Back to Journals » Open Access Journal of Contraception » Volume 11
Determinants of Postpartum IUCD Utilization Among Mothers Who Gave Birth in Gamo Zone Public Health Facilities, Southern Ethiopia: a Case-Control Study
Authors Jemal Mohammed S ![]() , Gebretsadik Kelbore W
, Gebretsadik Kelbore W ![]() , Endashaw Yesera G
, Endashaw Yesera G ![]() , Shegaze Shimbre M
, Shegaze Shimbre M ![]() , Assfa Mossa K, Nuriye Metebo K
, Assfa Mossa K, Nuriye Metebo K ![]() , Mesfin Yesgat Y
, Mesfin Yesgat Y ![]()
Received 25 April 2020
Accepted for publication 19 August 2020
Published 30 September 2020 Volume 2020:11 Pages 125—133
DOI https://doi.org/10.2147/OAJC.S257762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Seid Jemal Mohammed,1 Woiynshet Gebretsadik Kelbore,2 Gesila Endashaw Yesera,2 Mulugeta Shegaze Shimbre,3 Kenzudin Assfa Mossa,4 Keyredin Nuriye Metebo,1 Yibeltal Mesfin Yesgat1
1Department of Midwifery, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2School of Nursing, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 4Department of Public Health, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Correspondence: Seid Jemal Mohammed Email [email protected]
Background: The postpartum intrauterine contraceptive device (PPIUCD) is an effective, reliable, safe and recommended contraceptive method for the postpartum women. However, only a small proportion of women who gave birth at health facilities in the world have used it. There are limited studies about determinants of PPIUCD utilization. Therefore, this study aimed to assess determinants of postpartum IUCD utilization among mothers who gave birth in Gamo zone health facilities, southern Ethiopia.
Methods: A facility based unmatched case-control study was done at Gamo zone public health facilities, southern Ethiopia. Data were collected using a pretested interviewer-administered questionnaire from March 1 to April 15, 2019. The data were coded, cleaned and entered into Epi-Info version 3.5.1 and exported to SPSS version 25 for advanced analysis. Binary logistic regression was performed to identify the determinants of PPIUCD utilization.
Results: A total of 510 (175 cases and 335 controls) participants were involved in the study yielding a response rate of 95.1%. Partner support for IUCD insertion (AOR [95% CI]: 10 [4.03, 24.3]), birth interval (AOR [95% CI]: 9.7 [1.7, 55.1]), fertility plan (AOR [95% CI]: 4 [1.44, 10.84]), and timing of counseling (AOR [95% CI]:1.25 [0.034, 0.46]) are the determinant factors for postpartum IUCD.
Conclusion and Recommendation: Birth interval, fertility plan, timing of counseling, pregnancy plan and partner support were the determinant factors identified in this study. Therefore, counseling of both partners during antenatal follow-up, delivery and immediately after delivery by health professionals are recommended.
Keywords: postpartum intrauterine contraceptive device, PPIUCD, Gamo zone, unmatched case control, determinant factors
Background
Family planning (FP) is a means to achieve an individual’s and couple’s reproductive life. While, postpartum family planning (PPFP) is aimed to prevent unintended and closely spaced pregnancies within the first year following childbirth.1 The immediate postpartum period has several potential benefits for intrauterine contraceptive device (IUCD) placement because many women were known not to be pregnant and many of them want to avoid short pregnancy interval.2
The postpartum intrauterine contraceptive device (PPIUCD) is an effective, reliable, safe and recommended contraceptive method for the postpartum women. However, only a small proportion of women who gave birth at health facilities in the world have used it. Thus, previous studies reported that mothers who gave birth in the health facilities and utilized PPIUCD were 19.7–24.5% in India,3–5 23.7% in Egypt6 and 12.4% in Ethiopia,7 respectively.
The postpartum period is a highly vulnerable period for unintended pregnancy due to limited contraceptive options, especially to breast-feeding women. At the same time ovulation is highly unpredictable in both non-breast feeding and non-exclusive breast feeding women.8 Among 222 pregnancies estimated in 1,000 women aged 15–44 in East Africa, 39% of the pregnancies were unintended. One-third of unintended pregnancies in Africa were terminated by induced abortion.9 Each year, over half a million women die from complications of pregnancy and childbirth, and 99% of these women live in the developing world.10 In Ethiopia, 41.5% of the total pregnancies resulted from unintended pregnancy and of which 20.2% were from breast feeding mothers.11
The postpartum period is the time where the great unmet need will occur. In Ethiopia, 45.2% of postpartum mothers had an unmet need for modern contraceptives, of which 54.9% had an unmet need for spacing and 45.1% for limiting the number of children.12
Studies conducted on the determinants of postpartum IUCD across the world are extremely rare. Besides the underlining problem and as to the best of our knowledge; few studies have evaluated the determinants of postpartum IUCDs among mothers who gave birth at public health facilities. Therefore, this study assessed determinants of postpartum IUCD utilization among mothers who gave birth in Gamo zone public health facilities, southern Ethiopia.
Methods
Study Setting
The study was done from March 1 to April 15, 2019 at Gamo zone public health facilities. Previously the zone was termed as Gamo Gofa zone until the end of 2010 Ethiopian Fiscal Year (EFY). The Gamo zone is located 505km far from Addis Ababa and 275 km from Hawassa. Based upon the 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), the 2017 population projection for the Gamo Gofa zone was 2,043,668 (male: 1,013,533; female: 1,030,135); with an area of 18,010.99 square kilometers. Gamo Gofa has a population density of 144.68. While 157,446 or 9.88% are urban inhabitants, a further 480 or 0.03% are pastoralists. Currently the Gamo zone has five hospitals (one general and four primary) and 51 health centers. Among those health facilities only nine health facilities (three hospitals and six health centers) were providing postpartum IUCD service.
Study Design and Population
- A facility based unmatched case-control study design was used. The source of population was all mothers who gave birth at Gamo zone health facilities during the data collection period. Cases were all mothers who agreed to use PPIUCD after vaginal or intra-cesarean birth. Controls, were those mothers who were eligible for postpartum IUCD insertion but refused it and also did not utilize implants or bilateral tubal ligation.13 All mothers who had given birth at Gamo zone public health facilities where PPIUCD service is being given were eligible for inclusion in the study. Besides, WHO medical eligibility criteria for PPIUCD was observed and, women suffering from the following conditions, anemia (hemoglobin<10 g/dL, unresolved postpartum hemorrhage, PROM>18 hours, active genital tract infections, distorted uterine cavity, fibroid, congenital malformation of the uterus, obstructed labor14 and women who were unable to respond due to illness or disability were excluded from the study.
Sample Size and Sampling Techniques
Epi Info STATCALC was used to calculate the sample size by considering the following assumptions:- Time of counseling about PPIUCD, i.e., counseling during ANC follow-up as a determinant factor among cases and controls; 28.7% of cases and 17.6% of controls had counseling,13 95% two-sided confidence level, with a power of 80, one to two case to control ratio and odds ratio calculated= 1.771. The final maximum sample size taken from the Epi- Info output was 536. Thus 179 cases and 357 controls were recruited.
All nine public health facilities that provide PPIUCD services were included in the study. The total sample size was proportionally allocated to each of the nine health facilities based on the 2018 total delivery report. Cases were recruited successively in nine facilities that are providing PPIUCD service. While, controls were selected by using the simple random sampling method. Mothers in the delivery registration book who were eligible for PPIUCD but declined it were selected randomly as a control.
Operational Definition and Definition of Terms
PPIUCD utilization: A mother who used PPIUCD either vaginally or intra-cesarean after placenta removal within 10 minutes but not more than 48 hours.
Inter pregnancy period: the time period between deliveries of the last pregnancy to the onset of new conception.
Knowledge: the general information that respondents recognize about PPIUCD as a method of contraception and its benefits. It was measured by computing the mean value of 8eight questions (awareness with regards to IUCD for contraception, its duration, reversibility, site of placement and related questions) and classified as having a good knowledge (if the respondent replied greater than the mean mark of knowledge assessing questions) or not having a good knowledge (if the respondent replied less than the mean score for knowledge assessing questions).
Attitude: the general perception of participants that reflect and act about PPIUCD use. It was calculated by computing the mean value of seven questions (perception regarding insertion and removal of IUCD, misconceptions, myths and rumors assessing questions) and classified as a favorable attitude (if the respondent replied greater than the mean value of attitude assessing questions) or unfavorable attitude (if the respondent replied less than the mean value of attitude assessing questions).
Measurements
The data were collected using a structured interviewer administered questionnaire. The questionnaire was prepared by reviewing different published literatures for related factors of postpartum IUCD utilization and adapted to the objective of this study. Eight clinical nurses with data collection experience gathered the data. Two qualified midwives supervised the work. Training on data collection was provided.
The questionnaire was primarily prepared in English. The English version was translated to Amharic and Gamogna (the local languages) and translated back to English to ensure internal consistency. Data quality was ensured during collection, coding, entry and analysis. An ongoing monitoring and evaluation was made during the data collection. Moreover, the questionnaire was pre-tested (5% of the sample) in Arba Minch General Hospital 15 days prior to the actual data collection time. This was to make sure of the simplicity, clarity and logical arrangement of the questions. Based on the pre-test findings, the necessary modifications were employed. In addition, the supervisors and principal investigators supervised the whole activity of the data collection process and checked the filled questionnaires every day for completeness, correctness and necessary feedback was provided to the data collectors.
Data Processing and Analysis
Epi-Info version 3.5.1 was used for data coding, cleaning and entry. After entry the data were exported to statistical package for social science (SPSS) version 25 for analysis. Data were reported in the form of graphs, charts, tables and texts were used to report the data. A 2×2 table was computed to see the occurrence of event among cases and controls. Bivariate and multivariable logistic regression analysis was performed to assess the association between dependent and independent variables. Variables with a p-value <0.2 in the bivariate analysis were fitted to a multivariable logistic regression model.15 Variables with a p-value <0.05 in the final model were considered as statistically significant.
All the necessary assumptions for the application of multivariable logistic regression were maintained. Hosmer and Lemeshow’s goodness-of-fit test (p>0.05) was checked to see model fitness. Multi co-linearity and confounding effect had been checked. The variables without multi co-linearity were entered into the multivariable model. Only variables with p value < 0.05 were kept in the final model. Finally, odds ratio with its 95% confidence interval (CI) were used to show the degree of association between the independent variables and postpartum IUCD utilization.
Result
Socio-Demographic and Economic Characteristics of the Study Participants
A total of 510 participants (175 cases and 335 controls) were involved in the present study yielding a response rate of 95.1%. The mean age of cases was 28.13±4.66 SD and 26.87±5.05 SD for controls. Fifty-one (29.1%) cases and 191 (57%) controls were from rural areas. All cases and 323 (96.4%) controls were married. Regarding mother’s educational status, about a third of cases (32%) and controls (47.2%) had no formal education. With regard to partners’ educational status, majority of the cases (46.1%) have an education at college level and above, while 121 (36.1%) controls had no formal education. Looking at the socio-economic status of the participants, majority of cases (34.9%) were found in the fourth quintile and controls (30.1%) were found in the lowest quintile (Table 1).
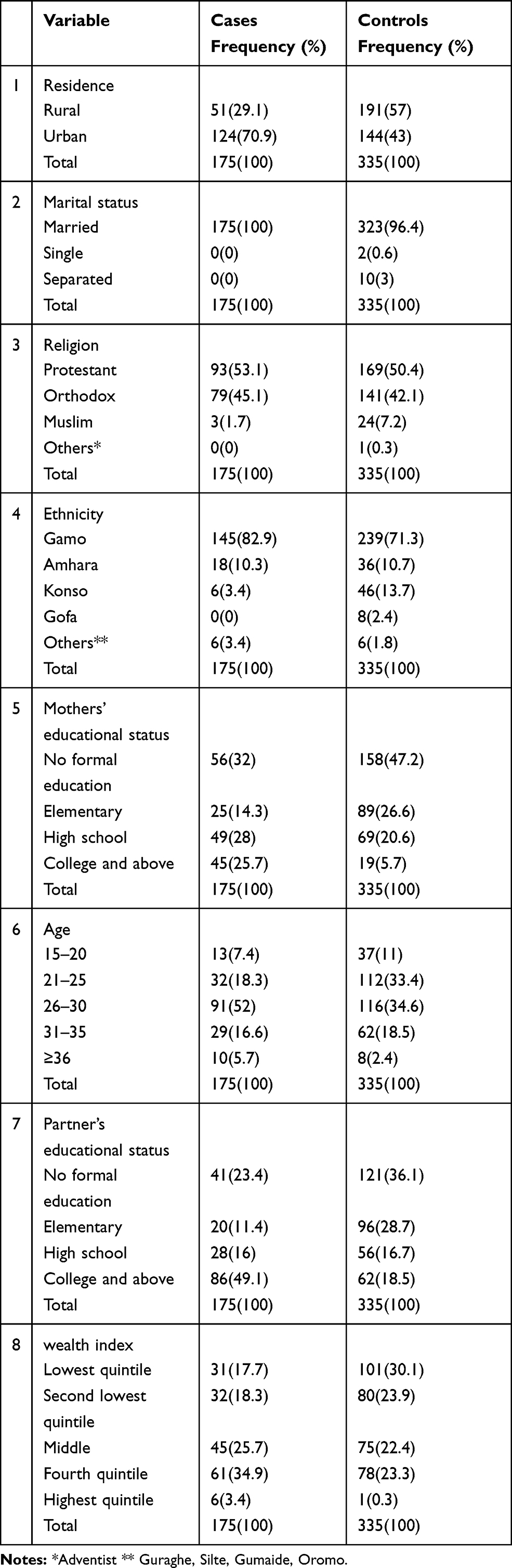 |
Table 1 Distribution of Socio-Demographic Characteristics of Respondents, Gamo Zone Public Health Facilities, March1 to April 15 2019 |
Obstetrics Characteristics of the Study Participants
The majority of the cases 142 (81.2%) and 245 (73.1%) controls were multigravida. One hundred fifty-four (88%) cases and 308 (91.9%) controls had ANC follow-up in their current pregnancy. Out of the women who started ANC follow-up, one hundred forty-six (93.6%) of cases and 423 (90.2%) controls had ANC follow-up of 3–4 times. The admission history during their last pregnancy was 30 (17.1%) of the cases and 82 (24.5%) of the controls had admission to a health facility. Unplanned pregnancy was reported in 43 (24.6%) of the cases and 84 (25.1%) controls. Greater than or equal to five children among the cases was 23 (13.1%) and 46 (13.7%) for the controls.
Birth by spontaneous vaginal delivery was reported among 133 (76%) of the cases and 236 (70.4%) of the controls (Figure 1). Majority of the cases 162 (92.6%) and controls 319 (95.2%) gave birth at a gestational age of 37–42 weeks. Birth intervals of 1–2 years was reported among the cases 19 (13.4%) and control 72 (29.5).
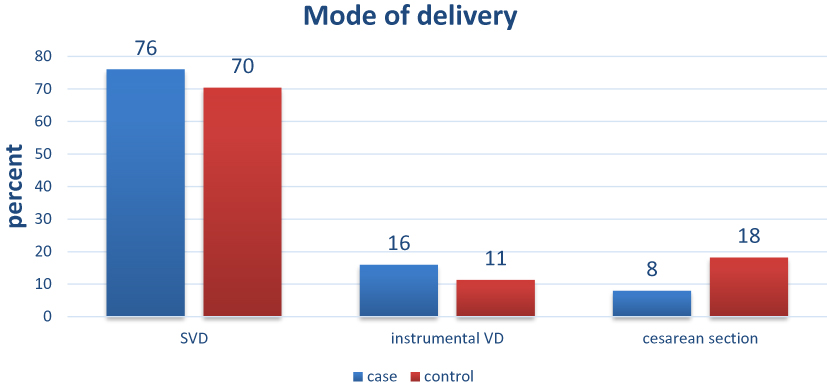 |
Figure 1 Distribution of modes of delivery within PPIUCD utilization, Gamo zone public health facilities, march1 to April 15 2019. |
Reproductive Health History of the Study Participants
The majority of the cases 172 (98.4%) and controls 317 (94.6%) had heard about family planning methods. However 46 (26.3%) of the cases and 101 (31.8%) of the controls had not used any modern contraceptives methods before their last pregnancy.
Regarding the type of modern contraceptive used by the participants before their current pregnancy, 34 (26.4%) of cases and only 4 (1.8%) controls used IUCD before their last pregnancy (cases = 129 and controls = 221). Fifty-seven (43.5%) cases and 16 (7.2%) controls had ever used IUCD. Almost all of cases (99.7%) and 76% of controls had received counseling and had heard about postpartum IUCD. The majority of cases (62%) and controls (53%) had received counseling about postpartum IUCD after delivery (Figure 2).
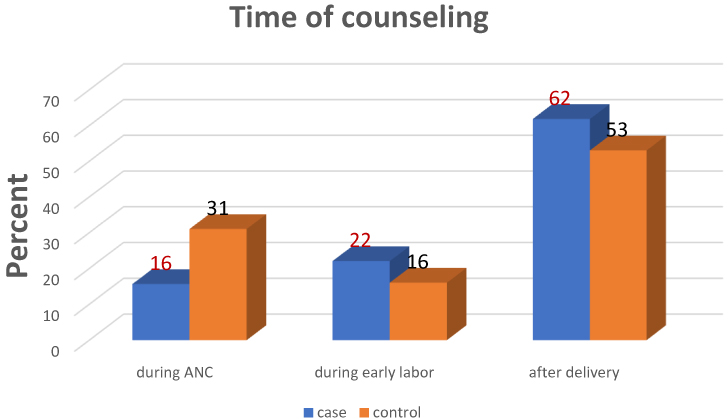 |
Figure 2 Timing of counseling for PPIUD of participants, Gamo zone public health facilities, March 1 to April 15 2019. |
Individual Client Related Factors
Almost all (170 [97.1%]) cases and 80 (23.7%) controls had a favorable attitude and 158 (90.3%) cases and 110 (32.8%) controls had good knowledge about postpartum IUCD. The majority of the cases (136; 77.7%) and only 49 (14.6%) controls had partner support for postpartum IUCD use.
Determinants of PPIUCD Utilization
Multiple logistic regression was performed to assess determinants of socio-economic and demographic variables, obstetric history and behavioral variables on postpartum IUCD utilization. The independent variables which associated with dependent variable in bi-variable analysis at P-value of less than 0.20 were included in the final model. A total of 15 variables entered for the final model while only five variables were significant. Variables (birth interval, fertility plan, timing of counseling, pregnancy plan, and partner support) were found to be significant.
Mothers who have partner support for IUCD insertion were ten times more likely to utilize PPIUCD than those do not have partner support (AOR [95 CI]: 10 [4.03, 24.3]).
Mothers who had a birth interval of 1–2 years and 3–5 years were about 12 and 10 times more likely to utilize PPIUCD than those who had greater than five years interval (AOR [95 CI]: 12.01 [1.5, 97.7], and 9.7 [1.7, 55.1]) respectively. Mothers who are spacers are four times more likely to utilize PPIUCD than limiters (AOR [95 CI] 4[1.44,10.84]).
The odds of mothers who were counseled during early labor were around 88% less likely to utilize PPIUCD than those who were counseled during ANC (AOR [95 CI]: 0.125 [0.034, 0.46]). The odds of mothers whose current pregnancy was planned were 4.4 times more likely to utilize PPIUCD than those who did not plan (AOR [95 CI]: 4.43 [1.4, 13.8]) (Table 2).
 |
Table 2 Multiple and Bivariate Logistic Regression Result of PPIUCD Utilization with Different Independent Factors, Gamo Zone Public Health Facilities, March1 to April 15 2019 |
Discussion
Most of mothers in developing countries are not interested in conceiving within two years after their delivery. But they are not practicing the contraception that prevents a pregnancy at this time. The postpartum period is the best time to attain reproductive health plan of an individual/couple which is convenient for the mothers and health professionals. Even though postpartum IUCD is the most effective, safest, and reliable contraceptive method, it is not being utilized widely. This study assessed the determinant factors of PPIUCD utilization among mothers who gave birth in Gamo zone public health facilities, Southern Ethiopia. Birth interval, fertility plan, timing of counseling, pregnancy plan, and partner support were found to be determinant factors for utilization of PPIUCD.
In our study mothers who had partner support for IUCD insertion during the postpartum period were more likely to utilize PPIUCD than mothers who did not have partner support. This finding is supported by a research conducted at Saint Paul’s Hospital Millennium Medical College, Addis Ababa. They reported that mothers who had partner support for immediate postpartum contraceptive utilization were 1.3 times more likely to use it than those who did not have partner support.16 A similar finding was obtained in the study carried out at Arba Minch Zuria wereda.17 The reason might be due to male partner’s dominance in decision-making over the mother not to be able to decide by themselves. This might suggest that male involvement is crucial for family planning services here in developing countries like Ethiopia.
In this study mothers who were counseled during early labor were less likely to utilize PPIUCD than those who were counseled during antenatal care. This finding is similar to studies conducted in different regions of India.18,19 This might be that mothers undergoing labor are much more concerned about the birth outcome than contraception. In addition, at this time mothers do not have the time to discuss with their partner. However, antenatal care counseling can solve such constraints. The mothers have the time to discuss their fears about postpartum IUCD and discuss their reproductive health plan with their partners.
Mothers who were spacers in their fertility plan were more likely to utilize PPIUCD than those who were limiters. This finding is contradicted with a study conducted in Sidama zone, south Ethiopia20 and Hossana town.21 The difference among studies might be due to a difference in the study design and the study population. This might be due to reversibility and long acting nature of IUCD enabling mothers to have children when they want. On the other hand, mothers who have the desire to limit number of children may chose a permanent method of contraception.
In this study mothers who had a birth interval of 1–2 and 3–5 years had a better PPIUCD utilization than birth interval of greater than five years. This finding is supported by a study done in M L BMedical college Jhansi, India.22 This might be explained by women who had a short pregnancy may regret not having a long acting and reversible method of contraception and this might initiate them to opt in than who had a long pregnancy period.
Mothers whose current pregnancy was planned are more likely to utilize postpartum IUCD than those whose pregnancy was not planned. This might be that a previously to chose planned pregnancy experience might guide them when the next pregnancy will come. Therefore they might have chosen long acting, reversible contraceptive for their plan and postpartum IUCD could be their best choice.
Strength of the Study
The inclusion of facilities that are providing postpartum IUCD service in the Zone within the study.
Limitations of the Study
The study was facility-based and lacks the observation insight of housing conditions related to the wealth index. Besides, facility-based study design may be prone to be bias confounded by other factors.
Conclusion
In this study birth interval, fertility plan, timing of counseling, pregnancy plan, and partner support were found to be determinants for utilization of PPIUCD.
Recommendation
Counseling about family planning utilization is a very important aspect for service delivery. Therefore, health professionals working at ANC are required to give adequate time for discussion on the pregnancy and fertility plan by incorporating partners.
The Federal Ministry of Health needs to integrate postpartum IUCD with other MCH services so as to incorporate with other counseling component in the form of flow chart.
Gamo zone hospitals and health centers should mobilize male involvement in family planning for improved uptake of PPIUCD in the zone.
Gamo zone health department and Woreda health offices should work on community education to increase women's awareness towards PPIUCD in order to achieve their pregnancy and fertility plan.
Abbreviations
ANC, antenatal care; BSc, Bachelor of Science; CI, confident interval; EDHS, Ethiopian Demographic Health Survey; FOMH, Ethiopian Federal Ministry Of Health; HEWs, health extension workers; IUD/IUCD, intra uterine device/intra uterine contraceptive device; PPFP, postpartum family planning; PPIUD/PPIUCD, postpartum intra uterine device/postpartum intra uterine contraceptive device; PROM, premature rapture of membrane; SD, standard deviation; SES, socio economic status; SPSS, statistical package for social science; WHO, World Health Organization.
Data Sharing Statement
Full data set and other materials relating to this study can be obtained from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
Ethics approval was obtained from the Institutional Research Ethics Review Board (IRB) Office, College of Medicine and Health Sciences Arba Minch University. Following the approval, official letter of cooperation from zonal health department was obtained to conduct the study in the nine health facilities’ providing postpartum IUCD. Data were collected after taking verbal consent according to the declaration of Helsinki from each participant. Purpose of study was explained and confidentiality was assured. Mothers whose age was less than 18 were considered to be early mature and gave oral informed consent. This is acceptable by Institutional Research Ethics Board (IRB) Office of Arba Minch University.
Funding
This research work is funded by Arba Minch University.
Disclosure
The authors declare that there is no financial and non-financial conflict of interests regarding the publication of this paper.
References
1. WHO. Programming Strategies for Postpartum Family Planning. World Health Organization (wwwwhoint). 56. 2013.
2. ACOG. Immediate postpartum long-acting reversible contraception. Am Coll Obstetric Gynecol. 2016;670(11):6.
3. Nisha S, Sathi MS, Cp V. Post-placental insertion of IUCD in a tertiary care centre - Acceptance and safety. J Evolution Med Dent Sci. 2016;5(80):5933–5938. doi:10.14260/jemds/2016/1340
4. Jairaj S, Cross Sectional SDA. Study on Acceptability and Safety of IUCD among Postpartum Mothers at Tertiary Care Hospital, Telangana. J Clin Diagnostic Res. 2016;10:1.
5. Jain N, Varshney K, Vaid NB, Guleria K, Vaid K, Sharma N. Acceptability, continuation and satisfaction of postpartum intrauterine contraceptive device (PPIUCD) and delayed insertion: a comparative study. Int J Reproduct Contraception Obstetrics Gynecol. 2017;6(1):8. doi:10.1002/ijgo.12086
6. Mohamed SA, Kamel MA, Shaaban OM, Salem HT. Acceptability for the Use of Postpartum Intrauterine Contraceptive Devices: assiut Experience. Med Principles Pract. 2003;12(3):170–175. doi:10.1159/000070754
7. Gonie A, Worku C, Assefa T, Bogale D, Girma A. Acceptability and factors associated with post-partum IUCD use among women who gave birth at bale zone health facilities, Southeast-Ethiopia. Contraception Reproduct Med. 2018;3(1):16. doi:10.1186/s40834-018-0071-z
8. Xu JX, Reusche C, Burdan A. Immediate postplacental insertion of the intrauterine device: a review of Chinese and the world’s experiences. Adv Contraception. 1994;10(1):71–82. doi:10.1007/BF01986532
9. Singh S, Sedgh G, Hussain R. Unintended Pregnancy: worldwide Levels, Trends, and Outcomes. Stud Fam Plann. 2010;41(4):4. doi:10.1111/j.1728-4465.2010.00250.x
10. Klima CS. Unintended pregnancy: consequences and solutions for a worldwide problem. J Nurse Midwifery. 1998;43(6):483–491. doi:10.1016/S0091-2182(98)00063-9
11. Olana R, Mohammedamin A, Abebe TW. Unintended pregnancy and associated factors among pregnant women in Arsi Negele Woreda, West Arsi Zone, Ethiopia. BMC Res Notes. 2018;11(1):671. doi:10.1186/s13104-018-3778-7
12. Tegegn M, Arefaynie M, Tiruye TY. Unmet need for modern contraceptives and associated factors among women in the extended postpartum period in Dessie town, Ethiopia. Contraception Reproduct Med. 2017;2(1):21. doi:10.1186/s40834-017-0048-3
13. Pradhan S, Kshatri JS, Sen R, Behera AA, Tripathy RM. Determinants of uptake of post-partum intra-uterine contraceptive device among women delivering in a tertiary hospital, Odisha, India. Int J Reproduct Contraception Obstetrics Gynecol. 2017;6(5):2017–2020. doi:10.18203/2320-1770.ijrcog20171968
14. Project TA. The Postpartum Intrauterine Device: A Training Course for Service Providers. Participant Handbook. New York: EngenderHealth. New York: EngenderHealth; 2008.
15. Bursac Z, Gauss H, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3(1):17. doi:10.1186/1751-0473-3-17
16. Belay LMB. Factors affecting long-term and permanent contraceptive uptake among immediate post-partum mothers at saint paul’s hospital millennium medical College, Addis Ababa, Ethiopia: A Cross-Sectional Study. Ethiopian J Reproduct Health. 2018;10(2).
17. Gultie T, Hailu D, Workineh Y. Predictors of long acting contraceptives utilization among reproductive age women in Arba Minch Zuria district, Ethiopia. Qual Prim Care. 2016;24(1):17–22.
18. Agarwal N, Gupta M, Sharma A, Arora R. Antenatal counselling as a tool to increase acceptability of postpartum intrauterine contraceptive device insertion in a tertiary care hospital. Int J Reproduct Contraception Obstetrics Gynecol. 2015;4(4):1137–1141. doi:10.18203/2320-1770.ijrcog20150442
19. S RR D, Agadi N. Determinants of Post - partum contraception practices in urban slums of central Karnataka, India.. Indian J Comm Health. 2016;28(3):280–285.
20. Bezabih LT, Abera M, Fikru C. Utilization of immediate post-partum intra uterine contraceptive device and associated factors: a facility based cross sectional study among mothers delivered at public health facilities of sidama Zone, South Ethiopia. J Pregnancy Child Health. 2017;4:3.
21. Earsido A, Gebeyehu A. Determinants of long acting and permanent contraceptive methods utilization among married women in hossana town, southern ethiopia: a case - control study. J Preg Child Health. 2015;2:165.
22. Gautam R, Arya K, Kharakwal S, Singh S, Trivedi M. Immediate PPIUCD Cu T 380A Complication, Safety. Overview Of Immediate Ppiucd Application In Bundelkhand Region; 2014:5045.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.