Back to Journals » Open Access Emergency Medicine » Volume 13
Determinants of Nurse Preparedness in Disaster Management: A Cross-Sectional Study Among the Community Health Nurses in Coastal Areas
Authors Emaliyawati E ![]() , Ibrahim K
, Ibrahim K ![]() , Trisyani Y
, Trisyani Y ![]() , Mirwanti R
, Mirwanti R ![]() , Ilhami FM, Arifin H
, Ilhami FM, Arifin H ![]()
Received 3 June 2021
Accepted for publication 19 July 2021
Published 5 August 2021 Volume 2021:13 Pages 373—379
DOI https://doi.org/10.2147/OAEM.S323168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Etika Emaliyawati,1,2 Kusman Ibrahim,3 Yanny Trisyani,1 Ristina Mirwanti,1 Fitri Muthiara Ilhami,4 Hidayat Arifin3
1Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 2Doctoral Study Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 3Department of Medical-Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 4Under-Graduate Program, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Etika Emaliyawati
Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia
Tel +62 817-222-086
Fax +62 22 7795596
Email [email protected]
Purpose: Because Indonesia has a high risk of natural disasters, nurse preparedness is necessary to reduce and prevent deaths in the aftermath of such disasters. The aim of this study was to determine the factors associated with nurse preparedness in disaster management among a sample of community health nurses in coastal areas.
Patients and Methods: A cross-sectional study was undertaken from May to August 2020. The sample consisted of 142 nurses who worked at six Public Health Centers in Pangandaran, West Java, Indonesia. Participants were recruited using the total sampling technique. The data were collected using the Emergency Preparedness Information Questionnaire and analyzed using Chi-Square and binary logistic regression.
Results: Of the 142 respondents, 54.24% had a high level of preparedness. Multivariate analysis showed that nurses with higher levels of preparedness had worked between 6 and 10 years (adjusted odds ratio (AOR): 12.755, 95% confidence interval (CI): 2.653– 61.314). Respondents who lacked disaster training were less likely to have a high level of disaster preparedness (AOR: 4.631, 95% CI: 1.604– 13.367). Respondents who had never served as disaster volunteers were also less likely to have disaster preparedness (AOR: 0.18, 95% CI: 0.053– 0.616).
Conclusion: With nearly half of the respondents (45.77%) having a low level of disaster preparedness, this topic needs more attention from the government and healthcare workers. Several actions are needed to improve community nurses’ disaster preparedness: providing them with routine disaster-related training, encouraging them to serve as volunteers in various disaster conditions, and offering them useful disaster-related information.
Keywords: nurses, disaster, disaster management, coastal area, preparedness
Introduction
The trend of disaster events in Indonesia continues. The National Agency for Disaster Management Indonesia recorded an increase in the incidence of disasters from August 2018 to August 2019 of around 7.3%. From January to August 2019, the average number of people affected by a disaster was 2.5% of the population.1 In the West Java province of Indonesia, the Pangandaran Regency ranks sixth in earthquake and tsunamis risk. These types of disasters result in injuries, missing people, deaths, displaced families, and economic problems.2 Frequent disasters require disaster management efforts that involve all possible parties, including nurses. Because nurses are the largest and most important group of healthcare providers in disaster management, their competencies need to be continually assessed and improved.3–5 Given these facts, disaster management preparedness remains a strong area of concern for nurses in disaster-prone areas.
Disaster management preparedness is a very important professional skill for nurses, as nurses with a strong sense of readiness can provide assistance to disaster victims.6 Furthermore, nurses can perform comprehensive relief management services, such as mapping the disaster location, providing disaster mitigation, triaging patients, and organizing first aid involving cross-sector collaboration and interdisciplinary professional teams.7–9 Nurse preparedness can be measured using the following eight dimensions: triage and basic first aid; detection; accessing critical resources and reporting; the incident command system (ICS); isolation, quarantine, and decontamination; psychological issues; epidemiology and clinical decision-making; and communication and connectivity.10 Another recent study reported that nurses with emergency preparedness competencies are more likely to have professional competence in disaster responses, maintain personal disaster preparedness, and report to work after a disaster.11
One of the roles of community public health centers (PHCs) is to minimize the effects of disasters on the population. Despite nurses being primarily responsible for most (72.97%) PHC disaster programs, previous study results indicated that 50% of PHC nurses had low disaster preparedness.12 Furthermore, nurses’ service capabilities for treating disaster victims at PHCs were limited to caring for victims flagged as green during triage (84.21%).13
Another study showed that high levels of readiness in nurses serving in disasters are related to nurse age, experience,14 knowledge,15 responsibilities,16 support from the government,17 and training.18 In addition, the average level of nurse preparation to respond to disaster conditions was low. Results from several other studies indicated that many nurses did not know the tasks required during disaster or post-disaster conditions.19–22 Providing nurses with disaster management training will increase their ability to handle disaster conditions. Other factors that can affect nurse preparedness include work experience, length of time spent preparing to face disasters, disaster volunteer experience, and access to information sources. Unfortunately, there is a lack of studies about the disaster preparedness of nurses working in disaster-prone coastal areas of Indonesia. Therefore, this study aimed to determine the factors associated with disaster management preparedness among community health nurses in coastal areas.
Patients and Methods
Study Design
A cross-sectional design was used for this study.
Setting and Sample
The study was conducted from May to August 2020 in six PHCs in the coastal areas of Pangandaran, West Java, Indonesia. The sample consisted of 142 community health nurses who were recruited using the total sampling technique. The inclusion criteria were community health nurses with a minimum of a diploma in nursing education who were employed at one of the PHCs in the coastal areas and had worked for a minimum of three months. The exclusion criteria were community health nurses who were on leave, too busy with their duties to participate in the study, or were not able to complete the study. The data were collected using questionnaires.
Variables
The independent variables were age, education level, gender, number of years working as a nurse (referred to as work history), disaster training, disaster preparedness knowledge sources, disaster volunteering, and disaster management experience. The age variable was divided into four categories: 21–25 years, 26–35 years, 36–45 years, and >45 years. Nursing education level was divided into three categories: diploma, Bachelor’s degree, and professional nursing education. Respondent gender was classified as either male or female. Work history was divided into four categories: ≤1 year, 2–5 years, 6–10 years, and >10 years. Responses about disaster training were divided into one of two categories: yes (having any level of training) or no (having no training). Preparedness knowledge sources were classified into the following categories: lectures, seminars, training, simulations, participation, and other methods. Disaster volunteering history was classified as either yes (have served as a volunteer) or no (have never served as a volunteer). Finally, disaster management was classified into ever (having provided disaster management services) or never (having provided these services).
The Emergency Preparedness Information Questionnaire (EPIQ) was used in this study to determine the dependent variable, preparedness level.23 The EPIQ assesses eight dimensions of preparedness: triage and basic first aid; detection; accessing critical resources and reporting; the ICS; isolation, quarantine, and decontamination; psychological issues; epidemiology and clinical decision-making; and communication and connectivity. The nurse preparedness variable was divided into two categories: Low (if the value was less than the mean) or High (if the value was greater than the mean). Each category was coded as Low = 0 and High = 1. The Cronbach’s alpha result was 0.951.
Data Analysis
To manage and analyze the data, we used STATA/MP version 16.1 (Mac). Chi-Square and Binary Logistic Regression were used to analyze the factors associated with nurse disaster management preparedness among the sample of community health nurses from the coastal areas. The significance value was p < 0.05, and the adjusted odds ratio (AOR) had a 95% confidence interval (CI).
Ethical Considerations
We received approval from the Health Ethics Commission of Universitas Padjadjaran (439/UN6.KEP/EC/2020) on April 30, 2020. Respondents were informed about the study objectives and provided informed consent and this study was conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and the study did not have the potential to harm the participants physically or mentally.
Results
The demographic data showed that more than half the participants (54.23%) had a high level of disaster preparedness and 45.77% had a low level of preparedness. One-third of the respondents were 26–35 years of age. Regarding education, 50% had either a diploma or professional nursing education and most had worked for more than 10 years. A majority of respondents had attended disaster training, served as a disaster volunteer, and gained knowledge about disasters while attending lectures. Apart from that, many respondents had never provided disaster management services.
The bivariate analysis conducted using Chi-Square showed that the variables of work history (X2: 13.784; p < 0.01), disaster training (X2: 16.986; p < 0.01), knowledge sources (X2: 13.972; p < 0.05), disaster volunteering (X2: 9.574; p < 0.01), and disaster management experience (X2: 5.459; p < 0.05) all had a significant correlation with nurse preparedness. In contrast, age, education level, and gender were not correlated with preparedness (Table 1).
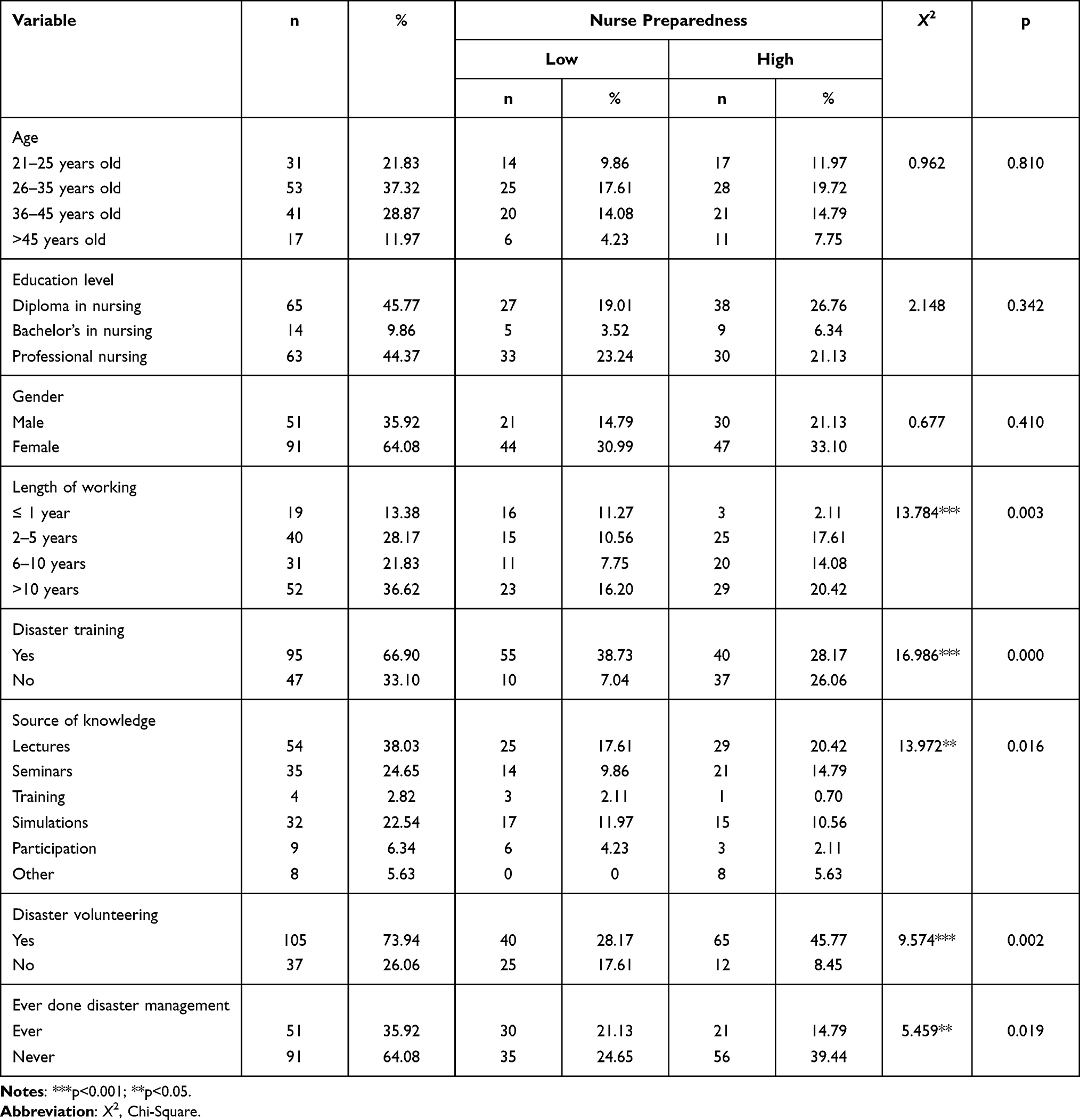 |
Table 1 Respondents’ Characteristics and Bivariate Analysis of Nurse Preparedness in Disaster Management Among the Community Health Nurses in the Coastal Areas (n=142) |
Multivariate analysis using binary logistic regression showed that nurses with a work history spanning 6–10 years were 12.755 times more likely to have a high level of preparedness than those with a work history of ≤1 year (AOR: 12.755; 95% CI: 2.653–61.314). Interestingly, nurses with no disaster training history were 4.631 times more likely to have a high level of preparedness than were those with such training (AOR: 4.631; 95% CI: 1.604–13.367). Finally, respondents who had never served as disaster volunteers were 0.18 times less likely to have a high level of preparedness than were those who had served as volunteers (AOR: 0.18; 95% CI: 0.053–0.616; Table 2).
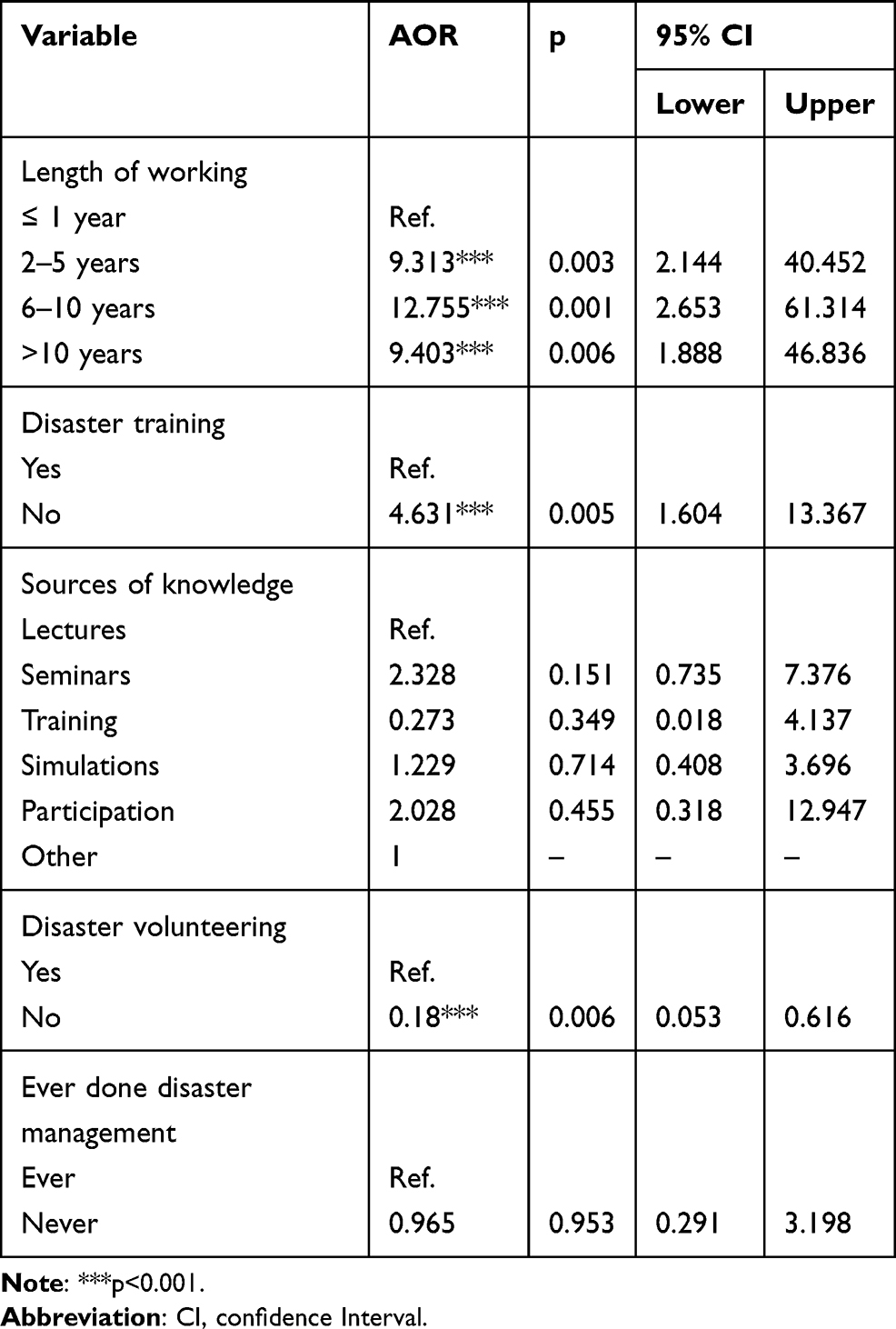 |
Table 2 Multivariate Analysis of Nurse Preparedness in Disaster Management Among the Community Health Nurses in Coastal Areas (n=142) |
Discussion
It is important to consider the disaster preparedness of nurses working in coastal areas that face disasters more frequently than non-coastal areas. The results of this study indicated that almost half of the nurses surveyed had a low level of disaster preparedness. This finding is consistent with study results showing low to moderate readiness among nurses in Cambodia, China, Laos, Nepal, and the Solomon Islands.24 Likewise, in the Philippines, three-quarters of nurses (80%) stated that they were not fully prepared to work during a disaster.25
In this study, we found that three factors were significantly correlated with preparedness among the nurses: work history, disaster training history, and service as a disaster volunteer. Disaster nurses are defined as nurses who have the expertise to help victims by minimizing life-threatening health risks.26 Given this definition, we can surmise that nurses are expected to be able to adapt to their environment and disaster conditions.23
The results of this study showed that work history had a significant relationship with disaster preparedness. This finding is likely due to the fact that these nurses gained a great deal of disaster management information and knowledge from working and living in a coastal area. The ideal work history is in the range of 6–10 years, a period when nurses are still active and enthusiastic at work and have good cognitive abilities. This finding is in line with that of a previous study showing that nurses with the ideal length of work history can have increased productivity, performance, and ability in providing care.27–30 However, it should be noted that nurses who have worked for a long time with a heavy workload can experience decreased productivity due to boredom and burnout when working as a disaster nurse.31,32
One surprising finding of this study was that nurses who had not participated in disaster training had a greater likelihood of having a higher level of disaster preparedness than those who had engaged in such training. This result may be due to the fact that the provided training was not effective enough to improve nurses’ disaster preparedness. This finding is consistent with previous studies indicating that a training approach that uses easy-to-understand methods is likely to be more effective.33,34 Based on this finding, it is important that future research be conducted to evaluate common disaster training methods. Our respondents indicated that most of their knowledge came from lectures, seminars, and simulations.
From these findings, we learned that nurses who have never volunteered during disaster conditions have a lower level of disaster preparedness. Conversely, nurses with volunteer experience have a higher level of self-confidence in dealing with disasters. These results are similar to those of previous research showing that experience dealing with and providing health services in disaster situations conveys a higher level of preparedness compared with nurses who have never been directly involved in disaster conditions.35 In addition, experience as a volunteer in a disaster area can improve nurses’ actions and preparedness levels.36 Indeed, disaster experience is one of the main predictors of nurse competence and preparedness.24 By providing opportunities for nurses to volunteer in disaster conditions, PHCs can help them improve their abilities and the quality of the services they provide in such conditions.
This study provides new information indicating that—due to the proportion of study respondents with low preparedness levels—efforts that address the salient factors are needed to increase the disaster preparedness among nurses in coastal areas. For example, nurses’ history of work experience, disaster training, and volunteering can serve as the basis for further policy formation to address this crucial issue. However, because this research was limited to specific areas in the Pangandaran Regency, future research covering more areas is needed to further explicate the factors that affect nurses’ disaster preparedness in coastal areas.
Conclusion
Almost half of the study participants had low levels of disaster preparedness. This finding requires serious attention, as the research was conducted in a disaster-prone location. Strengthening the cooperation from the government and PHCs to increase nurses’ capacity to work during disasters—through training and opportunities to volunteer in disaster conditions—are necessary to improve the ability of nurses to work during disasters. We suggest two specific methods for addressing this issue: offering nurses routine disaster-related training that involves them working as volunteers in various disaster conditions, and providing effective disaster-related information through seminars, flyers, and other media.
Funding
The study was funded by Universitas Padjadjaran with the Doctoral Dissertation Research Program scheme number 1427/UN6.3.1/LT/2020.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Badan Nasional Penanggulangan Bencana [National Board for Disaster Management]. Infografis Data Bencana Periode 1 Januari 2019 Hingga 31 Desember 2019 [Disaster Data Infographic Period 1 January 2019 to 31 December 2019]; 2019. Available from: https://bnpb.go.id/berita/2020-01-20-infografis-update-bencana-31-des-2019-per20jan2020jpg. Accessed November 13, 2020. Indonesian.
2. Substance Abuse and Mental Health Services Administration. Disaster Technical Assistance Center Supplemental Research Bulletin. Greater Impact: How Disasters Affect People of Low Socioeconomic Status; 2017. Available from: https://www.samhsa.gov/sites/default/files/programs_campaigns/dtac/srb-low-ses.pdf.
3. Pourvakhshoori N, Norouzi K, Ahmadi F, Hosseini M, Khankeh H. Nursing in disasters: a review of existing models. Int Emerg Nurs. 2017;31:58–63. doi:10.1016/j.ienj.2016.06.004
4. Al-Maaitah R, Conlan L, Gebbie K, et al. Core Competencies in Disaster Nursing; Version 2.0. International Council of Nurses; 2019. Available from: https://www.icn.ch/sites/default/files/inline-files/ICN_Disaster-Comp-Report_WEB.pdf.I
5. Aitsi-Selmi A, Egawa S, Sasaki H, Wannous C, Murray V. The Sendai framework for disaster risk reduction: renewing the global commitment to people’s resilience, health, and well-being. Int J Disaster Risk Sci. 2015;6(2):164–176. doi:10.1007/s13753-015-0050-9
6. Xia SS, Yang BX, Pm A. Application and effects of a disaster nursing simulationtraining for Chinese undergraduates. Nurse Educ Pract. 2018;28:156–162.
7. Pilemalm S, Mojir KY. ICT enabled cross-sector collaboration in emergency response: emerging forms of public-sector network governance. Int J Emerg Manag. 2020;16(3):249. doi:10.1504/IJEM.2020.113936
8. Xue C, Shu Y, Hayter M, Lee A. Experiences of nurses involved in natural disaster relief: a meta‐synthesis of qualitative literature. J Clin Nurs. 2020;29(23–24):4514–4531. doi:10.1111/jocn.15476
9. Al Harthi M, Al Thobaity A, Al Ahmari W, Almalki M. Challenges for nurses in disaster management: a scoping review. Risk Manag Healthc Policy. 2020;13:2627–2634. doi:10.2147/RMHP.S279513
10. Wisniewski R, Dennik-Champion G, Peltier JW. Emergency preparedness competencies: assessing nurses’ educational needs. J Nurs Adm. 2004;34(10):475–480. doi:10.1097/00005110-200410000-00009
11. McNeill C, Adams L, Heagele T, Swanson M, Alfred D. Emergency preparedness competencies among nurses. JONA J Nurs Adm. 2020;50(7/8):407–413. doi:10.1097/NNA.0000000000000908
12. Wahidah DA, Rondhianto R, Hakam M. Faktor-Faktor yang Mempengaruhi Kesiapsiagaan Perawat dalam Menghadapi Bencana Banjir di Kecamatan Gumukmas Kabupaten Jember [Factors Influencing Nurse Preparedness in the Face of Flooding in Gumukmas District in Jember]. Pustaka Kesehat. 2016;4(3):568–574.
13. Emaliyawati E, Prawesti A, Yosep I, Ibrahim K. Manajemen Mitigasi Bencana dengan Teknologi Informasi di Kabupaten Ciamis [Disaster Mitigation Management with Information Technology in Ciamis District]. J Keperawatan Padjadjaran. 2016;4(1):79–88. Indonesian. doi:10.24198/jkp.v4n1.8
14. Hodge AJ, Miller EL, Skaggs MKD. Nursing self-perceptions of emergency preparedness at a rural hospital. J Emerg Nurs. 2017;43(1):10–14. doi:10.1016/j.jen.2015.07.012
15. Setyawati AD, Lu YY, Liu CY, Liang SY. Disaster knowledge, skills, and preparedness among nurses in Bengkulu, Indonesia: a descriptive correlational survey study. J Emerg Nurs. 2020;46(5):633–641. doi:10.1016/j.jen.2020.04.004
16. Ning N, Kang Z, Jiao M, et al. Factors affecting emergency preparedness competency of public health inspectors: a cross-sectional study in northeastern China. BMJ Open. 2014;4(1):e003832. doi:10.1136/bmjopen-2013-003832
17. Kim H, Zakour M. Exploring the factors associated with the disaster preparedness of human service organizations serving persons with disabilities. Hum Serv Organ Manag Leadersh Gov. 2018;42(1):19–32. doi:10.1080/23303131.2017.1380737
18. Labrague LJ, Hammad K, Gloe DS, et al. Disaster preparedness among nurses: a systematic review of literature. Int Nurs Rev. 2018;65(1):41–53. doi:10.1111/inr.12369
19. Corrigan E, Samrasinghe I. Disaster preparedness in an Australian urban trauma center: staff knowledge and perceptions. Prehosp Disaster Med. 2012;27(5):432. doi:10.1017/S1049023X12001045
20. Ibrahim FAA. Nurses’ knowledge, attitudes, practices and familiarity regarding disaster and emergency preparedness–Saudi Arabia. Am J Nurs Sci. 2014;3(2):18–25. doi:10.11648/j.ajns.20140302.12
21. Kalanlar B. Effects of disaster nursing education on nursing students’ knowledge and preparedness for disasters. Int J Disaster Risk Reduct. 2018;28:475–480. doi:10.1016/j.ijdrr.2017.12.008
22. Salmani I, Seyedin H, Ardalan A, Farajkhoda T. Conceptual model of managing health care volunteers in disasters: a mixed method study. BMC Health Serv Res. 2019;19(1):241. doi:10.1186/s12913-019-4073-6
23. Baack S, Alfred D. Nurses’ preparedness and perceived competence in managing disasters. J Nurs Scholarsh. 2013;45(3):281–287. doi:10.1111/jnu.12029
24. Usher K, Mills J, West C, et al. Cross‐sectional survey of the disaster preparedness of nurses across the Asia–Pacific region. Nurs Health Sci. 2015;17(4):434–443. doi:10.1111/nhs.12211
25. Labrague LJ, Yboa BC, McEnroe-Petitte DM, Lobrino LR, Brennan MGB. Disaster preparedness in Philippine nurses. J Nurs Scholarsh. 2016;48(1):98–105. doi:10.1111/jnu.12186
26. Kulig JC, Edge D, Smolenski S. Wildfire disasters: implications for rural nurses. Australas Emerg Nurs J. 2014;17(3):126–134. doi:10.1016/j.aenj.2014.04.003
27. Hudak G. Keperawatan Kritis.
28. Goniewicz K, Goniewicz M, Burkle FM, Khorram-Manesh A. The impact of experience, length of service, and workplace preparedness in physicians’ readiness in the response to disasters. J Clin Med. 2020;9(10):3328. doi:10.3390/jcm9103328
29. Far SST, Marzaleh MA, Shokrpour N, Ravangard R. Nurses’ knowledge, attitude, and performance about disaster management: a case of Iran. Open Public Health J. 2020;13(1):441–446. doi:10.2174/1874944502013010441
30. Goniewicz K, Goniewicz M. Disaster preparedness and professional competence among healthcare providers: pilot study results. Sustainability. 2020;12(12):4931. doi:10.3390/su12124931
31. Diehl E, Rieger S, Letzel S, et al. The relationship between workload and burnout among nurses: the buffering role of personal, social and organisational resources. PLoS One. 2021;16(1):e0245798. doi:10.1371/journal.pone.0245798
32. Tavakoli N, Shaker SH, Soltani S, et al. Job burnout, stress, and satisfaction among emergency nursing staff after health system transformation plan in Iran. Emerg. 2018;6(1):e41–e41.
33. Nazli NNNN, Sipon S, Radzi HM. Analysis of training needs in disaster preparedness. Procedia - Soc Behav Sci. 2014;140:576–580. doi:10.1016/j.sbspro.2014.04.473
34. Potter MA, Miner KR, Barnett DJ, et al. The evidence base for effectiveness of preparedness training: a retrospective analysis. Public Health Rep. 2010;125(5_suppl):15–23. doi:10.1177/00333549101250S504
35. Phakdeechanuan K, Songwathana P, Sae-Sia W. Thai nurses’ learning needs regarding disaster nursing: high needs? Nurse Media J Nurs. 2015;5(2):56–66. doi:10.14710/nmjn.v5i2.10529
36. Whittaker J, McLennan B, Handmer J. A review of informal volunteerism in emergencies and disasters: definition, opportunities and challenges. Int J Disaster Risk Reduct. 2015;13:358–368. doi:10.1016/j.ijdrr.2015.07.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.