Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Developing a National Integrated Road Traffic Injury Registry System: A Conceptual Model for a Multidisciplinary Setting
Authors Sadeghi-Bazargani H, Sadeghpour A, Lowery Wilson M, Ala A, Rahmani F
Received 16 May 2020
Accepted for publication 24 August 2020
Published 23 September 2020 Volume 2020:13 Pages 983—996
DOI https://doi.org/10.2147/JMDH.S262555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Homayoun Sadeghi-Bazargani,1,2 Alireza Sadeghpour,1 Michael Lowery Wilson,3,4 Alireza Ala,5 Farzad Rahmani5
1Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 2International Safe Community Certifying Center, Stockholm, Sweden; 3University of Turku, Turku, Finland; 4Heidelberg Institute of Global Health (HIGH), University of Heidelberg, Heidelberg, Germany; 5Emergency Medicine Department, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Homayoun Sadeghi-Bazargani
Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Janbeh Borjeh Sharan, Golshar, Tabriz, Iran
Tel +98 9144027218
Email [email protected]
Alireza Sadeghpour
Shohada Hospital, Tabriz University of Medical Sciences, Golshar, Tabriz, Iran
Tel +98 9143119318
Email [email protected]
Introduction: Despite a high burden of traffic injuries, effective integrated or linked injury surveillance systems are rarely available in many low- and middle-income countries (LMICs). The aim of the current study was to define a conceptual model for developing a national integrated traffic injury registry in Iran.
Methods: A mult-method study financially and technically supported by the World Health Organization, Iranian Ministry of Health, Iranian Traffic Police, and the Iranian Legal Medicine Organization was conducted. A theoretical framework, forming the core conceptual components, was developed based on expert reviews. The preliminary conceptual model was developed by a panel of experts and tailored through a national workshop of 50 scientists, authorities and experts from nearly all sectors related to road safety promotion and injury management. It was then sent out to external reviewers in order to assess and improve the content validity of the model.
Results: The conceptual model was developed to have six components. These included 1) aims and core definitions; 2) content and core measurements; 3) data flow; 4) data collection routines; 5) organizational matrix; 6) implementation organization. The Haddon’s matrix was adapted to be used as the theoretical framework in defining the content and data flow components of IRTIR. Five subcomponents were defined in the content and core measurements component with each having several subcategories. Each subcomponent/subcategory was finally divided into several item groups to guide defining the final data measurement variables. The data flow component was defined with six data sequence stations. Through the organizational matrix component, five major organizations relevant to road traffic safety were defined as core data production contributors. Some organizations also owned several sub-organizations which contributed in this regard.
Conclusion: It is concluded that the IRTIR conceptual model includes the required six components for developing a national integrated registry for Iran. Its main component called, content and core measurements, leads the researchers in developing final data collection tools in developing the national registry of road traffic injuries in Iran.
Keywords: management information systems, injury surveillance, accident information systems, crash registry, road traffic injuries
Background
About 1.3 million people globally lose their lives as a result of road traffic crashes and 90% of these deaths occur in Low- and Middle-Income Countries (LMICs).1 The Eastern Mediterranean Region constitutes approximately 9.2% of the world’s traffic deaths, and is the only region where High-Income Countries (HICs) have a higher road traffic death rate than LMICs. The World Health Organization (WHO) estimated a rate of 20.5 deaths per 100 000 people in Iran which makes traffic crashes as Iran’s 5th leading cause of death and largest cause of years of life lost (YLL).1 The proportion of YLL due to Road Traffic Injuries (RTIs) in Iran is higher than in most other parts of the Eastern Mediterranean region and elsewhere in the world, and is one of the country’s most serious problems resulting in a loss of around 6–7% of GDP.1–3
Despite the magnitude of the problem, RTIs are preventable with involvement from multiple national sectors such as transport, police, health, education, and actions that address the safety of roads, vehicles, and road users within the country.4 Moreover, a lead agency that coordinates and monitors related organizations and road safety preventive activities are critical.5 A registry system can document the epidemiology, processes and outcomes of trauma injuries in an integrated context among related organizations and data sources.6 The diversity of data collection practices and regulations across jurisdictions hinder the development of valid, detailed and reliable databases for road safety.7 Given the significance of stringent quantitative reasoning in supporting road safety policies at national, regional or global levels, data quality, reliability, and stability are of the upmost importance.8 According to WHO recommendations for developing countries, particularly for the Eastern Mediterranean region countries. There exists a need to direct more attention to standardizing the programs of traffic crash registries, including the use of appropriate methods, clear definitions of variables and producing practical data to study the causes of traffic crashes.9,10
Based on expert ideas from Iranian road safety system in a recent study, among the most important challenges towards establishing a RTI surveillance system in Iran are the lack of a systemic approach to surveillance, absence of a lead agency, failure in stakeholder recognition, unclear objectives, failure in developing a shared plan between stakeholders and lack of ` data dissemination and giving feedback.11 While in Iran, eight different organizations such as police, Ministry of Health and Medical Education (MOHME) including national organization for emergency medical services (EMS) and hospitals, legal Medicine Organization, fire departments and Red Crescent organization collect data on RTIs;12,13 but there are some problems and gaps in integration, coverage and data collection tools resulting in inaccurate and non-comprehensive data on RTIs. For instance, most of collected RTI measurements in Iran are duplicated in each system. On the other hand, some variables driving under influence of drug and alcohol, child restraints and helmet use in relation to RTI prevention are missed in all systems.13 Although an integrated trauma registry system focused on RTIs is an urgent need for Iran as stated by the government as well as the parliament of Iran, this gap has not been fulfilled by now. The solution needed in this regard is to present a pragmatic model for addressing the challenges in developing an effective RTI surveillance system. In this paper, the aim was to develop a conceptual model for a national Integrated Road Traffic Injury Registry (IRTIR), as the first and basic step towards the practical development of an IRTIR in Iran.
A literature review of the national and international experiences regarding traffic data systems was performed with consideration given to the complexity of developing an integrated road traffic injury registry. With respect to this complexity, in order to achieve a comprehensive way which supports all the related organizations, both data producers and data users, with a clear map on their connections, capacities and needs, a conceptual model was considered to be the first step to behave like a road map for developing a sustainable registry system.14,15 This was the first step in developing the IRTIR with the eventual goal of arriving at a conceptual model. Based on the conceptual model, a national registry can be developed, piloted, scaled up to a national level, evaluated, revised or extended if needed. As part of the national research project, the aim of current study was to develop the conceptual model for the Iranian Integrated Road Traffic Injury Registry (IRTIR).
Methods
A multi-method study financially and technically supported by the World Health Organization, Iranian Ministry of Health, Iranian Traffic Police, and the Iranian legal Medicine Organization was conducted. IRTIR development is a national 4-year research project (2017–2020) aiming to develop the Iranian Integrated Traffic Injury Registry. The MOHME and Road Traffic Injury Research Center of Tabriz University of Medical Sciences in collaboration with other stakeholders were determined to develop and pilot the IRTIR, planned to establish a functional integrated data registry system. The developed project will be piloted in the northwest of Iran and later the model will be scaled up throughout the country. This scaled-up model can later be expanded to a national integrated trauma registry.
Preliminary Conceptualization
Preliminary conceptualization was done to define the core features of developing IRTIR, as well as the main components of the conceptual model. The preliminary conceptualization was done through a situation analysis using a review of available literature and an expert panel work.
In order to identify, what is currently measured about road traffic injuries in Iran as well as to identify the main domains of crash risk factors and outcomes, a review of the literature was done to explore national and international experiences of traffic data collection systems in the field of road safety. The aim of this was not to conduct a systematic review for detailing the global knowledge on injury surveillance and instead we aimed to identify some international available registries and study their features for practical use. However, we tried to follow the basic standards of conducting literature reviews. For this mean, through our preliminary review, we searched several sources including PubMed, Web of Science, Science Direct, SCOPUS, EMBASE, Google scholar, and SafetyLit. With respect to our purpose on developing the Iranian road traffic injury registry, we also searched some Iranian databases including Scientific Information Database (SID), Safety Literature of Iran (SafeLir), IranMedex and Magiran. At the same time, some official websites were also searched for grey literature including OpenGrey.eu, WHO.int and Google.com, as well as official websites of the Iranian Commission on Road Safety, Iranian Transportation Organization, and Iranian Traffic Police websites. Using key terms of [“crash(s)” OR “accident(s)” OR “collision(s)” OR “road traffic injury” OR “Road traffic accidents” OR “road safety” OR “trauma*” OR “injury(ies)”] AND [“surveillance” OR “data” OR “registry” OR “database” OR “variable(s)”] searches were done within search engines. Finally, 14 sets of international data collection tools belonging to Australia, China, UK, Europe, Ireland, Sweden, UAE, and USA were retrieved. Other than the literature review to identify some experiences on road traffic injury surveillance systems, the researchers visited the implemented data-systems of stakeholder organizations such as MOH, Police and Forensic Medicine Organization to identify what data is currently collected over the various domains of traffic accidents in Iran, details of which is now published showing that 15 data systems directly related to road safety existed in Iran.13 Moreover, the available national legislations/regulations in the field were inspected and the general aim was based on the available legislation/regulations of the Iranian Government Board16 to develop an integrated traffic injury registry.
The core research panel of experts was formed being responsible to develop the preliminary conceptual model. The panel included an injury epidemiologist (HSB), emergency care specialists and traumatologists (FR, KS AA, AS, AN and AM), a traffic police expert (MA), a crash investigation specialist (MS), a road infrastructure expert (H), a forensic medicine specialist (BSR), a social medicine specialist (MH) as well as an injury prevention and safety promotion specialist (DKZ).
The expert panel started with a brief explanation of the aims and summary presentation of conducted review. The principal investigator (HSB) played as the facilitator of the team who called for consensus on the discussion topics including determination of the core features and components of IRTIR. The panel members provided their comments on what components should be considered in a conceptual model and what should be considered as the core features of registry. The members contributed their ideas through brainstorming and the facilitator tried to summarize and make proposals for discussion and reaching consensus. The group members were guided that in cases of making decisions, everyone should actively state whether they consent, object, or stand aside often by hand gesture. In cases where consensus could not be reached this way, the nominal group technique was used. Four sessions of around 90-minute discussions were held until the preliminary conceptual model and core features of IRTIR were determined. The core features of IRTIR reached by the panel included; efficient coverage, flexibility, multi-sectoral linkage and integration capabilities, geographical information system outputs, unique IDs at several levels, validated tools, international registry standards, local needs, approved ethical protocols, implementation phasing, data usage protocol, data quality assurance, database security and encryption. The consensus reached by the research team experts developed the preliminary conceptual model to have three components including aims component, data component, and organizational matrix.
This was sent out to several external reviewers from various disciplines such as health sector experts, database experts, police experts and forensic medicine experts to give their comments on model relevance and adequacy.
Final Conceptualization Through Extended and External Expert Reviews
An extended panel of 50 road safety experts/authorities including experts from the Traffic Police of Iran, MOHME, Ministry of Roads and Urban Development, Legal Medicine Organization, the Judiciary Organization, Ministry of Industry, Mine and Trade (MIMT), as well as academic experts from several universities and the World Health Organization office of Iran was formed (Table 1).
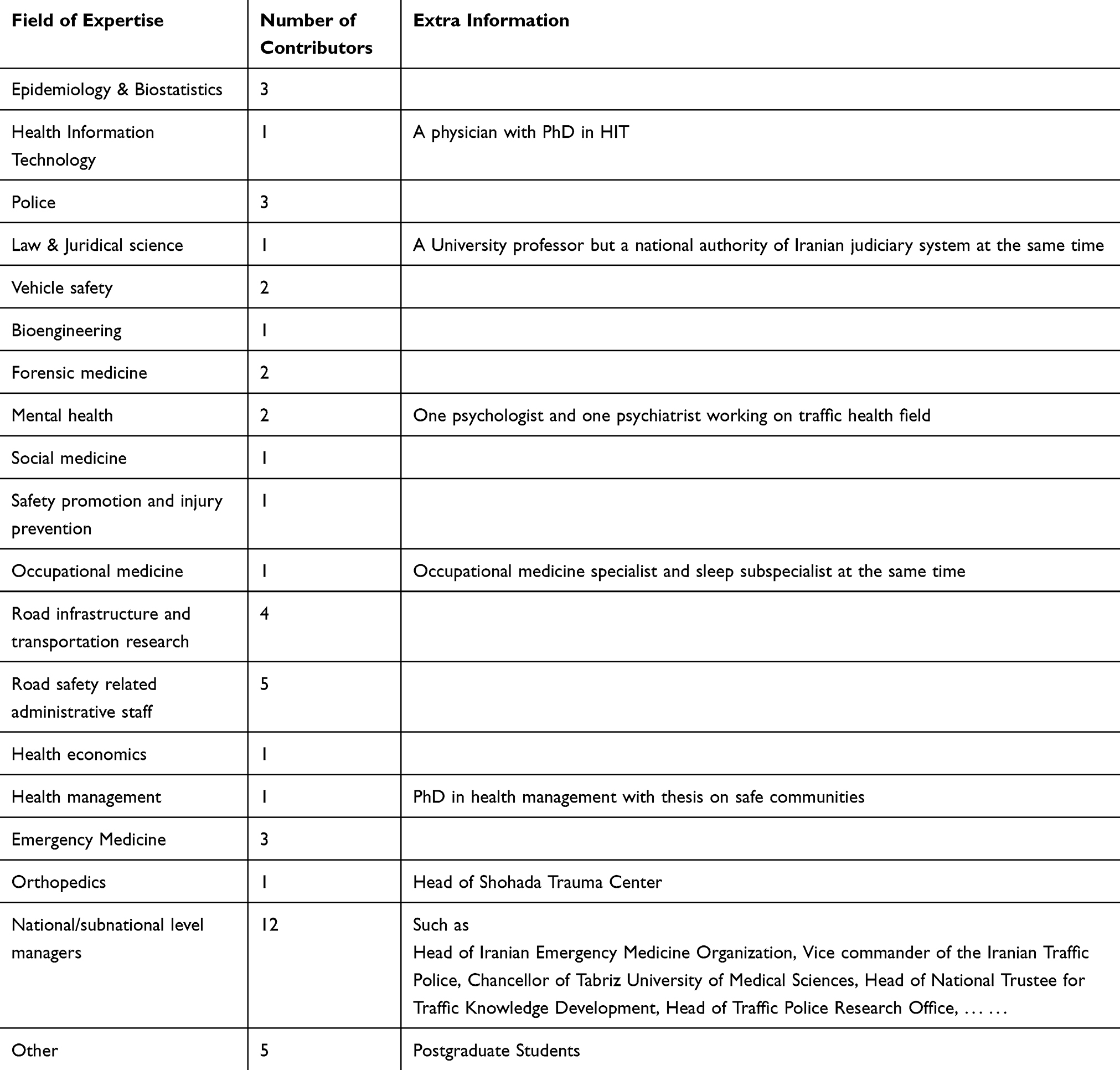 |
Table 1 Description of the Experts Contributing Development of the Conceptual Model for IRTIR |
After being briefed by the principal investigator (HSB) on project aims and demands, they were provided with a draft of the preliminary model and summary of relevant literature. They then continued discussions in the separate workgroups under infrastructure, vehicle, and human headings. Then they re-gathered and presented their comments and ideas in a summoned session. The improved conceptual model was developed through a nominal group technique to integrate and finalize the ideas summarized in each technical group. Updates of the model were developed and improved through review rounds among external reviewers in −0.
This conceptual model will be used to develop, implement and update the national road traffic injury registry system.
Ethical Approval
This project has been approved by the MOHME, Iranian Trustee for Traffic Knowledge Development and Road Traffic Injury Research Center under number 700/1482. The funding from MHOME came under contract number 700/D/581 signed by Secretary for Research and Technology. It has received ethical approval under number IR.TBZMED.REC.1396.465 from the Ethical Committee in Tabriz University of Medical Sciences; IRTIR is also supported by WHO under contract number 2017/742294-0 and the related concept note.
Patient and Public Involvement
No patient involved.
Results
As presented in Figure 1, the conceptual model for developing IRTIR was defined to have six components.
 |
Figure 1 The six components of the conceptual model for IRTIR. |
Component 1: Aims and Core Definitions
Aims
The general aim of IRTIR was determined as “to register road traffic crashes leading to injuries or fatalities in Iran”. The registration was decided to be more focused on variables needed for injury and fatality prevention, however, data beneficial for improving the quality of medical care or traffic scene management was also considered at a second level of importance.
IRTIR was not intended by itself to be used exclusively for research purposes but the rich data content of IRTIR could be a valuable source for initiating applied research. IRTIR was intended to register at least 95% of all severe road traffic injuries in Iran after full national implementation. It has been shown that under-reporting in road safety data decreases with the increase in accident severity and vice versa.17
Core Definitions
Data collection can occur at different stations or by different organizations, but it should follow definitions and standards that will be provided in IRTIR protocol. Data collections outside these definitions and standards by organizations involved in IRTIR will not be prevented unless they adversely affect IRTIR data collection procedures and standards. Any such data collection was not considered to be included in IRTIR or considered as associated with IRTIR neither as core measurements or complementary data. The core definitions of IRTIR are described below:
Road Traffic Crash: The following definition to include injury accidents was adopted from the glossary developed by the United Nations Economic Commission for Europe (UNECE) and the Organization for Economic Co-operation and Development (OECD) to be used for collection of data on transport in European Union country members. Any accident involving at least one road vehicle in motion on a public road or private road to which the public has right of access, resulting in at least one injured or killed person.
These accidents, therefore, include collisions between vehicles, between vehicles and pedestrians and between vehicles and animals or fixed obstacles, and with one road vehicle alone.18,19 This definition although different from the current official reference for national statistics is inclusive of all crashes based on the current definition. Using such a definition which is wider than the national definition allows for flexibility in potential future variations in national definitions as well as the capability for comparing Iranian traffic injury statistics with international statistics, especially European statistics.
Road Traffic Injury: “Fatal or non-fatal injuries incurred as a result of a road traffic crash”.20
Traffic Injury Fatality: A death occurring within 30 days of the road traffic crash.21,22 Although this definition was decided by Iranian Road Safety Commission, IRTIR will deposit data on traffic fatalities even beyond the given time period to ensure flexibility for future changes in definitions.
Serious Traffic Injuries: Fractures, concussions, internal lesions, crushing, severe cuts and laceration, severe general shock requiring medical treatment and any other serious lesions entailing hospitalization. For practical reasons any traffic injuries leading to hospitalization for a period of more than 24 hours is also considered as serious injury.18,19
Component 2: Content and Core Measurements
Various required fields of information were identified and defined in this component to be included in IRTIR. These core measurements (categories/subcategories) will later be used to define minimal dataset variables and a data dictionary.
As presented in Table 2, the main categories in this component were defined based on Haddon Matrix which is a well-known tool in road safety promotion and injury prevention. However, some differences from Haddon’s Matrix can be easily identified in it, as below:
- The Identification Characteristics: This part is specifically for general characteristics of a crash and the main related parts including human, vehicle, road and involved organizations that can together make a crash identification key for a database as well as identifying and linking various elements of registry.
- Miscellaneous section: This section refers to the items which cannot be exclusively classified as human or vehicle or environment factors or classified in a pre-crash, crash and post-crash phases of Haddon’s Matrix.
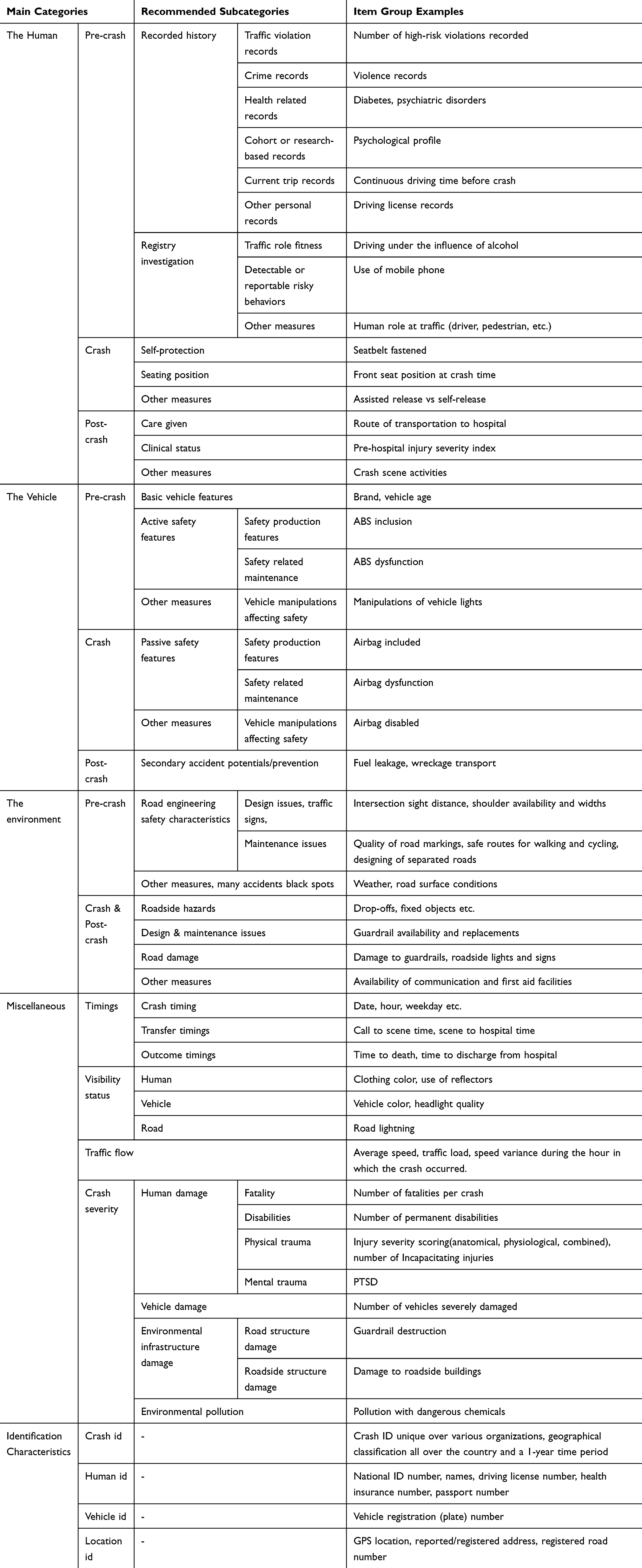 |
Table 2 The 2nd Component of the Iranian Integrated Road Traffic Injury Registry (IRTIR) Conceptual Model: Content and Core Measurements |
Component 3: Data Flow
Apart from the identification of what IRTIR is going to measure and collect, the conceptual model needed a component to define the flow of data over time in order to depict data stations and involved organizations from pre-crash to potential fatality. IRTIR will consider the collection of information starting from a crash station in two directions. First, this happens in the reverse direction extracting pre-crash data such as traffic violation records, and previous health records of the victims or those involved in a traffic crash and also the traffic flow recorded for a short period of time before the crash. The latter is easily retrievable from the traffic flow database of the Ministry of Roads & Urban Development (MRUD) extracted from installed traffic cameras. Secondly and most importantly, the forward data collection will be done forming the main data flow pathway. A wide range of data could be collected at various stations such as crash scene, ambulance transfer, outpatient and inpatient care, post-discharge follow-up and forensic examinations (Figure 2).
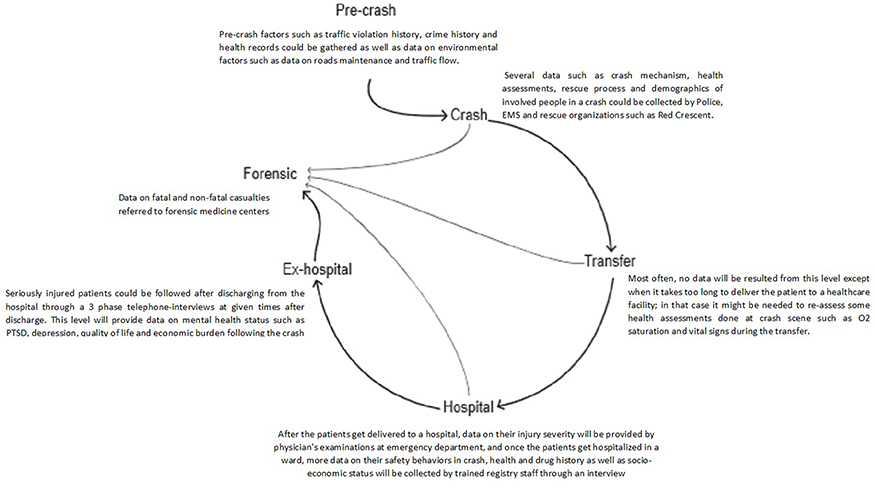 |
Figure 2 Data flow diagram of the Integrated Road Traffic Injury Registry. |
Component 4: Data Collection Routines
Data Collection Tools
All the data collection tools should either be pre-validated available tools or tools specifically developed, adapted and validated for this registry.
Data Collection and Deposition Types
Data can be collected or deposited in various forms as follows:
- Some data are collected using interviews and by completing paper questionnaires (such as nurse station data collection).
- Some data are collected and deposited using online forms and internet applications directly by the registrars (such as EMS data collection).
- Some data are extracted from currently available databases and added to the registry (Such as ICD10 data from a hospital information system).
- Some data are collected and directly deposited through automatic processes (such as data from traffic cameras)
- Other data types including GPS coordinates and crash scene photos.
Data Collection Extent and Volume
Although a minimum data registry will be implemented country-wide, it is neither cost-effective nor practical in a LMICs setting to collect a wide range of detailed data. A minimum dataset has to be defined for full coverage data collection. Some sentinel centers will also be allocated to collect a wider range of specialty data. At least one sentinel center has to be considered in each province.
Extended professional data collection is also considered with respect to crash characteristics through purposive sampling (such as expert crash analysis investigations at high-burden crashes).
Registrars
Various persons are involved in different stations of the IRTIR such as policemen, EMS staff, nurses, etc.
Component 5: Organizational Matrix
As far as the road safety complex is a multi-sectoral problem within the country, and there are several RTI-related organizations which are data producers and/or data users; so an integrated registry should include different organizations considering the laws, capabilities, limitations, and interests of several organizations.
The fifth component is then considered in the conceptual model to focus on detecting RTI-related organizations and clarifying their roles within the IRTIR. According to the preliminary expert panel discussions, five major organizations were identified to have the capability or the necessity in contributing to implementing the IRTIR. However, several other organizations could also have a role (Figure 3).
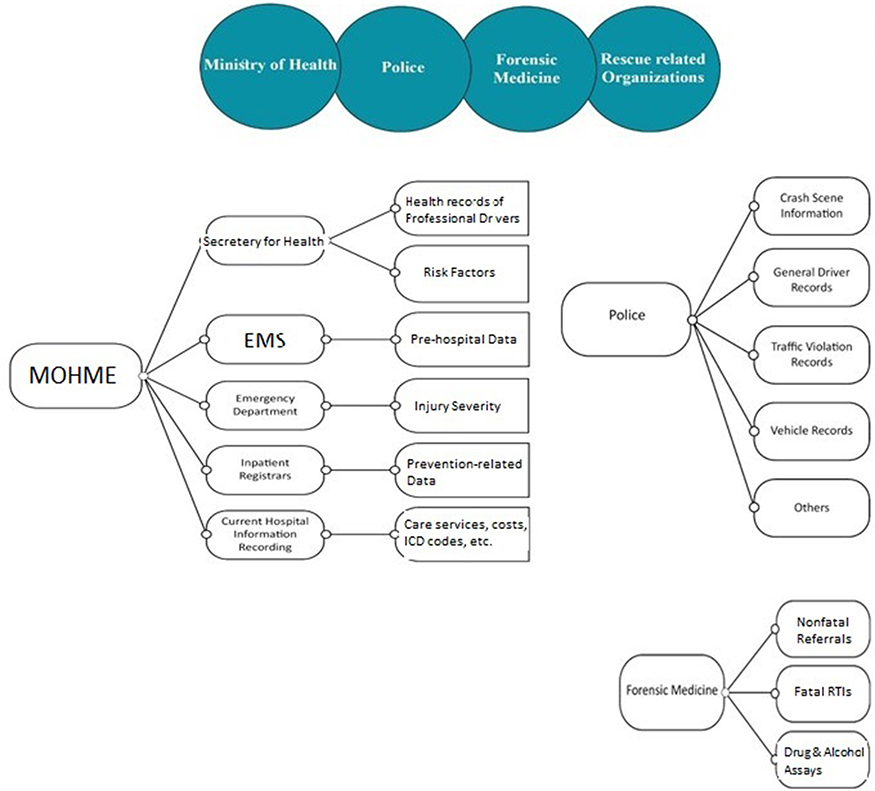 |
Figure 3 Various data produced by the three main traffic-related data production organizations in Iran. |
These major organizations include the Ministry of Health (MOHME), police, Legal Medicine Organization (LMO), the Ministry of Roads & Urban Development (MRUD) and rescue-related organizations (Red Crescent Organization and Fire Brigade Department). Nevertheless, the most important and bulk of data are produced by MOHME, traffic police and FMO (Figure 3). Other organizations having the potential to contribute include; Insurance companies, vehicle industries, municipalities, the National Environment Organization and the Meteorological Organization.
Component 6: IRTIR Implementation Organization
The last component of the conceptual model of IRTIR defines the implementation organization which is an important requirement for running a sustainable and reliable registry. Such an organization in the IRTIR is comprised of a national steering board and several executive committees.
National IRTIR Steering Board
A national steering board is necessary to form at the national level for policymaking, leading, and coordinating the organizations involved. The major organizations with legislated duties should have a representative(s) at the national level. These include Traffic Police, the MOHME, the Ministry of Roads & Urban Development (MRUD), Legal Medicine Organization, Judiciary Organization and rescue-related organizations such as the Red Crescent Organization and fire brigade departments.
The national EMS organization will represent as the leading body on behalf of the MOHME, and the National Road Safety Commission will represent as the leading body on behalf of the MRUD. The Road Traffic Injury Research Center (Iranian Traffic Knowledge Development Trustee) will act as the scientific body authority of the steering board; however, independent traffic health and safety scientists could also be included either as members or non-member observer/consultants. The membership or observer roles could also be considered for other related organizations if needed.
Executive Committees
Several executive committees task forces will support implementation and running of the IRTIR. These include information technology committee (technical committee), information usage regulation committee, evaluation and quality control committee, and the provincial administrative committees.
Discussion
To develop a national/regional sustainable trauma registry in LMICs is considered an urgent public health priority.23 Several potential users may be attributed to trauma registries. These include injury surveillance, aiding in clinical investigations and the assessment of outcomes.24 Good examples of trauma registries have been recently presented not only from western countries, but also from eastern countries such as a recent one from Saudi Arabia.25 These registries can provide vital information that may be helpful in designing injury prevention strategies, the process of allocating resources and backing policy-making efforts. This helps, as shown; to reduce the number of fatalities occurring due to traumatic incidents.26 It has been confirmed that by establishing trauma registries, a number of developments have occurred in health care systems and the process of policy-making in the health systems of developing countries.27 One of the essential pre-requisites to establishing a trauma center is to use an integrated and simultaneous trauma registry as a standard information collection system to enhance system performance. An advantage of a trauma registry is that it can act as a repository for special data that can be appraised and based on evidence.23
The capacity of a trauma registry to inform improvements in the quality of trauma care depends upon the quality of its data. Incomplete and erroneous data are a threat to the use of trauma registries;12,13 since the trauma term can refer to a wide range of injuries, sampling of a nonhomogeneous trauma population limits the generalizability and validity of its results.12 A review study showed that the definition and classification of trauma registry data quality is ambiguous.15 Moreover, most trauma registries do not have the infrastructure to track and document complications as they emerge, so the absence of important components of trauma care, such as pre-hospital deaths and complication rates, as well as the failure to incorporate measures of long‐term survival and functional outcomes among those who survive limits the utility of trauma registries in assessing the effectiveness of care and testing new therapeutic measures.14–16 Such limitations of a general trauma registry encouraged us to plan for developing a quality registry for RTIs which has also been the case in several other countries like England, the United States and Sweden.17
Most quality registries are disease-specific and target functional outcomes. Quality registries could provide benefits, such as a standard approach, which could provide better opportunities for collaboration across organizational boundaries, for example between different wards at the same hospital or between different healthcare providers such as hospitals, primary health care and nursing homes.18 Also, they have an audit spiral, in which outcome data are fed back into the programs in order to improve their process characteristics.19
Using only fatalities as an indicator of crash outcome could be beneficial, but hints at just the tip of the iceberg of RTIs. Crashes cause numerous serious RTIs, resulting in considerable economic and human harm. In addition, in several countries, the number of serious traffic injuries has not been decreasing as fast as the number of fatalities over the past years.
IRTIR has been developed as a project with flexibility in cost-effectiveness, so it has been considered as a quality registry for specific registration of fatalities and serious injuries caused by crashes. Fatalities are somehow easy to be categorized in the registry and there are difficulties in developing and using reliable injury severity scales for inclusion of serious RTIs. However, considering the importance of nonfatal injuries and at the same time the predictive value of injury severity scales for hospital mortality, we were convinced to include a valid scale for registering injury severity. Injury severity should include different dimensions such as a threat to life, disability, quality of life, injury burden, and cost. IRTIR uses the crash severity as the inclusion criteria for its data and is expected to reach a coverage of RTIs above 90% within the country. For most LMICs including Iran, it is not possible or reasonable to fully register all traffic accidents. So IRTIR as an approach for LMICs includes only the serious injuries for wide integrated data collection. As part of crash severity, for assessing the human sufferer, there will be a need for using trauma/injury severity scales. However, considering the feasibility and costs, it should be taken into account to have at least two choices of easy-to-measure scales at pre-hospital and general hospital levels and detailed scales to be used at reference trauma centers following the sentinel approach.
Instead of straightly proceeding to develop the registry protocol and minimum dataset, we preferred to develop a conceptual model beforehand. RTIs are a complex issue, so achieving a comprehensive way which includes all related organizations both data producers and data users with a clear map on their connections, capacities and needs, a conceptual model is a must. It makes a general view of the project and leads the steps to be taken in an effective way. The conceptual model behaves like a road map both at the start and long-term sustainability of IRTIR. Having a conceptual model helps to plan a step-by-step development or expansion of IRTIR even in a long run without losing the focus or losing connections and consequently disgracing previously collected data due to sequestered changes and replacements of data collection systems over time.
Integration in IRTIR
Data on road traffic fatalities are essential for monitoring country-level trends, tailoring prevention efforts, assessing progress and comparing the scale of road traffic deaths relative to deaths from other causes.10 Vital registration data fulfill these needs best as they are a record of all officially registered deaths and are not time-limited.1 Reported fatality data cannot be reliable when they reported by only one traffic-related organization; for example, there is a lack of coverage of police at the scene or people dying at hospital not followed by police.20 It is evident that linking data sources (ie, vital registration records, police data, insurance data, etc.) can improve official road traffic fatality estimates, but this process is not widely adopted.1 Surveillance of RTIs needs to follow a multi-sector structure within a country. For instance, data reported by police usually is very detailed in circumstances of the crash, such as date and place, mode of transport, and wide information on road, vehicle and human behavior. Considering the complexity of data and required skill, it is not likely for a police officer to the severity of injuries in a reliable way. On the other hand, hospital records of people attended due to RTIs usually include very little information on circumstances of the crash but it does contain data about the medical diagnosis, mechanism or external cause of injury, and interventions that can be used to depict the severity of injuries.20 The IRTIR conceptual model defines a proper context to link all RTI-related organizations aiming to capture the most accurate and comprehensive data from each organization and create a coordinated understanding of what is in data. The IRTIR will follow the fatalities caused by crashes from crash scene till hospital and/or forensic medicine investigations. So it has been predicted that fatality data resulting from the IRTIR will be the most accurate in country. The three positive notes behind developing the IRTIR could be cited as; existing national legislations to develop the IRTIR; developing it through a scientific method being executed by the national traffic knowledge development trustee supported by the World Health Organization; and perhaps the most important feature is the multi-sector contribution of both experts and policy makers are engaged in the development of the project that strengthens its successful implementation.
Content of IRTIR
By definition, a registry is a uniform set of information that is generated in a systematic and comprehensive manner to serve a predetermined purpose.21 In health care, disease‐specific registries have been used to serve a number of purposes, including prevention, quality improvement of care, and outcomes research.22 Unlike most disease registries that mainly target one aspect, such as a stroke registry that mostly focuses on care improvement,23 IRTIR mainly targets injury prevention and safety promotion. For instance, most health administrators such health sector authorities and police argue that in Iran that vehicle industries do not follow proper standards which cause serious safety issues for their users, while industrial administrators claim that as crashes are mostly a result of human-related factors, there is no blame on manufactured vehicles. This is while policy makers seek more robust evidence on similar issues to make stronger decisions. IRTIR can produce evidences on prevention issues. Other than producing prevention-related data, IRTIR aims also to improve the quality of care delivered to RTI victims. For instance, determining the injury severity for RTI-patients by ED physicians can estimate the number of predictable deaths and compare them to occurred deaths through a death audit process in different hospitals. The results could help health facilities to detect problems and improve their care. No doubt also, the data collected in the IRTIR can provide a good context for research studies as a complementary source of evidence.
Data Types in IRTIR
IRTIR looks for gathering RTI-related data from current routine data collection systems after some modifications and upgrades in them. Two types of data will be involved in IRTIR:
- Observational data collected by trained EMS personnel, police officers, ED physicians, hospital and post-discharge registrars and forensic medicine specialists.
- Data from the current Iranian transport intelligence systems such as SEPAHTAN and Vehicle Tracking System. The SEPAHTAN system (Smart Surveillance System of Fleet Traffic) includes an integrated set of software that can have an online control of public and heavy vehicles (such as buses, heavy trucks, etc.) in the country, which helps to assure the heeding rules by drivers. This system is used for professional drivers (28). Vehicle Tracking System is used for counting the number of vehicles passing through each road, their speed and violations. Linking this system with crash data will highly improve the richness of crash prevention evidence coming from IRTIR.
Although details of this registry will be published in the near future as the registry protocol with very detailed information on all measurement aspects and full comparisons, here we provide comparisons on conceptual issues of IRTIR with the two well-known registries to provide an earlier understanding of overall similarities.
Utilization
The information retrieved from such a registry could be used for various purposes some of which are listed as below.
- Exploring the common mechanisms and patterns of crashes to be used for prevention purposes.
- Exploring the prevalence and distribution of risk factors including human, vehicle and environments risk factors of road traffic accidents.
- Exploring the patterns and severity of injuries occurring after various crash mechanisms.
- Exploring the incidence of short-term consequences of crash such as PTSD.
- Exploring crash severity indicators with respect to human, vehicle and environment harms.
- Providing necessary information for efficient dispatch to crash scene and decision making for hospital referrals.
- Identifying preventable death cases for conducting death audits.
- Exploring indicators for quality of care and ranking emergency caregiving centers based on the severity adjusted crash fatality rates.
- Exploring direct costs due to traffic injuries.
- Exploring incidence rates for crash events, road traffic injuries and road traffic fatalities.
- Investigating trends of crash risk factor/outcome indicators.
- Investigating the effect of interventions on promoting road safety.
- Investigating effect of interventions on improving quality of emergency services.
- Providing managerial reports for evidence-informed decision makings and policy making.
- Providing information for conducting scientific research.
Conclusion
It is concluded that the IRTIR conceptual model includes the required six components for developing a national integrated registry for Iran. Its main component called content and core measurements leads the researchers in developing final data collection tools in developing the national registry of road traffic injuries in Iran and the other components facilitate the implementation and enrolment.
Strengths and Limitations of This Study
This study introduces a conceptual model for developing a national integrated traffic injury registry in Iran with applicability to the multidisciplinary field of road traffic injuries.
Considering the complexity in developing a road traffic injury registry, it can be considered as a strength and novelty of this study to develop a conceptual model before developing the registry.
A wide national collaboration both at individual and organizational levels as well as international contribution was planned to ensure a more robust model both scientifically and pragmatically.
As this was a conceptual model and not a protocol, a limitation of the study was that details on registry tools are not provided.
Abbreviations
IRTIR, Integrated Road Traffic Injury Registry; FARS, Fatality Analysis Reporting System; RRCGB, Reported Road Causalities Great Britain; ONS, Office for National Statistics; LIMCs, Low- and Middle-Income Countries; HICs, High-Income Countries; YLL, Years of Life Lost; RTIs, Road Traffic Injuries; MOHME, Ministry of Health and Medical Education; UNECE, United Nations Economic Commissions for Europe; OECD, Organization for Economic Co-operation and Development; MRUD, Ministry of Road & Urban Development.
Ethics Approval and Consent to Participate
This project has been approved by the MOHME, Iranian Trustee for Traffic Knowledge Development and Road Traffic Injury Research Center under number 700/1482. It has received ethical approval under number IR.TBZMED.REC.1396.465 from the Ethical Committee in Tabriz University of Medical Sciences.
Verbal informed consent was obtained from all the participants of the study.
Acknowledgments
The authors would like to acknowledge the Integrated Road Traffic Injury Registry research group members who are not listed as authors to this publication.
Peirhossein Kolivand, Mohammad-Hossein Somi MD, Naser Mikaeili PhD, Mousa Amiri PhD, Mashyaneh Haddadi MD, Mahmood Khodadoost MD, Shahriar Behzad Bassirat PhD, Samad Shams-Vahdati MD, Seyed-Hossein Ojaghi MD, Saleh Heydarian PhD Candidate, Nooshin Houshian MSc, Saeideh Sheikhi MSc, Davoud Khorasani MD, PhD, Mojtaba Kheirollahi PharmMD and Alireza Razzagi PhD.
The authors are thankful to Dr. Zendedel Dr. Nouri without whom this work could not have been done. We are thankful to Dr. Ranjbar and Dr. Hamilman for their kind support at all phases of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by following organizations: Iran’s Ministry of Health & Medical Education, Iranian Emergency Medicine Organization, Tabriz University of Medical Sciences and World Health Organization. Author MLW was supported by the Alexander von Humboldt-Stiftung, Bonn, Germany.
Disclosure
The authors declare that they have no competing interests with respect to the contents of this manuscript.
References
1. World Health Organization. Global status report on road safety 2018. 2018.
2. Ainy E, Soori H, Ganjali M, Le H, Baghfalaki T. Estimating cost of road traffic injuries in Iran using willingness to pay (WTP) method. PLoS One. 2014;9(12):e112721.
3. Sadeghi-Bazargani H, Ayubi E, Azami-Aghdash S, et al. Epidemiological patterns of road traffic crashes during the last two decades in Iran: a review of the literature from 1996 to 2014. Arch Trauma Res. 2016;5(3):e32985–e.
4. Organization WH. Road traffic injuries fact sheet reviewed. January, 2018. Available from: http://www.who.int/mediacentre/factsheets/fs358/en/.
5. Khorasani-Zavareh D, Mohammadi R, Khankeh HR, Laflamme L, Bikmoradi A, Haglund BJ. The requirements and challenges in preventing of road traffic injury in Iran: a qualitative study. BMC Public Health. 2009;9(1):486.
6. O’Reilly GM, Joshipura M, Cameron PA, Gruen R. Trauma registries in developing countries: a review of the published experience. Injury. 2013;44(6):713–721.
7. Dimitriou L, Antoniou C. Road safety data considerations. Accid Anal Prev. 2019;130:1–2.
8. Dimitriou L, Nikolaou P, Antoniou C. Exploring the temporal stability of global road safety statistics. Accid Anal Prev. 2019;130:38–53.
9. Organization WH. Global status report on road safety: time for action. World Health Organization; 2009.
10. Zhao Z, Svanström L. Injury status and perspectives on developing community safety promotion in China. Health Promot Int. 2003;18(3):247–253.
11. Sharifian S, Khani Jazani R, Sadeghi-Bazargani H, Khorasani-Zavareh D. Challenges of establishing a road traffic injury surveillance system: a qualitative study in a middle-income country. J Inj Violence Res. 2019;11(2):179–188.
12. Soltani G, Ahmadi B, Pourreza A, Rahimi A. Investigating prevalence of deaths from traffic accidents and factors associated with it in Yazd in 2009. SSU_Journals. 2014;21(6):831–839.
13. Sadeghi-Bazargani H. Road safety data collection systems in Iran: a comparison based on relevant organizations. Chin J Traumatol. 2020.
14. Rodman H. Are conceptual frameworks necessary for theory building? The case of family sociology. Sociol Q. 1980;21(3):429–441.
15. Aarons GA, Hurlburt M, Horwitz SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Dm Policy Ment Health. 2011;38(1):4–23.
16. Safety management of transportation and traffic crashes regulation. 2009.
17. Ahmed A, Sadullah AFM, Yahya AS. Errors in accident data, its types, causes and methods of rectification-analysis of the literature. Accid Anal Prev. 2019;130:3–21.
18. UNECE Ǧ. United nations economic commission for Europe (2009) illustrated glossary for transport statistics. 2017.
19. OECD. OECD health statistics 2017: definitions, sources and methods – injuries in road traffic accidents. 2018.
20. Peden M, Scurfield R, Sleet D, et al. World report on road traffic injury prevention. Geneva: World Health Organization; 2004.
21. Santé Omdl. Global status report on road safety 2013: supporting a decade of action. World Health Organization; 2013.
22. Commission E. Intersecretariat working group on transport statistics. Glossary of transport statistics, 3rd edition. Luxembourg: United Nations Economic and Social Council; 2003.
23. Tepas JJ editor. The National Pediatric Trauma Registry: A Legacy of Commitment to Control of Childhood Injury. Seminars in Pediatric Surgery. Elsevier; 2004.
24. Nwomeh BC, Lowell W, Kable R, Haley K, Ameh EA. History and development of trauma registry: lessons from developed to developing countries. World J Emerg Surg. 2006;1(1):32.
25. Ford JE, Alqahtani AS, Abuzinada SAA, et al. Experience gained from the implementation of the Saudi trauma registry (STAR). BMC Health Serv Res. 2020;20(1):18.
26. Paradis T, St-Louis E, Landry T, Poenaru D. Strategies for successful trauma registry implementation in low- and middle-income countries – protocol for a systematic review. Syst Rev. 2018;7(1):33.
27. Cassidy L, Olaomi O, Ertl A, Ameh E. Collaborative development and results of a Nigerian trauma registry. J Registry Manag. 2016;43(1):23–28.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.