Back to Journals » Patient Preference and Adherence » Volume 16
Development and Pilot Usefulness Testing of an Interactive Computerized Patient Decision Aid for Intraocular Lens Selection Before Cataract Surgery
Authors Tsai CB ![]() , Fang CL, Chen MS, Yen MY, Yeh CY, Lai ZM, Hsu ML, Wang ST
, Fang CL, Chen MS, Yen MY, Yeh CY, Lai ZM, Hsu ML, Wang ST
Received 10 October 2021
Accepted for publication 12 January 2022
Published 25 January 2022 Volume 2022:16 Pages 189—196
DOI https://doi.org/10.2147/PPA.S343655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Chong-Bin Tsai,1,2 Chien-Liang Fang,3,4 Ming-Shan Chen,5,6 Min-Yueh Yen,1 Chi-Yen Yeh,7 Zhi-Ming Lai,7 Mei-Ling Hsu,7 Shan-Tair Wang8
1Department of Ophthalmology, Ditmanson Medical Foundation Chiayi Christian Hospital, Chiayi City, Taiwan; 2Department of Optometry, College of Medical and Health Science, Asia University, Taichung, Taiwan; 3Division of Plastic and Reconstruction Surgery, Department of Surgery, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi City, Taiwan; 4Department of Food Nutrition and Health Biotechnology, College of Medical and Health Science, Asia University, Taichung City, Taiwan; 5Department of Anesthesiology, Ditmanson Medical Foundation Chiayi Christian Hospital, Chiayi City, Taiwan; 6Department of Biotechnology, Asia University, Taichung City, Taiwan; 7Department of Information Technology, Ditmanson Medical Foundation Chiayi Christian Hospital, Chiayi City, Taiwan; 8Department of Medical Research, Ditmanson Medical Foundation Chiayi Christian Hospital, Chiayi City, Taiwan
Correspondence: Chong-Bin Tsai, Department of Ophthalmology, Ditmanson Medical Foundation Chiayi Christian Hospital, No. 539 Zhongxiao Road, East District, Chiayi City, 60002, Taiwan, Tel +886-5-2765041 ext 8503, Fax +886-5-2774511, Email [email protected]
Purpose: Modern cataract surgeries aim to treat impaired vision and also improve quality of life. An appropriate pre-operative selection of the intraocular lens is important to post-operative quality of life. Patients often have difficulty in choosing the best fit for individual needs. Patient decision aids (PDAs) are useful tools to assist patients in such decision-making process. However, most PDAs are paper-based and lack user interaction. This study is aimed to develop and evaluate an interactive computerized patient decision aid (cPDA) to help patients in the selection of an appropriate intraocular lens model before cataract surgery.
Materials and Methods: Patients and their families who were making the decision regarding intraocular lens selection before cataract surgeries were eligible to participate in this study. A cPDA was built on an interactive robot, to help the patients in the decision-making process. The usefulness of the cPDA was measured with the Decision Self-Efficacy (DSE) scale and Preparation for Decision Making (PrepDM) scale.
Results: A total of 50 participants (18 men and 32 women) were enrolled in the pilot test. The mean pre-cPDA DSE score was 46.5 ± 13.6, and the post-cPDA DSE score was 72.6 ± 12.8. The average gain score on DSE was 26.1, and the standard deviation was 8.0. The gain score on DSE was statistically significant, and the effect size was bigger than 3. The patients with junior or senior high degrees had the highest gain score on DSE, and the ones with college or above degrees had the lowest. The patients with college or above degrees had the highest PrepDM score, and the ones with elementary school or below had the lowest. Age and sex were not significant correlates of PrepDM. The patients with college or above degrees had the highest preparedness, but the lowest gain on DSE.
Conclusion: Education levels are associated with the usefulness of cPDA, both for the preparedness and decision efficacy of patients. The results provide insight into the feasibility of cPDA for the decision-making of pre-operative intraocular lens selection.
Keywords: decision making, preparedness, decision self-efficacy, education level
Introduction
Cataract is the leading cause of visual impairment in aging populations.1 Modern cataract surgeries aim to not only treat impaired vision but also to improve quality of life. The continued development of intraocular lens (IOL) technology provides cataract patients numerous options of refractive corrections after cataract surgeries. Patients of different vocations, reading habits, and lifestyles will benefit from different models of IOL. Therefore, an appropriate decision of IOL selection is crucial to post-operative quality of life. Patients should be informed of the benefits and risks, and also consider their personal values and preferences, to make an appropriate decision. Patient decision aids (PDA) are evidence-based tools designed to help patients make specific and deliberate choices among health-care options.2 Presently, most PDA in use are paper-based and less approachable. Nonetheless, in the past decade, the practices of healthcare have moved toward an era of information technology. Therefore, computer-based decision aids are emerging in various fields of clinical practice.3 Although doctor-patient communications are essential in the shared decision-making process, computer-based decision aids may help patients to properly digest the vast amount of information before their discussion with doctors. The advantages of computer-based over paper-based decision aids are their ability to interact with users. Syrowatka et al had identified six important features of computer-based decision aids: content control, tailoring, patient narratives, explicit values clarification, feedback, and social support.4 In an attempt to apply these features in clinical practice, we developed and evaluated a computerized patient decision aid (cPDA) built on an interactive robot, to help patients in the selection of an appropriate IOL model before cataract surgery.
Materials and Methods
Development of the PDA
We searched for clinical researches published in English for IOL selections on PubMed between 2000 and 2019. The following keywords were used, “intraocular lens”, “monofocal”, “multifocal”, and “extended depth of focus”. The retrieved articles were reviewed for their level of evidence. The information regarding efficacy, safety, convenience, and cost were extracted from the reviewed articles.5–10 Important contents were adapted for the PDA, as recommended by the International Patient Decision Aids Standards (IPDAS) Collaboration.11,12 The PDA consisted of five parts. Part 1 is an introduction of the disease of cataract and its surgical management with IOL implantation. Part 2 lists all the IOL options and the strengths and weakness of each IOL model, including a tabular comparison of various options. Part 3 is comprised of a questionnaire to help patients rank their values and personal preferences of their visual needs in work and daily life. Part 4 is a small quiz to test the knowledge learned. Part 5 is a recommendation to the patients after considering their preferences and the knowledge they learned in the previous steps.
Computerize the PDA on a Robot
The cPDA was built on an interactive robot Zenbo (ASUSTek Computer Inc., New Taipei City, Taiwan). Zenbo is an Android-based robot equipped with a screen, speakers, camera, and multiple sensors to interact with users. The PDA were transformed into a user-machine dialogue with dialogue development environment (DDE) Editor and Zenbo APP Builder. The DDE Editor is a web-based interface to create and integrate conversational interfaces. The Zenbo APP Builder is a visual programming tool that allows developers to edit the codes by simply drag-and-drop-blocks, to control the flow and action on Zenbo. The interactive robot Zenbo can have dialogues with users through on-screen display and voice communication.
All five parts of the PDA were integrated into the cPDA. The cPDA first provides an introduction of the disease of cataract and its surgical management with IOL implantation. Then, it lists all the IOL options and the strengths and weakness of each IOL model, including a tabular comparison of various options, and will give a small quiz to test the knowledge learned. The quiz was in the form of a true or false test. If the patients failed the quiz, the cPDA would return to the prior sessions and then repeat the quiz. If the patients passed the quiz, the cPDA would proceed forward. After initial educational steps about relevant knowledge, the cPDA guides the patients through a series of questionnaires designed to help the patients assess their visual needs in detailed tasks, during sports, driving at night, desire to be glasses-free, as well as their financial concerns. The interactive cPDA provides specific questionnaires depending on the patient’s choice of preference. In the end, the cPDA summarizes the preferences and recommends an IOL selection (Figure 1).
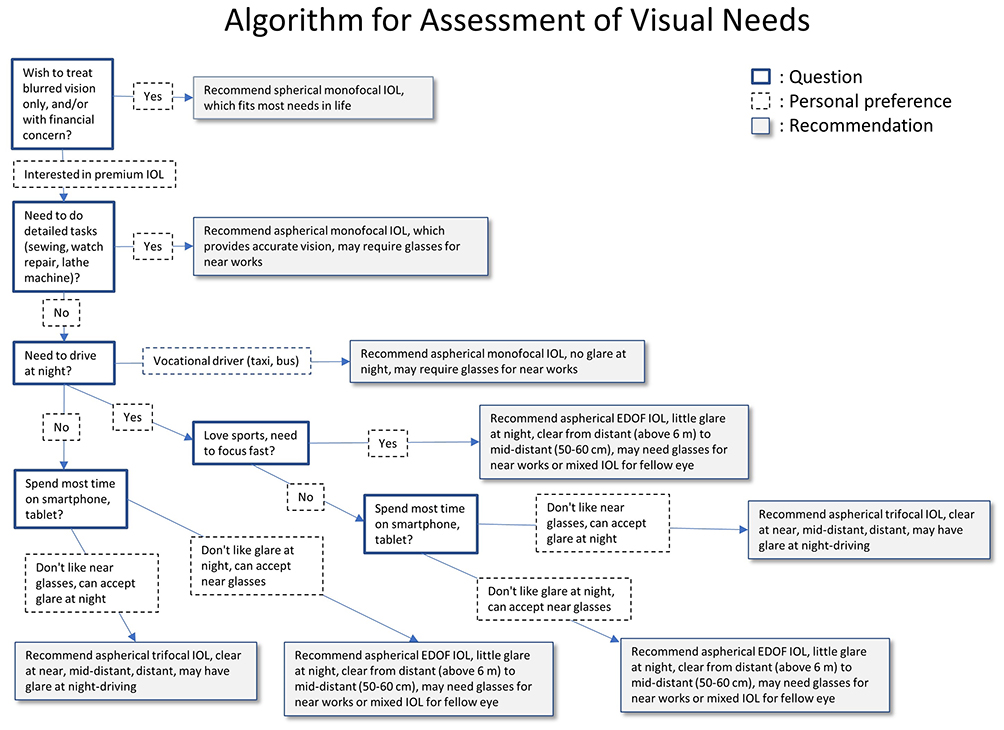 |
Figure 1 Algorithm for assessment of visual needs adopted by computerized patient decision aids. Abbreviations: EDOF, extended depth-of-focus; IOL, intraocular lens. |
Pilot Testing of the cPDA
We conducted a pilot study for the helpfulness of the cPDA for decision-making in IOL selection before cataract surgery. The study was approved by the Institutional Review Board of Ditmanson Medical Foundation Chiayi Christian Hospital (Permit No. 2020102) and was conducted in accordance with the Declaration of Helsinki. Patients and their families who were making the decision on IOL selection before cataract surgeries were eligible to participate in this study. Participants of different education levels were enrolled if they met the following criteria: (1) age of at least 20 years; (2) ability to speak and understand the Mandarin language; (3) no prior experience of decision-making in IOL selection. Informed consent was obtained from each participant in the study.
To test the helpfulness of the cPDA, we utilized two measurement tools, the Decision Self- Efficacy (DSE) scale13,14 and the Preparation for Decision Making (PrepDM) scale.15 Both scales and their Chinese versions were developed by the Ottawa Hospital Research Institute. The DSE scale consists of 11 items and the PrepDM scale consists of 10 items. Before the decision-making process, the participants complete the first half of the questionnaire for the pre-cPDA DSE scale. After receiving an introduction of basic operations, the participants went through the decision-making process with the aid of the cPDA (Figure 2). Each participant was tested individually in a separate room, to avoid interference. As the cPDA on robot Zenbo was interactive, the participants could order the robot to repeat certain steps of cPDA if they did not fully understand the information provided. After the process, the participants completed the second half of the questionnaire for the post-cPDA DSE scale and the PrepDM scale.
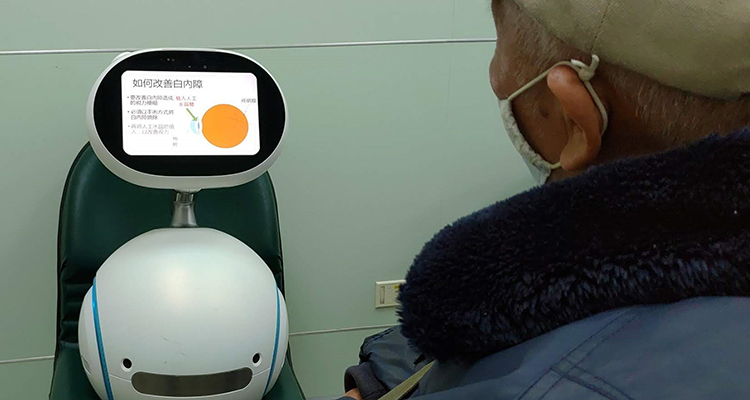 |
Figure 2 A participant underwent the decision-making process using the computerized patient decision aids on an interactive robot. The robot was equipped with a touchscreen, speakers, camera, and multiple sensors to interact with users. In the photo, the screen is explaining how the intraocular lens can treat the cataract via audio and graphic expression. |
Results
A total of 50 participants (18 men and 32 women) were enrolled in the pilot test. The average age was 68.9 (range from 33 to 78) years. The patients with elementary education or below consisted of 44%, those with junior or senior high were 40%, and those of college or above education comprised 16% (Table 1).
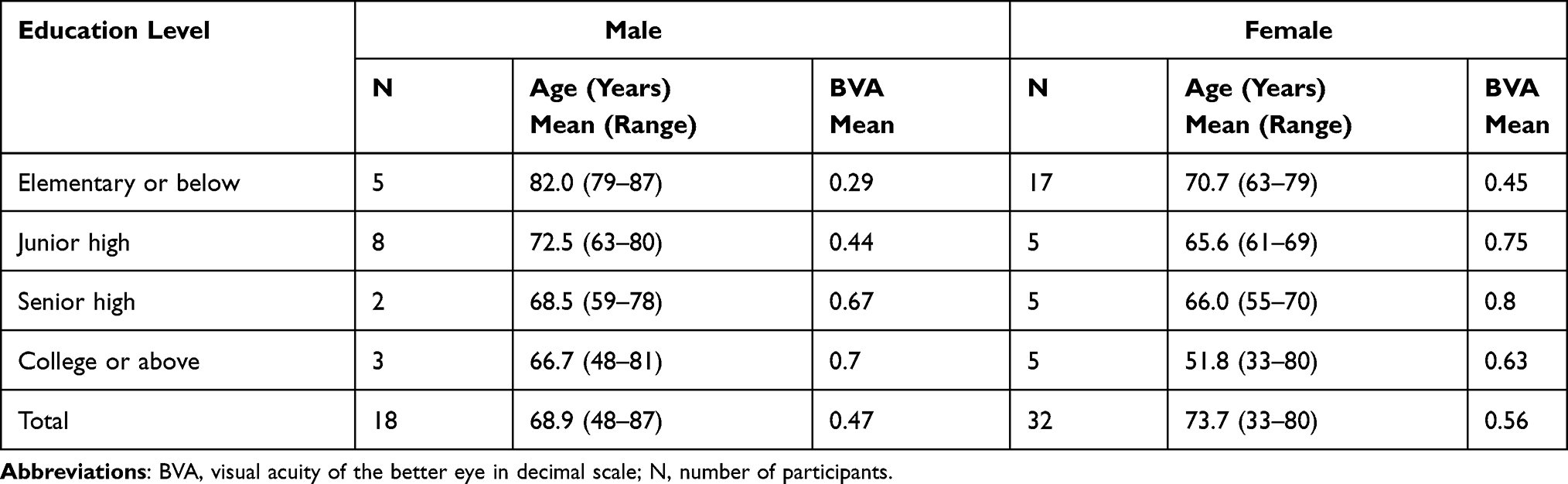 |
Table 1 Basic Information of Participants |
Difference of DSE Scores Before and After the cPDA
The pre-cPDA and post-cPDA scores on DSE were computed as the sum of item scores divided by 11 and multiplied by 25. The results were stratified into different education levels (Table 2). The mean for pre-cPDA DSE score was 46.5 and the standard deviation was 13.6. Its distribution was skewed to the right. The post-cPDA mean DSE was 72.6 and the standard deviation was 12.8. Its distribution was slightly skewed to the left. The average gain score on DSE was 26.1 and the standard deviation was 8.0. The Shapiro–Wilk test for normality indicated that the gain score on DSE was normally distributed (p=0.30). The 95% confidence interval for the gain score on DSE ranged from 23.8 to 28.4. In summary, the gain score on DSE was statistically significant and the effect size was more than three.
 |
Table 2 Pre-cPDA, Post-cPDA, and Gain Scores on DSE and PrepDM Scores Among Participants with Different Education Levels |
Age, Sex, and Education Level in Relation to Gain Score on DSE and PrepDM
The PrepDM scores were computed as the sum of item scores divided by 10 and multiplied by 25. Multiple linear regression of the gain score on DSE and PrepDM on age, sex, and educational level is presented in Table 3. The patients with junior or senior high degrees had the highest gain score on DSE, followed by those with elementary school degrees or below, while the patients with college or above degrees had the lowest. The difference between the highest and lowest gain score was 7.4 and the associated 95% confidence interval was 0.3–14.6. Age and sex were not significant predictors for the gain score on DSE. The patients with college or above degrees had the highest PrepDM score, followed by those with junior or senior high education, and those with elementary school degrees or below had the lowest. The difference between the lowest and highest score was −7.8 and the associated 95% confidence interval was from −13.0 to −2.5. Age, sex, and visual acuity of the better eye were not significant correlates of PrepDM. In summary, the patients with college or above degrees had the highest preparedness, but the lowest gain on DSE.
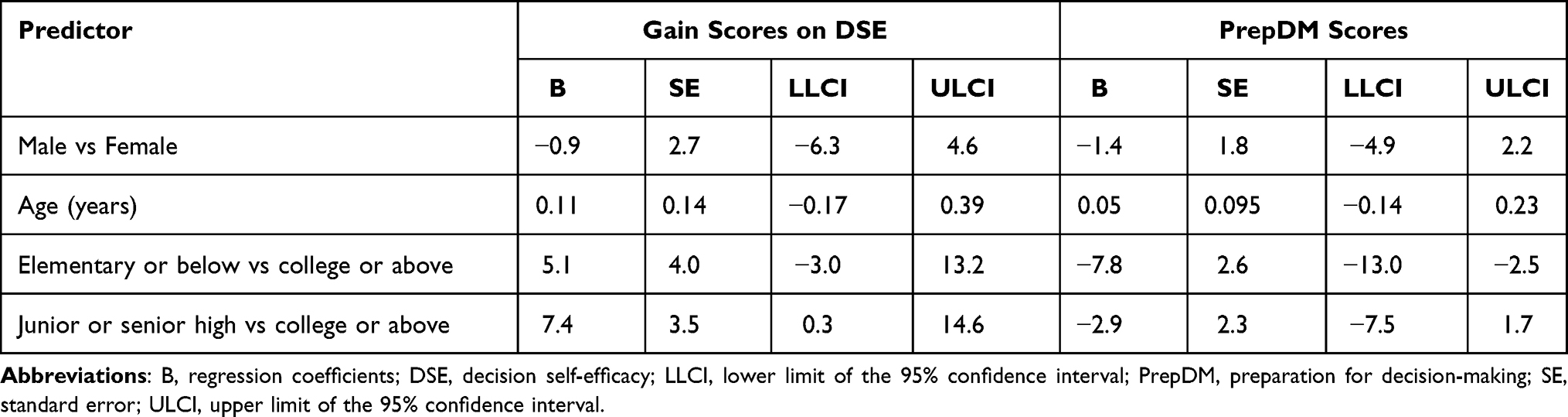 |
Table 3 Multiple Linear Regression of the Correlates for the Gain Scores on DSE and PrepDM Scores |
Discussion
In our pilot testing, patients of all education levels had significant gain of scores on DSE. The patients with junior or senior high degrees had the highest gain score on DSE, while those with college or above degrees had the lowest. The patients with college or above degrees had the highest PrepDM scores and those with elementary school degrees or below had the lowest scores (Figure 3). We proposed there are two possible factors that could explain these results: background knowledge, and understanding of the cPDA. The patients with college or above degrees might have made their own research on related issues before visiting our clinics and had more background knowledge, and therefore higher pre-cPDA DSE scores. With the help of cPDA, they had their doubts resolved and became the most prepared to make a decision. The patients with junior or senior high degrees might have limited background knowledge before the visit; however, they have a good understanding of the cPDA, and increased their confidence in decision-making after the cPDA. The patients with elementary school degrees or below might have both limited background knowledge before their visit and a limited understanding of the cPDA; they gained scores on DSE after the cPDA, and were the least prepared group among the participants.
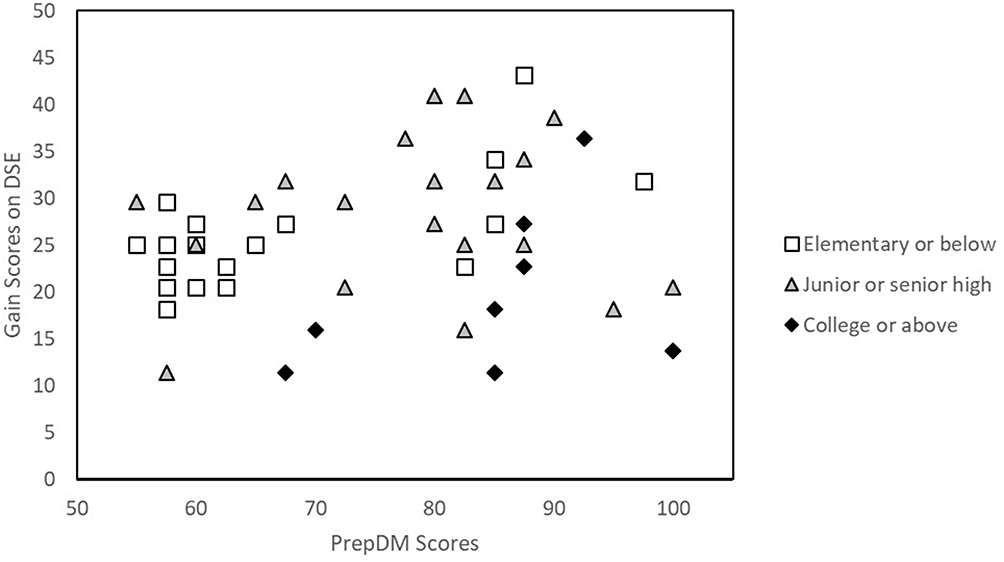 |
Figure 3 Plot of gain scores on DSE and PrepDM scores. The patients with junior or senior high degrees had the highest gain score on DSE, while those with college or above degrees had the lowest. The patients with college or above degrees had the highest PrepDM scores and those with elementary school degrees or below had the lowest. Abbreviations: DSE, decision self-efficacy; PrepDM, preparation for decision-making. |
Computer-based decision aids were reported to be associated with improvements in knowledge and decisional conflicts. Syrowatka et al4 published a systematic review on the features of computer-based decision aids from 58 studies. In their study, content control improved quality of decision-making, while tailoring reduced the quality of decision-making. The concept of content control allows patients with different health literacies to decide the amount of information presented, promotes autonomy, and empower patients to take ownership over health decisions.16 On the other hand, the concept of tailoring frames evidence according to patient demographics and clinical conditions, to present only viable treatment options with more accurate risk estimates. On the contrary to content control, tailoring utilizes a paternalistic model of presenting evidence and may reduce autonomy.17 The other two features of computer-based decision aids, which are explicit values clarification and feedback, also have positive effects on quality of decision-making. Explicit values clarification guides patients through specific steps to identify personal values and preferences.18 Computer-based decision aids which provide feedback to patients could further clarify explicit values. A summary of preferences gives feedback on how patients personally value risks, benefits, and optimal choice, and suggests which option is best based on the patients’ values and preferences.19
In our study, the cPDA on robot Zenbo has several of the above-mentioned features. The on-screen display and voice communication of the robot Zenbo make the cPDA capable of having dialogues with users. The cPDA was interactive, therefore the participants could order the robot to repeat certain steps if they did not fully understand the information provided (content control). The cPDA followed an algorithm designed to help the patients assess their needs in detailed tasks, during sports, driving at night, desire to be glasses-free, and financial concerns (explicit value clarification). At the end of the decision aids, the cPDA provided a summary of preferences and a recommendation on IOL selection (feedback). These features were reported to have positive effects on the improvement of the quality of decision-making.4
Our results show that the education level of patients may influence their self-efficacy and preparedness for decision-making. Although a lower education level has been reported to be associated with lower scores of involvements in shared decision-making,20 education level alone cannot reflect the patient’s capacity to obtain, process, and understand basic health information and services, ie, health literacy. Routinely screening patients for health literacy has not been shown to improve outcomes and is not recommended. Universal health literacy precaution was recommended to provide understandable and accessible information to all patients, regardless of their literacy or education levels.21 Such precautions should be taken into account to further improve cPDA design.
The cPDA used in the present study had the advantages of an initial interactive education stage, the ability to provide specific questionnaires depending on the patient’s choice of preference, and to provide a summary of preferences and a recommendation of IOL selection at the end of the decision aid. The preliminary results showed the cPDA might help the self-efficacy of the patients in decision-making. There are still disadvantages of the present cPDA. Only one language was available. The limited items in choices for preference did not allow patients to fully express their values and preferences. The status of health literacy of patients was not evaluated before the decision aids.
The interpretation of the analysis results must consider the limitations of this study. Due to the lack of a control group, it was not clear how much the gain was actually due to the cPDA. The sample size was small and limited to one institution. Factors that might affect the patient’s proficiency in using the cPDA, such as visual acuity, preferred language, cognitive ability, the presence of a doctor during the process, and other possible confounding factors were not studied. Whether the results could be replicated warrants further investigation. These limitations provide an indication for fields of further research.
Cataract is a disease of aging populations. Studies have shown that older patients tend to seek less information to make decisions and make decisions faster than younger individuals. Older patients have preferences for fewer choice options, face greater difficulties in understanding information about available options, and tend to disproportionally focus on emotional aspects when making decisions. Older patients tend to have variable preferences depending on their frailty, level of education, or cognitive and health status. Moreover, some, usually older and less educated, prefer to delegate decisions to their clinician.22 Most patients never knew about the complex knowledge of optics in the selection of IOL. A computer-based decision aid might help patients to assess their visual needs, clarify their values and preferences, and approach an optimal choice. However, it is the clinician’s responsibility to accompany the patients through the whole process of decision-making, to maximize post-operative satisfaction in cataract surgeries.
Conclusions
An interactive cPDA may be a promising tool for complex decisions such as IOL selection before cataract surgeries. The preliminary results showed that education levels may be associated with the usefulness of cPDA on the preparedness and decision efficacy of the patients, although many confounding factors, including language preference, cognitive ability, and health literacy, need to be studied to support the clinical application of cPDA. This pilot study may provide a proof-of-concept of the feasibility of cPDA for patients who are making decisions of IOL selection before their cataract surgery.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of Ditmanson Medical Foundation Chiayi Christian Hospital (Permit No. 2020102) and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from each participant in the study.
Funding
This study was not funded.
Disclosure
The authors declare no conflicts of interest regarding the publication of this paper.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
2. Joseph-Williams N, Newcombe R, Politi M, et al. Toward minimum standards for certifying patient decision aids: a modified delphi consensus process. Med Decis Making. 2014;34(6):699–710. doi:10.1177/0272989X13501721
3. Stacey D, Legare F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431. doi:10.1002/14651858.CD001431.pub5
4. Syrowatka A, Kromker D, Meguerditchian AN, Tamblyn R. Features of computer-based decision aids: systematic review, thematic synthesis, and meta-analyses. J Med Internet Res. 2016;18(1):e20. doi:10.2196/jmir.4982
5. Alio JL, Kaymak H, Breyer D, Cochener B, Plaza-Puche AB. Quality of life related variables measured for three multifocal diffractive intraocular lenses: a prospective randomised clinical trial. Clin Exp Ophthalmol. 2018;46(4):380–388. doi:10.1111/ceo.13084
6. Kaymak H, Breyer D, Alio JL, Cochener B. Visual performance with bifocal and trifocal diffractive intraocular lenses: a prospective three-armed randomized multicenter clinical trial. J Refract Surg. 2017;33(10):655–662. doi:10.3928/1081597X-20170504-04
7. Pepose JS, Qazi MA, Chu R, Stahl J. A prospective randomized clinical evaluation of 3 presbyopia-correcting intraocular lenses after cataract extraction. Am J Ophthalmol. 2014;158(3):436–446. doi:10.1016/j.ajo.2014.06.003
8. Shah S, Peris-Martinez C, Reinhard T, Vinciguerra P. Visual outcomes after cataract surgery: multifocal versus monofocal intraocular lenses. J Refract Surg. 2015;31(10):658–666. doi:10.3928/1081597X-20150611-01
9. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–440. doi:10.3928/1081597X-20190618-01
10. Jacobi PC, Dietlein TS, Luke C, Jacobi FK. Multifocal intraocular lens implantation in prepresbyopic patients with unilateral cataract. Ophthalmology. 2002;109(4):680–686. doi:10.1016/S0161-6420(01)01029-6
11. Elwyn G, O’Connor A, Stacey D, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ. 2006;333(7565):417. doi:10.1136/bmj.38926.629329.AE
12. Volk RJ, Llewellyn-Thomas H, Stacey D, Elwyn G. Ten years of the International Patient Decision Aid Standards Collaboration: evolution of the core dimensions for assessing the quality of patient decision aids. BMC Med Inform Decis Mak. 2013;13(Suppl 2):S1.
13. Bunn H, O’Connor A. Validation of client decision-making instruments in the context of psychiatry. Can J Nurs Res. 1996;28(3):13–27.
14. Cranney A, O’Connor AM, Jacobsen MJ, et al. Development and pilot testing of a decision aid for postmenopausal women with osteoporosis. Patient Educ Couns. 2002;47(3):245–255. doi:10.1016/S0738-3991(01)00218-X
15. Bennett C, Graham ID, Kristjansson E, Kearing SA, Clay KF, O’Connor AM. Validation of a preparation for decision making scale. Patient Educ Couns. 2010;78(1):130–133. doi:10.1016/j.pec.2009.05.012
16. Matsuyama RK, Kuhn LA, Molisani A, Wilson-Genderson MC. Cancer patients’ information needs the first nine months after diagnosis. Patient Educ Couns. 2013;90(1):96–102. doi:10.1016/j.pec.2012.09.009
17. Scherer LD, Ubel PA, McClure J, et al. Belief in numbers: when and why women disbelieve tailored breast cancer risk statistics. Patient Educ Couns. 2013;92(2):253–259. doi:10.1016/j.pec.2013.03.016
18. Fagerlin A, Pignone M, Abhyankar P, et al. Clarifying values: an updated review. BMC Med Inform Decis Mak. 2013;13(Suppl 2):S8. doi:10.1186/1472-6947-13-S2-S8
19. Witteman HO, Gavaruzzi T, Scherer LD, et al. Effects of design features of explicit values clarification methods: a systematic review. Med Decis Making. 2016;36(6):760–776. doi:10.1177/0272989X16634085
20. Brodney S, Fowler FJ, Stringfellow V, Valentine KD, Barry MJ. National survey of decision-making for antidepressants and educational level. J Am Board Fam Med. 2020;33(1):80–90. doi:10.3122/jabfm.2020.01.190120
21. Hersh L, Salzman B, Snyderman D. Health literacy in primary care practice. Am Fam Physician. 2015;92(2):118–124.
22. van Weert JC, van Munster BC, Sanders R, Spijker R, Hooft L, Jansen J. Decision aids to help older people make health decisions: a systematic review and meta-analysis. BMC Med Inform Decis Mak. 2016;16:45. doi:10.1186/s12911-016-0281-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.