Back to Journals » Journal of Asthma and Allergy » Volume 19
Designing an Incremental Egg Oral Immunotherapy Protocol: A Strategic Approach with Safety as a Priority
Authors Munyuen D ![]() , Yuenyongviwat A, Sangsupawanich P, Chauikaew K, Srisuk B, Chanklay T, Koosakulchai V
, Yuenyongviwat A, Sangsupawanich P, Chauikaew K, Srisuk B, Chanklay T, Koosakulchai V
Received 5 January 2026
Accepted for publication 5 March 2026
Published 14 March 2026 Volume 2026:19 591550
DOI https://doi.org/10.2147/JAA.S591550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Darin Munyuen, Araya Yuenyongviwat, Pasuree Sangsupawanich, Kokaew Chauikaew, Burat Srisuk, Tidawan Chanklay, Vanlaya Koosakulchai
Division of Allergy and Immunology, Department of Pediatrics, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Vanlaya Koosakulchai, Division of Allergy and Immunology, Department of Pediatrics, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand, Email [email protected]
Purpose: Egg oral immunotherapy (OIT) has demonstrated clinical efficacy; however, 10– 35% of patients discontinue treatment due to severe adverse reactions, particularly during the build-up phase. To improve safety, we developed an incremental egg OIT protocol with gradual dose escalation and an extended build-up period. This study aimed to evaluate the safety and efficacy of this protocol in children with egg allergy.
Patients and Methods: We retrospectively reviewed children aged 1– 18 years with hen’s egg allergy confirmed by oral food challenge (OFC) who initiated an incremental egg OIT protocol at Songklanagarind Hospital between August 2023 and March 2025. Demographic characteristics, serum specific immunoglobulin E (sIgE) levels to egg white, egg yolk, and ovomucoid, and adverse reactions during OIT were collected and analyzed.
Results: Fourteen patients were included; four underwent egg yolk OIT (EY-OIT) and ten underwent egg white OIT (EW-OIT). The median age was 44.5 months (IQR 31– 63) in the EY-OIT group and 29.5 months (IQR 22.5– 65.25) in the EW-OIT group. Mild adverse reactions occurred in 6 of 14 patients (43%). Reported reactions included active eczema and itchy throat in the EY-OIT group, and perioral erythema, active eczema, and acute urticaria in the EW-OIT group. No severe adverse reactions were observed during the OIT build-up and maintenance phases. Thirteen patients (92.9%) successfully escalated doses according to the protocol, and nine patients reached the target maintenance dose.
Conclusion: An incremental egg OIT protocol demonstrated a favorable safety profile in children with egg allergy. No severe adverse reactions occurred during the OIT build-up and maintenance phases, and most patients tolerated gradual dose escalation as planned, supporting the feasibility of this approach in real-world clinical practice.
Plain Language Summary: An incremental egg OIT strategy may offer a safer and more feasible approach to desensitization in children with egg allergy, with potential for broader implementation in routine clinical settings.
Keywords: egg allergy, egg oral immunotherapy, adverse reaction
Introduction
Egg allergy is one of the most common food allergies in Thai children, with a prevalence of approximately 41.6%.1 It typically manifests in infants and toddlers under 2 years old and gradually resolves by adolescence. A cohort study of 213 children aged 3 to 15 months found that the average age of resolution was 72 months.2 However, some studies have shown that 42% of children with egg allergy outgrow it by adolescence.3
The current standard management of food allergies is strict avoidance of allergenic food. However, accidental exposure still occurs in up to one-third of food-allergic individuals.4 Given that eggs are a staple in Thai cuisine, strict avoidance is often challenging. In addition, egg avoidance may lead to nutritional deficiencies and growth problems5 and significantly impact quality of life for both patients and caregivers.6
Oral immunotherapy (OIT) is an emerging treatment approach that involves the gradual ingestion of the allergenic food in increasing amounts. This method has been shown to reduce the severity of allergic reactions upon accidental exposure, and in some cases, lead to long-term tolerance.7 However, 10–35% of patients discontinue OIT due to adverse reactions.8 Most OIT programs are conducted in children older than 4 years, although some studies have initiated OIT in children younger than 4 years with peanut allergy, showing improved tolerance and higher chances of sustained unresponsiveness.9,10
Several studies demonstrated the efficacy of egg OIT, achieving desensitization rates of 70–90%.11–14 Furthermore, some studies report sustained unresponsiveness (SU) in 33% of patients after 1 year, increasing to 55% after 3 years of treatment.13,14 However, these studies also report a high incidence of adverse effects, particularly during the initial build-up phase, affecting 60–90% of patients, leading to treatment discontinuation in some cases. Rapid up-dosing protocols and short build-up durations may contribute to these outcomes. Moreover, existing egg OIT protocols vary substantially in terms of starting doses, up-dosing intervals, egg preparation methods, and target maintenance doses, which may influence both safety and efficacy.11–14 These limitations highlight the need for safer, more standardized, and practical approaches that are suitable for routine clinical implementation.
At the Division of Pediatric Allergy and Immunology, Songklanagarind Hospital, we have implemented an incremental egg OIT protocol which employed a slow up-dosing strategy with a longer build-up period, aiming to minimize severe reactions in pediatric patients with egg allergies since August 2023. In this protocol, we used boiled egg due to its accessibility and ease of preparation. The current study aims to evaluate the safety and efficacy of this OIT protocol in egg-allergic children.
Materials and Methods
Study Design and Study Population
This was a retrospective study in patients with hen’s egg allergy who initiated an incremental egg oral immunotherapy protocol at Songklanagarind Hospital, a tertiary hospital in Southern Thailand, during the period from August 2023 to March 2025. An incremental egg oral immunotherapy protocol was performed by pediatric allergists and nurses trained in the management of pediatric allergic reactions.
We included children aged 1 to 18 years who met the following criteria:
Inclusion Criteria
- A history suggestive of immediate IgE-mediated egg allergy, or severe atopic dermatitis warranting evaluation for suspected egg allergy.
- Evidence of IgE sensitization to egg yolk, egg white, or ovomucoid (serum specific IgE ≥ 0.35 kUA/L).
- Confirmed diagnosis of egg allergy by a positive oral food challenge (OFC) to boiled egg yolk or egg white.
Exclusion Criteria
- Uncontrolled asthma
- Chronic idiopathic urticaria
- Uncontrolled chronic diseases (gastrointestinal, cardiovascular, or neurological disease)
- Prior treatment with OIT
Study Methods
Oral Food Challenge Test Protocol of Egg Yolk (EY) or Egg White (EW)
Oral food challenge (OFC) was performed by using boiled egg yolk (EY) or egg white (EW) prepared by using chicken egg, size no. 2, and boiled in boiling water for 15 minutes. We divided EY or EW into 6 doses, with intervals of 30 minutes (Table 1).
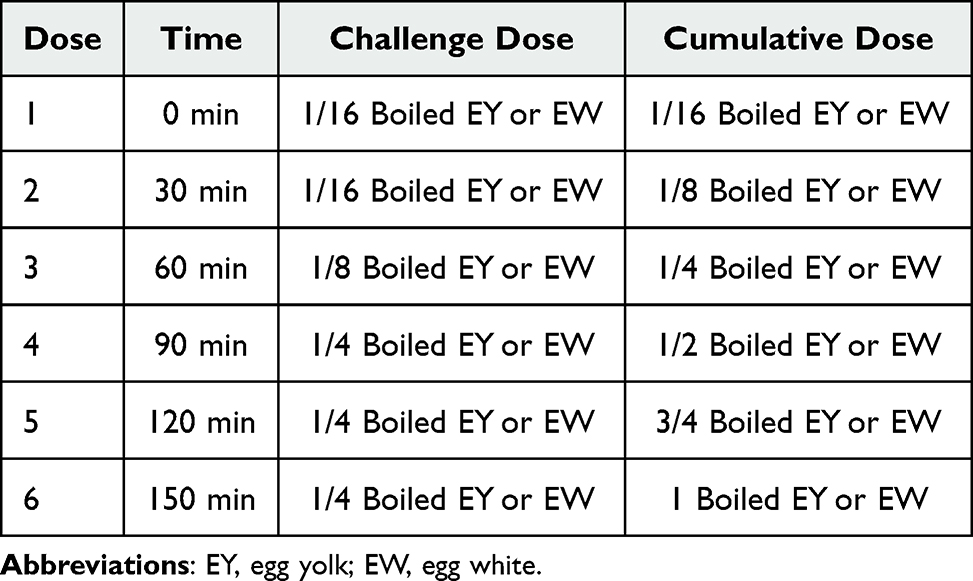 |
Table 1 The Oral Food Challenge Protocol of Egg Yolk (EY) or Egg White (EW) |
Confirmed egg allergy is defined as a positive oral food challenge test to boiled egg yolk or egg white, based on the EAACI 2023 and PRACTALL 2017 guidelines for IgE-mediated food allergy:
- Typical symptoms including generalized nonspecific pruritus, scratching, nasal pruritus, ocular pruritus, dyspnea (without objective signs), throat tightness, nausea, abdominal pain, oral/throat pruritus, complaints of weakness, dizziness, feeling unwell occurring within 2 hours of exposure and reproducible upon re-exposure, and
- Evidence of IgE sensitization and/or effector cell response to the allergen.
An Incremental Egg Oral Immunotherapy Protocol
All patients were admitted to the hospital for supervised oral food challenges (OFCs). Written informed consent was obtained from the parents or guardians of all participants before starting the protocol. The testing protocol began with an egg yolk OFC on day 1. If the patient developed an allergic reaction during the challenge, the result was considered positive, and egg yolk OIT was initiated the following day. The starting dose was determined based on the cumulative threshold dose, followed by the egg yolk OIT (EY-OIT) protocol. Patients who successfully passed the egg yolk OFC proceeded to undergo an egg white OFC on the next day. If a reaction occurred during the egg white OFC, egg white OIT was initiated on the following day, with the cumulative threshold dose as the starting point.
During the build-up phase, patients continued the daily threshold dose at home for three months, after which they returned to the hospital for dose escalation. The OIT dose was increased by one step every three months. Each step consisted of two divided doses (50%, 50%), administered 30 minutes apart, until the maintenance dose (Step 6) was achieved (Table 2). Antihistamines were prescribed one hour before egg ingestion starting from the first day of OIT and continued for at least one month at home, as well as during the first month of each subsequent dose escalation. Annual OFCs were performed to establish the new egg yolk threshold dosages for the patient who had not reached the target dosage.
 |
Table 2 Dose of Initial OIT and Step-Up OIT in the Build-Up Phase of Protocol |
In the maintenance phase, patients consumed the maintenance dose at least five days per week for 6–12 months. Thereafter, they were instructed to avoid egg yolk or egg white for one month, followed by an OFC to assess sustained unresponsiveness. sIgE to egg yolk, egg white, and ovomucoid was measured every 3–6 months during the OIT protocol. In addition, each patient was provided with a diary to record treatment compliance and any adverse reactions following egg ingestion (Figure 1).
 |
Figure 1 Incremental egg oral immunotherapy (OIT) protocol implemented at Songklanagarind Hospital. This figure outlines the structured build-up and maintenance phases of the incremental egg OIT protocol, including dose escalation steps, timing intervals between up-dosing visits, and progression to the target maintenance dose. Abbreviations: OFC, oral food challenge; OIT, oral immunotherapy. |
Data Collection and Definitions
A data collection form was created, and data was collected retrospectively from the hospital database of egg-allergic patients who received an incremental egg OIT protocol at Songklanagarind Hospital between August 1, 2023, and March 31, 2025.
Demographic information, including sex, age, comorbidities, additional food allergies, onset of egg allergy, symptoms of egg allergy, and the threshold dose of OFC, was recorded. The adverse reactions of the OIT protocol were referred to as the reactions at home, and the severity of allergic symptoms was assessed based on the Grading System of Systemic Allergic Reactions—WAO 2024.15 The efficacy of the OIT protocol was determined by the ability to tolerate gradual dose increases according to the protocol. sIgE to egg yolk, egg white, and ovomucoid were collected at the beginning and every 3 months during the OIT protocol.
Statistical Analysis
Data were collected and cleaned using Microsoft Excel and subsequently analyzed. Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate. Nominal variables were summarized using frequencies and percentages.
Results
Patient Baseline Characteristics
During the study period, a total of 24 patients who met the inclusion and exclusion criteria underwent OFC testing in Songklanagarind Hospital. Ten patients passed both OFC to EY and EW. Four and ten patients were OFC-positive to EY and EW and were enrolled in the EY-OIT and EW-OIT protocol, respectively.
In the EY-OIT group (n=4), the median age was 44.5 months (IQR 31–63.25), and 3 patients (75%) were male. Atopic dermatitis was present in all patients (4/4, 100%), allergic rhinitis in 3 patients (75%), and asthma in 2 patients (50%). Additional food allergies included cow’s milk in 2 patients (50%), wheat in 1 patient (25%), soy in 1 patient (25%), and peanut in 1 patient (25%). The median age of onset of yolk allergy was 12.5 months (IQR 6.25–32.25). Initial allergic manifestations included urticaria/angioedema in 2 patients (50%), anaphylaxis in 1 patient (25%), and other symptoms in 1 patient (25%). The median sIgE to egg yolk was 7.43 kUA/L (IQR 3.4–13.55), and the median OFC threshold dose was 854.5 mg of egg yolk protein (IQR 358–1857).
In the EW-OIT group (n = 10), the median age was 29.5 months (IQR 22.25–68.5), and 7 patients (70%) were male. Atopic dermatitis was observed in 8 patients (80%), allergic rhinitis in 4 patients (40%), and asthma in 1 patient (10%). Additional food allergies included cow’s milk in 6 patients (60%), wheat in 6 patients (60%), soy in 1 patient (10%), fish in 1 patient (10%), and peanut in 1 patient (10%). The median age at onset of egg white allergy was 6 months (IQR 6–8.25). Initial allergic reactions included urticaria/angioedema in 4 patients (40%), anaphylaxis in 2 patients (20%), severe atopic dermatitis in 1 patient (10%), and other symptoms in 3 patients (30%). The median baseline sIgE levels were 5.47 kUA/L (IQR 1.58–9.39) for egg white and 5.88 kUA/L (IQR 0.32–9.39) for ovomucoid. The median OFC threshold dose was 675 mg of egg white protein (IQR 450–2925) (Table 3).
 |
Table 3 Baseline Characteristics |
Adverse Reaction and Efficacy of an Incremental Egg Yolk OIT Protocol
Initial dosing of OIT was determined through an OFC, with all four patients experiencing mild reactions classified as grade 1–2 and managed with antihistamine and ondansetron. The starting dose of OIT varied among patients, ranging from 1/16 to 1/2 of a boiled egg yolk. After consuming the initial dose of OIT, two patients reported home reactions, specifically active atopic dermatitis and itchy throat which were managed with oral antihistamines. No severe adverse reactions were observed.
In the next visit, all patients attended the follow-up and underwent dose escalation. All patients were able to up-dose according to the protocol. The two patients who had previously experienced home reactions continued to report the same symptoms; however, they were able to step up their dose in visit 2. One patient (No. 2) successfully reached the maintenance target dose equivalent to one whole egg yolk.
At visit 3, the patient (No. 3) who completed 1 year of OIT but had not reached the target dose underwent OFC to evaluate their new threshold doses for egg yolk, and this patient could tolerate one boiled egg yolk without any adverse reaction. Patient No. 1 was also able to up-dose and successfully entered the maintenance phase.
In total, three patients successfully entered the maintenance phase, with the time from the build-up phase to maintenance ranging from 6 to 9 months. Blood samples for serum-specific IgE (sIgE) to egg yolk were collected at baseline and during the protocol, as summarized in Table 4.
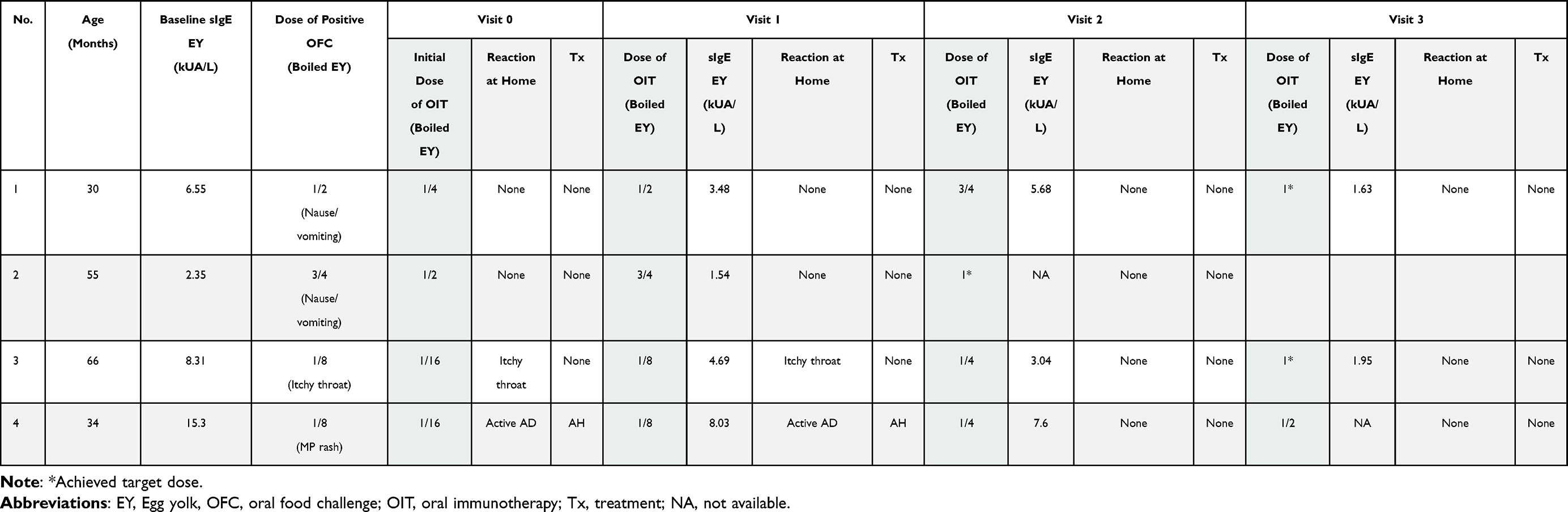 |
Table 4 Adverse Reactions During the Build-Up Phase in Patients Who Underwent an Incremental Egg Yolk OIT |
Adverse Reaction and Efficacy of an Incremental Egg White OIT Protocol
A total of 10 patients underwent treatment using an incremental egg white OIT protocol. Initial doses were determined via an oral food challenge test, during which one patient experienced a severe reaction (anaphylaxis) and was treated with adrenaline. The remaining patients had mild grade 1–2 reactions. Initial doses varied among patients, ranging from 1/16 to 3/4 of a boiled egg white. After consuming the initial dose of OIT, four patients reported home reactions, including perioral redness, acute urticaria, active atopic dermatitis, and maculopapular (MP) rash. These symptoms were managed with oral antihistamines. None of the patients required hospitalization for severe reactions.
In the following visit, all patients underwent dose escalation and nine patients (90%) were able to up-dose according to the protocol. Patient No. 3 was unable to escalate the dose due to acute urticaria while two patients (No. 8, 10) successfully reached the maintenance target dose. Two patients reported home reactions, specifically perioral redness and urticaria which were managed with oral antihistamines. No severe adverse reactions were observed.
At visit 2, six patients attended the follow-up for dose escalation. Four of them reached the maintenance dose and continued consuming at home without any adverse reaction. Two patients dropped out of the study due to refusing to consume eggs daily without any adverse reaction. Two patients still attempted dose escalation in visit 3.
As shown in Table 3, a total of six patients reached the maintenance phase, with durations from the build-up phase to maintenance ranging from 3 to 6 months. Serum specific IgE levels to egg white and ovomucoid were monitored at baseline and during the protocol, as summarized in Table 5.
 |
Table 5 Adverse Reactions During the Build-Up Phase in Patients Who Underwent an Incremental Egg White OIT |
Immunological Outcomes Change in Patients Undergoing Egg OIT Protocol
Following treatment with an incremental egg OIT protocol, there was a notable reduction in serum specific IgE levels to egg yolk, egg white, and ovomucoid in patients, when compared to baseline levels prior to treatment initiation. Serial monitoring throughout the treatment period demonstrated a gradual and continuous decline in specific IgE levels over the course of one year. This immunological improvement correlated with the patient’s ability to successfully escalate OIT doses in accordance with the protocol (Tables 4 and 5).
Discussion
In this study, we evaluated the safety and feasibility of an incremental egg oral immunotherapy (OIT) protocol in children with confirmed egg allergy. Our findings indicate that a slow up-dosing strategy using boiled egg yolk or egg white was well tolerated, with no severe adverse reactions observed during the OIT phase. Most patients were able to escalate doses according to the protocol, supporting the practicality of this approach in routine pediatric allergy practice.
Previous studies of egg OIT have primarily used freeze-dried egg white powder or pasteurized egg products, often employing rapid or semi-rush build-up schedules with target doses equivalent to one whole egg protein. These protocols have reported desensitization rates of 70–90%; however, adverse reactions were frequent, occurring in up to 60–90% of patients, and treatment discontinuation due to severe reactions was reported in 10–35% of cases.11–14 In contrast, our protocol utilized cooked egg yolk or egg white with a slower, incremental dose escalation at longer intervals (every three months), allowing more time for immunological adaptation and symptom monitoring. This strategy likely contributed to the absence of severe systemic reactions and the high proportion of patients who successfully progressed through the protocol. From an efficacy perspective, 92.9% of patients were able to escalate doses as planned, and a substantial proportion reached the maintenance phase within 3–12 months.
Long-term sustained unresponsiveness (SU) remains an important clinical consideration in egg OIT. Previous studies have reported SU rates ranging from 33% after one year to approximately 55% after three years of continued therapy.11,12,14 However, re-sensitization following discontinuation of OIT has also been described in a subset of patients, particularly when maintenance ingestion is inconsistent.14 Because our study primarily evaluated safety and feasibility during the build-up and maintenance phases, long-term sustained unresponsiveness was not systematically assessed.
Serial monitoring demonstrated a gradual reduction in serum specific IgE levels to egg yolk, egg white, and ovomucoid over the course of treatment. Although decreases in sIgE do not directly equate to clinical tolerance, these trends are consistent with immunological changes reported in previous OIT studies and may reflect a favorable treatment response when assessed longitudinally.11–14 Notably, patients in both the egg yolk and egg white OIT groups demonstrated similar tolerability, supporting the potential for a component-based approach tailored to individual sensitization profiles.
This study has several limitations. Its retrospective design and small sample size limit generalizability and preclude definitive conclusions regarding comparative efficacy. Additionally, the absence of a control group receiving strict avoidance therapy and the lack of a comparative rapid up-dosing protocol restrict direct evaluation of the relative safety and efficacy of different escalation strategies. Furthermore, sustained unresponsiveness was not systematically assessed, thereby limiting evaluation of long-term outcomes; longer follow-up studies are needed to determine the durability of tolerance after treatment cessation. Finally, although the inclusion criteria permitted a broad pediatric age range, the study population primarily consisted of toddlers and preschool-aged children; therefore, the findings may not be generalizable to older children or adolescents. Nevertheless, the real-world design of this study and the detailed documentation of adverse reactions provide meaningful insight into the practical implementation and safety of an incremental egg OIT protocol in routine clinical settings.
Conclusion
An incremental egg OIT protocol using cooked egg products was safe and feasible in children with egg allergy, with no severe adverse reactions observed during the OIT build-up or maintenance phases and good adherence to dose escalation. This approach may represent a practical alternative to more aggressive OIT protocols, particularly for young children or those at higher risk of adverse reactions, and warrants further investigation in larger prospective studies.
Disclosure of the Use of Generative AI and AI-Assisted Technologies
The authors used ChatGPT (OpenAI) during the preparation of this manuscript to assist with grammar checking, language refinement, and improving readability. The content was subsequently reviewed and edited by the authors to ensure accuracy and alignment with the scientific context.
Abbreviations
EY, egg yolk; EW, egg white; OFC, oral food challenge; OIT, oral immunotherapy; EY-OIT, egg yolk oral immunotherapy; EW-OIT, egg white oral immunotherapy; sIgE, serum specific immunoglobulin E; IQR, interquartile range; SD, standard deviation; SU, sustained unresponsiveness; WAO, World Allergy Organization; EAACI, European Academy of Allergy and Clinical Immunology.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional data protection policies but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board and Ethics Committee of Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University (REC 67-433-1-1). Written informed consent was obtained from the parents or legal guardians of all participants prior to enrollment.
Consent for Publication
Not applicable. This manuscript does not contain any identifiable individual person’s data, images, or videos.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no financial or non-financial competing interests related to this work.
References
1. Santadusit S, Atthapaisalsarudee S, Vichyanond P. Prevalence of adverse food reactions and food allergy among Thai children. J Med Assoc Thai. 2005;88(Suppl 8):S27–11.
2. Sicherer SH, Wood RA, Vickery BP, et al. The natural history of egg allergy in an observational cohort. J Allergy Clin Immunol. 2014;133(2):492–499. doi:10.1016/j.jaci.2013.12.1041
3. Savage JH, Matsui EC, Skripak JM, Wood RA. The natural history of egg allergy. J Allergy Clin Immunol. 2007;120(6):1413–1417. doi:10.1016/j.jaci.2007.09.040
4. Gupta RS, Springston EE, Warrier MR, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. 2011;128(1):e9–e17. doi:10.1542/peds.2011-0204
5. Jonsson M, Ekström S, Protudjer JLP, Bergström A, Kull I. Living with food hypersensitivity as an adolescent impairs health related quality of life irrespective of disease severity: results from a population-based birth cohort. Nutrients. 2021;13(7):2357. doi:10.3390/nu13072357
6. Stensgaard A, Bindslev‐Jensen C, Nielsen D, Munch M, DunnGalvin A. Quality of life in childhood, adolescence and adult food allergy: patient and parent perspectives. Clin Exp Allergy. 2017;47(4):530–539. doi:10.1111/cea.12849
7. Eapen AA, Lavery WJ, Siddiqui JS, Lierl MB. Oral immunotherapy for multiple foods in a pediatric allergy clinic setting. Ann Allergy Asthma Immunol. 2019;123(6):573–581. doi:10.1016/j.anai.2019.08.463
8. Burbank AJ, Sood P, Vickery BP, Wood RA. Oral Immunotherapy for food allergy. Immunol Allergy Clin North Am. 2016;36(1):55–69. doi:10.1016/j.iac.2015.08.007
9. Anagnostou K, Islam S, King Y, et al. Assessing the efficacy of oral immunotherapy for the desensitisation of peanut allergy in children (STOP II): a Phase 2 randomised controlled trial. Lancet. 2014;383(9925):1297–1304. doi:10.1016/S0140-6736(13)62301-6
10. Jones SM, Kim EH, Nadeau KC, et al. Efficacy and safety of oral immunotherapy in children aged 1-3 years with peanut allergy (the immune tolerance network IMPACT trial): a randomised placebo-controlled study. Lancet. 2022;399:359–371. doi:10.1016/S0140-6736(21)02390-4
11. Pérez-Rangel I, Rodríguez Del Río P, Escudero C, Sánchez-García S, Sánchez-Hernández JJ, Ibáñez MD. Efficacy and safety of high-dose rush oral immunotherapy in persistent egg allergic children: a randomized clinical trial. Ann Allergy Asthma Immunol. 2017;118(3):356–364.e3. doi:10.1016/j.anai.2016.11.023
12. Martín‐Muñoz MF, Belver MT, Alonso Lebrero E, et al. Egg oral immunotherapy in children (SEICAP I): daily or weekly desensitization pattern. Pediatr Allergy Immunol. 2019;30(1):81–92. doi:10.1111/pai.12974
13. Yanagida N, Sato S, Asaumi T, Nagakura K, Ogura K, Ebisawa M. Safety and efficacy of low-dose oral immunotherapy for Hen’s egg allergy in children. Int Arch Allergy Immunol. 2016;171(3–4):265–268. doi:10.1159/000454807
14. Sasamoto K, Yanagida N, Nagakura K-I, Nishino M, Sato S, Ebisawa M. Long-term outcomes of oral immunotherapy for anaphylactic egg allergy in children. J Allergy Clin Immunol. 2022;1(3):138–144. doi:10.1016/j.jacig.2022.03.005
15. Turner PJ, Ansotegui IJ, Campbell DE, et al. Updated grading system for systemic allergic reactions: joint statement of the world allergy organization anaphylaxis committee and allergen immunotherapy committee. World Allergy Organ J. 2024;17(3):100876. doi:10.1016/j.waojou.2024.100876
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.