Back to Journals » Patient Preference and Adherence » Volume 9
Developing a discrete choice experiment in Malawi: eliciting preferences for breast cancer early detection services
Authors Kohler R, Lee C, Gopal S, Reeve B, Weiner B, Wheeler S
Received 25 April 2015
Accepted for publication 19 June 2015
Published 14 October 2015 Volume 2015:9 Pages 1459—1472
DOI https://doi.org/10.2147/PPA.S87341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Racquel E Kohler,1 Clara N Lee,2 Satish Gopal,3 Bryce B Reeve,1 Bryan J Weiner,1 Stephanie B Wheeler1
1Department of Health Policy and Management, Gillings School of Global Public Health, 2Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 3UNC Project-Malawi, Tidziwe Center, Lilongwe, Malawi
Background: In Malawi, routine breast cancer screening is not available and little is known about women’s preferences regarding early detection services. Discrete choice experiments are increasingly used to reveal preferences about new health services; however, selecting appropriate attributes that describe a new health service is imperative to ensure validity of the choice experiment.
Objective: To identify important factors that are relevant to Malawian women’s preferences for breast cancer detection services and to select attributes and levels for a discrete choice experiment in a setting where both breast cancer early detection and choice experiments are rare.
Methods: We reviewed the literature to establish an initial list of potential attributes and levels for a discrete choice experiment and conducted qualitative interviews with health workers and community women to explore relevant local factors affecting decisions to use cancer detection services. We tested the design through cognitive interviews and refined the levels, descriptions, and designs.
Results: Themes that emerged from interviews provided critical information about breast cancer detection services, specifically, that breast cancer interventions should be integrated into other health services because asymptomatic screening may not be practical as an individual service. Based on participants’ responses, the final attributes of the choice experiment included travel time, health encounter, health worker type and sex, and breast cancer early detection strategy. Cognitive testing confirmed the acceptability of the final attributes, comprehension of choice tasks, and women’s abilities to make trade-offs.
Conclusion: Applying a discrete choice experiment for breast cancer early detection was feasible with appropriate tailoring for a low-income, low-literacy African setting.
Keywords: breast cancer, early detection, patient preferences, discrete choice experiment, Malawi, qualitative interviews
Introduction
Breast cancer rates are increasing in African countries,1 yet few have successfully adopted national cancer control plans or breast cancer early detection programs. Mammography is not widely available due to infrastructure costs and human resources it requires; therefore, many African countries rely on more pragmatic approaches to early detection, such as clinical breast exams (CBEs), and promoting breast health awareness.2,3 The Breast Health Global Initiative consensus statement suggests CBE may be the most resource-appropriate strategy in most African countries with limited resources; however, evidence regarding the feasibility and efficacy of detection and screening strategies in these settings remains unclear.4
Defining conditions under which women would seek out breast cancer early detection services would allow policymakers and ministries of health to base future programs on evidence. Previous studies from Africa suggest that lack of services, low breast cancer knowledge, privacy concerns, lack of transportation, and women’s roles and responsibilities may influence early detection and diagnosis behaviors of breast cancer.4–6 However, to date, no studies have assessed African women’s preferences about different breast cancer early detection methods or programs.
Preference elicitation techniques, such as discrete choice experiments (DCEs) and best–worst scaling (BWS), provide information about the value of hypothetical new services or delivery models and help estimate their potential uptake and utilization.7 These survey techniques are based on the premise that a good or service can be broken down into separate attributes, or characteristics, and the total preference for using a service is made up of the individual preferences of the attributes of the service.7–9 A DCE involves presenting respondents with hypothetical scenarios in a choice set and forcing respondents to choose between the scenarios in order to understand trade-offs between attributes and levels of attributes.8
Applying a DCE to breast cancer detection in Africa could be valuable to determine women’s preferences for future interventions, and to our knowledge, no previous studies have developed a DCE for breast cancer detection in low-income countries. The relevance of a DCE depends on identifying locally appropriate attributes and defining levels of the attributes that are plausible in the local context. Qualitative methods are recommended to understand important characteristics of the service and to help identify attributes and levels which the target population deems relevant.10,11 Additionally, some studies suggest that preference elicitation techniques are complex and may be difficult for populations with lower education levels, literacy, numeracy, or mental capacity to comprehend or use meaningfully.12,13 Few studies have used DCEs among vulnerable international or low-literacy populations, thus, we report the development and testing of a breast cancer early detection DCE among a low-income, low-literacy population. The objectives of this study were to understand factors that affect women’s intentions to use cancer detection services, to identify and select relevant attributes for a DCE, and to determine the optimal design of a DCE and its feasibility and acceptability in Malawi.
Methods
Study setting
This study was embedded within a larger mixed methods study of breast cancer knowledge and preferences conducted in Lilongwe, the capital of Malawi. The government provides basic health services free of charge through local health centers dispersed among rural villages, district hospitals, and central referral hospitals.14 The remaining proportion of health care is provided by mission hospitals, which are partly subsidized, and private clinics, which charge fees.15 Because of physician shortages, clinical officers, who undergo a shorter medical training compared to physicians,16 provide care in various primary and some specialty care settings.
Accessing health services is difficult for many Malawians, especially those lacking formal employment, economic stability, and transportation. Regarding breast cancer services, pathology and chemotherapy in Malawi are currently available at two large teaching hospitals in Lilongwe and Blantyre.17 Mammography is available at a private clinic in Lilongwe for ~$150 USD, but the national service delivery guidelines recommend CBE and education on breast self-exams (BSEs); no national breast cancer screening program exists.18 However, screening for cervical cancer has increased in the last decade and is available at many lower level health centers across the country.19
Literature review
The attribute development process began with a literature review focused on breast cancer detection services in sub-Saharan Africa. The search was conducted using PubMed, Web of Science, and Google Scholar databases and included published articles in English from 2000 to 2012. We used combinations of the following search terms: breast cancer, early detection, screening and discrete choice experiment, conjoint analysis, best worst scaling, and preferences. Additional articles were obtained through manual review of reference lists of retrieved articles. In this paper, we focus on the findings from preference studies regarding breast cancer screening as well as DCEs applied in other African settings.
Qualitative data collection
We conducted 30 individual interviews from April to August 2014 to provide a rich understanding of the factors affecting women’s choices regarding preventive health care and early detection of cancer.11 We recruited ten health care workers (HCWs) who provide routine women’s health care from multiple departments of a public referral hospital, district-level hospital, and public trust clinic for HIV patients. The semistructured interview guide included broad topics such as cultural perceptions of cancer, health system factors affecting cancer diagnosis and treatment, and knowledge and attitudes regarding breast cancer and early detection methods, as well as demographic and employment information. HCW interviews were conducted in English, recorded, and transcribed verbatim. On average, the HCW interviews lasted ~1 hour.
We also recruited 20 community residents and women attending family planning and reproductive health clinics because they were identified as potential target clients of future breast cancer detection services. We purposefully selected two clinics to recruit four women with positive health seeking behaviors, but with varying age and exposure to cancer services. We oversampled women in the community from residential areas in Lilongwe district. We selected two urban and two rural residential areas based on distance and access to district and central hospitals then randomly selected four households within each area to recruit women. Two local interviewers, who were trained in interview procedures, conducted and digitally recorded individual interviews in Chichewa, the local language. Semistructured interview guides collected demographic information about the participants as well as their health seeking behaviors and breast cancer knowledge, attitudes, preferences, and practices, as well as general preventive health care attitudes. At the end of the interview, the interviewer reviewed a fact sheet about breast cancer signs/symptoms, risk factors, and detection strategies. The interviewer informed each participant about CBE and BSE, but did not conduct an exam or provide formal instruction on BSE. Interviews lasted for 35 minutes on average and were transcribed verbatim, then translated into English.
We used Atlas.ti 7 (Atlas.ti Scientific Software Development, Berlin, Germany) to code the transcripts. Two coders independently applied a common codebook based on conceptual domains identified in the literature review and the social contextual framework.20 We revised codes and definitions as additional themes emerged. After applying the final codebook to all transcripts, we reviewed common co-occurring themes and looked for patterns within and across HCWs and community transcripts.
Designing the choice experiments
The data collection team worked with community outreach leaders, who lead a local community advisory board and are responsible for community education and sensitization programs, throughout the development of the DCE. After reviewing preliminary results of the qualitative interviews, we discussed the relevance of potential attributes to determine a smaller subset. We also identified plausible levels for the attributes based on responses, such as common transportation costs, reported travel times, and frequently mentioned health encounters. We used Sawtooth Software 8 (Sequim, Washington) to design two choice experiments and printed hard copies of choice cards with images. We proceeded to evaluate patient understanding of the experiments using cognitive interviewing methods described below.
In addition to the DCE, we developed a BWS exercise to determine which approach was more appropriate for the target population. BWS, also called maximum difference, is a discrete choice task in which a person is asked to select the best and the worst (or most important and least important) aspect within a scenario instead of choosing between scenarios.21 This exercise has the potential to produce robust data about the importance of attributes and levels at a lower level of cognitive burden.22,23
Cognitive interviews
Cognitive interviewing is a qualitative method that can help identify problems with comprehension and other cognitive processes that can be resolved by revising the instrument.24 We purposively recruited eight low-income and/or low-literacy women through the community advisory board contacts to ensure that the experiments were comprehensible and to check the adequacy of the attributes and levels. The same interviewers were trained in cognitive interview procedures and conducted the interviews in Chichewa; each cognitive interview was digitally recorded for analysis. The interviewer took detailed notes on the participant’s responses and whether or not she had difficulty with particular choice sets, wording, or images. The interviewers described the attributes, levels, and corresponding images, introduced the experiments, talked through a practice example, and administered the DCE and BWS experiments. During the interview, the respondents were asked to think aloud as they made their choices and provide feedback about the difficulty of the choices, comprehension of the attributes and levels, and acceptability of images and how they influenced understanding. At the end of each interview session, the interviewer wrote a detailed summary and debriefed with the rest of the data collection team to review problematic areas and make revisions appropriate for Malawian women with low-literacy levels.
This study was reviewed and approved by the University of North Carolina at Chapel Hill Institutional Review Board and the Malawia National Health Services Research Committee. All participants provided written and verbally recorded informed consent to participate in the study. Consent forms were read aloud to illiterate participants who also provided a thumb print if they could not sign their name.
Results
Identifying relevant attributes and levels from the literature
Because no studies from low-income countries have explored breast cancer detection preferences, we relied on studies from high-income countries, which examined characteristics of mammography screening services.25–31 Additionally, we identified one study that assessed preferences for BSE education,32 but none about CBE. We identified common conceptual domains, including attributes about the invitation or reminder to participate in screening, convenience, facility setting, privacy, accuracy and frequency of the intervention, and how results were relayed. In light of the Malawian context, we also considered how other DCEs conducted in Africa described and presented health interventions and considered additional concepts such as provider characteristics and health infrastructure.33–36 We used the list of potential attributes and levels from the literature (Table 1) to develop probing questions for the community and HCW interview guides, so we could explore these concepts in more detail.
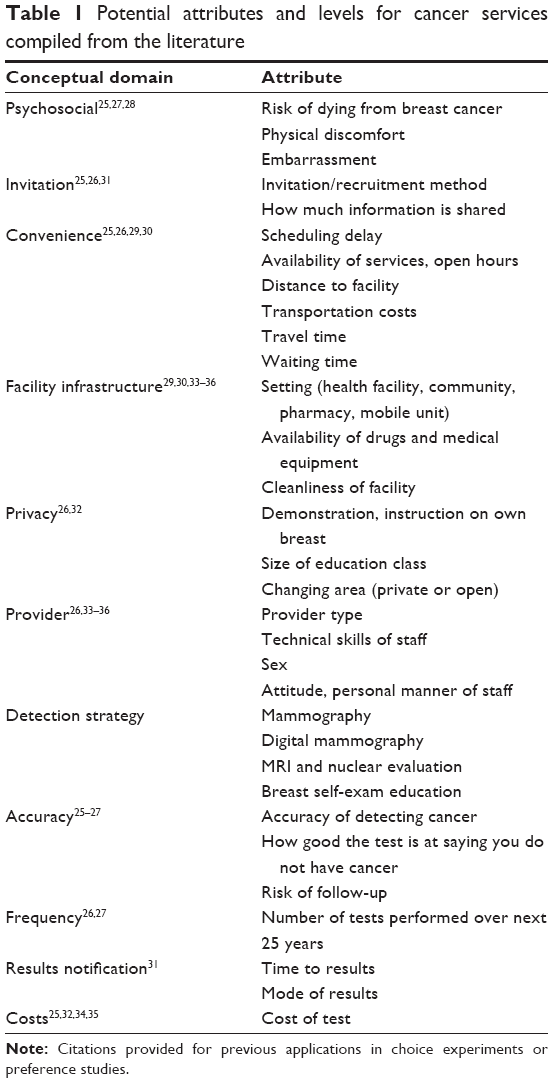 | Table 1 Potential attributes and levels for cancer services compiled from the literature |
Sample characteristics
The majority of HCWs we interviewed were female nurses, and the mean age was 37 years (Table 2, top panel). We purposively recruited workers from different departments, including oncology, surgery, obstetrics/gynecology, casualty, and HIV care. HCWs had been working at their current job for an average 3 years, and the mean professional experience was 12 years (ranging from 1 year to 35 years). Five of the HCWs provided cancer treatment, and two provided cervical cancer screening services.
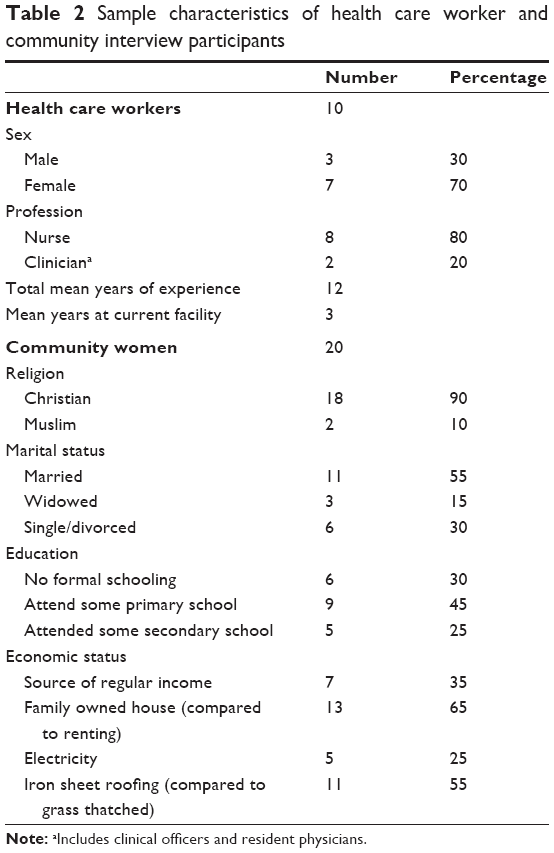 | Table 2 Sample characteristics of health care worker and community interview participants |
The mean age of the 20 community participants was 42 years (Table 2, bottom panel). The majority of women were Christians (18) and married (11). In terms of education, six women had no schooling, nine had some primary education, and only five attended secondary school. Seven women reported a regular income, and five had electricity.
Distance to the facility and travel time
The most common factor that the community women mentioned about why they chose to use certain health facilities was the distance or travel time to get there. Most women walked to the nearest facility and described how transportation costs to other hospitals were prohibitive. Some hired a ride on a bicycle or took a minibus to their preferred facility when they could afford it. Few women were able to estimate how far they traveled; instead, they described how long it took to walk and reach the facility. The HCWs also acknowledged the importance of distance and transportation costs as the primary drivers of where women sought care. But both groups mentioned that facility choices also depend on the severity of the health condition. Some women were willing to travel longer distances for specialty care at different facilities versus “for lighter ones [conditions] I can go to clinics”.
Costs of care and perceptions of quality
Although the women from the community described many differences between government and private facilities, most used government hospitals because “they are free, you don’t need to pay anything”. For some, their lack of financial resources kept them from accessing their preferred facility, which led to delaying care because of the costs. One woman explained:
The hospital that is near is private. So because of the prices they charge there, sometimes we cannot afford it and Area 25 health center (public facility) is far. As a result you just decide not to go the hospital anymore. As a result the problem worsens.
HCWs suggested that future services should be established and expanded at government facilities because “most people here are poor, so they would come to a government institution where there are free services”.
However, some women chose between nearby health centers based on past experiences or recommendations from their social network. The quality of services, especially the availability of medications or working equipment at the facilities, affected their preferences. Staff attitudes were also important, as one woman reflected, “It is how they welcome us [if] they receive us well when we go and tell our health problem”. HCWs also noted that facilities can get “overwhelmed with a lot of patients coming each and every day” and that patients are sometimes “sent back if the resources are not there”, which may affect where patients choose to get care.
Still other community women felt that they had no choice because of the referral requirements to get to the central hospital. As one participant described, “We do not choose because you are supposed to go to your clinic first, then at the clinic they will refer you to Central”. Similarly, HCWs thought it was important to offer cancer detection services at lower level health centers because that is where patients go first. But some also thought detection services should be provided “across the health system starting from the health surveillance assistants (HSAs) to the health care centers and the district hospital”.
Preferred health care workers and sex
Although the community women spoke generally about “doctors” and rarely differentiated between types of HCWs, the HCWs we interviewed had opinions about who should conduct a CBE or teach women about breast health and BSE. The two clinicians suggested that clinical officers should do CBEs because they might be more knowledgeable about breast cancer, and that antenatal care (ANC) nurses already perform breast health education and could increase those efforts. The nurses proposed that community workers and HSAs do the education, and that patients with breast cancer should get involved because they could give testimonies to encourage early detection. But the community women did not discuss preferences for doctors over nurses; they only made a distinction between HSAs and other health workers because HSAs are in the community more and wear different uniforms. However, their discussions did not indicate strong preferences for doctors or HSAs.
Additionally, patient–provider communication was mentioned as a potential factor in women’s decisions to seek cancer detection services. A few of the nurses thought some patients might be afraid of the hospital and HCWs if they suspect cancer because they might be scolded for delaying care and presenting with advanced symptoms. Another nurse explained:
There might be health workers who are not good at communicating, especially like breaking bad news. Being told you have cancer is bad news. So we may have people who are not tactical enough when they are breaking the bad news, so people are afraid of them. So people are afraid of that – the way you are told, ‘You have cancer, so there’s nothing we can do.’
Community women’s preferences for male or female HCWs also varied depending on the health issue or type of exam. Many women said if possible, they would prefer to be seen by a woman for a CBE because they would feel shy and embarrassed if a man attended to them. One woman explained:
We women would love to be checked by our fellow women. But the way we know how doctors are at the hospital, it is mixed…so when we go to the hospital, we don’t have the power to choose, like to say I want to be checked by a female doctor.
Some women recalled having a male HCW during delivery of their children, and accepted whoever was available because, “There can be no shame. I should just say a doctor is a doctor”. This attitude seemed to stem from women feeling that they had no choice as one participant explained, “you are sick, you don’t have the freedom to say that you should not assist me, that this other one will assist me”.
Interestingly, a few community women preferred male HCWs because they thought females were “cruel” and did not ask questions or take notes about their complaints; participants told stories of how female HCWs assumed a lot about patients and “just say bad things to you, so we do not like them”. Conversely, the male workers they encountered were more thorough during exams and gave “better treatment”. so some women trusted “the male ones because they show that they have a passion in their job”.
Privacy
We also found different preferences regarding privacy. Although community women talked about breastfeeding on the minibus, in church, and walking down the street, they thought breastfeeding was the only appropriate time for a woman to expose her breasts publicly. However, some did not consider their breasts to be “private parts”. Most were not embarrassed to expose their breasts during a physical exam, but felt shy if they were asked to expose their “private part down there” for a pelvic exam or cervical cancer screening. The Muslim participants said undressing “everywhere” or “down there” for a male HCW was “not allowed” and a few other women had similar preferences for females doing pelvic exams for the same reason. One woman explained, “The problem is down there. The breast is not a problem…as long as you are sick”. This caveat about accepting a male HCW as long as you were sick was common. Participants usually went on to say that it was okay for a male HCW to do the exam “because he was trained” but often clarified that it was acceptable only because “you need treatment”.
The importance of testing in a culture of curative care
In a country that has faced a significant HIV burden, it is not surprising that the importance of “testing” was a common theme that emerged. Nearly all the community women spoke positively about going to get checked because, “you think you are ok but maybe you are not ok…when you go to the hospital you are able to know” and they thought getting tested was “better than just staying” at home delaying. However, this was usually discussed in the context of a suspected health concern or symptom. Women were cautious about going to the hospital when they were not sick and worried whether they would be helped. Some thought going without a complaint was inconvenient to doctors or a burden on the health care system. A few noted the main issue was the lack of a specific facility where people could go for a well checkup or general physical exam, “so we usually wait until we are sick. That’s when we seek medical help”. Another woman described:
It has been established that we wait until we are sick…The problem is that when you go to the hospital while you are not sick, I don’t think they can assist you. They will just say, “Why are you coming here? You are wasting our time. We should assist the people who are sick”.
Similarly, the HCWs shared the perspective that people in Malawi have “poor health seeking behaviors. We only want people to come to the hospital when they are sick”. These sentiments often preceded discussions about staffing shortages and overcrowded hospitals. A few recalled how they had turned people away because of “queues and queues of sick patients”. These attitudes and health infrastructure challenges likely have implications for access to and demand for cancer detection services because “when they (patients) come and ask if they have the disease, we will ask them, ‘Why are you here? You are not sick. Go back’”. Nonetheless, they thought it was important to promote general wellness exams with CBEs and suggested establishing “clinics where someone can just go for medical checkups” or a dedicated “breast clinic day” for education, exams, and counseling.
Bundled services and point of entry into health system
We also explored whether community women would be interested in coming for early detection services alone, and how they could be integrated into other preexisting services and routine care. Many of the community women said they heard about BSE and/or breast cancer from a health talk at family planning, ANC, or a community health gathering. Participants from both groups thought CBEs would be more convenient if they were added to frequently used services, such as under five child health checkups, HIV voluntary counseling and testing, and cervical cancer screening. One nurse suggested,
Then it will be much easier for the patient because she comes for visual inspection with acetic acid but at the same time her breasts are examined for breast cancer, rather than her going home and coming back again another day.
HCWs also recommended emphasizing education beyond family planning and ANC visits. They thought that taking advantage of the large crowds in hospital waiting areas to educate women on breast cancer, BSE, and CBE might reach more women. These common, routine health encounters and health talks were cited as important opportunities to use the point of entry into care to offer additional breast cancer detection services and education.
Breast cancer risk perception and detection methods
In general, community women knew very little about breast cancer, signs, symptoms, or detection methods. They also had a low perceived risk of breast cancer and seemed more interested in early detection to make sure they were healthy enough to continue working, not because they were worried about having cancer. Only one participant said she feared the results and was hesitant to get checked; the rest of the women said it was “good to know how your body is”. They did not seem worried or anxious about having an exam that specifically looked for cancer as one woman explained:
That would not be a problem because I need to know…once I know, the doctors can treat me in time. […] it is better to know instead of not knowing because nothing can help you. You can just be living in ignorance. When you are told, you know.
Most of the community women were interested in “getting tested”, but they did not know what the test was. When asked specifically about having a CBE, nearly all of the women were willing and a majority asked for the interviewer to do the exam at the end of the interview. Participants were eager to learn more about breast cancer and how to do BSE; they often wanted to invite their neighbors to come over so the interviewer could tell more people about breast cancer.
We also asked HCWs about differences in detection modalities. Only four were aware of mammography; one said, “Of course, I don’t know much. I just heard it…” and another said he remembered learning about a machine to look for breast lumps in school. Only two knew that mammography was available in Malawi. Instead, the HCWs suggested educating women on BSE as a good way to help address breast cancer control in addition to CBEs. Interestingly, a few women brought up the point that HCWs were more knowledgeable than they were themselves about detecting breast problems. One woman questioned the accuracy of BSE and noted that she might miss a potential problem. A few other women were more interested in a CBE than BSE as one woman described, “I cannot recognize my problem myself, but the doctor was trained on that”.
Selecting the final attributes
After reviewing the responses, the data collection team and community outreach leaders discussed the feasibility of incorporating the emergent themes into a new breast cancer intervention and whether we should include those characteristics in the DCE. For example, we discussed where and how the services could be offered given the local context of care, and which types of facilities might be willing and interested in establishing an intervention. We narrowed the list of attributes in order to reduce the cognitive burden of the DCE while trying to reflect the range of situations women might experience. Based on the interviews, we decided to frame the choice within the governmental context and did not include a cost component for the service because public services are free. Instead, we included a quantitative attribute regarding travel time to estimate the relative value of other attribute levels. Due to the lack of local data regarding breast cancer risk and the limited access to mammography services, we did not include risk, mammography, or accuracy of detection methods. The final attributes and levels incorporated into the choice experiment (marked in final column of Table 3) were travel time (<1 hour by foot, 1–2 hours by foot, or >2 hours by foot), health worker type (doctor or HSA), health worker sex, health encounter (health talk in facility waiting area, community health gathering, cervical cancer screening, family planning clinic, or child under five clinic), and breast cancer early detection strategy (breast health awareness, CBE, or combination of awareness and exam).
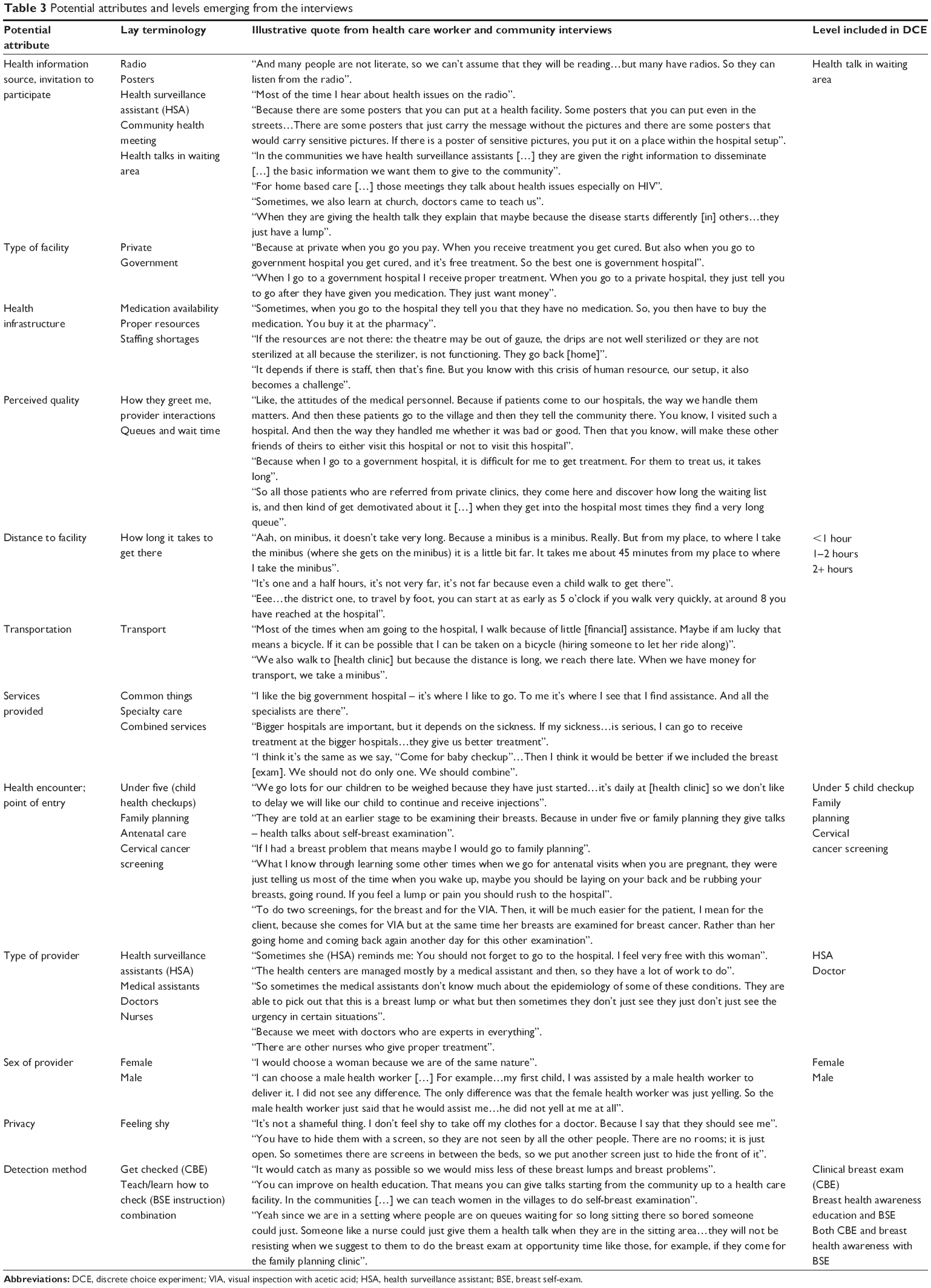 | Table 3 Potential attributes and levels emerging from the interviews |
Testing the choice experiments
During the cognitive interviews, an interviewer tested interpretation problems to determine the validity of the levels in the scenarios. Respondents had a hard time understanding what “breast health awareness” meant. They wanted to know whether it was just an explanation and suggestion to “feel for lumps”, whether it would include a demonstration, or whether they would receive instruction and training on how to conduct a BSE. Respondents thought the ranges of attribute levels were acceptable, but they also brought up the relevance of the different health encounters; for example, an older woman said she no longer needed family planning, so she thought the health talks and cervical screening visit were more convenient.
We explored how participants preferred to learn about the attributes – for example, whether distance to the health facility should be described by kilometers, travel time, or the cost of a minibus ride. Most of the women preferred walking time, except one woman who lived in town and thought the minibus cost was easier to understand. Because a large portion of the target population lived in rural areas and likely had to walk a long time before getting on a minibus, we used walking time in the final DCE.
We also tested the BWS exercise to assess the importance of different attributes. Women had trouble choosing only one most and one least important item, and women were confused about what to do because there were too many options. They wanted to say yes or no whether each level was important. Although one woman preferred the BWS exercise to the DCE, the rest commented that the DCE was easier because it required “one choice for the full thing” rather than “picking only one good thing” from each scenario.
The responses indicated that the DCE was feasible and women understood the tasks. When we asked respondents to identify differences in the scenarios, they were able to discuss differences and mentioned that the introduction helped them understand the differences in the attributes and levels. As they worked through the choice sets, we assessed whether they were able to make trade-offs. The women were able to explain the rationale of their choices. For example, one woman noted how she was mainly interested in the CBE, “I want the breast exam no matter how far I have to walk”.
Because most of the respondents had only a few years of primary school, they relied on the interviewer to read each scenario aloud and compared the options by looking at the cards. The women described how it was helpful to hear the full scenario described almost like a story or vignette, instead of just reading each attribute level of the scenario. To them, it was important to look at the full picture and compare the two scenarios on the card as they made trade-offs. They also noted how the images helped them understand the differences between each scenario and answer faster.
Based on the feedback received, we revised the attribute-level descriptions, updated our graphics, and summarized each hypothetical scenario to be read aloud to the participants. An example of one of the DCE sets is displayed in Figure 1.
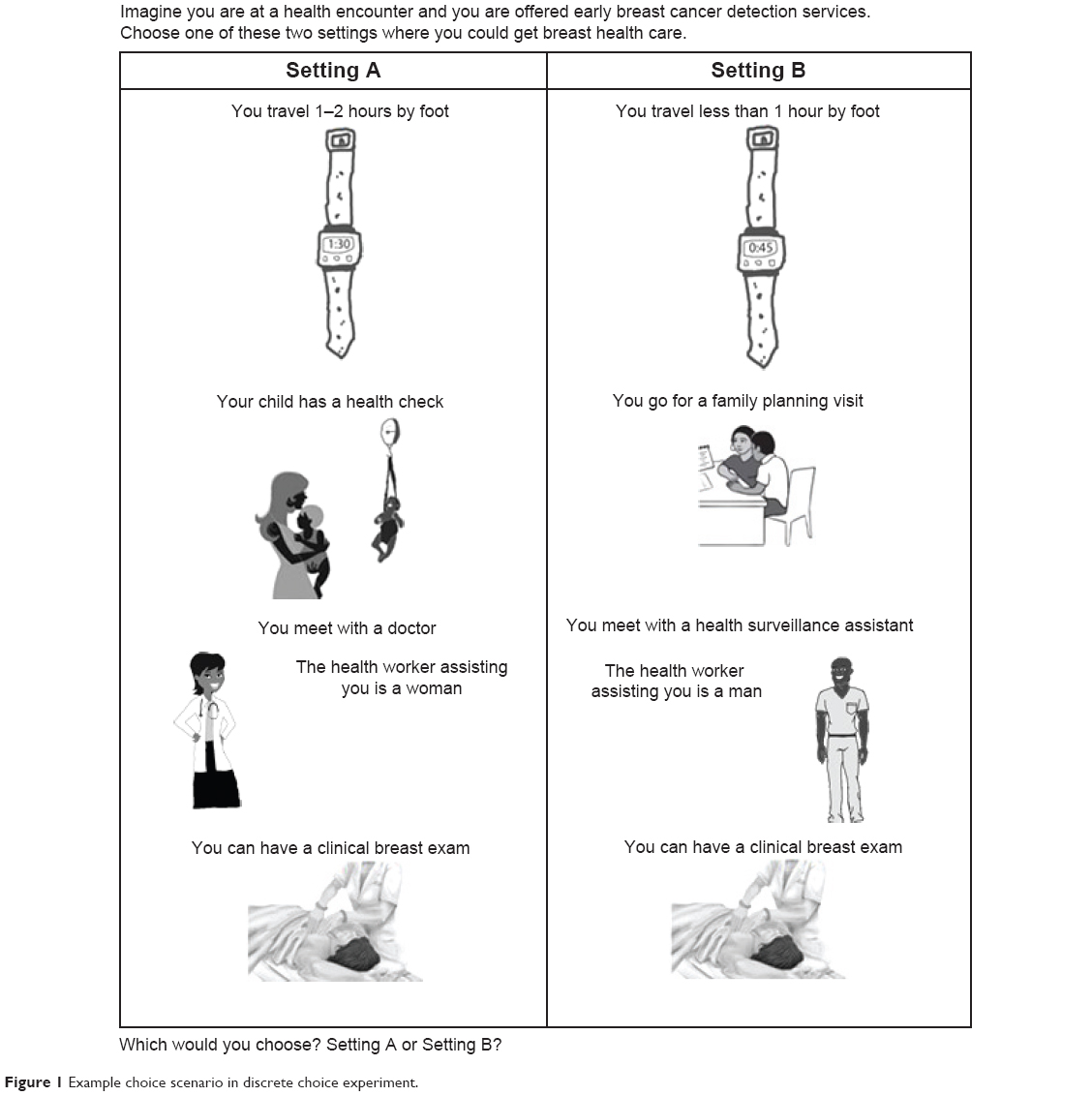 | Figure 1 Example choice scenario in discrete choice experiment. |
Discussion
This article describes the results of a systematic, qualitative process to develop attributes and levels for a choice experiment regarding a rarely used prevention service in a resource-poor setting. Although studies from other countries have identified barriers and facilitators to breast cancer screening, we are not aware of any that evaluate African women’s preferences for early detection services. In this manuscript, we explain major themes and preferences regarding breast cancer early detection in Malawi as well as the results of cognitive testing to determine the feasibility of administering a DCE in a low-literacy setting. We found that despite women’s low socioeconomic status in a health system with limited resources, preferences and experiences strongly influenced why and where women considered seeking services. We developed a final set of five attributes for the DCE, which can be used to assess trade-offs between attributes and levels. The attributes included in the DCE were travel time, health worker type and sex, health encounter type (point of entry), and breast cancer detection strategy.
The interviews identified some attributes that have been suggested in other breast cancer work, such as distance to the facility and transportation costs. However, we also found that perceptions of quality and previous health experiences were important considerations of preferred health facilities. Though most preferred the nearest free facility, some women were willing to travel farther to get specialty care, which may be an important distinction for cancer detection services if women notice symptoms or have a breast concern.
Preferences about the sex of HCWs varied. Despite feeling like they had no choice regarding HCWs, community women, especially Muslim women, expressed privacy concerns about physical exams by male health workers. Generally, women indicated that they would prefer a female HCW, but some preferred men. This may be due to the strong trust in HCWs, paternalistic health system, and perceptions of the hierarchy in local practice; for example, one woman noted, “When the nurses fail they do call a male doctor”. Cultural and religious beliefs may influence social norms and be barriers to CBE.37–39
Women’s discussions about health infrastructure challenges and going to the hospital for preventive screening highlighted potential social norms and structural factors that may influence demand for cancer detection services. Attitudes and preferences about going for testing and accepting male HCWs only when sick may have implications for barriers to early detection among asymptomatic women. The HCWs in this study were optimistic about integrating early detection into other health encounters to increase access and uptake, and the women seemed interested. Previous studies from South Africa, however, have had mixed results after combining breast and cervical cancer screening interventions.40,41
When we tested the choice experiments using cognitive interview methods, we found that women preferred the DCE over the BWS design because they felt restricted to choose only one best and worst option. Our findings supporting the validity and acceptability of the DCE format are similar to a recent study comparing BWS and DCE approaches at a university campus in Australia; the authors observed that participants had trouble choosing the worst attribute level and wanted to rank all the options in the scenario.42 Women in our study were able to complete the DCE tasks and were able to make trade-offs comparing the scenarios side-by-side. They found it helpful to hear a description of the full scenario and follow along with images. The literacy rate of the adult population in Malawi is ~61%, suggesting that a large proportion of the adult population cannot read and write.43 Thus, it was imperative that our DCE included images of all attribute levels to help improve respondents’ comprehension of the scenarios. The DCE design was ultimately chosen to ensure participants understood and could engage with the choices and to help address the low literacy of participants. The cognitive interviews supported women’s capacity to complete the experiment and helped to refine the design of the DCE, which was later administered in a larger quantitative study.
By starting with a systematic review of potential attributes and levels, we were able to build on the existing literature from high-income countries. The qualitative interviews with HCWs and community women helped provide realistic attributes and levels that improved the chance that the DCE reflects important and relevant characteristics of early detection services in Malawi. Cognitive interviews ensured comprehension of the attributes, levels, and images, and identified problem areas that required revisions.
Despite these strengths, we must address some limitations of this study. The nature of this qualitative research and the small sample size limits the generalizabilty of these findings. Additionally, the participants’ knowledge of breast cancer and detection methods was low, which may have limited their responses. However, a few participants had previous experiences with detection methods and other types of cancer screening. We also asked about prevention services more generally, so others were still able to engage in meaningful discussions about aspects of early detection. In terms of developing the DCE, we may not have accurately described all the attributes some participants consider important and relevant in the DCE, but we included the attributes that the majority of participants discussed that could potentially be tailored for future interventions.
This is the first study, to our knowledge, to develop a tool based on breast cancer detection preferences of low-literacy and low-income women. Although we set out to develop a context-specific preference tool for use in Malawi, our findings are far reaching beyond this specific setting. This DCE may be applicable in other African countries, with appropriate modifications, and could potentially be adapted to additional types of prevention services. For example, community interviews highlighted that women have modesty and privacy concerns, regarding pelvic exams and cervical cancer screening. Therefore, the basic DCE design could be modified to assess preferences for cervical cancer screening. However, the relevance of attributes should be explored through qualitative methods before administering the experiment. In addition, since this study began, other DCEs in African settings44,45 have been published, including two conducted in Malawi.46,47 They confirm the potential to apply DCEs more widely in African populations to inform policies and interventions to reduce health disparities.
Conclusion
We presented detailed information about our process of qualitatively developing and testing a preference elicitation tool for breast cancer early detection in a region where early detection is uncommon, preferences regarding health care choices are unknown, and few DCEs have been administered. Throughout this process, we identified many complex factors that influence Malawi women’s choices about whether to participate in early cancer detection services based on health care worker and community women’s input. Our findings suggest that assessing breast cancer detection preferences through a DCE is feasible in Malawi and possibly other low-income, low-literacy populations in Africa. A better understanding of women’s preferences may help determine how detection services should be delivered in Malawi and has potential to improve uptake and acceptability of future breast cancer early detection interventions.
Acknowledgments
The authors would like to thank and recognize additional research team members including Sylvia Thembulembu, Olivia Yambeni, and the Community Advisory Board from UNC Project Malawi. We would also like to thank Anna R Miller and Trisha Crutchfield from the University of North Carolina at Chapel Hill for their assistance with qualitative analysis and technical support. Sources of support for this study include Dr. Kohler’s pre-doctoral fellowship through the UNC Cancer Care Quality Training Program (R25 CA116339) and the UNC Hopkins Morehouse Tulane Fogarty Global Health Fellows Program (R25 TW009340).
Disclosure
Authors have no conflicts of interest to report.
References
Parkin DM, Bray F, Ferlay J, Jemal A. Cancer in Africa 2012. Cancer Epidemiol Biomarkers Prev. 2014;23(6):953–966. | ||
Harford JB. Breast-cancer early detection in low-income and middle-income countries: do what you can versus one size fits all. Lancet Oncol. 2011;12(3):306–312. | ||
Corbex M, Burton R, Sancho-Garnier H. Breast cancer early detection methods for low and middle income countries, a review of the evidence. Breast. 2012;21(4):428–434. | ||
Anderson BO, Cazap E, El Saghir NS, et al. Optimisation of breast cancer management in low-resource and middle-resource countries: executive summary of the breast health global initiative consensus, 2010. Lancet Oncol. 2011;12(4):387–398. | ||
Muthoni A, Miller AN. An exploration of rural and urban Kenyan women’s knowledge and attitudes regarding breast cancer and breast cancer early detection measures. Health Care Women Int. 2010;31(9):801–816. | ||
Maree JE, Wright SC. How would early detection be possible? An enquiry into cancer related knowledge, understanding and health seeking behaviour of urban black women in Tshwane, South Africa. Eur J Oncol Nurs. 2010;14(3):190–196. | ||
de Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. | ||
Ryan M, Gerard K. Using discrete choice experiments to value health care programmes: current practice and future research reflections. Appl Health Econ Health Policy. 2003;2(1):55–64. | ||
Lancaster KJ. A new approach to consumer theory. J Polit Econ. 1966;74(2):132–157. | ||
Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health – a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. | ||
Coast J, Al-Janabi H, Sutton EJ, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21(6):730–741. | ||
Shumway M, Sentell T, Chouljian T, Tellier J, Rozewicz F, Okun M. Assessing preferences for schizophrenia outcomes: comprehension and decision strategies in three assessment methods. Ment Health Serv Res. 2003;5(3):121–135. | ||
Woloshin S, Schwartz LM, Moncur M, Gabriel S, Tosteson AN. Assessing values for health: numeracy matters. Med Decis Making. 2001;21(5):382–390. | ||
Malawi Ministry of Health. Health Institutions. Social and Community Services; 2013. Available from: www.malawi.gov.mw | ||
Malawi Ministry of Health. Malawi Health Sector Strategic Plan 2011 – 2016: Moving Towards Equity and Quality. Lilongwe; 2011:148. Available from: http://malawipublichealth.org/wp-content/uploads/2014/03/Malawi-HSSP-Summary.pdf. Accessed: February 1, 2015. | ||
Muula AS. Case for clinical officers and medical assistants in Malawi. Croat Med J. 2009;50(1):77–78. | ||
Gopal S, Krysiak R, Liomba G. Building a pathology laboratory in Malawi. Lancet Oncol. 2013;14(4):291–292. | ||
Malawi Ministry of Health. Malawi National Reproductive Health Service Delivery Guidelines. Reproductive Health Unit. 2009:135–150. | ||
Malawi Ministry of Health. VIA Programme Report June 2011; Lilongwe, Malawi. 2011. | ||
Sorensen G, Emmons K, Hunt MK, et al. Model for incorporating social context in health behavior interventions: applications for cancer prevention for working-class, multiethnic populations. Prev Med. 2003;37(3):188–197. | ||
Flynn TN, Louviere JJ, Peters TJ, Coast J. Best-worst scaling: what it can do for health care research and how to do it. J Health Econ. 2007;26(1):171–189. | ||
Marley A, Pihlens D. Models of best-worst choice and ranking among multiattribute options (profiles). J Math Psychol. 2012;56(1):24–34. | ||
Flynn TN. Valuing citizen and patient preferences in health: recent developments in three types of best-worst scaling. Expert Rev Pharmacoecon Outcomes Res. 2010;10(3):259–267. | ||
Willis GB, Caspar R, Lessler J. Cognitive interviewing: a “how to” guide. Paper Presented at: Short Course Presented at the Meeting of the American Statistical Association; 1999. | ||
Liang W, Lawrence WF, Burnett CB, et al. Acceptability of diagnostic tests for breast cancer. Breast Cancer Res Treat. 2003;79(2):199–206. | ||
Gerard K, Shanahan M, Louviere J. Using stated preference discrete choice modelling to inform health care decision-making: a pilot study of breast screening participation. Appl Econ. 2003;35(9):1073–1085. | ||
Gyrd-Hansen D. Cost-benefit analysis of mammography screening in Denmark based on discrete ranking data. Int J Technol Assess Health Care. 2000;16(03):811–821. | ||
Gyrd-Hansen D, Søgaard J. Analysing public preferences for cancer screening programmes. Health Econ. 2001;10(7):617–634. | ||
Linsell L, Forbes LJ, Patnick J, Wardle J, Austoker J, Ramirez AJ. Women’s preferences for the delivery of the National Health Service Breast Screening Programme: a cross-sectional survey. J Med Screen. 2010;17(4):176–180. | ||
Gupta S, Vij A, Cafiero E, et al. Retail venue based screening mammography: assessment of women’s preferences. Acad Radiol. 2012;19(10):1268–1272. | ||
Marcus EN, Drummond D, Dietz N. Urban women’s preferences for learning of their mammogram result: a qualitative study. J Cancer Educ. 2012;27(1):156–164. | ||
Bech M, Sørensen J, Lauridsen J. Eliciting women’s preferences for a training program in breast self-examination: a conjoint ranking experiment. Value Health. 2005;8(4):479–487. | ||
Hanson K, McPake B, Nakamba P, Archard L. Preferences for hospital quality in Zambia: results from a discrete choice experiment. Health Econ. 2005;14(7):687–701. | ||
Kruk ME, Paczkowski M, Mbaruku G, de Pinho H, Galea S. Women’s preferences for place of delivery in rural Tanzania: a population-based discrete choice experiment. Am J Public Health. 2009;99(9):1666–1672. | ||
Kruk ME, Paczkowski MM, Tegegn A, et al. Women’s preferences for obstetric care in rural ethiopia: a population-based discrete choice experiment in a region with low rates of facility delivery. J Epidemiol Community Health. 2010;64(11):984–988. | ||
Christofides NJ, Muirhead D, Jewkes RK, Penn-Kekana L, Conco D. Women’s experiences of and preferences for services after rape in South Africa: interview study. BMJ. 2006;332(7535):209–213. | ||
Mariani-Costantini R. Diagnosis: breast cancer screening in rural African communities. Nat Rev Clin Oncol. 2013;10(4):185–186. | ||
Abuidris DO, Elsheikh A, Ali M, et al. Breast-cancer screening with trained volunteers in a rural area of Sudan: a pilot study. Lancet Oncol. 2013;14(4):363–370. | ||
Anderson BO. Understanding social obstacles to early breast cancer detection is critical to improving breast cancer outcome in low- and middle-resource countries. Cancer. 2010;116(19):4436–4439. | ||
Maree J, Lu X, Wright S. Combining breast and cervical screening in an attempt to increase cervical screening uptake. An intervention study in a South African context. Eur J Cancer Care. 2012;21(1):78–86. | ||
Tum SJ, Maree JE, Clarke M. Creating awareness and facilitating cervical and breast cancer screening uptake through the use of a community health worker: a pilot intervention study. Eur J Cancer Care. 2013;22(1):107–116. | ||
Whitty JA, Walker R, Golenko X, Ratcliffe J. A think aloud study comparing the validity and acceptability of discrete choice and best worst scaling methods. PLoS One. 2014;9(4):e90635. | ||
UNICEF. Malawi Country Statistics; 2014. Available from: http://www.unicef.org/infobycountry/malawi_statistics.html. Accessed March 2014. | ||
Chamot E, Mulambia C, Kapambwe S, et al. Preference for human papillomavirus-based cervical cancer screening: results of a choice-based conjoint study in Zambia. J Low Genit Tract Dis. 2014;19(2):119–123. | ||
Ostermann J, Njau B, Brown DS, Mühlbacher A, Thielman N. Heterogeneous HIV testing preferences in an urban setting in Tanzania: results from a discrete choice experiment. PLoS One. 2014;9(3):e92100. | ||
Abiiro GA, Torbica A, Kwalamasa K, De Allegri M. Eliciting community preferences for complementary micro health insurance: a discrete choice experiment in rural Malawi. Soc Sci Med. 1982;2014(120):160–168. | ||
Michaels-Igbokwe C, Lagarde M, Cairns J, Terris-Prestholt F. Using decision mapping to inform the development of a stated choice survey to elicit youth preferences for sexual and reproductive health and HIV services in rural Malawi. Soc Sci Med. 2014;105(0):93–102. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.