Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Describing the characteristics, treatment pathways, outcomes, and costs of people with persistent noncancer pain managed by community pain clinics and generating an indicative estimate of cost-effectiveness: feasibility study protocol
Authors Al-Aujan S, Saja Almazrou, Knaggs R, Elliott R
Received 9 October 2015
Accepted for publication 17 December 2015
Published 18 May 2016 Volume 2016:9 Pages 237—245
DOI https://doi.org/10.2147/JMDH.S97904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shiekha AlAujan,1 Saja AlMazrou,1 Roger D Knaggs,1,2 Rachel A Elliott1
1Division for Social Research in Medicines and Health, The School of Pharmacy, University of Nottingham, Nottingham, UK; 2Pharmacy Department and Pain Management Service, Nottingham University Hospitals NHS Trust, Nottingham, UK
Background: Low back pain (LBP) and fibromyalgia (FM), also known as chronic widespread pain (CWP), are highly prevalent chronic painful conditions that have substantial impact on patients, health care systems, and society. Diagnosis is complex and management strategies are associated with various levels of evidence for effectiveness and cost-effectiveness. Multidisciplinary pain services have been shown to be effective in some settings and therefore are recommended by clinical practice guidelines as a rational treatment option to manage these patients. Knowing that these services are resource intensive, evidence is needed to demonstrate their cost-effectiveness. This study aims to describe the management of patients with LBP and FM in two community pain clinics to derive an indicative estimate of cost-effectiveness compared with standard practice.
Methods: This is a prospective observational multicenter study, using patient-level data. The data from this study will be combined with modelling of the long-term economic impact of community pain clinics in treating people with LBP and FM. Newly referred patients with LBP and FM who provide written consent will be included. We will collect data on functional disability, pain intensity, quality of life, and health resource utilization. Follow-up data at the 3- and 6-month points will be collected by patient-completed questionnaires and health care contact diaries. Health care resource use from diaries will be compared with patient electronic records to assess the agreement between these recording methods. Patient cohort characteristics, treatment pathways, resource use, and outcomes derived from this study will be integrated in a decision analysis model to assess the cost-effectiveness of community pain clinics compared with standard care. This feasibility study will address key methodological issues such as sample estimates and retention rate to inform the design of a future randomized controlled trial.
Keywords: community pain clinics, back pain, fibromyalgia, cost-effectiveness
Introduction
Low back pain (LBP) and fibromyalgia (FM), which is also known as chronic widespread pain (CWP), are highly prevalent worldwide,1,2 affecting 9.4% and 2.7% of the general population, respectively.3,4 Both conditions have substantial effects on physical function, psychological well-being, and quality of life.5–10 According to the global burden of disease study in 2010,11 back pain was the leading cause of years lived with disability and the third leading cause of disability adjusted life years (DALYs) after ischemic heart disease and chronic obstructive pulmonary disease.
The economic burden of both conditions is also substantial. People with these conditions are regarded as great utilizers of health care resources.12–15 Recently, it has been reported that health resource utilization such as prescriptions and visits for patients with back pain and FM were double those of the matched controls.14,15 In the United Kingdom,15 primary care consultations and referral to secondary care for LBP accounted for 58% and 22.3% of the total health care costs for back pain, respectively. Furthermore, indirect costs to society are significant, due to lower productivity and higher absenteeism.16,17
Managing these conditions is challenging due to many factors. First, the etiology is complex and not specific.18–20 Also, they can be exacerbated by a wide range of sociodemographic and psychosocial factors such as illness behavior beliefs and distress.18,21,22 Therefore, no single treatment is adequate to control all symptoms.
In order to manage pain within a biopsychosocial framework, which addresses pain as a dynamic interaction between physiological, social, and psychological elements, a multidisciplinary management approach is recommended by national and international guidelines.21,23–25 Effectiveness of the multidisciplinary management approach has been widely investigated in LBP and FM.
In LBP, a systematic review of randomized controlled trials suggested that multidisciplinary pain services are more effective than standard care (SC) in reducing functional disability using the Roland Morris Disability (RMD) score (standardized mean difference [SMD]: 0.23, 95% confidence interval [CI]: 0.06–0.4) and pain intensity using visual analogue scale (VAS) (SMD: 0.21, 95% CI: 0.04–0.37).26 In 2008, results from a systematic review indicated that multidisciplinary pain services were better than standard medical treatment in FM.27 However, results are inconclusive due to the great variability of the interventions, outcomes, and study durations. The major limitation with these systematic reviews is that the methodological quality of most studies included was low.
Given that multidisciplinary pain services are resource intensive;28,29 evidence is needed to demonstrate the cost-effectiveness of these services in LBP and FM. A small number of cost-effectiveness studies have been undertaken in Europe and the USA,30–40 others are still in progress in Spain and the Netherlands.41,42 These studies were conducted alongside clinical trials; however, they have methodological limitations in study design. Compliance to treatment was either inadequate32,33,35,36,38–40 or not clearly reported.30,31,37 Moreover, some aspects of treatments/sessions did not appear to be equally used by all participants.32,34,36,38 Therefore, the effect cannot be directly attributed to multidisciplinary pain service.
In addition, threats to external validity may impede the application of the results to real practice.43 These threats come from restrictive patient eligibility criteria such as employees,30,33 recruiting from various practice settings, ie, primary and secondary care setting, and variability of intervention. This variability is either between intervention in terms of treatment components and health care staff or between study participants.
Among these studies, a wide range of comparators were used such as surgery36,37 physiotherapy/exercise,32,39,40 and cognitive behavioral therapy.32,34,39,40 Six studies compared multidisciplinary pain service with usual care.30,31,33,38–40 The definition of usual care varies according to the country and study context, this will also limit the applicability of results. Therefore, results about the cost-effectiveness of these services have been inconclusive because of the variety of interventions, participants, and outcome measures.
Community pain clinic in Nottingham
The project will take place in two community pain clinics (CPC) in Nottingham, UK. These two clinics are operated by the same clinic staff, therefore, the type and quality of health care provided are the same in both clinics. Patients may have consultations with members of the multidisciplinary team (including a pain consultant, a physiotherapist, a biopsychosocial practitioner, and a nurse) for supported self-care management, or community services such as physiotherapy, or more specialist secondary care services. The community pain clinic facilitates access to a wide range of diagnostic and treatment pathways such as MRI, rehabilitation programs, and minor procedures such as trigger point injections. In addition, complex surgical interventions can be offered. Further details on the community pain clinic in Nottingham can be found in the review by Hobbs and Knaggs.44
LBP and FM represent the majority of patients referred to the clinic, therefore these conditions will be the main focus of this study.
Before establishing the CPC, patients with LBP and FM were treated initially by their GPs. If treatment failed to improve patients’ outcomes, then referrals to secondary care may have been considered. This SC pathway may lead to increased rates of development of chronic pain due to the delay in diagnosis and treatment and the long waiting time to be referred to secondary care.45–47 Alongside the detrimental effects of treatment delay, there appears to be a high level of inappropriate spinal surgery unit referrals, suggesting that more targeted use of this service is needed.48
Anecdotally, impressions are that patients are benefiting from the CPC and if it were expanded, patients in the locality would benefit from better pain management. However, financial constraints prevent the possibility of expanding, or even continuity, of the current service. Evidence so far suggests that multidisciplinary pain clinics can be effective, although the effectiveness of the Nottingham CPC is not known. Given that it is likely that these types of services are highly costly and require integration between health care sectors, the effectiveness, patient acceptability, and cost-effectiveness of CPCs needs to be investigated.
Electronic administrative records can be used to estimate health resource use. It reduces data recording burden for patients, and generally provides more detail about types of health care contacts. However, the data can be time-consuming to access, and may only be reliable and complete for a specific sector (eg, hospital stays are not always recorded reliably in GP recording systems49). In addition, in the management of LBP, we envisage that people will use other treatments maybe outside the NHS, such as private osteopathy and physiotherapy. Patient diaries allow us to capture that patient cost. Therefore, in this observational study, we will use both methods to capture resource use data to allow us to assess which method is more reliable for future work in this patient group.
Commissioners and decision makers need support to make decisions about service provision, so waiting for the full evaluative trial to be completed will not produce timely evidence to support decision-making. It has long been recognized that economic evaluation should be iterative, generating progressively firmer estimates of cost-effectiveness and helping to maximize the efficiency of health care research and development, while still allowing the best evidence available at any one time to support decision-making.50 Therefore an indicative economic evaluation will be carried out to compare the cost-effectiveness of CPC and SC in managing LBP and FM using published estimates of effectiveness and cost.
The paucity of economic evaluations of multidisciplinary pain management services and the variable levels of evidence underpinning the effectiveness of these services suggest that cost-effectiveness studies need be conducted before this model of care is more widely implemented. Therefore, the aim of this study is to carry out an evaluation of the CPC in Nottingham to inform decision-makers and commissioners about the effectiveness and cost-effectiveness of this service and, therefore, allocating resources in an efficient manner.
Specific objectives are to:
- Describe the demographic characteristics of patients with LBP and FM and their treatment pathway in the CPC.
- Determine clinical outcomes and health care costs of the CPC using patient reported outcome measures and routinely recorded health care resource use.
- Assess the reconciliation between patient-reported and routinely recorded health care resource use data and derive cost estimations by combining the two methods.
- Derive indicative estimates of cost-effectiveness of CPC compared with SC in managing LBP and FM combining data from this study with published estimates of effectiveness for multidisciplinary pain clinics and long-term costs and outcomes associated with LBP and FM.
- Inform the design of a future cluster randomized trial to evaluate the effectiveness and cost-effectiveness of CPC.
Methods
Study design
This is a prospective observational multicenter study, using patient-level data. The data from this study will be combined with modelling of the long-term economic impact of community pain clinics in treating people with LBP and FM. The study design is summarized in Figure 1.
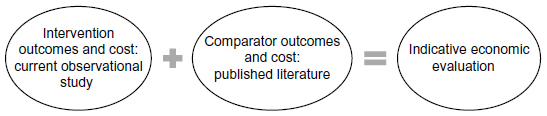 | Figure 1 Overall study design. |
Study setting
The study will be conducted at the Nottinghamshire primary–secondary care interface. Newly referred patients to Nottingham West Clinical Commissioning Group and Newark and Sherwood CCGs who fit the eligibility criteria will be invited. Recruiting from two clinics will increase the number of participants, and therefore the study will be powered to detect difference in primary outcomes.
Sample size and justification
This is not an interventional study; so, a sample size is not required to derive an effect size. However, the sample obtained in this study will provide data to inform a future sample size calculation. The largest sample possible is also required to provide richer information about the patient cohort using CPC for LBP and FM.
Ethical approval
Ethical approval for the study has been obtained from North East York and East Midland-Nottingham 1 Research Ethics Committees (REC reference numbers 15/NE/0162 and 15/EM/0190).
Inclusion criteria
- Adults (18 years or older), attending the pain clinic for the first time and who have LBP or FM for at least 3 months.
- Participants will be required to have good understanding of the English language and the ability to understand study documents and provide written consent.
As this study will include patients with different disease states, the exclusion criteria for each condition is listed below:
Exclusion criteria for people with low back pain
- Having an underlying organic pathology for low back pain such as infection or cancer.
- Having had a spinal surgical procedure in the past 6 weeks or having to undergo surgery within 3 months.
- Having severe psychiatric disorders such as major depression or psychosis.
- Being pregnant or having given birth in the past 3 months.
Exclusion criteria for people with fibromyalgia
- Not having a confirmed diagnosis of FM.
- Having severe psychiatric disorders such as major depression or psychosis.
Outcome measures
Disease-specific outcome measures will be used for each disease group population. Roland Morris Disability Questionnaire51 will be used to assess the functional disability for patients with LBP and to assess the functionality of patients with FM the Revised Symptoms Impact Questionnaire (SIQR)52 will be used.
Pain intensity will be measured using the short-form Brief Pain Inventory (BPI),53 whereas health status will be assessed by EuroQol-5 Dimension-3 level instrument (EQ-5D-3L).54 A summary of the outcome measures recorded during the study is provided in Table 1.
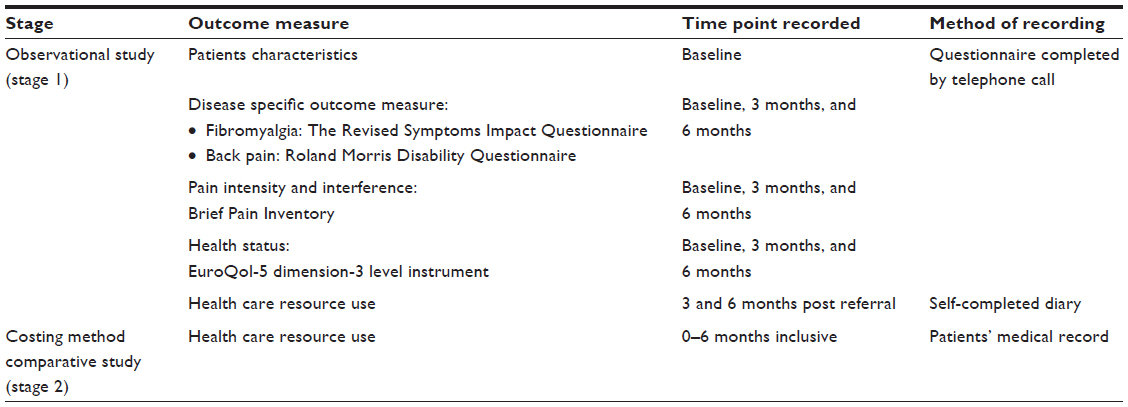 | Table 1 Summary of collected data |
Study regimen
This study will involve three main stages. For each stage, the aim, methodological features, outcome measures or data collected, and duration are described below.
Stage 1: observational study – assess the clinical outcomes and health care use in CPC
The pain clinic consultant will have the responsibility of identifying eligible patients at triage.44 The initial patient approach will be from the pain clinic consultant, who will inform the participant of all aspects pertaining to participation in the study.
The questionnaires will be piloted using a small number of patients (approximately 5–10 patients) attending the two CPCs to examine the type, accuracy, and practicality of resource use data collection tools and outcome measure tools.55 These patients will be included in the final analysis if no further amendments to the study design or data collection tools are made.
This pilot study will follow the same procedure of the main study in terms of identification, recruitment, and contact method. The main study will follow the procedure detailed: The pain clinic consultant will identify and invite eligible patients to take part in the study and will explain the study to the eligible patient. If the patient has initially expressed interest in being involved in the study, the consultant will provide the patient with the study information pack. The patient will be asked to provide his/her contact details by clinic staff to arrange a telephone call with the researcher within 24–72 hours to allow the patient to consider participation in the study. To maximize retention of the study participants, each patient will determine the preferred time slot of the day for researcher to contact him/her.
Within 24–72 hours of the initial patient encounter, the researcher will contact the patient to confirm the consent and answer any questions related to the study. The patient will need to sign the consent form and send it back to the researcher by post.
The patient will be asked to answer questions related to his/her baseline pain, physical function, and health status. In addition, demographic data of patients will be obtained. The researcher will contact the patient by phone to collect clinical outcome data after 3 and 6 months. Patients will be encouraged to record their health resource use using diaries. These diaries will be returned by post at 3 and 6 months.
Stage 2: assess the agreement between patients’ self-reported health resource use and medical records in CPC
This stage aims to assess health care utilization data collection methods, when resource use data are obtained from either medical records or patient self-report using a diary, by assessing the reconciliation between these two approaches and resulting cost estimations derived from the resource use data obtained. Health care resource use data from the previous stage, using patient-reported methods, will be compared with health care resource data elicited from medical records of CPC patients.
These data will be collected retrospectively for 6 months from the date of CPC referral. A data analyst will extract the data required. Data extracted will include medication use and primary and secondary health care service use; principally GP visits, emergency department visits, inpatient, outpatient attendances, and other community services (ie, physiotherapy). The data will be extracted from GP practices that use SystmOne56 and EMIS57 to record patients’ data electronically.
Stage 3: indicative economic evaluation
Data collected from the study will be used to inform an indicative economic evaluation. Cost-effectiveness will be investigated by generating differences in costs and outcomes between SC and CPC. Published evidence on costs and outcomes for SC will be combined with outcomes and costs from the patient cohort in this study to generate mean incremental quality adjusted life years (QALY) and costs. The data will be gathered from participants for 6 months. The costs and benefits of CPC will be calculated over a 6-month period (short term). The long-term (5–10 years) costs and outcomes will be estimated using decision analysis modelling. This period will be sufficient to observe the effect of intervention on costs and outcomes;58 therefore, two models will be constructed. The data sources for the two models are illustrated in Table 2.
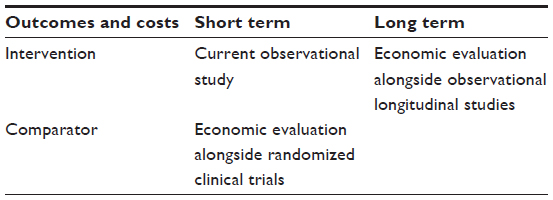 | Table 2 Data sources for economic models |
The costs will be collected from health provider perspective. Intervention cost will be calculated using a “bottom–up” approach. Patients’ visits to CPC and the types of treatments received will be gathered from the medical records. Direct medical cost such as visits to GP, nurses, other health care professionals, and hospitals will be recorded in costing diary. Direct nonmedical costs such as travel expenses will be also recorded in costing diary. These diaries will be administered twice during the study (3 months period).
Direct health care costs will be obtained from the following sources: costs of treatment interventions and investigations will be derived from NHS reference costs,59 costs of health staff from the Personal Social Services Research Unit (PSSRU),60 and medication costs from the British National Formulary61 (March–September 2015). All costs will be expressed in 2015–2016 pounds sterling. The discount will be applied in the long-term model only; we will discount effects and costs at an annual rate of 3.5%. The UK Treasury recommended 3.5% discount rate for both costs and outcomes.62 In addition, different discount rates will be tested in the sensitivity analysis.
Short term
We will conduct a short-term (6 months) cost-effectiveness decision analysis model from NHS perspective. Markov model inputs will be based on the data derived from the current observational study and published literature. The short-term effect of SC on outcomes and cost will be obtained by conducting a systematic review of cost-effectiveness studies of multidisciplinary pain management services in LBP and FM.
Long term
The long-term benefit of multidisciplinary pain management services needs to be evaluated as these services are cost intensive. Moreover, little is known about the long-term effectiveness. Therefore, the model input will be based on data from published literature. Longitudinal observational studies which aim to evaluate the effectiveness and cost-effectiveness of multidisciplinary pain management services in LBP and FM will be used. The data source for the models is illustrated in Table 2.
Analyses
Stage 1: observational study
We will describe the study population and their outcomes using simple descriptive statistics, percentages for categorical, and mean and SD for continuous variables.
Changes within outcome measures over the duration of the study will be assessed using paired t-tests for continuous data and McNemar tests for dichotomous data.
Unit costs will be combined with resource-use from the two collection methods to generate two estimates of patient-level costs.
We will determine baseline factors associated with change of outcome measures or cost over the course of patient follow-up. This will be performed using multiple linear and logistic regression for continuous and binary outcome variables, respectively. P-values less than 0.05 will be considered statistically significant.
Stage 2: costing methods comparative study
Nonparametric bootstrapping will be used to compare arithmetic means of costs data.63 Pairwise t-tests will be applied to the data generated by bootstrapping. Level of agreement between electronic and self-reported resource-use will be estimated by using the Lin concordance correlation coefficient,64 which can be applied to nonnormally distributed data such as resource use data. The Lin coefficient value lies between 1, indicative of perfect agreement, and –1, indicative of perfect inverse agreement.
Stage 3: indicative economic evaluation
This economic study will be performed according to the intention-to-treat principles. For missing data during follow-up, we will use complete case analysis.
We will carry out incremental analysis, which is mean difference in cost between CPC and SC divided by the mean in QALY difference to generate incremental cost-effectiveness ratio (ICER). Nonparametric bootstrapping with 1,000 iterations will be used to calculate the confidence interval around the ICER and cost difference.
To assess the robustness of the results, deterministic univariate and multivariate sensitivity analyses will be performed. Probabilistic sensitivity analysis (PSA) will be undertaken for base-case scenario and univariate and multivariate analysis. Sampling incremental costs and QALY will be conducted by Monte Carlo simulation using TreeAge Pro. We will use cost-effectiveness planes and cost-effectiveness acceptability curves (CEACs) to present the results. All statistical analyses will be conducted using STATA 11.1.65 TreeAge Pro66 will be used to build the decision analysis model.
Discussion
The major strengths in this study design are that we will use validated gold standard measures for each of these patient outcomes to assess which best reflects the success and acceptability of the service from the patient perspective. We also need to obtain detailed information on treatment pathways. This is essential to understand the nature and variability of the complex intervention. It is also needed to allow us to estimate resource use and cost, associated with managing patients by the CPC. Treatment pathway and associated resource use data can be obtained either by accessing routine medical records, or by patient report. Neither method is without its limitations. In this study, we will use both methods to capture resource use data to allow us to assess which method is more reliable for future work in this patient group.
Moreover, the choice of study design was based on the Medical Research Council (MRC) recommendation for evaluating complex intervention. Multidisciplinary pain clinics such as the Nottingham CPC are considered as “complex” interventions. This complexity is derived by the number of interacting components within the clinic and variety of intended outcomes. There are known difficulties and methodological challenges in evaluating complex interventions. The MRC published a framework which recommends evaluating the intervention through observational and developmental work, followed by an exploratory trial before conducting the definitive evaluation. This is required to identify key uncertainties in the design and assessment of the intervention and its evaluation.67
Recruitment and retention rates are major limitations on any prospective study design. In this study, several data collection methods were considered, such as postal questionnaires, face-to-face interviews, and phone calls. However, there are some practical difficulties in using interviews, as patients may be referred to other health care specialists outside the clinic during the study period. For postal questionnaires, there is a risk of low response rate. Given that the study period is relatively short (6 months), telephone calls were chosen for data collection over other methods to maximize the response rate and to facilitate patient tracking. In addition, each patient will determine the preferred time slot of the day for researcher to contact him/her. If the patients did not respond to the first phone call, the researcher will contact the patient twice within 1 hour. The total number of calls will be three times, each is 20 minutes apart. Another attempt will be made on the following day in case of no response. Furthermore, the patient will be approached by letter to re-establish the contact. Participants who do not respond to phone calls after these attempts will be presumed to have withdrawn from the study and no further contact will be made.
Acknowledgments
All patient-related paperwork, which include questionnaires, diaries, patient information sheet, and the consent form have been reviewed by Antony Chuter. Mr Chuter has significant experience in providing the patient perspective to health services research projects; he was the PPI coinvestigator for an evaluation of the New Medicine Service Project and worked with the Expert Patient Program, Royal College of General Practitioners, and currently he is Chair of the Patient Liaison Committee (British Pain Society) and Chair of Pain UK.
Disclosure
SA and SA are funded by doctoral studentships from the Ministry of Higher Education in Saudi Arabia. The authors report no other conflicts of interest in this work.
References
Kohlmann T. [Musculoskeletal pain in the population]. Schmerz. 2003;17(6):405–411. German | |
Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656. | |
Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. | |
Queiroz LP. Worldwide epidemiology of fibromyalgia. Curr Pain Headache Rep. 2013;17(8):356. | |
Yilmaz F, Sahin F, Ergoz E, et al. Quality of life assessments with SF-36 in different musculoskeletal diseases. Clin Rheumatol. 2008;27(3):327–332. | |
Verbunt JA, Pernot DH, Smeets RJ. Disability and quality of life in patients with fibromyalgia. Health Qual Life Outcomes. 2008;6(8):1477–7525. | |
Birtane M, Uzunca K, Tastekin N, Tuna H. The evaluation of quality of life in fibromyalgia syndrome: a comparison with rheumatoid arthritis by using SF-36 Health Survey. Clin Rheumatol. 2007;26(5):679–684. | |
Hoffman DL, Dukes EM. The health status burden of people with fibromyalgia: a review of studies that assessed health status with the SF-36 or the SF-12. Int J Clin Pract. 2008;62(1):115–126. | |
Buchbinder R, Blyth FM, March LM, Brooks P, Woolf AD, Hoy DG. Placing the global burden of low back pain in context. Best Pract Res Clin Rheumatol. 2013;27(5):575–589. | |
Froud R, Patterson S, Eldridge S, et al. A systematic review and meta-synthesis of the impact of low back pain on people’s lives. BMC Musculoskelet Disord. 2014;15:50. | |
Murray CJL, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448–457. | |
Wolfe F, Anderson J, Harkness D, et al. A prospective, longitudinal, multicenter study of service utilization and costs in fibromyalgia. Arthritis Rheum. 1997;40(9):1560–1570. | |
Robinson RL, Birnbaum HG, Morley MA, Sisitsky T, Greenberg PE, Claxton AJ. Economic cost and epidemiological characteristics of patients with fibromyalgia claims. J Rheumatol. 2003;30(6):1318–1325. | |
Hughes G, Martinez C, Myon E, Taieb C, Wessely S. The impact of a diagnosis of fibromyalgia on health care resource use by primary care patients in the UK: an observational study based on clinical practice. Arthritis Rheum. 2006;54(1):177–183. | |
Hong J, Reed C, Novick D, Happich M. Costs associated with treatment of chronic low back pain: an analysis of the UK General Practice Research Database. Spine. 2013;38(1):75–82. | |
Knight T, Schaefer C, Chandran A, Zlateva G, Winkelmann A, Perrot S. Health-resource use and costs associated with fibromyalgia in France, Germany, and the United States. Clinicoecon Outcomes Res. 2013;5:171–180. | |
Ricci JA, Stewart WF, Chee E, Leotta C, Foley K, Hochberg MC. Back pain exacerbations and lost productive time costs in United States workers. Spine. 1976;31(26):3052–3060. | |
Fourney DR, Andersson G, Arnold PM, et al. Chronic low back pain: a heterogeneous condition with challenges for an evidence-based approach. Spine. 2011;36(21 Suppl):S1–S9. | |
Russell IJ, Larson AA. Neurophysiopathogenesis of fibromyalgia syndrome: a unified hypothesis. Rheum Dis Clinic North Am. 2009; 35(2):421–435. | |
Clauw DJ, Arnold LM, McCarberg BH. The science of fibromyalgia. Mayo Clin Proc. 2011;86(9):907–911. | |
Waddell G. The Back Pain Revolution. Edinburgh, Scotland: Churchill Livingstone; 2004. | |
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. | |
Savigny P, Kuntze S, Watson P, et al. Low Back Pain: Early Management of Persistent Non-Specific Low Back Pain. London, UK: National Collaborating Centre for Primary Care and Royal College of General Practitioners; 2009. | |
Carville SF, Arendt-Nielsen S, Bliddal H, et al. EULAR evidence-based recommendations for the management of fibromyalgia syndrome. Ann Rheum Dis. 2008;67(4):536–541. | |
Keel P. Pain management strategies and team approach. Baillieres Best Pract Res Clin Rheumatol. 1999;13(3):493–506. | |
Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst Rev. 2014;9:CD000963. | |
Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology (Oxford). 2008;47(5):670–678. | |
Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment and cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain. J Pain. 2006;7(11):779–793. | |
Robinson RL, Jones ML. In search of pharmacoeconomic evaluations for fibromyalgia treatments: a review. Expert Opin Pharmacother. 2006;7(8):1027–1039. | |
Skouen JS, Grasdal AL, Haldorsen EM, Ursin H. Relative cost-effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low back pain on long-term sick leave: randomized controlled study. Spine. 2002;27(9):901–909; discussion 909–910. | |
Luciano JV, Sabes-Figuera R, Cardenosa E, et al. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: an economic evaluation alongside a 12-month randomized controlled trial. Clin J Pain. 2013;29(8):702–711. | |
Smeets RJ, Severens JL, Beelen S, Vlaeyen JW, Knottnerus JA. More is not always better: cost-effectiveness analysis of combined, single behavioral and single physical rehabilitation programs for chronic low back pain. Eur J Pain. 2009;13(1):71–81. | |
Lambeek LC, Bosmans JE, Van Royen BJ, Van Tulder MW, Van Mechelen W, Anema JR. Effect of integrated care for sick listed patients with chronic low back pain: economic evaluation alongside a randomised controlled trial. BMJ. 2010;341:c6414. | |
Goossens ME, Rutten-van Molken MP, Leidl RM, Bos SG, Vlaeyen JW, Teeken-Gruben NJ. Cognitive-educational treatment of fibromyalgia: a randomized clinical trial. II. Economic evaluation. J Rheumatol. 1996;23(7):1246–1254. | |
Gusi N, Tomas-Carus P. Cost-utility of an 8-month aquatic training for women with fibromyalgia: a randomized controlled trial. Arthritis Res Ther. 2008;10(1):R24. | |
Rivero-Arias O, Campbell H, Gray A, Fairbank J, Frost H, Wilson-MacDonald J. Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial. BMJ. 2005;330(7502):1239. | |
Johnsen LG, Hellum C, Storheim K, et al. Cost-effectiveness of total disc replacement versus multidisciplinary rehabilitation in patients with chronic low back pain: a Norwegian multicenter RCT. Spine. 2014;39(1):23–32. | |
Zijlstra TR, Braakman-Jansen LM, Taal E, Rasker JJ, van de Laar MA. Cost-effectiveness of Spa treatment for fibromyalgia: general health improvement is not for free. Rheumatology. 2007;46(9):1454–1459. | |
McBeth J, Prescott G, Scotland G, et al. Cognitive behavior therapy, exercise, or both for treating chronic widespread pain. Arch Intern Med. 2012;172(1):48–57. | |
Beasley M, Prescott GJ, Scotland G, et al. Patient-reported improvements in health are maintained 2 years after completing a short course of cognitive behaviour therapy, exercise or both treatments for chronic widespread pain: long-term results from the MUSICIAN randomised controlled trial. RMD Open. 2015;1(1):e000026. | |
Berenguera A, Pujol-Ribera E, Rodriguez-Blanco T, et al. Study protocol of cost-effectiveness and cost-utility of a biopsychosocial multidisciplinary intervention in the evolution of non-specific sub-acute low back pain in the working population: cluster randomised trial. BMC Musculoskelet Disord. 2011;12:194. | |
Lambeek LC, Anema JR, van Royen BJ, et al. Multidisciplinary outpatient care program for patients with chronic low back pain: design of a randomized controlled trial and cost-effectiveness study. BMC Public Health. 2007;7:254. | |
Ramsey S, Willke R, Briggs A, et al. Good research practices for cost-effectiveness analysis alongside clinical trials: the ISPOR RCT-CEA Task Force report. Value Health. 2005;8(5):521–533. | |
Hobbs G, Knaggs R. Commissioning for pain management services. Br J Healthc Manag. 2011;17(7):302–306. | |
Melloh M, Elfering A, Kaser A, et al. What is the best time point to identify patients at risk of developing persistent low back pain? J Back Musculoskelet Rehabil. 2015;28(2):267–276. | |
Melloh M, Elfering A, Stanton TR, et al. Low back pain risk factors associated with persistence, recurrence and delayed presentation. J Back Musculoskelet Rehabil. 2014;27(3):281–289. | |
Choy E, Perrot S, Leon T, et al. A patient survey of the impact of fibromyalgia and the journey to diagnosis. BMC Health Serv Res. 2010;10:102. | |
Department of Health. The Musculoskeletal Services Framework. 2006. Available from: http://webarchive.nationalarchives.gov.uk/ 20130107105354/http:/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4138413. Accessed August 18, 2015. | |
Byford S, Leese M, Knapp M, et al. Comparison of alternative methods of collection of service use data for the economic evaluation health care interventions. Health Econ. 2007;16(5):531–536. | |
Sculpher M, Drummond M, Buxton M. The iterative use of economic evaluation as part of the process of health technology assessment. J Health Serv Res. 1997;2(1):26–30. | |
Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;8(2):141–144. | |
Bennett RM, Friend R, Jones KD, Ward R, Han BK, Ross RL. The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. 2009;11(4):R120. | |
Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23(2):129–138. | |
EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. | |
Drummond M, Coyle D. The role of pilot studies in the economic evaluation of health technologies. Int J Technol Assess Health Care. 1998;14(3):405–418. | |
The Phoenix Partnership (TPP). SystmOne. 2015. Available from: http://www.tpp-uk.com/products/systmone. Accessed July 30, 2015. | |
EMIS Health. EMIS. 2015. Available from: https://www.emishealth.com/. Accessed July 30, 2015. | |
Comans T, Raymer M, O’Leary S, Smith D, Scuffham P. Cost-effectiveness of a physiotherapist-led service for orthopaedic outpatients. J Health Serv Res Policy. 2014;19(4):216–223. | |
Department of Health. NHS National Schedule of Reference Costs 2012–2013. 2013. Available from: https://www.gov.uk/government/publications/nhs-reference-costs-2012-to-2013. Accessed August 18, 2015. | |
Personal Social Services Research Unit (PSSRU). Unit Costs of Health and Social Care. 2015. Available from: http://www.pssru.ac.uk/project-pages/unit-costs/. Accessed July 30, 2015. | |
Joint Formulary Committee. British National Formulary. 69th ed. London, UK: BMJ Group and Pharmaceutical Press; 2015. | |
Her Majesty’s Treasury. The Green Book: Appraisal and Evaluation in Central Government: Treasury Guidance Great Britain. London, UK: TSO; 2003. | |
Briggs A, Gray A. The distribution of health care costs and their statistical analysis for economic evaluation. J Health Serv Res Policy. 1998;3(4):233–245. | |
Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45(1):255–268. | |
StataCorp LP. Stata Statistical Software: Release 11.1 [computer program]. College Station, TX: StataCorp LP; 2009. | |
TreeAge Software, Inc. TreeAge Pro 2015: Release 1.0 [computer program]. Williamstown, MA: TreeAge Software, Inc.; 2015. | |
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.