I was unaware of this service. Anything which assists a person to feel supported/have the opportunity to further discuss medications is very much appreciated. (Patient no 230)
I was unaware of the MUR until invited to discuss my medication with the pharmacist. (Patient no 30)
Discussion
A new questionnaire was devised, piloted, and tested for the purpose of measuring patient satisfaction with the MUR service in the UK. The CVI and piloting established the clarity, relevance, and appropriateness of all 12 items on the MUR-PSQ-v2. Exploratory factor analysis extracted two unique factors labeled as “experiencing the service” and “judging the service” without dual loadings. Moreover, Cronbach’s α revealed high internal consistency between the items grouped under each of the two factors. The results of the survey infer a high degree of patient satisfaction with experiencing the MUR service as well as with judging its impact although this result is not conclusive considering the low response rate, which was estimated to be 24%.
The two factors identified through factor analysis, “experiencing the service” and “judging the service”, concurred with the layout of the MUR-PSQ-v2, in which the first half focuses on the patient experience with the consultation while the second half focuses on the outcomes and evaluations of the MUR service itself. These two factors bear some important similarities and differences with factors identified in previous patient satisfaction questionnaires. Previous questionnaires examining patient satisfaction with pharmacy services have generated multiple factors that are arguably irrelevant to the MUR adherence-focused service, including factors such as “financial aspects,” “product availability”, and “technical quality.”15,28,29 While the updated MacKeigan and Larson tool14 produced two dimensions that share some commonality with the “experiencing the service” factor, the MUR-PSQ-v2 factor “judging the service” is new, perhaps because the current questionnaire is rooted in patients’ perspectives, which is detailed elsewhere.19 In comparison to previous instruments,14–16,28–30 limiting the questionnaire to 12 specific items also avoided drawbacks commonly identified in previous surveys such as lengthy completion time and multiple dual loadings.
When analyzing people’s responses on the MUR-PSQ-v2, a high degree of satisfaction with the MUR service was found, which as stated earlier, needs to be treated with caution in light of the low response rate. This is in line with two previous formal studies that have shown high patient satisfaction with community pharmacy services16,30 and with one study that more informally examined patient satisfaction with the MUR service.31 Of particular interest was item 7, “I wanted to have an MUR consultation’, which produced a considerably lower score than all the other items – ie, 33% of the respondents did not agree/strongly agree with this statement. Despite this response, patients who received the MUR service and returned the questionnaire were very satisfied with it. Similarly, previous qualitative studies showed that patients who take part in MURs did not necessarily want the service at first or think they will benefit from it.19,32 This is in line with a general reluctance to use community pharmacy services, as reported elsewhere.33–35 However, what is important about the current study is that it has shown that reluctance to take part does not equate with satisfaction once the service is experienced. Therefore, it can be argued that focusing on patient recruitment processes, eg, whether reluctant patients are being recruited, is not a valid measure of patient satisfaction with the MUR service.
To our knowledge, this is the first quantitative, national study of patient satisfaction with the MUR service carried out in the UK. In addition, this is one of only a handful of “pharmacy adherence service” patient satisfaction questionnaires developed on the basis of patients’ perspectives. This case is being made because, as demonstrated in the “Introduction” section, a highly relevant in-depth review by Panvelkar et al13 unearthed only five relevant instruments, and our own search found one more research questionnaire,16 none of which was developed through patient collaboration. And although the MUR-PSQ-v2 was not developed actively with patients, it was nonetheless based on patient perspectives and organized into a framework of MUR satisfaction as illustrated in a previously published paper.19 Another strength of the current study is that the MUR-PSQ-v2 underwent thorough testing before, during, and after development to enhance its trustworthiness. With only 12 items included in the questionnaire, the instrument can be deemed to be easy to use and also to compute for the purpose of analysis. The study provides a mechanism for measuring people’s satisfaction with the MUR service. This could be useful for auditing, comparing, and improving this pharmacy adherence service. In addition, since medication adherence reviews are offered as a pharmacy service across a number of European countries,6 the MUR-PSQ-v2 provides a basis for adaptation and use in Europe and beyond.
A limitation of the study is the apparent low response rate for the survey, which was calculated by dividing the number of responses returned to the researchers by the total number of patient packs which pharmacists declared to have handed out, the latter determined during a retrospective telephone survey. The potential for an “over statement” bias cannot be ruled out, with pharmacists overstating the number of patient packs they distributed to patients in order to demonstrate better engagement with the project, which would superficially inflate the denominator and result in a lower response rate. On the face of it, the current response rate means that it is possible the survey did not capture responses from a large proportion of questionnaire recipients, either because they were unable to complete the questionnaire or were not satisfied with their MUR and did not want to report this.
Having said that, looking at recent literature in this field, the response rate is similar to another satisfaction study in pharmacy that also relied on the postal service36 (19.2% response rate), which is important considering that studies which rely on handing out and being handed back questionnaires within the pharmacy setting still do not result in sizeable response rates (45.85%37 and 58%38). The decision to ask patients to post their questionnaires directly back to the researchers was made to reduce the chances of introducing unwanted bias. For example, posting the completed questionnaires directly to the research team meant that individual pharmacists delivering the service were bypassed, thereby eliminating the risk of pharmacists concealing less favorable returned responses from the research team, and the process was also thought to encourage honest patient responses by affording anonymity.
There is of course the possibility of selection bias in terms of whom the pharmacists chose to receive the MUR patient packs, which could only be addressed through more labor-intensive, less cost-effective methodologies relying on independent researchers handing out and collecting back the satisfaction questionnaires, which was outside of the scope of this study. However, by virtue of the questionnaire’s design, it was important that patients completed the MUR-PSQ-v2 away from the pharmacy, having had the opportunity to reflect on their experience in order to answer the questions associated with factor 2, “judging the service”.
Conclusion
This study has produced the MUR-PSQ-v2 as a tool to measure patient satisfaction with the adherence-focused MUR service. This is the first MUR-PSQ based on a framework built on patients’ perspectives. Survey scores revealed that patients who completed and returned the survey were satisfied with their MUR service despite initial reluctance to participate. The development of the MUR-PSQ-v2 is a significant advancement for evaluating patient satisfaction with community pharmacy adherence services such as the MUR. Future research will confirm the findings of this study with a wider population of patients, and the questionnaire could be used for auditing, comparing, and improving the MUR and other adherence services in the UK and beyond.
Acknowledgments
The authors would like to acknowledge and thank the pharmacies, pharmacists, and patients who participated in the study. Without their contributions, the study could not have been successful. We also thank the East of England Respiratory Strategic Clinical Network for helping with the dissemination of questionnaires during the content validation phase and Day Lewis Pharmacy Group for helping to disseminate the questionnaires during the formal data collection period.
Disclosure
Dr Caroline Parkhurst is employed by the Day Lewis Pharmacy Group. The authors report no other conflicts of interest in this work.
References
Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003. | ||
Holloway K, van Dijk L. The World Medicines Situation 2011: Rational Use of Medicines. Geneva: World Health organization; 2011. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. | ||
Simpson S, Eurich D, Majumdar S, et al. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ. 2006;333:15. | ||
Bulajeva A, Labberton L, Leikola S, et al. Medication review practices in European countries. Res Social Adm Pharm. 2014;10:731–740. | ||
The Prescribing Services Negotiating Committee. Medicines Use Review (MUR). Available from: http://psnc.org.uk/services-commissioning/advanced-services/murs/. Accessed March 7, 2017. | ||
Murray C, Frenk J. A framework for assessing the performance of health systems. Bull World Health Organ. 2000;78:171–731. | ||
Aharony L, Strasser S. Patient satisfaction: What we know about and what we still need to explore. Med Care Res Rev. 1993;50:49–79. | ||
Clearly P, McNeil B. Patient satisfaction as an indicator of quality care. Inquiry. 1988;25:25–36. | ||
Ley P. Improving patients’ understanding, recall, satisfaction and compliance. In: Broome K, editors. Health psychology. London: Chapman and Hall; 1989:74–102. | ||
Jackson J, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52:609–620. | ||
Marshall G, Hays R, Sherbourne C, et al. The structure of patient satisfaction with outpatient medical care. Psychol Assess. 1993;5:477–483. | ||
Panvelkar PN, Saini B, Armour C. Measurement of patient satisfaction with community pharmacy services: a review. Pharm World Sci. 2009;31:525–537. | ||
Larson L, Rovers J, MacKeigan L. Patient satisfaction with pharmaceutical care: update of a validated instrument. J Am Pharm Assoc. 2002;42:44–50. | ||
Traverso M, Salamano M, Botta C, et al. Questionnaire to assess patient satisfaction with pharmaceutical care in Spanish language. Int J Qual Health Care. 2007;19:217–224. | ||
Sakharkar P, Bounthavong M, Hirsch J, et al. Development and validation of PSPSQ 2.0 measuring patient satisfaction with pharmacist services. Res Social Adm Pharm. 2015;11:487–498. | ||
Lima TM, Aguiar PM, Storpirtis S. Evaluation of quality indicator instruments for pharmaceutical care services: A systematic review and psychometric properties analysis. Res Soc Adm Pharm. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1551741117300475. Accessed September 8, 2017. | ||
Donabedian A. Evaluating the quality of medical care. Milbank Q. 2005;83(4):691–729. | ||
van den Berg M, Donyai P. A conceptual framework of patient satisfaction with a pharmacy adherence service. Int J Clin Pharm. 2014;36:182–191. | ||
Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29:489–497. | ||
Tourangeau R. Cognitive science and survey methods: A cognitive perspective. In: Jabine T, Straf M, Tanur J, et al, editors. Cognitive Aspects of Survey Methodology. Washington, DC: National Academy Press; 1984:73–100. | ||
Lynn M. Determination and quantification of content validity. Nurs Res. 1986;35:382–385. | ||
Field A. Discovering Statistics using SPSS. London: Sage Publications; 2005. | ||
Terwee CB. Protocol for systematic reviews of measurement properties. Knowledge Center Measurement Instruments. 2011:13. Available from: http://www.cosmin.nl/images/upload/files/Protocol klinimetrische review version nov 2011.pdf | ||
Fabrigar L, Wegener D, MacCallum R, et al. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4:272–299. | ||
Streiner D, Norman G, Cairney J. Health Measurement Scales: A Practical Guide to their Development and Use. 5th ed. Oxford: Oxford University Press; 2014:159–196. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
MacKeigan LD, Larson LN. Development and validation of an instrument to measure patient satisfaction with pharmacy services. Med Care. 1989;27(5):522–536. | ||
Hasan S, Sulieman H, Stewart K, et al. Assessing patient satisfaction with community pharmacy in the UAE using a newly-validated tool. Res Social Adm Pharm. 2013;9:841–850. | ||
Gourley G, Gourley D, Rigolosi E, et al. Development and validation of the pharmaceutical care satisfaction questionnaire. Am J Manag Care. 2001;7:461–466. | ||
Youssef S, Hussain S, Upton D. Do patients perceive any benefit from medicines use reviews offered to them in community pharmacies? Pharm J. 2010;284(7589):165–166. | ||
Latif A, Boardman H, Pollock K. Understanding the patient perspective of the English community pharmacy Medicines Use Review (MUR). Res Social Adm Pharm. 2013;9:949–957. | ||
Gidman W, Cowley J. A qualitative exploration of opinions on the community pharmacists’ role amongst the general public in Scotland. Int J Pharm Pract. 2012;21:288–296. | ||
McMillan S, Kelly F, Sav A, et al. Consumer and carer views of Australian community pharmacy practice: awareness, experiences and expectations. J Pharm Health Serv Res. 2013;5:29–36. | ||
Wood K, Gibson F, Radley A, et al. Pharmaceutical care of older people: what do older people want from community pharmacy? Int J Pharm Pract. 2015;23:121–130. | ||
Moon J, Kolar C, Brummel A, Ekstrand M, Holtan H, Rehrauer D. Development and validation of a patient satisfaction survey for comprehensive medication management. J Manag Care Spec Pharm. 2016;22(1):81–86. | ||
Alomi YA, Kurdy L, Aljarad Z, Basudan H, Almekwar B, Almahmood S. Patient satisfaction of pharmaceutical care of primary care centers at Ministry of Health in Saudi Arabia. J Pharm Pract Community Med. 2016;2(23):79–87. | ||
Malewski DF, Ream A, Gaither CA. Patient satisfaction with community pharmacy: Comparing urban and suburban chain-pharmacy populations. Res Soc Adm Pharm. 2015;11(1):121–128. |
Supplementary materials
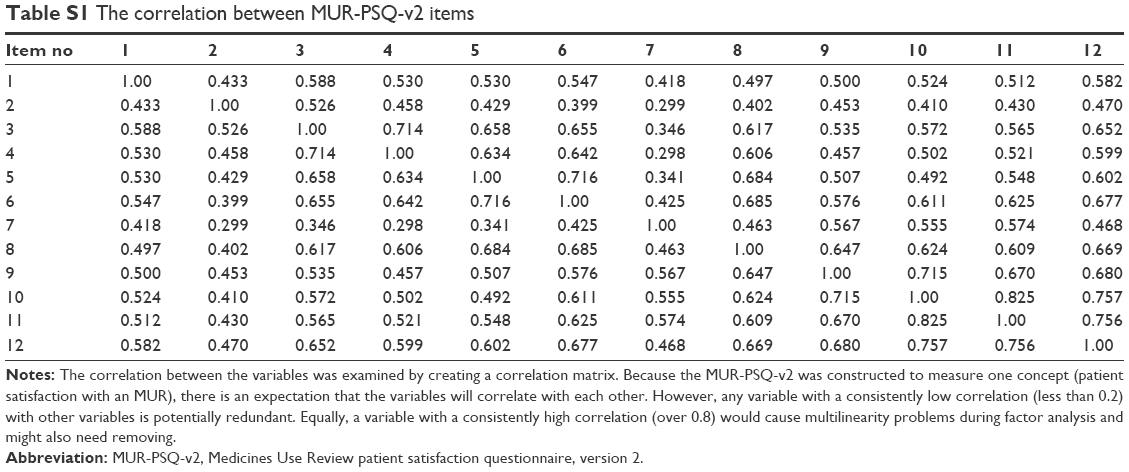 | Table S1 The correlation between MUR-PSQ-v2 items |
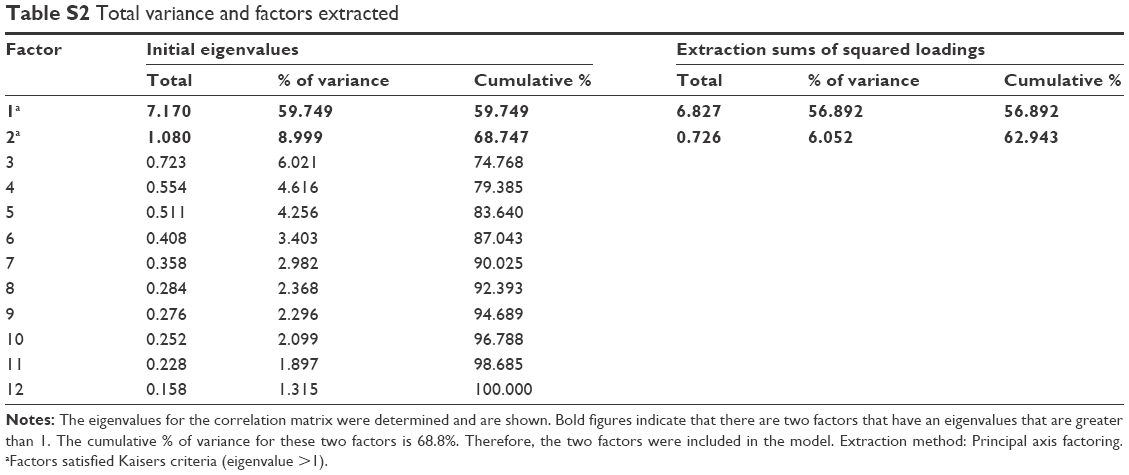 | Table S2 Total variance and factors extracted |
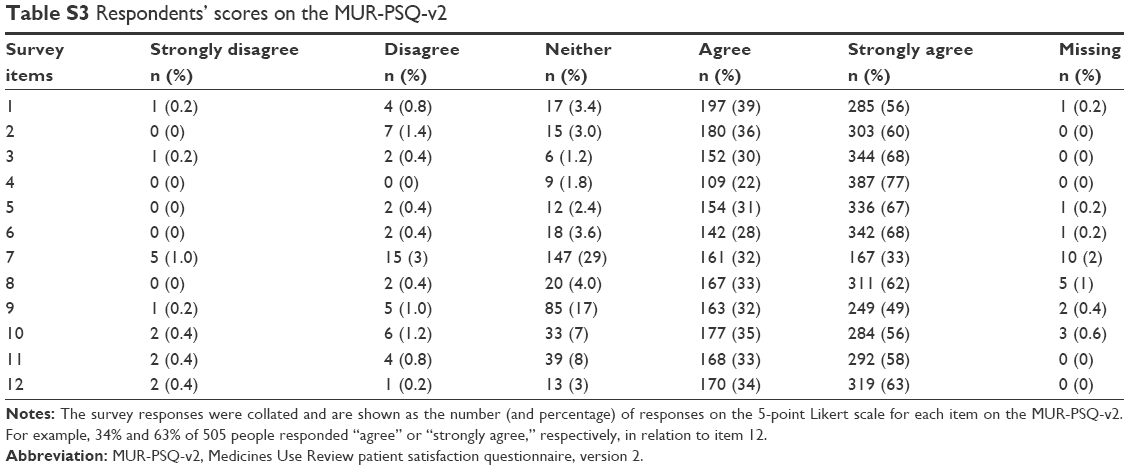 | Table S3 Respondents’ scores on the MUR-PSQ-v2 |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.