Back to Journals » Open Access Journal of Contraception » Volume 13
Determinants of Intrauterine Contraceptive Device Discontinuation Among Women Using Family Planning, in Southwest Ethiopia: Unmatched Case–Control Study
Authors Wolde TF ![]() , Bayisa K, Bekele F
, Bayisa K, Bekele F ![]()
Received 30 November 2021
Accepted for publication 17 March 2022
Published 8 April 2022 Volume 2022:13 Pages 39—47
DOI https://doi.org/10.2147/OAJC.S351930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Tarekegn Fekede Wolde,1 Kenbon Bayisa,2 Firomsa Bekele3
1Department of Nursing, College of Health Sciences, Mettu University, Mettu, Ethiopia; 2Department of Midwifery, College of Health Sciences, Mettu University, Mettu, Ethiopia; 3Department of Pharmacy, College of Health Sciences, Mettu University, Mettu, Ethiopia
Correspondence: Tarekegn Fekede Wolde, Department of Nursing, College of Health Sciences, Mettu University, Mettu, Ethiopia, Tel +251901613369 ; +251969544523, Email [email protected]
Background: Although the intrauterine contraceptive device is an effective, reliable, safe, and recommended contraceptive method, it is still underutilized and has a high discontinuation rate in Ethiopia. The study aims to assess determinants of the discontinuation of IUCDs among women using family planning in Ilu Aba Bor Zone.
Methods: A facility-based unmatched case–control study was conducted from September to October, 2021 among 168 (56 cases and 112 controls) IUCD-user women in public health facilities in south-west Ethiopia. Pretested, structured and interviewer administered questionnaires were used for data collection. The data were coded, cleaned and entered to Epi-data version 3.1 and exported to SPSS version 23 for advanced analysis. A binary logistic regression was used to estimate the degree of association between the outcome variable and independent variables. Finally, variables with a p-value less than 0.05 at 95% confidence interval were declared as statistically significant with outcome variable.
Results: A total of 168 (163) respondents participated in the study, with a response rate of 97%. The mean (+SD) age of the respondents was 31.36 ± 5.916. Regarding the educational status of respondents about 36 (64.3%) of cases and 90 (84.1%) of controls have formal education, and about 42 (75%) of cases’ husbands and 97 (90.65%) of controls’ husbands have formal education, respectively. Experiencing side effects (AOR = 2.36; 95% CI: 1.01, 5.55), lack of follow up (AOR = 4.069; 95% CI: l.30, 12.69), and planning for next pregnancy (AOR 4.14; 95% CI: 1.58, 10.88) were found to be the main determinants of intrauterine device discontinuation.
Conclusion: The findings of the study showed that lack of follow-up after insertion of the IUCD, experiencing side effects, and having a plan for the next pregnancy were found to be the main determinants of intrauterine device discontinuation. Hence, arranging recommended regular follow-up and treating side effects are very important to sustain intrauterine device utilization.
Keywords: intra uterine contraceptive device, family planning, determinants, Ethiopia
Introduction
An intrauterine contraceptive device (IUCD) is a small, flexible T-shape frame made of plastic, a highly effective and long-acting reversible family planning method that is safe for use by most women, including during breastfeeding.1 Contraceptive discontinuation is the phenomenon of starting a contraceptive method and then stopping it within one year of its use. Discontinuation of effective methods of contraception, including IUCD is a universal problem, though rates vary widely by population and country.2,3 Moreover, nearly 20–50% of reversible modern method users discontinue using a method during the first 12 months of initiating it.4 Furthermore, according to a WHO 2012 report, taking evidence from 60 demographic and health surveys, on average about 38% of women discontinued the use of reversible contraceptives by the 12th month and 64% by the 36th month; in this report, 13% was IUCD discontinuation in the first 12 months, and 13.1% globally and in developing countries respectively.3
Moreover, according to the EDHS 2016 report among family planning users, 35% discontinued any family planning in the first 12 months. Of this, IUCD accounts for about 13% of the total.5 In addition, the IUCD discontinuation rate in Wolkite, Ethiopia is 13.2% in the first year. After 12 months, more than 30% of women had discontinued the method.6
Despite the IUCD’s effectiveness, its discontinuation may lead to unplanned pregnancies,7–9 unwanted births, termination of pregnancies, and preventable medical costs.10 Globally, an estimated 33 million unwanted pregnancies were reported due to discontinuation by either traditional or modern contraceptive users.11
Many putative factors were revealed as the main barriers contributing to IUCDs being discontinued. A few factors that affect IUCD continuation are traveling time and not having used contraceptives before,12 and being far from health facilities for side effect management.4,9,13 Other factors include inconvenience of side effects14–18 and the need to conceive,4 method dissatisfaction,6,19 maternal educational level,20,21 area of residence17 and household economic status.22 Furthermore, prior short-term method users,6 lack of pre-post IUCD insertion counseling, partner disapproval, and lack of information.23,24 Therefore, identifying the determinants of IUCD discontinuation has paramount importance for utilizing IUCDs as per the recommendations. Therefore, this study aims to identify the determinants of IUCD discontinuation among users in southwest Ethiopia.
Materials and Methods
Study Setting and Period
The study was conducted in a public health facility in southwest Ethiopia. The zone has 22 woredas, with a total population of 968,303 based on 2007 national population survey. Currently the zone has 5 hospitals (1 specialized, 1 general and 3 primary), 40 health centers and one Family Guidance Association that provides an IUCD service. The study was conducted from September to October, 2021.
Study Design
A facility based retrospective unmatched case control study.
Study Populations
Randomly selected past users of IUCD (cases) and randomly selected current users of IUCD (control).
Eligibility Criteria
Inclusion
Case: All women who discontinued using IUCD and came to a selected health facility during data collection.
Control: All women who were using IUCD method and came to a selected health facility during data collection.
Sample Size Determination and Sampling Techniques
To determine the sample size for this study, the outcome variable and various factors significantly associated with the outcome variable were considered and then determined using Epi Info statistical software and using double population proportion by considering 95% CI, power of 80%, and case to control ratio of 1:2. Thus, three factors were considered to calculate the sample size, and then the variable with the largest sample size was used by considering the following: The rate of IUCD use of 60%, IUCD discontinuation of 34.8%, with an odds ratio of 2.813, and considering side effects as a major determinant, the largest calculated sample size was 151.2. Finally, adding a 10% non-response rate, the total sample size was 168 (56 cases and 112 controls). The simple random sampling technique was used after proportionally allocating each of the selected health facilities to select study unit.
Quality Control and Data Collection Tool
To assure the quality of the data, the structured questionnaire was developed by reviewing different literatures. A pretested questionnaire was administered prior to the actual data collection period on 5% of the sample size in a similar context and population which is not included in the actual study. A half-day training was given for both data collectors and supervisors prior to data collection. The final version of the questionnaire, which was prepared in English, was translated into the native local language “Afan Oromo” and translated back to English by language experts.
Data were collected by five trained BSc midwifery professionals who are working on MCH and had prior experience in data collection through face-to-face interview and of them one was the supervisor. The collected data were checked for completeness and consistency on a daily basis. Lastly, 5% of the data were double-entered in order to compare and assure the quality of the data.
Data Processing and Analysis
The collected data were checked and rechecked for completeness, consistency, and accuracy by the supervisors and principal investigator every day for necessary corrections. The data were cleaned, entered into Epi data version 3.1, and then transported to SPSS version 23 for further analysis. Descriptive statistics, tables and statements were used to describe the data. The Hosmer and Lemeshow goodness-of-fit test was used to check model fitness. Bivariable and multivariable logistic regression analysis were performed to identify the determinants. All variables with a p < 0.25 in the bivariate analysis were entered into the multivariable logistic regression analysis. Multivariable logistic regression analysis was used to see the net effects of each independent variable in explaining variation in the outcome variable. Odds ratio along with the 95% confidence interval was used to ascertain the certain association and statistical significance between variables. Finally, statistical significance were set at a p-value of <0.05.
Operational Definition
Cases: All IUCD users who were permanent residents of the area (residents for 6 months), and discontinued IUCD method in the selected health facilities during the study period.
Controls: All women who were permanent residents of the area (residents for 6 months), and who are still using IUCD in selected health facilities during the study period.
IUCD discontinuation: an episode when a woman discontinues the method irrespective of the reason for discontinuing.
Results
Socio-Demographic Characteristics
Among 56 cases and 112 controls of IUCD users intended to be included in the study from 13 public health facilities, 56 cases and 107 controls participated which yields a response rate of 97%. The mean (+SD) age of the respondents is 31.36 ±5.916. Moreover, about 32 (57%) cases and 86 (80.4%) controls live in urban areas and 40 (71.4%) cases and 95 (88.8%) controls live less than one hour from the health facility (Table 1).
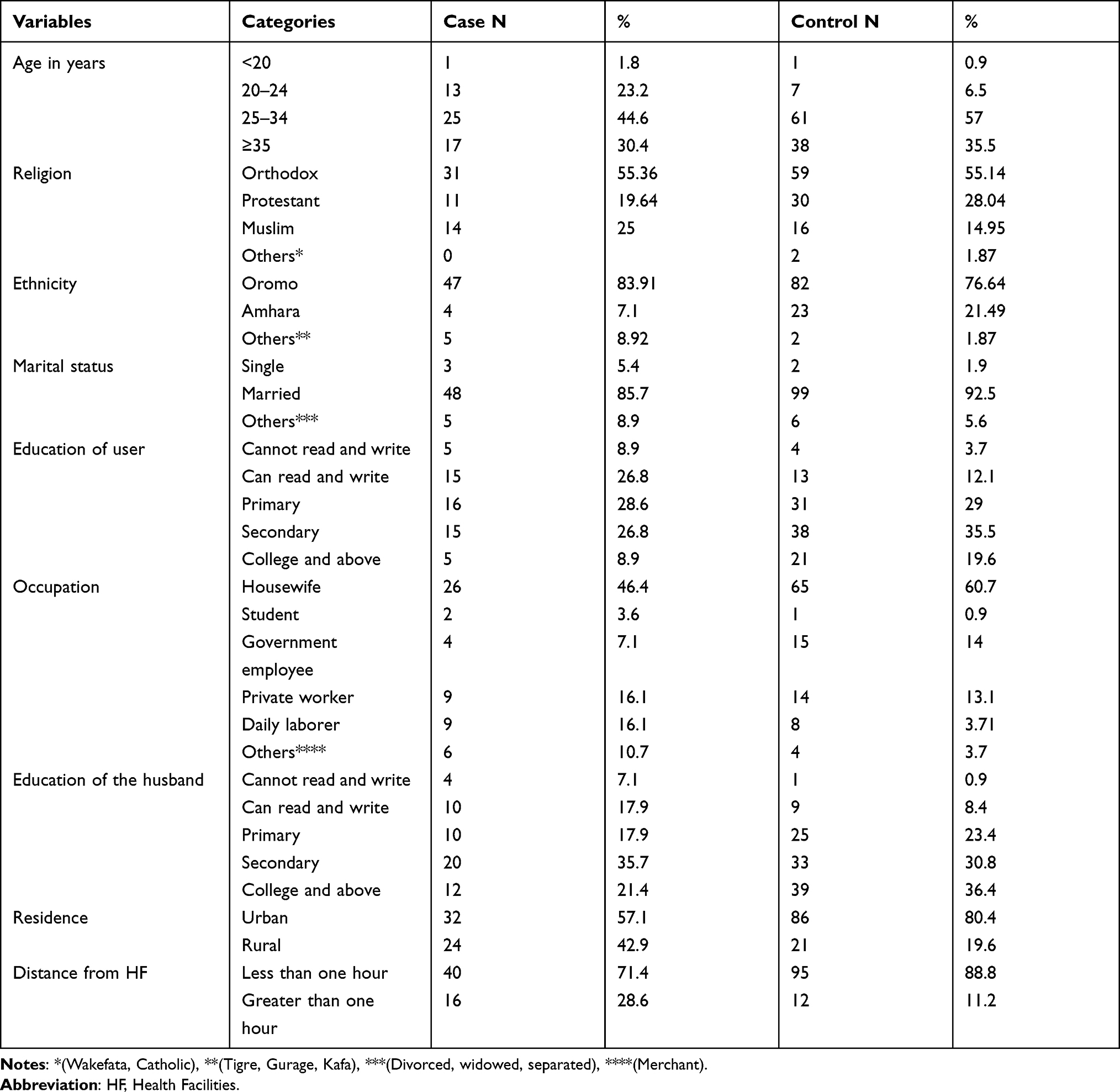 |
Table 1: Socio-Demographic Characteristics of Study Participants at Public Health Facilities in Southwest Ethiopia, 2021 |
Reproductive Characteristics of Study Respondents
The majority of the cases (48; 82.1%) and controls (101; 96.3%) had been pregnant and most of them had been pregnant 2–4 times for both cases and controls. About 38 (67.9%) cases and 73 (68.2%) controls have plans to get pregnant in the future and among these the majority of cases and controls want to get pregnant within two years. Among users who discontinued their IUCD about 50% experienced side effects while only 17.8% of controls experienced side effects (Table 2).
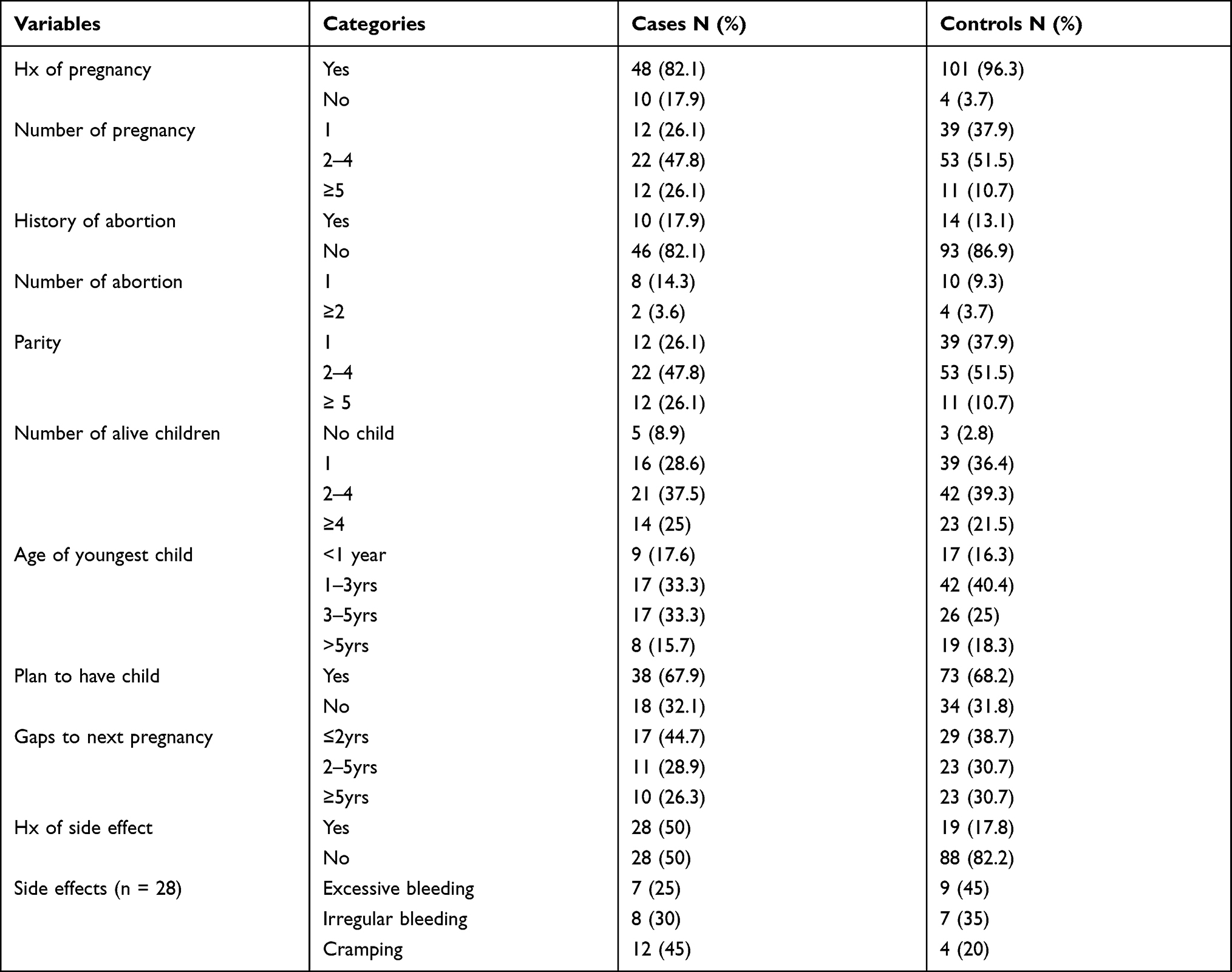 |
Table 2: Reproductive Characteristics of Study Participants in Southwest Ethiopian Public Health Facilities, 2021 |
Individual Related Characteristics of Respondents
Regarding the training related to family planning the majority of cases and controls have no training with 85.7% and 94.4%, respectively. About 84% of users who discontinued IUCD have no follow-up while at most half of the continued users have a follow-up; of the total discontinuation group only 67.9% had discussed this with a service provider. The majority of cases and controls received counseling, 75% and 88%, respectively and most of them use the method since it has long-term protection. About 66.1% of cases and 68.2% of controls had been told the benefits and side effects of the method at the time of insertion; of the total discontinuation group only 16.1% had followed up while about 55.1% of IUCD users had followed up. Among cases, the main side effects and reasons reported for discontinuation are wanted to conceive (25%), followed by automatic expulsion (21.43%) and heavy bleeding (21.43%) (Table 3).
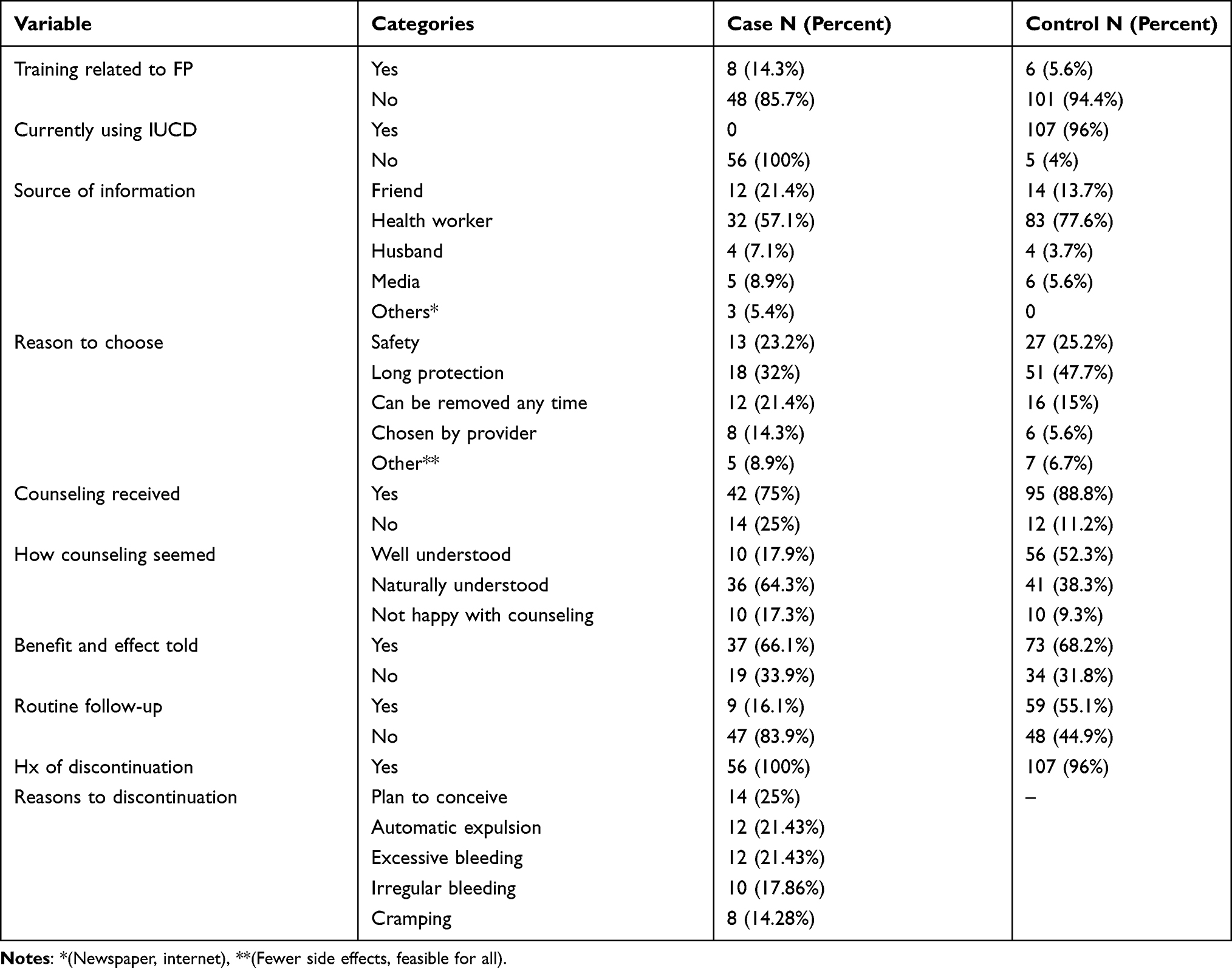 |
Table 3: Individual Related Characteristics of Study Participants in Health Facilities in Southwest Ethiopia, 2021 |
Determinants of IUCD Discontinuation
On bivariate analysis residence, educational status, distance from the health facility, lack of regular follow-up, counseling, training, plan to be pregnant, how counseling seems and side effects were candidates for multivariable analysis.
However, side effects, having followed up and planning to have next pregnancy were significantly associated with IUCD discontinuation. Those users who had experienced side effects are at least two times more likely to discontinue IUCD compared with their counterparts (AOR = 2.36; 95% CI: 1.01, 5.55). The IUCD users who had no follow-up are four times more likely to discontinue IUCD than those who had a follow-up (AOR = 4.069; 95% CI: 1.30, 12.69). Moreover, the users who intend to have a child in the future were at least four times more likely to discontinue than those who have no plan to do so (AOR of 4.139; 95% CI: 1.58, 10.88) (Table 4).
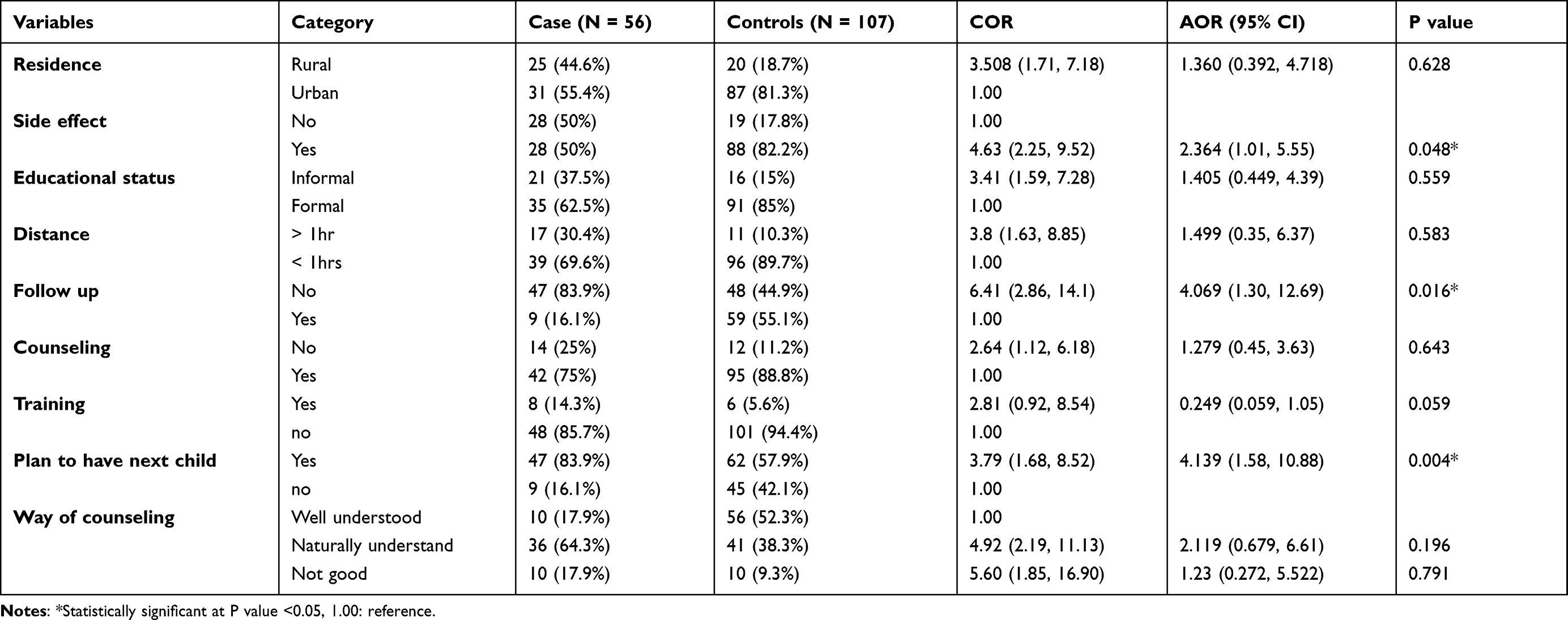 |
Table 4 Bivariable and Multi-Variable Analysis Showing Factors Associated with IUCD Discontinuation Among IUCD User Women in Southwest Ethiopia, Public Health Facilities, 2021 |
Discussion
This is the first study, to my knowledge, to examine the factors associated with the discontinuation of IUCD in southwest Ethiopian health facilities. The study assessed the factors affecting the discontinuation of IUCD in southwest Ethiopia, in order to identify factors that may encourage the discontinuation of IUCD and to present approved recommendations.
After controlling for confounding variables, IUCD use was associated with follow-up after insertion, plan to have a child in the future, and experiencing side effects. This study found a strong association between follow-up practice and IUCD discontinuation. There was also a strong association between side effects and IUCD discontinuation. In addition, a reproductive intention was also associated with IUCD discontinuation. Discontinuation of IUD due to side effects: This finding is similar to a study done in Pakistan, however, it is far removed from the finding of a study done in Karachi that indicates the family planning users who experienced side effects are 15 times more likely to discontinue again, which is supported by the finding of a study conducted in Hawasa and Nepal.16,17
This study finding shows that those who discontinued use of IUCDs were two times more likely to experience side effects than the users, which is in line with the result of a study done in Hawassa that revealed family planning users who experienced side effects were at least two times more likely to discontinue the method than those who did not experience side effects, and those who had a desire to be pregnant were two times more likely to discontinue18,19. The users who had no follow-up were four times more likely to discontinue IUCD use than the users who had follow-up. This finding is higher than the study done in Hawassa which showed that users who did not have a follow-up were three times more likely to discontinue the method than those who had a follow-up. Thus, the difference might be due to population variation.16 The finding is again similar to a study done in Nepal which showed the IUCD discontinuation due to side effects is three times greater.20 According to this finding among respondents, users who planned to get pregnant in the future were four times more likely to discontinue their IUCD, which is in line with a study done in Asosa. One of the limitations of the current study is the likelihood of the presence of recall bias due to the nature of the case-control design adopted in this study since the exposure status was assessed for different factors retrospectively. Another limitation was the lack of enough literature for further discussion across the study area.
Strength and Limitation
The current study has several methodological strengths. Women from a large database were recruited, and a high response rate was achieved. Detailed standardized interviews were carried out and pretesting was done to minimize rater bias.
Because of the retrospective method, it could be argued that the observed associations are a result of recall bias. However, the strong study design and results that are consistent with those of previous studies suggest that the observed associations are valid. Because of the small sample size, low power is the limitation of discontinuation analysis. Understanding socio-cultural determinants of IUCD use was not possible in this study, as the study was purely quantitative. The absence of matching controls might also affect the findings of the study.
Conclusion
Intrauterine device discontinuation was found to be high, despite its effectiveness. Having future plans to get pregnant and lack of necessary follow-up were the major determinants of IUCD discontinuation. Another determinant found to be significantly associated with IUCD discontinuation was experiencing side effects after insertion of the method.
Abbreviations
ANC, Antenatal care; DHS, Demographic and health survey; FP, Family planning; HC, Health center; HF, Health facility; IUCD, Intrauterine contraceptive device; NGO, Non-governmental organization; WHO, World Health Organization.
Data Sharing Statement
Data are available from corresponding author on reasonable request.
Ethical Considerations
Ethical approvals for the study were obtained from Mettu University College of Health Science, review committee. A permission letter was written from the Woreda health office. Verbal consent from each participant was obtained after explaining the purpose of the study. Written informed consent, risk, and benefit of the study were taken from individuals ready to participate in the study. To prevent the risk of back retrieval of confidential information such as names of the participants, during data collection assigned code numbers were given by the investigators, and this study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no financial or non-financial was received for this work.
Disclosure
All Authors declare that there no competing interests concerning this work.
References
1. Kouyate RA. A Guide for Developing Family Planning Messages for Women in First Year Postpartum. Baltimore, Maryland: Jhpiego; 2010.
2. Janine B, Ilene S. Contraceptive discontinuation and switching among Honduran women. Int Perspect Sex Reprod Health. 2011;37 (01):16–23. doi:10.1363/3701611
3. Ali M, Shah I. Causes and Consequences of Contraceptive Discontinuation: Evidence from 60 Demographic and Health Surveys; 2012.
4. Vadnais D, Abderrahim N. Women lives and experiences: changes in the past ten years. Research Findings from the Demographic and Health Surveys; 2006.
5. Csa I. Central Statistical Agency (CSA)[Ethiopia] and ICF. Ethiopia Demographic and Health Survey, Addis Ababa. Central Statistical Agency; 2016.
6. Girum T. Early discontinuation of long acting reversible contraceptives among married and in union women: a systematic review and meta-analysis. Ann Med Health Sci Res. 2017;7:113–118.
7. New York, N.D.o.E.S.A., United Nations., Population Division. Accelerating achievement of the MDGs by lowering fertility: overcoming the challenges of high population growth in the least developed countries [population facts]; 2010.
8. Blumenthal PD, Voedisch A, Gemzell-Danielsson K. Strategies to prevent unintended pregnancy: increasing use of long-acting reversible contraception. Hum Reprod Update. 2011;17 (1):121–137. doi:10.1093/humupd/dmq026
9. Thobani R, Jessani S, Azam I, et al. Factors associated with the discontinuation of modern methods of contraception in the low income areas of Sukh initiative Karachi: a community-based case control study. PLoS One. 2019;14 (7):e0218952. doi:10.1371/journal.pone.0218952
10. Trussell J. The cost of unintended pregnancy in the United States. Contraception. 2007;75 (3):168-170.
11. Casey PM, Long ME, Marnach ML, Bury,JE. Bleeding related to etonogestrel subdermal implant in a US population. Contraception. 2011;83 (5):426–430. doi:10.1016/j.contraception.2010.09.012
12. Hameed W, Azmat SK, Ali M, et al. Determinants of method switching among social franchise clients who discontinued the use of intrauterine contraceptive device. Int J Reprod Med. 2015;2015:8.
13. Bradley SEK, Khan S. Levels, trends, and reasons for contraceptive discontinuation [DHS analytical studies]. Calverton, MD: ICF Macro; 2009.
14. Vadnais D, Kols A, Abderrahim N. Women's lives and experiences: changes in the past ten years. ORC Macro; 2006.
15. Pandey D, Tiwari S. Study of pattern related to side effects and removal of IUCD usage. Int J Community Med Public Health. 2015;2 (2):172–175. doi:10.5455/2394-6040.ijcmph20150520
16. Azmat SK, Shaikh BT, Hameed W. Rates of IUCD discontinuation and its associated factors among the clients of a social franchising network in Pakistan health. BMC Women’s Health. 2012;12. doi:10.1186/1472-6874-12-8
17. Subash T, Paudel IS, Sailesh B, Ranjila J, Kabita T. Factors affecting IUCD discontinuation in Nepal: a nested case-control study Asia-Pacific. J Public Health. 2012.27 (2):1280–1287
18. Park MH. Ngo TD Dynamics of IUD use in Vietnam: implications for family planning services at primary health care level. Int J Women’s Health. 2011;3:429–434.
19. Thapa S, Paudel IS, Bhattarai S, Joshi R, Thapa K. Factors affecting IUCD discontinuation in Nepal: a nested case-control study. Asia Pacific Journal of Public Health. 2015 Mar;27(2):NP1280–7.
20. Azmat K, Shaikh BT, Hameed W. Rates of IUCD discontinuation and its associated factors among the clients of a social franchising network in Pakistan. BMC Women’s Health. 2012;12:8.
21. Ideta ZS, Mekonen L, Seifu W, Shine S. Contraceptive discontinuation, method switching and associated factors among reproductive age women in Jimma Town, Southwest Ethiopia. Fam Med Med Sci Res. 2017;6:213.
22. Trussell J. The cost of unintended pregnancy in the United States. Contraception. 2007;75 (3):168–170. doi:10.1016/j.contraception.2006.11.009
23. Teshome S, Negera E, Sileshi T, Tadele A. The rate of intra uterine contraceptive device use and associated factors among married women of reproductive age in Mettu rural community, south west Ethiopia. J Prim Care Community Health. 2020;11:1–8.
24. Belay Amare A, Bezatu M. Discontinuation of Long acting contraception and associated factors among female users in health facilities of Hawassa City, Southern Ethiopia. Contraception. 2020;11:113–123.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.