Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Design and validation of standardized clinical and functional remission criteria in schizophrenia
Authors Mosolov S, Potapov A, Ushakov U, Shafarenko A, Kostyukova A
Received 15 April 2013
Accepted for publication 7 August 2013
Published 28 January 2014 Volume 2014:10 Pages 167—181
DOI https://doi.org/10.2147/NDT.S46799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Sergey N Mosolov,1 Andrey V Potapov,1 Uriy V Ushakov,2 Aleksey A Shafarenko,1 Anastasiya B Kostyukova1
1Department of Mental Disorders Therapy, Moscow Research Institute of Psychiatry, Moscow, Russia; 2Moscow Psychiatric Outpatient Services #21, Moscow, Russia
Background: International Remission Criteria (IRC) for schizophrenia were developed recently by a group of internationally known experts. The IRC detect only 10%–30% of cases and do not cover the diversity of forms and social functioning. Our aim was to design a more applicable tool and validate its use – the Standardized Clinical and Functional Remission Criteria (SCFRC).
Methods: We used a 6-month follow-up study of 203 outpatients from two Moscow centers and another further sample of stable patients from a 1-year controlled trial of atypical versus typical medication. Diagnosis was confirmed by International Classification of Diseases Version 10 (ICD10) criteria and the Mini-International Neuropsychiatric Interview (MINI). Patients were assessed by the Positive and Negative Syndrome Scale, including intensity threshold, and further classified using the Russian domestic remission criteria and the level of social and personal functioning, according to the Personal and Social Performance Scale (PSP). The SCFRC were formulated and were validated by a data reanalysis on the first population sample and on a second independent sample (104 patients) and in an open-label prospective randomized 12-month comparative study of risperidone long-acting injectable (RLAI) versus olanzapine.
Results: Only 64 of the 203 outpatients (31.5%) initially met the IRC, and 53 patients (26.1%) met the IRC after 6 months, without a change in treatment. Patients who were in remission had episodic and progressive deficit (39.6%), or remittent (15%) paranoid schizophrenia, or schizoaffective disorder (17%). In addition, 105 patients of 139 (51.7%), who did not meet symptomatic IRC, remained stable within the period. Reanalysis of data revealed that 65.5% of the patients met the SCFRC. In the controlled trial, 70% of patients in the RLAI group met the SCFRC and only 19% the IRC. In the routine treatment group, 55.9% met the SCFRC and only 5.7% the IRC. Results of the further independent sample demonstrated that 35% met the IRC, 65% the SCFRC, and 56% of patients met both the symptomatic and functional criteria. In the controlled trial of RLAI and olanzapine, 40% and 35% of patients, respectively, met the IRC, while 70% and 55%, respectively, met the SCFRC.
Conclusion: In schizophrenia outpatients, a greater proportion of stable cases is detected in remission by SCFRC in comparison with IRC. The SCFRC were more sensitive to the full spectrum of schizophrenia. The SCFRC appear to be valid as a tool and clinically useful as they produce a comprehensive assessment of treatment effectiveness for a wide range of patients.
Keywords: schizophrenia, schizoaffective disorder, remission criteria, PANSS, PSP, long-acting risperidone (RLAI)
A Letter to the Editor has been received and published for this article.
Introduction
There is a need for more precise measures of both care quality and the long-term outcome of schizophrenia treatment. A similar requirement exists for a standardized integrative comparison measure of the effectiveness of treatment, as well as standardized criteria for remission of schizophrenia.1,2 Such tools could improve evaluation and prediction of outcome for doctors, patients, and their relatives, so that European Federation of Associations of Families of People with a Mental Illness (EUFAMI) might further explore remission as an important concept for new strategy development in psychiatry.3
Achieving and maintaining remission is the primary aim of outpatient treatment; however, clinicians need to be able to set realistic goals. Schizophrenia is characterized by significant heterogeneity in phenomenology, course and outcome. Therefore, treatment requires a new approach in assessing remission.
Dividing remission into partial and complete, based on residual symptoms using the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV)4 and the International Classification of Diseases Version 10 (ICD10)5, is subjective and does not give an indication of the benefits of treatment or a level of success. Outcome can be defined along dimensional and categorical lines.
There are a number of conceptual studies of schizophrenia remission in Russian psychiatry. These projects mainly relate to the analysis of remission dynamics and typology in different forms of schizophrenia.6–11 The categorical approach is based on the stability of achieved therapeutic effect and the severity of residual symptoms. It differentiates remission into symptomatic, with positive symptoms (ie, thymopathic, obsessive, hypochondriacal, paranoid) and syndromic, with predominantly negative symptoms and personality changes – the so-called “deficit syndrome”, sthenic, pseudopsychopathic (autistic, dependent personality change, Verschrobener-like), apathetic, and asthenic.12 (See the Supplementary information). Furthermore, many authors6–9,11 describe the three main structured components of remission: 1) residual positive symptoms and associated secondary negative symptoms; 2) primary negative symptoms associated with progressive or stable deficit; and 3) compensatory mechanisms. Despite a wide coverage of the different stable states in schizophrenia, a categorical approach has several drawbacks, such as the absence of clear operational criteria, including duration and stability. It is also subjective and does not assess social and cognitive functioning. Moreover, the categorical approach ignores modern multiple-factor models of schizophrenia symptomatology.
The International Remission Criteria (IRC)1 use a dimensional approach, based on the assessment of eight core symptoms on the Positive and Negative Syndrome Scale (PANSS),13 which present discriminated components of the disorder. They incorporate the five diagnostic criteria for schizophrenia as specified in the DSM-IV and in compliance with the three-factor dimensional schizophrenia model,14 including the positive factor (delusions, hallucinations, and unusual thought content), the factor of disorganization (thought disorder, mannerism, and posturing), and the negative factor (blunted affect, social withdrawal, and the lack of speech spontaneity). Remission may be determined when all these symptoms are completely absent or very faintly expressed (1–3 PANSS level) during 6 consecutive months.1 Further cross-sectional naturalistic studies have demonstrated wide assessment variability of the IRC in different populations with schizophrenia, but (in total) about one-third of the outpatients met the IRC.15–19 Approximately 70%–80% of patients in the naturalistic prospective or therapeutic studies maintained this status for more than 6 months.20–28 In a recent German naturalistic study, only 10.3%–13.2% of patients met the IRC within 1 year.28,30 In the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, within 6 months, only 11.7% met the IRC.31 These studies, from the point of view of the suggested criteria, indicate that the overwhelming majority of schizophrenia patients are permanently symptomatic. However, this does not correspond to clinical reality.
Additional IRC limitations were found in further studies. First, the suggested threshold level for the chosen symptoms was only achievable in approximately 20% of the clinically stable patients.32,33 Second, Wobrock et al34 found that the possibility of remission varied within the different ICD10 diagnoses. Remission was most likely in patients with paranoid schizophrenia (odds ratio [OR] =1.54) and least likely in patients with residual schizophrenia (OR =0.41). Third, Eberhard et al35 demonstrated that not all of the suggested eight PANSS symptoms were specific for the diagnosis of remission in schizophrenia. The most nonspecific symptom was lack of spontaneity of speech (N6). Through discriminant analysis, it was also identified that the most distinctive symptoms were depression (G6) and preoccupation (G15). In addition, the authors insisted on including the item “lack of judgment and insight” (G12), showing interplay between cognitive impairment and adequate patient self-judgment and self-control. Other studies showed a close relationship between cognitive deficit and the stability of remission.17,20,25 A number of authors indicated that the IRC were mainly nonspecific and hardly differed from the psychosis global severity assessment of the Clinical Global Impression-Schizophrenia scale, which determined remission as a “not more than mild” level of psychotic intensity.16,18,36 It is obvious that major limitations of the IRC include low sensitivity, particularly for the continuous forms of the disease’s course, as they lack a social functioning assessment which ignores the quality and psychopathologic peculiarities of remission in different clinical forms and types of schizophrenia, including affective symptoms, cognitive functioning, insight, and compensatory personality phenomena.
Therefore, the design and validation of the new standardized schizophrenia remission criteria for different clinical forms and courses of the disease and a categorical typology of remissions, including the level of social functioning, are of obvious interest.
The main aim of this study was to develop and validate the Standardized Clinical and Functional Remission Criteria (SCFRC) in schizophrenia.
Materials and methods
To develop and validate the SCFRC, the study was designed in three stages:
- First stage: a cross-sectional study with a 6-month follow-up was conducted at two health care centers at a standard Moscow psychiatric outpatient service to determine remission stability and whether the patient met the IRC. The rate and specificity of remission for various clinical forms and courses were identified using the ICD10 classification. We analyzed the prevalence of PANSS symptoms, with symptom severity corresponding to the three-factor schizophrenia model and the Russian categorical remission typology.
- Second stage: we performed a naturalistic, controlled trial of modern versus routine therapeutic approaches in a group of stable patients who did not satisfy the remission criteria within 6 months. The modern approach used at the first health care area, relied on monotherapy with risperidone long-acting injection (RLAI). The second health care area used the routine approach and employed first-generation antipsychotics (1-year observational therapeutic study).
The SCFRC were formulated on the basis of these two studies. - Third stage: validation of the proposed SCFRC was carried out, based on a reanalysis of the cross-sectional study, and the controlled trial. The SCFRC were compared with the IRC in these studies for applicability and validation.
The first and second stages of the study were conducted in the Moscow Psychiatric Outpatient Services #21 (Moscow) at two randomly chosen psychiatric care districts, where all patients with an ICD10 diagnosis of schizophrenia (F20.0, F20.1, F20.2, F20.3, F20.5, and F20.6) and schizoaffective disorder (F25) were examined. Patients with a diagnosis of F20.8 (other schizophrenia); of F20.9 (unspecified schizophrenia); and of other psychotic, schizotypal, and delusion disorders were excluded. In addition, the number of patients who became stable within 6 months but who did not correspond to the remission criteria was calculated. Stability was defined as no change of a PANSS total score >20% and/or >1 point for any of positive subscale items – P1, P2, P3, and P6, regardless of the baseline rating. Categorical remission types were determined by the Smulevich classification,12 differentiated into symptomatic, with positive symptoms (thymopathic, obsessive, hypochondriacal, paranoid) and syndromic, with predominantly negative symptoms (sthenic, pseudopsychopathic, apathetic, and asthenic) (see Supplementary materials).
However, remission types corresponded more closely to the definitions of Zenevich,11 in which the leading sign, symptom, or group of symptoms, which best characterized the patient state in remission, was used to separate specific types. Zenevich described sthenic, pseudopsychopathic, paranoid, autistic, apathetic, hypochondriac, and asthenic types of remissions and considered that, in reality, the types have no clear borders, which was why he proposed differentiating by the leading clinical sign that best characterized the patient state in remission. Besides clinical criteria, he also proposed to use additional social and occupational criteria. A hierarchy of remission variants, based on the type of personality and the leading compensatory mechanisms, as defined by Kotsyubinsky et al,6 was also used. Kotsyubinsky et al described the sthenic, asthenic, thymopathic, psychasthenic, pseudopsychopathic, paranoid, autistic, apathetic, and hypochondriac types of remissions and proposed a hierarchy of five variants of compensatory reactions: full judgment and correct appraisal of psychotic symptoms, dual judgment of psychotic symptoms, rationalization, repression, and amalgamation, that correspond to a different level of personality integrity and social functioning.
At the second stage, all stable patients not meeting symptomatic remission criteria were given the opportunity to participate in a 1-year controlled trial. The first health care area patients (first group) were offered the option to switch from their current antipsychotic medication to the RLAI within a government-reimbursement program, while the second health care area patients (the second, or control group) continued treatment with routine naturalistic therapy (mostly first-generation antipsychotics). Data were collected during regular visits to the attending psychiatrist after obtaining a written, informed consent for participation in every study. In addition, 203 of 233 patients met the inclusion criteria and gave informed consent to participate in the study – 114 at the first health care center and 89 at the second. At both, most patients were women (56.2%); mean age was 52±15.0 years; and mean disease duration was 24.4±13.2 years. Also, 144 (70.9%) of the patients experienced paranoid schizophrenia (F20.0); ten patients had undifferentiated schizophrenia (F20.3; 4.9%), 28 had residual (F20.5; 13.8%), six had the simple form (F20.6; 2.95%), and nine had schizoaffective disorder (F25; 4.4%).
Hebephrenic (F20.1) and catatonic (F20.2) schizophrenia forms were identified in isolated cases; two (1%) and four (2%), respectively. The mean total PANSS score across the sample was 69.2±24.9. In the Global Assessment of Functioning (GAF) scale,4 56.7±11.0; 62.1% of the patients were treated with first-generation antipsychotics in different combinations, 12.3% of the patients received other atypical antipsychotics, 6.9% received traditional and atypical antipsychotics’ combination, and 18.7% did not receive antipsychotic agents.
At the first health care area, 42 patients were enrolled in the RLAI group. Then, 35 patients from the second center continued routine treatment assigned in outpatient service. Groups were comparable within basic clinical and demographic parameters. The mean age was 43.7±13.4 years in the first group and 45.4±14.2 years in the second group. The mean disease duration was 16.8±11.7 years and 15.7±12.3 years, respectively. The majority of patients in both groups had paranoid schizophrenia (71.4% in the RLAI group and 68.5% in the group of routine therapy). The mean PANSS score was 65.7±11.3 in the first group and 68.3±10.5 in the second group. The mean Personal and Social Performance (PSP) score was 52.3±13.4 points in the first group and 54.4±12.9 in the second. Extrapyramidal side effects on the Simpson–Angus Scale were 4.4±5.7 and 4.9±5.2 points, respectively.
Treatment was administered by the district psychiatrist during regular medical check-up visits to the outpatient services in each area. At the first health care area, the long-acting RLAI (dose range, 25 mg/37.5 mg/50 mg) was given every 2 weeks. All other antipsychotic agents were prohibited; only 2 mg or 4 mg of risperidone tablets were allowed during the titration period or in the case of the exacerbation of psychotic symptoms, but for no longer than 2 weeks. In the second area, patients were treated by the routine approach: 24 (68.6%) patients received monotherapy with traditional neuroleptics (seven, haloperidol; five, haloperidol decanoate; four, fluphenazine decanoate; three, trifluoperazine; two, zuclopenthixol decanoate; two, flupenthixol decanoate; and one, chlorpromazine), five (14.3%) patients had monotherapy of atypical antipsychotics (two oral risperidone, one clozapine, one quetiapine) and six (17.1%) patients had a combination treatment with several antipsychotics. Antiparkinsonian (anticholinergic) drugs, antidepressants, mood stabilizers, hypnotics, and benzodiazepines were temporarily allowed if required.
At the third stage, two independent validation studies were conducted with database reanalysis of the cross-sectional and pharmacotherapeutic studies. The outpatients ranged in age from 18 to 65 years, with an ICD10 diagnosis of schizophrenia (F20) or schizoaffective disorder (F25), with a global PANSS score of no less than 60. They were enrolled in a nested comparative randomized study of RLAI and olanzapine. Patient status was independently evaluated before treatment and at months 3, 6, 9, and 12 (raters used the IRC and the SCFRC). In total, 40 patients were enrolled in the study, distributed randomly among therapeutic groups with 20 patients in each group. Groups were comparable by basic clinical and demographic parameters. In the group of RLAI, the mean age was 32.5±8.18 years, and the mean illness duration was 9.3±6.6 years. In the group of olanzapine, the mean age was 36.5±9.04 years, and the mean illness duration was 12.9±9.03 years.
Symptomatic and functional criteria of SCFRC in comparison with the IRC (without duration criterion) were validated using an independent sample of schizophrenia outpatients. Independent experts verified diagnosis, rated scales, and assessed the IRC and the SCFRC. All voluntary consented patients at one health care area of the Moscow Psychiatric Outpatient Services #1 in Moscow were enrolled in accordance with the same criteria as at the first stage. Therefore, 104 patients were enrolled in the study; 57 (55%) were women. Paranoid schizophrenia with continuous course (F20.00) was diagnosed in 25 (24%) patients, paranoid schizophrenia with episodic course and progressive deficit (F20.01) in 23 (22%), paranoid schizophrenia with episodic course and stable deficit (F20.02) in 27 (26%), paranoid schizophrenia with remittent course (F20.03) in five (15%), undifferentiated schizophrenia (F20.3) in seven (7%), and schizoaffective disorder (F25) was diagnosed in eight patients. The mean age of the patients was 46.9±14.1 years; the mean duration of the illness was 18.2±11.4 years. Eighty-five (82%) were treated with first-generation antipsychotics, including different combinations. Seven (7%) were treated with second-generation antipsychotic agents. Three (3%) were treated with a combination of atypical and traditional antipsychotic agents. Nine (9%) patients did not receive any antipsychotic treatment.
Assessment
The IRC assessment was performed, according to the operational criteria set up by the Remission Schizophrenia Working Group.1 The symptomatic criteria included eight core PANSS items (delusions, unusual thought content, hallucinations, conceptual disorganization, mannerisms or posturing, blunted affect, social withdrawal, lack of spontaneity) with a score ≤3. The duration criterion was symptomatic remission maintained over 6 consecutive months.
The ICD10 diagnosis in all studies was verified by the Mini-International Neuropsychiatric Interview (MINI),37 as well as by the analysis of data received from the patient medical files. Further verification was obtained in interviews with both the patient and their relatives. In the cross-sectional population study with the 6-month follow-up, symptomatology of the homogeneous outpatient cohort was assessed using the validated Russian language version of PANSS,38 and social functioning with the GAF scale.4 In the observational 1-year trial, the symptom severity was assessed with PANSS,38 functioning level with the PSP scale,39 and compliance with Rating of Medication Influences.40 All adverse events were registered during treatment. Extrapyramidal symptoms were additionally assessed using the Simpson–Angus Scale.41
Statistical analysis
Statistical analysis was performed using the software STATISTICA 6.0 (StatSoft Inc., Tulsa, OK, USA). Descriptive statistics, such as the mean value, standard deviation, and 75th percentile (the threshold value for at least 75% of cases) were used. Statistical variance for quantitative data, expressed in absolute values with normal distribution and equal dispersions, was calculated using the two-sided Student’s t-test. Comparison of independent continuous non-normally distributed variables was performed using the Mann–Whitney U test. For relative values, the Fisher criterion was used. Dependent variables were compared using the Wilcoxon matched-pair test and the Friedman analysis of variance (ANOVA). Spearman’s rank order correlation (R-values) was used as a measure of association between remission probability and different baseline patient characteristics in the 1-year observational study. The predictive value of various factors in the population study was assessed with logistic regression. The general linear univariate model procedure was used to perform analysis of covariance (ANCOVA) to determine the effect of the PANSS item scores (covariates) on the degree of symptomatic remission (dependent variable), depending on different ICD10 diagnoses as the categorical factor. The OR procedure and the logistic regression were used to evaluate associations between categorical factors (ICD10 diagnoses, illness courses, etc) and symptomatic remission. Missing data were substituted with sample averages in the cross-sectional population study, and in the 6-month follow-up and the 1-year observational therapeutic studies, the last observation carried forward procedure was used.
Ethical considerations
The local ethics committee of the Moscow Research Psychiatry Institute approved the study design, methods, therapeutic interventions, and the text of the patient information list in compliance with the Declaration of Helsinki. All included patients provided separate informed consent for participation in different parts of the study.
Results
First-stage results, cross-sectional population study with prospective 6-month follow-up
The cross-sectional study identified 64 out of the 203 outpatients (31.5%) as corresponding to the IRC symptomatic criteria; at the same time, 139 subjects (68.5%) did not meet the IRC. Only 53 patients (26.1%), who previously corresponded to the IRC, maintained their status during the further 6-month follow-up period without changing their treatment regimen. In the same period, 105 out of the 139 patients (51.7%), who did not previously meet symptomatic criteria, remained stable throughout. Most patients, who met the IRC, were diagnosed as having episodic (21/39.6%) or remittent (eight/15.0%) courses, according to the ICD10, of paranoid schizophrenia, or schizoaffective disorder (nine/17.0%). The subjects with more severe illness forms predominated in the group of stable patients who did not meet the symptomatic criteria. These forms included continuous (43/41.0%) and episodic with stable deficit (31/29.5%) courses of paranoid schizophrenia, undifferentiated (six/5.7%), residual (16/15.2%), and hebephrenic (two/1.9%) or catatonic (three/2.9%) schizophrenia.
All patients were assessed according to their category of clinical remission. Out of 203 patients, 15 (7.4%) had remissions with no residual symptoms. Symptomatic remission, with residual positive symptoms, was observed in 84 patients (46% from all patients in remission), and syndromic remission, with “deficit status” and the domination of different negative symptoms or personality changes, in 83 patients (45.6%) (Table 1).
 | Table 1 Distribution of categorical (clinical) remission types (cross-section population study) |
The association of a categorical remission clinical type with an ICD10 diagnosis was evaluated in the stable patients, who met or did not meet the IRC. Paranoid schizophrenia patients with a continuous course had a mean total PANSS score of 74.2±9.2 and a GAF score of 53.0±6.9. The most frequently observed remission types were paranoid and apathetic, in 25 patients (55.6%) and 15 patients (33.3%), respectively. In paranoid schizophrenia with an episodic course, the PANSS mean score was 55.1±7.7 and GAF, 67.9±12.3. Those patients in remission were more variable: paranoid remission – 18 (34.6%); pseudopsychopathic – 10 (19.2%); thymopathic – 7 (13.5%); and asthenic – 7 (13.5%). Half of the patients with remittent courses of paranoid schizophrenia had an intermission – 4 (50%); 2 (25%) patients had paranoid and 2 (25%) had thymopathic remission types. The PANSS mean score was 40.4±4.0, and the GAF score was 78.3±4.5. In the undifferentiated schizophrenia form, PANSS and GAF mean scores were 66.8±11.0 and 58.5±6.3, respectively. Variants of remission types were: paranoid, three (37.5%); pseudopsychopathic, two (25%); thymopathic, one (12.5%); and asthenic, one (12.5%). Residual schizophrenia was characterized by apathetic remission prevailing, eight (32%); then thymopathic, four (16%); pseudopsychopathic, four (16%); paranoid, three (12%); and asthenic, two (8%). In simple schizophrenia, different negative symptoms and other axis impairments were dominant, so that apathetic four (66.7%) and asthenic two (33.3%) remissions were observed most frequently. The PANSS and GAF mean scores were 57.8±2.3 and 59.3±7.5, respectively. In schizoaffective disorder, most of the patients had intermission – 5 patients (55.6%). Both thymopathic and asthenic remission were observed in an equal number of patients, two (22.2%) each. The PANSS mean score was 41.9±6.2; GAF, 79.8±4.6.
In 53 patients, who met the IRC, 28.3% had remissions with no residual symptoms, 30.2% were in thymopathic remission type; 26.4%, asthenic; 7.5%, sthenic; 3.8%, paranoid; 1.9% hypochondriacal and pseudopsychopathic. Among 105 stable patients, who did not meet IRC, 46.7% had a paranoid type of remission; 29.5% apathetic; 19.1% pseudopsychopathic; and 1.9% asthenic. Other variants were observed in isolated cases. In short, the patients who satisfied the IRC showed the most favorable remission types (sthenic, asthenic, and thymopathic) without expressed deficit symptoms or gross personality pathology. In the stable patient group, who did not meet IRC, more severe personality changes were observed (pseudopsychopathic, paranoid, and apathetic types of remission), and among compensatory mechanisms we observed that isolation, and an amalgamation of psychotic experiences prevailed.
The analysis of patients in different categories of remission identified the essential psychopathological domains from which the quantified operational criteria of remission were designed. First, there are positive symptoms, which in the majority of stable outpatients, do not achieve threshold PANSS levels suggested by the IRC group. Second, there are negative symptoms (asthenic, apathetic, and abulic symptomatology, emotional flattening, social withdrawal, and autism). Third, there are thought and speech disorders and affective symptoms (depression and acquired cyclothymia). Participation of compensatory mechanisms, specific for certain remission types and clinical forms, indicates that it is necessary to allocate insight and judgment as one of the most important components of remission.
Categorical remission types were analyzed in contrast with the three-factor dimensional model of schizophrenia. This model could not describe all the observed symptomatology. Affective symptoms must be included within standardized criteria. In addition, we found other symptoms that are not recognized in the IRC: volitional impairment expressed by vacillation and ambivalence (changes related to dependent personality change), impulsivity, and internal motive control disturbances in patients with pseudopsychopathic remission, lack of communicativeness, social avoidance, and emotional withdrawal in autistic remission, as well as disbulic signs in pseudopsychopathic remission and Verschrobener personality changes.
The severity of eight PANSS symptoms of IRC was followed. Threshold for 3 and fewer points appeared to be unachievable for some types and courses of schizophrenia in spite of long-term stability and treatment with the most modern medications.25 First, the IRC-proposed threshold was achievable by all symptoms in only paranoid schizophrenia with remittent course and schizoaffective disorder. Second, the different clinical types of schizophrenia failed to meet this level in different symptomatic dimensions. Thus, paranoid schizophrenia with continuous course and undifferentiated schizophrenia did not meet symptomatic remission for positive and negative symptom dimensions, while for paranoid schizophrenia with episodic course, residual, and simple schizophrenia, only negative symptom dimension was unachievable. The logistic regression model revealed that the ICD10 diagnosis (remittent and episodic with progressive deficit paranoid schizophrenia, F20.01, F20.03, and schizoaffective disorder F25 versus other) (OR =5.95) and the GAF score (OR =1.29) significantly predicted the outcome of symptomatic remission; whereas, the history of psychotic disorder in first-degree relatives (OR =0.44) and presence of disability (OR =0.64) decreased the likelihood of symptomatic remission. Age, illness duration, and previous antipsychotic treatment (atypical versus typical) variables did not reach statistical significance.25
Second-stage results, 12-month prospective naturalistic therapeutic study
While using IRC as a treatment efficacy measure, it was found out that after switching to RLAI, three times more patients achieved remission (19%) in comparison to the control group continuing routine therapy (5.7%).25 The correlation, ANCOVA and regression analyses demonstrated that, first, a lower PANSS total score (status severity) and more favorable diagnosis, according to the ICD10, are associated with a higher probability of remission. Second, remission is not predetermined by a mere symptom reduction. Third, remission is closely related to social functioning improvement, and an initial lower level of social and cognitive functioning is associated with a lesser probability of remission.
Standardized clinical and functional remission criteria
The SCFRC were formulated, based on the data of the cross-sectional population and observational pharmacotherapeutic studies (Table 2).
 | Table 2 SCFRC in schizophrenia according to the ICD10 diagnosis |
The PANSS level of all symptoms should be 3 points or less for determining remission in schizoaffective disorder, episodic course with progressive deficit and remittent courses of paranoid schizophrenia. The PSP functioning level should be 71–80 or more.
For continuous paranoid schizophrenia the severity threshold for the items “delusions” and “unusual thought content” should be 5 points or less; for “hallucinations,” it should be 4 points or less. For negative symptoms (“blunted affect”, “passive or apathetic social withdrawal”, and “lack of spontaneity and flow of conversation”), an acceptable level is 4 points or less. Symptoms of disorganization (“conceptual disorganization”, “mannerisms and posturing”) should be 3 points or less. Intensity of “depression” and “lack of judgment and insight” items should be not higher than 3 and 4, respectively. The PSP functioning level should be not less than 51–60 points.
To determine symptomatic remission in paranoid schizophrenia with episodic course and stable deficit, symptom severity level of positive (“delusions”, “unusual thought content”, “hallucinations”) and disorganization factors (“conceptual disorganization”, “mannerism and posturing”) should be 3 points or less. Intensity of “blunted affect” and “passive or apathetic social withdrawal” negative symptoms is compliant with a level of 4 points or less, and for the item “lack of spontaneity and flow of conversation” – 3 points or less. Intensity of “depression” and “lack of judgment and insight” should be at 3 points or less. The PSP functioning level should be about 51–70 points.
A level of 4 points or less is acceptable in undifferentiated schizophrenia for intensity of positive (“delusions,” “unusual thought content”, “hallucinations”) and negative (“blunted affect” and “passive or apathetic social withdrawal”, “lack of spontaneity and flow of conversation”) symptoms. Symptoms of disorganization factor (“conceptual disorganization”, “mannerism and posturing”) should be at a level of 3 points or less. Severity of “depression” and “lack of judgment and insight” should be at 3 points or less. The PSP functioning level should not be less than 51–60 points.
In residual schizophrenia, symptoms “delusions” and “hallucinations” are absent, but some patients in remission experience symptoms of “unusual thought content”, the severity of which should not be higher than 3 points. Symptoms of disorganization factor (“conceptual disorganization”, “mannerism and posturing”) should be at a level of 3 points or less. Negative symptomatology (“blunted affect” and “passive or apathetic social withdrawal”, “lack of spontaneity and flow of conversation”) should be consistent with a level of 4 points or less. Severity of “depression” and “lack of judgment and insight” should be at 3 points or less. The PSP functioning level should be around 51–70 units.
The pseudopsychopathic type of remission is possible in some cases of paranoid schizophrenia with continuous or episodic course with stable deficit, undifferentiated schizophrenia, and residual schizophrenia. To determine remission adequately in these patients, additional PANSS items should be used. Thus, in the clinical variant of autistic remission, severity of “emotional withdrawal” should be at a level of 4 or less. In remission with the acquired traits of dependent personality level of “disturbance of volition”, the level should not be above 3 points. Additional items of supplemental PANSS subscale for assessment of aggression risk (“difficulties in delay of gratification” and “affective lability”) should produce a level of 4 points or less in a genuine pseudopsychopathic variant of remission.
In simple schizophrenia, positive symptoms are absent: “mannerisms and posturing” may be at a minimal level of 3 points or less. Negative symptoms (“blunted affect” and “passive or apathetic social withdrawal”, “lack of spontaneity and flow of conversation”) should be at a level of 4 points or less. Severity of “depression” and “lack of judgment and insight” should be at 3 points or less. The PSP functioning level should be about 51–70 points.
Results of third-study stage, standardized clinical and functional remission criteria validation
Database reanalysis of cross-sectional population and 1-year prospective observational pharmacotherapeutic study
Repeated data analysis of the cross-sectional population study demonstrated that 65.5% of patients corresponded to the new SCFRC, while only 31.5% of patients met the symptomatic IRC (Figure 1). Data reanalysis of the 1-year observational therapeutic study demonstrated that the SCFRC cover about four times more stable patients than the IRC. After 12 months of treatment, 70% of patients corresponded to the SCFRC in the RLAI group and 55.9% in the routine therapy group. At the same time, in the RLAI group, only 19% of patients satisfied IRC; in the control group, it was 5.7% (Figure 2).
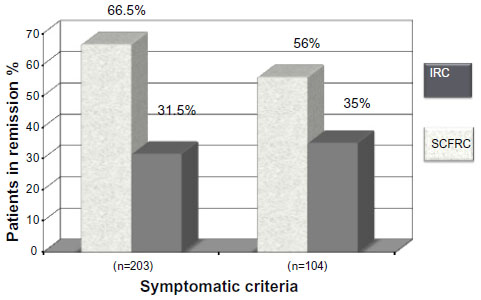 | Figure 1 Comparative sensitivity and validity of symptomatic IRC and SCFRC in two independent populations of schizophrenic outpatients. |
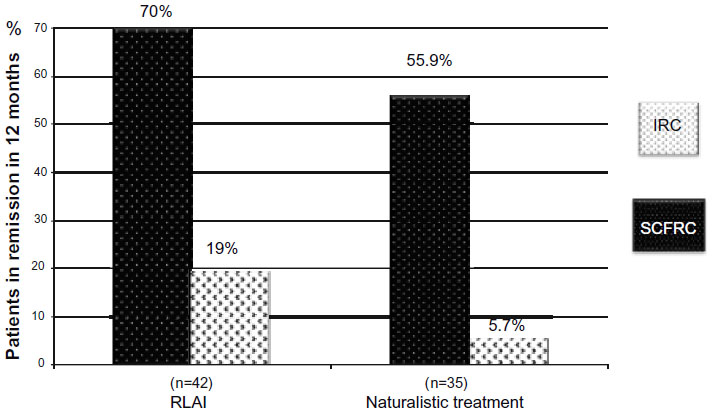 | Figure 2 Comparative sensitivity and validity of IRC and SCFRC. |
Results of nested open-label randomized trial; 12-month study of RLAI versus olanzapine
At 12 months, 45% of the patients corresponded to the symptomatic, and 40% to the symptomatic and duration IRC criteria in the RLAI treatment group, 50% of patients met the symptomatic criteria, and 35% met the duration criterion within the olanzapine group. When SCFRC was used, in the RLAI group, 80% of patients met the symptomatic criteria, and 70% met the duration criterion. In the olanzapine group, 60% and 55% of patients met those criteria, respectively. Therefore, by considering the broader range of clinical forms and courses, remission in schizophrenia could be diagnosed more widely. Difference in remission rates between SCFRC and IRC is shown in Figure 3.
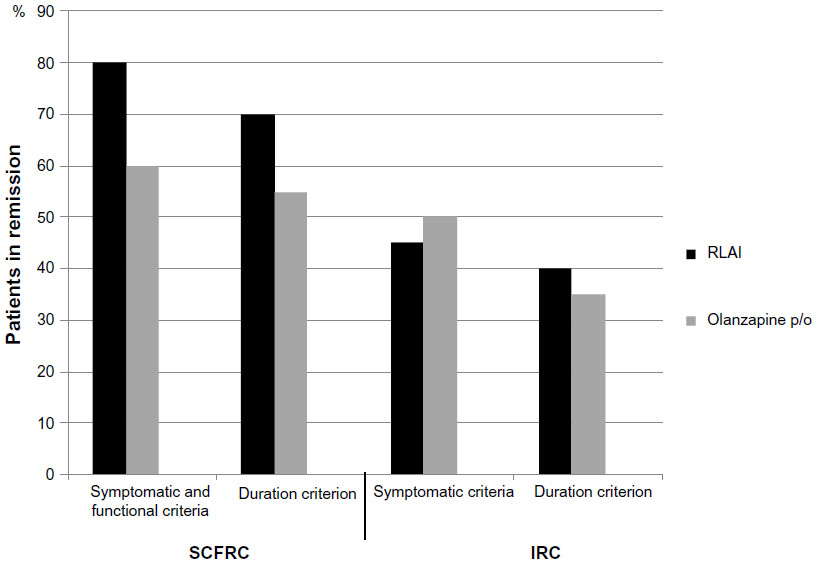 | Figure 3 Remission rate according to SCFRC and IRC on 12 months of comparative randomized trial of RLAI and olanzapine. |
Results of remission criteria validation in independent outpatient sample, a cross-sectional population study
Only 35% of the patients met the symptomatic IRC, 65% of the patients satisfied the symptomatic SCFRC, and 67% the functional criterion; 56% of patients met both symptomatic and functional remission criteria (Figure 1). Rate distribution for both of the remission criteria (dependent on the ICD10 diagnosis) is shown in Table 3.
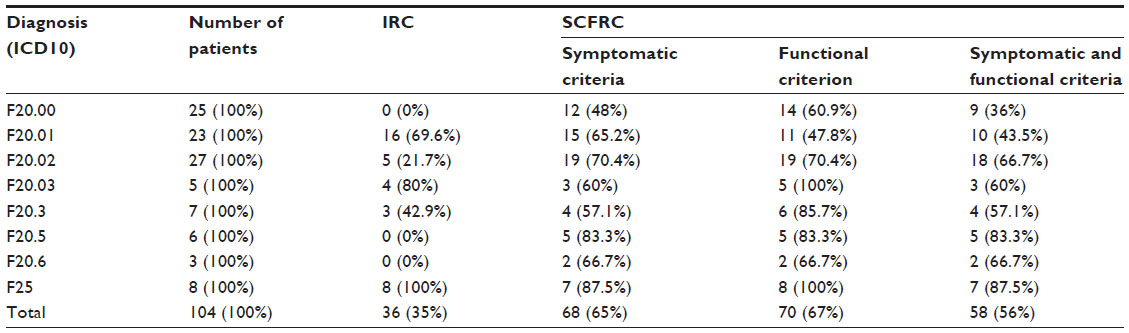 | Table 3 Distribution of patients in remission who met the SCFRC and the IRC, according to the ICD10 diagnosis in an independent sample of schizophrenic outpatients (cross-sectional population study) |
Any patient with continuous paranoid schizophrenia did not meet the IRC; at the same time, 36% of patients met the SCFRC. However, 69.6% of the patients with episodic course and progressive deficit paranoid schizophrenia met the IRC, and only 43.5% met the SCFRC. Moreover, 80% of patients with remittent paranoid schizophrenia, and 100% of patients with schizoaffective disorder met the IRC, and only 60% and 85.5% achieved the SCFRC symptomatic threshold for these diagnoses. In other words, the suggested criteria were more sensitive in respect to these patients, and this should alert the clinician with regards to possible treatment modification to achieve a better outcome.
One-factor analysis of the variance of conformity between the ICD10 diagnosis and the remission criteria discovered an absence of any statistically significant influence of diagnosis on the SCFRC, which demonstrates a greater diagnostic stability in comparison with IRC, in which the diagnostic sensitivity changed, according to the ICD10 diagnosis (Figure 4).
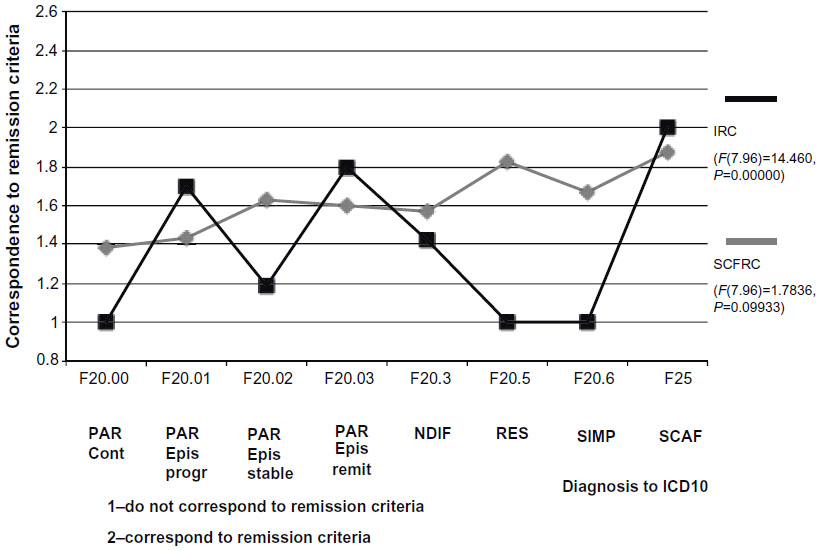 | Figure 4 One-way analysis of variance of correspondence to the remission criteria (IRC and SCFRC) to diagnosis by ICD10. |
In Table 4, the descriptive statistics are presented for every PANSS item of the SCFRC and the PSP score, according to the ICD10 diagnosis. Overall, the suggested symptom thresholds were adequate for all diagnosis variants. The mean score for the item “conceptual disorganization” was slightly higher than suggested in the group of continuous paranoid schizophrenia patients, which decreased the SCFRC achievement rate for this diagnosis.
 | Table 4 Descriptive statistics of PANSS items and mean PSP score, according to ICD10 diagnosis |
Discussion
The international expert working group for consensus on remission criteria in schizophrenia defined remission as:
[…] an improvement in core signs and symptoms to the extent that any remaining symptomatology is of such low intensity that it no longer interferes significantly with behavior, and is below the threshold typically utilized in justifying an initial diagnosis of schizophrenia1
and offered the IRC, based on eight symptoms.
Lately, it has been shown that the suggested approach and criteria were only partially reflecting clinical reality. According to the results of a few past studies, only one-third of the cases in the patient population achieve symptomatic remission,17,19,24 and only approximately 10% maintain remission in the long-term.29–31 Our recent study from a city outpatient schizophrenia sample has shown that the majority of patients with a stable symptomatology and chronic illness course (about 80%) do not achieve the suggested IRC. This remains the case, even after switching to treatment with a more modern long-acting atypical antipsychotic (RLAI).25 Results of this study concur with the Wobrock et al34 data; that is to say, that paranoid schizophrenia patients with episodic or remittent courses are more likely to meet the IRC than patients with other ICD10 diagnosis types (for example, residual schizophrenia), as well as with the data of other investigators, who indicated that symptoms such as depression, illness insight, cognitive impairment, and, most essentially, level of social functioning, should be considered in remission criteria.17,20,35,42,43 Otherwise, for most chronic patients in stable status, clinically evaluated by the attending psychiatrist as to their possible remission, the symptomatic IRC threshold is not met. Our preliminary cross-sectional study of the outpatient schizophrenia population with the 6-month follow-up period also demonstrated that the most important factors influencing the ability to meet the IRC were the type of disease course, the severity of status, and the level of functioning.25 So, we believe that definition of remission formulated by Zenevich11 as:
[…] a resolution or alleviation of psychopathological symptoms and achievement of various levels of functional recovery that include an interval from full recovery (symptomatic and functional) to marked deficit […]
is close to actual clinical practice and allows the development of a more efficient remission model in schizophrenia.
Our operational remission criteria are based on this approach and, from the one hand, we are considering the Kraepelinian schizophrenia forms and course types accordance to the ICD10, with clinical (categorical) peculiarities of the different deficit states in schizophrenia (affective symptoms, disturbance of volition, insight of illness, and some other important PANSS symptoms were added), as well as a level of social adaptation. On the other hand, we based our criteria on the contemporary dimensional model and used validated operational definitions and intensity grades of PANSS symptoms with the quantified assessment of the functioning level by the PSP scale. The most important features of the proposed SCFRC are the following: first, these criteria encompass all the symptoms of the IRC, use operational definitions of the most widespread, internationally accepted and validated scales (PANSS and PSP), and consider all three dimensions of schizophrenia phenomenology. Second, it is noteworthy that an episodic course with a progressive deficit, a remittent course of paranoid schizophrenia and schizoaffective disorder, was pooled in a single remission group because of the possibility to achieve minimal level for all chosen symptoms. Third, symptoms from the Supplemental Aggression Risk subscale of PANSS (difficulty in delay of gratification and affective lability) were chosen for the description of the volition distortion, which is frequently present in patients with so-called pseudopsychopathic remission. Practically all positive symptoms were excluded from the remission criteria for simple and residual schizophrenia. However, remission criteria were not developed for hebephrenic and catatonic schizophrenia, due to their low prevalence in our population study.25 A validation of the SCFRC showed that they cover a greater percentage of the stable schizophrenia outpatients in comparison with the IRC. This is more consistent with the domestic approach to remission in schizophrenia and also considers diversity of disease outcomes. In addition, the SCFRC differentially estimates the possibility of remission in the whole spectrum of the ICD10 schizophrenia diagnoses and could serve as a strict integral standard to status evaluation, which allows for more accurate decision-making, concerning both the remission quality and any prediction of the course of the individual’s illness.
The development and the validation of the suggested criteria have a number of limitations. First, the sample size is not sufficient. It covers only outpatient schizophrenia subjects, who have regular medical check-ups, in a city district population of approximately 50,000 people. In spite of the fact that the outpatient psychiatric service and city area were chosen randomly, we do not believe that the sample was broadly representative. Indeed, in other populations – for example, in the rural areas – different data could be obtained. Second, the influence on the symptomatology assessment of the subjective factors cannot be excluded, as well as the additional psychotherapeutic effect, for example, more frequent visits for treatment and, additionally, because the study was not blinded and was conducted by two investigators at one site. Third, the study was observational and did not have strict explorative (scientific) objectives so that the relevance of the suggested criteria (symptoms and its PANSS levels) can only be asserted with reasonable confidence regarding the paranoid and partially residual schizophrenia forms. Other forms were observed rarely. The samples were not representative, and the criteria for these groups are preliminary as the suggestion for discussion and confirming in special patient samples. This very fact does not allow setting up any operational criteria for the catatonic and the hebephrenic forms.
Furthermore, it is unclear whether the different forms of the illness and their courses are stable over a lifespan, and thus whether the remission criteria will correspond to these possible course changes. In addition, the suggested criteria, unfortunately, do not consider such important factors as cognitive functioning, compliance, and quality of life, including subjective tolerance to long-term pharmacotherapy. The importance of considering cognitive impairment in remission criteria was shown in many studies17,20,42 including our study,25 but it is a difficult task to choose simple but not exhaustive tests for the routine dynamic assessment of cognitive functioning, which are inclusive for all categories of schizophrenia patients. Fourth, the validation process was not sufficient, did not include such generally accepted validation approaches as concurrent validity, contrasted groups validity, interrater reliability, or a sensitivity/specificity/efficiency analysis. We also did not assess the criteria of long-term stability and undertook only external validation of symptomatic criteria (cross-sectional naturalistic study) in a limited schizophrenia outpatient population of one city area of psychiatric health care service and one open controlled trial with simple randomization. In spite of the fact that the assessment was done by independent experts and that the SCFRC demonstrated greater sensitivity, the final results should be interpreted with caution, and the suggested criteria need to be discussed and validated in further independent prospective studies.
Conclusion
Based on our studies, we suggest the extended operational SCFRC, which cover different clinical forms and courses of schizophrenia and schizoaffective disorder, as well as a level of social functioning. These new criteria are more acceptable in comparison with international ones (IRC) for a wide range of schizophrenia patients. They allow a more realistic modeling of therapeutic goals and may encourage clinicians to look for more effective treatment approaches, including modern antipsychotic pharmacotherapy in combination with psychosocial, psychoeducational, and psychotherapeutic activities to achieve more increased and better qualitative remission in a larger number of patients.
Author contributions
SNM provided the idea and the design of the study, participated in the study organization, patient consulting, data analysis, and drafting of the manuscript. AVP performed clinical assessments, including the scale rating and cognitive testing, statistical analysis, and participated in text drafting. UVU, as a district psychiatrist at Moscow Psychiatric Outpatient Service #21, was responsible for patient recruitment, diagnosing, and treatment. AAS and ABK were independent raters in validation studies and performed all assessments at Moscow Psychiatric Outpatient Service #1 and in a comparative open-label randomized 12-month study of RLAI and olanzapine. All authors contributed toward data analysis, drafting, and revising the manuscript. All authors read and approved the final manuscript.
Acknowledgments
The authors thank the executive chief doctors of Moscow Psychiatric Outpatient Services #21 (Dr Larisa Burygina) and #1 (Dr Irina Zabelina), as well as all the medical personnel for their help in organizing and facilitating this study. The authors are also very thankful to Professor Steven Hirsch and to Dr Timothy Brow for the language editing and professional advice as well as to Ms Emma Brow and Dr Dkhaval Mavani for their English editing and technical support.
Disclosure
SNM has been a consultant or/and a free speaker for AstraZeneca, Bristol-Myers Squibb, Janssen-Cilag, Eli Lilly and Company, Lundbeck, Pfizer, and Sanofi-Aventis. UVU has been a free speaker for Janssen-Cilag. AVP, AAS, and ABK report no conflicts of interest in this work.
Supplementary materials
Glossary
Deficit syndrome
An observed state in a patient following acute psychotic illness whereby the patient has marked negative symptoms as described by the IRC and/or new personality traits (changes or shift in personality) and/or cognitive deficit, including thought disturbances, loosening of associations, etc. So the term resembles the contemporary notion of primary negative symptoms and marked cognitive disturbances acquired during the illness process (in the older Kraepelinian sense of “defect”).
Disbulia
Weakness and uncertainty of volition, any disturbance of the will or of the mental processes that lead to purposeful action (hyperbulia, hypobulia, abulia, or parabulia), usually related to Verschrobener personality changes.
Pseudopsychopathic
A variant of syndromic remission with predominant acquired personality changes following an acute psychotic episode and demonstrating symptoms and signs relating to typical psychopathy as measured on the Psychopathy Check List - Revised (PCL-R) but without necessarily premorbid evidence of personality disorder.44
Verschrobener-like
Eccentric, quirky, peculiar, odd, strange, queer, crank, extravagant, with unpredictable behavior, usually a consequence of personality changes or shift after an acute psychotic episode (a relatively light variant of pseudopsychopathic deficit syndrome).
Clinical typology of remission in schizophrenia as observed for the SCFRC
Symptomatic, with the participation of positive symptoms
In the treated paranoid type remission patients, there was a delusional component of varying severity. The most characteristic feature was that, despite the presence of encapsulated and actively produced delusions, patients were fully or partially compensated socially; this was observed from historical data for at least 6 months. The same characteristic feature in remission patients was seen with hallucinatory and hallucinatory-paranoid types.
Hypochondria remission was characterized by persistent somatic complaints, followed by a continuous desire to be treated and the presence of senestopatii (somatesthesia) with emotional flattening, isolation, and introversion.
In patients of the obsessive remission type, signs of anankastic temperament, pedantic, unchanging commitment to the daily routine, rituals, propensity to household rechecking, and transient obsessive flashes (blasphemous thoughts, contrasting obsessions, obsessive doubts) were observed.
The thymopathic type of remission was characterized by the presence of mood change, such as of postschizophrenic depression (F20.4, ICD10), or cyclothymia, hyperthymia, or depression, which developed during recovery in affective and delusional episodes.
Syndromic, with predominant negative symptoms and personality changes – “deficit syndrome”
Asthenic remission patients were defined by the presence of elevated reactivity, vulnerability, fragility, lability, hyperesthesia, and rapid exhaustion. They were prone to feebleness and weakness. Thus, they were often observed to be more or less closed and had reduced social contact.
The sthenic variants were characterized by well-known tenacity and perseverance in achieving their goals, were productive in their contact with others, and prudent in their work. Despite their focus, they lacked situational understanding and flexibility. They had narrow interests, were emotionally labile, sharp, self-centered, coldly calculating – while being excessively pedantic.
In cases with apathetic remission, the patients were characterized by flattening of emotional displays to the point of emotional dullness, with lack of interests, weak motivation, poor accessibility, lack of friends, and passivity. In some, there was a complete indifference to the environment. These patients not only stayed at home, but they could perform simple household work, while either partially or completely taking care of themselves.
The clinical features of pseudopsychopathic-type remission included emotional and volitional impairment and, in particular, the inability to inhibit desires and to submit to the demands of others, with a lack of a sense of duty, responsibility, and persistent successive interests, and the presence of affective flatness, emotional shallowness, and moral coarsening, excessive egocentrism, explosive, combustible, and inability to empathize. In remission of the dependent personality type, Verschroben-like, and autistic changes were characteristic features, which included a reduced need for social contact and emotional attachment. These patients were shut off from the outside world, inaccessible, isolated, “unsociable”, and “gloomy”. They were also characterized by an autistic tendency, demonstrating vagueness of judgment, pedantry, and pretentiousness.
References
Andreasen NC, Carpenter WT Jr, Kane JM, et al. Remission in schizophrenia: proposed criteria and rational for consensus Am. J. Psychiatry. 2005;162:441–449. | |
Liberman RP, Kopelowicz A, Venture J, Gutkind D. Operational criteria and factors related to recovery from schizophrenia. Int Rev Psychiatry. 2002;14(4):256–272. | |
EUFAMI – Remission in schizophrenia – related survey, 2007, Oct. Available from: http://www.eufami.org/images/eufami/main/file/syrvey/%20press%20-%20final.pdf. | |
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders – DSM-IV-TR. 4th edition. Arlington, VA: American Psychiatric Association; 2000. | |
World Health Organization: The ICD-10. Chapter 5. Classification of Mental and Behavioural Disorders. 10th edition. World Health Organization. Geneva – 1994. Available from: http://www.who.int/classifications/icd. | |
Kotsyubinsky AP, Skorik AI, Aksenova IO, et al. Schizophrenia: vulnerability – stress – diathesis – disease. – Saint-Petersburg: Hippocrates+, 2004; p. 88–109. Russian. | |
Melekhov DE. Clinical basis for work capacity forecast in schizophrenia. Moscow, Russia. MedGiz. 1963:198. Russian. | |
Morozov VM. Remissions in schizophrenia and work and disability expertise questions. Zhurnal Nevrologii. i Psihiatrii S S Korsakov.1953;10:770–774. Russian. | |
Sverdlov LS. Clinico-psychopathological and clinico-psychological analyses of therapeutic remissions in acute schizophrenia episodes. Biological therapy in rehabilitation system of mentally ill patients. Leningrad, Russia. Meditsina. 1980:48–60. Russian. | |
Vovin R Ya. Remission dynamics in schizophrenia and rational psychopharmacotherapy. Prophylactic and antirecidive therapy of mental diseases. Leningrad. Meditsina. 1986:5–16. Russian. | |
Zenevich GV. Remissions in Schizophrenia. Leningrad, Russia. Meditsina. 1964:216. Russian. | |
Smulevich AB, Andrutshenko AN, Beskova DA. The problem of remission in schizophrenia: clinical and epidemiological study. Zh Nevrol Psikhiatr Im S S Korsakova. 2007;107(5):4–15. Russian. | |
Kay SR, Fizbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. | |
Liddle PF. The symptoms of chronic schizophrenia. A reexamination of the positive-negative dichotomy. Br J Psychiatry. 1987;151: 145–151. | |
Docherty JP, Bossie CA, Lachaux B, et al. Patient-based and clinician-based support for the remission criteria in schizophrenia. Int Clin Psychopharmacol. 2007;22(1):51–55. | |
Haro JM, Novick D, Suarez D, Alonso J, Lépine JP, Ratcliffe M; SOHO Study Group. Remission and relapse in the outpatient care of schizophrenia: three-year results from the Schizophrenia Outpatients Health Outcomes Study. J Clin Psychopharmacol. 2006;26(6):571–578. | |
Helldin L, Kane JM, Karilampi U, Norlander T, Archer T. Remission and cognitive ability in a cohort of patients with schizophrenia. J Psychiatry Res. 2006;40(8):738–745. | |
Leucht S, Beitinger R, Kissling W. On the concept of remission in schizophrenia. Psychopharmacology (Berl). 2007;194(4):453–461. | |
Li CT, Su TP, Chou YH, et al. Symptomatic resolution among Chinese patients with schizophrenia and associated factors. J Formos Med Assoc. 2010;109(5):378–388. | |
Buckley PF, Harvey PD, Bowie CR, Loebel A. The relationship between symptomatic remission and neuropsychological improvement in schizophrenia patients switched to treatment with ziprasidone. Schizophr Res. 2007;94(1–3):99–106. | |
De Hert M, van Winkel R, Wampers M, Kane J, van Os J, Peuskens J. Remission criteria for schizophrenia: evaluation in a large naturalistic cohort. Schizophr Res. 2007;92(1–3):68–73. | |
Gorwood P, Peuskens J; European Group On Functional Outcomes, Remission in Schizophrenia. Setting new standards in schizophrenia outcomes: symptomatic remission 3 years before versus after the Andreasen criteria. Eur Psychiatry. 2012;27(3):170–175. | |
Kane JM, Crandall DT, Marcus RN, et al. Symptomatic remission in schizophrenia patients treated with aripiprazole or haloperidol for up to 52 weeks. Schizophr Res. 2007;95(1–3):143–150. | |
Kurihara T, Kato M, Reverger R, Tirta IG. Remission in schizophrenia: a community-based 6-year follow-up study in Bali. Psychiatry Clin Neurosci. 2011;65(5):476–482. | |
Mosolov SN, Potapov AV, Ushakov UV. Remission in schizophrenia: results of cross-sectional with 6-month follow-up period and 1-year observational therapeutic studies in an outpatient population. Ann Gen Psychiatry. 2012;11(1):1 doi: 10.1186/1744-859X-11-1. | |
San L, Ciudad A, Alvarez E, Bobes J, Gilaberte I. Symptomatic remission and social/vocational functioning in outpatients with schizophrenia: prevalence and associations in a cross-sectional study. Eur Psychiatry. 2007;22(8):490–498. | |
van Os J, Drukker M, à Campo J, Meijer J, Bak M, Delespaul P. Validation of remission criteria for schizophrenia. Am J Psychiatry. 2006;163(11):2000–2002. | |
Wunderink L, Sytema S, Nienhuis FJ, Wiersma D. Clinical recovery in first-episode psychosis. Schizophr Bull. 2009;35(2):362–369. | |
Wolter A, Preuss UW, Krischke NR, Wong WM, Zimmermann J. Remission, prediction and stability of symptoms in schizophrenia: A naturalistic 12-month follow-up study. Int J Psychiatry Clin Pract. 2010;14(3):160–167. | |
Zimmermann J, Wolter A, Krischke NR, Preuss UW, Wobrock T, Falkai P. Response and remission in schizophrenic subjects. Nervenarzt. 2011;82(11):1440–1448. German. | |
Levine SZ, Rabinowitz J, Ascher-Svanum H, Faries DE, Lawson AH. Extent of attaining and maintaining symptom remission by antipsychotic medication in the treatment of chronic schizophrenia: evidence from the CATIE study. Schizophr Res. 2011;133(1–3):42–46. | |
Lasser RA, Bossie CA, Gharabawi GM, Kane JM. Remision in schizophrenia: Results from a 1-year study of long-acting risperidone injection. Schizophr Res. 2005;77(2–3):215–227. | |
Mosolov SN, Potapov AV, Dediurina IUM, Ushakov UV, Tsukarzi EE. The validation of international criteria for remission in schizophrenia in the outpatient population. Zh Nevrol Psikhiatr Im S S Korsakova. 2010;110(5):71–75. Russian. | |
Wobrock T, Köhler J, Klein P, Falkai P. Achieving symptomatic remission in out-patients with schizophrenia – a naturalistic study with quetiapine. Acta Psychiatr Scand. 2009;120(2):120–128. | |
Eberhard J, Levander S, Lindström E. Remission in schizophrenia: analysis in a naturalistic setting. Compr Psychiatry. 2009;50(3):200–208. | |
Lambert M, Schimmelmann BG, Naber D, et al. Prediction of remission as a combination of symptomatic remission and adequate subjective well-being in 2960 patients with schizophrenia. J Clin Psychiatry. 2006;67(11):1690–1697. | |
Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33. | |
Mosolov SN. Scales of psychometric assessment in schizophrenia and conception of positive and negative syndromes, Moscow, Russia, Novy Tsvet, 2001. Russian. | |
Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329. | |
Weiden P, Rapkin B, Mott T, et al. Rating of medication influences (ROMI) scale in schizophrenia. Schizophr Bull. 1994;20(2):297–310. | |
Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl. 1970;212:11–19. | |
Lambert M, Karow A, Leucht S, Schimmelmann BG, Naber D. Remission in schizophrenia: validity, frequency, predictors, and patients’ perspective 5 years later. Dialogues Clin. Neurosci. 2010; 12(3):393–407. | |
Emsley R, Chiliza B, Asmal L, Lehloenya K. The concepts of remission and recovery in schizophrenia. Curr Opin Psychiatry. 2011;24(2):114–121. | |
Hare RD. A research scale for the assessment of psychopathy in criminal populations. Personality and Individual Differences. 1980;1(2):111–119. Available from: http://dx.doi.org/10.1016/0191-8869(80)90028-8. Accessed January 6, 2014. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.