Back to Journals » Drug Design, Development and Therapy » Volume 19
Determination the ED90s of Different Concentrations of Initial Ropivacaine Volume for Labor Analgesia with Dural Puncture Epidural: A Randomized Sequential Allocation Study
Authors Sun M, Chen Y ![]() , Sun L, Deng Y, Xu X, Zhang L, Xiong X
, Sun L, Deng Y, Xu X, Zhang L, Xiong X ![]()
Received 4 June 2025
Accepted for publication 16 August 2025
Published 27 August 2025 Volume 2025:19 Pages 7405—7413
DOI https://doi.org/10.2147/DDDT.S544672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Meijuan Sun,1,* Yi Chen,2,* Linsen Sun,1 Yu Deng,1 Xiaoxiao Xu,1 Liang Zhang,1 Xiangsheng Xiong1
1Department of Anesthesiology, Huai’an Hospital Affiliated to Yangzhou University (The Fifth People’s Hospital of Huai’an), Huaian, People’s Republic of China; 2Department of Anesthesiology and Perioperative Medicine, General Hospital of Ningxia Medical University, Yinchuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangsheng Xiong, Department of Anesthesiology, Huai’an Hospital Affiliated to Yangzhou University (The Fifth People’s Hospital of Huai’an), Huaian, People’s Republic of China, Email [email protected]
Background: This study aims to determine the 90% effective doses (ED90) of the initial ropivacaine volume at varying concentrations (0.075%, 0.1%, 0.125%) administered under dural puncture epidural (DPE) for epidural labor analgesia.
Methods: Ninety ASA II-class patients with cervical dilation < 5 cm and VAS scores > 5 were allocated into three groups (0.075%, 0.1%, and 0.125% ropivacaine concentrations) for epidural labor analgesia. The first patient in each group received an initial bolus of ropivacaine combined with sufentanil 0.3 μg/mL in a 10 mL volume. Subsequent doses were determined by an up-and-down sequential allocation method based on adequate analgesia (VAS score < 3) within 30 minutes post-administration, using 2 mL incremental/decremental adjustments. The primary outcome was the ED90s of the initial ropivacaine bolus required for effective analgesia under DPE. Maternal analgesia characteristics and neonatal outcomes were recorded.
Results: The ED90 values for the 0.075%, 0.1%, and 0.125% ropivacaine groups were 13.30 mL (95% CI, 10.00– 14.00), 10.80 mL (95% CI, 8.00– 12.00), and 8.90 mL (95% CI, 8.00– 10.00), respectively. Maternal and neonatal outcomes were comparable across groups.
Conclusion: Compared to 0.075% concentration of ropivacaine, the 0.1% and 0.125% concentrations achieved 18.8% and 33.0% reductions in initial analgesic volume requirements. However, comparable analgesic effects and maternal satisfaction were observed across all groups.
Keywords: initial ropivacaine volume, ropivacaine, epidural labor analgesia, dural puncture epidural
Introduction
Epidural labor analgesia, a widely utilized pain relief method during childbirth, provides safe and effective pain control while minimizing motor function inhibition, blocks nociceptive sensations to reduce negative psychological effects such as tension and anxiety, and ultimately improves maternal and neonatal outcomes.1–5 Recent advancements in techniques such as dural puncture epidural (DPE) and programmed intermittent epidural bolus (PIEB) have significantly enhanced the quality of the childbirth experience.6,7 Previous studies have extensively demonstrated the advantages of DPE over conventional epidural labor analgesia (EPL),8 optimized PIEB time intervals combined with DPE protocols,9 and determined optimal PIEB doses,10 collectively establishing a robust practical foundation for the clinical implementation of combined DPE and PIEB techniques.
Current evidence supports the use of lower-concentrations of local anesthetics for epidural labor analgesia to improve maternal pain relief while reducing complications such as motor blockade, thereby optimizing the childbirth experience.11 Nevertheless, clinical practice continues to employ ropivacaine at varying concentrations (0.075%, 0.1%, and 0.125%).12,13 The initial volume of ropivacaine at these concentrations may critically influence the onset time, analgesic efficacy of labor analgesia, and subsequent analgesic regimens, such as PIEB. To address this gap, this study aims to determine the 90% effective doses (ED₉₀) of the initial ropivacaine volume at varying concentrations (0.075%, 0.1%, 0.125%) administered under DPE combined with PIEB for epidural labor analgesia.
Methods
Ethical Approval and Study Design
After approved by the Ethics Committee (No. KY-P-2024-009-01) and registered with Chinese Clinical Trials Registry (No. ChiCTR2400086367), this sequential allocation study was conducted at Huai’an Hospital Affiliated to Yangzhou University (The Fifth People’s Hospital of Huai’an) between July 2024 to May 2025. This study was conducted in accordance with the principles of the Declaration of Helsinki. Eligible participants included patients admitted for vaginal delivery (spontaneous or induced labor) meeting the following criteria: age ≥18 years, singleton term pregnancy, multidisciplinary approval for epidural labor analgesia (obstetrician, anesthesiologist, and midwife consensus), cervical dilation <5 cm, VAS score >5, and ASA class II. Exclusion criteria including: contraindications to epidural labor analgesia (epidural contraindications, hypersensitivity to ropivacaine or sufentanil), severe gestational hypertension/diabetes mellitus, macrosomia, fetal distress, or concurrent use of alternative analgesics.
Randomization and Group Assignments
All patients provided written informed consent prior to enrollment and underwent a standardized epidural labor analgesia protocol with uniform maternal-neonatal care. Using a computer-generated randomization sequence, patients were allocated in a 1:1:1 ratio to three groups receiving different concentrations of ropivacaine: 0.075%, 0.1%, and 0.125%. Following group assignment, patients in each group were allocated to different initial volumes based on the up-and-down sequential allocation method. Before initiating epidural labor analgesia, maternal monitoring included continuous electrocardiogram (ECG), non-invasive blood pressure (BP), and transcutaneous oxygen saturation (SpO₂), an 18-gauge intravenous access established in the upper limb for crystalloid infusion. Fetal heart rate monitoring was performed both pre- and post-analgesia initiation to ensure fetal safety.
Blinded Intervention
Epidural labor analgesia was administered by experienced obstetric anesthesiologists. Before initiating epidural labor analgesia, an independent evaluator (not involved in the administration or management of epidural labor analgesia) opened a sealed group allocation envelope containing group allocation and protocol details. Ropivacaine solutions of varying concentrations were prepared accordingly, diluted with normal saline. Both initial bolus and PIEB solutions were labeled generically as “ropivacaine” without concentration disclosure. The patients and the administering anesthesiologists remained blinded to group assignments.
Technical Procedure and Up-and-Down Sequential Allocation Implementation
Epidural labor analgesia was performed at the L2-3 interspace. Following epidural space confirmation (absence of cerebrospinal fluid or blood return), dural puncture was conducted with a standard pencil-point 25-gauge needle (Nanjing Ningchuang Medical Equipment Co., Ltd, Nanjing, China) followed by epidural catheter insertion (4 cm depth). A test dose of 3 mL 1% lidocaine was administered, followed by a 5-minute observation period to exclude intrathecal spread. This study employed a up-and-down sequential allocation design: The first patient in each group received an initial bolus of ropivacaine (7.5 mg [0.075%], 10 mg [0.1%], or 12.5 mg [0.125%]) combined with sufentanil 0.3 µg/mL in a 10 mL volume. If adequate analgesia (VAS score < 3) was achieved within 30 minutes, the subsequent patient received a 2 mL dose reduction in initial ropivacaine dose (1.5 mg, 2 mg, or 2.5 mg for respective groups) with the same sufentanil concentration. If adequate analgesia was not achieved, the current patient received an additional rescue bolus (8 mL ropivacaine + sufentanil 0.3 µg/mL), while the subsequent participant was assigned to receive a 2 mL increased initial ropivacaine volume. Analgesia failure was defined as persistent VAS ≥ 3 after two consecutive rescue bolus doses, resulting in study exclusion and subsequent management (additional boluses or catheter replacement) per the attending anesthesiologist’s judgment. The PIEB protocol: A 10 mL solution containing ropivacaine and sufentanil 0.3 μg/mL was administered via an electronic pump at 40-minute intervals. For patient-controlled epidural analgesia (PCEA), the demand dose was set at 8 mL with a 20-minute lockout period. The sensory block was evaluated using a sterile needle to confirm that the level was at least T10.
Study Outcomes
The primary outcome was the determination of the effective dose required to achieve adequate analgesia, defined as a VAS score <3 within 30 minutes post-administration, in 90% of patients (ED90) for the initial ropivacaine bolus administered under the DPE technique for epidural labor analgesia. Secondary outcomes including VAS scores (0–10; 0 = no pain, 10 = unbearable pain) at specified time points: every 10 minutes during the first 30 minutes, then hourly thereafter; time from analgesia initiation to VAS ≤1; total duration of analgesia; proportion of patients achieving VAS ≤1 within 10 minutes, asymmetry (defined as a difference in sensory blockade level >2 dermatomes between left and right sides), and T6, S1, and S2 sensory blockade; sensory blockade level; number of rescue boluses and PCEA administrations; Bromage score (0: full flexion of knees and ankles; 1: partial knee flexion with full ankle flexion; 2: inability to flex knees with partial ankle flexion; 3: inability to flex knees or ankles) and incidence of motor blockade; duration of labor stages; rate of conversion to cesarean delivery; neonatal Apgar scores at 1 and 5 minutes; and maternal satisfaction score (1–5; 5 = highest satisfaction).
Sample Size Calculatation
The sample size was determined based on previously reported literature indicating that 20–40 cases with 6 reversals would suffice for up-and-down sequential allocation design. Consequently, 30 patients per group were enrolled for final analysis.14
Statistical Analysis
All statistical analyses were performed with IBM SPSS Statistics version 23.0 (IBM SPSS, Inc, Chicago, IL), with P < 0.05 denoting statistical significance. For continuous variables, normality was assessed using the Kolmogorov–Smirnov test. Normally distributed variables were compared using one-way ANOVA, followed by Bonferroni post hoc test for intergroup comparisons with statistically differences across groups. Non-normally distributed variables were compared using the Kruskal–Wallis test, followed by Dunn’s test for intergroup comparisons with statistically differences across groups. Categorical variables were assessed using χ²-tests; paired tests would be conducted across groups demonstrating statistically differences. The ED90s of the initial ropivacaine volume at varying concentrations (0.075%, 0.1%, 0.125%) administered under DPE for epidural labor analgesia was determined using isotonic regression analysis.
Results
Eight patients were excluded, with a final analysis of 30 patients per group included (see Figure 1 for enrollment flowchart). There were no statistically significant differences among the three groups in terms of maternal demographic characteristics, baseline values including maternal blood pressure and heart rate, fetal heart rate, as well as obstetric values including cervical dilation, spontaneous labor, and stage of labor (Table 1).
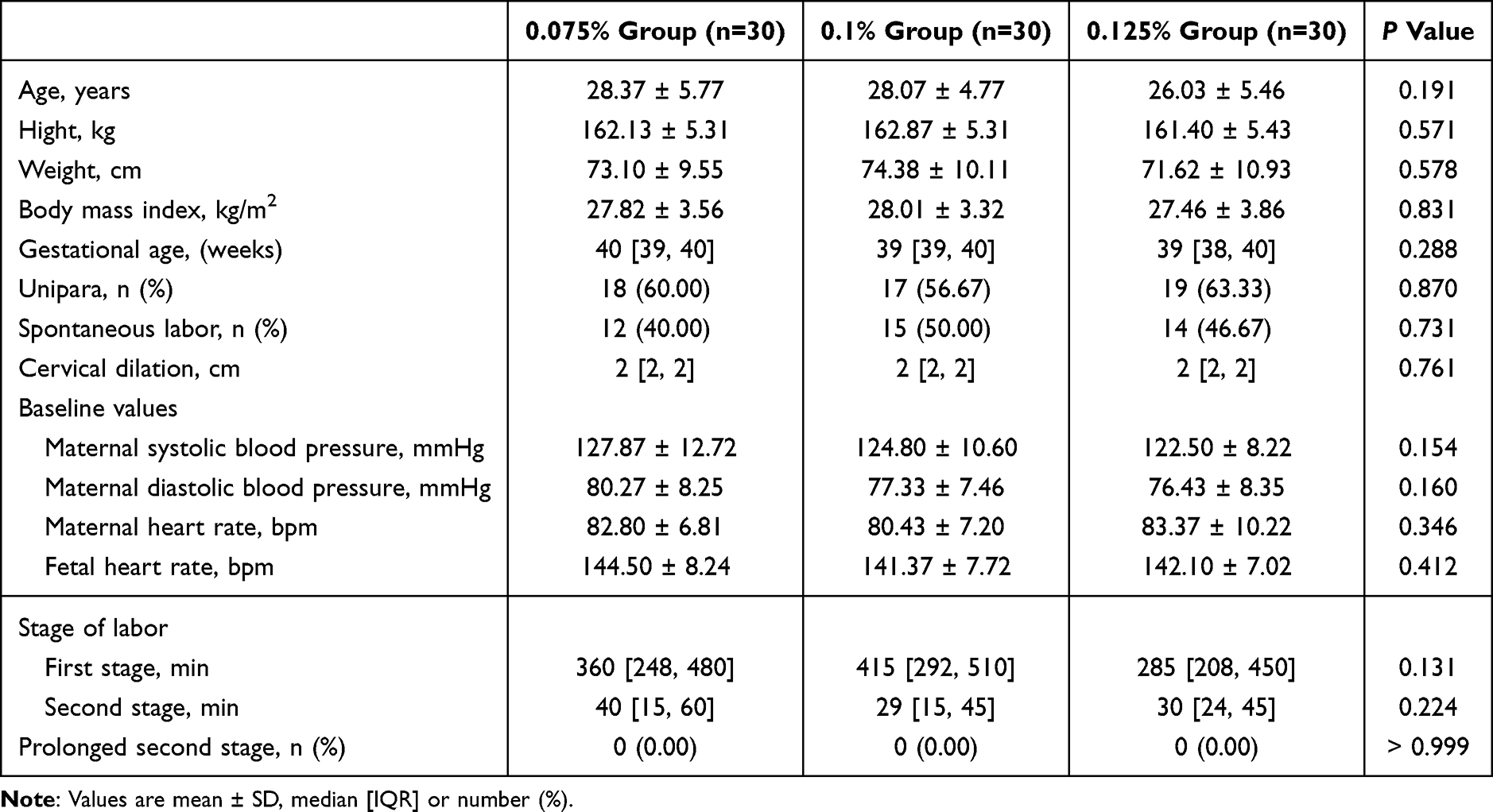 |
Table 1 Maternal Baseline and Obstetric Characteristics |
 |
Figure 1 Recruitment flow diagram. |
The ED90 values of the initial volume for the 0.075%, 0.1%, and 0.125% ropivacaine groups were 13.30 mL (95% CI, 10.00–14.00), 10.80 mL (95% CI, 8.00–12.00), and 8.90 mL (95% CI, 8.00–10.00), respectively. When converted to total drug mass, these equated to 8.67 mg (95% CI, 8.10–9.00), 10.80 mg (95% CI, 10.00–15.00), and 11.13 mg (95% CI, 10.00–12.50) of ropivacaine. The corresponding dose sequences are presented in Figure 2.
 |
Figure 2 The sequence of the initial ropivacaine dose at different concentrations. |
No statistically significant differences were observed among the three groups with respect to the maternal analgesic quality characteristics, including duration of analgesia, VAS scores, sensory block, rescue bolus administration, rescue PCEA administration, Bromage scores, patient satisfaction, and neonatal Apgar scores (Table 2).
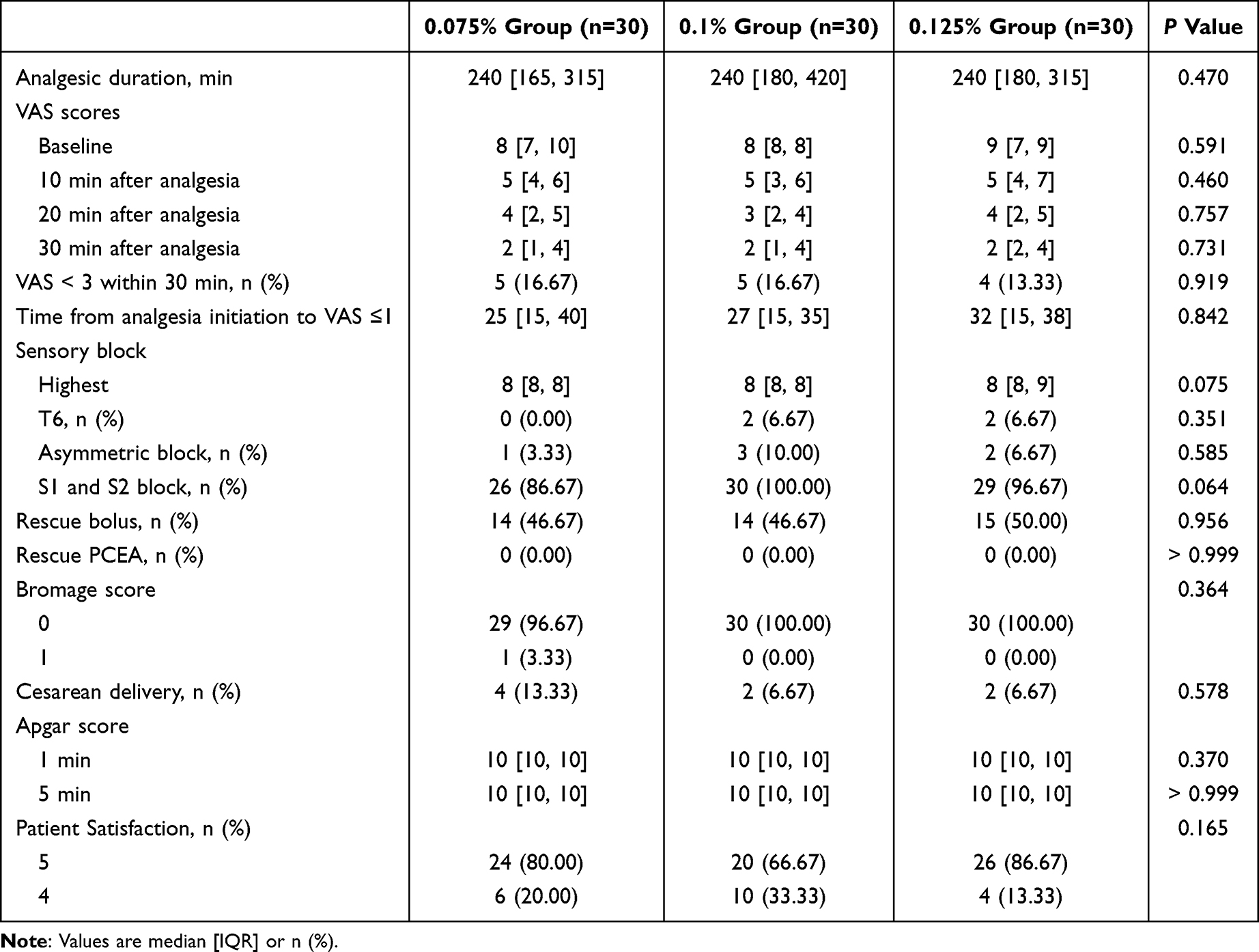 |
Table 2 Maternal Analgesia Quality Characteristics and Neonatal Outcomes |
Discussion
This randomized sequential allocation study demonstrated that the ED90 values of the initial volume for 0.075%, 0.1%, and 0.125% ropivacaine groups were 13.3 mL (95% CI, 10.0–14.0), 10.8 mL (95% CI, 8.0–12.0), and 8.9 mL (95% CI, 8.0–10.0), respectively. Dose conversion based on concentration yielded equivalent values of 8.67 mg (95% CI, 8.10–9.00), 10.80 mg (95% CI, 10.00–15.00), and 11.13 mg (95% CI, 10.00–12.50).
Limited studies have evaluated the optimal initial ropivacaine volume for combined DPE and PIEB techniques in epidural labor analgesia. Ngan Kee et al15 compared initial ropivacaine doses of 7, 15, 20, 30, 45, and 60 mg (total volume 20 mL) for EPL, defining adequate analgesia as achieving maternal pain relief at 30 minutes post-administration. They reported ED50 and ED90 values of 15.3 mg (95% CI: 13.7–17.1) and 40.6 mg (95% CI: 32.4–51.1), respectively. Similarly, Lee et al 16 tested initial ropivacaine doses of 10, 20, 30, 40, and 50 mg (20 mL total volume) for EPL, targeting a ≥ 50% reduction in pain scores within 30 minutes post-administration, and found ED50 and ED95 values of 18.4 mg (95% CI: 13.4–25.4) and 55.9 mg (95% CI: 35.3–88.5), respectively. In study using DPE technique, Maeda et al 17 compared DPE and EPL using 20 mL bupivacaine (without adjuvants), demonstrating that the ED90 for achieving a NRS score < 3 at 30 minutes was 29.30 mg (95% CI: 28.55–31.56) with DPE, significantly lower than the ED90 of 45.25 mg (90% CI: 42.80–52.03) for EPL. Given the reported potency ratio of 0.75 between ropivacaine and bupivacaine,15 the extrapolated ED90 for ropivacaine under DPE would approximate 22.0 mg, which remains notably higher than the ED90 values observed in our study.
The observed lower ED90 may be attributed to the concurrent use of opioids and implementation of the DPE technique. Vertommen JD et al18 compared 0.125% bupivacaine with versus without 1 μg/mL sufentanil for epidural labor analgesia, the opioid-containing regimen demonstrating a higher rate of adequate analgesia (1.1% [4 of 348 patients] vs 8.4% [29 of 347 patients], P < 0.001), accompanied by faster onset time and longer analgesia duration. Similarly, Yau et al19 compared three regimens - plain 0.125% bupivacaine (Group P), 0.125% bupivacaine with 2.5 μg/mL epinephrine (Group A), and 0.125% bupivacaine with 2.5 μg/mL epinephrine plus 0.5 μg/mL fentanyl (Group FA) using a 10 mL bolus - the combination with epinephrine and fentanyl significantly reduced analgesic failure rates (defined as > 50% baseline pain score post-administration or requiring supplemental analgesia within 30 minutes) (6.7% vs 26.7% vs 33.3%), induced lower 15-minute VAS scores (0 vs 2.2 vs 3.0), and achieved faster onset (15 vs 22 vs 28 minutes) with prolonged duration (120 vs 90 vs 75 minutes). These findings suggest that opioid adjuvants enhance epidural labor analgesia quality through faster onset and prolonged duration of pain relief.
Additionally, the DPE technique enhances epidural labor analgesia by allowing minimal opioid migration from the epidural to the subarachnoid space. This procedure involves puncturing the dural with a 25G or 27G needle during epidural placement without administering intrathecal medication, thereby creating a pressure gradient that facilitates epidural local anesthetic diffusion into the subarachnoid space, resulting in faster onset and more complete sacral blockade compared to EPL.8,20 Zang et al 21 reported no significant differences in overall analgesic quality or adverse event rates between DPE and combined spinal-epidural (CSE) techniques. Outcomes included asymmetric blockade at 30 minutes post-analgesia, rescue bolus interventions, epidural catheter adjustment or replacement, and anesthesia method conversion during cesarean delivery. However, Lacombe et al22 cautioned that unintentional dural puncture with larger-gauge needles may increase risks of chronic headaches, lower back pain, and auditory disturbances. Our preliminary data demonstrated that initial volumes of 12 mL ropivacaine (three concentrations of 0.075%, 0.1%, and 0.125%) combined with sufentanil 0.3 μg/mL achieved VAS < 1 within 14.90 ± 8.01, 11.76 ± 6.17, and 11.77 ± 5.64 minutes, respectively.23 These findings suggest that low-concentration ropivacaine (12 mL) with sufentanil fulfills the initial analgesic requirements within 30 minutes for the majority of patients under DPE technique.
The EJA expert consensus recommends using low-concentration bupivacaine or ropivacaine (< 0.1%) combined with opioids for epidural labor analgesia.13 Compared to higher concentrations (≥ 0.1%), lower (0.08–0.1%) and ultra-low (< 0.08%) concentrations of local anesthetics provide comparable analgesic efficacy while achieving superior clinical outcomes: higher rates of spontaneous vaginal delivery, shorter duration of the second labor stage, and reduced total local anesthetic consumption.11 The lower ED90 (expressed as milligram equivalents) observed in the 0.075% ropivacaine group compared to the other two concentrations in this study may be explained by the aforementioned meta-analysis. The study conducted by Baliuliene et al24 compared the analgesia efficacy of different concentrations of bupivacaine (0.0625%, 0.1%, 0.125%) in epidural lobar analgesia, revealing that higher concentrations were associated with increased total local anesthetic consumption and increased risk of motor blockade. Notably, at 0.0625% concentration, despite inferior analgesic efficacy compared to higher concentrations, maternal satisfaction remained unaffected. Consequently, these findings collectively support the utilization of lower concentrations local anesthetics for epidural labor analgesia. With the decrease in local anesthetic concentration, there is a reduction in associated adverse events such as motor blockade, prolonged second stage of labor, and risk of local anesthetic toxicity; however, the analgesic efficacy remains similar, which may lead to greater patient satisfaction.25,26
Due to the up-and-down sequential allocation design, initial volumes varied significantly among patients. Consequently, rescue boluses were administered for VAS ≥ 3 at 30 minutes post-analgesia to ensure efficacy. However, the comparable number of rescue interventions across groups may still have influenced maternal satisfaction. We implemented a PIEB regimen based on Yao et al,9 who determined the ED90 for PIEB time intervals using 0.1% ropivacaine combined with sufentanil 0.3 µg/mL (10 mL). Their randomized trial comparing time intervals of 35, 40, 45, 50, and 55 minutes reported an ED90 of 37.0 min (95% CI: 28.4–40.9). Given that 0.1% ropivacaine represented the intermediate concentration in our study, we adopted a conservative 40-minute PIEB interval. All three groups demonstrated comparable analgesic efficacy and neonatal outcomes. These findings underscore the clinical advantages of low-concentration local anesthetic regimens in epidural labor analgesia.
This study has several limitations. Firstly, we did not investigate higher (eg, 0.15%) or lower (eg, 0.0625%) ropivacaine concentrations due to concerns about motor blockade risks at higher concentrations and potential inadequate analgesia at lower concentrations. However, as these concentrations have been reported in existing literature, our findings cannot provide evidence for their clinical application. Secondly, the inclusion of multiparous women and those with cervical dilation >5 cm may affect result generalizability, given that multiparous women typically have shorter labor durations and lower analgesic requirements, while initiating analgesia beyond 5 cm dilation may not align with current practice standards supporting analgesia initiation at any labor stage.
In conclusion, when using 0.075%, 0.1%, and 0.125% ropivacaine combined with 0.3 µg/mL sufentanil under DPE and PIEB techniques, the initial bolus requirements were 13.3 mL, 10.8 mL, and 8.9 mL respectively. Compared to 0.075% concentration of ropivacaine, the 0.1% and 0.125% concentrations achieved 18.8% and 33.0% reductions in initial analgesic volume requirements. However, comparable analgesic effects and maternal satisfaction were observed across all groups.
Data Sharing Statement
The data that support the study findings are available from the corresponding author upon reasonable request.
Funding
This work was supported by the Science and Education Integration Research Development Foundation of Jiangsu College of Nursing (No. SH202410250318).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kearns RJ, Lucas DN. Neuraxial analgesia in labour and the foetus. Best Pract Res Clin Anaesthesiol. 2023;37(1):73–86. doi:10.1016/j.bpa.2023.02.005
2. Callahan EC, Lee W, Aleshi P, George RB. Modern labor epidural analgesia: implications for labor outcomes and maternal-fetal health. Am J Obstet Gynecol. 2023;228(5S):S1260–S1269. doi:10.1016/j.ajog.2022.06.017
3. Chau A, Bibbo C, Huang CC, et al. Dural puncture epidural technique improves labor analgesia quality with fewer side effects compared with epidural and combined spinal epidural techniques: a randomized clinical trial. Anesth Analg. 2017;124(2):560–569. doi:10.1213/ANE.0000000000001798
4. Chau A, Tsen L. Neuraxial labor analgesia: initiation techniques. Best Pract Res Clin Anaesthesiol. 2022;36(1):3–15. doi:10.1016/j.bpa.2022.04.004
5. Kianian S, Bansal J, Lee C, et al. Perioperative multimodal analgesia: a review of efficacy and safety of the treatment options. APS. 2024;2:9. doi:10.1007/s44254-023-00043-1
6. Gunaydin B, Erel S. How neuraxial labor analgesia differs by approach: dural puncture epidural as a novel option. J Anesth. 2019;33(1):125–130. doi:10.1007/s00540-018-2564-y
7. Song Y, Song Y, Sheng Z, et al. Exploration of the optimal programmed intermittent epidural bolus volume with the dural puncture epidural technique for labour analgesia: a biased-coin up-and-down sequential allocation study. Can J Anaesth. 2025;72(2):254–261. doi:10.1007/s12630-024-02855-6
8. Han HS, Reed SE, Mehdiratta JE, et al. Quality of labor analgesia with dural puncture epidural versus standard epidural technique in obese parturients: a double-blind randomized controlled study. Anesthesiology. 2022;136(5):678–687. doi:10.1097/ALN.0000000000004137
9. Yao HQ, Huang JY, Deng JL, et al. Randomized assessment of the optimal time interval between programmed intermittent epidural boluses when combined with the dural puncture epidural technique for labor analgesia. Anesth Analg. 2023;136(3):532–539. doi:10.1213/ANE.0000000000006201
10. Xiao F, Yao HQ, Qian J, et al. Determination of the optimal volume of programmed intermittent epidural bolus when combined with the dural puncture epidural technique for labor analgesia: a random-allocation graded dose-response study. Anesth Analg. 2023;137(6):1233–1240. doi:10.1213/ANE.0000000000006451
11. Halliday L, Kinsella M, Shaw M, et al. Comparison of ultra-low, low and high concentration local anaesthetic for labour epidural analgesia: a systematic review and network meta-analysis. Anaesthesia. 2022;77(8):910–918. doi:10.1111/anae.15756
12. Men X, Wang Q, Dong JF, et al. 0.75% ropivacaine may be a suitable drug in pregnant women undergoing urgent cesarean delivery during labor analgesia period. BMC Anesthesiol. 2024;24(1):212. doi:10.1186/s12871-024-02597-4
13. Guasch E, Brogly N, Mercier FJ, et al. European minimum standards for obstetric analgesia and anaesthesia departments: an experts’ consensus. Eur J Anaesthesiol. 2020;37(12):1115–1125. doi:10.1097/EJA.0000000000001362
14. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
15. Ngan Kee WD, Ng FF, Khaw KS, Lee A, Gin T. Determination and comparison of graded dose-response curves for epidural bupivacaine and ropivacaine for analgesia in laboring nulliparous women. Anesthesiology. 2010;113(2):445–453. doi:10.1097/ALN.0b013e3181bdf9da
16. Lee BB, Ngan Kee WD, Wong EL, Liu JY. Dose-response study of epidural ropivacaine for labor analgesia. Anesthesiology. 2001;94(5):767–772. doi:10.1097/00000542-200105000-00013
17. Maeda A, Villela-Franyutti D, Lumbreras-Marquez MI, et al. Labor analgesia initiation with dural puncture epidural versus conventional epidural techniques: a randomized biased-coin sequential allocation trial to determine the effective dose for 90% of patients of bupivacaine. Anesth Analg. 2024;138(6):1205–1214. doi:10.1213/ANE.0000000000006691
18. Vertommen JD, Vandermeulen E, Van Aken H, et al. The effects of the addition of sufentanil to 0.125% bupivacaine on the quality of analgesia during labor and on the incidence of instrumental deliveries. Anesthesiology. 1991;74(5):809–814. doi:10.1097/00000542-199105000-00002
19. Yau G, Gregory MA, Gin T, Oh TE. Obstetric epidural analgesia with mixtures of bupivacaine, adrenaline and fentanyl. Anaesthesia. 1990;45(12):1020–1023. doi:10.1111/j.1365-2044.1990.tb14878.x
20. Contreras F, Morales J, Bravo D, et al. Dural puncture epidural analgesia for labor: a randomized comparison between 25-gauge and 27-gauge pencil point spinal needles. Reg Anesth Pain Med. 2019:rapm–2019–100608. doi:10.1136/rapm-2019-100608.
21. Zang H, Padilla A, Pham T, et al. Combined spinal-epidural vs. dural puncture epidural techniques for labour analgesia: a randomised controlled trial. Anaesthesia. 2025;80(1):29–37. doi:10.1111/anae.16433
22. Lacombe A, Downey K, Ye XY, Carvalho JCA. Long-term complications of unintentional dural puncture during labor epidural analgesia: a case-control study. Reg Anesth Pain Med. 2022;47(6):364–369. doi:10.1136/rapm-2021-103266
23. Mao J, Chen Y, Sun L, et al. A randomized sequential allocation study on the optimum programmed intermittent epidural boluses interval time with different concentrations of ropivacaine combined with the dural puncture epidural technique for labor analgesia. Front Pharmacol. 2025;15:1508514. doi:10.3389/fphar.2024.1508514
24. Baliuliene V, Macas A, Rimaitis K. The optimal concentration of bupivacaine and levobupivacaine for labor pain management using patient-controlled epidural analgesia: a double-blind, randomized controlled trial. Int J Obstet Anesth. 2018;35:17–25. doi:10.1016/j.ijoa.2018.05.002
25. Wang TT, Sun S, Huang SQ. Effects of epidural labor analgesia with low concentrations of local anesthetics on obstetric outcomes: a systematic review and meta-analysis of randomized controlled trials. Anesth Analg. 2017;124(5):1571–1580. doi:10.1213/ANE.0000000000001709
26. Mei Z, Wang Q, Song S, Lu W, Yu J. Optimum programmed intermittent epidural bolus interval time of ropivacaine 0.0625% with dexmedetomidine 0.4 mug/mL at a fixed volume of 10 mL: a randomized controlled trial. Front Pharmacol. 2024;15:1368222. doi:10.3389/fphar.2024.1368222
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.