Back to Journals » Journal of Blood Medicine » Volume 15
Determine Complete Blood Count Reference Values Among Healthy Adult Populations
Authors Abbas AB ![]() , Aldomaini A, Al-Qadri AA, Algorbani Z, Aljamali S, Alsiri S, Alghorbani K, Abo Osba’a S
, Aldomaini A, Al-Qadri AA, Algorbani Z, Aljamali S, Alsiri S, Alghorbani K, Abo Osba’a S
Received 27 August 2024
Accepted for publication 13 December 2024
Published 19 December 2024 Volume 2024:15 Pages 513—522
DOI https://doi.org/10.2147/JBM.S488050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Abdul Baset Abbas, Abeer Aldomaini, Amah Alrahman Al-Qadri, Zahra’a Algorbani, Sara Aljamali, Safa Alsiri, Khadeeja Alghorbani, Saba Abo Osba’a
Medical Laboratories Department, Faculty of Medicine and Health Sciences, Ibb University, Ibb City, 70270, Yemen
Correspondence: Abdul Baset Abbas, Email [email protected]; [email protected]
Background: Complete blood counts (CBC) are commonly used in diagnostic medicine to evaluate normal and abnormal hematological status. Furthermore, reference values (RVs) of CBC supplied by researchers are the most reliable means of the judgment-making stage and can aid interpretation and accurate diagnosis of diseases. Reference values vary between peoples because of differences in lifestyle, dietary habits, ethnicity and environment. Moreover, the Clinical and International Standards Institute (CISI) advises determining the RVs for each area. There are no RVs for CBC in Yemen. Therefore, this study aimed to determine the common RVs of CBC for healthy adults in Ibb City in the middle of Yemen.
Methods: A cross-sectional study was conducted from April 1, to November 30, 2023. Of the 623 adults who participated in this study, 433 (aged 18– 80 years) were included in the final analysis after applying exclusion criteria. The mean, median, and 95th percentile RVs (2.5th-97.5th percentiles) were calculated for gender, age, and residence by the GraphPad Prism 8.0.1.
Results: The RVs of hemoglobin (Hb) 11.16– 17.54g/dl, red blood cells (RBC) 3.890– 6.340× 1012/l, hematocrit (HCT) 33.03– 49.30%), mean corpuscular volume (MCV) 72.83– 94.55fl), mean corpuscular hemoglobin (MCH) 23.95– 33.55pg, mean corpuscular hemoglobin concentration (MCHC) 32.97– 36.7354g/dl, platelet (PLT) count 140.0– 418.6× 109/l, total white blood cells (WBC) 2.810– 8.797 × 109/l and WBC differential count (basophils 0.000– 1.000%, neutrophils 30.10– 69.17%, eosinophils 1.500– 5.000%, lymphocytes 23.86– 63.45% and monocytes1.873– 5.600%). Significantly higher median values were observed in males compared to females for Hb (P< 0.0001), RBC (P< 0.0001), HCT (P< 0.0001), lymphocyte (P=0.0197) and monocytes (P=0.0009). Contrariwise, females demonstrated significantly higher neutrophils (P=0.0009), eosinophils (P=0.0020), basophils (P< 0.0001) and platelets (P=0.0324) than males. This study showed differences in the RVs of CBC compared to those reported in other countries in the Middle East, Asia, Africa, and Europe.
Conclusion: In this study, the reference values of CBC are considered as a benchmark that may assist in accurately judging laboratory results and enhancing medical and clinical services for adults in Ibb City, Yemen.
Keywords: reference values, RVs, adults, CBC, Ibb, Yemen
Introduction
Reference values (RVs) are the range of values between and involving lower and upper limits, which were derived from the study of a considerable number of healthy people, to which results can be compared to assist interpretation.1–4 These typically mean 95% of the results between 2.5th and 97.5th percentiles of the laboratory test values for reference people.1–3 These usually mean 95% of the results between 2.5th and 97.5th percentiles of the laboratory test values for reference people.5 Complete blood counts (CBC) are commonly used in diagnostic medicine to evaluate normal and abnormal hematological status.5,6 Moreover, the RVs of CBC parameters are affected by several factors such as lifestyle, dietary habits, ethnicity, environment, sex, age, pregnancy,3,7,8 exercise, stress, geography5,9,10 and environmental elements such as climate and altitude.11–14 Furthermore, RVs of CBC have not yet been determined in many developing countries, but depend on literature,15–18 textbook5,19–21 or brochures of the reagent kits1,3,22 which rely on specimens obtained from developed countries people.1,3,5,15–22 Additionally, several studies accomplished in African and Asian countries indicate distinctions in RVs compared to those determined in American and European countries.8,19,20,23–26 Likewise, other studies in the Middle East have informed discrepancies in RVs.2,15,27–29 Moreover, the Clinical and International Standards Institute (CISI) and the International Federation of Clinical Chemistry (IFCC) have advised establishing of RVs for each area.3,5,30 Moreover, disparities and variations of RVs in different countries cannot be used for the whole population, and there are no RVs for CBC in Yemen. Therefore, this study aimed to determine CBC RVs among adults in Ibb City, Yemen.
Material and Methods
Study Design, Period and Area
A cross-sectional study was conducted from April 1 to November 30, 2023. The study society is in Ibb City, approximately 193 km south of Sana’a. Ibb City at 13°58′N and 44°10′E with an altitude of 6,725 feet (2,050 meters) above sea level. CBC tests were carried out at the hematology department of Alpha Medical Laboratories.
Sample Size and Sampling Techniques
The subjects of this study were selected from healthy adults (volunteers) aged between 18 and 80 years. According to the Clinical and Laboratory Standards Institute (CLSI) recommendation, a minimum of 120 individuals are enough to determine reference values.31–33 To maximize the confidence, the investigators increased the number of participants to 623. Of the 623 adults selected randomly from the society of the study, 433 were elected, while 190 (30.50%) were excluded through a medical health questionnaire and physical examination by a physician during the recruitment process.
Exclusion criteria were consumption of any nutritional supplements (vitamins and minerals) or any medication, having a history of diseases (anemia, diabetes, liver disease, heart disease, kidney disease, high blood pressure, arthritis and thyroid disorders), fever, tonsillitis, appendicitis, allergies skin rash or receiving or donating blood within the past year. In case of females who were menstruating, pregnant or breastfeeding were excluded. Furthermore, of the 453 participants who consented to the study through a sampling technique, 20 were excluded based on serological test outcomes (hepatitis C virus (HCV) antibodies, hepatitis B surface antigen (HBsAg) and C-reactive protein (CRP) agglutination test level (≥6 mg/l). Of 433 participants were included in the final analysis after employing exclusion criteria for establishing RVs of CBC parameters for adults (253 males and 180 females) in Ibb City, in the middle of Yemen.
Sampling Methods and Analysis
The participants were interviewed using a standardized questionnaire. Data collected included socio-demographic and medical history information. Approximately 2.5 mL of blood was collected using an EDTA-K3 (Jiangsu Xinkang Medical Instrument Co., Ltd, China). Blood samples were sent to the laboratory and tested immediately for HCV antibodies, HbsAg, CRP and CBC. CBC was measured using a Mindray BC-5000 automatic hematology analyzer (Shenzhen Mindray Bio-Medical Co., Ltd., China). The CBC parameters include hemoglobin (Hb), red blood cells (RBC), white blood cells (WBC), hematocrit (HCT), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), platelet (PLT) count and WBC differential count (basophils, neutrophils, eosinophils, lymphocytes and monocytes).
Quality Assurance
The data quality was verified using a standard questionnaire designed in English with consistency and high accuracy and translated into Arabic (the country language). The questionnaire contents were collected from previous research to reduce errors and bias. Further, the research team trained before collecting data and sampling to minimize observer and technological bias. Mindray BC-5000 automatic hematology analyzer (Shenzhen Mindray Bio-Medical Co., Ltd., China) was calibrated according to the manufacturer’s guidelines. Mindray BC-5800 controls were conducted before and after testing the samples.
Statistical Analysis
The results of the laboratory tests and questionnaires were entered into a Microsoft Excel spreadsheet. Statistical analyses were achieved using GraphPad Prism 8.0.1 (GraphPad Inc. USA). Ringoringo et al reported flexibility in determining the RVs depending on the desire, either by calculating mean-2SD or determining the lower and upper limits at and between 2.5th-97.5th, 3rd-97th, or 5th-95th percentiles.34,35 On the other hand, Zeh et al, Fiseha et al and Fondoh et al used the mean, median and RVs percentiles.29,36,37 Accordingly the mean, median and nonparametric 95% RVs (2.5th and 97.5th percentiles) were calculated for CBC according to CLSI guidelines.32 The ROUT method (Q = 1%) was used to identify outliers. The normality of the results was determined using the Shapiro–Wilk, Anderson-Darling and Kolmogorov–Smirnov tests. Furthermore, descriptive statistics were used to calculate and compare means, medians and 2.5th-97.5th percentiles between each variable such as gender. The potential disparities in RVs were tested using the Mann–Whitney U-test. P values ≤0.05 were counted statistically significant.
Results
A total of 433 healthy adults (253 males and 180 females) were included in the analysis to establish the RVs of CBC for adults. As revealed in Table 1, the mean age and standard deviation of the participants were 29.72 ± 10.64 years, ranging from 18 to 80 years and the mean body weight and standard deviation were 58.04 ± 10.04 Kg. The majority of the participants (72.28%) were from urban communities.
 |
Table 1 Demographic Characteristics of Participants |
Table 2 presents the mean, median and 95% reference values (RVs) (2.5th −97.5th percentiles) of CBC parameters among healthy adults according to gender. The combined mean, median and RVs for both males and females were as follows: 14.33, 14.30 (11.16–17.54g/dl) for Hb, 4.835, 4.800 (3.890–6.340×1012/l) for RBC, 40.90, 40.80 (33.03–49.30%) HCT, 85.73, 86.20 (72.83–94.55fl) for MCV, 30.06, 30.40 (23.95–33.55pg) for MCH, 35.02, 35.10 (32.97–36.73 g/dl) for MCHC, 5.245, 5.100 (2.810–8.797×109/l) for WBC, 49.36, 48.95 (30.10–69.17%) for neutrophils, 43.31, 43.60 (23.86–63.45%), 3.453, 3,500 (1.500–5.0000%) for eosinophil, 3.931, 4.000 (1.873–5.600%) for monocyte, 0.335, 0.000 (0.000–1.000%) for basophil and 270.4, 269.0 (140–418.6×109/l) for platelets. Significantly higher median values were observed in males compared to females for Hb, RBC, HCT, lymphocytes and monocytes. Contrariwise, females demonstrated significantly higher neutrophils, eosinophils, basophils and platelets than males. Moreover, MCH and MCHC were statistically significant differences.
 |
Table 2 Mean, Median and 95% Reference Values (RVs) (2.5th −97.5th Percentiles) of CBC Parameters Among Healthy Adults According to Gender |
The combined mean, median and RVs of absolute neutrophils (2.643, 2.465 and 0.990–5.170×109/l), absolute lymphocytes (2.195, 2.165 and 23.86–63.45×109/l), absolute eosinophils (0.175, 0.1600 and 0.0460–0.384×109/l) absolute monocytes (0.217, 0.2000, and 0.077–0.433×109/l) and absolute basophils (0.017, 0.000 and 0.000–0.070×109/l). Absolute eosinophils and absolute basophils were statistically significant differences according to gender.
Discussion
RVs provide necessary data to help individual health evaluation.36 Moreover, RVs are affected by several factors.38,39 To the best of our knowledge, studies on CBC RVs in Yemen are nonexistent. RVs depend on the manufacturers’ guidelines and textbooks, which are often established by non-Yemeni populations. Thus, this study aimed to determine the RVs of CBC in Ibb City, Yemen.
Briefly, the RVs in this study for CBC were varied (more or less) in numbers, decimal numerals, or percentages from the reference values of other studies. The RVs of the CBC parameters may agree or disagree with RVs reported in other studies conducted in Saudi Arabia,5 Oman,28 Kuwait,30 Iraq,2 Morocco,3 Ethiopia,29 Iran,27 Pakistan,1 the United Kingdom (UK)40 and France41 as shown in Table 3.
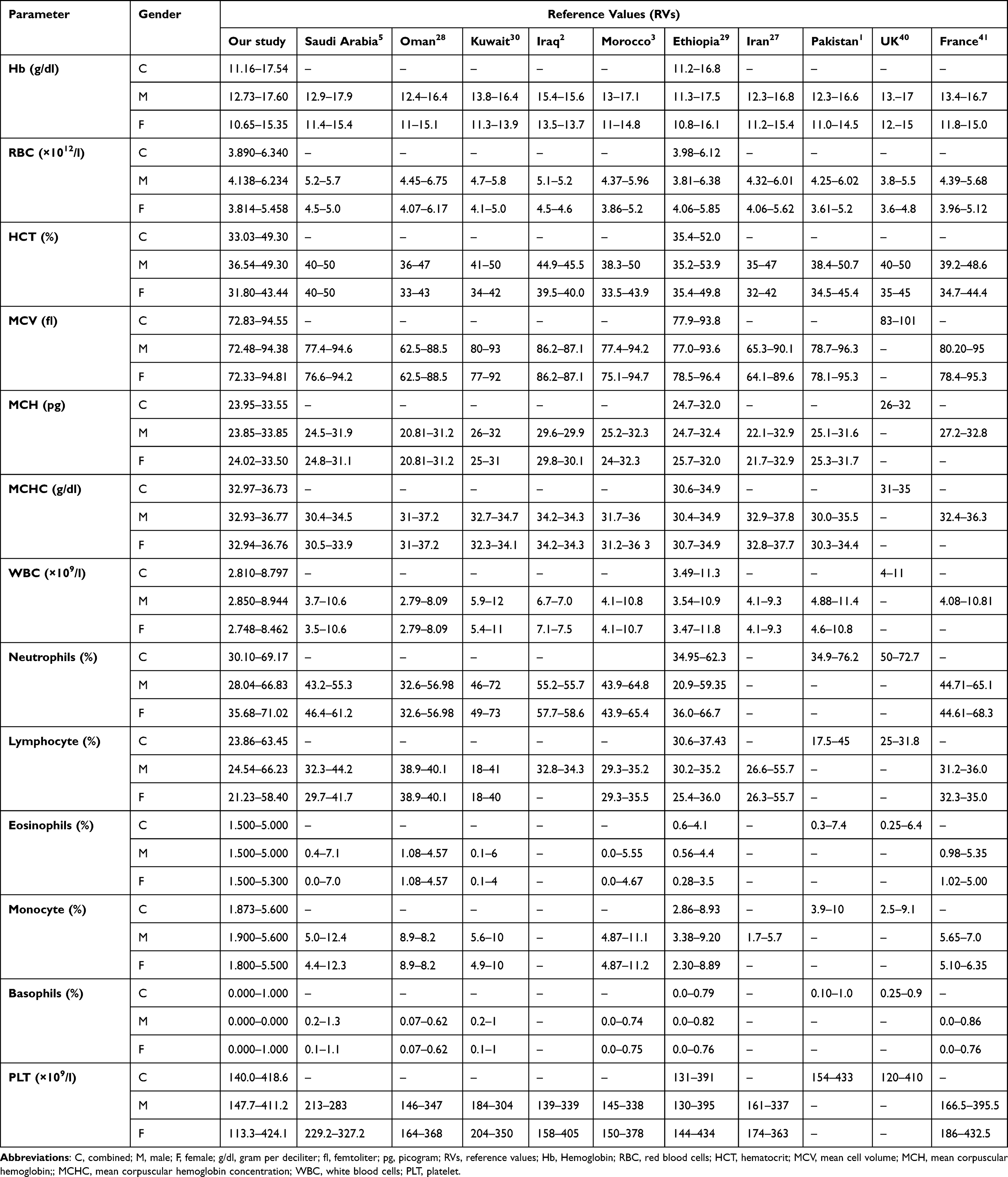 |
Table 3 The Comparison of Reference Values (RVs) Obtained in This Study with Studies in Different Countries |
In this study, males had higher Hb, RBC, HCT, lymphocytes and monocytes than females. These results are consistent with those reported in previous studies.1–3,5,27–30,40,41 This may be partly a result of the impact of loss of menstrual blood and androgen hormone on erythropoiesis.42–44 Moreover, the findings of females have higher levels of neutrophil, which are similar to studies in Saudi Arabia,5 Iraq,2 Ethiopia,29 and France.41 In addition, eosinophil percentage in females is higher than that in males, this report is different than studies in Saudi Arabia,5 Kuwait,30 Morocco3 and Ethiopia.29 Likewise, the basophil percentage in females is higher than that in males, which disagrees with studies done in Saudi Arabia,5 Kuwait,30 Ethiopia29 and France.41 It be related to geographic dissimilarities, ethnic background, sociodemographic disparities, social lifestyle and habits, dietary customs, ecological factors and laboratory diagnostic techniques.5,42,45
Our results showed that the RVs for MCV, MCH and MCHC were almost equal between males and females. These outcomes are consistent with studies accomplished in Saudi Arabia,5 Oman,28 Iraq2 and Pakistan.1 Additionally, the RV for PLT was higher in females compared to males as reported in Saudi Arabia.5 It is probably due to menarche through cross-motivating megakaryopoiesis.42,46 This study’s limitation is that the RVs of the CBC parameters in neonates and children are missing.
Conclusion
In conclusion, the RVs of CBC established in the current study are considered a benchmark that may assist in interpreting and accurately judging laboratory results for adults in Ibb City, Yemen. The results displayed significant differences between males and females in Hb, RBC, HCT, MCH, MCHC, neutrophils, lymphocytes, eosinophils, monocytes, basophils and platelets.
Abbreviations
C, combined; M, male; F, female; g/dl, gram per deciliter; fl, femtoliter; pg, picogram; RVs, reference values; Hb, Hemoglobin; RBC, red blood cells; HCT, hematocrit; MCV, mean cell volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; WBC, white blood cells; PLT, platelet.
Data Sharing Statement
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available because they contain information that can compromise the privacy of the research participants.
Ethical Considerations
The Medical Laboratories Department, Faculty of Medicine and Health Sciences, Ibb University Ethical Committee, granted ethical approval for this research after following due process (Reference No.: MDL-MHS-IBBU/IBA002/2023 dated February 6, 2023). The Research Ethics Committee complied with the Declaration of Helsinki for the Protection of Human Subjects. Participants were informed about the study and provided written informed consent.
Acknowledgments
We would like to express our deep gratitude to all of our colleagues in the Department of Medical Laboratories, Faculty of Medicine and Health Sciences, Ibb University, who participated in this study for their sincere cooperation. We thank Dr. Mohammed Musaad Al-Ahmadi, Dr. Talal Al-Hajami, Dr. Saddam Al-Joami and Dr. Majed Al-Joubhi at Alfa Medical Laboratories, and Dr. Hafed Nomman AL-Fahd at Al-Rafah Medical Laboratories for their help in the practical part of this research. Finally, we thank Dr. Rashad Fairooz for language review.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas; participated in drafting, revising or critically reviewing the article. Final approval was given for publication; all authors have agreed to the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shaikh MS, Ahmed S, Khalid A, Hayat MH, Shaikh MU, Ali N. Establishment of population specific reference intervals in healthy Pakistani adults for 21 routine and special haematology analytes. EJIFCC. 2022;33(3):220.
2. Abdullah DA, Mahmood GA, Rahman HS. Hematology reference intervals for healthy adults of the city of Sulaymaniyah, Iraq. Int J Gene Med. 2020;13:1249–1254. doi:10.2147/IJGM.S270800
3. Bakrim S, Motiaa Y, Benajiba M, Ouarou A, Masrar A. Establishment of the hematology reference intervals in a healthy population of adults in the Northwest of Morocco (Tangier-Tetouan region). Pan Afr Med J. 2018;29(1):1–18. doi:10.11604/pamj.2018.29.169.13042
4. Timbrell NE. The role and limitations of the reference interval within clinical chemistry and its reliability for disease detection. British J Biomed Sci. 2024;81:12339. doi:10.3389/bjbs.2024.12339
5. Bakr S, AlFattani A, Al-Nounou R, et al. Hematologic reference intervals for healthy adult Saudis in Riyadh. Ann Saudi Med. 2022;42(3):191–203. doi:10.5144/0256-4947.2022.191
6. Dacie JV. Dacie and Lewis practical haematology. Elsevier Health Sci; 2006.
7. El-Hazmi MA, Warsy AS. Normal reference values for hematological parameters, red cell indices, HB A2 and HB F from early childhood through adolescence in Saudis. Ann Saudi Med. 2001;21(3–4):165–169. doi:10.5144/0256-4947.2001.165
8. Buchanan AM, Muro FJ, Gratz J, et al. Establishment of haematological and immunological reference values for healthy Tanzanian children in Kilimanjaro Region. Tropical Med Int Health. 2010;15(9):1011–1021.
9. Bosire EM, Nyamache AK, Gicheru MM, Khamadi SA, Lihana RW, Okoth V. Population specific reference ranges of CD3, CD4 and CD8 lymphocyte subsets among healthy Kenyans. AIDS Res Ther. 2013;10:1–7. doi:10.1186/1742-6405-10-24
10. Mair C, Hawes S, Agne H, et al. Factors associated with CD4 lymphocyte counts in HIV-negative Senegalese individuals. Clin Exp Immunol. 2008;151(3):432–440. doi:10.1111/j.1365-2249.2007.03573.x
11. Robins EB, Blum S. Hematologic reference values for African American children and adolescents. Am J Hematol. 2007;82(7):611–614. doi:10.1002/ajh.20848
12. Beutler E, West C. Hematologic differences between African-Americans and whites: the roles of iron deficiency and α-thalassemia on hemoglobin levels and mean corpuscular volume. Blood. 2005;106(2):740–745. doi:10.1182/blood-2005-02-0713
13. Elbadry RM, Alghamdi FGA, Alamri HMM, et al. Complete blood count variation in relation to high and low altitude in different areas of Albaha Region, Saudi Arabia: a comparative study. Int J Med Dev Countries. 2022;6(9). doi:10.24911/IJMDC.51-1660661284
14. Ichihara K, Ozarda Y, Barth JH, et al. A global multicenter study on reference values: 1. Assessment of methods for derivation and comparison of reference intervals. Clin Chim Acta. 2017;467:70–82. doi:10.1016/j.cca.2016.09.016
15. Shaheen NA, Rehan H, Moghairi A, et al. Hematological indices in the adult Saudi population: reference intervals by gender, age, and region. Front Med. 2022;9:901937. doi:10.3389/fmed.2022.901937
16. Kratz A, Ferraro M, Sluss PM, Lewandrowski KB. Normal reference laboratory values. N Engl J Med. 2004;351(15):1548–1563. doi:10.1056/NEJMcpc049016
17. Cheng CK-W, Chan J, Cembrowski GS, Van Assendelft OW. Complete blood count reference interval diagrams derived from NHANES III: stratification by age, sex, and race. Lab Hematol. 2004;10(1):42–53. doi:10.1532/LH96.04010
18. Rosenfeld LG, Malta DC, Szwarcwald CL, et al. Reference values for blood count laboratory tests in the Brazilian adult population, National Health Survey. Revista Brasileira de Epidemiologia. 2019;22:E190003. doi:10.1590/1980-549720190003
19. Roshan T, Rosline H, Ahmed S, Rapiaah M, Wan Zaidah A, Khattak M. Hematological reference values of healthy Malaysian population. Int j Lab Hematol. 2009;31(5):505–512. doi:10.1111/j.1751-553X.2008.01068.x
20. Humberg A, Kammer J, Mordmüller B, Kremsner PG, Lell B. Haematological and biochemical reference intervals for infants and children in Gabon. Tropical Med Int Health. 2011;16(3):343–348. doi:10.1111/j.1365-3156.2010.02705.x
21. Ramezani A, Shams M, Zarinfar N, et al. Hematological reference values for healthy males in the central part of Iran. Iran j Pathol. 2014;9(1):50–55.
22. Klee GG, Ichihara K, Ozarda Y, et al. Reference intervals: comparison of calculation methods and evaluation of procedures for merging reference measurements from two US medical centers. Am J Clin Pathol. 2018;150(6):545–554. doi:10.1093/ajcp/aqy082
23. Koram K, Addae M, Ocran J, Adu-Amankwah S, Rogers W, Nkrumah F. Population based reference intervals for common blood haematological and biochemical parameters in the Akuapem north district. Ghana Med J. 2007;41(4):160–166. doi:10.4314/gmj.v41i4.55284
24. Saathoff E, Schneider P, Kleinfeldt V, et al. Laboratory reference values for healthy adults from southern Tanzania. Tropical Med Int Health. 2008;13(5):612–625. doi:10.1111/j.1365-3156.2008.02047.x
25. Lugada ES, Mermin J, Kaharuza F, et al. Population-based hematologic and immunologic reference values for a healthy Ugandan population. Clin Vaccin Immunol. 2004;11(1):29–34. doi:10.1128/CDLI.11.1.29-34.2004
26. Rasouli M, Pourmokhtar M, Sarkardeh S. Hematological reference intervals for healthy Iranian blood donors. Int J Hematol-Oncol Stem Cell Res. 2017;11(4):305.
27. Moradinazar M, Najafi F, Pasdar Y, et al. Establishing hematological reference intervals in healthy adults: ravansar non‐communicable disease cohort study, Iran. Int J Lab Hematol. 2021;43(2):199–209. doi:10.1111/ijlh.13371
28. Al-Mawali A, Pinto AD, Al-Busaidi R, Al-Lawati RH, Morsi M. Comprehensive haematological indices reference intervals for a healthy Omani population: first comprehensive study in Gulf cooperation council (GCC) and Middle Eastern countries based on age, gender and ABO blood group comparison. PLoS One. 2018;13(4):e0194497. doi:10.1371/journal.pone.0194497
29. Fiseha T, Alemayehu E, Mohammed O, et al. Reference intervals of haematological parameters for apparently healthy adults in Northeast Ethiopia. Int J Gene Med;2023. 5309–5321. doi:10.2147/IJGM.S430751
30. Al-Jafar H. Provisional study of Kuwait adult hematology reference range. J Hematol Thromb. 2016;2(1):4.
31. Geffre A, Friedrichs K, Harr K, Concordet D, Trumel C, Braun JP. Reference values: a review. Vet Clin Pathol. 2009;38(3):288–298. doi:10.1111/j.1939-165X.2009.00179.x
32. Horowitz GL, Altaie S, Boyd JC. Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline. CLSI; 2010.
33. Solberg HE. Statistical treatment of collected reference values and determination of reference limits. Ref Values Lab Med. 1981;1981:193–205.
34. Ringoringo HP. Prevalence of iron deficiency anemia and reference range of complete blood count, reticulocyte parameters in infants aged 9–11 months. Int J Gene Med. 2022;15:8017. doi:10.2147/IJGM.S383055
35. Ringoringo HP, Purnamasari L, Yunanto A, Syahadatina M, Hidayah N. Reference range of complete blood count, Ret-He, immature reticulocyte fraction, reticulocyte production index in healthy babies aged 1–4 months. Sci Rep. 2023;13(1):423. doi:10.1038/s41598-023-27579-3
36. Zeh C, Amornkul PN, Inzaule S, et al. Population-based biochemistry, immunologic and hematological reference values for adolescents and young adults in a rural population in Western Kenya. PloS one. 2011;6:e21040.
37. Fondoh VN, Fondoh RM, Awasom CN, et al. Haematological reference intervals for healthy adults in Bamenda, Cameroon. Afr J Lab Med. 2020;9(1):1–8. doi:10.4102/ajlm.v9i1.1193
38. Maksane SN, Dandekar SP, Shukla A, Bhatia S. Hepatic enzyme’s reference intervals and their modulating factors in Western Indian population. Indian J Clin Biochem. 2016;31:108–116. doi:10.1007/s12291-015-0508-y
39. Tahmasebi H, Trajcevski K, Higgins V, Adeli K. Influence of ethnicity on population reference values for biochemical markers. Crit Rev Clin Lab Sci. 2018;55(5):359–375. doi:10.1080/10408363.2018.1476455
40. Osei‐Bimpong A, McLean R, Bhonda E, Lewis S. The use of the white cell count and haemoglobin in combination as an effective screen to predict the normality of the full blood count. Int j Lab Hematol. 2012;34(1):91–97. doi:10.1111/j.1751-553X.2011.01365.x
41. Troussard X, Cornet E, Bardet V, et al. Full blood count normal reference values for adults in France. J Clin Pathol. 2014;67(4):341–344. doi:10.1136/jclinpath-2013-201687
42. Romeo J, Wärnberg J, Gómez‐Martínez S, et al. Haematological reference values in Spanish adolescents: the AVENA study. Eur J Haematol. 2009;83(6):586–594. doi:10.1111/j.1600-0609.2009.01326.x
43. Gordon AS, Mirand EA, Wenig J, Katz R, Zanjani ED. Androgen actions on erythropoiesis. Ann N.Y. Acad Sci. 1968;149(1):318–335. doi:10.1111/j.1749-6632.1968.tb15167.x
44. Rushton DH, Dover R, Sainsbury AW, Norris MJ, Gilkes JJ, Ramsay ID. Why should women have lower reference limits for haemoglobin and ferritin concentrations than men? BMJ. 2001;322(7298):1355–1357. doi:10.1136/bmj.322.7298.1355
45. Al-Marzoki JM, Al-Maaroof ZW, Kadhum AH. Determination of reference ranges for full blood count parameters in neonatal cord plasma in Hilla, Babil, Iraq. J Blood Med. 2012;113–118. doi:10.2147/JBM.S35895
46. Miri-Dashe T, Osawe S, Tokdung M, et al. Comprehensive reference ranges for hematology and clinical chemistry laboratory parameters derived from normal Nigerian adults. PLoS One. 2014;9(5):e93919. doi:10.1371/journal.pone.0093919
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.