Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Determining the Feasibility of a Mail-In Saliva Sample Protocol for Persons Living with HIV in Two Urban Northeast United States Clinics
Authors Mara MD ![]() , Miguel C, Lin NH, Beckwith CG, Henshaw M
, Miguel C, Lin NH, Beckwith CG, Henshaw M
Received 24 August 2024
Accepted for publication 18 April 2025
Published 2 October 2025 Volume 2025:17 Pages 337—349
DOI https://doi.org/10.2147/HIV.S492850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Matthew D Mara,1,2 Cynthia Miguel,3 Nina H Lin,4 Curt G Beckwith,5 Michelle Henshaw2,6
1General Dentistry, Boston University Henry M. Goldman School of Dental Medicine, Boston, MA, USA; 2Office of Global and Population Health, Boston, Massachusetts, University Henry M. Goldman School of Dental Medicine, Boston, MA, USA; 3Social Determinants of Health Analytics, Highmark Health, Pittsburgh, PA, USA; 4Division of Infectious Diseases, Department of Medicine, Boston University School of Medicine, Boston, MA, USA; 5Division of Infectious Diseases, Department of Medicine, Alpert Medical School of Brown University, Providence, Rhode Island, USA; 6Health Policy and Health Services Research, Boston University Henry M. Goldman School of Dental Medicine, Boston, MA, USA
Correspondence: Matthew D Mara, General Dentistry, Boston University, 560 Harrison Ave, Third Floor, Boston, MA, 02118, USA, Email [email protected]
Abstract:
Background: Mail-in saliva samples are a participant-centered means of monitoring patients’ oral and overall health that may help to reduce unnecessary medical trips and more efficiently use provider time. The use and acceptability of mail-in saliva samples have been studied in high-risk populations; however, it has not been studied in cohorts of people living with HIV (PLWH).
Objective: To investigate the feasibility of PLWHs’ willingness to provide mail-in saliva samples, 900 saliva collection kits were mailed to a randomized sample of PLWH across two urban and diverse clinics in the Northeast United States in 2019– 2020.
Results: 73/900 (8%) packages were returned to study personnel, with 100% (73/73) containing saliva deemed usable for analysis. 55/900 (6%) of packages were returned to the study team undeliverable. Further information may be gained from investigating the influence of personalized test results, health literacy, the requirement of the oral health survey, and study compensation that may affect an individual’s motivation to participate in the study.
Conclusion: While findings suggest limited feasibility of mail-in saliva collection without personalized test results in a cohort of PLWH in terms of response rate, all returned saliva samples were usable for analysis suggesting that addressing potential barriers may improve response rates and the feasibility of using mail-in salivary diagnostics to monitor disease progression in PLWH in future studies.
Keywords: respondent driven sampling, adherence interventions, saliva diagnostics, remote collection, disease monitoring
Saliva is an increasingly crucial diagnostic fluid as it is known to contain molecules enriched from an individual’s blood that mirror the body’s overall health.1 The benefits of salivary diagnostics include its non-invasive nature, low risk of adverse effects, and ease of collection.2,3 The simplicity of collecting saliva samples makes it possible to utilize collection protocols in various settings, employing non-health professionals and/or self-administration in collection procedures. Additionally, the literature suggests that saliva sample collection is successful in diverse communities when culturally relevant and patient-centered approaches are considered in recruitment.3
The use of saliva for diagnostic tests has made it possible to diagnose, monitor, and even help predict disease progression over time.4,5 Testing saliva affords the ability to assess the prevalence of microbes, chemicals, and immunologic markers, showing promise in detecting and monitoring diabetes, cardiovascular disease, viral infections, cancers, and oral and systemic diseases, such as Sjögren’s syndrome and periodontal disease.6 The use of salivary diagnostics may be especially useful for disease monitoring for patients living with HIV (Human Immunodeficiency Virus) who are more likely to experience comorbid chronic infections like periodontal disease, hypertension, and diabetes.7–9 Continued advances in proteomic technology may increase the accessibility and affordability of salivary diagnostics for disease detection and diagnosis.10,11
Remote or at-home saliva sampling has the potential to improve patient and research participant compliance, as patients reported that saliva collection was easy to do at home, more convenient, and preferred over blood and urine samples.12–14 Research participants in longitudinal cohorts have demonstrated the ability to collect, successfully package, and mail saliva samples to the lab, eliminating the need for in-person saliva collection. Studied cohorts included children and adults taking antiepileptic medication, women as part of a breast cancer screening program, and random samples of university faculty, students, and staff. Among participants, response rates ranged from 60% to 71%, and of those samples mailed, 93% were packaged correctly and usable for analysis in the study that reported this outcome.14–16 While research supports the feasibility of using the postal service for remote saliva collection and disease monitoring, there have been few studies that have used these procedures in underserved populations and no studies with people living with HIV (PLWH) who typically could benefit from more frequent monitoring of health.
Saliva collection may be particularly beneficial for diagnosing and monitoring disease progression in a population of PLWH. Comorbidity is more common and occurs earlier in PLWH compared to individuals without HIV, necessitating more frequent medical visits for monitoring and screening.4 Saliva is rich in proteomic and metabolic biomarkers that have been shown to assist in diagnosing and monitoring inflammation, cancers, an individual’s response to medication, and indicators of behavioral traits such as addiction, impulsivity, and aggression.17 Therefore, PLWH may benefit from monitoring saliva to assess HIV-medication-associated risk factors such as ART (Antiretroviral therapy) toxicities and an increased cancer risk due to CMV (Cytomegalovirus) reactivation, on top of traditional health concerns such as obesity, smoking, and diabetes that increase the likelihood of comorbidity of health conditions such as cardiovascular disease and elevate risk of heart attack and stroke.18 Thus, establishing a remote saliva collection protocol for PLWH could be a low-cost, accessible, and patient-centered means of disease monitoring for this population.
Mail-in saliva samples may benefit PLWH, given the potential to increase access to health professionals, given many experience barriers to in-person medical and dental visits. A 2019 report from the CDC suggests that as few as 50% of the 1.2 million PLWH in the United States were retained in care after diagnosis.19 Factors associated with decreased retention in medical care for PLWH include (1) individuals’ acceptance of their HIV status, (2) coping ability with concurrent mental illness, substance use, and HIV-related stigma, (3) familiarity with their healthcare providers, (4) lack of support systems, (5) logistical barriers to care, including poor access to medical providers.20,21 Retention metrics are often calculated by in-person patient interactions (ie, missed visits, appointment adherence, visit consistency, and gaps in care). This suggests that mail-in health monitoring programs may improve communication, patient engagement, and adherence to medical and dental visits.22,23
This study aimed to assess the feasibility of a mail-in saliva sample protocol in two unique urban infectious disease clinics, testing the hypothesis that PLWH are able to return mail-in saliva samples at a rate of 60–71% of other populations cited in the literature.
Description of Cohorts
We recruited participants from two independent HIV infectious disease outpatient clinics associated with the Providence-Boston Center for AIDS Research (CFAR): the Center of Infectious Diseases (CID) of Boston Medical Center in Boston, MA, and the Immunology Center (IC) of The Miriam Hospital in Providence, RI.
Center for Infectious Diseases
Center for Infectious Diseases (CID) is the outpatient HIV and infectious disease clinic at Boston Medical Center and part of the Boston University School of Medicine. It is the largest safety-net hospital clinic in the Boston area and serves a diverse patient population. CID provides care for one of the largest HIV/HCV coinfection populations in the state, foreign-born patients and minority patients. It also provides care for a large proportion of HIV serodiscordant couples and offers pre-exposure prophylaxis (PrEP) and individuals with active or a history of intravenous drug use (IVDU) and /or alcohol or substance use disorders.
Immunology Center
The Immunology Center (IC) of The Miriam Hospital, located in Providence, Rhode Island, is a Ryan White HIV/AIDS-funded center that provides comprehensive care for PLWH. The IC provides care to over 80% of PLWH in Rhode Island. The IC provides primary care in a “medical home” model, which includes comprehensive HIV and primary care. The IC provides screening and treatment for sexually transmitted infections and substance use disorders and provides mental health and social services on site.
Table 1 provides descriptive characteristics of the CID and IC clinic populations.
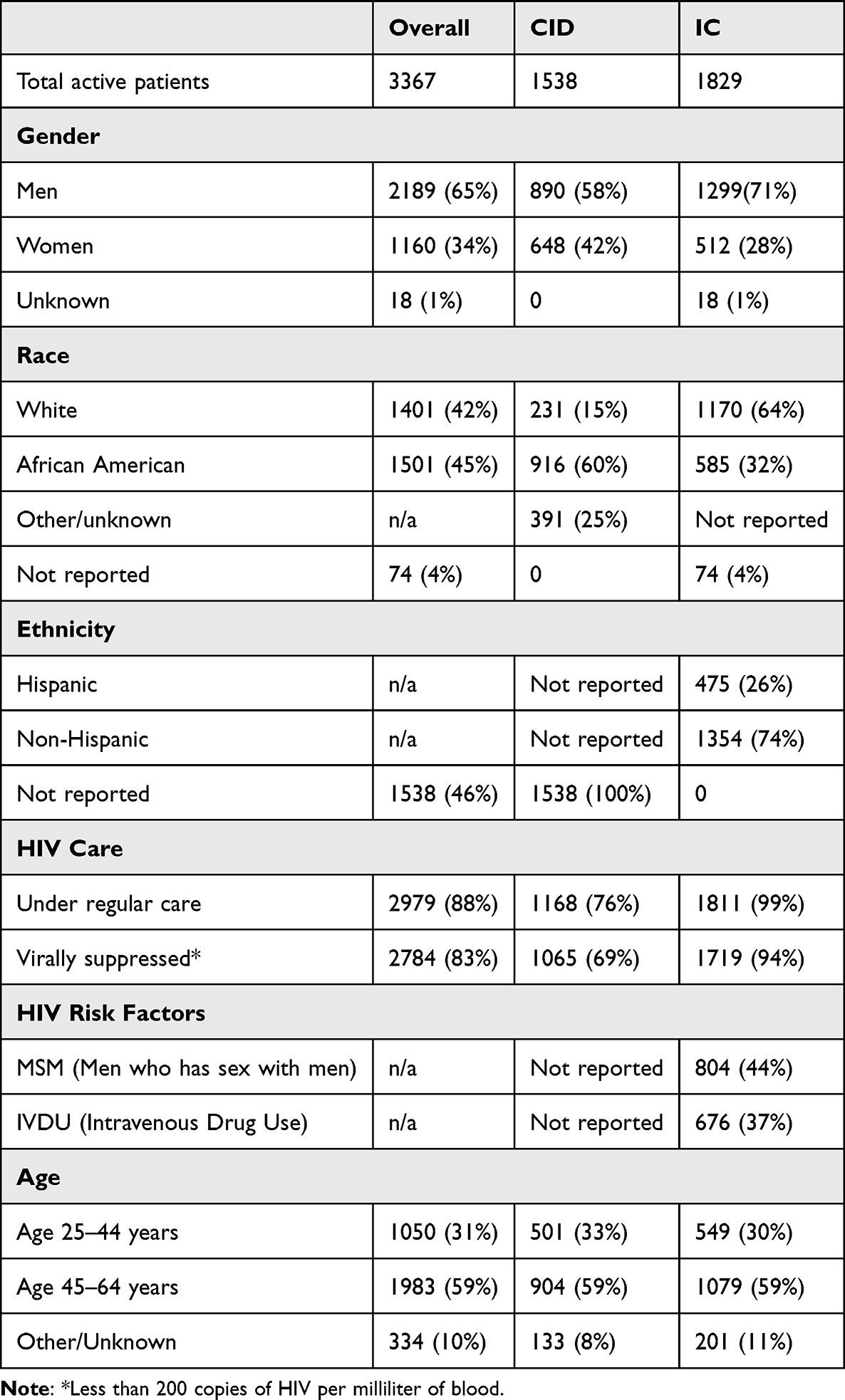 |
Table 1 Description of CID and IC Cohorts |
Methods
A cross-sectional study design was employed with the CID and IC clinic populations to better understand the feasibility of a mail-in saliva collection protocol for persons living with HIV. Cross-sectional study designs are commonly used to test feasibility for several factors including 1) time and resource efficiency, 2) elicit feedback on initial assessment implementation of an intervention, 3) assess participant acceptability and 4) provide preliminary data collection and proof of concept.24
The representative sample size (n=900), 30% of total population of CID and IC active patients, was randomly selected from each clinics’ database of active patients (CID = 1538, IC = 1829), using a simple randomization scheme. Based on response rates noted in literature of mail-in saliva samples in other cohorts, an estimated response rate of 55% was utilized to support a predicted confidence level of 99%.14–16
To ensure ethical conduct in medical research involving human subjects, this study adheres to the principles outlined in the Declaration of Helsinki and was exempt from full board review as determined by the institutional review boards at Boston University/Boston University Medical Center (H-37866). This study utilized a waiver of documentation of consent. Participant privacy and confidentiality was protected throughout the study design as all data collected were anonymous. Additionally, included as our data management plan prior to mailing the packages, a single research assistant was trained on how packages were processed, and saliva samples were stored. The following quality systems were in place throughout the duration of the study 1) all packages were returned to the same location, 2) the same research assistant processed all packages using standardized, objective criteria, 3) samples were stored using standardized labels, 4) surveys were stored in locked cabinets, and 5) outlier data were checked against written survey to ensure accurate data entry.
Saliva Collection Kit Description
A total of 900 (n=480 CID and n=420 IC) packages were pre-sealed and assembled for a random sample mailing to CID and IC patients. The mailing of packages was completed in phases; CID packages were mailed in September 2019, and IC packages were mailed in January 2020. Packages were mailed in Tyvek envelopes with return labels addressed to the CID or IC, respectively. Due to complexities in the mailing process, instructions did not include a desired return date or timeline for participants.
Packages included (1) a cover letter introducing the study and providing study contact information signed by a provider from their respective clinic, (2) a one-page study fact sheet, (3) a consent form (which included a waiver of signed documentation of consent), (4) a saliva collection protocol compete with figures and pictures to aid with saliva collection, (5) a 9-page oral health self-report instrument (which included basic self-report demographic questions), (6) directions for how to access an Amazon gift card, (7) a 50mL screw-top test tube for saliva collection, (8) liquid absorbent material, (9) packing material, (10) an itemized packing list, (11) a sealable biohazard bag, (12) a small sealable biohazard envelope, and (13) a UN3373 biological substance category B folded cardboard box with pre-applied business reply label. In each saliva sample kit, documents were labeled with a unique study ID and sealed. The saliva sample return kit included the following items to comply with UN3373 requirements: (1) a rigid cardboard box adequately labeled, (2) an itemized packing list, (3) absorbent material, (4) protective packing material, and (5) two impermeable packing layers (sealable biohazard bag and small sealable envelope).
Saliva samples from this study were determined to be potentially infectious materials by the Boston University Environmental Health and Safety Office. While it is known that HIV is not transmissible in saliva, it is possible that samples may include blood or other potentially infectious bodily materials.25 Even though other well-known mail-in saliva sample kits do not follow mailing requirements of potentially infectious materials, in the context of a clinical research study, the Boston University Environmental Health and Safety Office required saliva samples to be returned using the UN3373 biological substances category B shipping requirements because the saliva samples were coming exclusively from a cohort of PLWH. UN3373 requires triple packaging to prevent exposure of biological materials during mailing.26
In addition to the items listed above, CID individuals received consent to participate in an optional dental screening and a consent to contact form. If interested, CID-based individuals could complete the form providing their name and preferred contact method for scheduling a dental screening.
Selection Process
Each clinical research team from the two sites determined the total number of patients of record that met eligibility criteria. For the CID, eligibility criteria included (1) being a patient of record at CID clinic, (2) seen in the clinic for HIV care within the last 18 months, and (3) English listed as their preferred language. Exclusion criteria included incarcerated individuals and individuals listed as receiving no mail contact. For the IC, the same inclusion criteria were used; however, additional exclusion criteria were considered: (1) individuals who listed their address as confidential and (2) if at the same address, more than one individual was eligible; only the first name on the list was considered eligible, and all additional individuals were excluded.
The study team prepared a random list of numbers to select individuals for participation from the master list of numbered eligible clinic patients. Sealed packages ready to be addressed to participants were delivered to the CID and IC, where mailing labels were prepared. All packages were mailed directly from the clinics. No identifiable information was shared with the study team.
Participant Instructions
If an individual was not interested in participating, they were instructed to discard the entire package. Individuals who wished to participate were instructed to review the consent document, complete the oral health self-report survey, collect the saliva sample, and package the materials as directed on the instruction sheet. CID participants could also review an additional consent form for a dental screening and complete a contact sheet if they wished to participate. Once completed, participants were instructed to package the self-report survey, saliva sample, and contact sheet in the provided return package and mail the package to the study team.
Package Receipt, Processing, and Participant Remuneration
Once received, packages from both the CID and IC were opened under a negative pressure fume hood in accordance with specific laboratory procedures approved by the Boston University Institutional Biosafety Committee. One research assistant opened all packages, recorded study IDs, assessed adherence to packing instructions, and stored all saliva samples in a −80° Celsius freezer. Returned saliva samples were analyzed for usability based on the quantity of saliva in the enclosed tube. Saliva samples were considered usable if the sample had a minimum visible amount of saliva, a quantity large enough for most standard laboratory tests.
Participants were instructed to call the study phone number seven business days after they mailed their packages to ensure the study site received the sample. At this call, they are asked to provide their study ID, which the research assistant matched with a received sample to allow for study compensation. Participants received a twenty-five-dollar Amazon gift card for the return of the saliva sample and oral health survey. The Amazon gift card instruction sheet allowed participants to write down the electronic gift card code. Participants were not required to provide contact information (name, phone number, or email) to receive the Amazon gift card code. Amazon gift cards were selected for study remuneration as they allowed members of the research team to share access codes and ensure values were added to accounts over the phone without the collection of participant names or contact information.
Results
A total of 73 individuals (n=30 from the CID and n=43 from the IC) of the 480 packages sent from the CID and 420 packages sent from the IC responded to the mailing, with response rates of 6.25% and 10%, respectively, over a six-month period. Figure 1 depicts participation across the CID and IC cohorts.
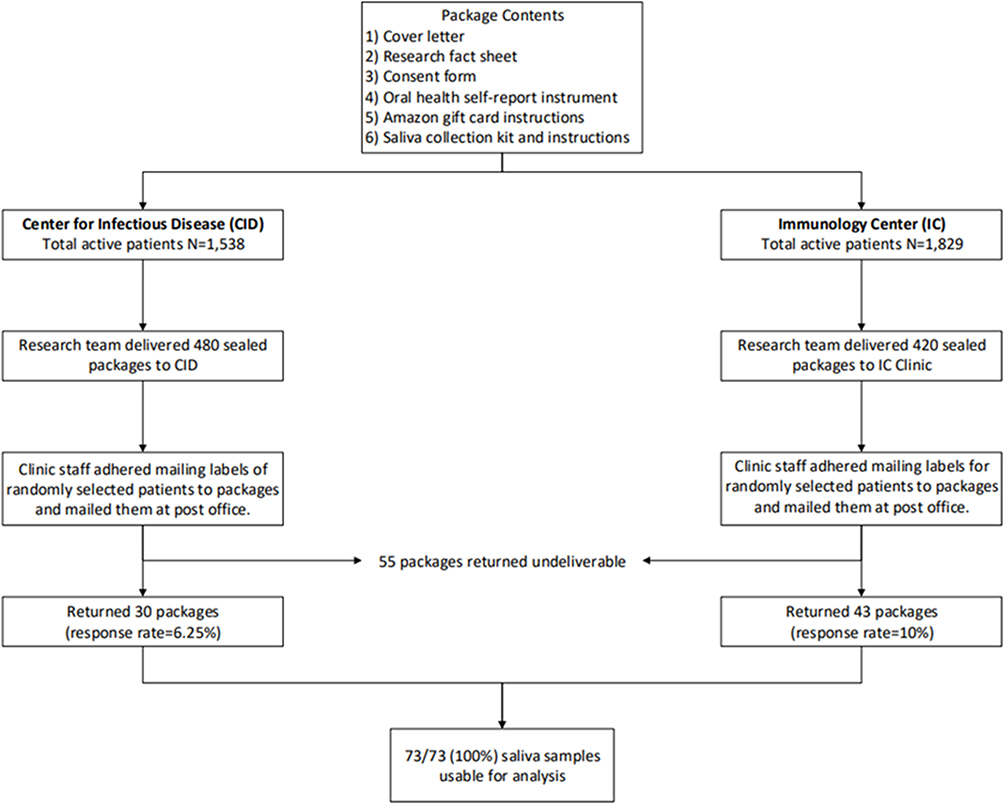 |
Figure 1 Study flowchart. |
A total of 55/900 (6%) packages were returned to the CID or IC indicated by the postal services as “undeliverable”. Over the six months, the study was open, 114 unique study contacts commonly addressed questions about receiving study compensation, and an additional 15 unique study contacts were logged where the research team described the saliva collection process to a prospective participant over the phone. One package from the CID cohort was returned taped flat with a note from the participant stating they did not want to participate and were excluded from the analysis. One mailing returned included an additional sample marked “urine”, while two respondents included additional packing material to protect their saliva sample further. While most packages from both the CID and IC were returned within two months of the postmark date, one package was returned six months after initial mailings.
Table 2 provides demographic information from individuals who returned the saliva sample collection kit. The study population was similar in most characteristics to the general patient population of the CID and IC clinic patients; however, in general the study population had a more significant proportion of black individuals (12/73, 16%) and a lower proportion of white participants (1/73, 1%) than the clinic cohorts. It is also noted that most respondents identified as males (41/73, 56%) and were over the age of 45 (51/73, 70%).
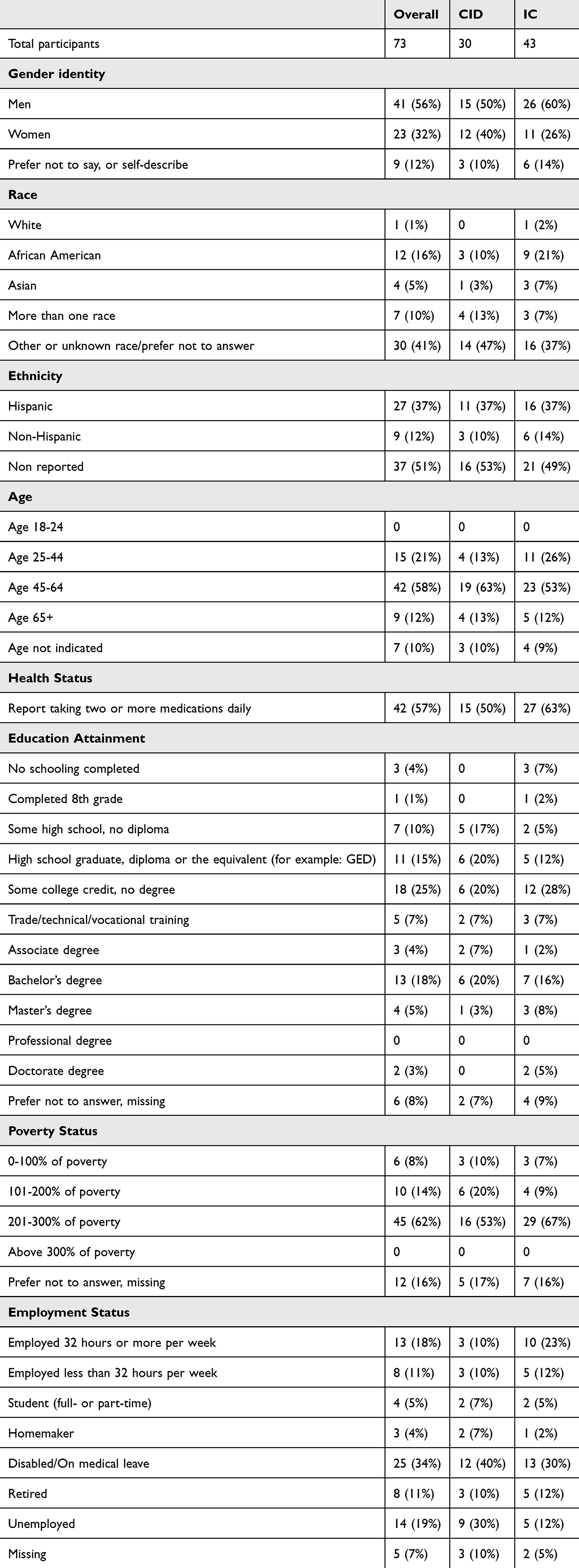 |
Table 2 Demographic Features of Individuals Who Returned the Outreach Mailing |
Table 3 summarizes the mailing results, indicating the percentage of individuals who called to claim study compensation (56/73, 77%) and those who returned saliva samples but failed to return the oral health survey (6/73, 8%). Between the two cohorts, response rates of returned packages were similar, 6% CID and 10% ID, with a similar number of packages returned as undeliverable, CID 7% and ID 5%.
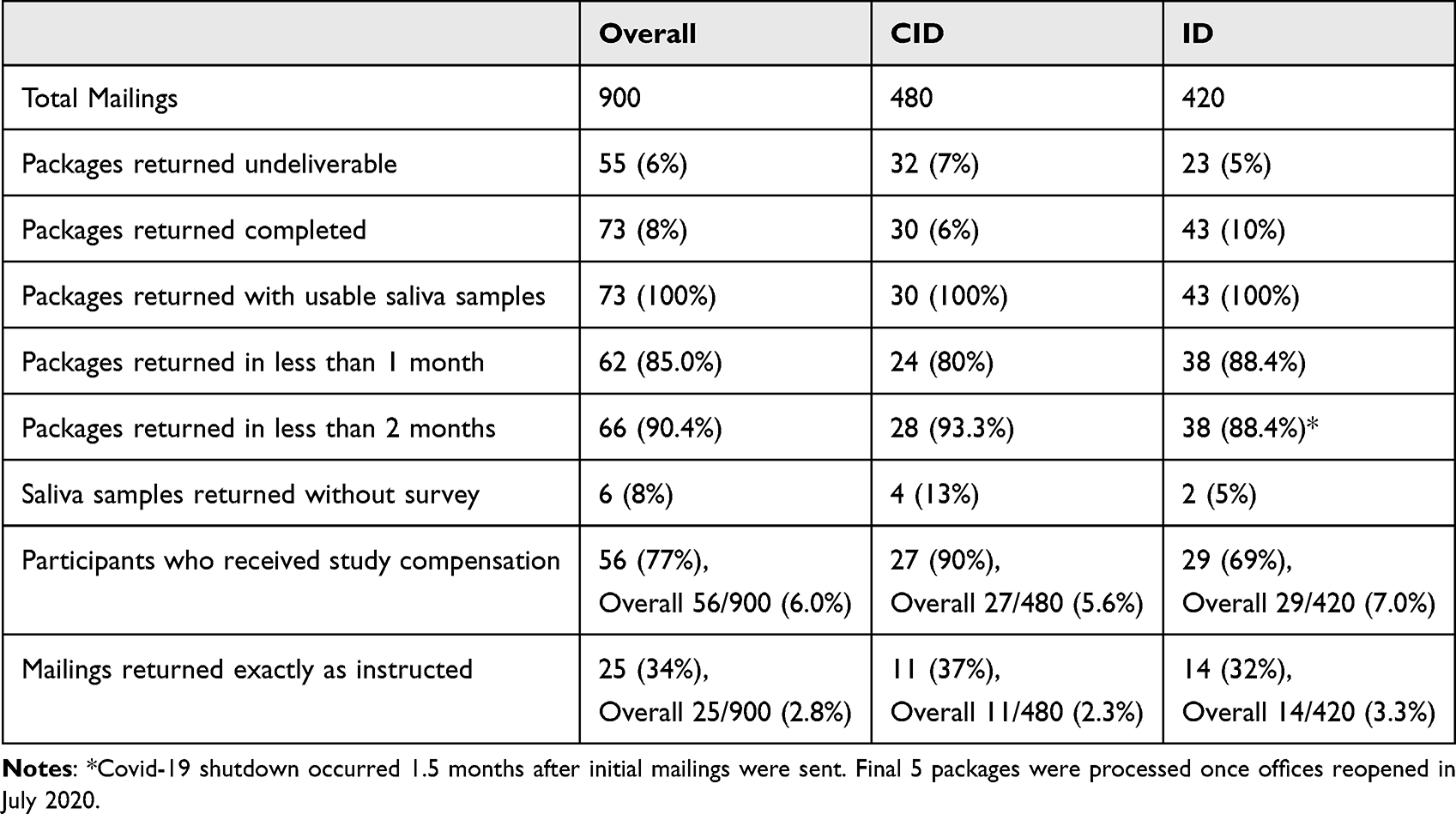 |
Table 3 Results From Mailing |
Discussion
The 8% overall response rate suggests that mail-in saliva collection has limited feasibility in this cohort of PLWH. Findings suggest that age of respondents is representative of the overall combined clinic population; however, racial and ethnic differences between respondents and the overall clinical population were noted. For example, a higher percentage of responses were expected from non-Hispanic as compared to Hispanic individuals from the IC cohort based on available clinic level data. Additionally, results significantly differ from the 60–71% response rates documented in other populations.14–16 However, this conclusion must be interpreted cautiously. The inclusion of a saliva sample is known to affect response rates from mail-in surveys negatively; there is little known about the converse, how the inclusion of a survey influences the response rate of saliva collection.15 The study design should have provided participants the option to return only the saliva sample, which could have influenced the response rate as compared to other studied cohorts. More information is needed in future studies to assess barriers related to the receipt of randomly sampled mailings, factors that influence response rate, and strategies to increase the acceptability and willingness of PLWH to return saliva samples in the future.
Receipt of Random Sampled Mailings
Elements fundamental to this study design (ie, randomization of mailing to recipients, individuals not knowing in advance that they would be receiving the package, and a signed cover letter from a clinic provider who may not be a recipient’s primary infectious disease provider) may prevent the complete assessment of the cohorts’ willingness to return mail-in saliva samples as the total number of packages received by intended recipients was unknown. While only 55 (6%) of the total packages were returned to the CID or IC as undeliverable, it is uncertain that the remaining packages were delivered to their intended recipients. Known factors, such as transience among PLWH, may have strongly influenced response rates beyond hesitancy of contributing a mail-in saliva sample.27 Our study design could not control for transience as no direct contact was made between the research team and eligible participants. Our results highlight the importance of accounting for some proportion of undelivered packages when calculating sample sizes in future studies.
Challenges with Mail-in Saliva Samples
All returned packages included saliva samples that were considered usable for analysis. This suggests that all individuals who opted to respond were able to collect a usable amount of saliva. Additionally, most salvia samples (66%, 48/73) were packaged incorrectly. The most common mistakes in returning the saliva sample include less than-ideal saliva quantity (still considered usable), inversion of the order of non-penetrable layers placed with the return shipment, and unsealed plastic bags and envelopes. This suggests that further detail and guidance beyond a picture-based packing instruction sheet are needed to help individuals in this cohort correctly package and mail in their saliva samples. Preparing UN3373 specimens is a multi-step process and often requires training to package correctly.28 In future studies, it may be beneficial to provide participants with additional resources, such as access to an online video, to assist in correctly packaging the samples.
Additionally, PLWH may have more trouble preparing sufficient saliva samples. PLWH are known to experience xerostomia (dry mouth), which makes it harder to prepare saliva samples if their immune response is compromised.29 Additionally, polypharmacy is a known risk factor for xerostomia, and PLWH is known to have a higher prevalence of polypharmacy as compared to the general population.30,31 Over half of the study respondents indicated taking more than two or more medications daily, suggesting polypharmacy-induced xerostomia is possible within the study cohort and could be a factor influencing a respondent’s decision not to participate in the study.
Reluctance/Hesitance to Participate
Other potential factors contribute to hesitancy or reluctance to participate in a saliva-based study. It is crucial to consider the role of study compensation in an individual’s willingness to participate in research. While study compensation for participant samples of biological materials, such as saliva, is widely used, more information should be available regarding the type and amount of compensation. Individuals who completed the mail-in saliva sample and survey were eligible to receive a $25 Amazon gift card, which may have needed adequate compensation for the time respondents needed to complete the survey.
Another factor that may have influenced individuals’ reluctance or hesitance to participate in the study is the multiple pages of reading materials, as literacy may be a factor preventing participation. The aim of the study and all study materials made it necessary for individuals to return both the survey and saliva samples, and the response rate may have been higher if respondents had the choice to complete one or both of the study elements. As a result, it is unclear if recipients would have been more likely to participate if they had the option of only submitting the saliva sample.
The complexity of the study design may have been a barrier to participation. PLWH has varying levels of health literacy, which may be influenced by other factors such as age, racial disparities, and viral suppression, affecting the individual’s ability to understand this study’s rationale or importance and respond promptly.32 Fifteen participants called study personnel for help with packaging the saliva sample. One participant from the CID cohort called study personnel to help read some study questions. This suggests that the literacy of study materials should be carefully considered.
Lastly, general reluctance to participate in research projects among PLWH is a likely factor. PLWH may be more reluctant to participate in research that does not directly benefit them and is for the “sake of science” compared to the general population due to a distrust in research and recruitment activities in their community.33 While response rates are low when participating in a research study, it is possible that individuals would be more likely to respond if there was information yielded that benefited or was related to their personal health. For example, over 26 million people have taken an at-home ancestry test, most of which utilize a saliva collection protocol, suggesting that individuals are motivated to complete a saliva sample when results are personal.34 Therefore, it is possible that with clinical applications of the mail-in saliva sample, participants would have more of a vested interest in completing the mail-in saliva sample as it would provide specific personal information and potentially prevent a medical office visit.
Study Strengths
Despite the limited results, future research may look to utilize elements of the study methodology and research design to anonymously sample and remunerate research participants. For example, the research protocol directed participants to call a member of the research team to share their participant ID and receive renumeration using an Amazon gift card code no sooner than seven business days from when the package was mailed. This protocol allowed participants to receive remuneration without the need to share their name or contact information. Additionally, the sampling protocol provided guidelines for researchers to anonymously and randomly select participants. This may be beneficial for future studies, particularly for researchers seeking to recruit participants based on a specific element of their health status.
Additionally, it may be important to note that the study was conducted prior to the COVID-19 pandemic. We believe this is important as use of telemedicine has increased dramatically as a direct result of the COVID-19 pandemic, especially in older adults with chronic health conditions.35 While it is impossible to assess, we postulate that the increase in telemedicine visits may have an impact on the overall feasibility of this study as personal experience with collecting samples as part of Covid-19 testing may affect respondents’ willingness to self-administer a saliva sample collection and mail it for analysis.
Study Limitations
As noted above, there were several limitations of the study that limit the generalizability of research findings: 1) participants were not informed they would receive the study mailing, 2) the oral health survey was required and participants were not offered to only return the saliva sample, 3) the complexity of the study design including reading materials which could have negatively impacted participation, 4) known reluctance of PLWH to participate in research studies, 5) potentially insufficient remuneration, and 6) lack of study follow-up to review individual results.
Additional limitations exist within the level of demographic data available at the clinic level. For example, both the CID and IC do not report key variables such as complete data on race and ethnicity, education level, and household income. Without clinic level data on these variables, it is unclear how specific factors such as ethnicity, educational attainment, and poverty status play a role in an individual’s willingness to collect and mail a saliva sample.
Future Directions
Next steps should focus on collection of qualitative data to better understand specific factors such as ethnicity, educational attainment, and poverty status that influence PLWH’s willingness to participate in mail-in studies. Findings from individual interviews and/or focus groups could provide further information on acceptability of the methods and compensation levels for participation, among other factors that may have influenced one’s decision not to participate. Future studies may also explore saliva sample return rates when the survey is excluded from the study mailing to determine if individuals are more willing to return a saliva sample when additional study documents or tasks are minimized.
Conclusion
The results of this study lead us to the conclusion that the current study design of randomly sampled mailing with a request to return a paired saliva sample and health survey with minimal remuneration had limited feasibility as a means of patient-centered monitoring of oral and other diseases in cohorts of PLWH. Additional studies are needed to identify facilitators and barriers to remote saliva collection and assessing dental health among PLWH. Despite the limitations of this study, future research may utilize components of the study methodologies, including randomly sampled mailing, anonymous delivery of study compensation, and saliva collection protocols.
Author Information
Matthew Mara is an Assistant Professor of General of General Dentistry at Boston University. Henry M. Goldman School of Dental Medicine (ORCiD: 0000-0001-6376-6394). Cynthia Miguel, MPH is a Senior Clinical and Population Health Data Analyst at Highhmark Health. Nina H. Lin, MD is an Assistant Professor of Medicine at Boston University School of Medicine (ORCiD: 0000-0002-4913-0442). Curt G. Beckwith is Professor of Medicine at the Alpert Medical School of Brown University (ORCiD: 0000-0002-8430-8111). Michelle Henshaw, DDS, MPH is a Professor of Health Policy and Health Services Research and Associate Dean of Global and Population Health at Boston University Henry M. Goldman School of Dental Medicine (ORCiD: 0000-0003-2586-8466).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
This work was facilitated by the Providence/Boston Center for AIDS Research (P30AI042853). We thank Kendrick Smaellie (Boston University Henry M. Goldman School of Dental Medicine) for administrative support and assistance logging saliva samples. Additionally, we would like to thank Dr. Bing Liu (Boston University Henry M. Goldman School of Dental Medicine) for advising saliva collection logistics. We thank Dena Kivett (Boston Medical Center) and Samantha Roche (Boston Medical Center) for logistical work identifying Boston-based individuals who met inclusion criteria. We thank Lauri Bazerman (Providence-Boston Center for AIDS Research/Miriam Hospital) for handling the logistics of Providence-based mailings.
Funding
This work was supported by the National Institutes of Health under Grant number P30AI042853.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pappa E, Vougas K, Zoidakis J, Vastardis H. Proteomic advances in salivary diagnostics. Biochimica Et Biophysica Acta. 1868;(11):140494. doi:10.1016/j.bbapap.2020.140494
2. Samaranayake L. Saliva as a diagnostic fluid. Int Dental J. 2007;57(5):295–299. doi:10.1111/j.1875-595x.2007.tb00135.x
3. Samayoa C, Santoyo‐Olsson J, Escalera C, et al. Participant-centered strategies for overcoming barriers to biospecimen collection among spanish-speaking Latina breast cancer survivors. Cancer Epidemiol Biomarkers Prev. 2020;29(3):606–615. doi:10.1158/1055-9965.epi-19-0942
4. Streckfus C, Bigler L. Saliva as a diagnostic fluid. Oral Dis. 2002;8(2):69–76. doi:10.1034/j.1601-0825.2002.1o834.x
5. Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics – current views and directions. Exp Biol Med. 2016;242(5):459–472. doi:10.1177/1535370216681550
6. Zhang C-Z, Cheng X-Q, Li J-Y, et al. Saliva in the diagnosis of diseases. Int J Oral Sci. 2016;8(3):133–137. doi:10.1038/ijos.2016.38
7. Maciel RA, Klück HM, Durand M, Sprinz E. Comorbidity is more common and occurs earlier in persons living with HIV than in HIV-uninfected matched controls, aged 50 years and older: a cross-sectional study. Inter J Infect Dis. 2018;70:30–35. doi:10.1016/j.ijid.2018.02.009
8. Ryder MI, Nittayananta W, Coogan M, Greenspan D, Greenspan JS. Periodontal disease in HIV/AIDS. Periodontology. 2000;60(1):78–97. doi:10.1111/j.1600-0757.2012.00445.x
9. Webel AR, Schexnayder J, Cioe PA, Zuñiga JA. A review of chronic comorbidities in adults living with HIV: state of the science. J Assoc Nurses AIDS Care. 2021;32(3):322–346. doi:10.1097/JNC.0000000000000240
10. Castagnola M, Scarano E, Passali GC, et al. Salivary biomarkers and proteomics: future diagnostic and clinical utilities. Acta Otorhinolaryngol Italica. 2017;37(2):94–101. doi:10.14639/0392-100X-15988
11. Liu J, Duan Y. Saliva: a potential media for disease diagnostics and monitoring. Oral Oncol. 2012;48(7):569–577. doi:10.1016/j.oraloncology.2012.01.021
12. Dhima M, Salinas TJ, Wermers RA, Weaver AL, Koka S. Preference changes of adult outpatients for giving saliva, urine and blood for clinical testing after actual sample collection. J Prosthodont Res. 2013;57(1):51–56. doi:10.1016/j.jpor.2012.09.004
13. Pittman TW, Decsi DB, Punyadeera C, Henry CS. Saliva-based microfluidic point-of-care diagnostic. Theranostics. 2023;13(3):1091–1108. doi:10.7150/thno.78872
14. Tennison M, Ali I, Miles MV, D’Cruz O, Vaughn B, Greenwood R. Feasibility and acceptance of salivary monitoring of antiepileptic drugs via the US postal service. Therapeutic Drug Monitoring. 2004;26(3):295–299. doi:10.1097/00007691-200406000-00013
15. Etter JF, Perneger TV, Ronchi A. Collecting saliva samples by mail. American J Epidemiol. 1998;147(2):141–146. doi:10.1093/oxfordjournals.aje.a009426
16. Sakhi AK, Bastani NE, Ellingjord-Dale M, Gundersen TE, Blomhoff R, Ursin G. Feasibility of self-sampled dried blood spot and saliva samples sent by mail in a population-based study. BMC Cancer. 2015;15(1). doi:10.1186/s12885-015-1275-0
17. Liao C, Chen X, Fu Y. Salivary analysis: an emerging paradigm for non‐invasive healthcare diagnosis and monitoring. Interdisciplinary Med. 2023;1(1). doi:10.1002/inmd.20230009
18. Martínez-Sanz J, Serrano-Villar S, Vivancos MJ, Rubio R, Moreno S. Management of comorbidities in treated HIV infection: a long way to go: HIV, comorbidities and aging. Int J Antimicrob Agents. 2022;59(1):106493. doi:10.1016/j.ijantimicag.2021.106493
19. Center for Disease Control. How Do I Keep Patients with HIV in Care?. Www.cdc.gov. Available from: https://www.cdc.gov/hiv/clinicians/treatment-care/retention.html.
20. Jaafari Z, McFarland W, Eybpoosh S, et al. Barriers and facilitators of access to HIV prevention, care, and treatment services among people living with HIV in Kerman, Iran: a qualitative study. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-08483-4
21. Rajabiun S, Mallinson RK, McCoy K, et al. “Getting me back on track”: the role of outreach interventions in engaging and retaining people living with HIV/AIDS in medical care. AIDS Patient Care STDs. 2007;21(s1):S–20–S–29. doi:10.1089/apc.2007.9990
22. Yehia BR, Fleishman JA, Metlay JP, et al. Comparing different measures of retention in outpatient HIV care. AIDS. 2012;26(9):1131–1139. doi:10.1097/qad.0b013e3283528afa
23. Hall HI, Gray KM, Tang T, Li J, Shouse L, Mermin J. Retention in care of adults and adolescents living with HIV in 13 US areas. J Acquir Immune Defic Syndr. 2012;60(1):77–82. doi:10.1097/QAI.0b013e318249fe90
24. Pearson N, Naylor PJ, Ashe MC, et al. Guidance for conducting feasibility and pilot studies for implementation trials. Pilot Feasibility Stud. 2020;167. doi:10.1186/s40814-020-00634-w
25. Baron S, Poast J, Cloyd MW. Why is HIV rarely transmitted by oral secretions? Archiv Internal Med. 1999;159(3):303. doi:10.1001/archinte.159.3.303
26. Daklapack. Category B. UN3373.com. Available from: https://www.un3373.com/category-biological-substances/category-b/#:~:text=Category%20B&text=Diagnostic%20specimens%2C%20assigned%20to%20UN.
27. Clemenzi-Allen A, Neuhaus J, Geng E, et al. Housing instability results in increased acute care utilization in an urban HIV clinic cohort. Open Forum Infect Dis. 2019;6(5). doi:10.1093/ofid/ofz148
28. Iwen PC, Stiles KL, Pentella MA. Safety considerations in the laboratory testing of specimens suspected or known to contain the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Am J Clin Pathol. 2020;153(5):567–570. doi:10.1093/ajcp/aqaa047
29. Ramírez-Amador V, Patton LL, Naglik JR, Nittayananta W. Innovations for prevention and care of oral candidiasis in HIV-infected individuals: are they available?-A workshop report. Oral Dis. 2020;26(Suppl. 1):91–102. doi:10.1111/odi.13391
30. Marcott S, Dewan K, Kwan M, Baik F, Lee Y, Sirjani D. Where dysphagia begins: polypharmacy and xerostomia. Fed Pract. 2020;37(5):234–241.
31. Okoli C, de Los Rios P, Eremin A, Brough G, Young B, Short D. Relationship between polypharmacy and quality of life among people in 24 countries living with HIV. Preventing Chronic Dis. 2020;17(E22). doi:10.5888/pcd17.190359
32. Rebeiro PF, McPherson TD, Goggins KM, et al. Health literacy and demographic disparities in HIV care continuum outcomes. AIDS Behav. 2018;22(8):2604–2614. doi:10.1007/s10461-018-2092-7
33. Hoffman KA, Baker R, Kunkel LE, et al. Barriers and facilitators to recruitment and enrollment of HIV-infected individuals with opioid use disorder in a clinical trial. BMC Health Serv Res. 2019;19(1). doi:10.1186/s12913-019-4721-x
34. Regalado A. More than 26 million people have taken an at-home ancestry test. MIT Technology Review. Available from: https://www.technologyreview.com/2019/02/11/103446/more-than-26-million-people-have-taken-an-at-home-ancestry-test/#:~:text=Although%2023andMe%20has%20not%20publicly.
35. Nittari G, Savva D, Tomassoni D, et al. Telemedicine in the COVID-19 era: a narrative review based on current evidence. Int J Environ Res Public Health. 2022;19(9):5101. doi:10.3390/ijerph19095101
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.